Key Characteristics of Infants and Implications of the Recent Formula Shortage
In recent weeks, the United States has been grappling with a baby formula shortage following supply chain issues, a voluntary recall, and the closing of a plant that produces a large share of the country’s formula. Data for the week ending May 28th show that the nationwide out-of-stock percentage for baby formula reached 74% among U.S. retailers. Since it is recommended that infants receive breast milk or formula until they are age one, this shortage has had a significant impact across the country. Infants in low-income families and infants of color, who are often covered by Medicaid, may be particularly impacted by the shortage resulting in potential short and long-term health risks. To better understand who may be particularly affected and at risk from the formula shortage, we analyzed data from the 2019 American Community Survey and data from the Centers for Disease Control and Prevention’s (CDC’s) National Immunization Survey for infants born in 2018 to describe the size and characteristics of the U.S. infant population as well as their use of formula.
Who does the formula shortage impact?
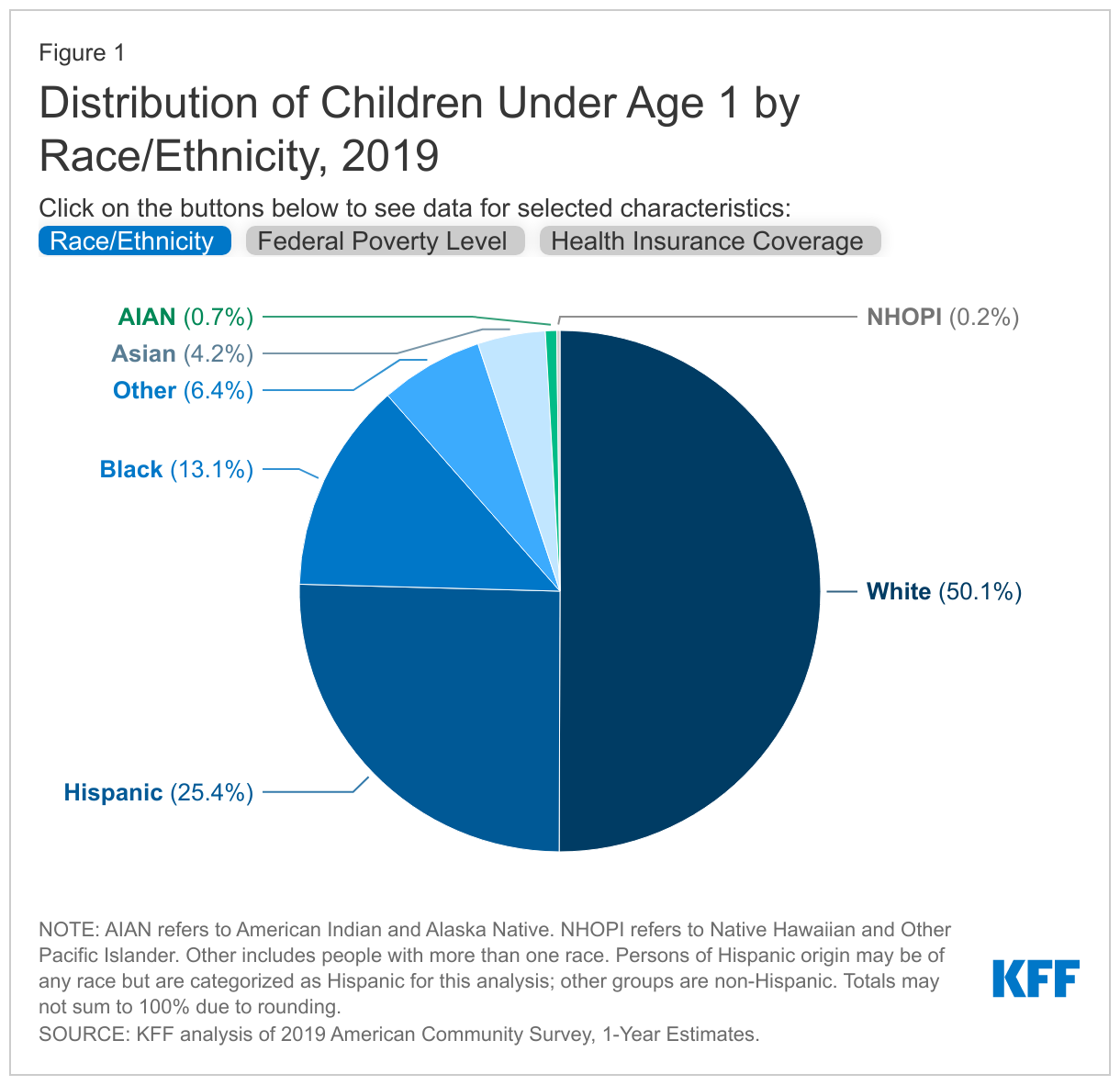
As of 2019, there were approximately 3.4 million infants under the age of one in the U.S..1 Almost half of children under the age of one are children of color, including more than a quarter who are Hispanic (25.4%), 13.1% who are Black, and 4.2% who are Asian (Figure 1). Smaller shares are American Indian or Alaska Native (AIAN) or Native Hawaiian or Other Pacific Islander (NHOPI) (<1% each). Nearly four in ten children under the age of one live in a family with income below 200% of the Federal Poverty Level (FPL), including 18.2% below poverty and 21.1% between 100-200% FPL (the FPL was $20,578 for a family of three in 2019). Over four in ten (42.0%) of all children under the age of one are covered by Medicaid/CHIP.
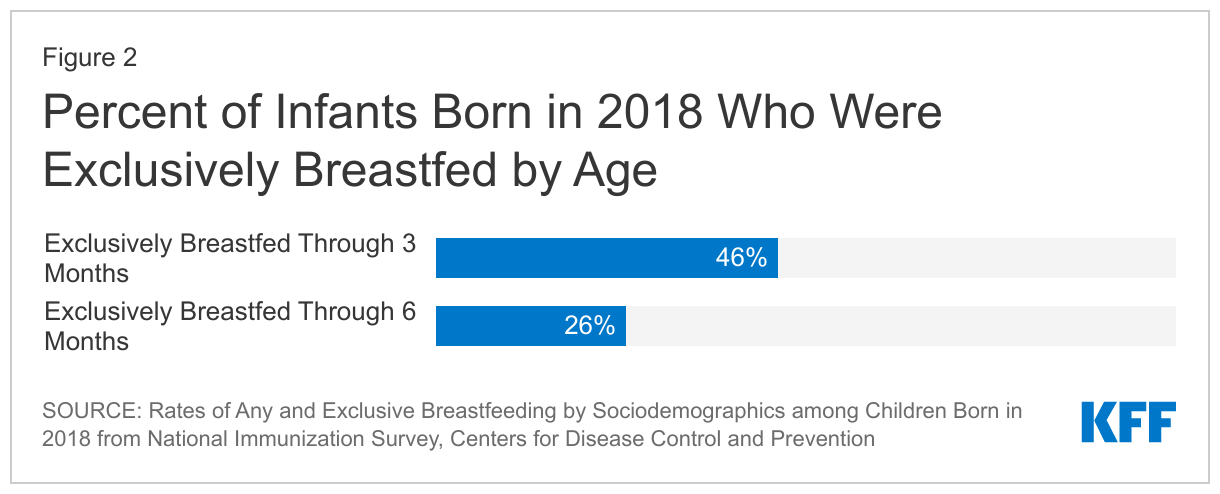
More than half (54%) of infants born in 2018 received formula, either exclusively or as a supplement, by three months of life (Figure 2). The CDC reports that 46% of babies born in 2018 were exclusively breastfed through three months of age and 26% through six months. The CDC also reports that, among babies born in 2018, 19% of breastfed infants were supplemented with formula within two days of life.
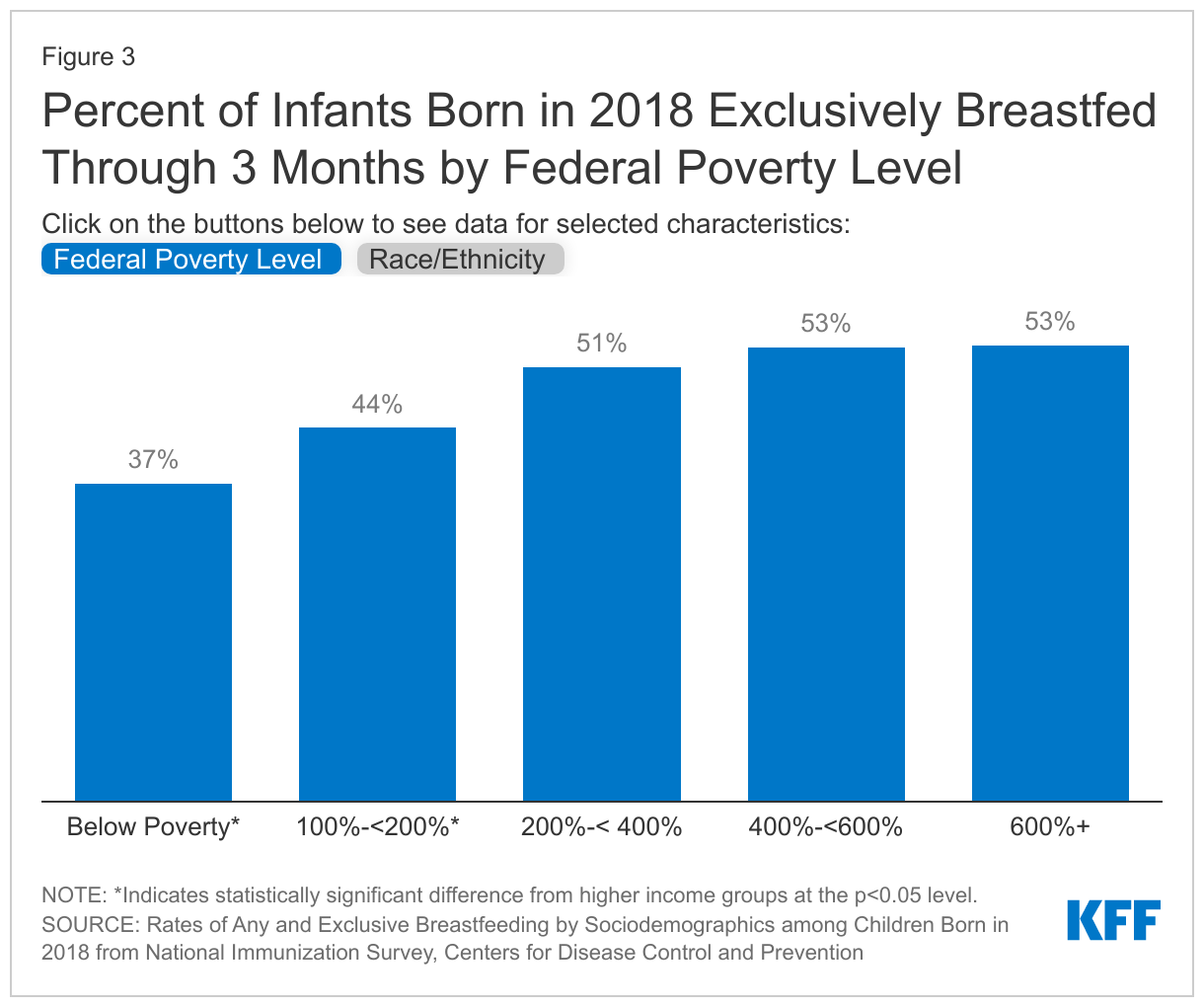
Infants in low-income families, infants of color, and infants living in rural communities are more likely to use formula and therefore may be hardest hit by the formula shortage. Infants in lower income households are less likely than those in higher income households to report exclusive breastfeeding through the first three months of life (Figure 3). Similarly, data show that lower shares of Black and Hispanic infants are exclusively breastfed through their first three months of life compared to White infants (Figure 3). CDC data also show Black infants born in 2018 are less likely to be ever breastfed compared to Asian, White, and Hispanic infants. Infants living in rural areas are also less likely to be ever breastfed than those in urban areas. In addition to already being more likely to use formula, low-income families also may have less time and resources to search for and purchase in-stock formula, and those living in rural areas may have fewer retailers available in their proximity to access formula. Moreover, babies with complex health needs may require specific formula types, which may be more difficult to find.
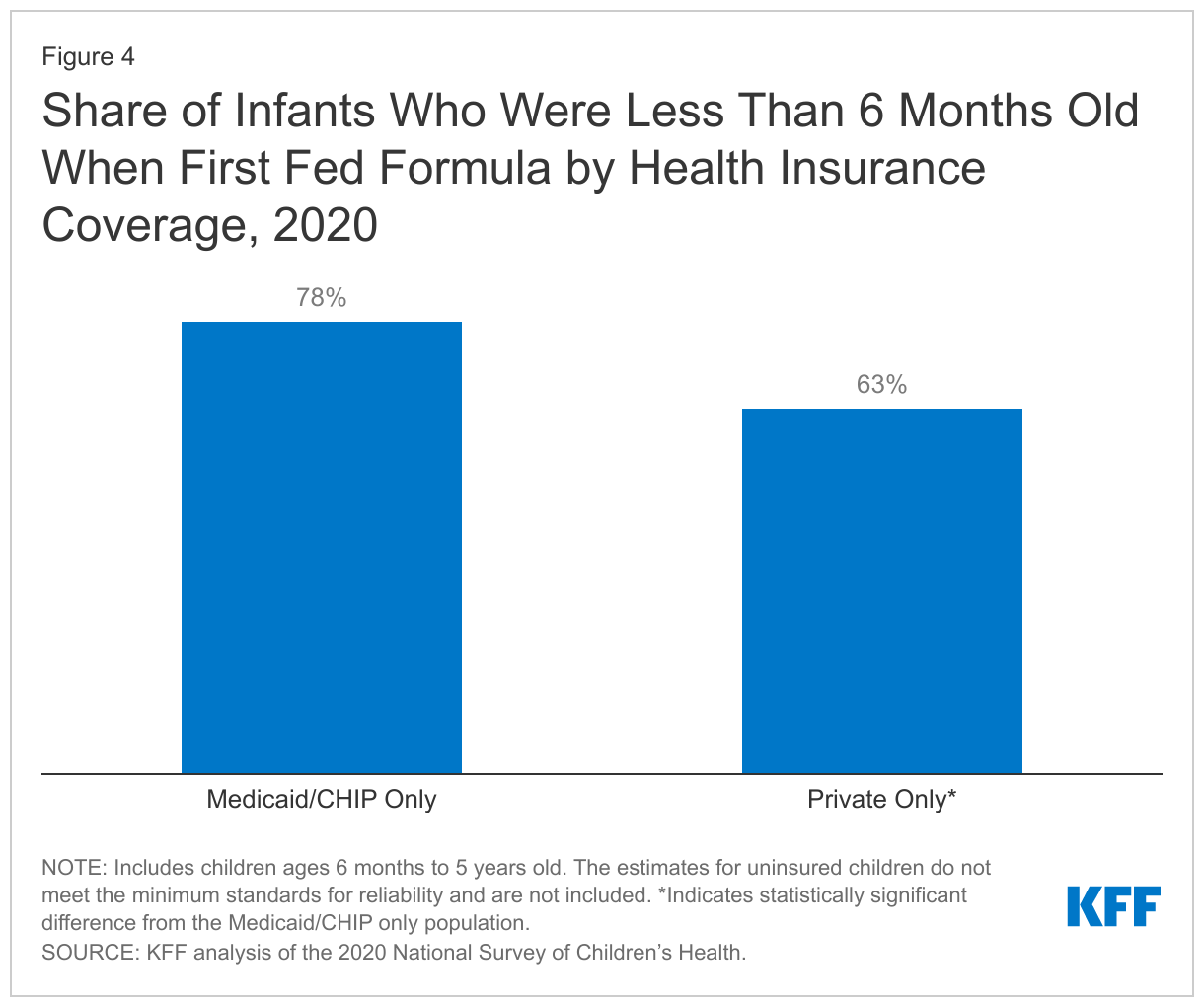
Medicaid and CHIP cover many infants that are likely being hardest hit by the formula shortage. The majority of children under the age of one covered by Medicaid and CHIP are infants in low-income families and infants of color, who are more likely to be impacted by the formula shortage.2 Over one-third (34%) of all children who reported receiving formula during the first 12 months of their life were covered by Medicaid/CHIP only.3 Also, infants with Medicaid/CHIP as their sole source of coverage were more likely to report receiving formula for the first time before 6 months old compared to infants with private insurance only (Figure 4).
Almost half of all formula in the U.S. is purchased by families enrolled in WIC. WIC is a nationwide program designed to support low-income women, infants, and children up to age five found to be at nutritional risk. State WIC programs provide infant formula to WIC participants and typically enter into rebate contracts with infant formula manufacturers, providing one brand of formula in exchange for a rebate. CDC data show infants enrolled in WIC are less likely to report ever being breastfed compared to those not receiving or ineligible for WIC. In addition, approximately three quarters of individuals eligible for the Special Supplemental Nutrition Program for WIC were also enrolled in Medicaid.
What are the implications of the formula shortage?
There may be health and economic consequences for infants and families who are not able to access enough formula. Baby formula provides vitamins and nutrients essential for a baby’s growth during an important period of child development. Without these nutrients, children can face significant short- and long-term health complications, including dehydration, slow growth, behavior problems, and developmental delays. Diluting formula or formula alternatives can also be dangerous for babies, slowing growth and possibly causing health issues including seizures. The data above suggest that low-income infants and infants of color may be at increased risk for facing these health risks, which may contribute to widening disparities in health for these groups. Infants with allergies or special health needs may also find it more difficult to find the specific formula they need, increasing their risk for health complications. Moreover, as the primary source of coverage for a majority of low-income children, Medicaid programs would be responsible for providing medical care to infants experiencing health complications. Further, the formula shortage comes at a time when inflation and prices for household goods and gas have risen, putting a strain on family budgets. There may be financial implications for families, with some WIC recipients reporting paying out of pocket to obtain the formula they need.
There are limited options for families navigating the formula shortage. The Department of Health and Human Services advises families to try different brands of formulas and to try formulas made in a different country. For infants relying on hypogenic or medical specialty formula, families are advised to talk to a pediatrician or other health care provider about substitutes, who may also be able to submit urgent product requests to Abbott Nutrition, which is releasing some specialty formulas on a case-by-case basis. As a major source of coverage for infants, Medicaid providers and health plans can be a source of trusted information to families about formula options and switching formula brands. State health agencies and WIC offices are also providing tips and information on how to access formula during this time.
A number of legislative actions have been taken to increase access to formula, especially for low-income families. While the formula plant that shutdown recently reopened, it will take weeks to bring the plant to full capacity and the shortage is expected to last until July. In the meantime, the Biden Administration has invoked the Defense Production Act (DPA) and is expediting the import of infant formula through Operation Fly Formula and addressing price gouging. President Biden also recently signed the Access to Baby Formula Act of 2022 into law, which waives certain WIC requirements during an emergency, and states are adopting flexibilities that expand the brands, sizes, and types of formula available to WIC recipients and allow for exchanges of formula purchased by WIC recipients. The House also passed a bill on May 18th that provides $28 million in emergency funding to the U.S. Food and Drug Administration (FDA) to provide resources to address the shortage and prevent future shortages. While these measures are expected to increase the availability of formula in the short-term, some are raising questions on the consolidation of the U.S baby formula market and how a shortage like this will be prevented in the future.