Key Takeaways
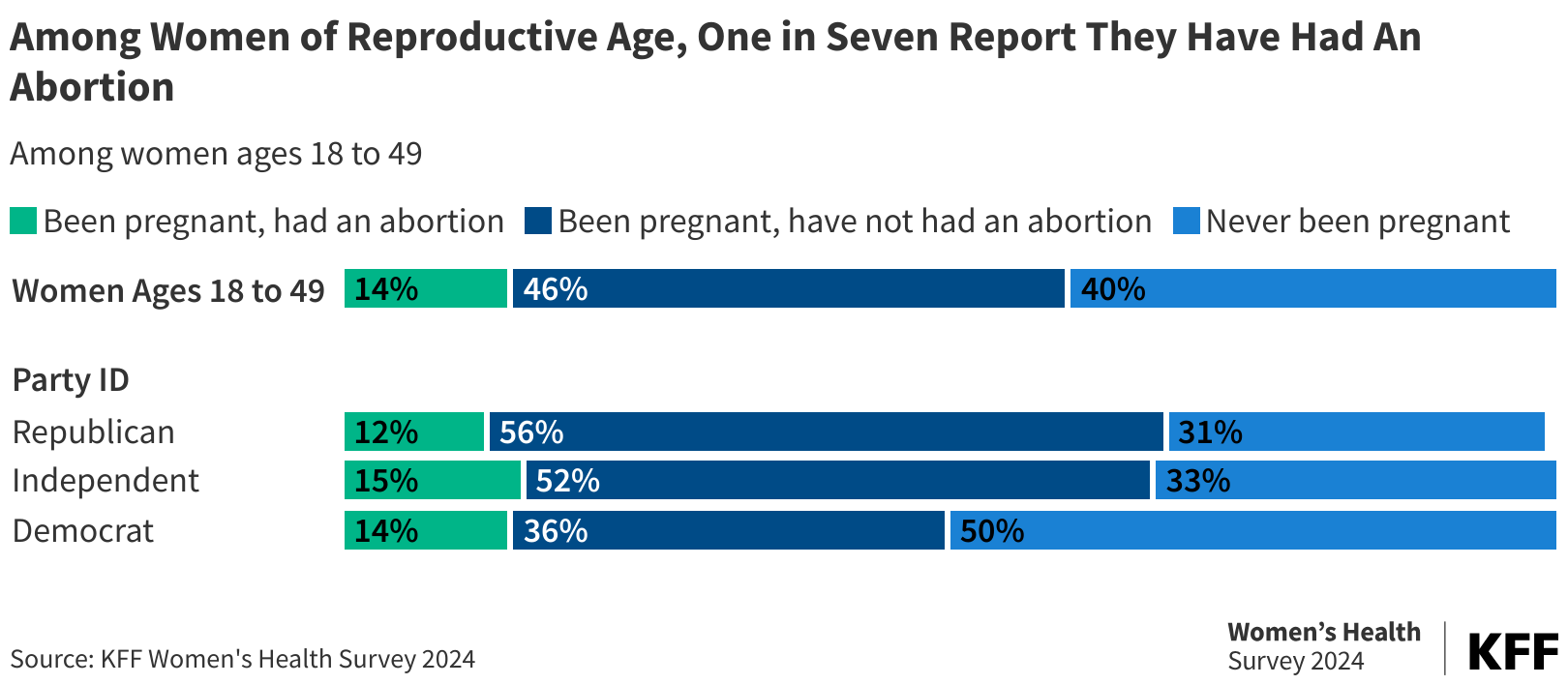
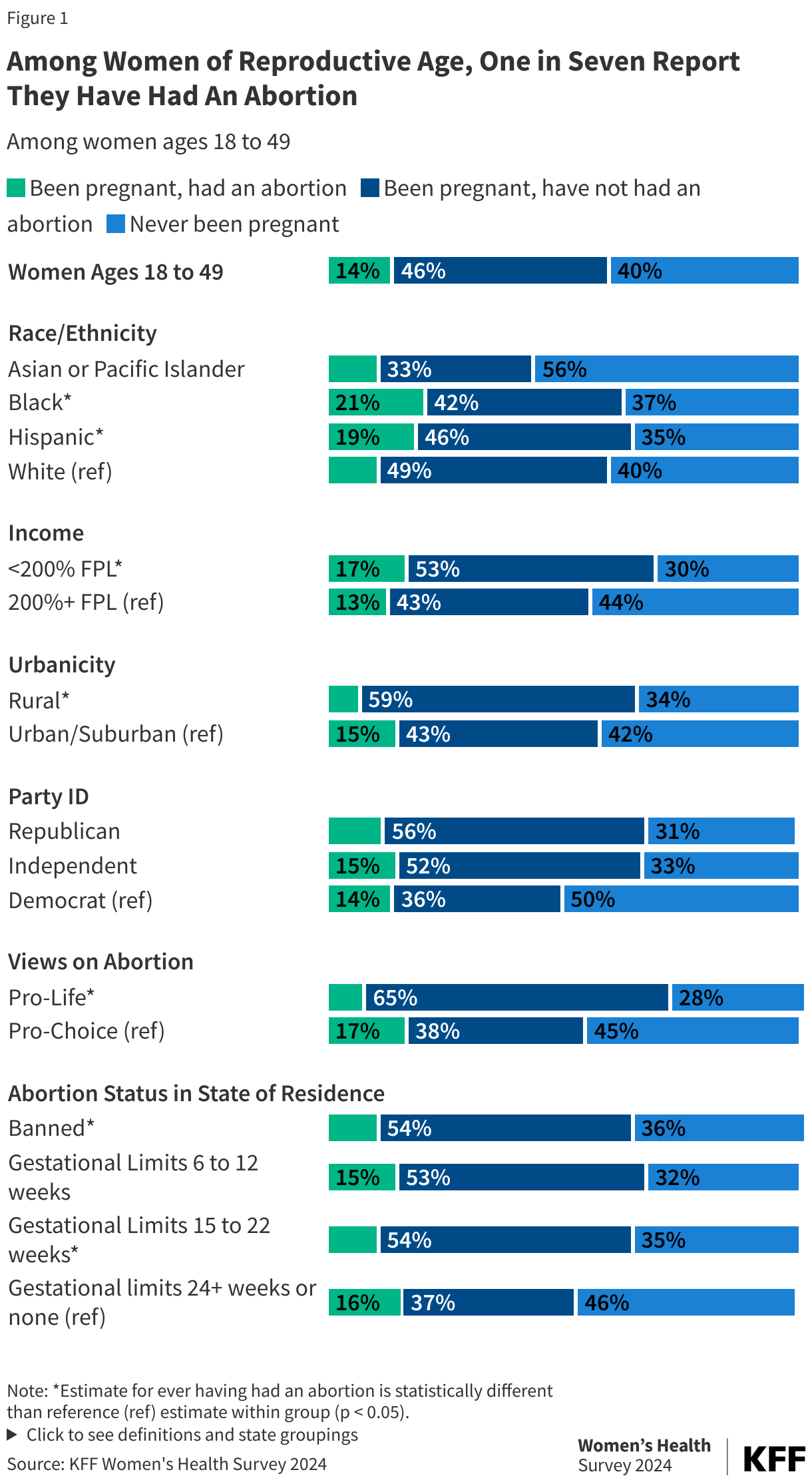
- Among women of reproductive age, one in seven (14%) have had an abortion at some point in their life. Larger shares of Black (21%) and Hispanic (19%) women report having had an abortion compared to 11% of White women. Across partisanship, similar shares of Republican women, Democratic women, and independents report having had an abortion.
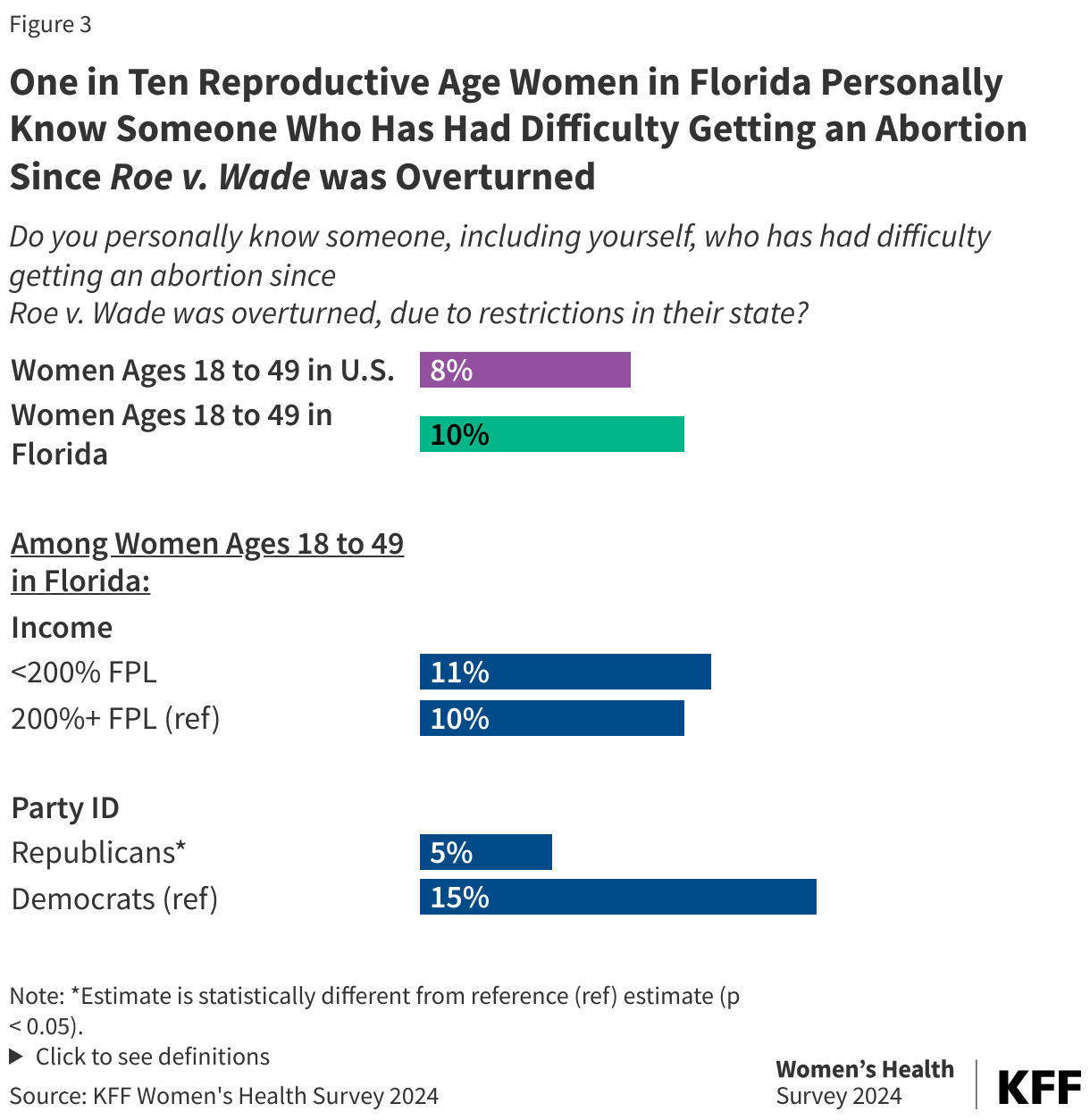
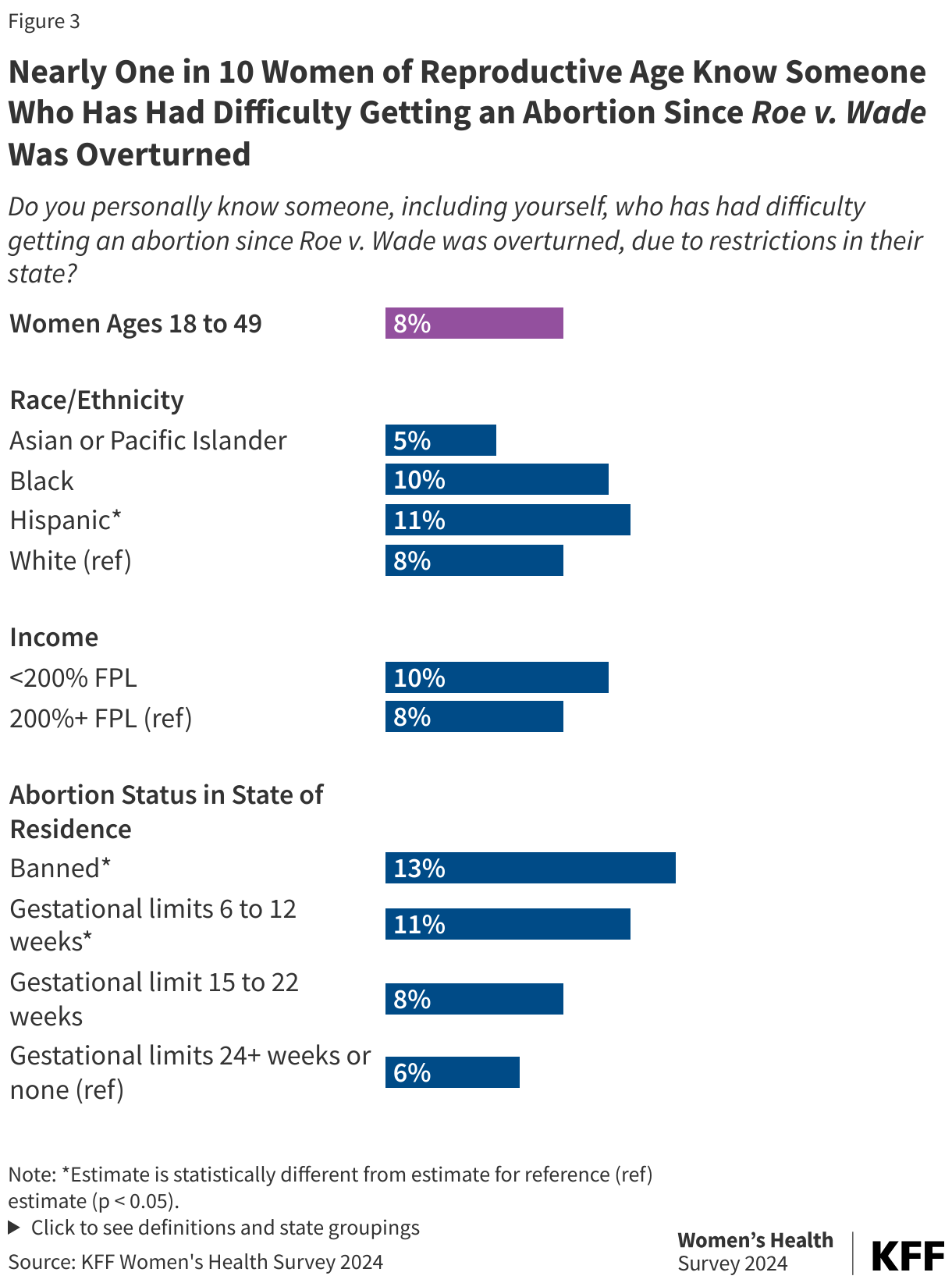
- Nearly one in ten (8%) women of reproductive age personally know someone who has had difficulty getting an abortion since Roe v. Wade was overturned, including 11% of Hispanic women and 13% of women living in states with abortion bans.
- Among women of reproductive age who report knowing someone personally who has had difficulty getting an abortion since Roe v. Wade was overturned, many say they had to travel out of state for care (68%), did not know where to go (40%), and/or did not have the money to cover the cost (35%).
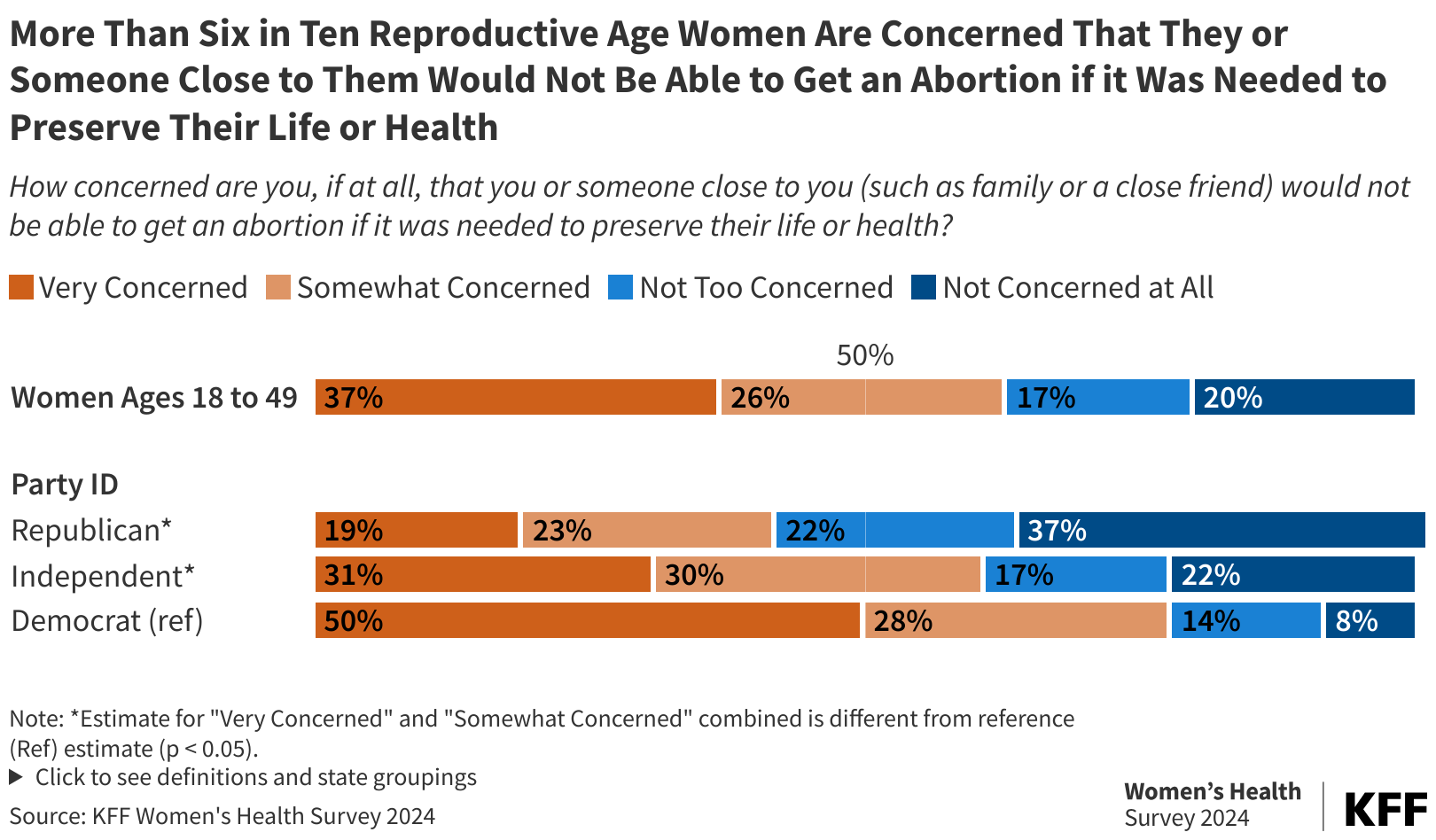
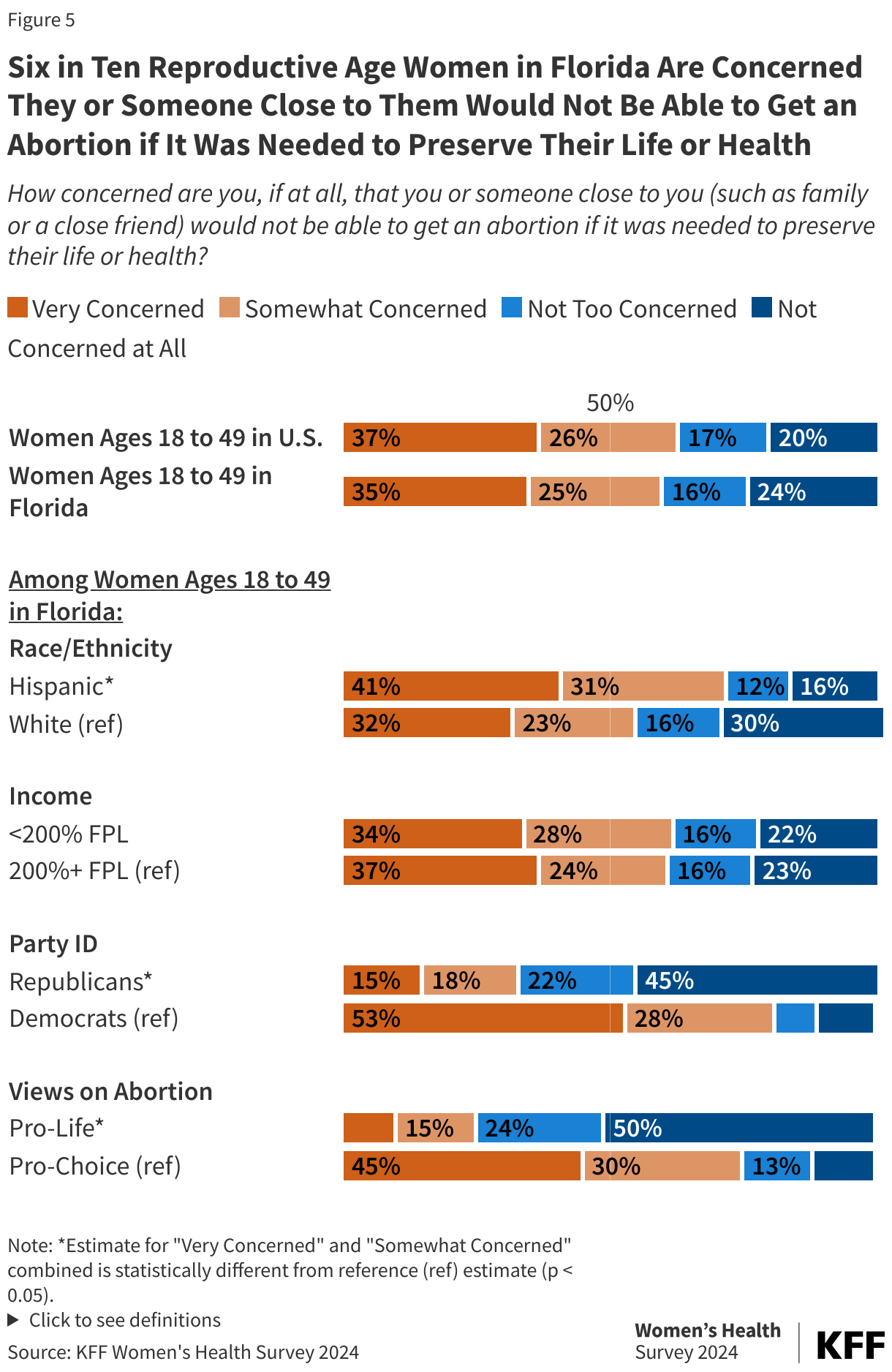
- More than six in ten women of reproductive age are concerned that they, or someone close to them, would not be able to get an abortion if it was needed to preserve their life or health (63%) and that abortion bans may affect the safety of a potential future pregnancy for themselves or someone close to them (64%).
- Less than half of reproductive age women in the United States are aware of the current status of abortion policy in their state (45%). Nearly a quarter describe the status incorrectly (23%) and a third are unsure about the status of abortion in their state (32%).
- One in four (26%) reproductive age women say if they needed or wanted an abortion they would not know where to go nor where to find information.
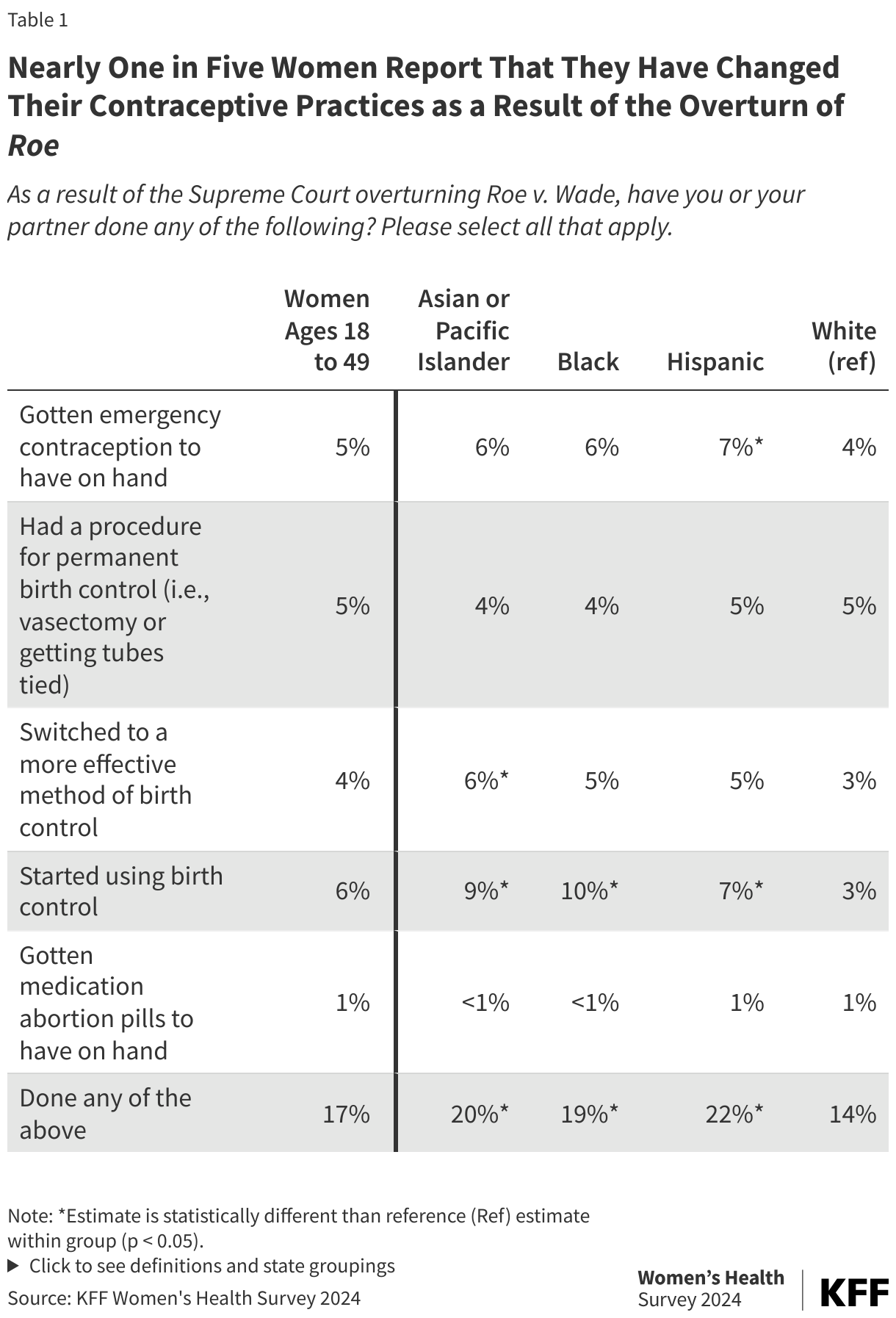
- Nearly one in five women (17%) of reproductive age report they have changed their contraceptive practices as a result of Roe being overturned. Actions taken include starting birth control, getting a sterilization procedure, switching to a more effective method, or purchasing emergency contraceptive pills to have on hand.
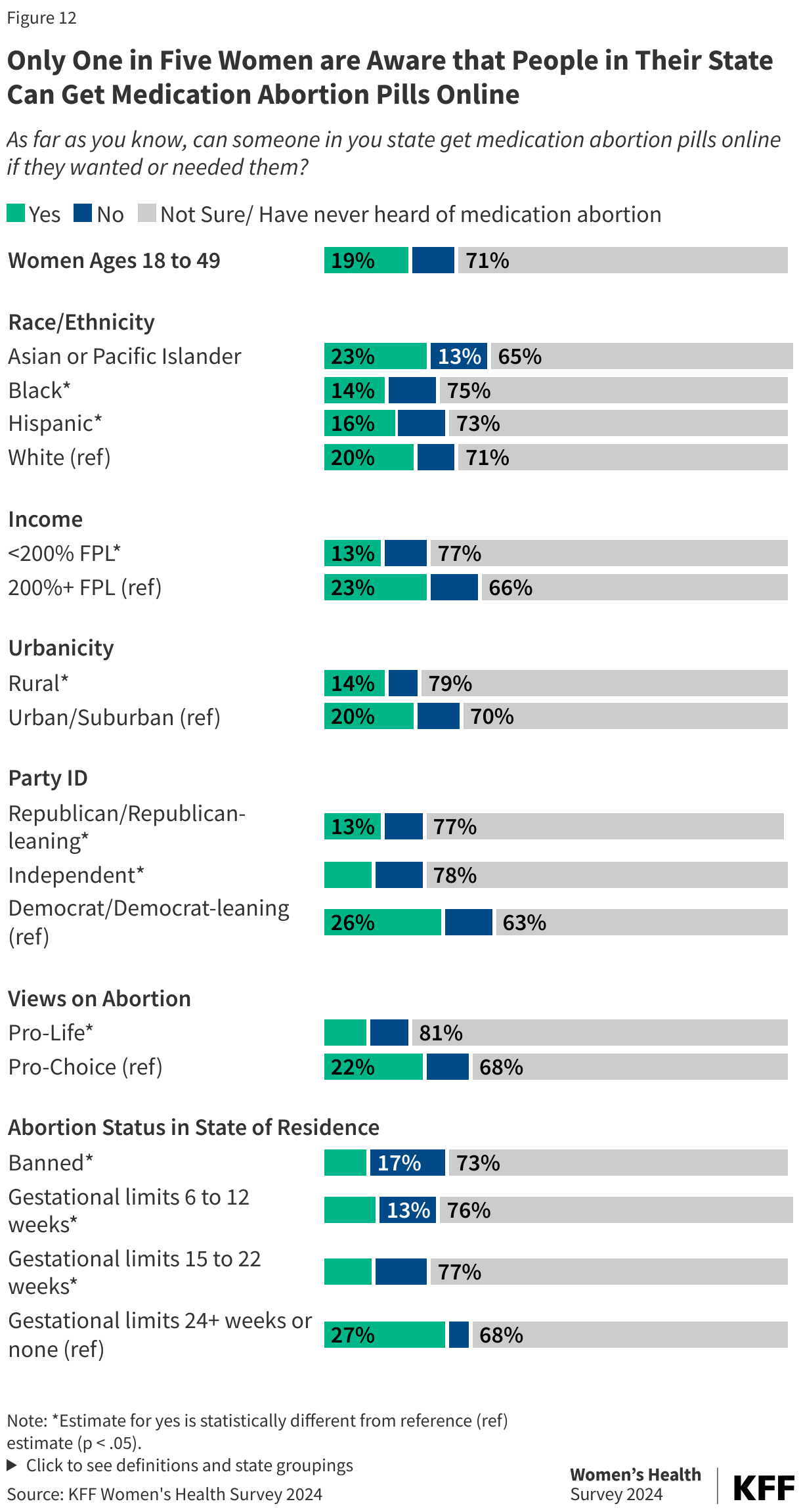
- While two-thirds of women have heard about medication abortion pills, only 19% of women say people in their state can get medication abortion pills online.
- Three in four reproductive age women in the United States think abortion should be legal in most or all cases (74%). The majority support a nationwide right to abortion (70%), oppose a nationwide abortion ban at 15 weeks (64%), and oppose leaving it up to the states to determine the legality of abortion (74%). This is the case for the majority of women who are Democrats and independents as well as smaller but still substantial shares of Republicans.
Introduction
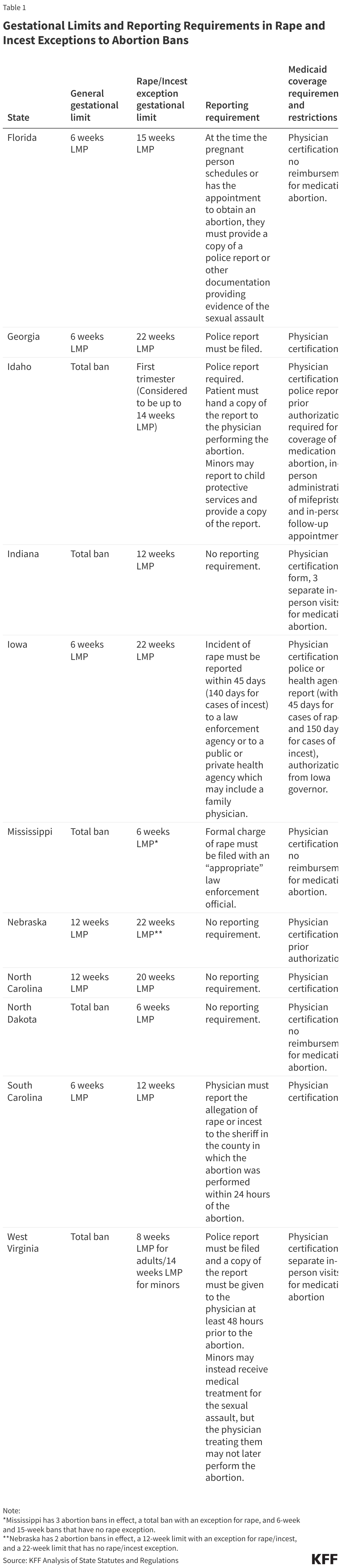
In the two years since the Dobbs decision, which overturned Roe and eliminated the federal standards that had protected the right to abortion for almost 50 years, the abortion landscape in the United States has drastically changed. Abortion is banned in 14 states and an additional six states have implemented early gestational limits between 6 and 15 weeks.
Abortion will likely be a key issue in the upcoming 2024 election. The Democratic and Republican parties have starkly different visions of what access to abortion in the U.S. should look like. Vice President and Democratic Nominee Kamala Harris has been an outspoken advocate of abortion rights and has thrown her support behind efforts to restore Roe v. Wade’s abortion standards in all states. Former President Donald Trump endorses leaving abortion policy up to states, allowing full bans to stay in effect, although he has also previously said he would consider a 15 or 16-week national ban on abortion. At the state level, voters in up to 11 states will vote on abortion-related ballot initiatives that will shape access to abortion in their states.
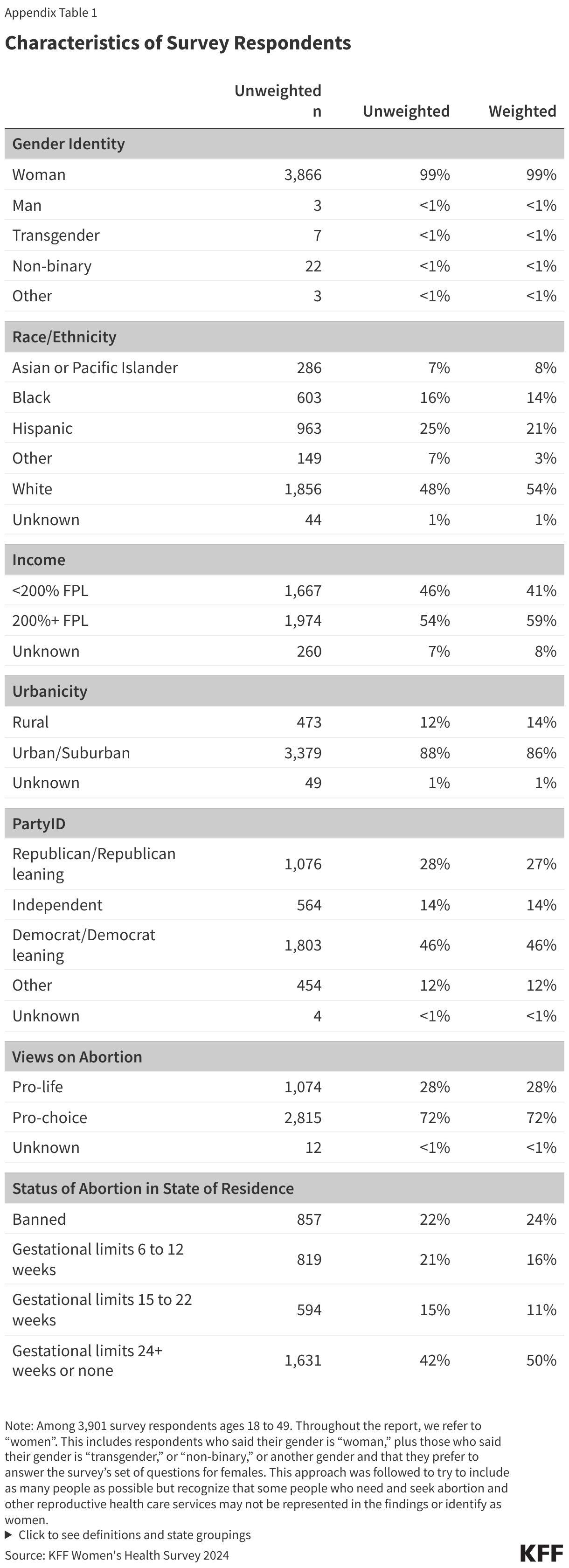
This brief provides new information about women’s experiences with abortion, the fallout of overturning Roe v. Wade, women’s knowledge about abortion laws in their states including medication abortion, as well as their opinions on the legality of abortion. The 2024 KFF Women’s Health Survey was fielded from May 15 to June 18, 2024, before President Biden withdrew from the 2024 Presidential race, and was developed and analyzed by KFF staff. It is a nationally representative survey of 5,055 women and 1,191 men ages 18 to 64, and the findings in this brief are based on a sample of 3,901 women ages 18 to 49. See the methodology section for detailed definitions, sampling design, and margins of sampling error.
Findings
Women’s Experiences With Abortion
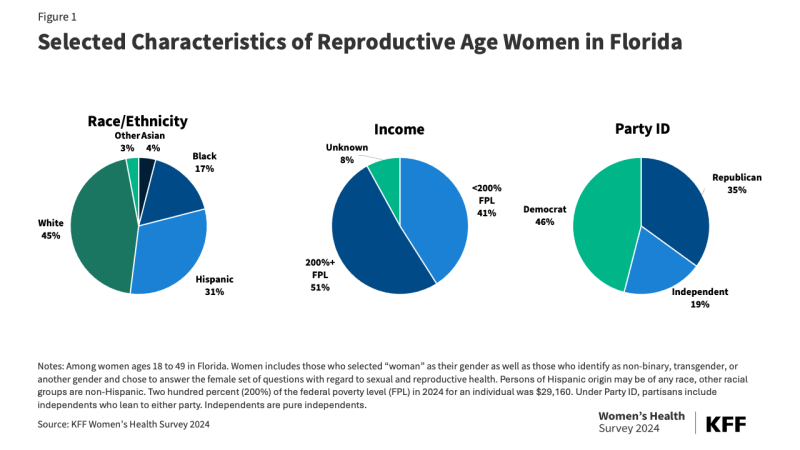
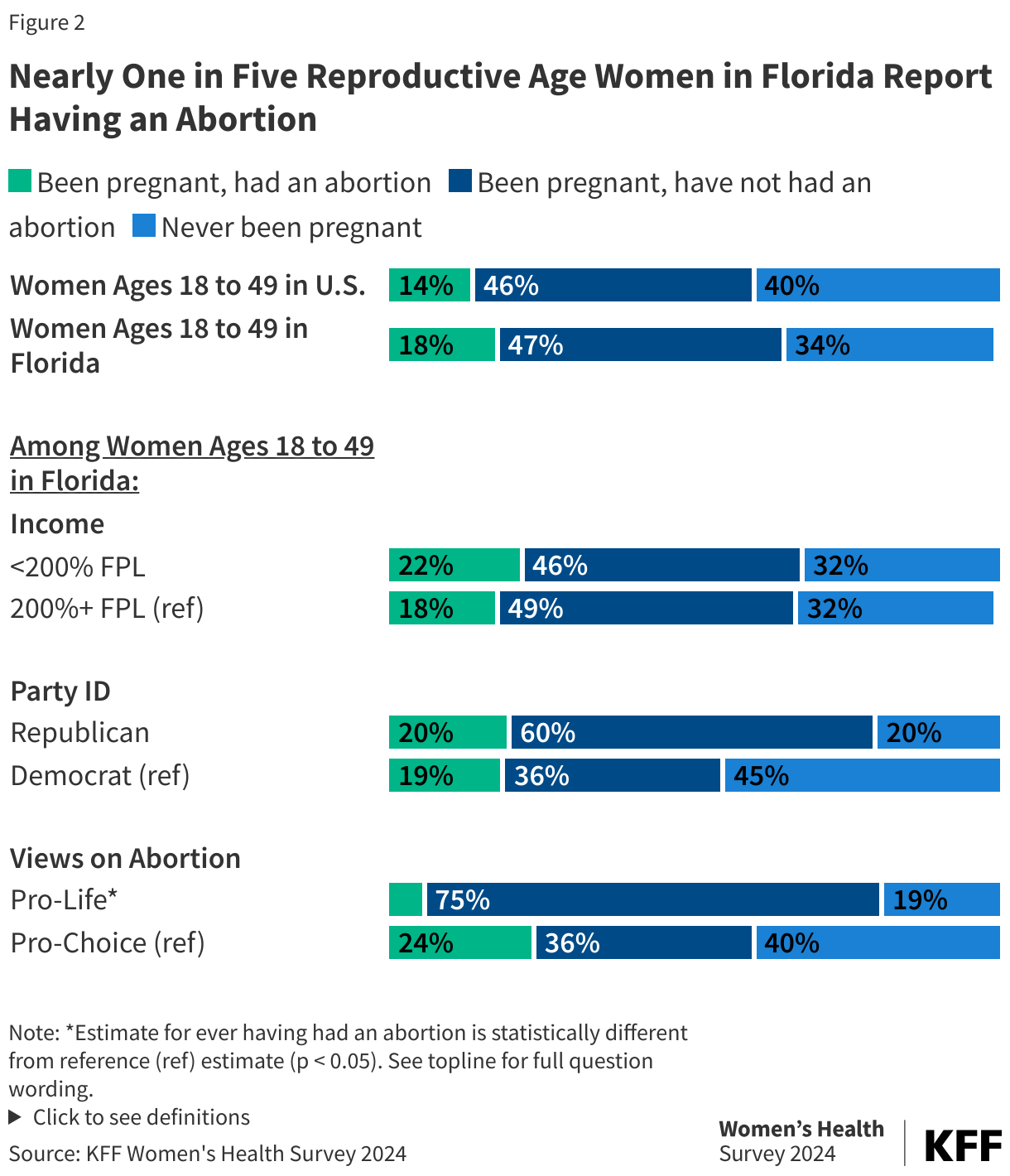
Among women of reproductive age, one in seven (14%) report having had an abortion at some point in their life. Larger shares of Black (21%) and Hispanic (19%) women report having had an abortion compared to 11% of White women (Figure 1). A higher share of women with lower incomes had an abortion (17%) compared to women with higher incomes (13%).
Smaller shares of women living in rural areas report having had an abortion compared to those living in urban/suburban areas (7% vs. 15%, respectively). Many rural women face long travel distances to access abortion services.
Similar shares of Republican women (12%), independent women (15%), and Democratic women (14%) say they have had an abortion. Throughout this brief, partisans include independents who lean to either party, while independents are individuals who say they do not lean toward either political party. Nearly one in 10 women (8%) who currently identify as pro-life say they have had an abortion compared to almost one in five (17%) who currently identify as pro-choice.
Smaller shares of women living in states with abortion bans or gestational limits between 15 and 22 weeks have had an abortion compared to women living in states with gestational limits at or after 24 weeks or without any gestational limits. Even before the Dobbs decision, abortion access was very limited in many of the states that currently ban abortion or have gestational limits before viability. Most of these states had laws restricting access to abortion, including waiting periods, counseling and ultrasound requirements, and insurance coverage restrictions which resulted in the closure of many abortion clinics in the years preceding the Dobbs decision.
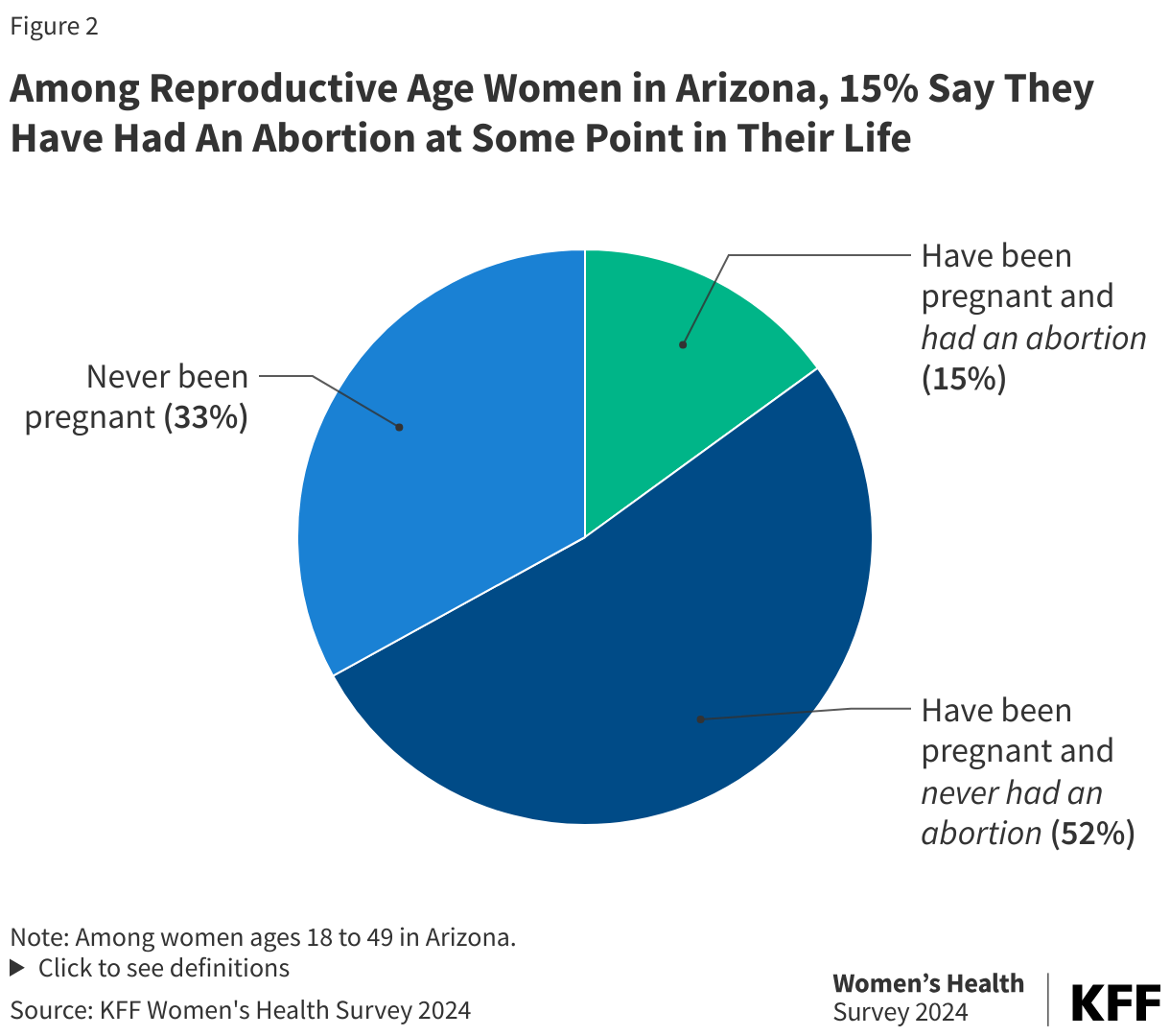
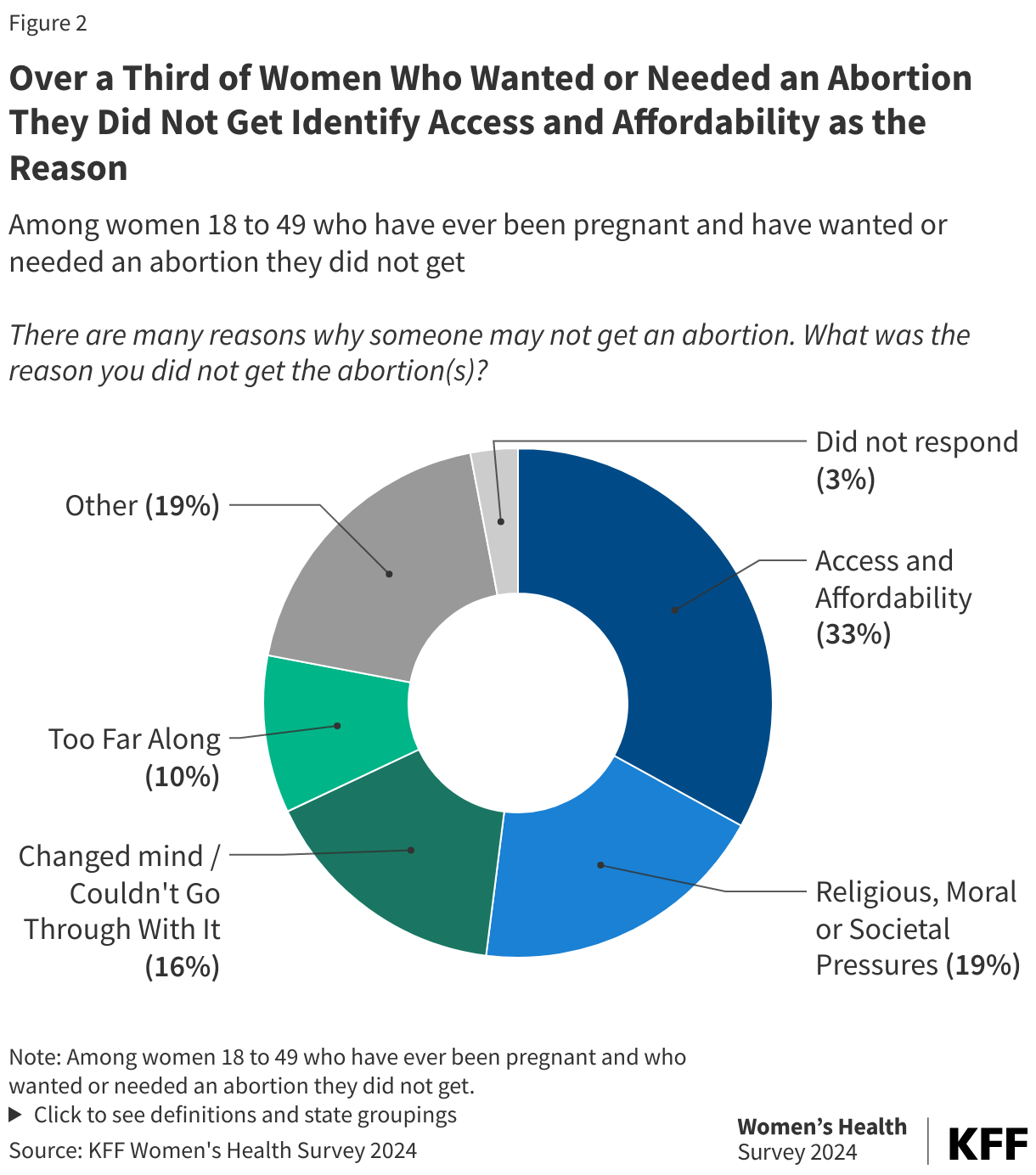
Among women who say they have ever wanted or needed an abortion, 15% (2% of all reproductive age women) report that at some point in their lives, they have wanted or needed an abortion that they did not get (Figure 2). A larger share of Black women (24%) (5% of all Black women of reproductive age) who have ever been pregnant and have wanted or needed an abortion report that they have wanted or needed an abortion they did not get compared to White women (12%) (1% of all White women of reproductive age). When asked why they did not get a wanted or needed abortion, a third (33%) report access and affordability issues, with affordability issues making up the majority of the category. One in five women also identify religious, moral, or societal pressures as the reason why they did not get the abortion, and another 16% say they changed their mind or couldn’t go through with the abortion. One in 10 women say they were too far along to end the pregnancy. Among the women who report ever wanting or needing an abortion they did not get, 31% say they had an abortion at some other time (data not shown).
In their own words: There are many reasons why someone may not get an abortion. What was the reason you did not get the abortion(s)?
“Unable to afford the procedure and would be reaching [the] point where it would be too late to complete if able.”
“Was a day over the amount of days in order to have an abortion. I waited too long to get it.”
“Changed my mind. Decided to keep the baby but was initially scared and unsure of what to do.”
“I decided I wanted to keep and raise my child despite societal pressures that would advise against it (I was a minor).”
“My family made me feel like I couldn't and I was scared so I followed through with my pregnancy.”
“I was intimidated by the child's father showing up at the clinic.”
“I could not afford to go out of state and had no way out of [the] state.”
“Ended up miscarrying before proceeding with appointment.”
“I was too far along in the pregnancy when I found out I was pregnant”
“Religious reasons. We are Catholic and it's not an option for us.”
“The service wasn't easily accessible to me, and my partner's family pressured me into having the child.”
“Guilt, moral compass”
“Nurse convinced me not to get it.”
“I could not afford it at the time and unsure if I really wanted to do it.”
“Family pressure, difficulty finding a place to perform an abortion.”
“I lived an hour and a half from the location and my ride didn’t show up.”
The Impact of Overturning Roe
Two years after the Supreme Court overturned the constitutional right to abortion, 14 states have banned abortion, and 11 states have implemented gestational restrictions between 6 and 22 weeks LMP (last menstrual period). Nationally, 8% of reproductive age women say they personally know someone, including themselves, who has had difficulty getting abortion care since Roe was overturned due to the restrictions in their state (Figure 3). Larger shares of Hispanic women (11%) than White women (8%) report knowing someone who has experienced difficulty getting an abortion. Similarly, larger shares of women living in states with abortion bans (13%) and women living in states with gestational limits between 6 and 12 weeks (11%) report knowing someone who has experienced difficulty compared to women living in states with gestational limits at or after 24 weeks or without gestational limits (6%). Even in states with few abortion restrictions, access to abortion services can be limited by lack of providers, poor coverage, and other factors.
Among those who say they know someone (including themselves) who had difficulty getting abortion care since Roe was overturned, the majority report they (or the person they knew) had to travel out of state (68%) (Figure 4). Women with higher incomes who say they or someone they know had difficulty accessing abortion care are more likely to report that they or the person they know had to travel out of state compared to women with lower incomes (75% vs. 62%). Many abortion patients living in states with abortion bans or restrictions have to travel to neighboring states to get abortion care, while others may need to travel farther.
Among women who say they or someone they know had difficulty accessing abortion, four in ten women say they or a person they know did not know where to go when trying to get an abortion (40%), three in ten women say they could not afford the cost (35%), and nearly three in ten say they had to take time off work (28%).

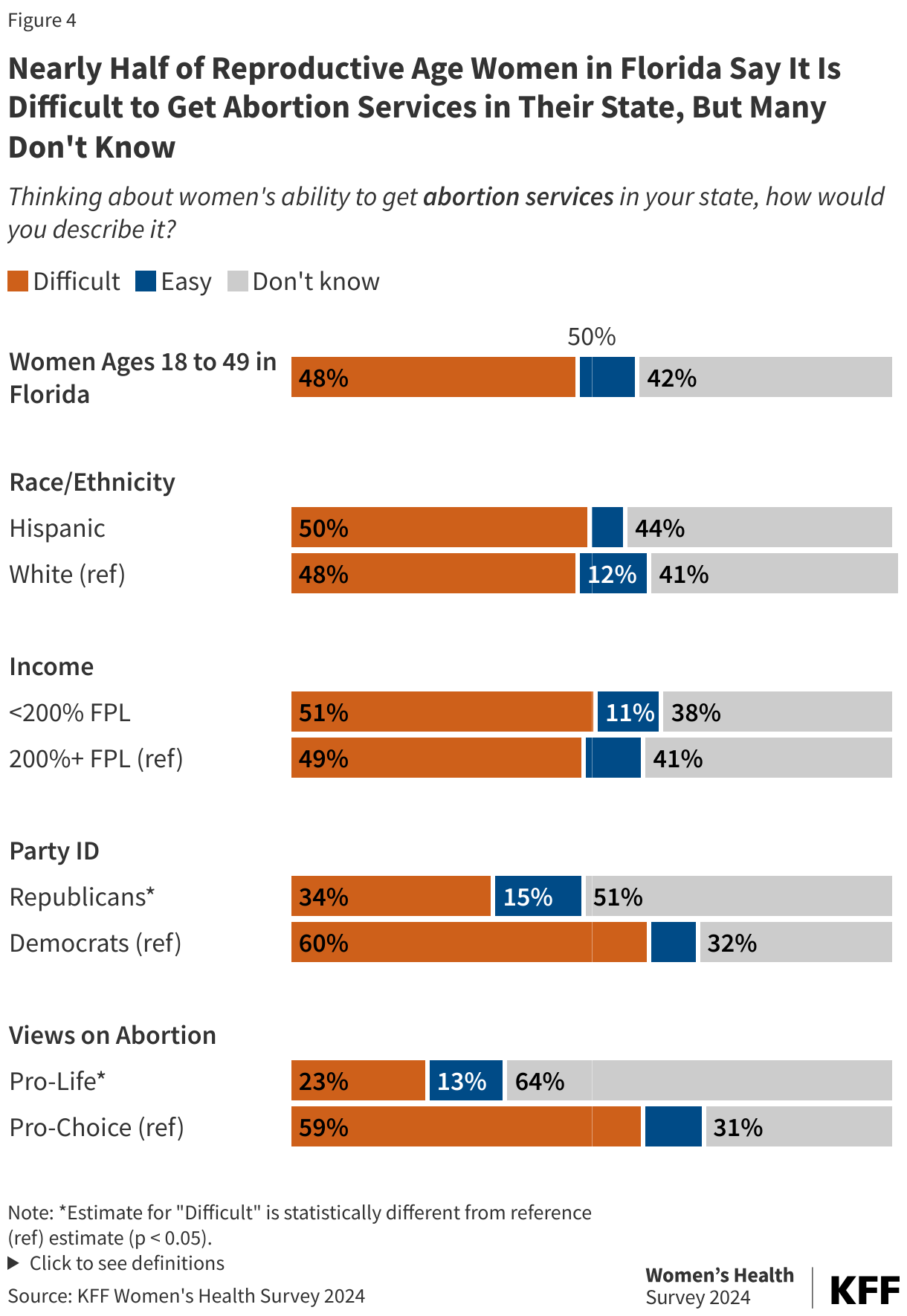
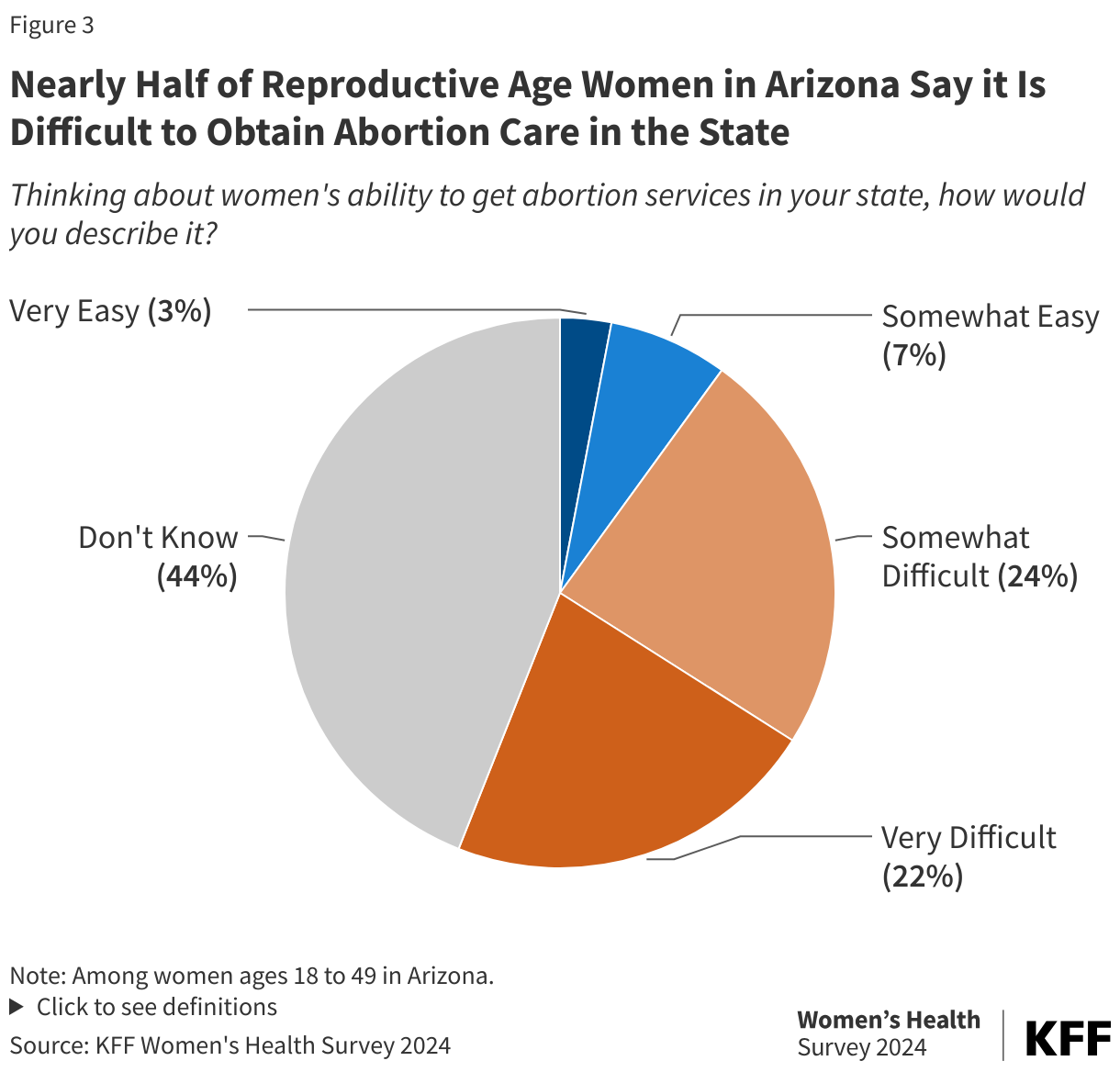
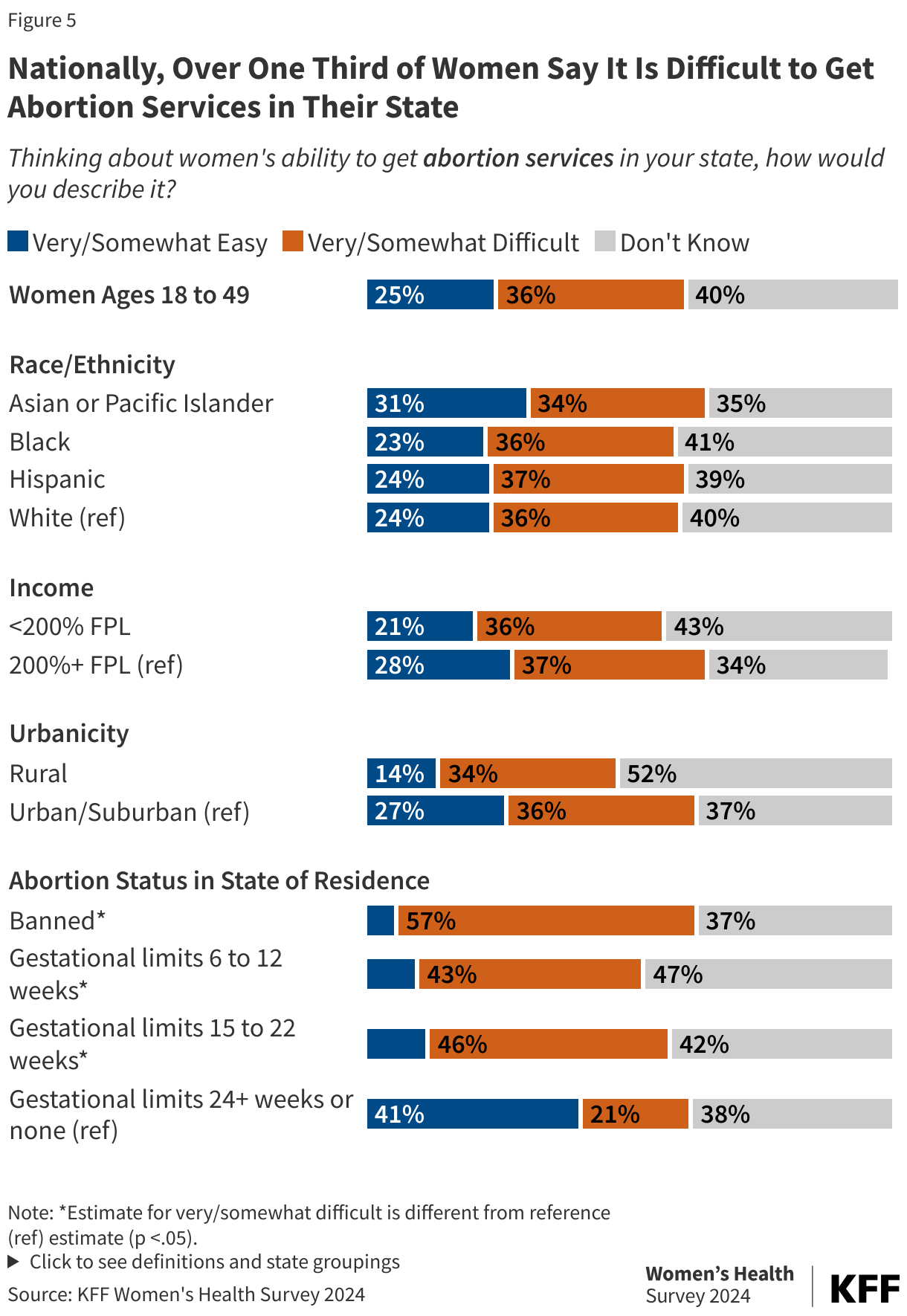
When asked about women’s ability to get abortion services in their state, more than half of women residing in states with abortion bans (57%) and over four in ten women in states with gestational limits say it is difficult to access abortion care in their state (Figure 5). Notably, one in five (21%) women residing in states with gestational limits at or after 24 weeks or without gestational limits say it is difficult to get abortion services in their state. While abortion may not be restricted, limitations on Medicaid and insurance coverage of abortion, the scarcity of abortion providers in rural communities, stigma, and other factors (such as the need to take time off from work and childcare costs) are still barriers to abortion.
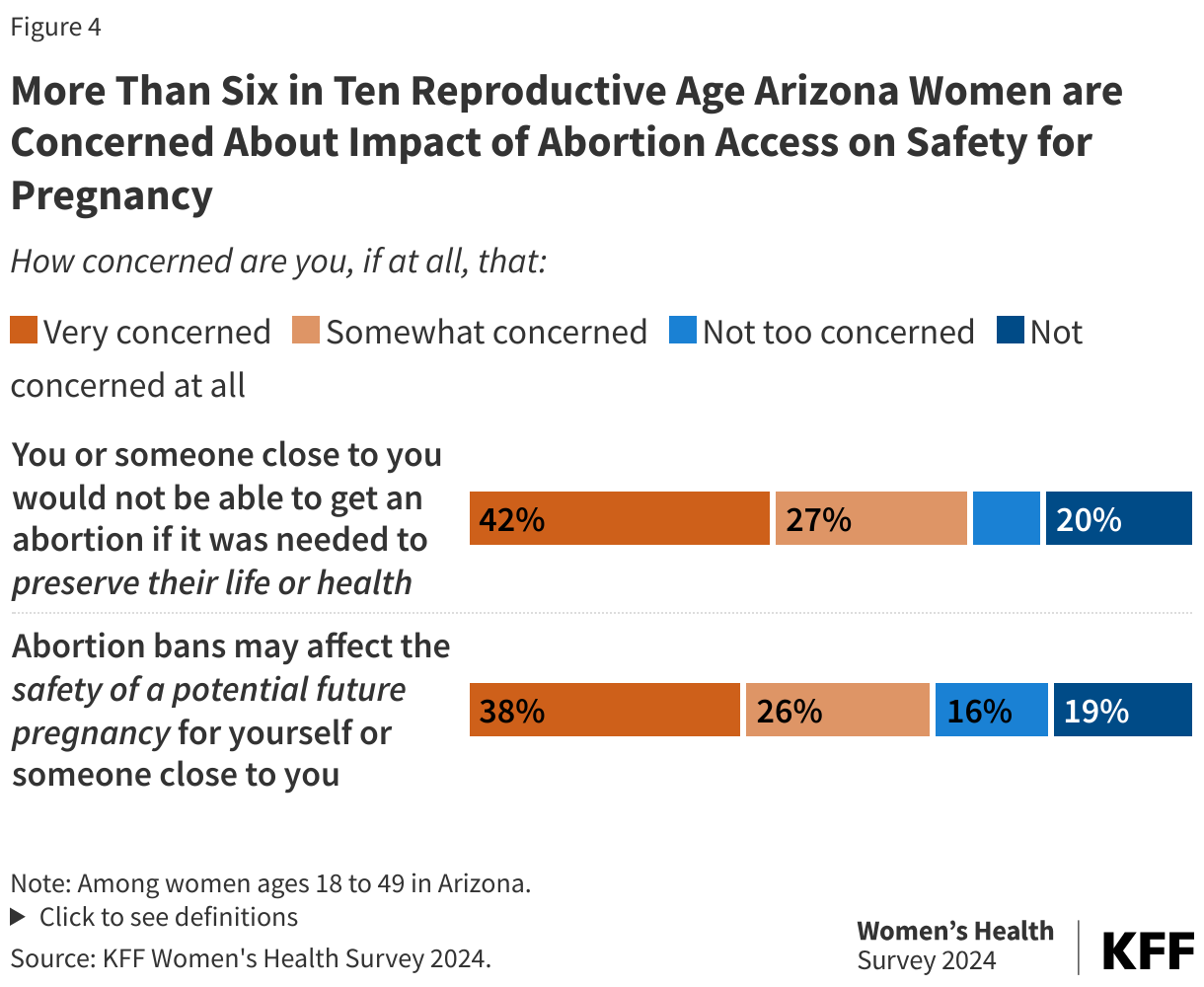
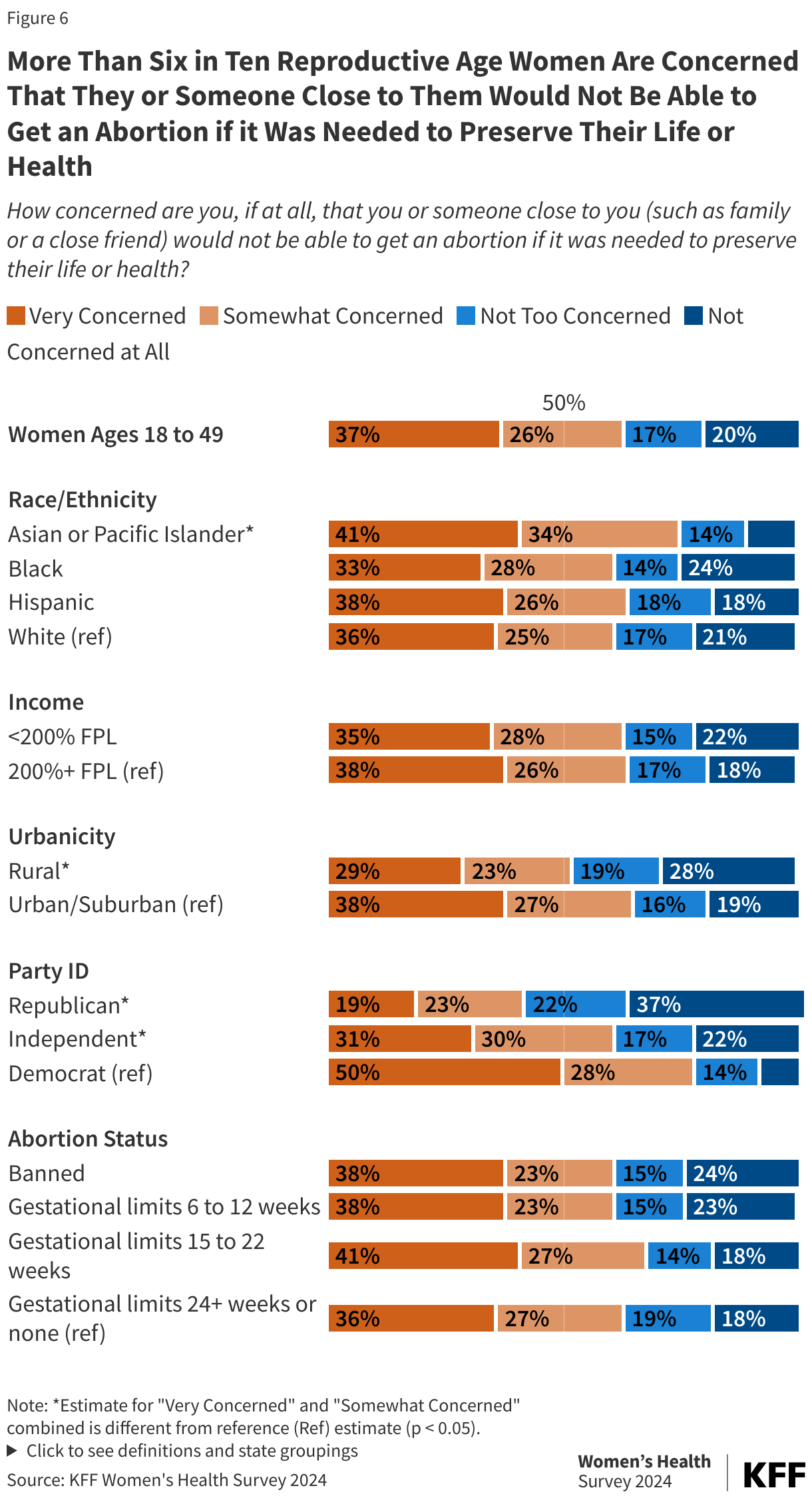
Over six in ten reproductive age women in the U.S. (63%) are concerned that they or someone close to them would not be able to get an abortion if it was needed to preserve their life or health (Figure 6). While all states with abortion bans and abortion restrictions have an exception in their law to “prevent the death” or “preserve the life” of the pregnant person, six states with abortion bans or early gestational restrictions do not have health exceptions. In general, health exceptions have often proven to be unworkable except in the most extreme circumstances. The abortion policies in these states are generally unclear about how ill or close to death a pregnant person would have to be to qualify for the exception.
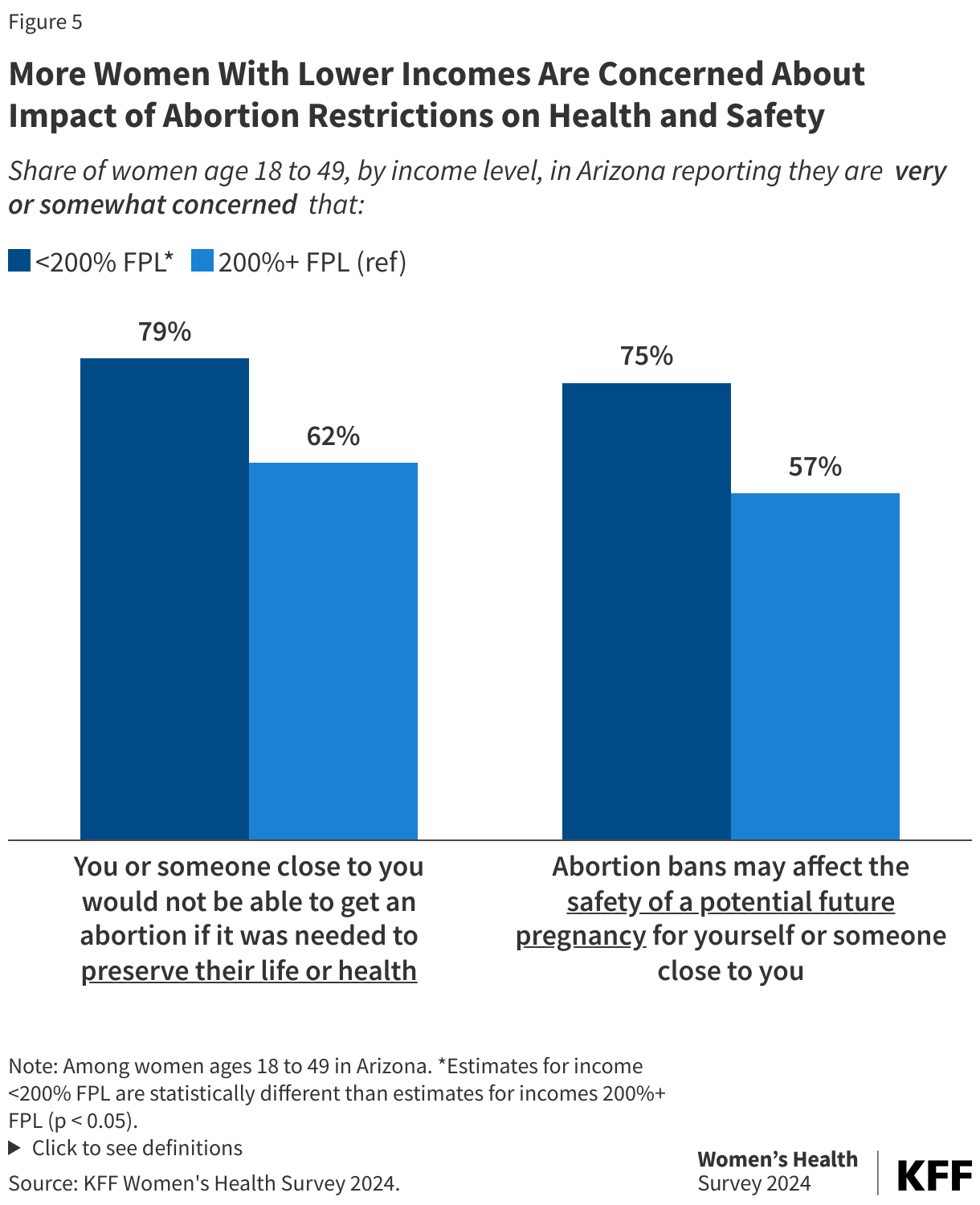
With the exception of Republican women, a majority of reproductive age women in all subgroups report that they are very or somewhat concerned about access to abortion if it was needed to preserve their life or health. Larger shares of Asian or Pacific Islander women (75%) than White women (61%) are concerned, and smaller shares of women residing in rural areas (52%) are concerned compared to those residing in urban/suburban areas (65%). Compared to Democratic women (78%), smaller shares of women who identify as independent (61%) are concerned that they or someone close to them would not be able to get an abortion if it was needed to preserve their life or health; however, less than half of Republican women report being somewhat or very concerned (41%).
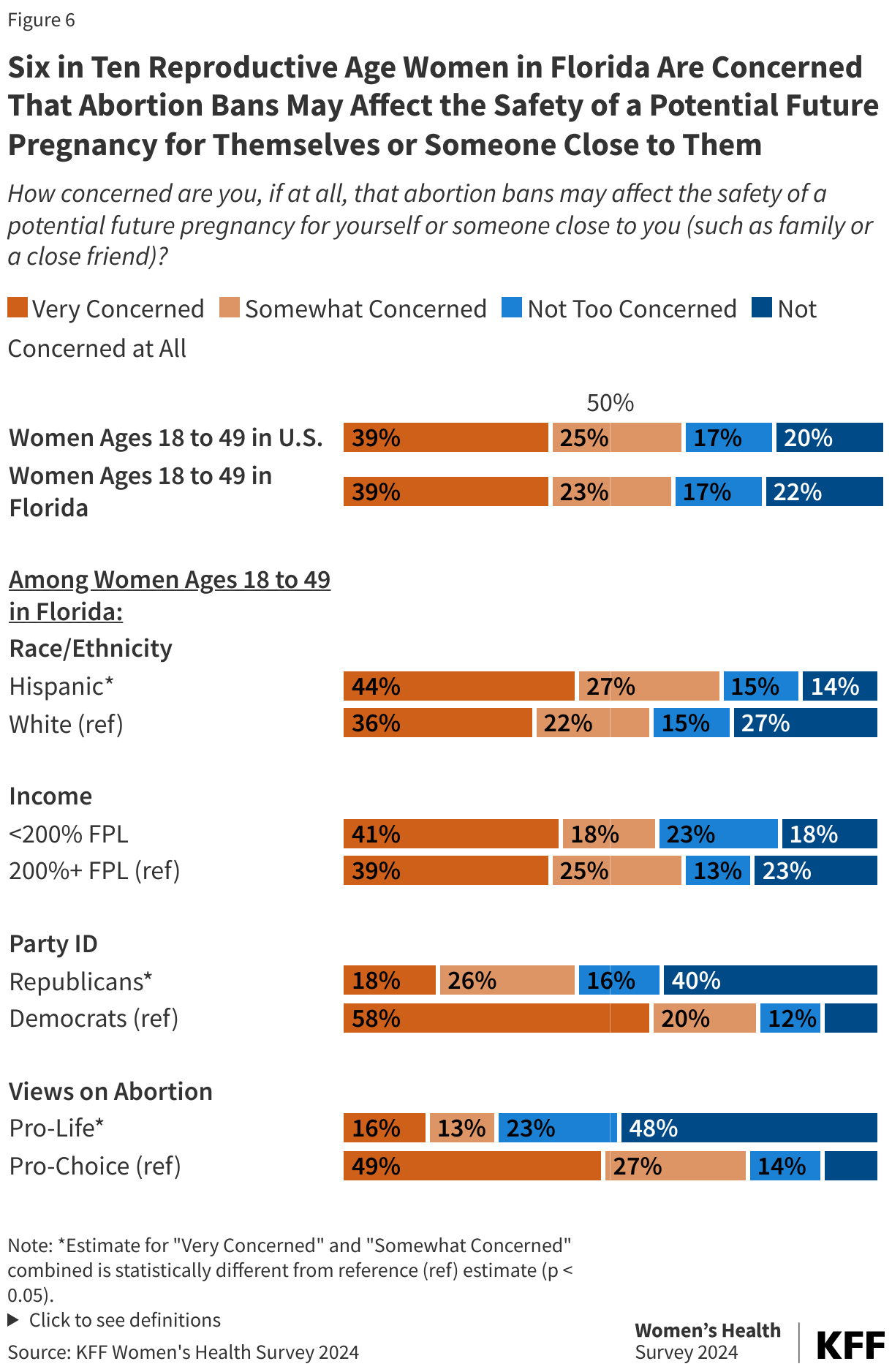
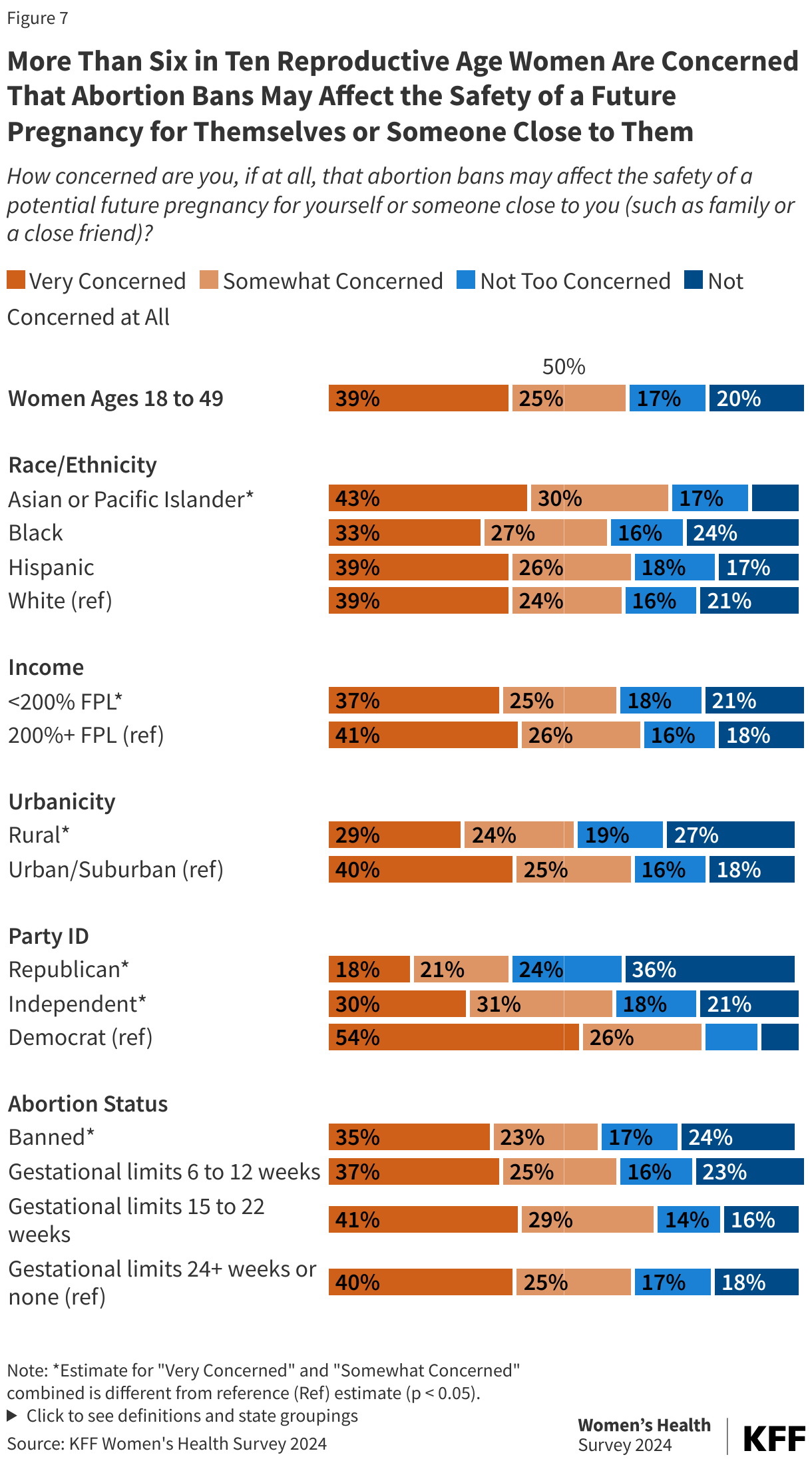
Similarly, over 6 in 10 (64%) reproductive age women say they are concerned that abortion bans may affect the safety of a potential future pregnancy for themselves or someone close to them (Figure 7). Across most subgroups—except across party affiliation— majorities of women say that they are somewhat or very concerned. Four in ten (39%) Republican women say they are concerned about the impact of abortion bans on the safety of potential pregnancies for themselves or someone close to them, compared to almost eight in 10 Democratic women and six in 10 independent women.
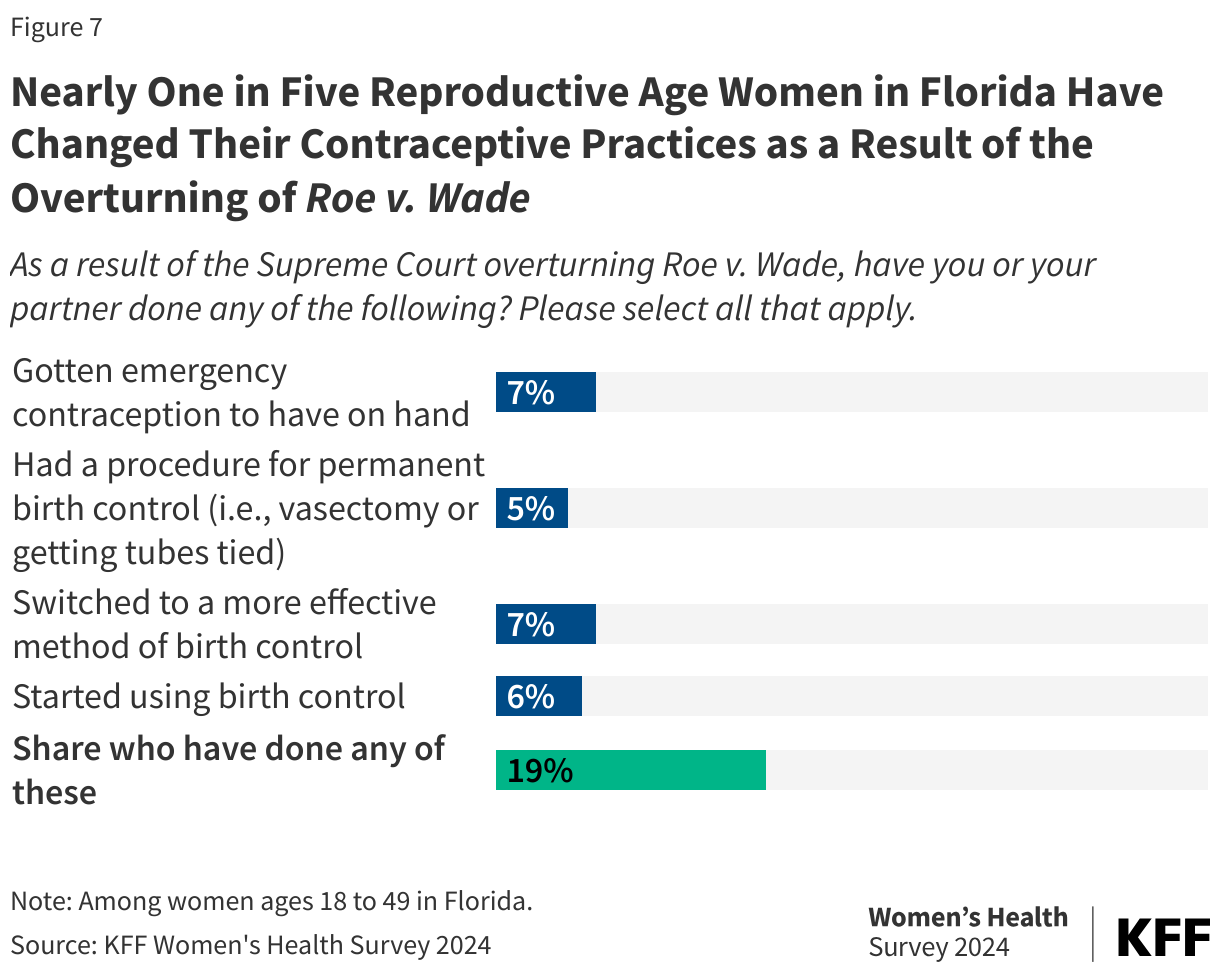
Nearly one in five women (17%) of reproductive age report they have changed their contraceptive practices as a result of Roe being overturned. Larger shares of Asian or Pacific Islander, Black, and Hispanic women report they started to use birth control (9%, 10%, and 7%, respectively) compared to White women (3%) (Table 1). A higher share of Asian or Pacific Islander women report that they have switched to a more effective method of birth control compared to White women (6% vs. 3%), and 7% of Hispanic women report that they have gotten emergency contraception to have on hand compared to 4% of White women.
Awareness of Abortion Availability and Policy
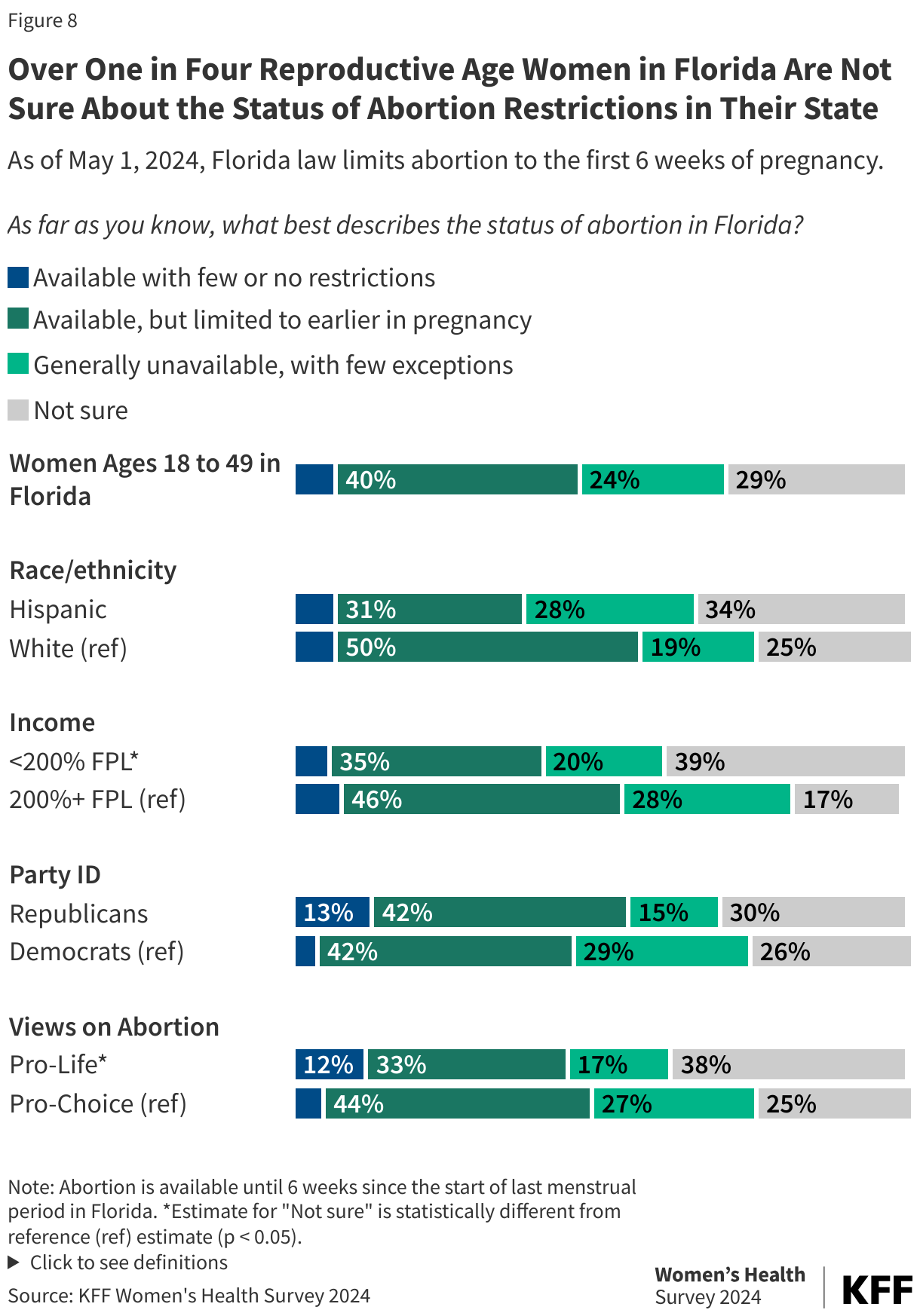
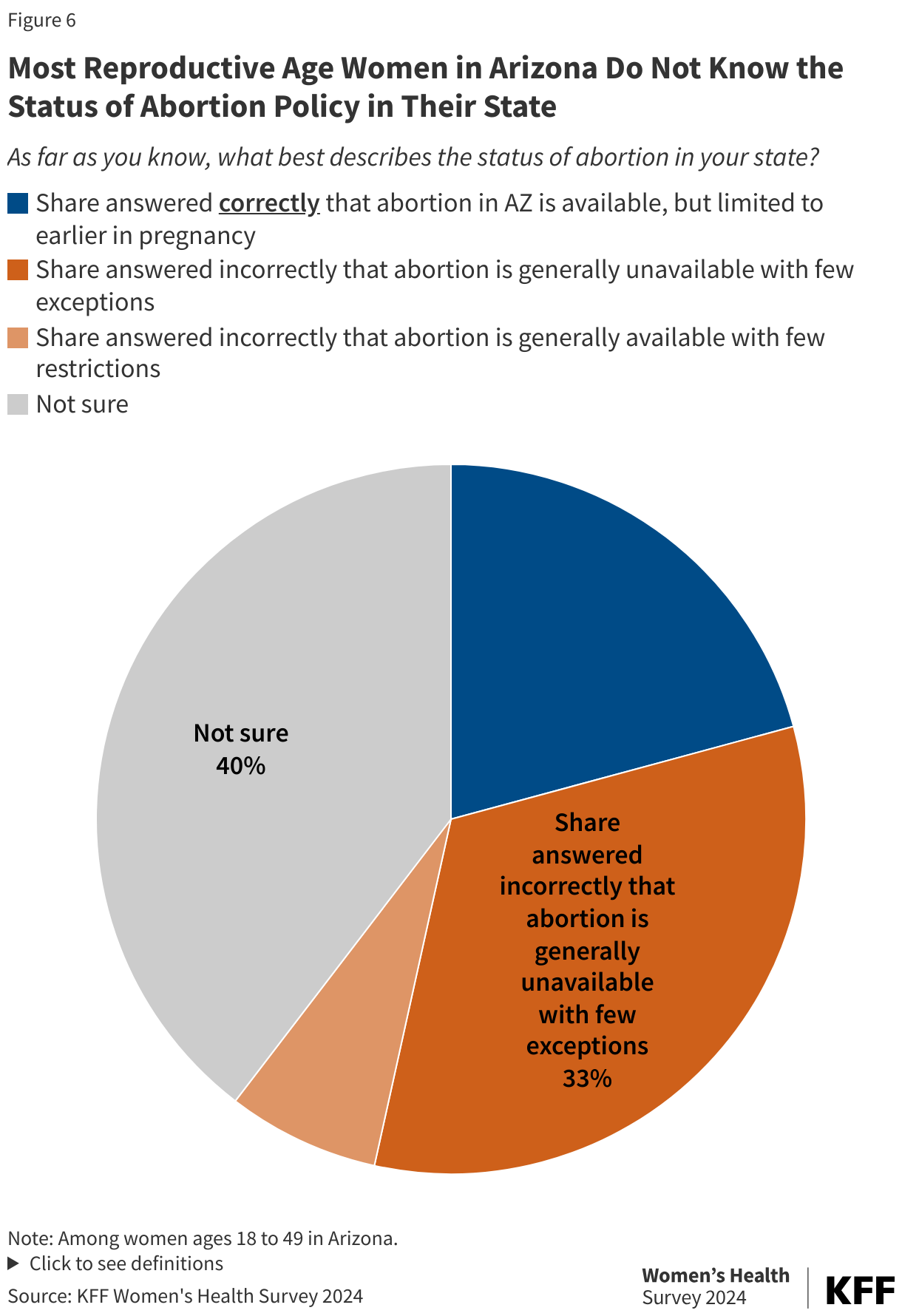
Nationally, most women of reproductive age are unaware of the status of abortion legality in the state they live in. While 45% can correctly describe the status of abortion in their state, 23% of reproductive age women could not answer correctly and another third (33%) say they are not sure (Figure 8). Awareness is highest among women who live in states where abortion is fully banned (51%) or in states with gestational limits at or after 24 weeks or without bans (47%). Smaller shares of women living in states with gestational limits at 15 to 22 weeks (33%) and limits at 6 to 12 weeks (38%) are aware of the status of abortion in their state. Consistently across state abortion groupings, about a third of women say they are not sure on the status of abortion in their state.

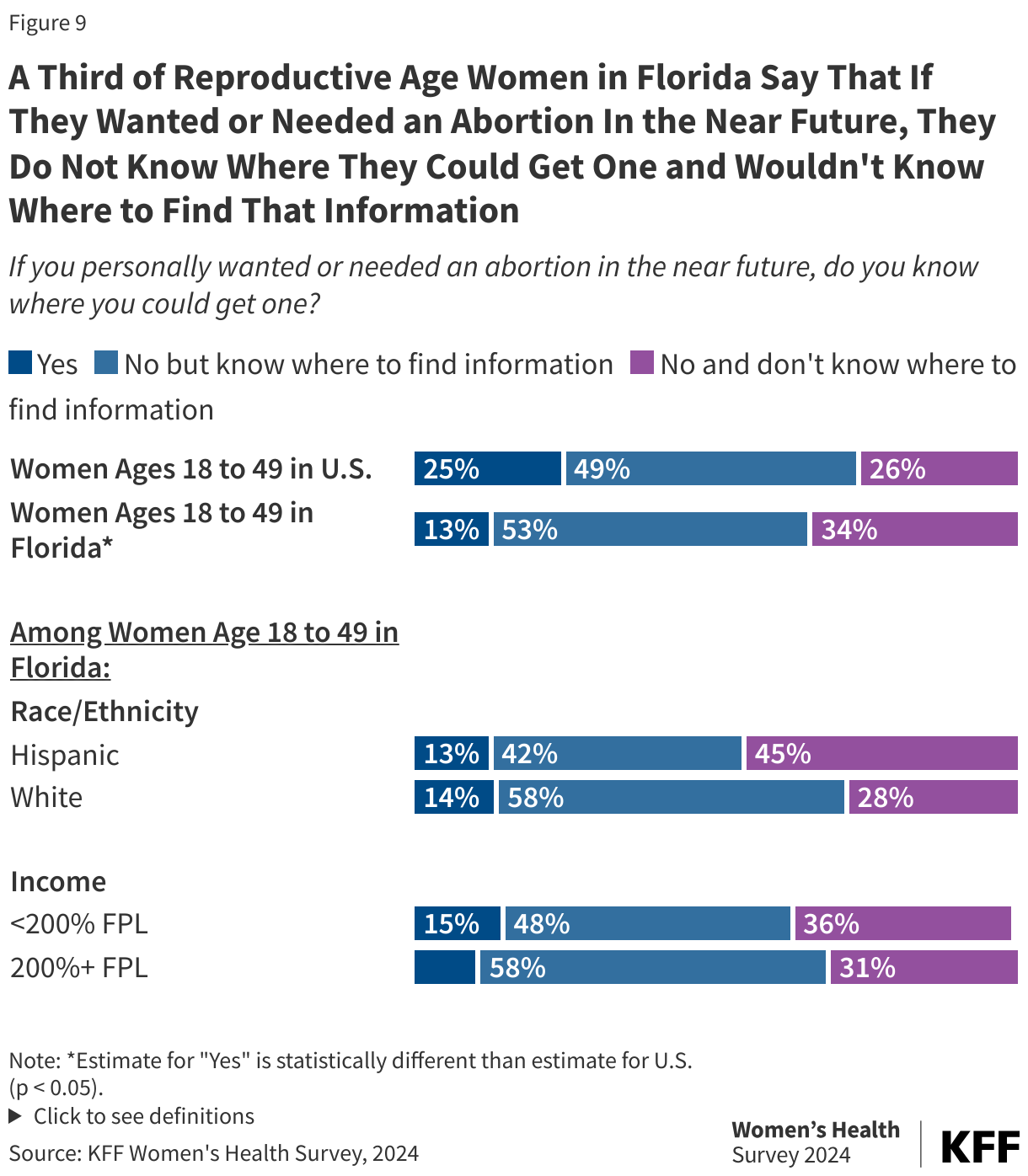
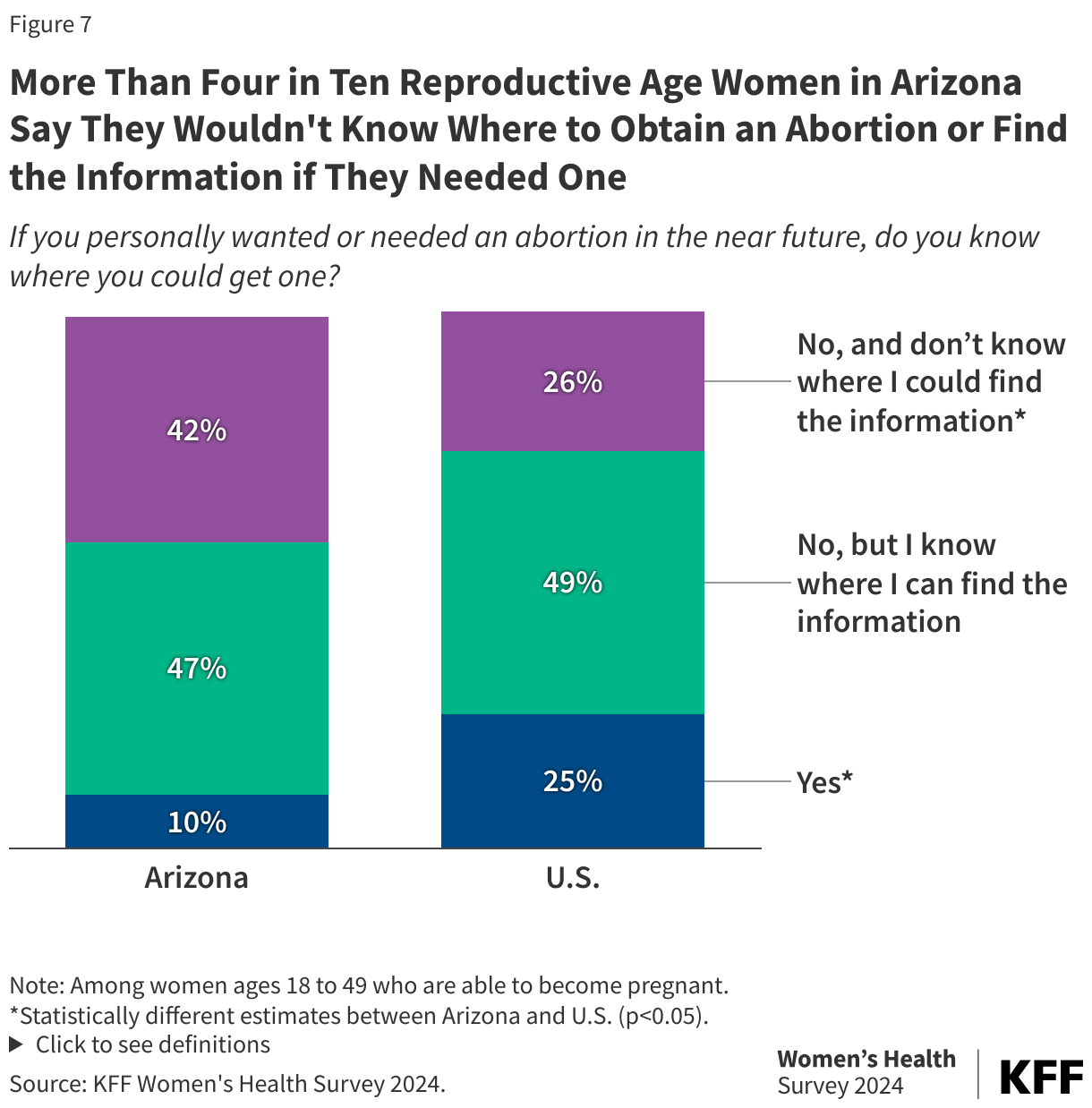
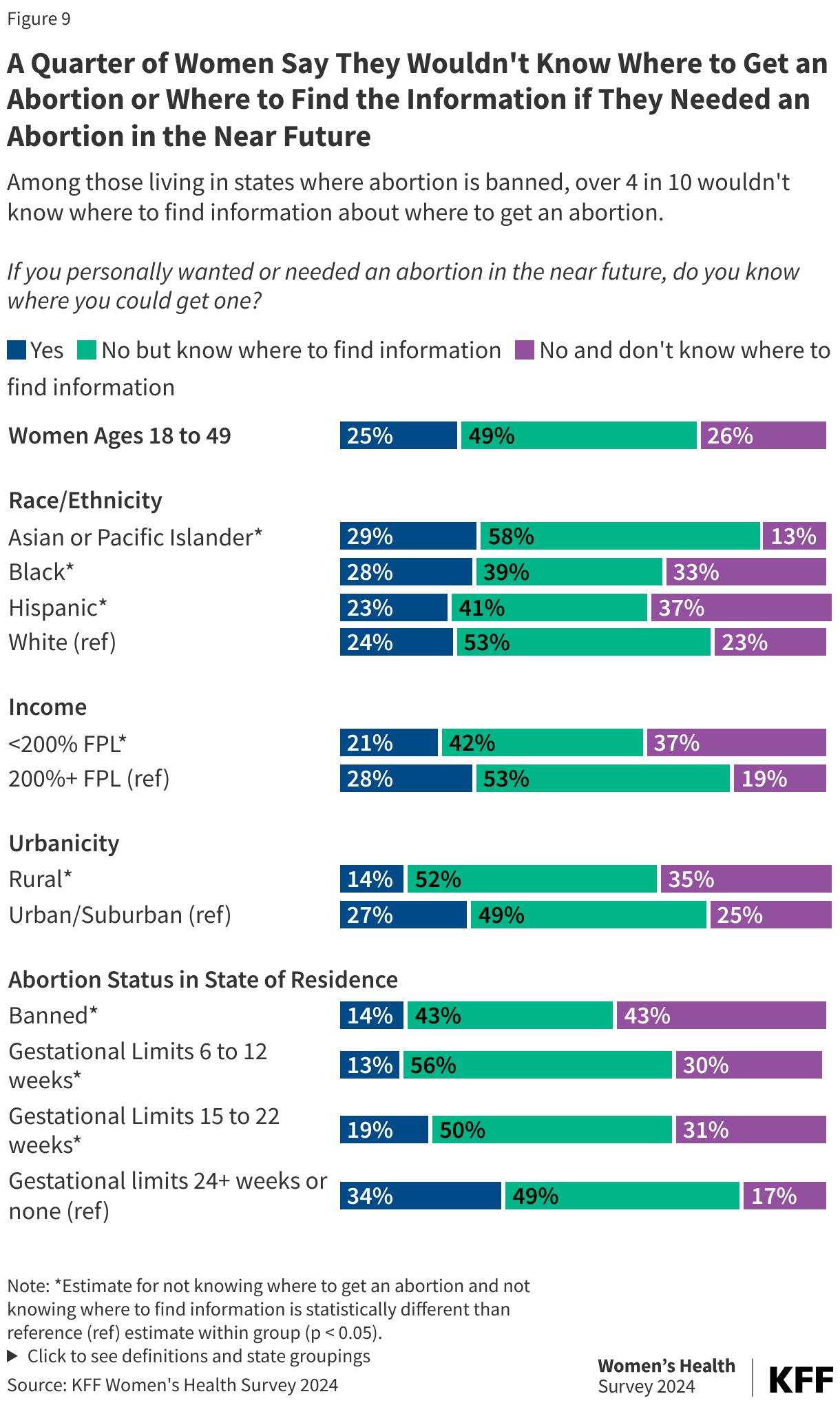
One in four (26%) women of reproductive age in the U.S. report that if they needed or wanted an abortion in the near future they would not know where to go or where to find the information (Figure 9). A quarter of women say they would know where to go for an abortion and half (49%) say they would not know where to go, but would know where to find that information. Since the Dobbs decision, websites like abortionfinder.org and ineedana.com provide individuals seeking abortion services with directories of abortion clinics and services that provide medication abortion via telehealth.
Over a third of Hispanic women (37%) and a third of Black women (33%) report that if they wanted or needed an abortion in the near future, they wouldn’t know where to find information compared to 23% of White women. More women with lower incomes (37%) and women living in rural areas (35%) report they wouldn’t know where to go or find that information compared to women with higher incomes (19%) and women living in urban/suburban areas (25%). Over four in 10 (43%) women living in states where abortion is banned say they wouldn’t know where to find information compared to 17% of women in states with gestational limits at or after 24 weeks or without gestational limits. Women living in banned states seeking abortion services must either travel out of state or obtain medication abortion drugs from companies that will ship pills without requiring a clinician visit or from clinicians practicing in states with shield-laws, which offer clinicians a measure of legal protection from attempts by law authorities in abortion ban states to enforce bans in states that support abortion access.
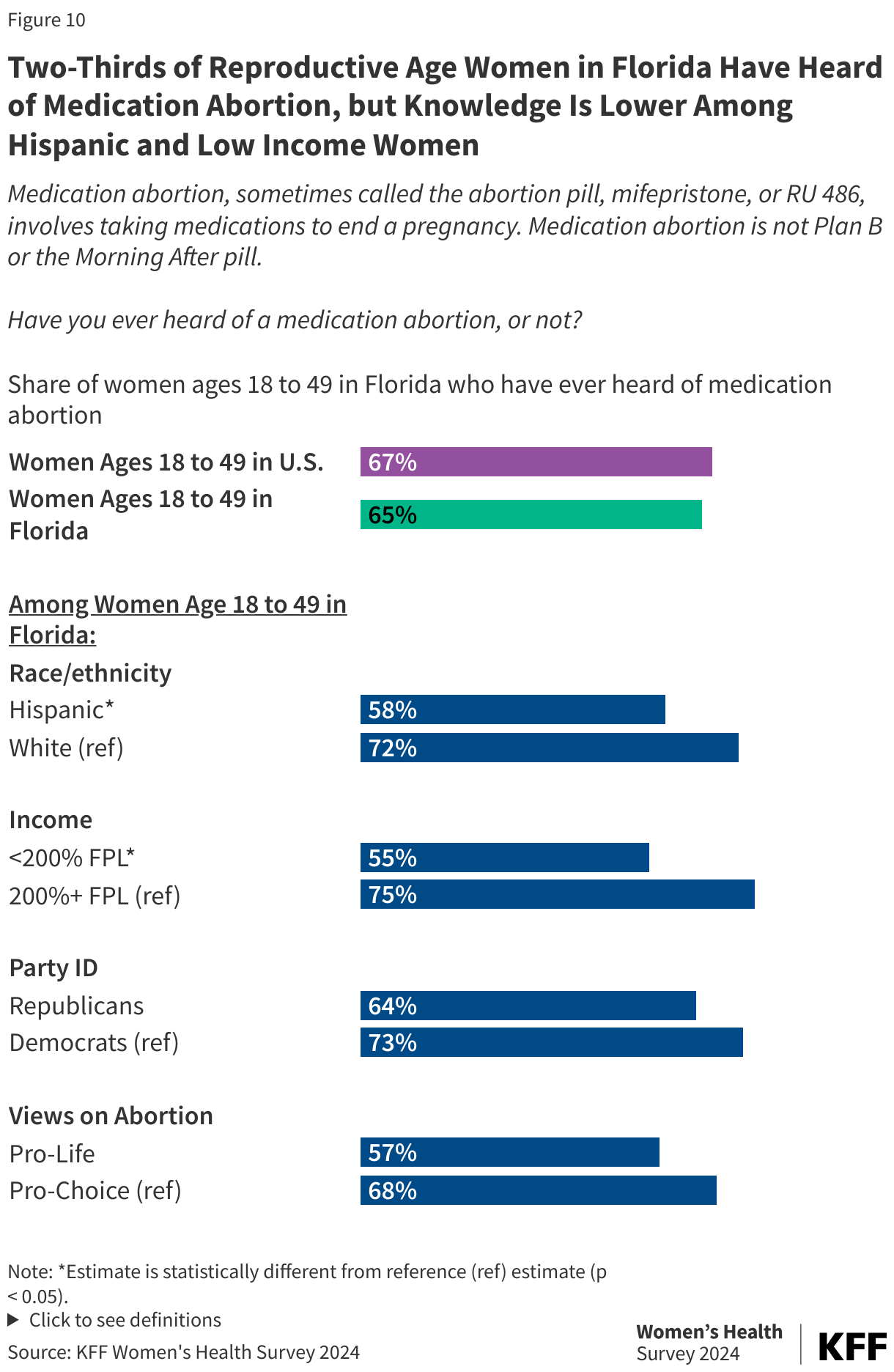
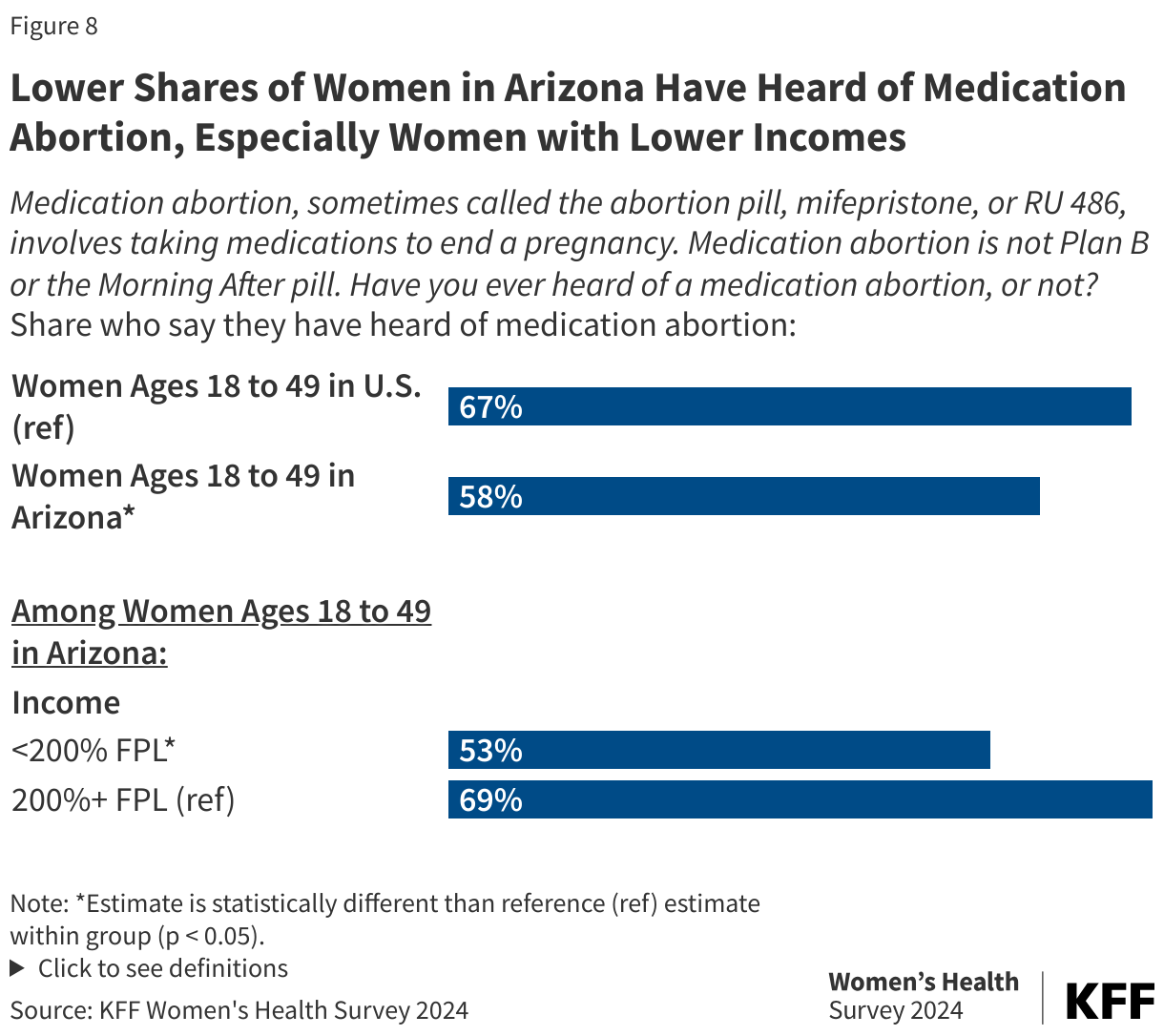
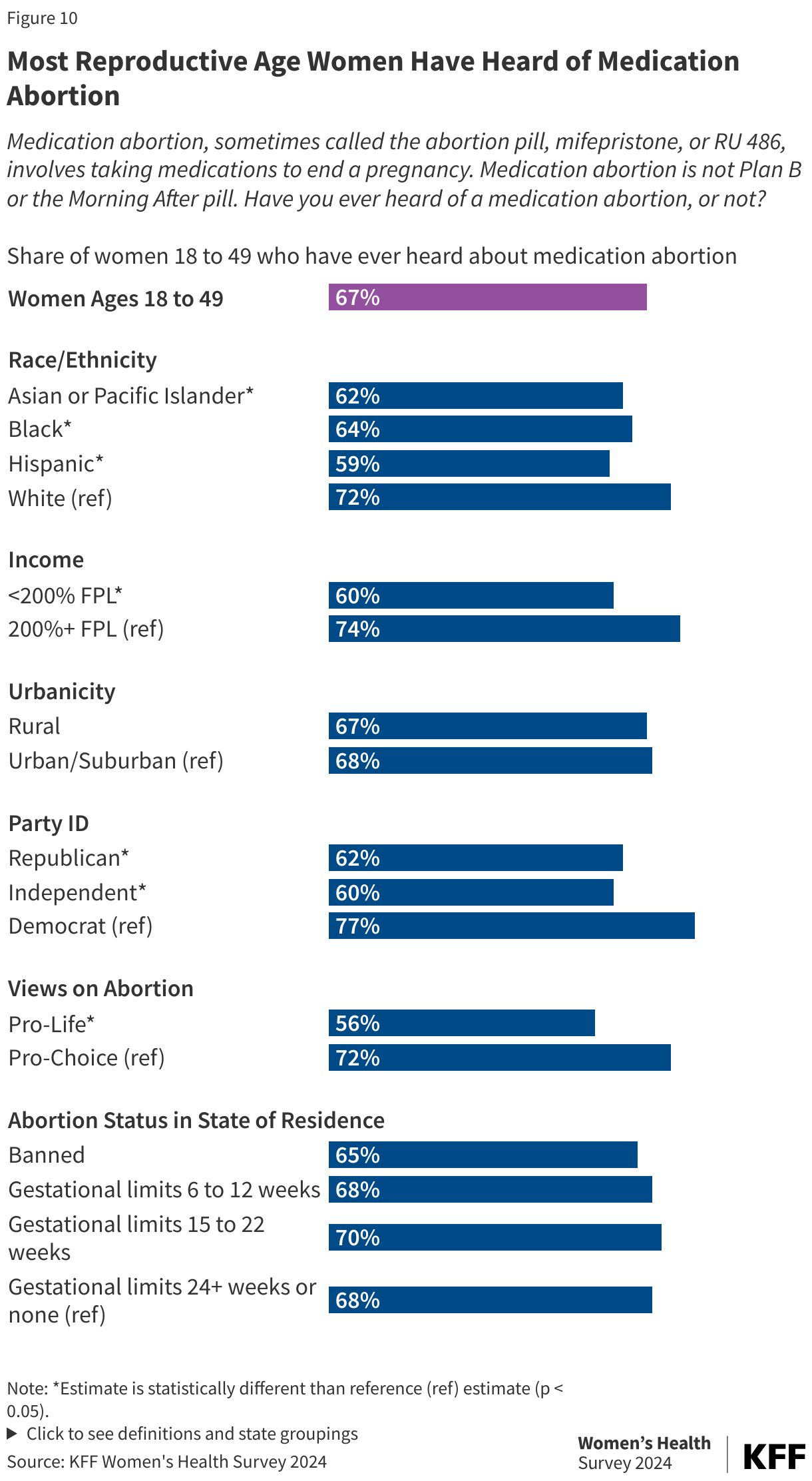
In the United States, medication abortion is the most common abortion method. It involves taking two different medications, mifepristone and misoprostol, and it has been approved by the FDA to end pregnancies up to 10 weeks gestation. Two-thirds (67%) of women of reproductive age report that they have heard about medication abortion (Figure 10). While still majorities, relatively smaller shares of Asian or Pacific Islander (62%), Black (64%), and Hispanic (59%) women report having heard about medication abortion compared to White women (72%). Similarly, smaller shares of women with lower incomes (60%) have heard about medication abortion compared to women with higher incomes (74%). Compared to women who identify as pro-choice (72%) and women who are Democrats (77%), smaller shares of women who identify as pro-life (56%) or are Republican/Republican leaning (62%) or independents (60%) report hearing of medication abortion.
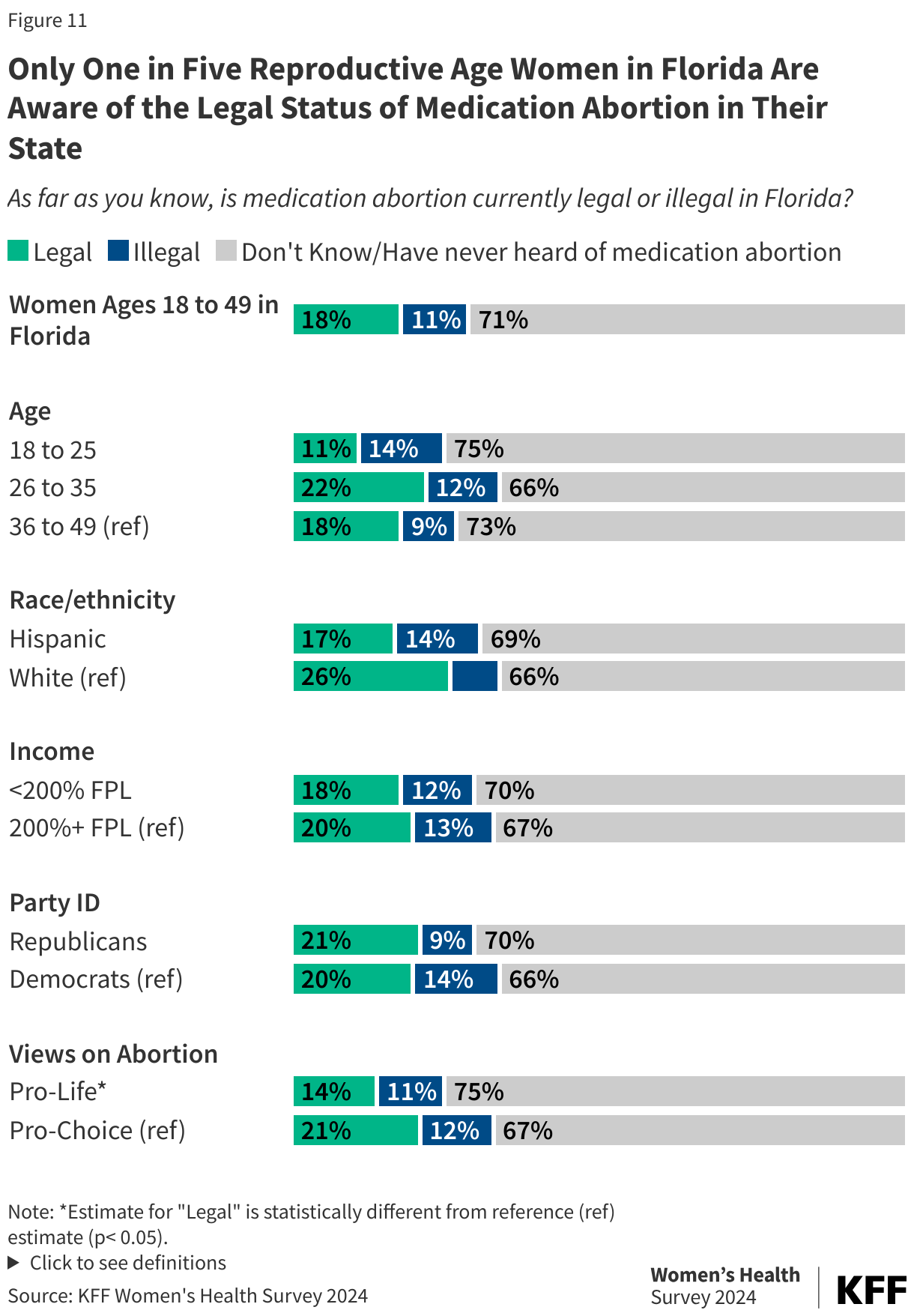
The majority of women are unsure of the legal status of abortion in their state. While neither mifepristone nor misoprostol are explicitly banned in any state and the drugs can still be used for miscarriage management treatment, their use for abortion is banned in the 14 states with abortion bans. Medication abortion, for the purposes of abortion, is legal in all states with gestational restrictions as well as states without any limits, but is not legal to use for abortion after the state’s gestational limit (for example, after 6 weeks LMP in Iowa, Florida, Georgia, and South Carolina).
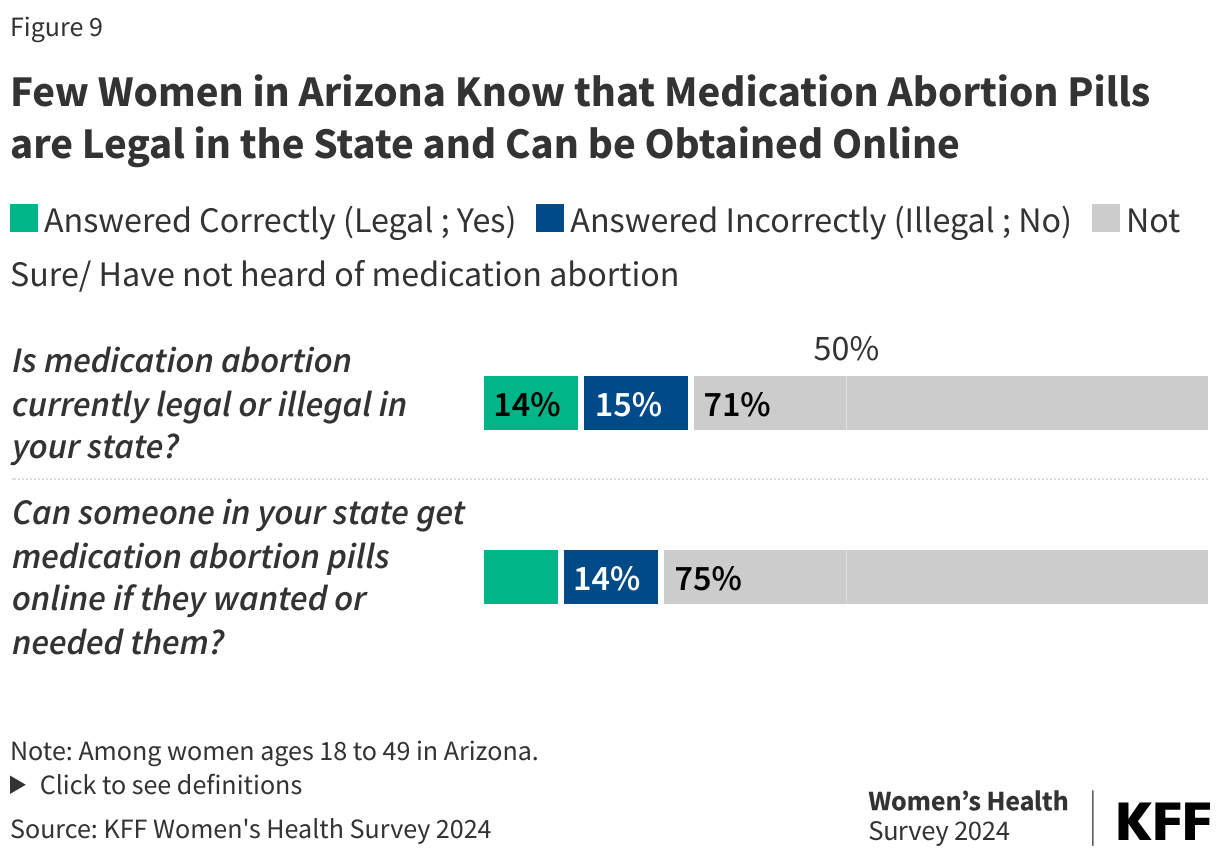
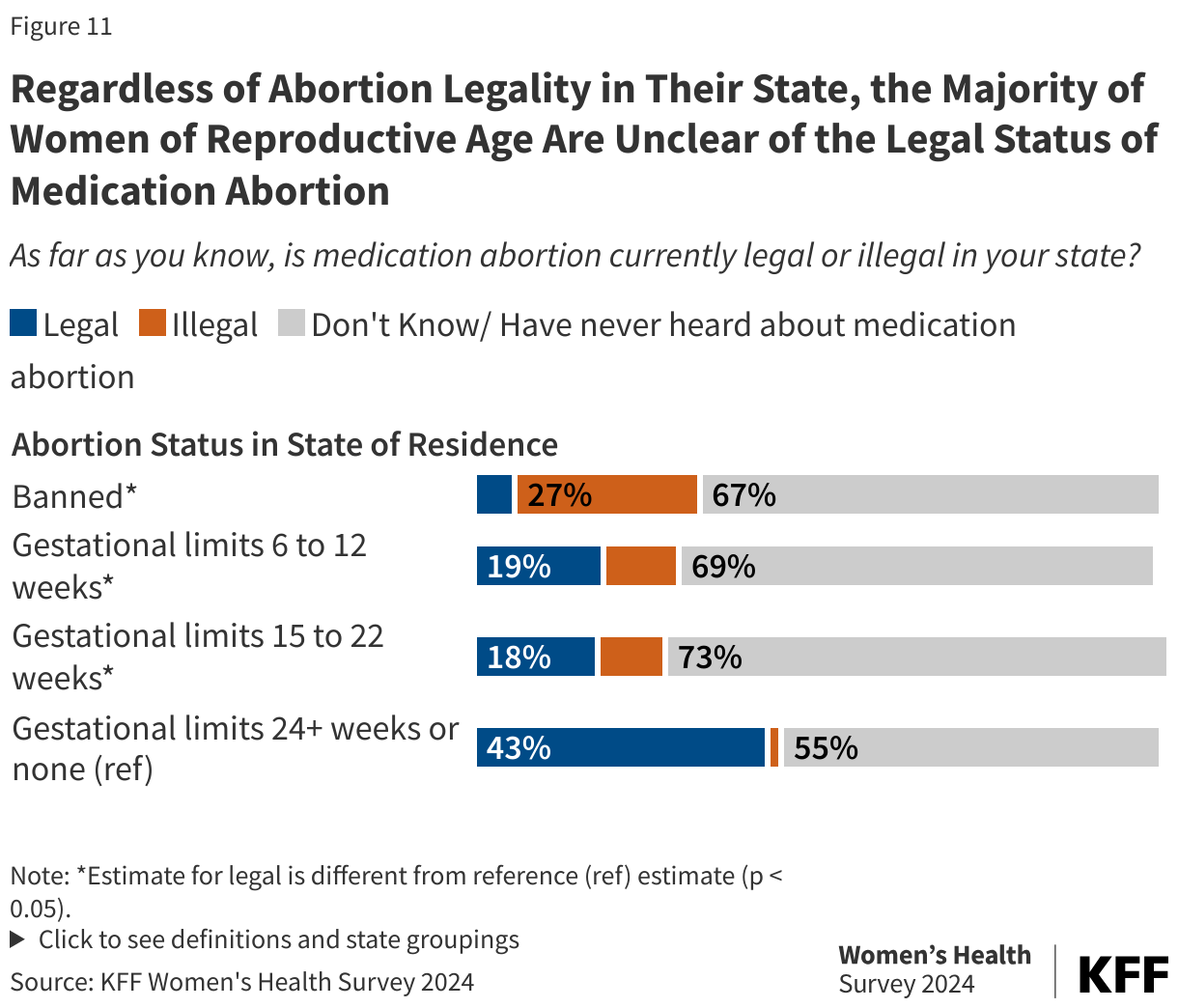
The majority of women of reproductive age are unclear about the legal status of medication abortion in their state, regardless of the legal status of abortion in their state (Figure 11). A larger share of women living in states with gestational limits at 24 weeks or without gestational limits (43%) report that medication abortion is legal in their state compared to women living in states with gestational limits between 6 to 12 weeks (19%) and gestational limits between 15 to 22 weeks (18%). Among women living in states where abortion is banned, 6% say medication abortion is legal in their state and 27% say it is illegal. Regardless of the status of abortion in their state of residence, majorities of women of reproductive age are not aware of the legal status of medication abortion in their state or have never heard of medication abortion.
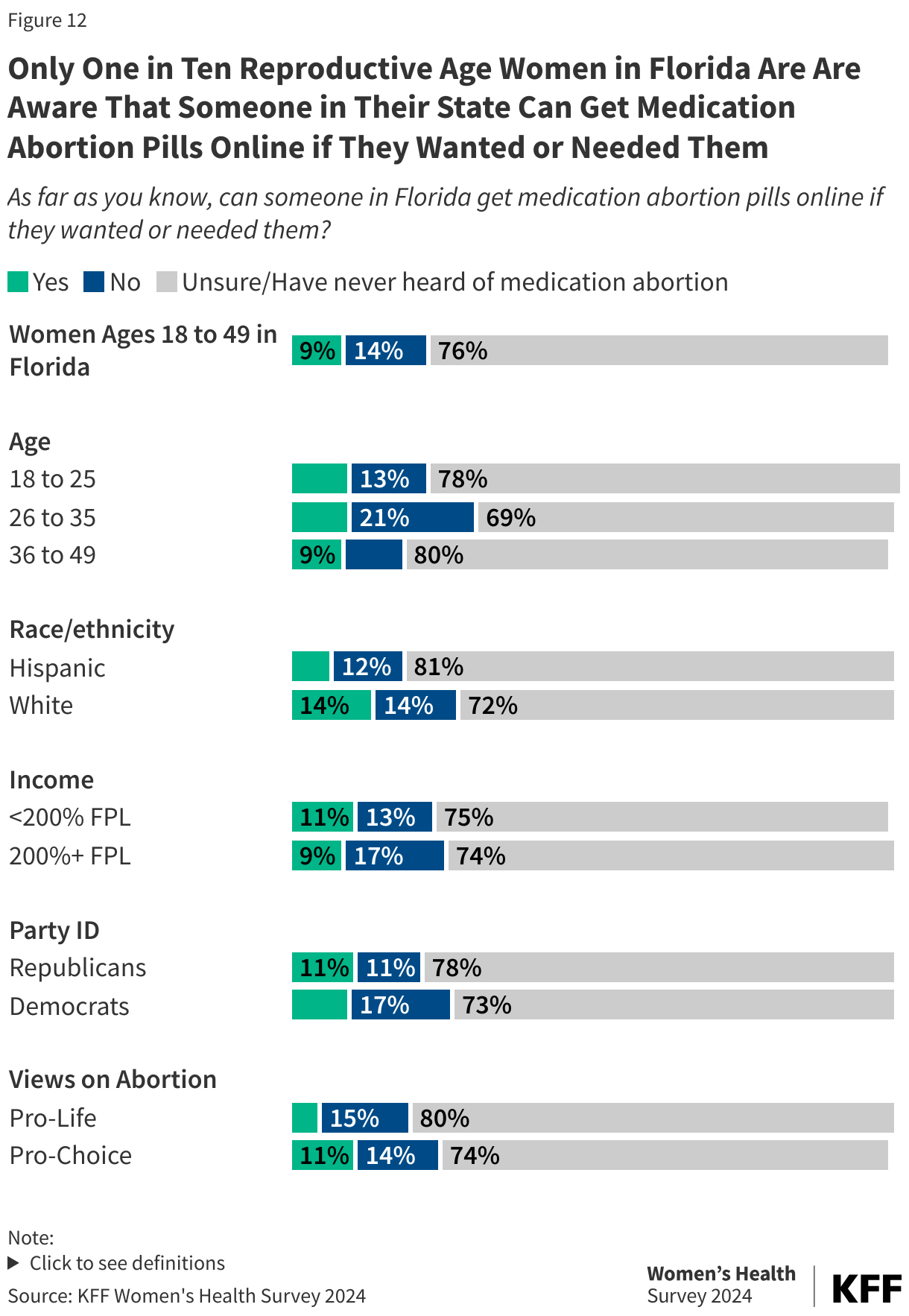
Overall, only one in five (19%) women of reproductive age are aware that medication abortion pills are available online. Since state abortion bans and restrictions have gone into effect, new online services have been created that sell medication abortion pills through online organizations. Among women of reproductive age, 10% say individuals in their state cannot get medication abortion pills online and about three-quarter (71%) were unsure or had never heard of medication abortion (Figure 12). Small shares of women living in states where abortion is banned or states with gestational limits know that people in their states can get medication abortion pills online compared to women living in states without any gestational limits or limits after 24 weeks.
Opinions on Abortion Policy
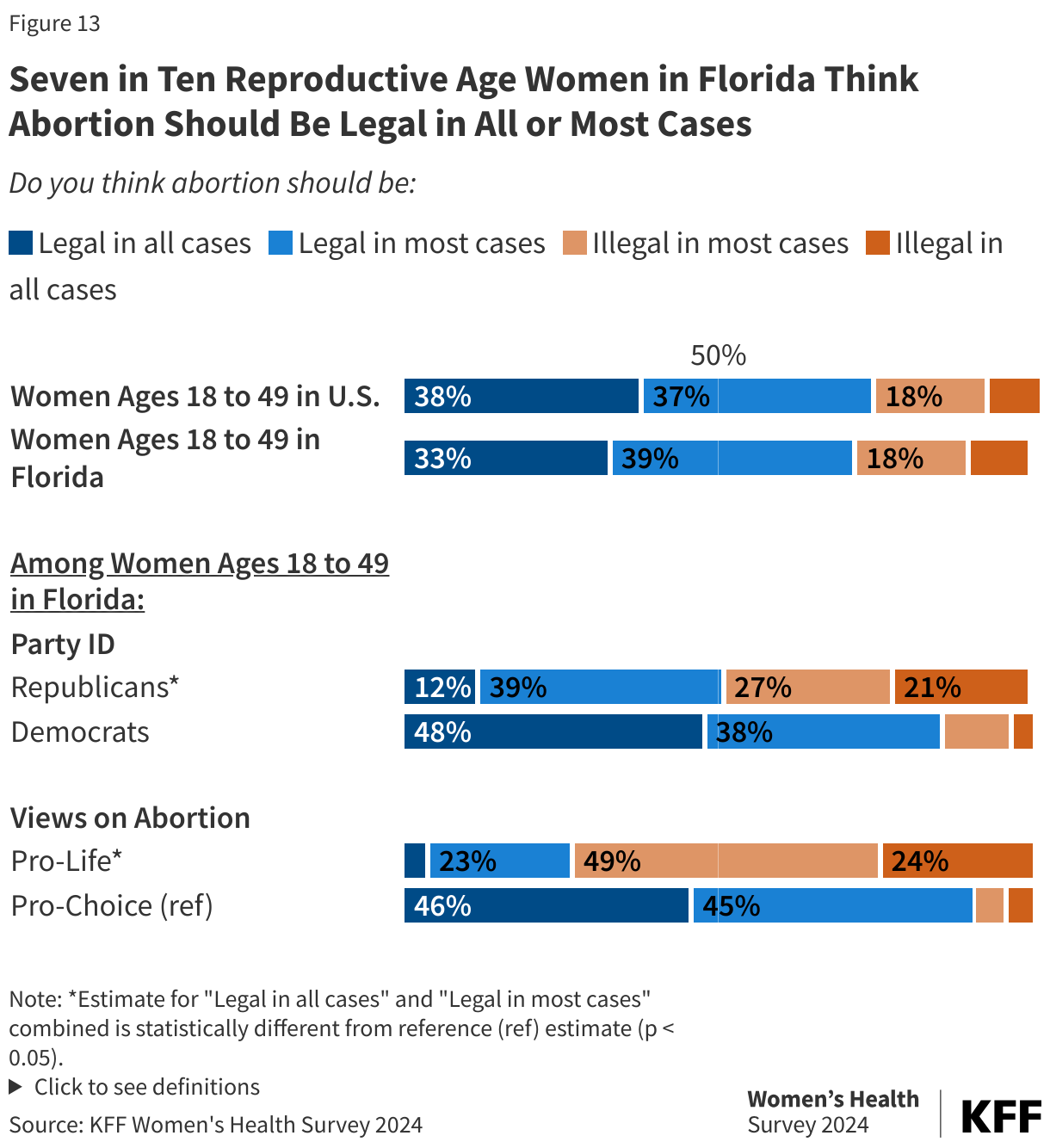
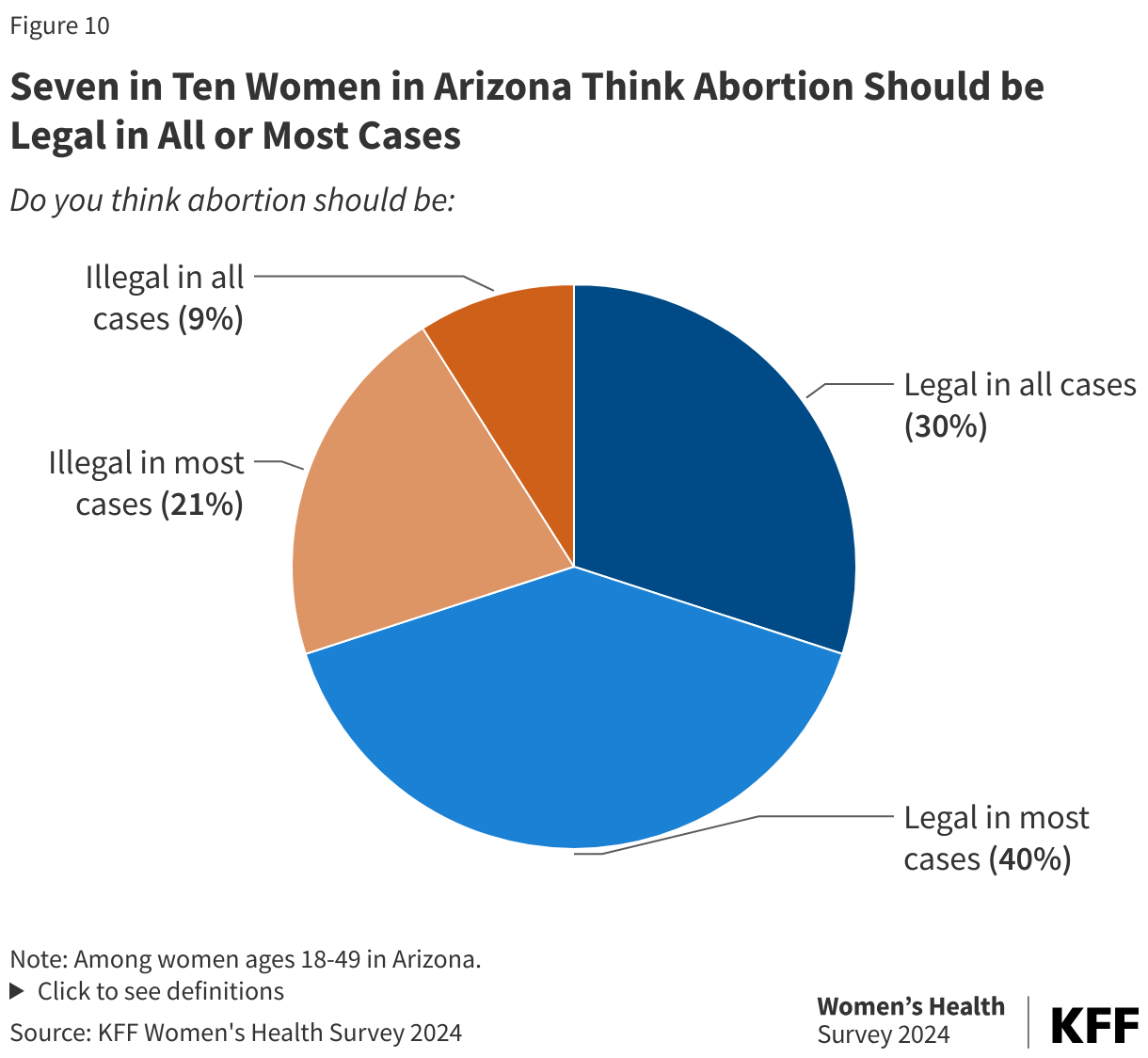
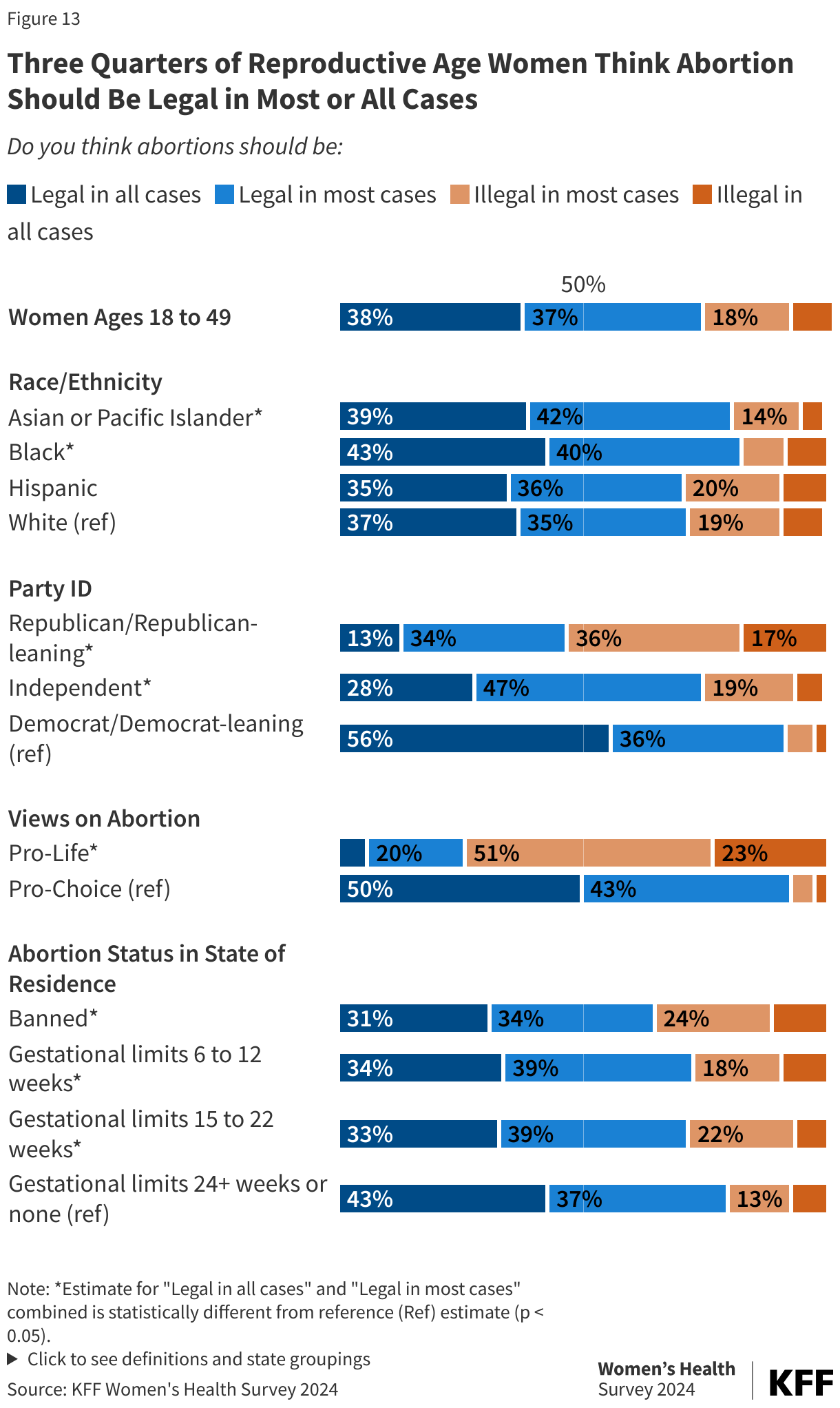
Three in four (75%) women of reproductive age in the United States, the age group that is most directly impacted by state abortion policies, think that abortion should be legal in most or all cases—38% say legal in all cases and 37% legal in most cases. Only 8% of women say that abortion should be illegal in all cases. This trend is consistent with prior polls which have found that the majority of Americans believe that abortion should be legal.
Across various subgroups, except those who identify as Republican or pro-life, majorities of reproductive age women think abortion should be legal in all or most cases. Among those ages 18 to 49, over eight in 10 Black women (83%) and Asian or Pacific Islander women (83%), and almost three-quarters of Hispanic women (73%) and White women (72%) think abortion should be legal (Figure 13). In contrast, slightly less than half (48%) of Republican women of reproductive age think abortion should be legal, 36% say abortion should be illegal in most cases and 17% say abortion should be illegal in all cases. Not surprisingly, among women who identify as pro-life, 74% say that abortion should be illegal in all or most cases, but one in four (25%) believe that abortion should be legal in all or most cases.
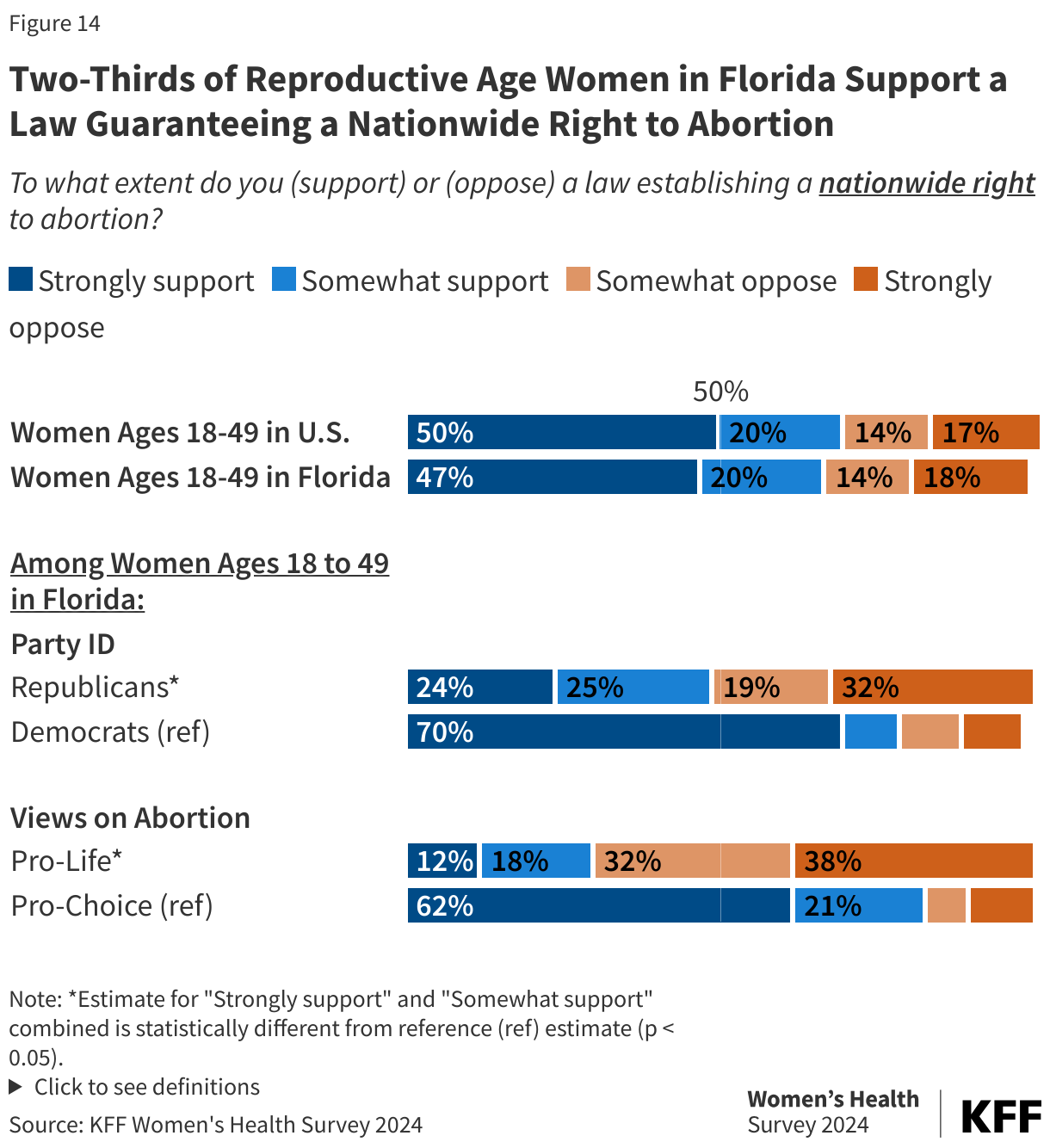
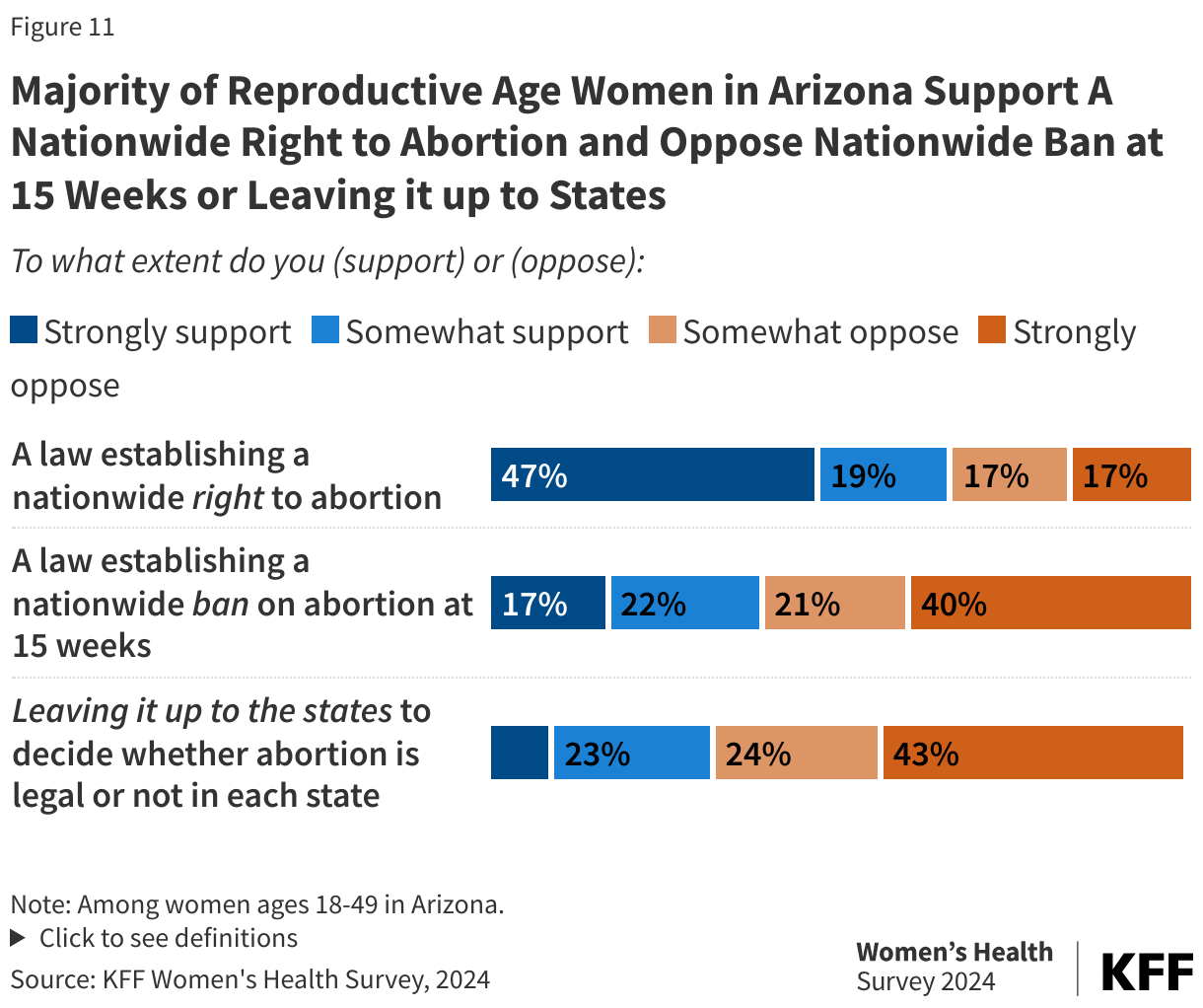
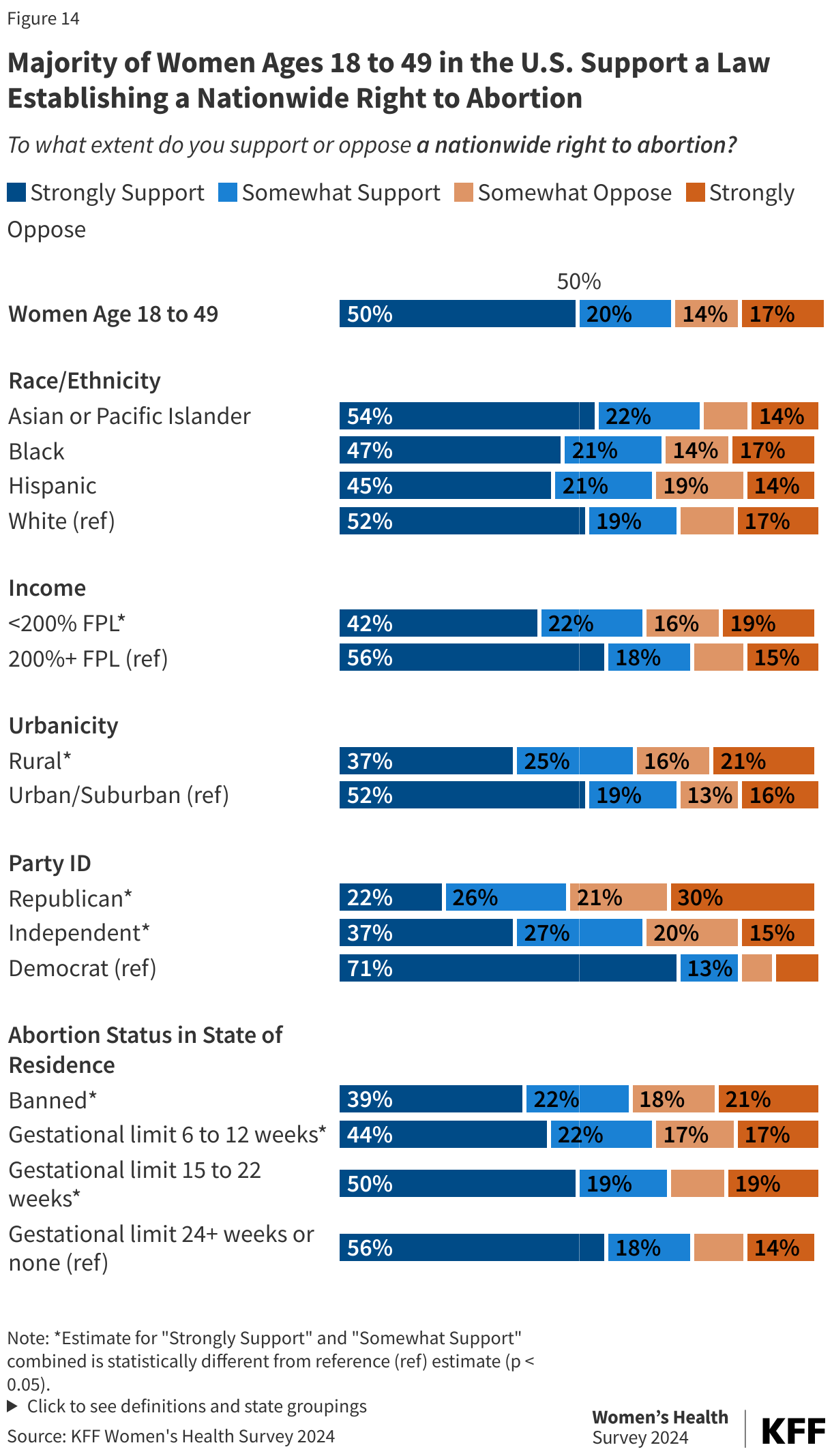
Seven in ten reproductive age women (70%) support a law guaranteeing a federal right to abortion, with half (50%) saying they strongly support this (Figure 17). While similar shares of Asian, Black, Hispanic, and White reproductive age women support a nationwide right to abortion, support varies widely by income, urbanicity, and party affiliation (Figure 14). Though still a majority, smaller shares of reproductive age women with lower incomes (64%) and women who live in rural communities (62%) support a nationwide right to abortion compared to their urban/suburban (71%) and higher income counterparts (74%). Support is strongest among Democratic (84%) women, but two thirds (64%) of women who identify as independents and nearly half of Republican women (48%) strongly or somewhat support establishing a federal right to abortion. More than three times as many Democrats (71%) than Republicans (22%) strongly support a law that would guarantee this right.
More than half of all women of reproductive age support a law establishing a nationwide right to abortion, regardless of the abortion status in their state of residence. While there are smaller shares of support among women who reside in states with bans and gestational limits before viability, over four in 10 women in these states strongly support a law guaranteeing a federal right to abortion.
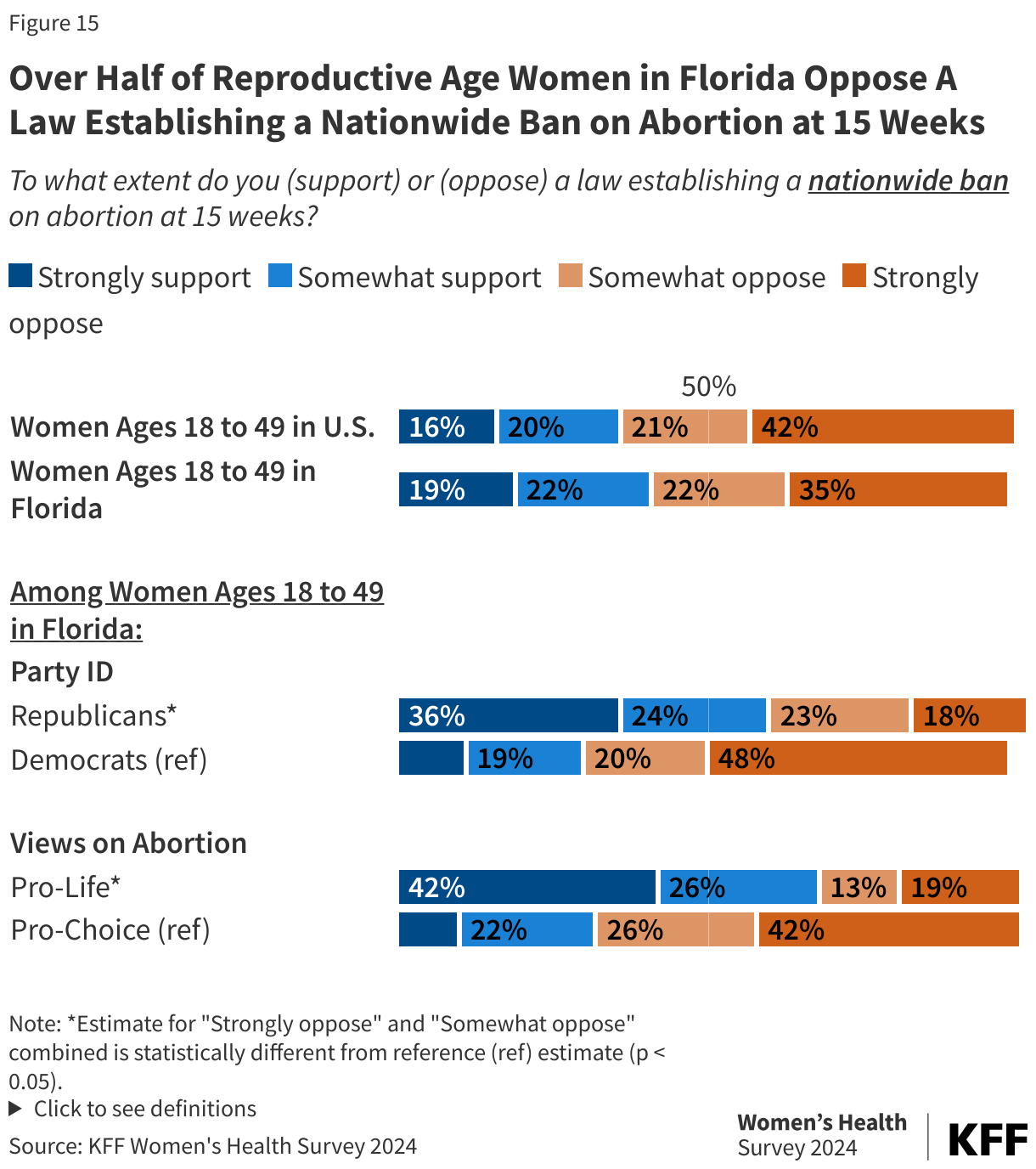
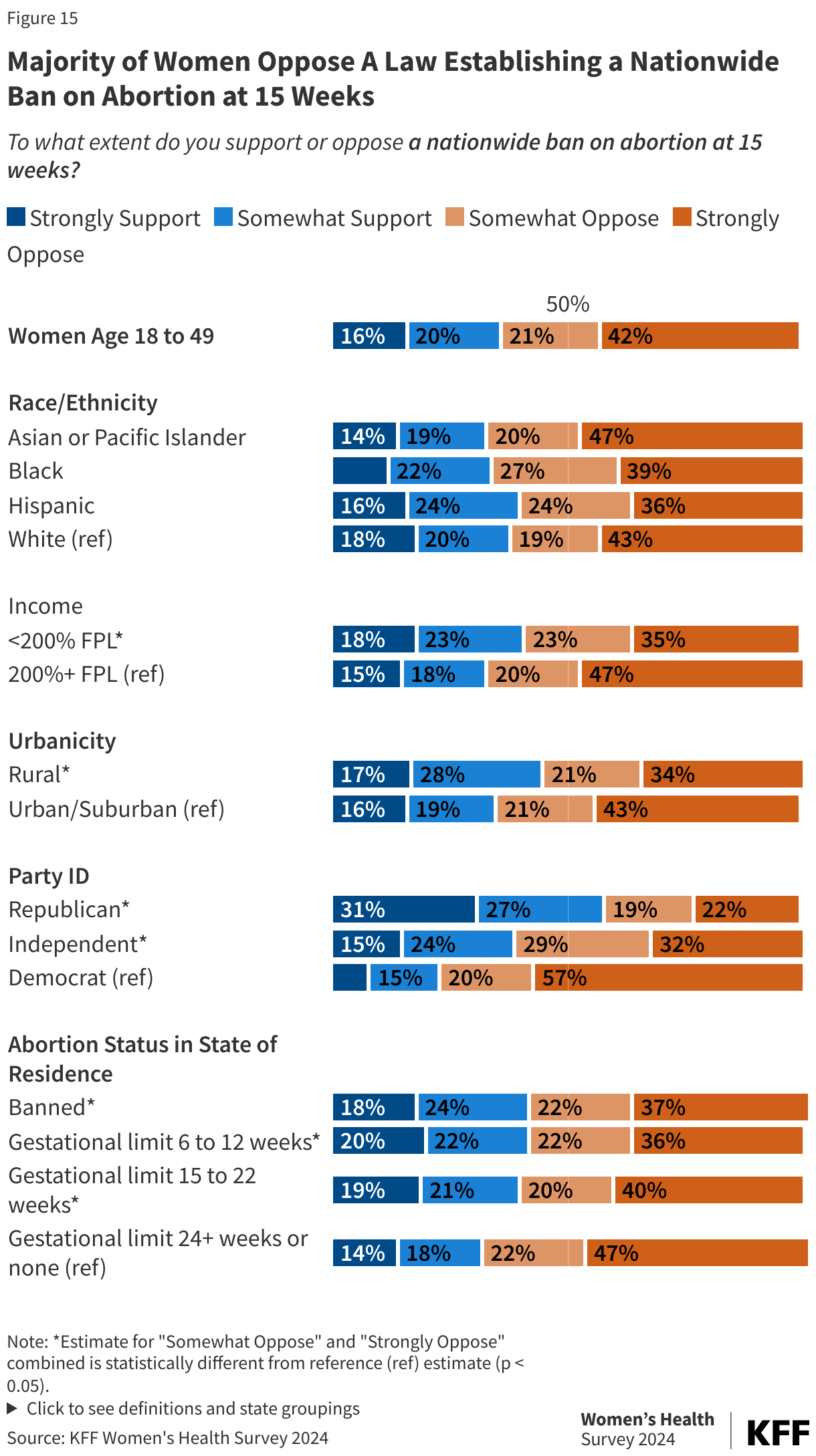
On the issue of abortion, former President Trump has previously said he would consider a national ban at 15 or 16 weeks, a position also proposed by other Republican elected officials. Overall, six in ten women of reproductive age (63%) oppose a law that would establish a nationwide ban on abortion at 15 weeks (Figure 15). While still a majority, smaller shares of those with lower incomes (58%) and those who reside in rural areas (55%) oppose a national abortion ban at 15 weeks. Six in ten women in states with abortion bans and gestational limits before viability oppose a national ban on abortion at 15 weeks.
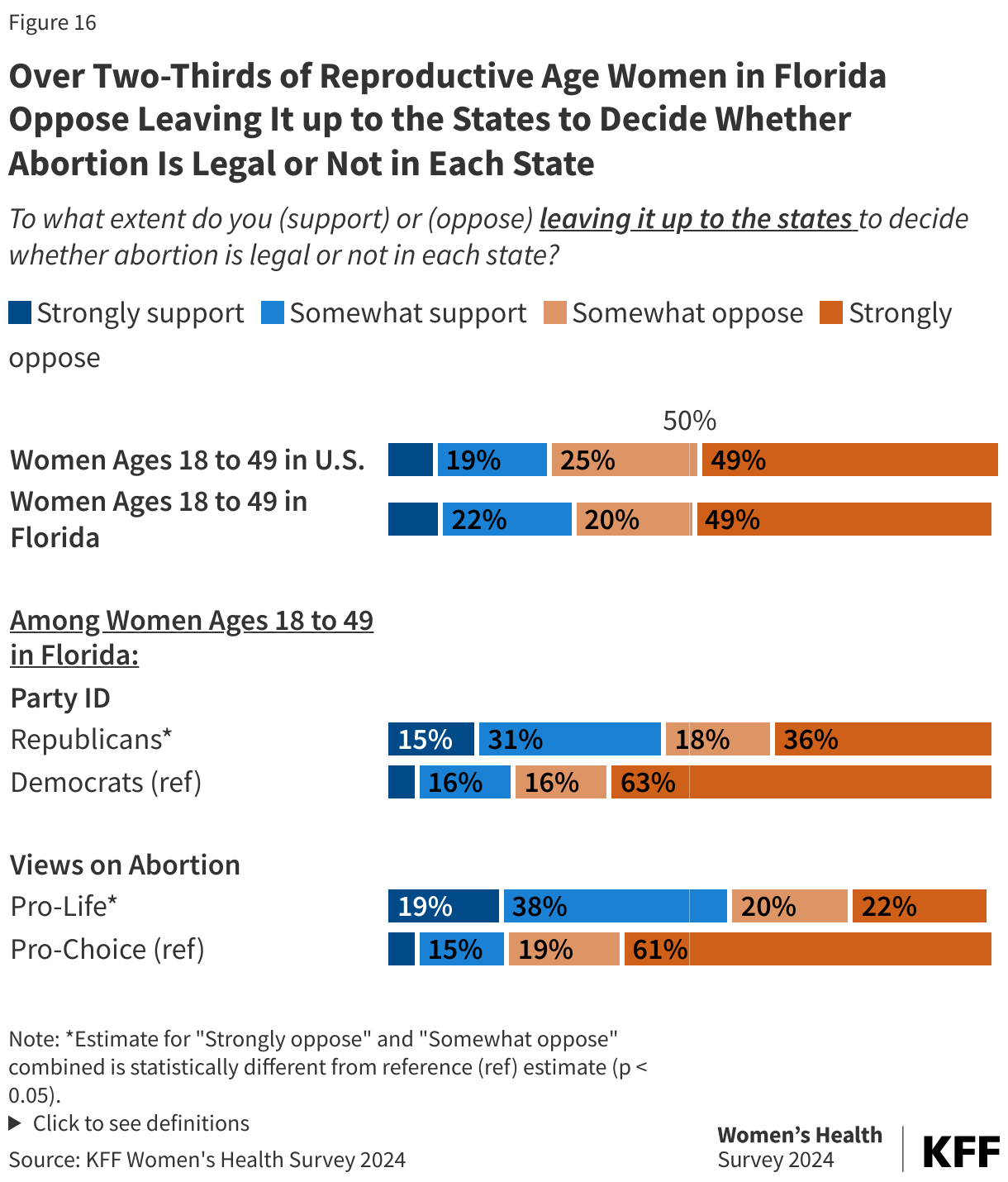
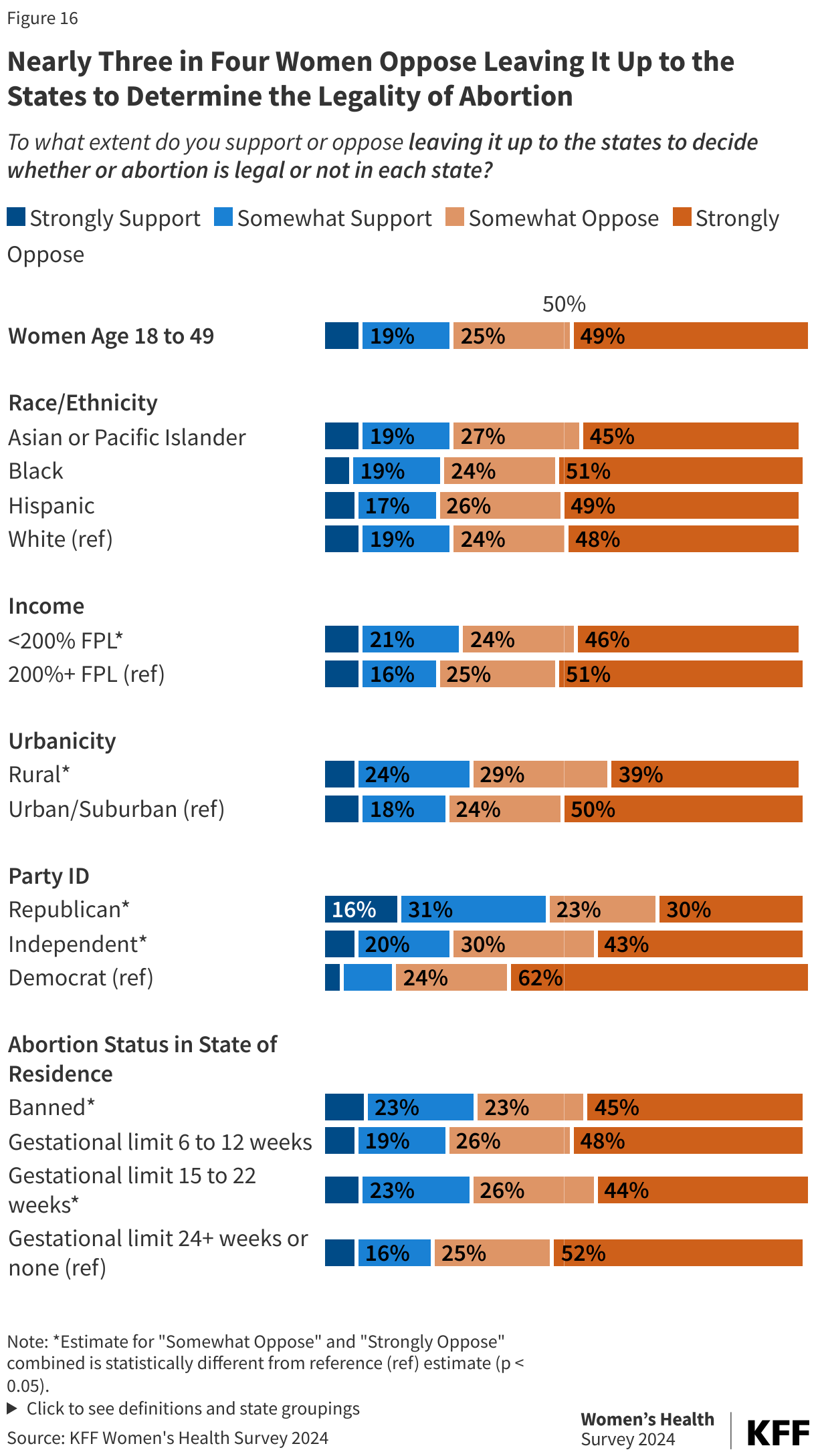
Most recently, former President Trump announced he supports leaving abortion policy up to the individual states, allowing the current bans and restrictions to stay in effect across half the country. Overall, nearly three in four women of reproductive age (74%) oppose this approach (Figure 16). Similar shares of Asian (72%), Black (75%), Hispanic (75%), and White (72%) reproductive age women oppose leaving abortion policy up to the states. Compared to their counterparts, larger shares of women with higher incomes (76%) and those who live in urban/suburban communities (74%) oppose having states decide whether abortion should be legal or illegal in their states.
At least half of all women oppose this approach regardless of party affiliation, but opposition is highest among Democratic women (88%). While there is slight variation in support/opposition by abortion status in a woman’s state of residence, over two thirds of those in states with abortion bans and gestational limits oppose leaving the legality of abortion up to individual states.