Women’s Health Insurance Coverage
Introduction
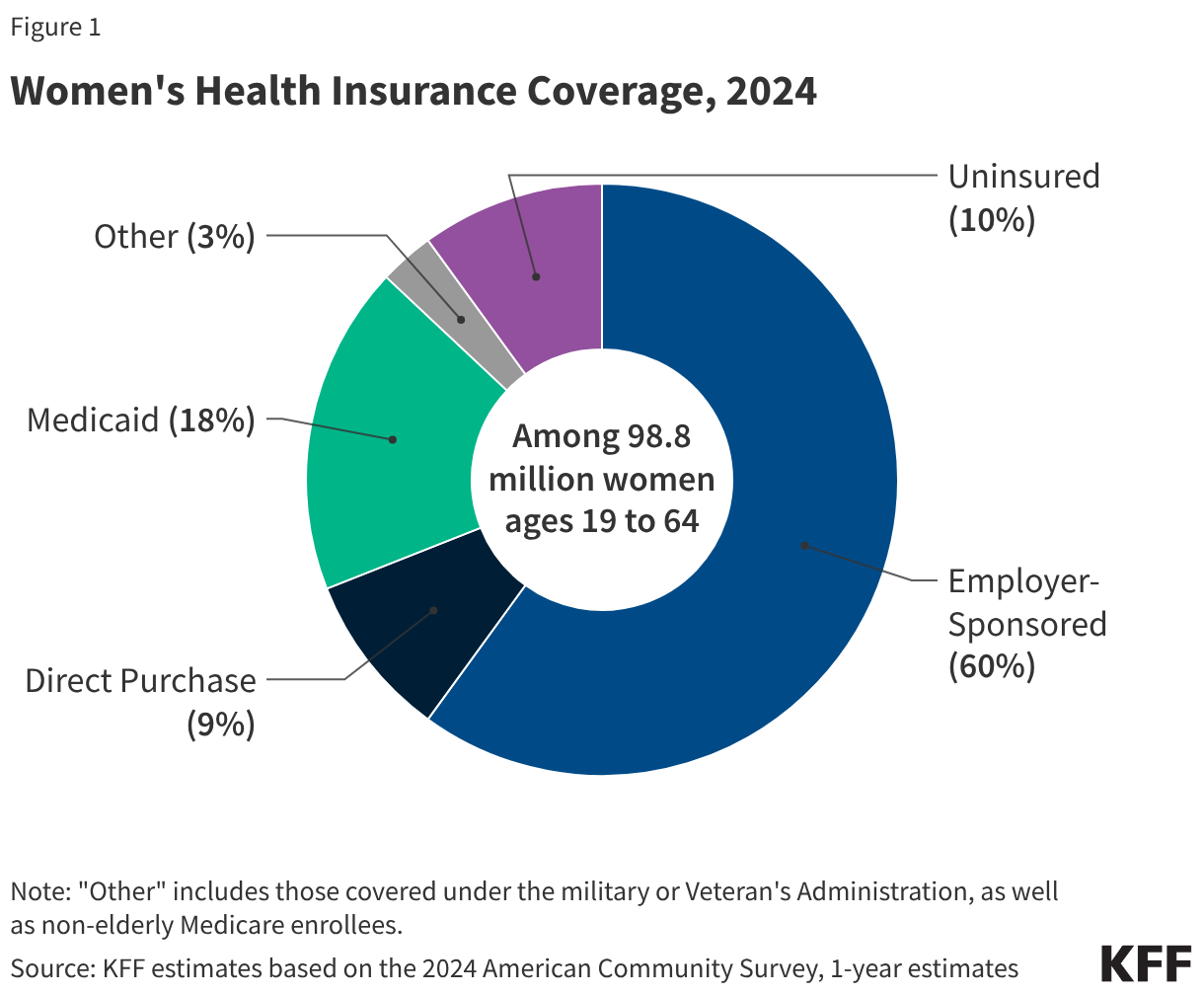
Health insurance coverage is an important factor in making health care affordable and accessible to women.1 Women with health coverage are more likely to obtain needed preventive, primary, and specialty care services, and have better access to new advances in women’s health. Among the 98.8 million women ages 19 to 64 residing in the U.S., most (90%) had some form of coverage in 2024. Over the past decade, the Affordable Care Act (ACA) has expanded access to affordable coverage through a combination of Medicaid expansions, private insurance reforms, and premium tax credits. However, while the uninsured rate has declined significantly in the past decade, gaps in private sector coverage, enrollment and eligibility barriers in publicly-funded programs, and persistent affordability challenges have left one in ten women uninsured. In addition, recent federal policy changes in Medicaid and the expiration of the ACA enhanced premium tax credits are expected to lead to a significant increase in the number of uninsured over the next several years. This factsheet reviews major sources of coverage for women residing in the U.S. in 2024, discusses the impact of the ACA on women’s coverage, and the coverage challenges that many women continue to face.
Sources of Health Insurance Coverage
Employer-Sponsored Insurance
Approximately 59.7 million women ages 19-64 (60%) received their health coverage from employer-sponsored insurance in 2024 (Figure 1).2
- Women in families with at least one full-time worker are more likely to have job-based coverage (70%) than women in families with only part time workers (33%) or without any workers (16%).3
- In 2024, annual insurance premiums for employer sponsored insurance averaged $8,951 for individuals and $25,572 for families. Family premiums have increased 24% between 2019 and 2024. On average, workers paid 16% of premiums for individual coverage ($1,368) and 25% for family coverage ($6,296) with the employers picking up the balance.
Non-Group Insurance
The ACA expanded access to the non-group or individually purchased insurance market by offering premium tax credits to help individuals afford coverage purchased through state-based health insurance Marketplaces. It also included many insurance reforms to alleviate some of the long-standing barriers to coverage (such as gender rating, lack of maternity coverage, and pre-existing condition exclusions, having a disproportionate effect on women) that were common in the non-group insurance market prior to the ACA. In 2024, about 9% of women ages 19 to 64 (approximately 8.9 million women) and 9% of their male counterparts purchased insurance in the non-group market.4 This includes individuals who purchased private policies from the ACA Marketplace in their state, as well as those who purchased coverage from private insurers that operate outside of Marketplaces under similar rules.
- Most individuals who seek insurance policies in their state’s Marketplace qualify for assistance with the costs of coverage. Individuals with incomes below 400% of the Federal Poverty Level (FPL) ($65,280 for an individual under 65 in 2024) can qualify for assistance in the form of federal tax credits which lower premium costs.
- Enhanced federal subsidies that began as part of two COVID era bills that temporarily increased the amount of financial assistance already eligible marketplace enrollees received as well as extended Marketplace subsidies to people with incomes above 400% FPL expired and were not renewed by Congress. As a result, out-of-pocket premium payments for Marketplace enrollees have risen 58% on average, making health coverage unaffordable for some individuals. A KFF survey shows that nearly one in ten (9%) of 2025 Marketplace enrollees has become uninsured.
- The ACA set new standards for all individually purchased plans, including plans available through the Marketplace as well as those that existed prior to the ACA. The ACA bars plans from charging women higher premiums than men for the same level of coverage (gender rating) or from disqualifying women from coverage because they had certain pre-existing medical conditions, including pregnancy. All direct purchase plans must also cover certain “essential health benefits” (EHBs) that fall under 10 different categories, including maternity and newborn care, mental health, and preventive care.
Medicaid
The state-federal program for individuals with low-incomes, Medicaid, covered 18% of adult women ages 19 to 64 in 2024, compared to 14% of men. Historically, to qualify for Medicaid, women had to have very low incomes and be in one of Medicaid’s eligibility categories: pregnant, mothers of children 18 and younger, a person with a disability, or over 65. Women who didn’t fall into these categories typically were not eligible regardless of how poor they were. The ACA allowed states to broaden Medicaid eligibility to most individuals with incomes less than 138% of the FPL regardless of their family or disability status, effective January 2014. As of March 2026, 40 states and DC have expanded their Medicaid programs under the ACA.
- Medicaid covers the poorest population of women. Forty-three percent of women with lower incomes (below 200% FPL) and 51% of women living below the federal poverty level (100% FPL) have Medicaid coverage.5
- By federal law, all states must provide Medicaid coverage to pregnant women with incomes up to 133% of the federal poverty level (FPL) through 60 days postpartum. However, in recent years, there has been a growing interest in expanding the length of the postpartum coverage period, and to date, all but one state has opted to take steps to extend postpartum Medicaid coverage to 12 months.
- H.R. 1, the 2025 budget reconciliation law, made significant changes to the Medicaid program. For the first time, Medicaid eligibility for adults in the ACA Medicaid expansion group will be conditioned on meeting work requirements starting January 1, 2027. KFF research shows that most adult women covered by Medicaid meet work requirements or would qualify for one of the law’s exemptions, but many would be at risk of losing coverage because of the administrative burdens related to reporting requirements. The Congressional Budget Office (CBO) estimates that these requirements will reduce federal Medicaid spending by $326 billion over the next 10 years but will also increase the number of uninsured by 5.3 million in 2034.
- Medicaid financed 40% of births in the U.S. in 2024, is a major source of publicly-funded family planning services, and accounts for over half (61%) of all long-term care spending, which is critical for many frail elderly women.
- Under federal law Medicaid coverage of abortion is very limited. The federal Hyde Amendment prohibits federal spending on abortions, except when the pregnancy is a result of rape or incest, or when it jeopardizes the life of the pregnant person. Among the 37 states and DC where the provision of abortion is legal, 17 states and DC follow the Hyde restrictions, while the other 20 states use their own unmatched funds to pay for abortions for Medicaid enrollees who seek abortion in other circumstances.
Uninsured
On average, women have lower incomes and have been more likely than men to meet Medicaid’s traditional eligibility categories; pregnant, parent of children under 18, disabled, or over 65. As a result, women are more likely than men to qualify for Medicaid and less likely to be uninsured. In 2024, 13% of men ages 19-64 were uninsured compared to 10% of women in the same age bracket (9.8 million women).
Uninsured women often have inadequate access to care, get a lower standard of care when they are in the health system, and have poorer health outcomes. Compared to women with insurance, uninsured women have lower use of important preventive services such as mammograms, Pap tests, and timely blood pressure checks. They are also less likely to report having a regular doctor.
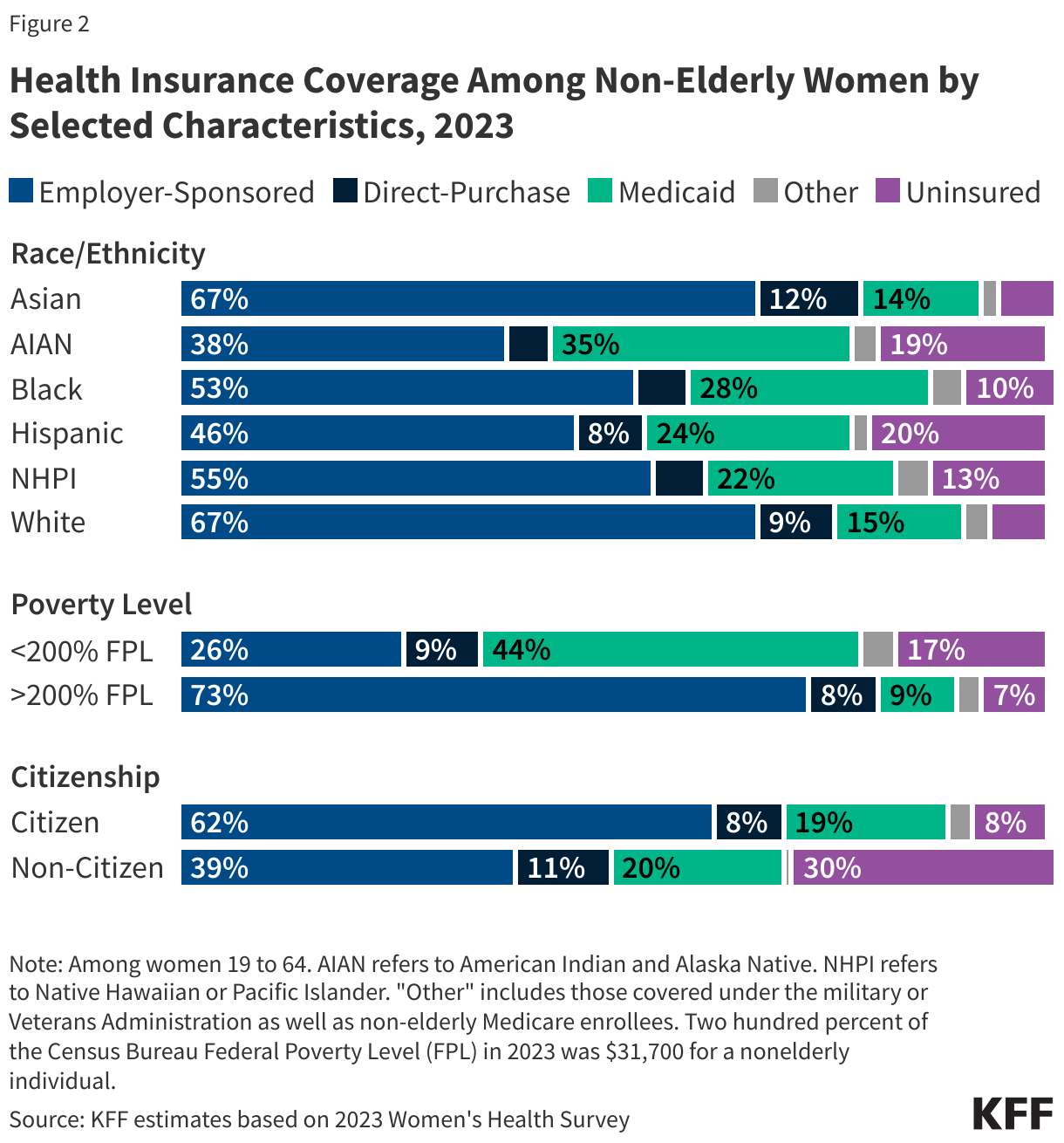
- Women with lower incomes, women of color, and women who are non-citizens are at greater risk of being uninsured (Figure 2). One in five (18%) women with incomes under 200% of the FPL ($32,640 for an individual in 2024) are uninsured (Appendix Table 2), compared to 7% of women with incomes at or above 200% FPL. One in five Hispanic (20%) and American Indian and Alaska Native (19%) women are uninsured. A higher share of women in single parent households are uninsured (11%) than women in two-parent households (7%) (data not shown).6
- The majority of women who are uninsured live in a household where someone is working: 69% are in families with at least one adult working full-time and 83% are in families with at least one part-time or full-time worker.7
- There is considerable state-level variation in uninsured rates across the nation, ranging from 20% of women in Texas to 3% of women in Massachusetts (Figure 3). Of the 18 states with uninsured rates above the national average (10%), nine have not adopted the ACA Medicaid expansion.
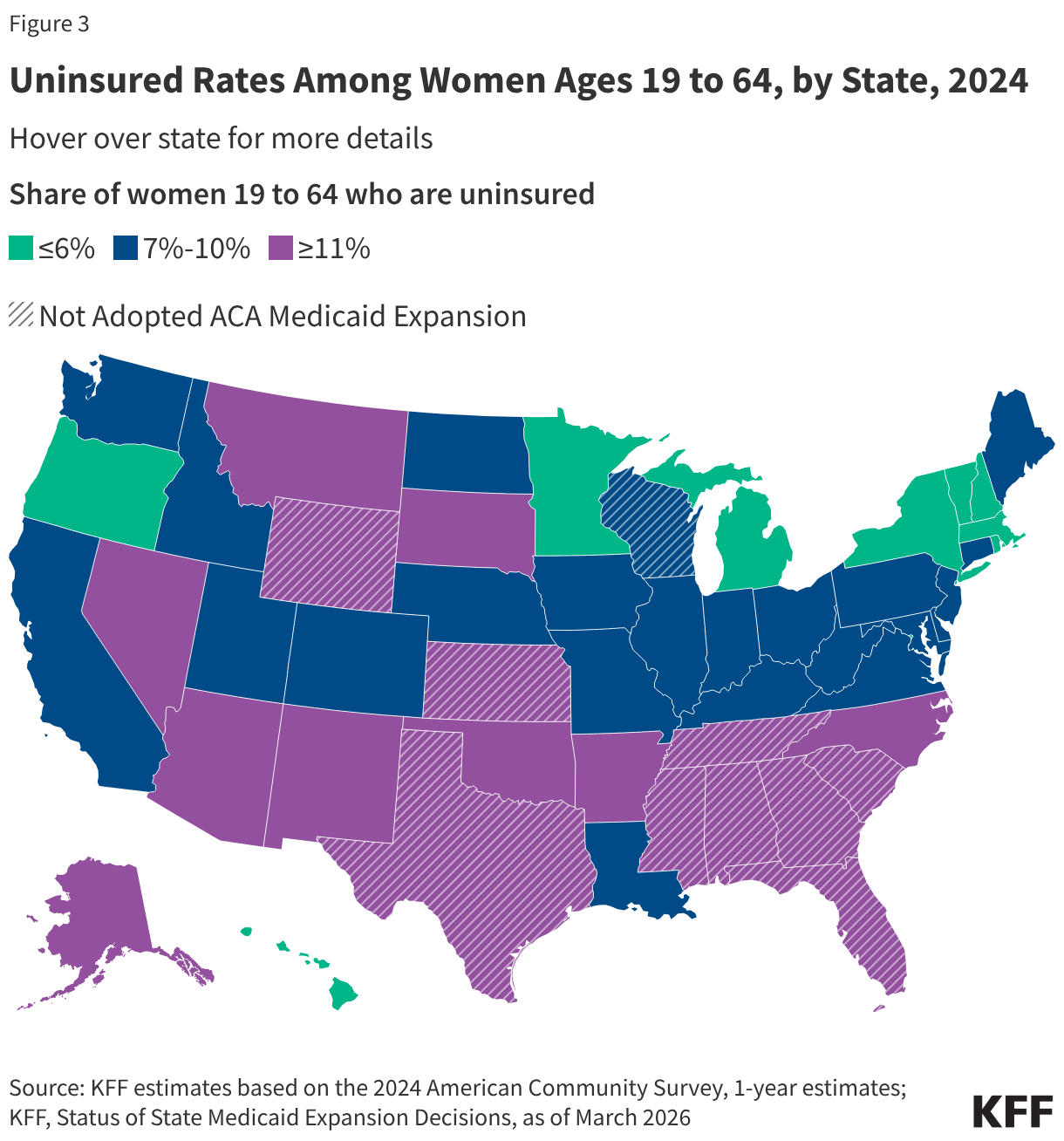
- In states that have not adopted the ACA Medicaid expansion, approximately 667,900 women with household incomes below the federal poverty level and are uninsured fall into a “coverage gap” because they earn too much to qualify for Medicaid but not enough to qualify for Marketplace premium tax credits. Other uninsured women are not eligible for any assistance with health coverage due to their immigration status, their income, or because they have an offer of coverage from an employer even if can’t afford the premiums.
- Between the changes to Medicaid made by H.R. 1 and the expiration of the enhanced ACA tax credits, CBO estimates that the number of uninsured people will increase by more than 14 million by 2034.
Scope of Coverage and Affordability
The ACA set national standards for the scope of benefits offered in private plans. In addition to the broad categories of essential health benefits (EHBs) offered by marketplace plans, all privately purchased plans must cover maternity care, which had been historically excluded from most individually purchased plans prior to the ACA. In addition, most private plans must cover preventive services without co-payments or other cost sharing. This includes screenings for breast and cervical cancers, well woman visits (including prenatal visits), prescribed contraceptives, breastfeeding supplies and supports such as breast pumps, and several STI services. Twenty-five states have laws banning coverage of most abortions from the plans available through the state Marketplaces. These restrictions were in place prior to the Supreme Court’s 2022 decision to overturn Roe v Wade.
Affordability of coverage continues to be a significant concern for many women, both for those who are uninsured as well as those with coverage. The leading reason why uninsured adults report that they haven’t obtained coverage is that it is too expensive. Under employer-sponsored insurance, the major source of coverage for women, 65% of all covered workers with a general annual deductible have deductibles of $1,000 of more for single coverage. With the impending growth in the uninsured due to the expiration of the enhanced subsidies in the Individual market and the implementation of major changes to Medicaid from H.R. 1, health care affordability will grow as a major national problem for increasing numbers of women.
Appendix Tables
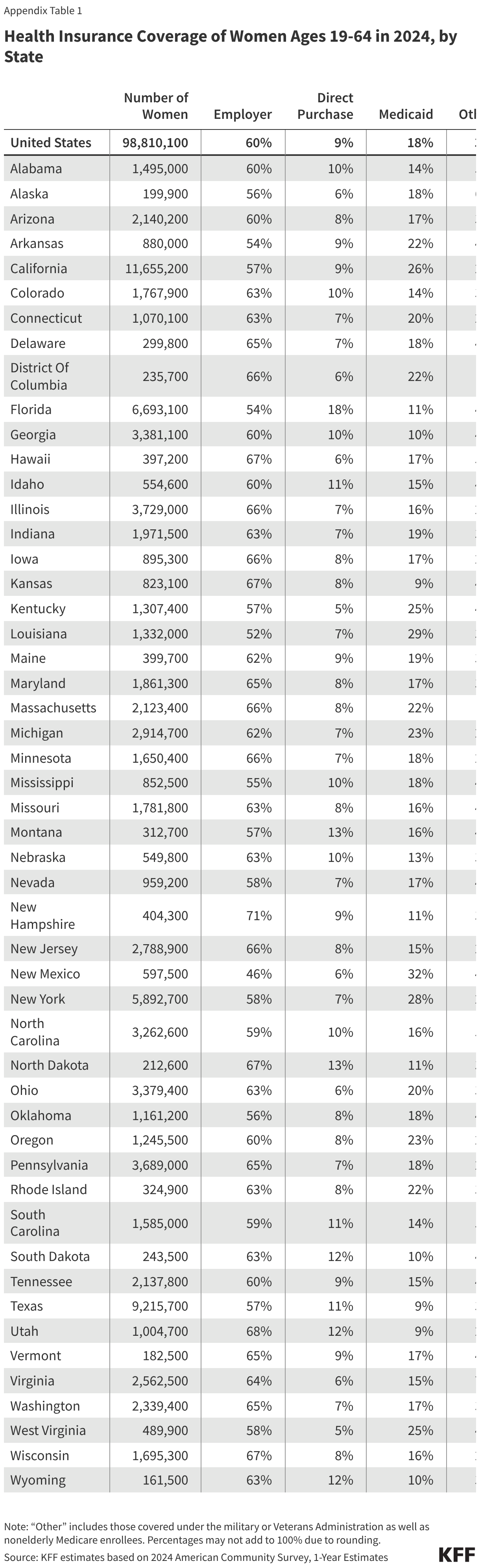
Health Insurance Coverage of Women Ages 19 to 64 in 2024, by State
Health Insurance Coverage Women Ages 19 to 64 with Lower Incomes in 2024, by State

Health Insurance Coverage of Reproductive Age Adult Women Ages 19-49 in 2024, by State

Endnotes
- This factsheet is based on KFF analysis of data from the American Community Survey (ACS), which stratifies data by an individual's sex as male or female. Throughout this brief we refer to “women” but recognize that not all people who are born as females identify as "women." ↩︎
- KFF estimates based on 2024 American Community Survey, 1-Year Estimates. ↩︎
- Ibid. ↩︎
- Ibid. ↩︎
- Ibid. ↩︎
- KFF estimates based on 2024 American Community Survey, 1-Year Estimates. ↩︎
- Ibid. ↩︎