The ‘Pandemic Agreement’: What it is, What it isn’t, and What it Could Mean for the U.S.
This brief was updated on June 18 to reflect developments at the 2024 World Health Assembly.
Member states of the World Health Organization (WHO) are in the process of negotiating a new international ‘pandemic agreement’ (also referred to as a ‘pandemic accord’ or ‘pandemic treaty’). Since 2021, member states have held a series of meetings to draft this new agreement. Earlier this year it was expected the process would culminate with a vote on a final text at this year’s World Health Assembly (WHA) in May 2024 but due to a lack of consensus on a number of articles, member states chose to extend the timeline for negotiations until next year, with an expectation that a final vote on any agreement would take place at the May 2025 WHA (potentially earlier if agreement is reached before then).
The Biden administration has supported the concept of an agreement, and has been engaged in negotiations since the process launched. At the same time, several issues have been raised by U.S. policymakers and others, including whether and how the U.S. should ultimately choose to become a party to the agreement. . Given that the negotiating timeline has been extended into next year, the outcome of the U.S. Presidential election this fall is likely to have significant implications for U.S. positions on the agreement and its participation in negotiations in 2025. If President Trump were to be elected, for example, it is unclear if he would support an agreement, given his criticism of WHO and his move to withdraw from the organization when he was President, as well as his overall “America First” approach to international engagement.
What is the Pandemic Agreement?
The pandemic agreement is a potential international agreement currently being negotiated by the 194 member states of the WHO, including the U.S. Many governments and WHO leadership felt it was necessary to develop a new agreement to address some of the weaknesses in capacities and lack of international cooperation that occurred during the global response to COVID-19. The formal negotiation process (known as the International Negotiating Body, or INB) was launched in 2021. In the view of the WHO Director-General, there would be three key benefits to a new agreement: driving a more equitable global response, helping safeguard national health systems, and enhancing cooperation among member states during pandemics.
According to the latest publicly available draft text (dated 13 March), the overall objective of this new pandemic agreement is to help the world “prevent, prepare for and respond to pandemics.” Among the provisions included (all of which are still being negotiated) are definitions and principles, aspirational goals for improving pandemic preparedness and response capacities, supply chain and logistics, communication, and oversight and implementation for the agreement, with some of the more contested and debated provisions being financing for pandemic preparedness and response, pathogen access and benefit sharing (PABS), intellectual property rights, technology transfer and research and development for pandemic-related products. Also a topic for debate has been the inclusion of the concept of common but differentiated responsibilities (CBDR), meant to address equity concerns by asking richer countries to take on greater obligations to address common goals in pandemic preparedness and response than poorer countries.
What are possible outcomes of the agreement negotiations?
Earlier this year, it was expected there would be a vote on an agreement the 2024 WHA meeting, which occurred in May. However, given the lack of consensus on a number of issues in the agreement, member states decided they needed more time for negotiations and extended the INB’s mandate through May 2025. The next formal INB meeting is scheduled for July 2024, with additional negotiating meetings expected beyond that and into next year. There is an expectation that member states will vote on a final text of any agreement at the WHA in May 2025.
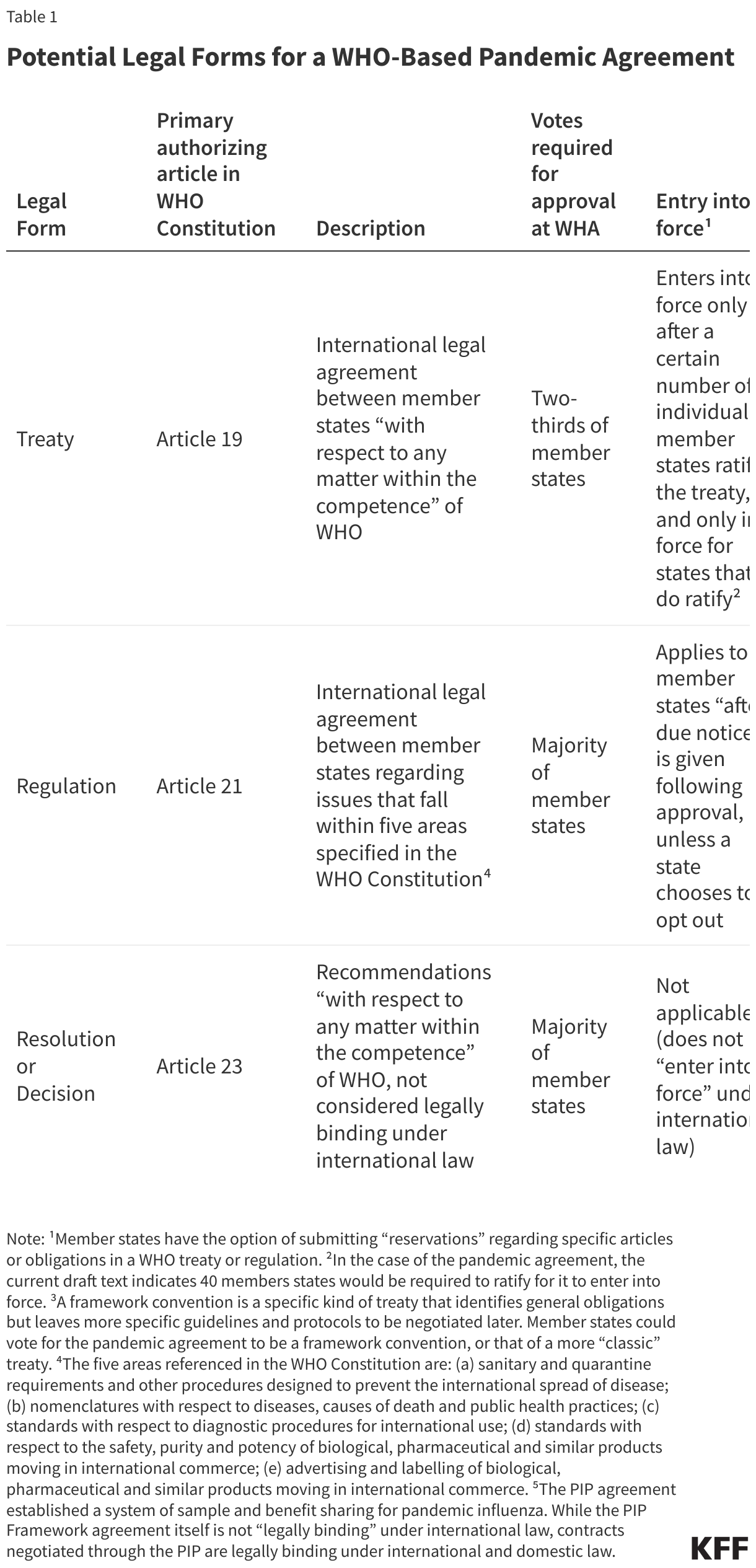
If member states vote in favor, the agreement would be adopted as one of several different types of international legal agreements allowed under the WHO Constitution. Which form it takes is the subject of ongoing negotiation at the INB, but possibilities include a “treaty”, a “regulation” or a “resolution”/”decision,” each of which has specific characteristics and implications (see Table 1).
- Treaty: Proponents of the agreement, and most member states, have supported a “treaty” as the preferred outcome as it is expected to have the greatest influence and broadest potential scope. Indeed, the latest draft of the agreement includes text that indicates adoption and ratification as a treaty (Article 34), but this could change. However, a treaty would have the highest bar to clear in terms of votes needed for approval, subsequent ratification by a minimum number of member states to enter into force, and only would apply to member states that do ratify the treaty.
- Regulation: If the agreement is approved as a “regulation,” in contrast, it would enter into force immediately for all member states (unless they opt-out), but this form could be seen as less influential compared to a treaty and could have some limitations on the issues it can directly address.
- Resolution or Decision: Finally, WHO member states could choose to approve an agreement as a “resolution” or “decision”, which would essentially be a statement of support for certain principles without specific legal or other obligations for member states and would therefore be seen as the weakest and least ambitious form of agreement.
What has been the U.S. engagement with and positions on the agreement so far?
The Biden Administration has been actively participating in the negotiations since the INB was formed in 2021. Co-led by the State Department and the Department of Health and Human Services, the U.S. representatives’ stated goals are to “ensure any agreement will leave all countries better prepared for pandemics, allow data and laboratory samples to be shared more quickly and transparently, and support more equitable global access to drugs, vaccines, and tests during health emergencies.” Earlier this year the U.S. supported completing negotiations and holding a vote on the agreement at this year’s WHA meeting but joined other member states in voting to extend the negotiations until next year given the lack of consensus on several issues in the text. However, Biden Administration officials have stated they are optimistic about reaching consensus eventually, and that the “contours of the agreement are in place”.
With closed-door negotiations still ongoing, information about U.S. positions on different components of the agreement is limited and may be subject to change. Statements from officials indicate U.S. support for the overall principles in the draft agreement, such as the aspirational goals for building pandemic preparedness capacities and calls for international cooperation. U.S. officials also have come out in favor of a some kind of PABS system where countries would commit to share pathogen samples and information, and manufacturers of vaccines, drugs and other pandemic-related products would “set aside a dedicated percentage of production for equitable distribution during pandemics." In contrast, U.S. representatives have made critical comments about the idea of requiring intellectual property rights on pandemic-related products to be waived on a temporary basis during a pandemic, saying “eliminating intellectual property protections will not effectively improve equitable access during pandemic emergencies, and will in fact harm the systems that have served us well in the past”. While U.S. officials have voiced support for voluntary technology transfer goals in the agreement, they have been critical of including language that requires mandatory technology transfer. At recent INB meetings, U.S. officials have voiced opposition to the common but differentiated responsibilities (CBDR) concept and argued against creating a new pooled funding mechanism for pandemic preparedness and response through the agreement.
What objections are being raised in the U.S. about the agreement, and is there evidence supporting these objections?
Some U.S. policymakers and observers have raised objections to the agreement in part or in full. Below are some of the commonly expressed objections, and available evidence regarding the objections:
- Concerns about U.S. sovereignty and/or ceding authority to WHO. Some Republican members of Congress have expressed concerns that an agreement would threaten U.S. sovereignty and could cede power to WHO. However, regardless of which type of instrument is ultimately adopted, an agreement would not change WHO’s power or member state sovereignty. WHO itself is not to be a party to an agreement, but rather its role is to provide a forum for the negotiations held by member states themselves. The current draft (Article 24) makes this point explicitly, saying the agreement “should not be interpreted” as providing WHO with any authority over domestic laws or policy. There is no mechanism included or possible for punishing member states for not meeting the goals of the agreement. Biden administration representatives involved in the negotiations have similarly stated that an agreement would not provide WHO with “...any authority to direct U.S. health policy or national health emergency response actions.” In addition, governments can choose not to be a party, opt out, or register reservations for any agreement. The U.S. government has regularly submitted reservations to other international agreements regarding federalism and its obligations, including to the WHO-based IHR revision approved in 2005.
- Concerns about financial burden on U.S. taxpayers and/or U.S. companies. Some Republican lawmakers have expressed concerns than an agreement would require U.S. contributions, placing a financial burden on U.S. taxpayers. In addition, some lawmakers and pharmaceutical industry groups have raised concerns that an agreement would require contributions from U.S. pharmaceutical companies involved in producing pandemic-related products (such as tests, treatments, and vaccines), placing an undue financial burden on those companies. At this time, there is no language in the draft agreement text requiring contributions from member states such as the U.S. However, the text does propose (Article 20) a “Coordinating Financial Mechanism” to support global pandemic preparedness efforts, which would include a “pooled fund” drawing from several sources including voluntary contributions from governments. It also includes language (Article 12) creating a system for pathogen access and benefit sharing (PABS), for which manufacturers of pandemic-related products such as pharmaceutical companies may be expected to pay annual contributions (amounts not specified) to support the PABS system and would be expected to provide WHO (or another mechanism for global sharing) a 10% share of their production of relevant diagnostics, therapeutics, or vaccines at no cost plus an additional share (10%) at reduced prices during pandemics. Current draft language (Article 12) also proposes that manufacturers can make further voluntary, non-monetary contributions “such as capacity-building activities, scientific and research collaborations, non-exclusive licensing agreements, arrangements for transfer of technology and know-how.”
- Concerns about intellectual property rights, and implications for U.S. pharmaceutical company innovation and development of pandemic-related products. S. lawmakers from both parties, along with pharmaceutical industry groups, have raised concerns that an agreement could “undermine” intellectual property (IP) rights and pharmaceutical innovation by requiring companies to “give away” IP protections on pandemic-related products they develop, thereby reducing incentives to invest in research and development of such products. At this time, the revised draft text of the agreement does not require companies to give up IP protections. One section (Article 11) recommends countries and companies consider supporting “time-bound waivers of intellectual property rights” in order to speed or scale up manufacturing of pandemic related products but the preamble of the current draft recognizes “protection of intellectual property rights is important for the development of new medical products,” while also recognizing concerns about IP on prices of those products.
- Concerns about transparency of U.S. positions on the agreement provisions and its adoption. Civil society groups and others have raised questions about the transparency of U.S. engagement with the agreement negotiations, and the lack of access to draft negotiating texts. While throughout the process an official draft negotiating text has been released on only a few occasions, this is in large part due to the multiple parallel closed-door negotiations that took place earlier focusing on different sections of the agreement, resulting in a lack of an “interpretable” text given the amount of edits being suggested by member states. In addition, policymakers and others have criticized the U.S. negotiators for not being transparent about whether they will seek ratification of the agreement through the U.S. Senate, allowing a role for Congress in its consideration, or seek to approve an agreement solely through Executive Agreement. While Senate ratification followed by Presidential signature is the formal process by which treaties are ratified under the U.S. Constitution, the U.S. President has the option of acceding to a treaty/agreement through executive action alone, without the advice and consent of the Senate.1 In fact, the great majority (estimated at over 90%) of all U.S. international legal agreements are approved via executive action rather than formal Senate approval.
A few other concerns have been raised about the agreement, for which there is little evidence. For example, some Republican members of Congress have raised a concern that the agreement would direct U.S. tax dollars to be used to fund abortion overseas. However, there is no evidence – in statements from participating governments, the WHO, or in the text of the draft itself – indicating funds associated with agreement are meant to or could be used in support of abortion, which in any case is not an activity linked to the pandemic preparedness capacity-building that is the subject of the agreement. Further, U.S. law and current policies have long prohibited U.S. foreign assistance from supporting abortion overseas. Another concern raised by some Republicans and other stakeholders is that China has undue influence at WHO and therefore the validity of any agreement negotiated under WHO is compromised. The origin of the agreement can be traced back as an initiative of primarily European member states rather than China, and China’s role has been that of one of many member states rather than a controlling force shaping negotiations.
Looking Ahead
While agreement has been reached on some articles of a draft pandemic agreement, there is also much that remains to be determined in terms of the specific wording and content and indeed whether an agreement will be reached at all. Member states remain engaged in rounds of negotiations and much could change between now and a final version of the agreement. The expectation is that the negotiations will conclude in 2025, and given that U.S. elections will be held in November 2024 there remains some uncertainty about the future of U.S. engagement. This is especially true if President Trump were to be elected, given his prior administration’s history of speaking out against WHO and moving to withdraw the U.S. from WHO membership, as well as his more general “America First” approach to international engagement. With Republican lawmakers and associated groups echoing those calls to withdraw U.S. support for WHO, U.S. engagement with and approval of any future agreement could be very different depending on the 2024 electoral results.
- For further information on the process and implications of U.S. international treaty adoption, see reports from KFF and Congressional Research Service. ↩︎