What Does the Recent Literature Say About Medicaid Expansion?: Economic Impacts on Providers
Issue Brief
A substantial body of research has investigated effects of the Affordable Care Act (ACA) Medicaid expansion, adopted by all but 11 states as of January 2023. Prior KFF reports published in 2020 and 2021 reviewed more than 600 studies and concluded that expansion is linked to gains in coverage, improvement in access and health, and economic benefits for states and providers; these generally positive findings persist even as more recent research considers increasingly complex and specific outcomes. This research provides context for ongoing debates about whether to expand Medicaid in states that have not done so already, where coverage options for many low-income adults are limited. In non-expansion states, over two million individuals fall into a coverage gap. Prior efforts at the federal level to temporarily close the coverage gap were unsuccessful in 2021 and 2022, and Republican control of the House of Representatives following the November 2022 midterm elections makes it highly unlikely that Congress will do so in the near future. So, attention once again turns back to non-expansion states, where many officials cite economic concerns about adopting Medicaid expansion.
While states have to cover 10% of the cost of expanding Medicaid, the federal government covers the remaining 90%, providing an infusion of federal funds to expansion states. By financing coverage for low-income people who are likely to otherwise be uninsured, Medicaid expansion provides potential economic benefits to the health care providers who provide care to that population.
This issue brief updates prior KFF literature reviews by summarizing 24 studies published between April 2021 and December 2022 on the economic impact of Medicaid expansion on providers. These studies identify positive effects of Medicaid expansion on the finances of hospitals and other providers, in line with prior research. These findings are particularly relevant given fiscal stress experienced by Medicaid providers during the coronavirus pandemic. While federal relief funds helped prop up hospital margins in the first two years of the pandemic, hospitals began facing increased challenges in 2022 due to ongoing pandemic effects, decreases in government relief, and broader economic trends such as pressure on wages.
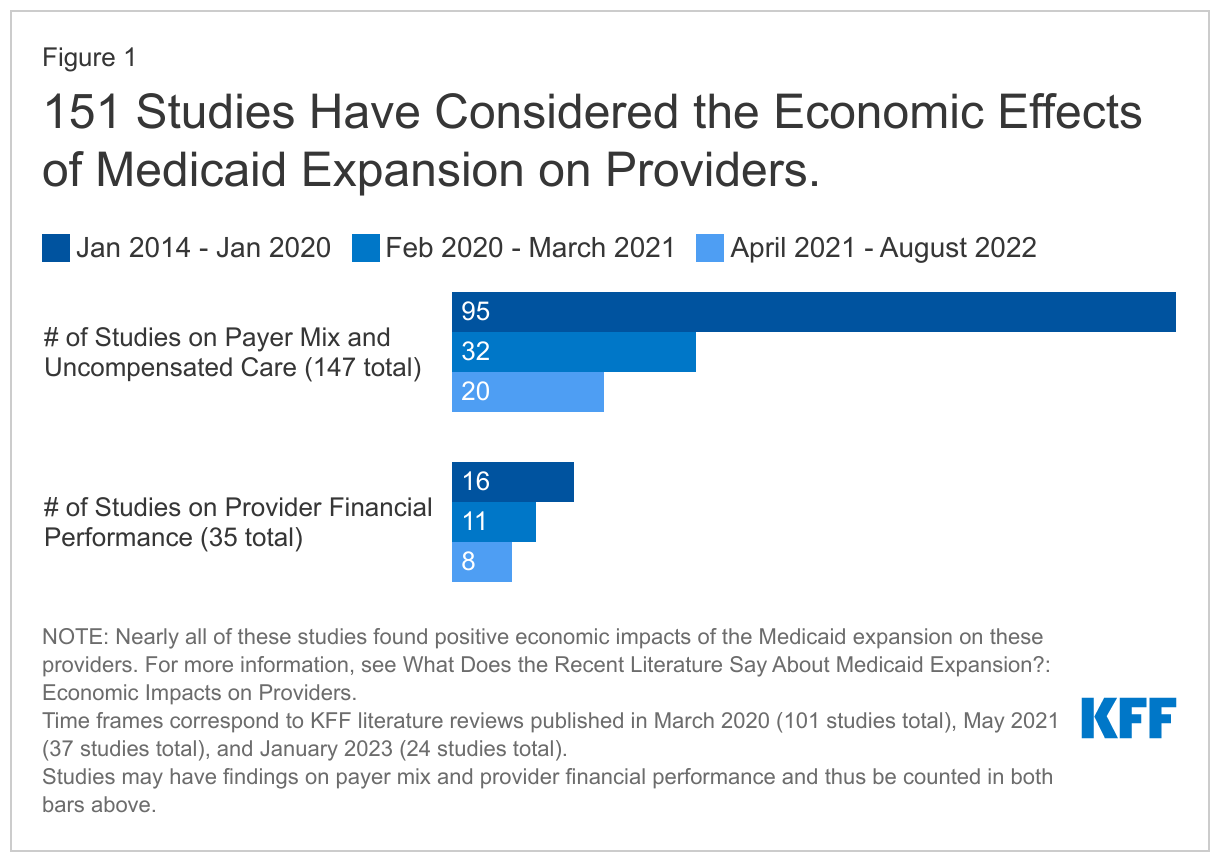
Our methodology is consistent with that of prior analyses. Study findings fall into two topic areas: impacts on payer mix and on the financial performance of providers (Figure 1). Within each topic area, we first briefly summarize findings from earlier research (published between January 2014 and March 2021) and then highlight key findings from recent research that add to this body of evidence. For more information about earlier studies, see the 2021 and 2020 literature review sections on the economic impacts on providers. For citations from January 2014 through December 2022, see the Bibliography.
Payer Mix and Uncompensated Care
Prior studies overwhelmingly found that Medicaid expansion has resulted in payer mix improvements (declines in uninsured patients and/or increases in Medicaid-covered patients). Findings include payer mix improvements for hospitalizations, emergency department visits, and visits to community health centers and other safety-net clinics. Studies identify payer mix improvements overall and among patients being treated for a range of specific conditions, including different types of cancer, traumatic injuries, and substance use disorder. In line with payer mix improvements, studies also find decreased uncompensated care costs (UCC) overall and for specific types of hospitals, including those in rural areas.
Consistent with previous research, nearly all recent studies find that expansion has resulted in payer mix improvements, including among patients treated for specific conditions, as well as decreases in UCC. Of eighteen studies that consider the impact of expansion on payer mix, eleven find both decreases in the proportion of uninsured patients and increases in Medicaid-covered patients,1 ,2 ,3 ,4 ,5 ,6 ,7 ,8 ,9 ,10 ,11 and an additional five studies find increases in Medicaid patients but did not study or found no impact of expansion on the proportion of uninsured patients.12 ,13 ,14 ,15 ,16 ,17 In line with these improvements, three studies also find decreased UCC for hospitals and other providers.18 ,19 ,20 Notably, all studies that considered emergency department visits found payer mix improvements. Studies continue to consider and find payer mix improvements for patients treated for specific conditions, such as different types of surgery and behavioral health admissions. Although studies evaluating payer mix most frequently consider hospitals, two recent studies considered coverage of primary care patients; both found that Medicaid-covered visits to primary care providers increased.21 ,22 ,23 Just two recent studies found no impact of expansion on payer mix but were narrowly focused on critical access and safety-net provider.24 ,25
Financial Performance of Hospitals and Other Providers
Prior research found that Medicaid expansion has improved the financial performance of hospitals and other providers, though these effects may vary somewhat by hospital type. Studies show that expansion contributed to increased hospital revenue overall and from specific services. A few studies indicate that expansion reduced the number of annual hospital closures. Although studies find that expansion has improved provider operating margins and profitability, these findings vary by provider type. For example, a few studies find that despite declines in UCC, improvements in financial performance were stronger for (or only observed among) rural and small hospitals. A small number of studies suggest that improvements in payer mix and UCC at hospitals may have been partially offset by increases in unreimbursed Medicaid care and declines in commercial revenue.
Recent studies continue to find mostly positive financial impacts of expansion on specific types of hospitals, clinics, and other providers. Of eight studies in this area, six find that expansion resulted in positive financial outcomes for a range of provider types,26 ,27 ,28 ,29 ,30 ,31 while two recent studies suggest that these positive effects did not extend to critical access hospitals or free and charitable clinics.32 ,33
- Hospitals. Studies suggest that hospitals experienced higher reimbursements and that decreased uncompensated care costs outweighed increases in unreimbursed Medicaid care for a net positive effect.34 ,35 One study found that expansion was associated with a large reduction in hospital closures, but that this effect was concentrated among hospitals without obstetrics units, while expansion had no lasting effects on closures of hospital-based obstetrics units.36 Federal law requires all states, including those that have not expanded Medicaid, to provide Medicaid coverage to pregnant women with incomes up to at least 138% of the poverty level.37
- Clinics and primary care providers. Studies find that federally qualified health centers and community health centers experienced increased revenue following expansion.38 ,39 Also, one study found higher salary growth for primary care providers in expansion versus non-expansion states.40
Looking Ahead
These new studies add to the body of prior research finding overwhelmingly positive economic effects of expansion on providers. Such findings are particularly relevant given the fiscal stress experienced by Medicaid providers during the coronavirus pandemic, including recent challenges faced by hospitals as federal relief funds expire. This research also provides context for ongoing debates about whether to expand Medicaid in states that have not done so already. Additionally, earlier literature on the financial impact of expansion on states found positive effects, including budget savings, revenue gains, and overall economic growth. Although research in this area appears to have slowed, these findings remain relevant: state costs continue to be a key issue in expansion debates and there have been fluctuations in state economic conditions during the COVID-19 pandemic. Future research could also capture the effect of the additional temporary fiscal incentive included in the American Rescue Plan Act (ARPA) of 2021 (estimated to more than offset the state costs of expansion for the first two years following implementation).41
Bibliography
Bibliography, January 2014 to December 2022
Bibliography (.pdf)
Endnotes
- Diana Hamer et al., "Effect of Medicaid Expansion on Visit Composition in a Louisiana Health Care System," Ochsner Journal 22 no. 2 (June 2022): 154-162, https://doi.org/10.31486/toj.21.0106 ↩︎
- Fan Zhao and Roch A. Niango, "Medicaid Expansion’s Impact on Emergency Department Use by State and Payer," Health Policy Analysis 25 no. 4 (April 2022), https://doi.org/10.1016/j.jval.2021.09.014 ↩︎
- Jayani Jayawardhana, "Impact of Medicaid Expansion on Mental Health and Substance Use Related Emergency Department Visits," Substance Abuse 43 no. 1 (July 2021): 356-363, https://doi.org/10.1080/08897077.2021.1941521 ↩︎
- Vashisht V. Madabhushi, "Impact of the Affordable Care Act Medicaid Expansion on Reimbursement in Emergency General Surgery," Journal of Gastrointestinal Surgery 26 (May 2021): 191-196, https://doi.org/10.1007/s11605-021-05028-8 ↩︎
- Ankit Mishra et al., "ACA Medicaid Expansion Reduced Disparities in Use of High-volume Hospitals for Pancreatic Surgery," Pancreas Presented at the Academic Surgical Congress 2020 170 no. 6 (December 2021): 1785-1793, https://doi.org/10.1016/j.surg.2021.05.033 ↩︎
- Benjamin B. Albright et al., "Medicaid Expansion Reduced Uninsured Surgical Hospitalizations And Associated Catastrophic Financial Burden," Health Affairs 40 no. 8 (August 2021), https://doi.org/10.1377/hlthaff.2020.02496 ↩︎
- Ashley Lall et al., "Analysis of Emergency Department Utilization in Medicaid Expansion and Non-expansion States," Cureus 13 no. 10 (October 2021), https://doi.org/10.7759/cureus.18561 ↩︎
- Blake T. McGee et al., "Associations of Medicaid Expansion With Access to Care, Severity, and Outcomes for Acute Ischemic Stroke," Circulation: Cardiovascular Quality and Outcomes 14 no. 10 (October 2021), https://doi.org/10.1161/CIRCOUTCOMES.121.007940 ↩︎
- Theodoros V. Giannouchous et al., "The Effect of the Medicaid Expansion on Frequent Emergency Department Use in New York," Administration of Emergency Medicine 61 no. 6 (September 2021): 749-762, https://doi.org/10.1016/j.jemermed.2021.07.003 ↩︎
- Michael K. Dalton et al., "The Impact of the Affordable Care Act’s Medicaid Expansion on Patients Admitted for Burns: An Analysis of National Data," Burns 48 no. 6 (September 2022): 1340-1346, https://doi.org/10.1016/j.burns.2021.10.018 ↩︎
- Gianna Dingillo, Christine E. Alvarado, and Christopher W. Towe, "Affordable Care Act Medicaid Expansion is Associated With Increased Utilization of Minimally Invasive Lung Resection for Early Stage Lung Cancer," The American Surgeon (November 2022), https://journals.sagepub.com/doi/10.1177/00031348221138081 ↩︎
- Each of the studies that found no impact studied providers that saw very small numbers of uninsured patients in both time periods. ↩︎
- Nina Mulia, Camiillia K. Lui, Kara M. K. Bensley, and Meenakshi S. Subbaraman, "Effects of Medicaid Expansion on Alcohol and Opioid Treatment Admissions in U.S. Racial/Ethnic groups," Drug and Alcohol Dependence 231 no. 1 (February 2022), https://doi.org/10.1016/j.drugalcdep.2021.109242 ↩︎
- Jacques A. Greenberg et al., "Association of the Affordable Care Act With Access to Highest-Volume Centers for Patients with Thyroid Cancer," Surgery 171 no. 1 (September 2021): 132-139, https://doi.org/10.1016/j.surg.2021.04.059 ↩︎
- Jacob K. Greenberg, Derek S. Brown, Margaret A. Olsen, and Wilson Z. Ray, "Association of Medicaid Expansion Under the Affordable Care Act with Access to Elective Spine Surgical Care," Journal of Neurosurgery Epub ahead of print (September 2021), https://doi.org/10.3171/2021.3.SPINE2122 ↩︎
- Hannah T. Neprash, Anna Zink, Bethany Sheridian, and Katherine Hempsted, "The Effect of Medicaid Expansion on Medicaid Participation, Payer Mix, and Labor Supply in Primary Care," Journal of Health Economics 80 (December 2021), https://doi.org/10.1016/j.jhealeco.2021.102541 ↩︎
- Gianna Dingillo, Christine E. Alvarado, and Christopher W. Towe, "Affordable Care Act Medicaid Expansion is Associated With Increased Utilization of Minimally Invasive Lung Resection for Early Stage Lung Cancer," The American Surgeon (November 2022), https://journals.sagepub.com/doi/10.1177/00031348221138081 ↩︎
- Taitane Santos, Simone Singh, and Gary J. Young, "Medicaid Expansion and Not-For-Profit Hospitals’ Financial Status: National and State-Level Estimates Using IRS and CMS Data, 2011-2016," Sage Journals Medical Care Research and Review 79 no. 3 (April 22, 2021): 448-457, https://doi.org/10.1177/10775587211009720 ↩︎
- Paula Chattarjee, Rachel M. Werner, and Karen E. Joynt Maddox, "Medicaid Expansion Alone Not Associated With Improved Finances, Staffing, Or Quality At Critical Access Hospitals," Health Affairs 40 no. 12 (December 2021), https://doi.org/10.1377/hlthaff.2021.00643 ↩︎
- Qian Lou, Ali Moghtaderi, Anne Markus, and Avi Dor, "Financial Impacts of the Medicaid Expansion on Community Health Centers," Health Services Research 57 no. 3 (October 2021): 634-643, https://doi.org/10.1111/1475-6773.13897 ↩︎
- However, only one of these studies found that uninsured visits decreased (the other found no change). ↩︎
- Diana Hamer et al., "Effect of Medicaid Expansion on Visit Composition in a Louisiana Health Care System," Ochsner Journal 22 no. 2 (June 2022): 154-162, https://doi.org/10.31486/toj.21.0106 ↩︎
- Hannah T. Neprash, Anna Zink, Bethany Sheridian, and Katherine Hempsted, "The Effect of Medicaid Expansion on Medicaid Participation, Payer Mix, and Labor Supply in Primary Care," Journal of Health Economics 80 (December 2021), https://doi.org/10.1016/j.jhealeco.2021.102541 ↩︎
- Paula Chattarjee, Rachel M. Werner, and Karen E. Joynt Maddox, "Medicaid Expansion Alone Not Associated With Improved Finances, Staffing, Or Quality At Critical Access Hospitals," Health Affairs 40 no. 12 (December 2021), https://doi.org/10.1377/hlthaff.2021.00643 ↩︎
- Karen E. Lasser et al., "Changes in Hospitalizations at US Safety-Net Hospitals Following Medicaid Expansion," Jama Network Open Health Policy 4 no. 6 (June 2021), https://doi.org/10.1001/jamanetworkopen.2021.14343 ↩︎
- Yanlei Ma, David Armstrong, Gaetano Forte, and Hao Yu, "Effects of the Affordable Care Act Medicaid Expansion on the Compensation of New Primary Care Physicians," Official Journal of the Medical Care Section, American Public Health Association 60 no. 8 (August 2022): 636-644, https://journals.lww.com/lww-medicalcare/Abstract/2022/08000/Effects_of_the_Affordable_Care_Act_Medicaid.13.aspx ↩︎
- Shiyin Jiao, R. Tamara Konetzka, Harold A. Pollack, and Elbert S. Huang, "Estimating the Impact of Medicaid Expansion and Federal Funding Cuts on FQHC Staffing and Patient Capacity," Multidisciplinary Journal of Population Health and Health Policy 100 no. 2 (April 2022): 504-524, https://doi.org/10.1111/1468-0009.12560 ↩︎
- Taitane Santos, Simone Singh, and Gary J. Young, "Medicaid Expansion and Not-For-Profit Hospitals’ Financial Status: National and State-Level Estimates Using IRS and CMS Data, 2011-2016," Sage Journals Medical Care Research and Review 79 no. 3 (April 22, 2021): 448-457, https://doi.org/10.1177/10775587211009720 ↩︎
- Caitlin Carrol, Julia D. Interrante, Jamie R. Daw, and Katy Backes Kozhimannil, "Association Between Medicaid Expansion and Closure of Hospital-Based Obstetric Services," Health Affairs 41 no. 4 (April 2022), https://doi.org/10.1377/hlthaff.2021.01478 ↩︎
- Vashisht V. Madabhushi, "Impact of the Affordable Care Act Medicaid Expansion on Reimbursement in Emergency General Surgery," Journal of Gastrointestinal Surgery 26 (May 2021): 191-196, https://doi.org/10.1007/s11605-021-05028-8 ↩︎
- Qian Lou, Ali Moghtaderi, Anne Markus, and Avi Dor, "Financial Impacts of the Medicaid Expansion on Community Health Centers," Health Services Research 57 no. 3 (October 2021): 634-643, https://doi.org/10.1111/1475-6773.13897 ↩︎
- Julie S. Darnell and Lindsay O'Brien, "Location, Location, Location: The Affordable Care Act's Impact on Free Clinics Depends on What State They're In," Journal of Health Care for the Poor and Underserved 33 no. 2 (May 2022): 887-901, https://doi.org/10.1353/hpu.2022.0070 ↩︎
- Paula Chattarjee, Rachel M. Werner, and Karen E. Joynt Maddox, "Medicaid Expansion Alone Not Associated With Improved Finances, Staffing, Or Quality At Critical Access Hospitals," Health Affairs 40 no. 12 (December 2021), https://doi.org/10.1377/hlthaff.2021.00643 ↩︎
- Vashisht V. Madabhushi, "Impact of the Affordable Care Act Medicaid Expansion on Reimbursement in Emergency General Surgery," Journal of Gastrointestinal Surgery 26 (May 2021): 191-196, https://doi.org/10.1007/s11605-021-05028-8 ↩︎
- Taitane Santos, Simone Singh, and Gary J. Young, "Medicaid Expansion and Not-For-Profit Hospitals’ Financial Status: National and State-Level Estimates Using IRS and CMS Data, 2011-2016," Sage Journals Medical Care Research and Review 79 no. 3 (April 22, 2021): 448-457, https://doi.org/10.1177/10775587211009720 ↩︎
- Caitlin Carrol, Julia D. Interrante, Jamie R. Daw, and Katy Backes Kozhimannil, "Association Between Medicaid Expansion and Closure of Hospital-Based Obstetric Services," Health Affairs 41 no. 4 (April 2022), https://doi.org/10.1377/hlthaff.2021.01478 ↩︎
- Thus, the authors note that because Medicaid eligibility limits for pregnant individuals were already at or higher than the newly expanded limit for adults, the expansion would likely only improve the financial performance of obstetrics units indirectly (if hospitals used the additional revenue to cross-subsidize obstetric services). ↩︎
- Shiyin Jiao, R. Tamara Konetzka, Harold A. Pollack, and Elbert S. Huang, "Estimating the Impact of Medicaid Expansion and Federal Funding Cuts on FQHC Staffing and Patient Capacity," Multidisciplinary Journal of Population Health and Health Policy 100 no. 2 (April 2022): 504-524, https://doi.org/10.1111/1468-0009.12560 ↩︎
- Qian Lou, Ali Moghtaderi, Anne Markus, and Avi Dor, "Financial Impacts of the Medicaid Expansion on Community Health Centers," Health Services Research 57 no. 3 (October 2021): 634-643, https://doi.org/10.1111/1475-6773.13897 ↩︎
- Yanlei Ma, David Armstrong, Gaetano Forte, and Hao Yu, "Effects of the Affordable Care Act Medicaid Expansion on the Compensation of New Primary Care Physicians," Official Journal of the Medical Care Section, American Public Health Association 60 no. 8 (August 2022): 636-644, https://journals.lww.com/lww-medicalcare/Abstract/2022/08000/Effects_of_the_Affordable_Care_Act_Medicaid.13.aspx ↩︎
- Thus far, Missouri and Oklahoma implemented expansion in July 2021 following successful ballot initiatives the prior summer, and South Dakota plans to implement expansion in July 2023 following a successful ballot initiative in November 2022. ↩︎