The Impact of Gun Violence on Children and Adolescents
The United States experienced a sharp increase in firearm mortality among youth in recent years, with firearms becoming the leading cause of death for children and adolescents by 2020. Beyond firearm deaths, there are many more youth who survive gunshot wounds or are otherwise exposed to gun violence, which can lead to negative behavioral health outcomes. For example, increased youth suicide risk has been linked to communities exposed to school shootings. School shootings in the U.S. have increased in prevalence over time, as has exposure of school-aged children to these shootings, up from 19 per 100,000 school-aged children from 1999-2004 to 51 per 100,000 from 2020 to 2024.
The new Trump Administration has revoked multiple gun safety initiatives in the interest of preserving Second Amendment rights. These initiatives include dismantling the School Safety Committee, an Executive Order to review and revise firearm regulations by the Bureau of Alcohol, Tobacco, and Firearms that may infringe on Second Amendment rights, and the removal of the former Surgeon General’s advisory that identified gun violence as a public health crisis.
This brief explores the impacts of gun violence on children and adolescents (ages 17 and below) and current policies affecting gun accessibility and safety. Key findings include:
- Firearm death rates among children and adolescents increased 46% from 2019 to 2021, primarily driven by gun assaults. From 2021 to 2023, the firearm death rate has held steady at 3.5 per 100,000 children and adolescents. The increase in gun deaths during the pandemic is most pronounced among Black and Latino youth, among which gun assaults also account for the majority of firearm deaths.
- Nonfatal firearm injuries are two to four times more likely to occur than fatal ones, and Black youth are much more likely than their White peers to be injured by or exposed to a gun violence incident.
- Exposure to gun violence can have severe adverse effects on the mental health and well-being of children and adolescents, including increased likelihood of depression, PTSD, anxiety, and poor academic performance.
- The new Trump Administration has rolled back multiple Biden-era gun safety policies. Simultaneously, access to mental health and trauma support may be impacted by federal budget cuts and restructuring.
How have firearm deaths changed in recent years among children and adolescents?
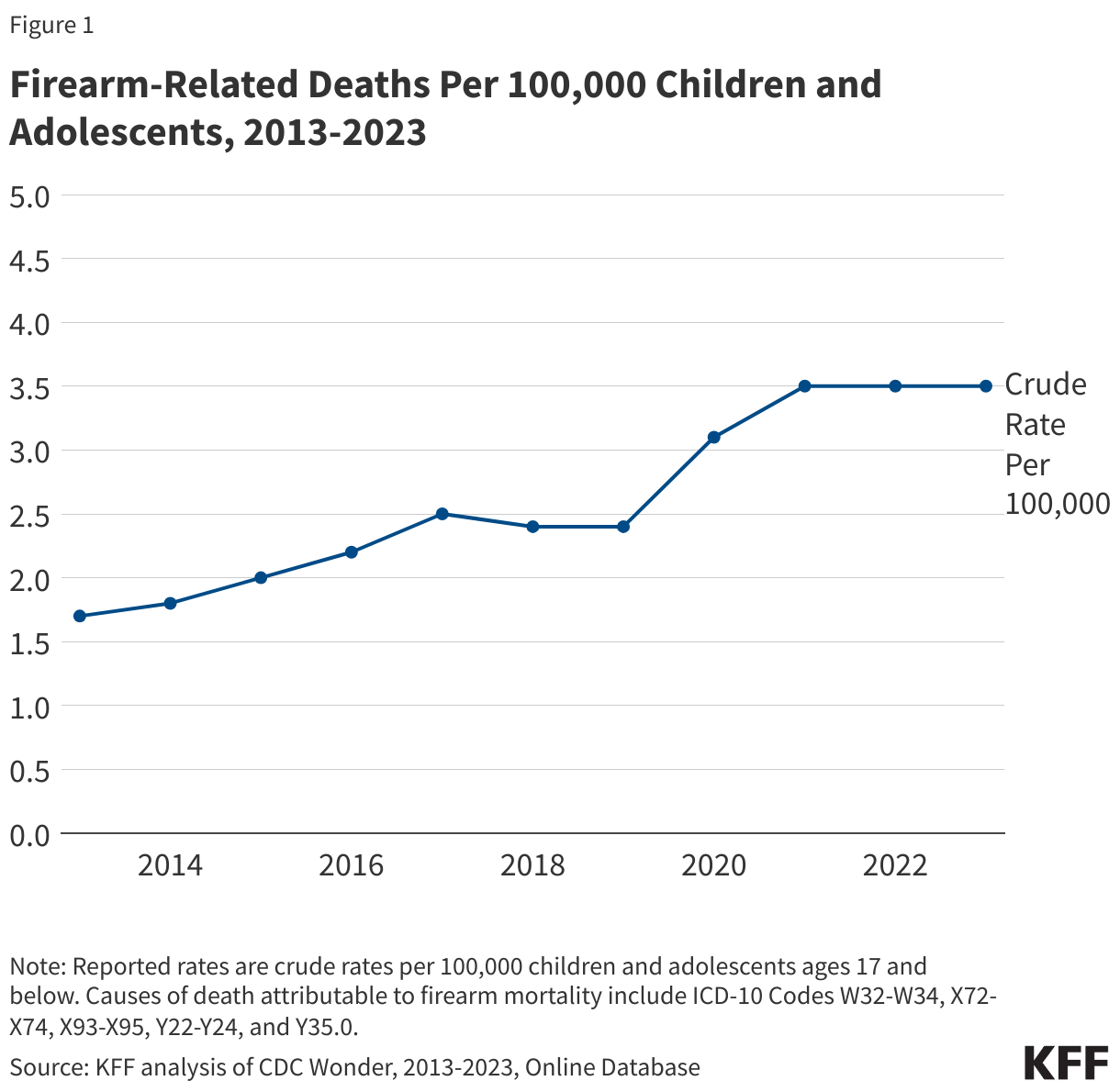
Firearm-related deaths have increased among children and adolescents since the pandemic began, with seven children per day dying by firearm in 2023. From 2013 to 2023, nearly 21,000 children ages 17 and younger died by firearm.1 During this period, firearm death rates gradually rose until 2017, then slowed through 2019, before sharply rising with the onset of the pandemic and holding steady in 2023 (Figure 1). From 2019 to 2023, the firearm death rate among children and adolescents increased by 46% (from 2.4 to 3.5 per 100,000). This translates to seven children per day dying by firearm in 2023.
Recent increases in firearm deaths were driven by gun assaults, which accounted for nearly two out of three firearm deaths among children and adolescents in 2023. Gun assault deaths among children and adolescents have increased over the past decade, resulting in 1,622 deaths in 2023 (Figure 2). Leading up to the pandemic, gun assaults made up about half of all child and adolescent firearm deaths. However, from 2019 to 2023, the share of these firearm deaths attributed to gun assaults grew from 54% to 63%.

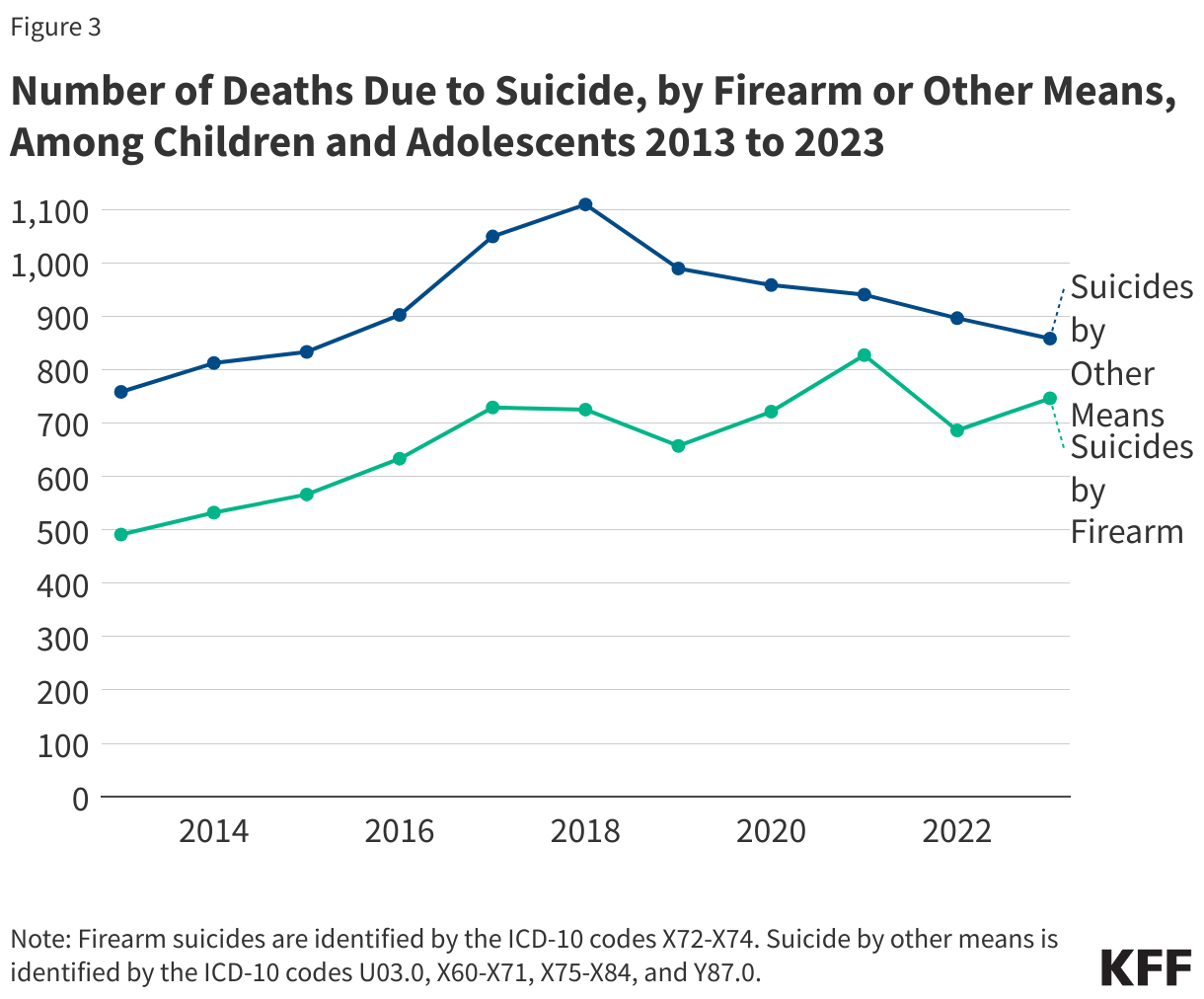
Among child and adolescent firearm deaths in 2023, 29% were suicides and 5% were accidental. Suicides by firearm have increased over the past decade among children and adolescents, peaking in 2021 with 827 deaths (Figure 3). Suicides by other means, however, have consistently declined since 2019. In 2023, firearms were involved in 47% of total suicide deaths among children and adolescents.
How do youth firearm deaths vary by demographic characteristics?
Firearm death rates have sharply increased among Black and Hispanic children and adolescents since the pandemic began. In 2023, the rate of firearm deaths among Black youth was 11.7 per 100,000 – substantially higher than any other racial and ethnic group and over four times higher than White youth (Figure 4). Additionally, from 2018 to 2023, the rate of firearm deaths nearly doubled among Black youth and increased by 73% among Hispanic youth. While firearm death rates for American Indian and Alaska Native (AIAN) youth fluctuated over the same period, they remained higher than the rates of their White, Hispanic, and Asian peers throughout the period. White youth experienced relatively stable and lower firearm mortality rates from 2018 to 2023, while Asian youth had the lowest firearm mortality rates across the period (Figure 4).

The recent increases in firearm deaths among Black and Hispanic children and adolescents were primarily driven by gun assaults. Since the onset of the pandemic, the gap in gun assault death rates between Black and White children and adolescents has significantly widened. The gun assault death rate among Black youth grew from 4.9 to 10.3 per 100,000 between 2018 and 2022, dropping slightly to 9.7 in 2023. Among White youth, it remained steady and below 1.0 per 100,000 (Figure 4). The gun assault death rate among Hispanic youth doubled 0.9 to 2.0 per 100,000 between 2018 and 2022 before dropping slightly to 1.8 per 100,000 in 2023.
In 2023, Black youth accounted for 46% of all youth firearm deaths although they made up only 14% of the U.S. youth population (Figure 5). From 2018 to 2023, the share of firearm deaths attributed to Black children and adolescents grew from 35% to 46%; and the share attributed to Hispanic children and adolescents grew from 16% to 19%.

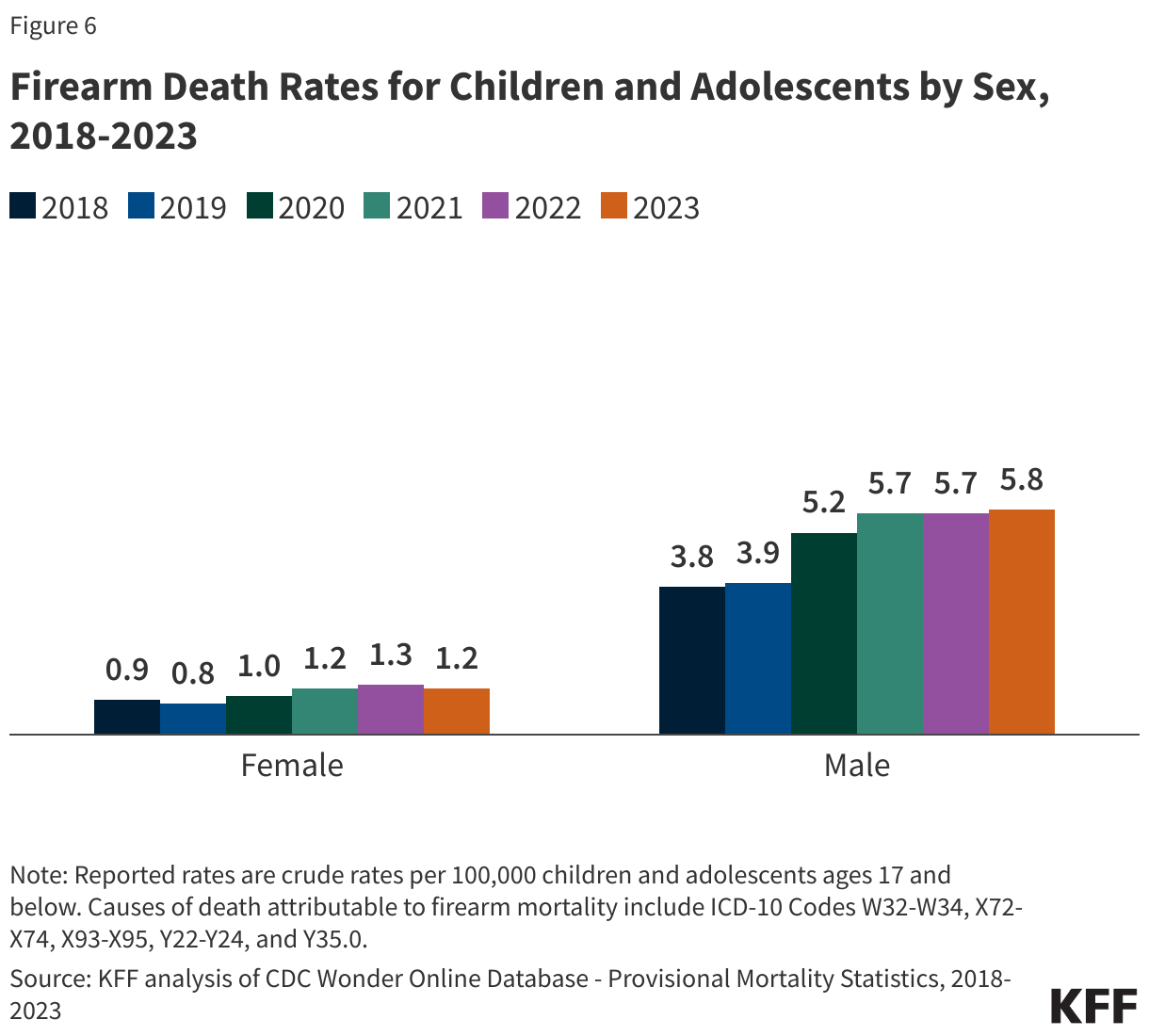
Firearm death rates for male children and adolescents are over four times higher than their female peers. From 2018 to 2023, the rate of deaths due to firearms increased by 53% among male children and adolescents but remained lower and stable among females (Figure 6).
Among firearm deaths, suicides by firearm are more common among adolescents compared to younger children, while accidental gun deaths are more common among younger children than adolescents (Figure 7). Gun assaults accounted for roughly two-thirds of firearm deaths among both adolescents and younger children in 2023. The second most common type of firearm death among adolescents was firearm suicides (32%), and among younger children was accidental gun deaths (21%).

Firearm death rates among children and adolescents vary considerably by state; however, almost all states have seen growth in these death rates in pandemic years. From 2020 to 2023 the states with the highest firearm death rates among children and adolescents were the District of Columbia, Mississippi, and Louisiana (10.3, 9.0, and 8.8 per 100,000 respectively for combined years, 2020-2023. The District of Columbia was also among the states with the highest school shooting exposure rates among school-aged children and adolescents in the 2020-2024 period (356 per 100,000, respectively). The states with the lowest firearm death rates were Massachusetts, New Jersey, and New York (0.7, 0.9, and 1.1 per 100,000 respectively for combined years, 2020-2023). Almost all states experienced an increase in firearm death rates from pre-pandemic to pandemic years, with the largest changes seen in Nebraska, Connecticut, and North Carolina (125%, 100%, and 100% respectively) (Figure 8).

What do we know about nonfatal firearm injury exposure among children and adolescents?
The number of nonfatal firearm injuries far exceeds the number of firearm fatalities among children and adolescents. However, estimates vary, with research suggesting nonfatal firearm injuries occur anywhere from two to four times more often than firearm fatalities. Recent data also indicate that since the pandemic began, nonfatal firearm injuries among children and adolescents have increased. The majority of youth nonfatal firearm injuries are a result of assaults.
Many children and adolescents are exposed to gun violence, even if they are not directly injured. Data on exposure to gun violence among youth is generally limited. However, a recent KFF analysis found that 51 per 100,000 U.S. school-age children were exposed to a school shooting from 2020-2024. Additionally, a CDC analysis found that in 34% of unintentional child and adolescent firearm deaths, at least one other child was present during the incident. Prior data from the National Survey of Children’s Exposure to Violence found that 8% of children and adolescents were exposed to a shooting in their lifetime, with a higher share (13%) reported among adolescents (ages 14-17). Further, in a recent KFF poll, 17% of adults in the U.S. reported witnessing someone being injured by a gun.
Black children and adolescents are more likely to experience firearm injuries and exposures than their White peers.Leading up to the pandemic, Black and male children and adolescents were more likely to experience nonfatal firearm injuries than their peers. This disparity among Black youth firearm injuries and exposures has been exacerbated since the pandemic began. In general, children of color are more often exposed to gun violence than their White peers. Children living in areas with a high concentration of poverty are more likely to experience firearm-related deaths, and poverty disproportionately affects children of color.
How does gun violence affect the mental health and well-being of children and adolescents?
Gun violence can adversely affect the mental health and well-being of children and adolescents. Exposure to gun violence is linked to post-traumatic stress disorder and anxiety, in addition to other mental health concerns among youth. Gun violence may also lead to challenges with school performance, including increased absenteeism and difficulty concentrating. In response to indirect gun violence, such as witnessing a shooting or hearing gunshots, many children and adolescents report feeling sad, anxious, or fearful. Children and adolescents are exposed to gun violence in multiple ways, outlined below.
- Neighborhood and community violence. Many children and adolescents experience violence within their communities. Firearm homicides occurring within an adolescent’s community have been linked to anxiety and depression among adolescents, particularly for females. Other analyses have similarly found an association between incidents of neighborhood firearm homicides and poor mental health outcomes among youth.
- Suicide. Suicides are the second leading cause of death among adolescents and many suicides involve a firearm. Research has found that access to firearms, particularly in the home, is a risk factor for suicide deaths among children and adolescents. Nearly half of suicide attempts occur within 10 minutes of the current suicide thought, further underscoring access to firearms as a risk factor for suicide.
- Domestic or intimate partner violence. Women and children are often the victims of intimate partner violence, which may involve firearms. The presence of a firearm in the home is linked to the escalation of intimate partner violence to homicides. Even when firearms are not used, they may serve as a means of threatening and intimidating victims of domestic violence.
- Mass shootings.Although mass shootings, including school shootings, account for a small portion of firearm-related deaths, they can negatively impact the mental health of children and communities at large. Research has found that youth antidepressant use and suicide risk increased in communities with exposures to school shootings. Additionally, a survey prior to the pandemic found that the majority of teenagers and their parents felt at least somewhat worried that a school shooting may occur at their school. School shootings are on the rise, with the U.S. average yearly rate of student exposure to a school shooting increasing threefold over time (from 19 per 100,000 students in 1999-2004 to 51 in 2020-2024). In response to school shootings, nearly all schools practice active shooter drills, which may have a negative psychological impact on participants. Although research is limited on how mass shootings affect individuals not directly exposed to them, current literature suggests that information and knowledge of mass shootings may be linked to increased levels of fear and anxiety.
Youth survivors of firearm injuries are at increased risk of mental health and substance use issues, in addition to chronic physical health conditions. An analysis of commercially insured children and adolescents found that, in the year following a firearm injury, survivors were significantly more likely to experience psychiatric and substance use disorders compared to their peers. Additionally, the increases in psychiatric disorders were more pronounced among youth with more severe firearm injuries compared to youth with less severe firearm injuries. Youth gunshot survivors are more likely to utilize mental health services following their injury compared to their uninjured peers. However, a study of youth survivors enrolled in Medicaid found that more than three out of five survivors had not received mental health services within the first six months following their injury.
Negative mental health impacts can extend to the family members of youth gun violence victims.Parents, particularly mothers, of youth firearm-injury survivors had an increase in psychiatric disorders and mental health visits in the year following the firearm incident, based on an analysis of commercially insured individuals. These increases in psychiatric disorders and mental health visits were more pronounced among families of youth firearm fatalities.
Gun violence disproportionately impacts Black children and adolescents, leaving them more vulnerable to negative mental health outcomes. In addition to increased assaults, firearm suicides, and exposure to community violence, Black communities are disproportionately exposed to police shootings. Research found that Black people living near the scene of a police killing of an unarmed Black individual experienced worsened mental health in the months that followed. Separately, despite mental health concerns among Black youth injured by gun violence, research on mental health service utilization in the months following a firearm injury is mixed, with one study finding higher utilization among Black youth compared to their White peers, and another study finding the reverse. Historically, Black individuals are less likely to receive mental health treatment and face additional barriers to care, such as the lack of culturally competent care.
What policies address child and adolescent exposure to gun violence and poor mental health?
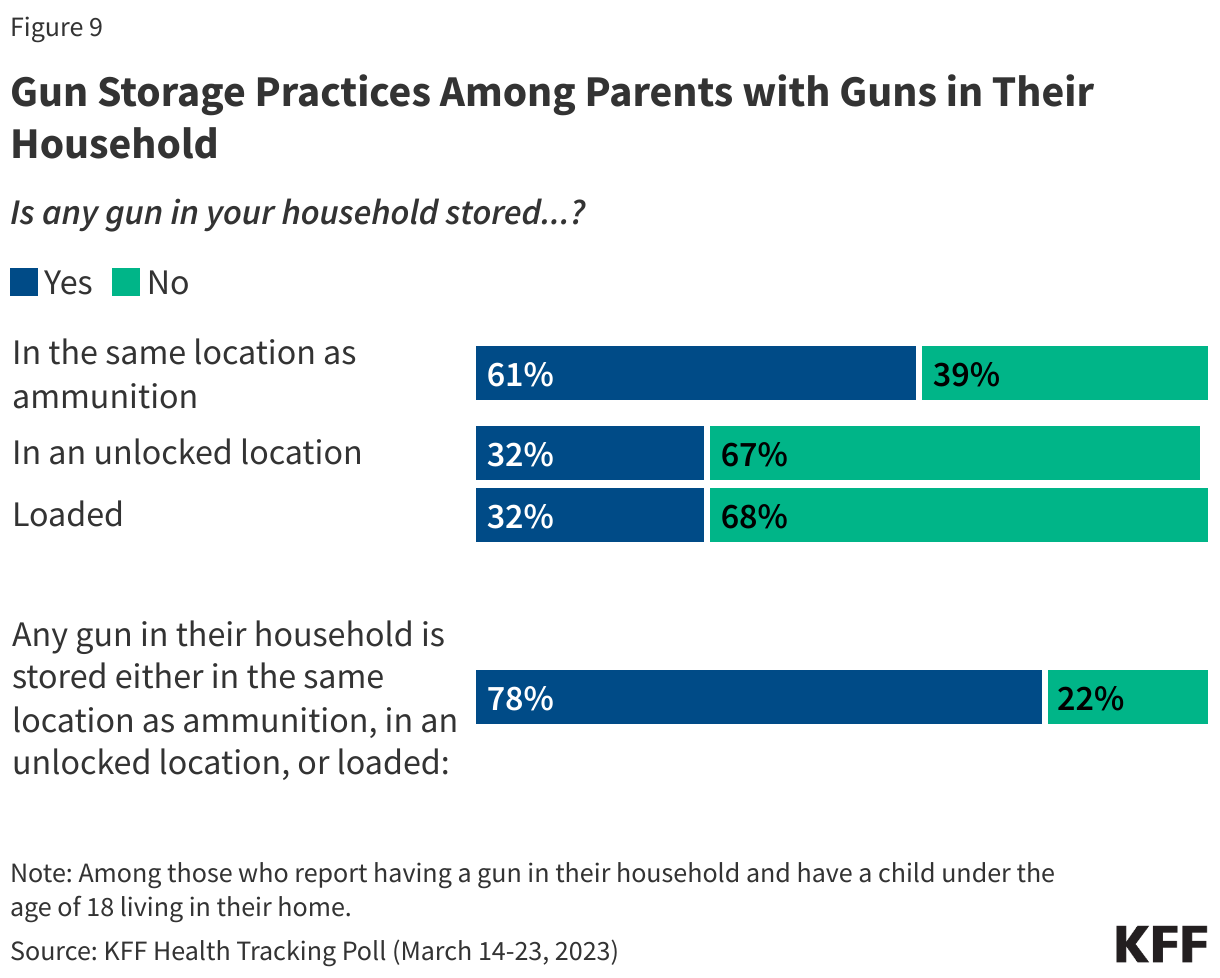
Gun control debates are deeply divided politically in the U.S.; but beyond gun control, other approaches seek to reduce the impact of firearms on health, for example, through safe storage practices.Safe storage and child access prevention provisions have been linked to a reduction in adolescent firearm homicides and non-fatal gun injuries. These provisions vary widely across states; some states have multiple provisions, while others have none. Some states have also enacted unique approaches to promote gun safety. For example, beginning with the 2023-2024 school year, local education agencies in California are required to notify parents annually on the safe storage of firearms; and some states provide tax rebates on safe storage devices. The Biden-Harris administration put forth additional steps to promote safe storage of firearms, including guidance from the U.S. Department of Justice, which was taken offline during the current Trump Administration. A KFF poll found that 44% of parents with children under the age of 18 have a gun in their household. Among parents with guns in their home, about one-third said a gun is stored loaded (32%) or stored in an unlocked location (32%) (Figure 9). More than half of parents (61%) said any gun in their home is stored in the same location as ammunition. The KFF poll also found that only 8% of parents said their child’s pediatrician talked to them about gun safety.
The Trump Administration is rolling back some Biden-era policies aimed at addressing gun reform and expanding youth mental health services for children and adolescents. During the Biden Administration, the Bipartisan Safer Communities Act (BSCA) was passed in response to increasing gun violence. The BSCA outlined provisions on gun reform and improving access to youth mental health services, including through schools. However, in May 2025, the Trump administration canceled $1 billion in BSCA grant funding for school-based mental health services. Gun safety groups fear that President Trump will attempt to further weaken or eliminate the BSCA. Additionally, other measures that may address youth mental health and gun violence trauma, including the rollout of 988, may also be in jeopardy. Under the Trump Administration, the Department of Government Efficiency (DOGE) laid off about a quarter of the 988 Hotline’s digital communications team. New federal funding freezes have also been put in place on prevention work by federal authorities to stop terrorism and mass shootings.
Gun violence disproportionately affects many children and adolescents of color, particularly Black children and adolescents, and this disparity has grown since the pandemic. Children and adolescents of color may also face added barriers to mental health care in light of long-standing cultural inequities and a lack of culturally informed care. In years prior, mental health initiatives aimed at Black and Latino people were introduced in Congress and SAMHSA announced funding opportunities to create a Behavioral Health Center of Excellence aimed at improving behavioral health equity for Hispanic and Latino communities. SAMHSA’s funding, however, has been cut by the Trump Administration by approximately $11.4 Billion, preventing the entity from using money that was previously earmarked for mental health and substance use disorder resources.
Gun violence can lead to increased mental health and substance use concerns. The recent increase in child and adolescent firearm injuries and deaths come at a time when concerns about youth mental health have grown but access to and utilization of mental health care may have worsened.
- KFF analysis of youth firearm mortality is based on data from Center for Disease Control and Prevention (CDC) Wonder injury and mortality database. In this analysis, firearm-related deaths are defined as gun assault deaths, suicide deaths by firearm, deaths due to accidental firearm discharge, legal intervention leading to firearm death, and firearm deaths from an undetermined cause. ↩︎