A Look at State Take-Up of ARPA Mobile Crisis Services in Medicaid
Rising concerns about mental health and substance use disorder have led to new policy initiatives and funding to improve access and quality of services to address the mental health crisis. Notably, a relatively new three-digit number to reach the 988 Suicide and Crisis Lifeline provides 24/7 access to crisis counselors for everyone, regardless of financial ability. In addition to 988, federal guidelines detail a comprehensive crisis continuum that contains three core components: crisis call centers, mobile crisis units and short-term crisis stabilization centers.
While crisis call centers are accessible nationwide, the availability and characteristics of other components of the crisis continuum–mobile crisis units and stabilization centers–vary across and within states, as does the financing of these systems. Medicaid is a larger payer of behavioral health services and enrollees are disproportionately affected by behavioral health conditions, which include mental health and substance use disorders. The American Rescue Plan Act (ARPA), passed in 2021, had several Medicaid-focused provisions to improve access to mobile crisis. This policy watch examines what mobile crisis is, what changes to mobile crisis were included in ARPA and how many states are implementing ARPA approved mobile crisis services.
What is mobile crisis?
Mobile crisis units provide in-person crisis stabilization services for people experiencing a mental health or substance use disorder crisis. These mobile crisis units–typically activated by crisis hotlines, providers, or first responders–provide community-based interventions in settings that feel comfortable to the individual, like their homes. For instance, in areas with a robust continuum of behavioral health crisis services, if an individual calls the 988 lifeline and their needs surpass what can be managed over the phone, the counselor on the line may dispatch a mobile crisis team directly to the caller’s location—similar to how 911 can dispatch an ambulance. Upon arrival, this team could deliver face-to-face crisis stabilization services to help address the mental health crisis. Per Substance Abuse and Mental Health Services Administration (SAMHSA) guidelines mobile crisis teams are made up of master’s level mental health clinicians and paraprofessionals (such as peer support workers) and are available 24/7. However, however, the actual composition and availability of teams may vary. These services may help to reduce unnecessary involvement by law enforcement, emergency room visits, and hospitalizations by providing in-person crisis intervention services and linkages to subsequent behavioral health care.
Many states offer some kind of mobile crisis service and most state Medicaid programs reimburse for mobile crisis services, but the characteristics, delivery, and accessibly of these services vary widely across states. Most states report the presence of mobile crisis services in their state, but only half of states have these services available statewide and even fewer states have these services available 24/7. In 2022, about three-quarters of Medicaid programs (33 in total) reported some coverage for mobile crisis services. However, it’s unclear how closely these services follow the guidelines provided in SAMHSA’s crisis guidelines.
What changes did ARPA include for Medicaid mobile crisis services?
ARPA included several provisions to improve and expand mobile crisis systems in Medicaid. The changes were intended to better align the delivery of mobile crisis with SAMHSA’s crisis guidelines and make these services more robust and uniform in Medicaid. ARPA included $15 million in state planning grants for qualifying mobile-crisis services, a higher federal match rate for qualifying mobile crisis services, and federal administrative matching funds for the development or implementation of technology to support crisis continuum–such as technology to help dispatch mobile crisis units.
Under ARPA, the federal government provides a temporary enhanced Medicaid match rate for qualifying community mobile crisis services. To be eligible for enhanced ARPA funding, the services need to meet specific standards–listed in ARPA legislation which are detailed in a letter to state health officials, and include requirements such as the following:
- Availability of services: These community-based teams must be available 24/7, every day of the year.
- Training requirements: All team members must be trained in trauma-informed care, de-escalation strategies, and harm reduction.
- Team composition: Mobile crisis teams should have at least one behavioral health professional and may also include a paraprofessional, such as a peer support specialist or nurse.
- Community linkages: Mobile crisis must have established linkages to community partners.
Medicaid programs can access the 85% enhanced federal match for ARPA mobile crisis services for eligible Medicaid enrollees between the period April, 1, 2022 to March 31, 2027, for up to 12 fiscal quarters. To access this funding, states must first gain approval by amending their state plan or through a waiver authority unless existing mobile crisis services meet ARPA standards. States must also detail their approach for reimbursement in their state plan and/or managed care contracts. Similar to other services, Medicaid reimbursement for benefits are tied to approved services for eligible enrollees. To the extent an individual needs mobile crisis and is uninsured, providers may work to help enroll that individual in Medicaid. If eligible, providers can file claims with retroactive coverage and individuals may be able to access additional follow-up care.
How many states have approval to implement ARPA community-based mobile crisis services?
As of November 2023, 13 states obtained CMS approval for state plans amendments to cover ARPA community-based mobile crisis intervention services, making them eligible for enhanced federal matching funds under the American Rescue Plan Act (ARPA) option (Figure 1). Twenty-five other states reported some coverage for mobile-crisis services in 2022, but it is unclear whether they meet standards for crisis services laid out in ARPA. More than half of all states in a 2022 survey reported plans to adopt the ARPA community-based mobile crisis services option so more states may be in the process of obtaining approvals for these services. Some states may also have ARPA qualifying mobile crisis approved through waivers not captured in count of state plan amendments.
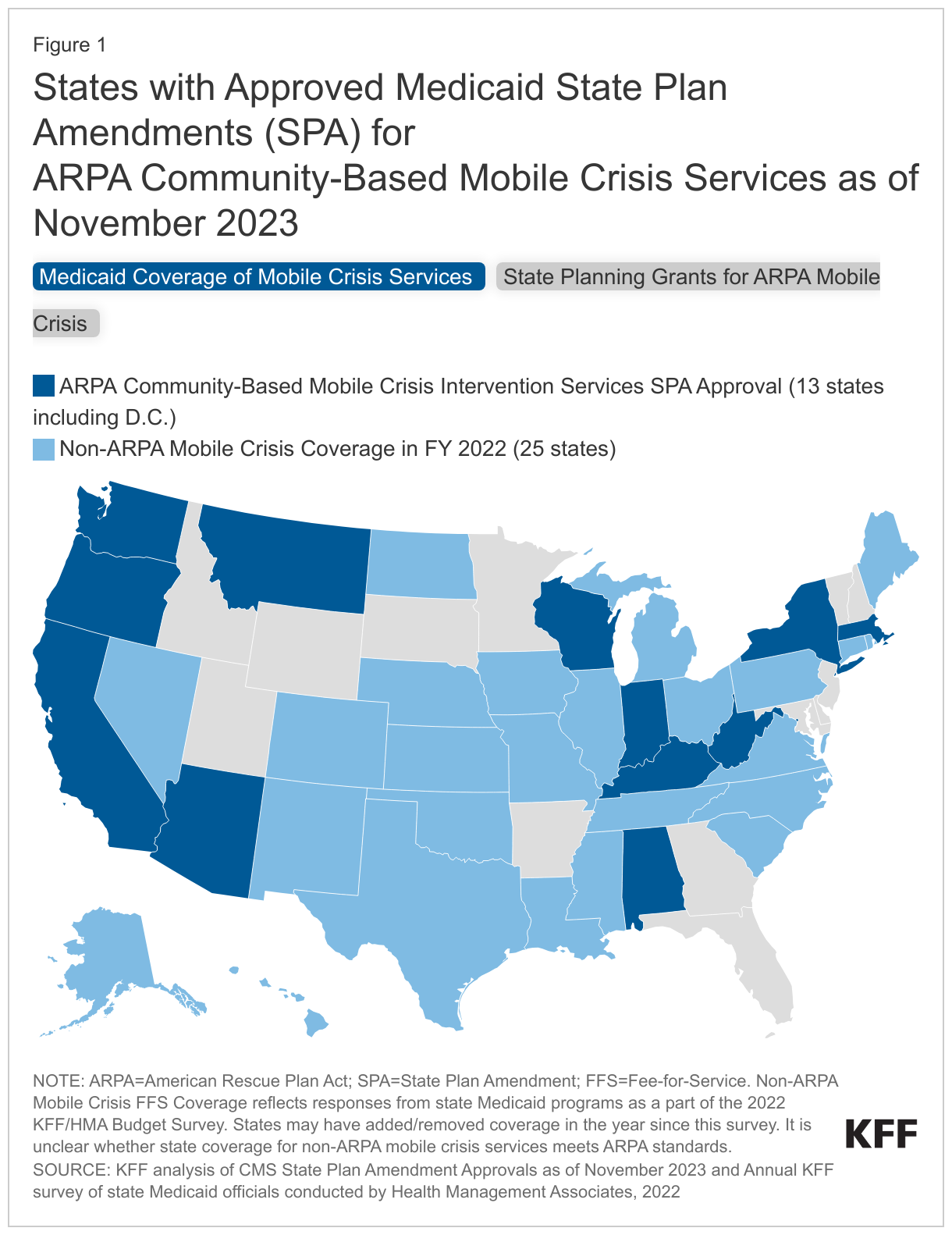
Twenty (20) states received state planning grants for ARPA community-based mobile crisis intervention services. Of these, eight received approvals for coverage of these services through state plan amendments. The other 12 states that were awarded planning grants have not yet received approval through state plan amendments, though they may have requests under review with CMS.
Looking ahead
Beyond the ARPA incentives, recent Department of Justice (DOJ) investigations into police handling of mental health calls could spur expansion of mobile crisis. Specifically, in March 2023 a DOJ investigation found that Louisville violated the Americans with Disabilities Act (ADA) by using police for mental health calls that posed no safety threat and could have been managed by a behavioral health response, such as a mobile crisis team. More recently, the DOJ reported similar violations of the ADA against people with behavioral health disabilities in the city of Minneapolis and other investigations are underway. More broadly, a continuum of crisis services can mitigate use of law enforcement, emergency departments, and sometimes jails in responses to mental health emergencies.
Despite developments and recent expansions, implementation challenges may pose barriers to expanding mobile crisis services. Medicaid officials reported workforce shortages as a primary obstacle in expanding mobile crisis services, which affect 24/7 staffing for mobile crises and timely care delivery in rural regions. Officials also pointed to gaps in provider training, lack of technological infrastructure needed to link crisis services, and lack of adequate and sustainable funding as other barriers facing mobile crisis expansions.
The introduction of the 988 Suicide and Crisis Lifeline, with its simple three-digit access prompted a 30% increase in contact volume its first year, highlighting the demand for straightforward, easily navigable, and affordable mental health services. Although 988 has facilitated easier contact with crisis counselors, the availability of follow-up services and other mental health services vary across states. This includes mobile crisis units and crisis stabilization centers, as well as a comprehensive outpatient system, which together would provide a fuller range of support than 988 can offer by itself.