New Alzheimer’s Drugs Spark Hope for Patients and Cost Concerns for Medicare
This post was updated on July 6, 2023, to reflect FDA’s approval of Leqembi, additional details from CMS about patient registries, and updated Medicare spending projections.
The FDA has just granted traditional approval to Leqembi (lecanemab), an anti-amyloid monoclonal antibody treatment for Alzheimer’s disease, after granting accelerated approval this past January. Clinical trial results showed that Leqembi, made by Eisai and Biogen, slowed the rate of cognitive decline and reduced amyloid plaques, the protein that accumulates in the brains of people with Alzheimer’s disease – though not without the risk of adverse events. FDA’s approval of a drug that can slow the progression of cognitive decline in patients with Alzheimer’s disease offers long-awaited hope for these patients and their families, but also raises concerns about the potential impact on Medicare spending.
Now that the FDA has granted traditional approval to Leqembi, Medicare will cover it for all indicated populations – patients with mild cognitive impairment or mild dementia with confirmed amyloid plaques – outside of the randomized clinical trials required for drugs with accelerated approval under Medicare’s coverage with evidence development. At the same time, the Centers for Medicare & Medicaid Services (CMS) will require physicians and other clinicians to participate in prospective data collection efforts for Leqembi users, known as registries, to inform questions about how the drug is working, including benefits and harms to patients and whether it improves health outcomes, based on real-world evidence. CMS has announced it will establish its own registry, to be made available on CMS’s website, and will also provide access to registries established by other organizations on the same site. Yet questions remain about the registry requirement for Leqembi, including whether the data collection system is ready for use, how data about the drug’s benefits and risks will be collected, how easy it will be for providers to participate in the registry, the costs involved with collecting the data, and whether the registry requirement will make it harder for patients to access the drug.
Notwithstanding these questions about the registry requirement and how it might affect access to Leqembi, broader access to the drug under Medicare outside of clinical trials will lead to higher Medicare spending, based on the drug’s annual price of $26,500 and expected demand for it among patients with Alzheimer’s disease. Yet the exact number of Medicare beneficiaries who meet the prescribing requirements for Leqembi is unknown and the take-up rate among eligible individuals for a drug like this one is difficult to estimate.
Eisai has estimated that take-up will be ‘approximately 100,000 individuals by year 3’ – an estimate that some consider conservative – and will increase ‘gradually’ over time. Based on this estimate of take-up, which represents 1.5% of the 6.7 million older adults in the US with Alzheimer’s disease, annual Medicare spending on Leqembi would be $2.7 billion (assuming all are enrolled in Part B), which would make it the third most costly drug covered by Medicare Part B, based on 2021 total spending (Figure 1). If take-up is somewhat higher, for example, 5% of those with Alzheimer’s disease, this would translate to $8.9 billion in total annual spending, while a 10% take-up rate would amount to $17.8 billion.
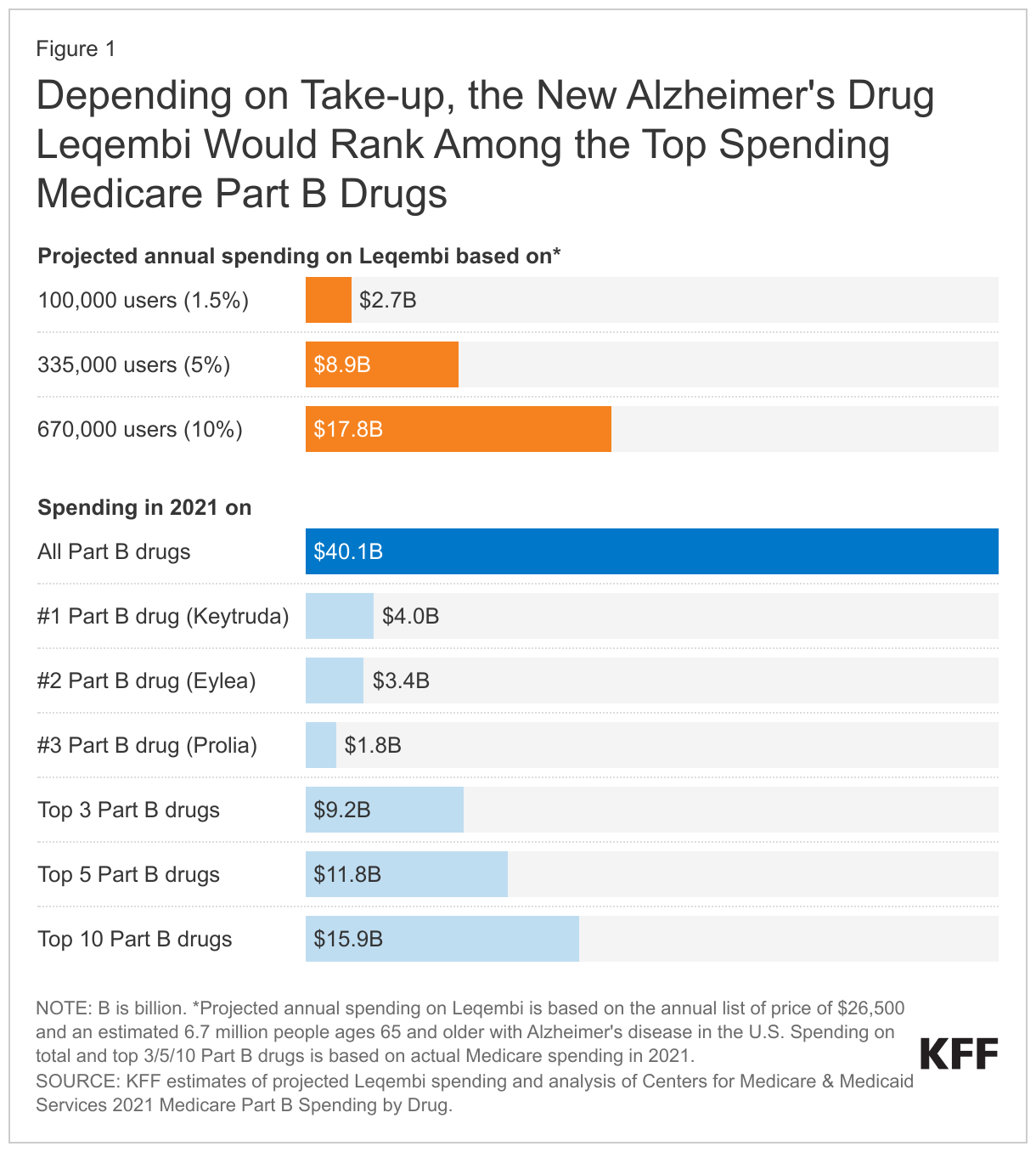
To put these amounts in context, projected Medicare spending on Leqembi would be roughly equal to spending on the top 3 Part B drugs combined in 2021 based on the 5% take-up rate. At the 10% take-up rate, projected spending on this one drug alone would exceed spending on the top 10 Part B drugs in 2021 and would represent close to half of the $40 billion spent in total on the 600+ Part B covered drugs in 2021. And these estimates do not include additional costs to Medicare associated with PET scans or multiple MRIs that may be needed in conjunction with use of Leqembi nor potential offsets if treatment with Leqembi helps reduce spending on other services, such as hospitalizations due to falls or skilled nursing facility stays.
Higher Medicare Part B spending would likely lead to higher Medicare Part B premiums, which are set to cover roughly 25 percent of program costs. In the case of Aduhelm, the anticipation of substantially higher Medicare Part B spending due to coverage of that drug contributed to a 15% jump in the Part B premium between 2021 and 2022, an increase substantially above the norm. Medicare’s subsequent decision to limit coverage of Aduhelm contributed to a modest (3%) decline in the Part B premium for 2023.
At Leqembi’s current $26,500 list price, Medicare patients administered the drug will be responsible for more than $5,000 out of pocket each year, based on a 20% coinsurance requirement in traditional Medicare. Medicare Advantage enrollees are also typically responsible for the 20% coinsurance for Part B drugs up to their plan’s out-of-pocket maximum. (In 2022, the weighted average out-of-pocket maximum in Medicare Advantage plans was nearly $5,000 for in-network services and just over $9,200 for in-network and out-of-network combined). Beneficiaries may pay less if they have supplemental insurance, such as Medigap or Medicaid, that covers Medicare cost sharing. The Inflation Reduction Act includes a new cap on out-of-pocket drug spending under Medicare Part D beginning in 2024 that will provide significant financial relief to people who take high-priced Part D drugs, but there is no similar cap on out-of-pocket spending for drugs, like Leqembi, that are covered under Medicare Part B.
Even with Medicare coverage, therefore, Leqembi could be beyond the reach of many people with Medicare, whose median income is around $30,000 per person. And with higher rates of dementia and lower incomes among older Hispanic and Black adults than among older White adults in the US, the high cost of treatment could raise equity concerns if it means Black and Hispanic beneficiaries are less likely to gain access to this treatment because they can’t afford it.
To address concerns about the effect of high-priced drugs on Medicare program spending, the Inflation Reduction Act requires Medicare to negotiate the price of top spending drugs, but manufacturers of biologic drug products like Leqembi will be exempt from having CMS-negotiated prices take effect for 13 years from the drug’s licensure date. In the case of Leqembi, its manufacturers will have between now and 2036 to recoup investments in research and development and earn revenue from Medicare before possibly having negotiated pricing take effect. While broader access to Leqembi is expected to provide modest clinical benefits to older adults with mild cognitive impairment and mild dementia stage of Alzheimer’s disease, a significant increase in Medicare spending and premiums is a distinct possibility, and one that Medicare, patients, and taxpayers are likely to confront in the not-too-distant future.
This work was supported in part by Arnold Ventures. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.