New Federal Support for the Public Health Workforce: Analysis of Funding by Jurisdiction
Findings
Key Takeaways
- New federal funding of $3 billion provided to health departments from the American Rescue Plan is designed to build and bolster what has been a depleted public health workforce in the United States.
- The funding, distributed through the CDC’s Public Health Infrastructure Grants (PHIG) program, has been provided to 107 different jurisdictions, including state, county, city, and territorial health departments.
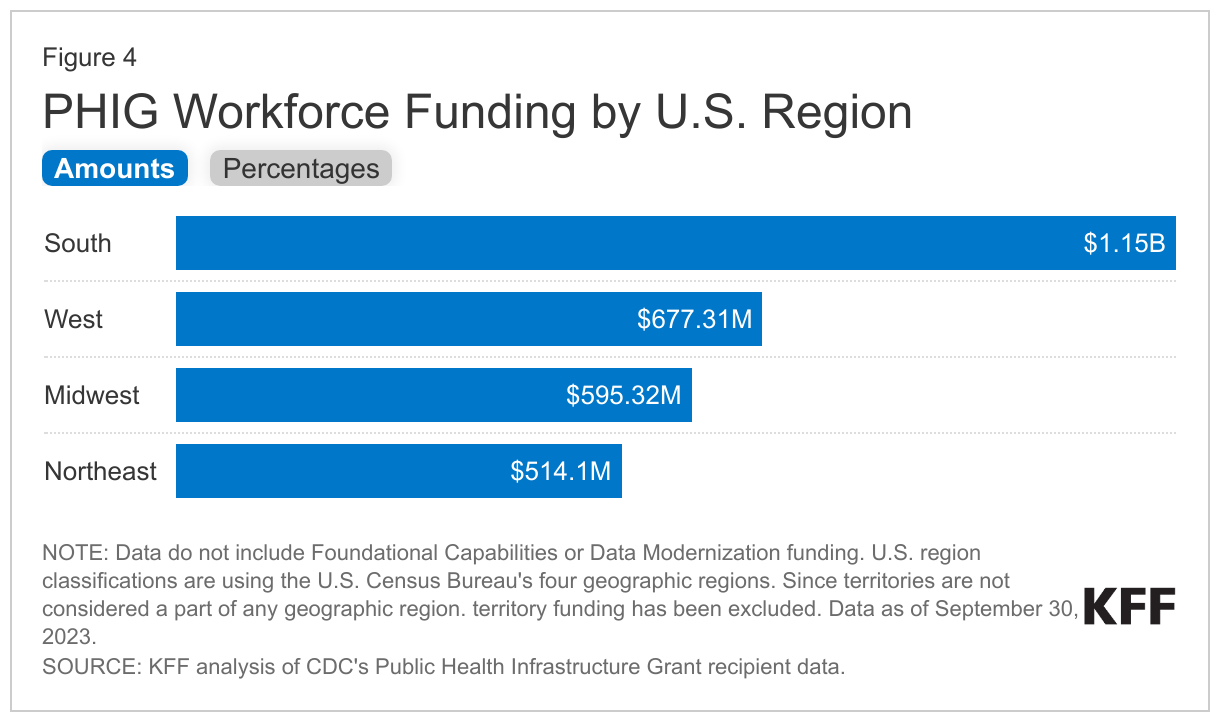
- By region, health departments in the South have received the largest share of funding (39%), followed by those in the West (23%), Midwest (20%) and Northeast (17%).
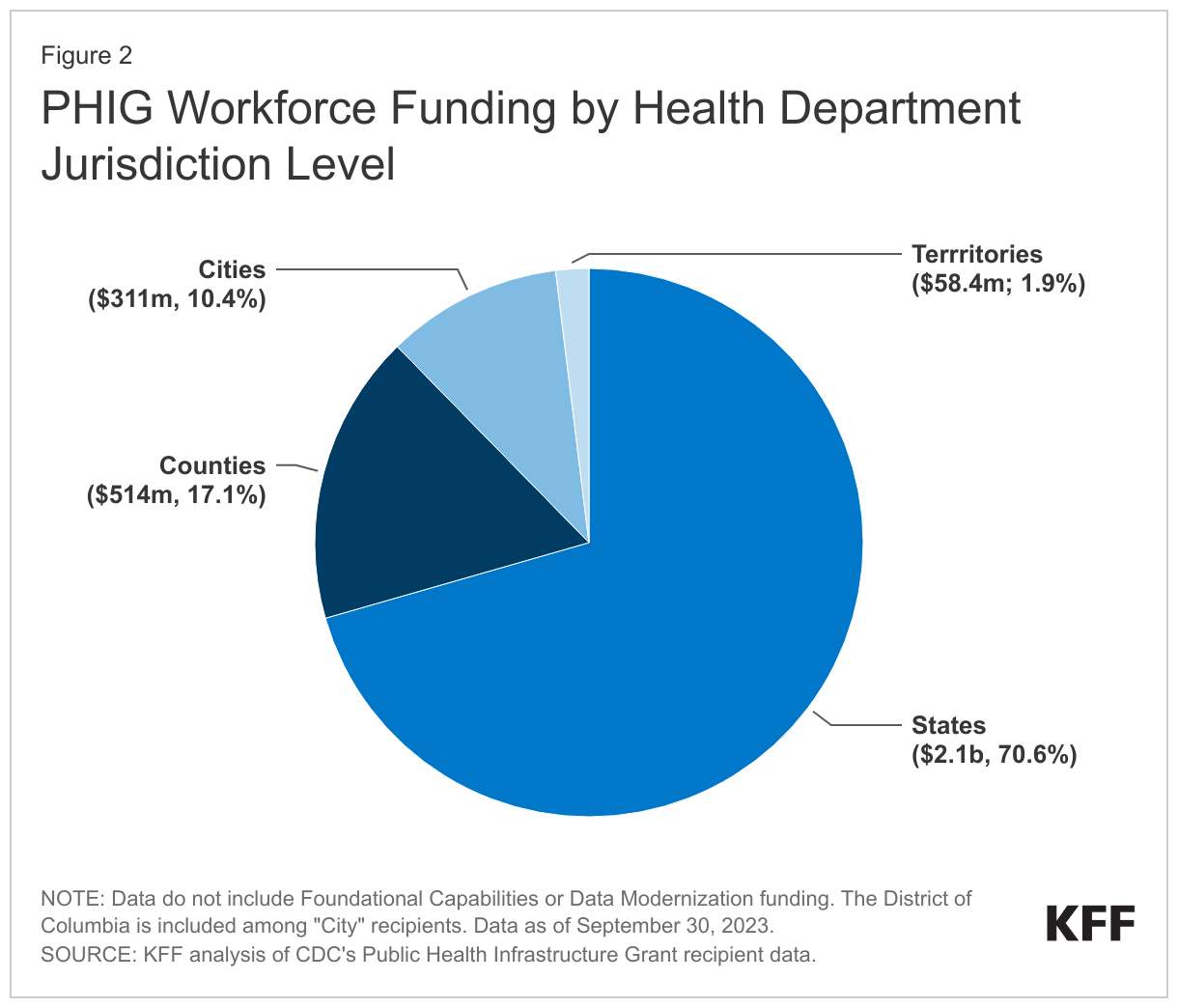
- State health departments have received the greatest share of workforce funding (70.6%) followed by counties (17.1%), cities (10.4%), and territories (1.9%).
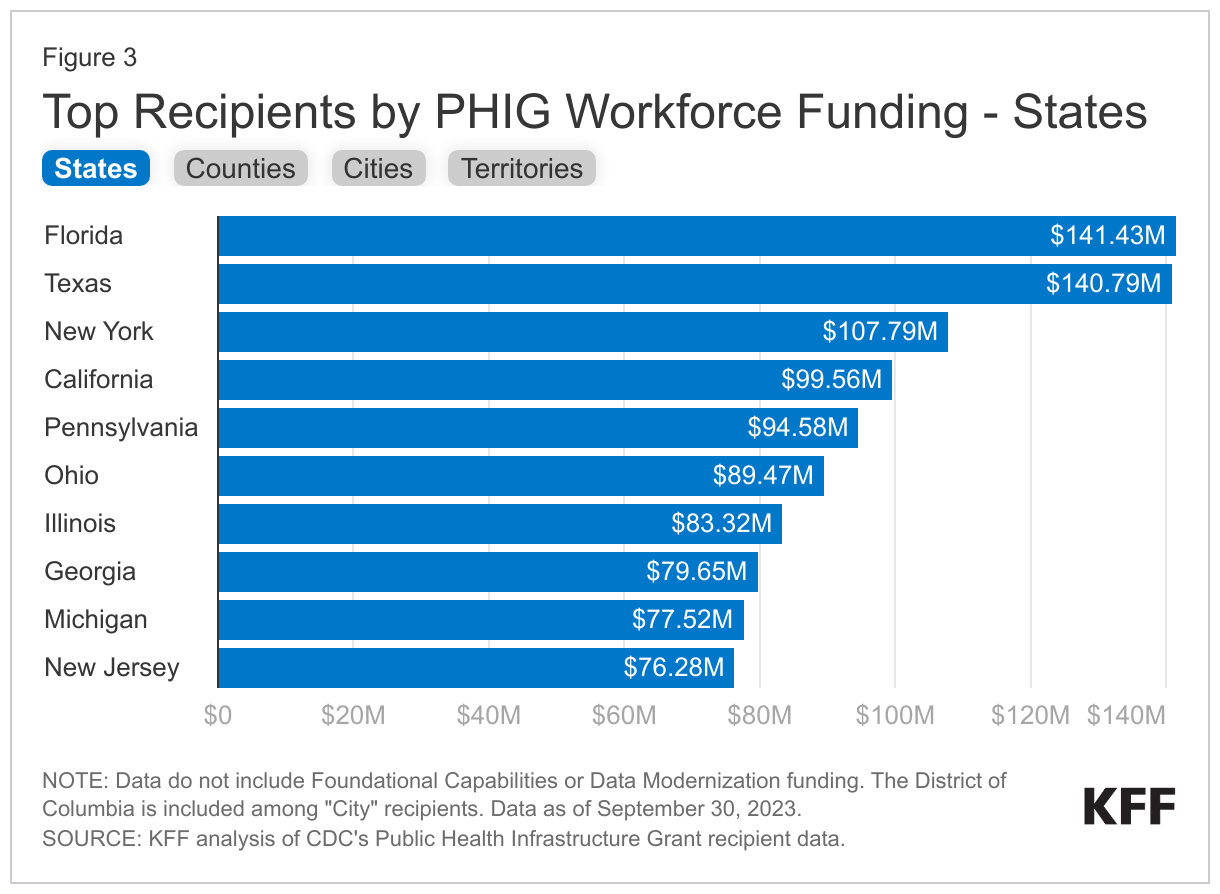
- Among states, Florida received the largest amount of workforce support ($141.4 million), followed by Texas ($140.8 million), and New York ($107.8 million). Together the top ten funded states accounted for 47% of all state funding and 33% of funding overall.
- Jurisdictions report that they plan to use PHIG workforce funds to hire or retain more than 6,000 staff over the five-year grant period, with most planned hires/retentions in Texas, Florida, and Missouri by the end of the grant.
- The size, scope, and flexibility of this funding is unprecedented, as it exceeds any funding provided for the workforce thus far, reaches many more jurisdictions, and extends over a five-year period.
- Data on outcomes and impacts will take longer to materialize, and challenges remain, including the remaining gap between estimated workforce needs and planned staff hires and retentions, and questions about workforce sustainability after the five-year grant period ends.
Introduction
COVID-19 highlighted and exacerbated existing weaknesses in the U.S. public health system, particularly in the public health workforce, which had already been depleted. Public health departments at all levels – including states, counties, large cities, and territories – faced numerous challenges in mounting a response to the pandemic due to a lack of staff, limited funding, and outdated data and communication capabilities, among other issues, and concerns remain about preparedness for future pandemics. In response, Congress provided $7.7 billion through the American Rescue Plan to help shore up the public health workforce, which included funds to be directed to public health departments. In turn, the Centers for Disease Control and Prevention used some of these funds to create a new, five-year, $3 billion Public Health Infrastructure Grants (PHIG) program to help public health departments recruit, retain, and train workers, including to better prepare for future pandemics (the PHIG also includes an additional $140 million for “foundational capabilities” and $200 million for “data modernization”). PHIG launched in 2022 with the $3 billion in workforce funds awarded to health departments in the first year of the grant. The PHIG program is significant for several reasons:
- It is a “non-categorical and cross-cutting” grant mechanism, in contrast to most federal public health funding which is generally targeted to specific diseases, activities, or populations;
- It provides funding for a multi-year period – in this case, five years – as opposed to most public health funding which is typically provided annually (or at most over a two- to three-year period, as was done with other ARPA funding);
- The number of local jurisdictions eligible for funding is significantly greater than other CDC funding mechanisms, including others funded through ARPA; and
- The amount of funding made available for public health jurisdictions to expand their workforce exceeds any prior grant mechanism; for example, the next largest amount was $2 billion in ARPA funds1 awarded in 2021 for a two-year period primarily to address COVID (although those funds could be used for preparedness).
Using newly available data from the CDC, this issue brief analyzes the distribution of PHIG workforce funding by jurisdiction, as well as jurisdictional plans for enhancing the workforce (data on foundational capacities and data modernization are not included), to provide an initial snapshot of how this new funding will be used. Data are as of September 30, 2023.
Overview of PHIG Workforce Funding
As described in the grant announcement, PHIG workforce funds are intended to “reinforce and expand the public health workforce by hiring, retaining, supporting, and training the workforce and by strengthening relevant workforce planning, systems, processes, and policies.” Jurisdictions can use these funds to fill vacancies and create new positions, as well as invest in worker well-being and engagement, along with other activities. Key characteristics and requirements of the grant include:
- As many as 111 jurisdictions, including state2 , county, city, and territorial health departments, are eligible to receive PHIG funds. Counties serving a population of 2,000,000 or more and cities serving a population 400,000 or more are eligible as direct recipients.
- A funding formula based on the size of the population served by a jurisdiction as well as an adjustment factor for “community vulnerability”, using the U.S. Census’s Community Resilience Estimates, is used to determine allocations. The base funding amount for all awards is set at $2.5 million and the ceiling at $150 million.
- Jurisdictions are expected to focus their workforce efforts on six key activities and have some flexibility to choose among these (see Table 1). While encouraged to include all six activities in their plans, they are required to include #1 (recruit and hire new public health staff) and #6 (strengthen support for implementation). Under #6, recipients must hire a Workforce Director to help oversee implementation and at least one staff member to conduct evaluation.
| Table 1: PHIG Workforce Strategy Key Activities and Examples | |
| Key Activity | Examples |
| 1. Recruit and hire new public health staff | Conduct workforce needs assessments, expand recruitment efforts, revise job pay scales, offer hiring incentives, establish internships and fellowships |
| 2. Retain public health staff | Offer retention incentives such as loan repayment and moving expenses, revise terms for existing jobs to allow for more pay or benefits, maximize hybrid work opportunities |
| 3. Support and sustain the public health workforce | Adopt workplace programs for staff well-being, strengthen employee engagement, conduct staff viewpoint surveys, share and use employee input in strategic planning and other workplace initiatives |
| 4. Train new and existing public health staff | Add training offerings, establish or revise training tracks or certificate programs, support staff who enroll in outside trainings |
| 5. Strengthen workforce planning, systems, processes, and policies | Create or revise a workforce development strategy, catalyze the collection and use of workforce data, refresh online recruitment and hiring portals, conduct quality improvement on existing systems |
| 6. Strengthen support for implementation of this grant | Hire a Workforce Director to manage the grant, staff to conduct program evaluation and performance measurement, and a Data Modernization Director. |
| SOURCE: HHS/CDC PHIG Grant Opportunity – “U.S. Public Infrastructure, Workforce, and Data Systems” June 2022. | |
Findings
PHIG workforce funding has been awarded to 107 public health departments across the country, with most channeled to state jurisdictions, and the largest share to the South, largely reflecting the size of a jurisdiction’s population.
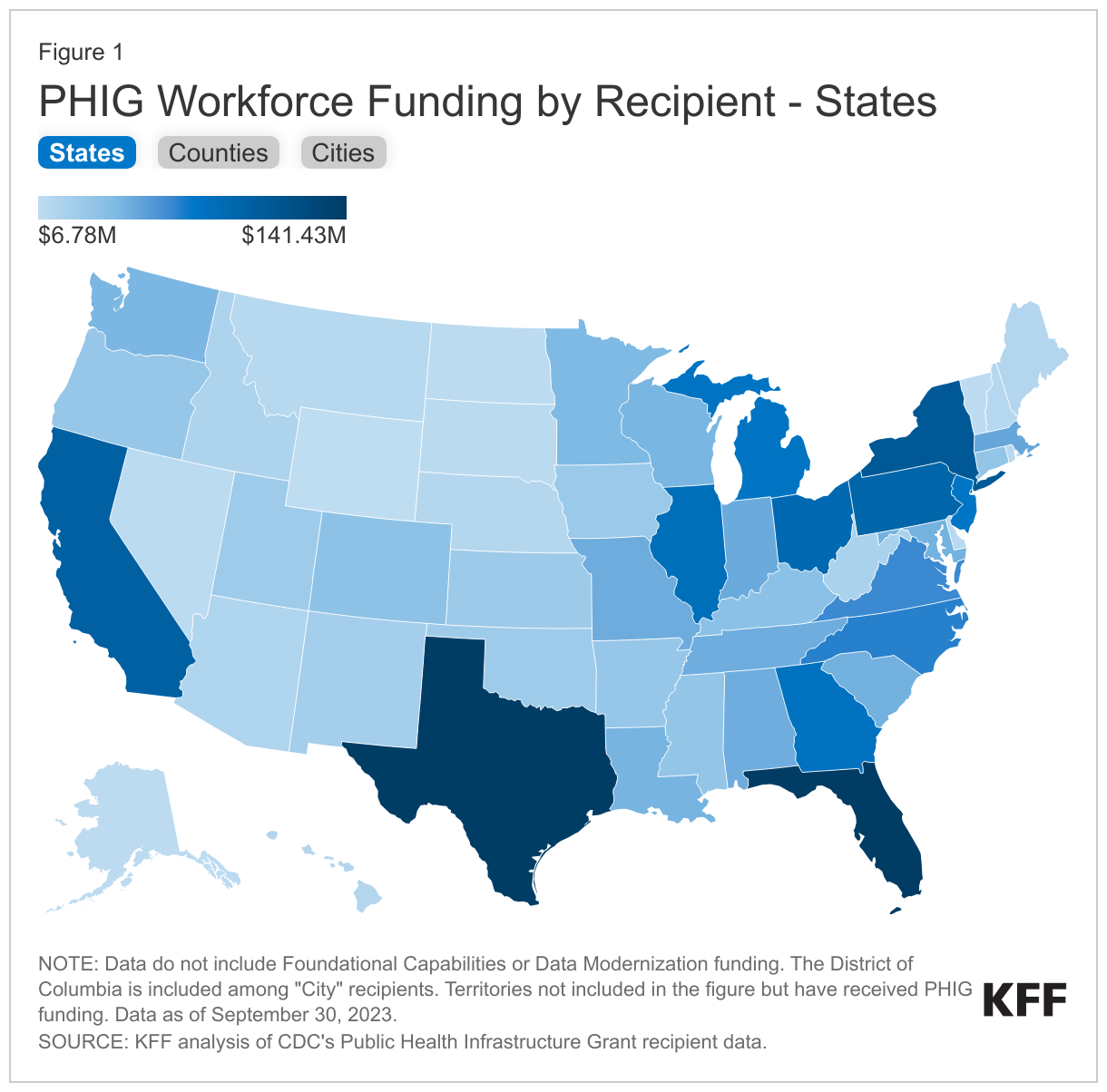
- The 107 health department recipients include those in all 50 states and Washington D.C., 27 counties, 21 cities, and eight territories (see Figure 1).
- State health departments have received the largest share of funding (70.6%), followed by counties (17.1%), cities (10.4%), and territories (1.9%) (see Figure 2).
- The top ten funded states accounted for 47% of all state funding and 33% of funding overall. Among states, Florida received the largest amount ($141.4 million), followed by Texas ($140.8 million), and New York ($107.8 million) (see Figure 3).
- The top ten funded counties accounted for 61% of all county funding and 10% of funding overall. Among counties, Los Angeles County, California received the largest amount ($79.8 million), followed by Maricopa County, Arizona ($38.0 million), and Miami-Dade County, Florida ($27.8 million).
- The top ten funded cities accounted for 71% of all city funding and 7% of funding overall. Among cities, New York City received the largest amount ($84.6 million), followed by Chicago ($27.1 million), and Houston ($23.3 million).
- The eight territories received 2% of funding overall. Among territories, Puerto Rico received the largest amount ($34.9 million), followed by Guam ($4.3 million), and the U.S. Virgin Islands ($3.6 million).
- By region, health departments in the South have received the largest share of funding (39%), followed by the West (23%), Midwest (20%) and Northeast (17%) (see Figure 4).
Funding per capita for all recipients combined was $8.95, with significant variation in some cases. For example, per capita funding for territories was almost twice that of states. This partly reflects the fact that there is a base funding amount for all jurisdictions, regardless of population size.3
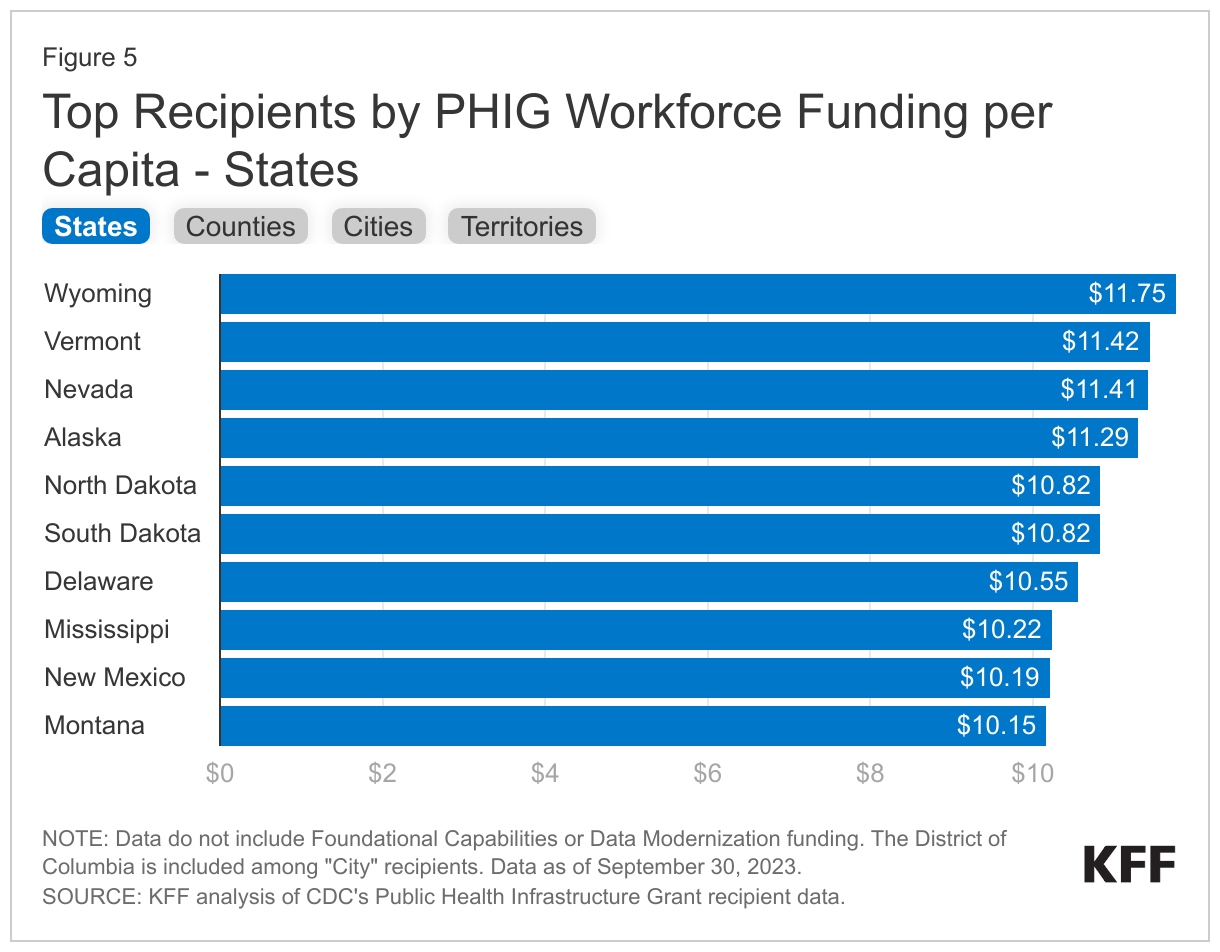
- Per capita funding was $8.95 overall, though it ranged among all jurisdictions from a low of $7.49 for the state of Utah to a high of $125.69 for the territory of Palau.
- Comparing across jurisdiction types, states had the lowest per capita funding ($8.57), followed by counties ($9.10) and cities ($11.00). Territories, which generally have the lowest population size of any jurisdiction, received $15.91 per capita.
- Within states, funding per capita ranged from $7.49 in Utah to $11.75 in Wyoming. In counties, it ranged from $8.03 in King County, Washington to $11.87 in Douglas County, Nebraska. Among city recipients per capita funding amounts ranged from $9.43 in Columbus to $13.88 in Long Beach, and in territories it ranged from $11.27 in Puerto Rico to $125.69 in Palau (see Figure 5).
Most workforce funding is being channeled to the two required workforce activities under the grant – “strengthening grant implementation” and “recruitment and hiring” – although there is variation across jurisdictions.
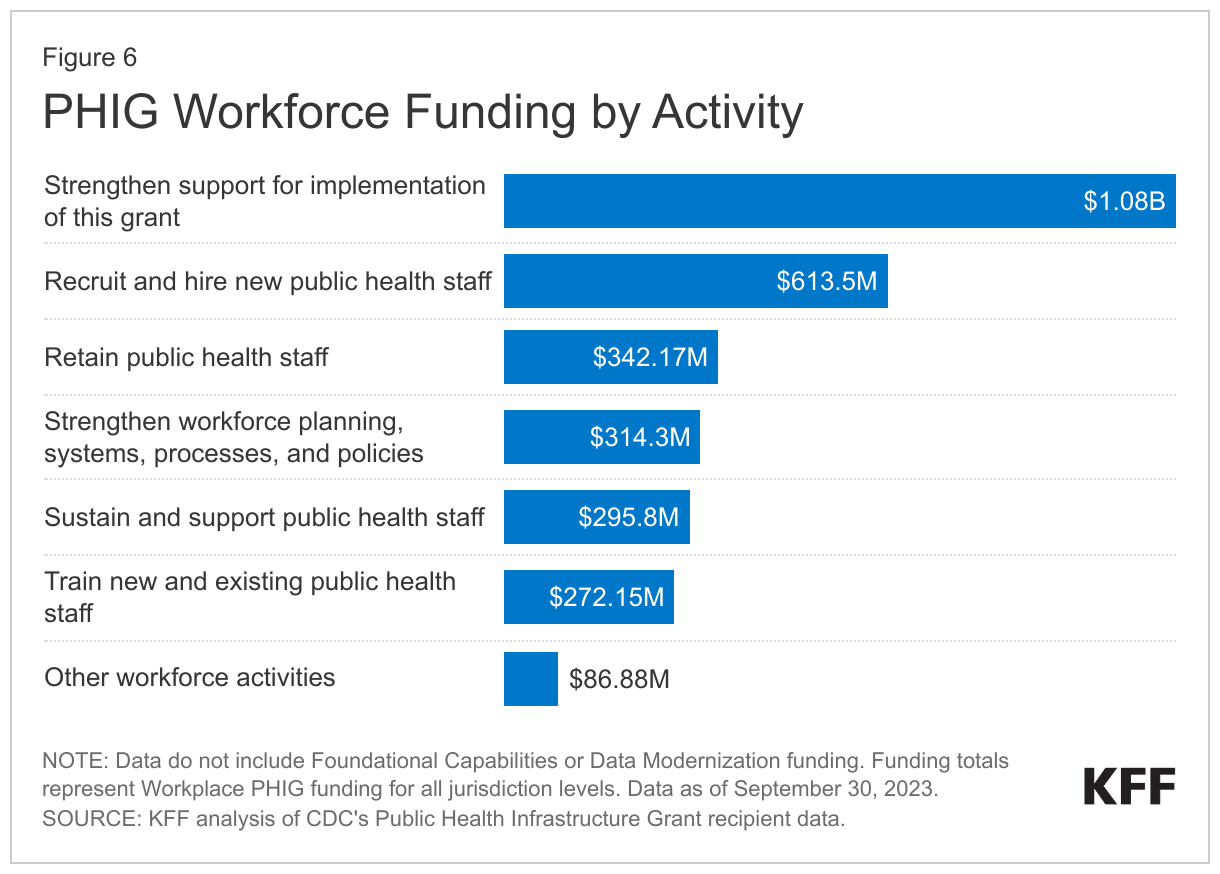
- More than a third ($1.1 billion or 36%) of funding is to “Strengthen support for implementation of this grant”, which includes hiring a Workforce Director and evaluation staff. The next largest category is recruitment and hiring of staff ($613 million or 20%) followed by staff retention ($342 million or 11%). The remaining 33% is divided among four other activities (see Figure 6).
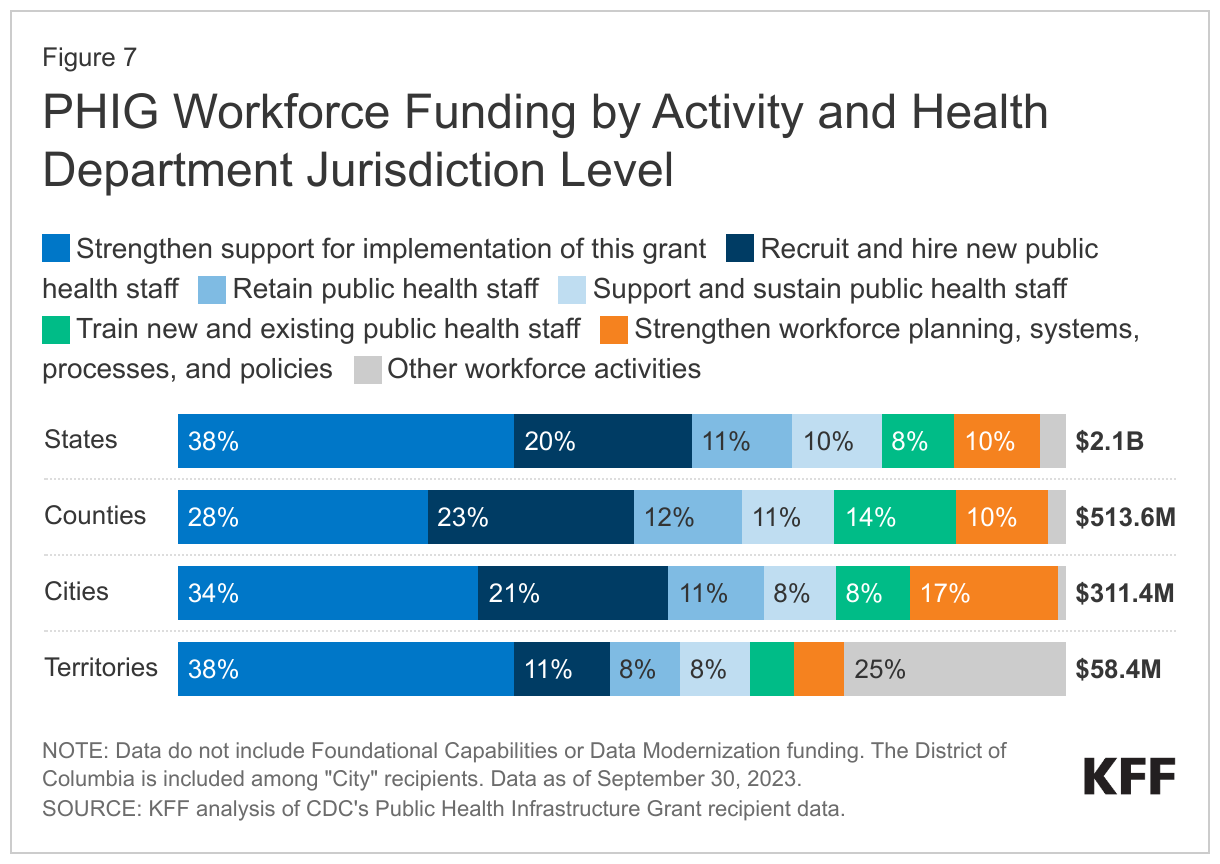
- There is some variation by jurisdiction level. For example, states were more likely to use funds for strengthening grant implementation (38%) than counties (28%), and counties were more likely to use funding for recruitment and hiring (23%) than territories (11%) (see Figure 7).
- Only seven jurisdictions did not channel most workforce funding to the two required categories. For example, in two jurisdictions (Washington and Fulton County, Georgia), “Support and sustain the public health workforce” was the top funded category and in two jurisdictions (Austin and Dallas County, Texas), “Retain public health staff” was the top category.
Jurisdictions report that they plan to hire or retain more than 6,000 staff over the five-year grant period, with the largest share expected to support organizational competencies.4
- In year 1, jurisdictions plan to hire or retain 3,862 staff, rising to 6,152 by year 5.
- State jurisdictions plan to hire the greatest number of staff (2,471 staff in year 1 and 3,822 by year 5), followed by counties (800 and 1,207), cities (377 and 754), and territories (214 and 369). The average number of staff to be hired/retained across all jurisdictions is 36.4 in year 1 and 58.0 in year 5, though this varies by health department level.
- The jurisdictions planning to hire/retain the most staff in year 1 are Texas (433), Los Angeles County (189), and Florida (186); by year 5, it is Texas, Florida, and Missouri.
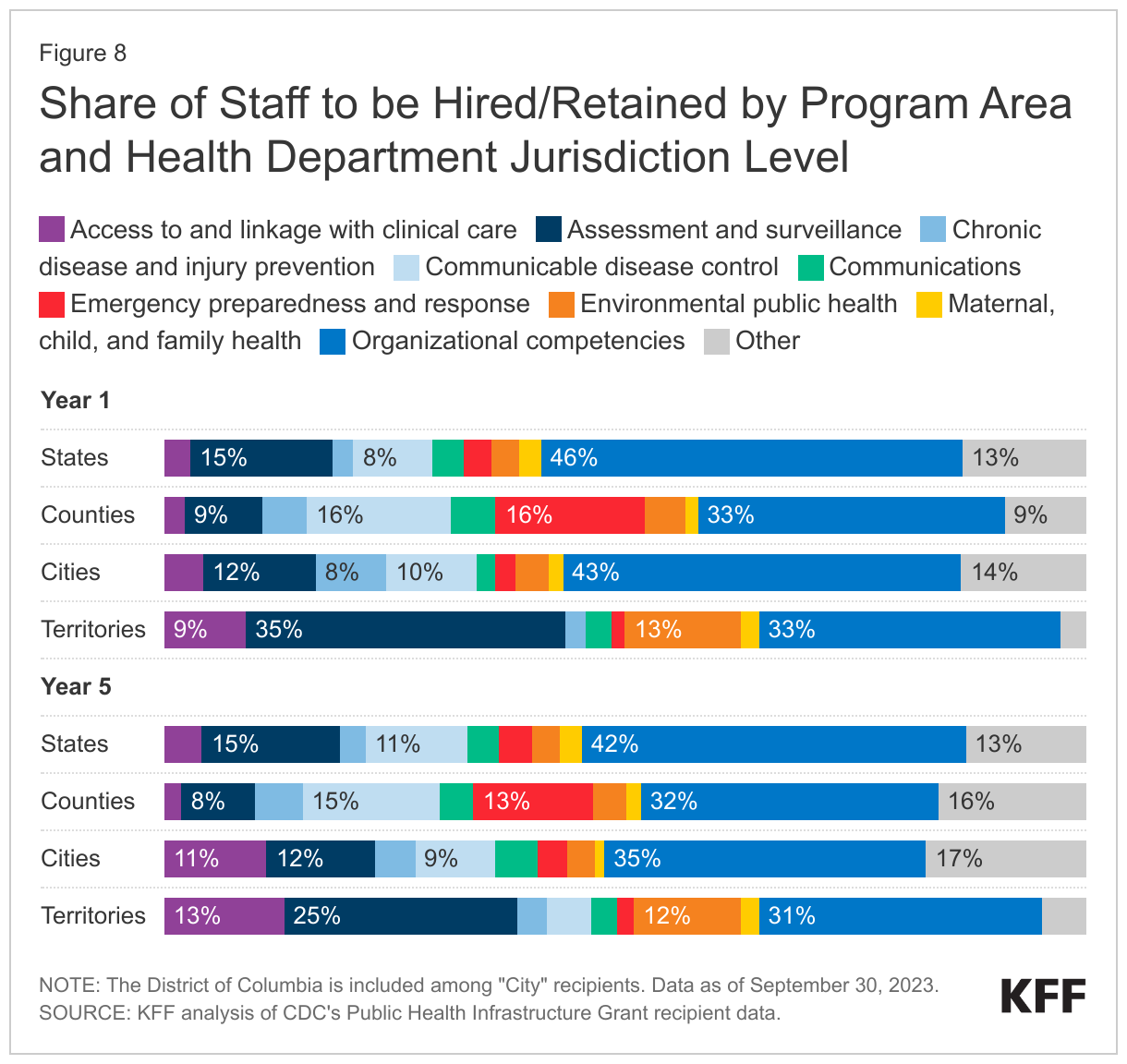
- When asked for expected hiring/retention numbers across ten defined public health program areas, jurisdictions reported the largest share of expected hires/retained staff by year 5 in “Organizational competencies” (38% of all staff hires and retentions), followed by “Assessment and surveillance” (14%) and "Other” (14%). The program areas with the smallest shares of planned hires/retained staff are “Maternal, child, and family health” (2%), “Chronic disease and injury prevention (3%), and “Environmental public health” (4%). There is some variation by health department level. For example, by year 5, 42% of staff hired/retained by states are expected in organizational competencies compared to 31% by territories in that category. Territories plan for a greater share of staff in assessment and surveillance (25%) compared to other jurisdiction types (see Figure 8).
Discussion
New federal funding of $3 billion provided to health departments from the American Rescue Plan is designed to build and bolster what has been a depleted public health workforce in the United States. The size, scope, and flexibility of the funding is unprecedented, as it exceeds any funding provided for the workforce thus far, reaches many more jurisdictions, and extends over a five-year period. This analysis of initial data from the CDC provides an early look at how funding has been distributed across the country and what jurisdictions plan to do with this support. As shown here, states have received the largest share of funding, (70.6%), followed by counties (17.1%), cities (10.4%), and territories (1.9%), reflecting the size of the populations they serve. Jurisdictions plan to use funds to hire or retain more than 6,000 staff by the end of the five-year period, with states leading the way in this area. Most funding will be channeled to the two required areas of the grant, strengthening support for implementation through hiring key personnel and recruitment and hiring of staff, followed by staff retention more generally. Across all these areas there is notable variation among recipients, which appears to reflect the design of the PHIG in allowing flexibility to address the unique needs of different jurisdictions.
Still, while these data provide an early snapshot of how this funding will be used, data on outcomes and impacts will take a much longer time to materialize. Moreover, despite the size of the grant and multi-year nature of the funding, there are challenges that remain. First, the planned number of staff hires and retentions represent only a fraction of estimates of the need for a public health workforce in the U.S. Additionally, while funding is provided for a five-year period, longer than most jurisdictional grants, there are questions about the sustainability of hiring beyond this period, with jurisdictions already expressing concerns about the future. More broadly, the extent to which this funding can help plug the very deep hole, even temporarily, in the public health workforce that would be required to adequately prepare and respond to future threats remains to be seen. Monitoring the impact of these investments, including how enduring they may be, will be important for assessing the strength of the nation’s public health infrastructure and its ability to handle new challenges going forward.
Appendix


Endnotes
- At least 25% of these awards were required to be used school-based health programs. ↩︎
- The grant also requires that no less than 40% of workforce funds provided to state health departments be distributed to local health departments that have not received direct funding from the grant. ↩︎
- Population served estimates consider counties within states and cities within states and counties, so population is not counted more than once. ↩︎
- Data on staff to be hired/retained based on workforce and foundational capabilities funds. Jurisdictions potentially will have additional hires via data modernization funds, but that data is not yet available. ↩︎