Another, more direct way to measure the performance of the health system is to examine the quality of care provided in a hospital or clinical setting. However, inconsistent and imperfect quality metrics make it difficult to compare quality of care in the U.S. and its peers.
In comparison to peer nations, across the limited measures available internationally, the U.S. performs better on some and worse on other indicators of quality of care. For example, the U.S. performs worse on certain measures of treatment outcomes (such as maternal mortality) and some patient safety measures (such as obstetric trauma with instrument and medication or treatment errors). The U.S. performs similarly to or better than peer nations in other measures of treatment outcomes (such as mortality rates within 30 days of acute hospital treatment) and patient safety (such as rates of post–operative sepsis).
Hospital Mortality Rates
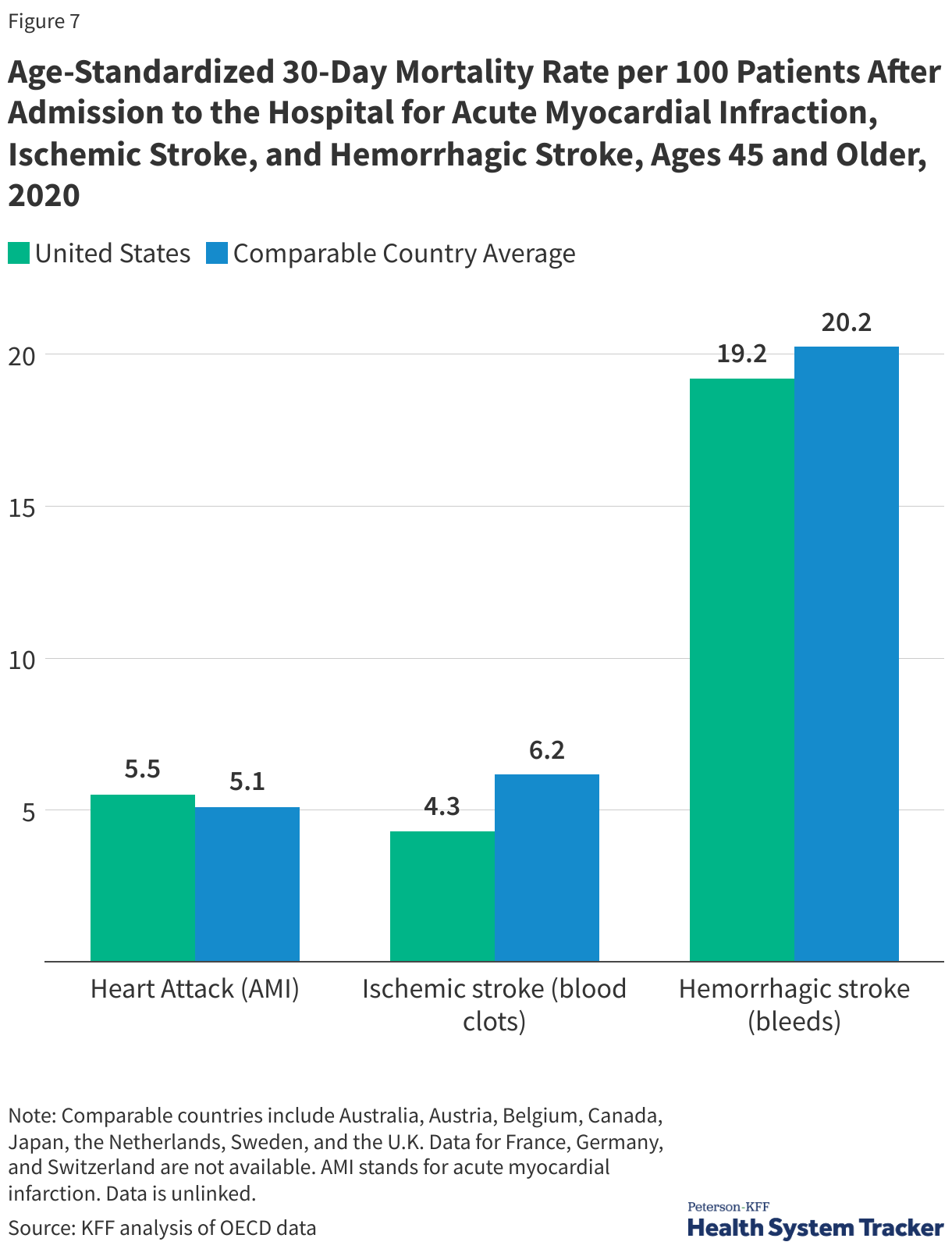
Mortality within 30 days of being admitted to a hospital is not entirely preventable, but high quality of care can reduce the mortality rate for certain diagnoses. The 30-day mortality rates after hospital admissions for heart attacks (acute myocardial infarction) and hemorrhagic stroke (caused by bleeding) are similar in the U.S. and comparable countries average. The 30-day mortality rate for ischemic strokes (caused by blood clots) was 4.3 deaths per 100 patients in the U.S. in 2020, compared to an average of 6.2 deaths per 100 patients in similar countries. While the U.S. has lower mortality rates due to these conditions than the average across peer nations, it is important to note that several peer nations have lower rates than the U.S.
Maternal Health
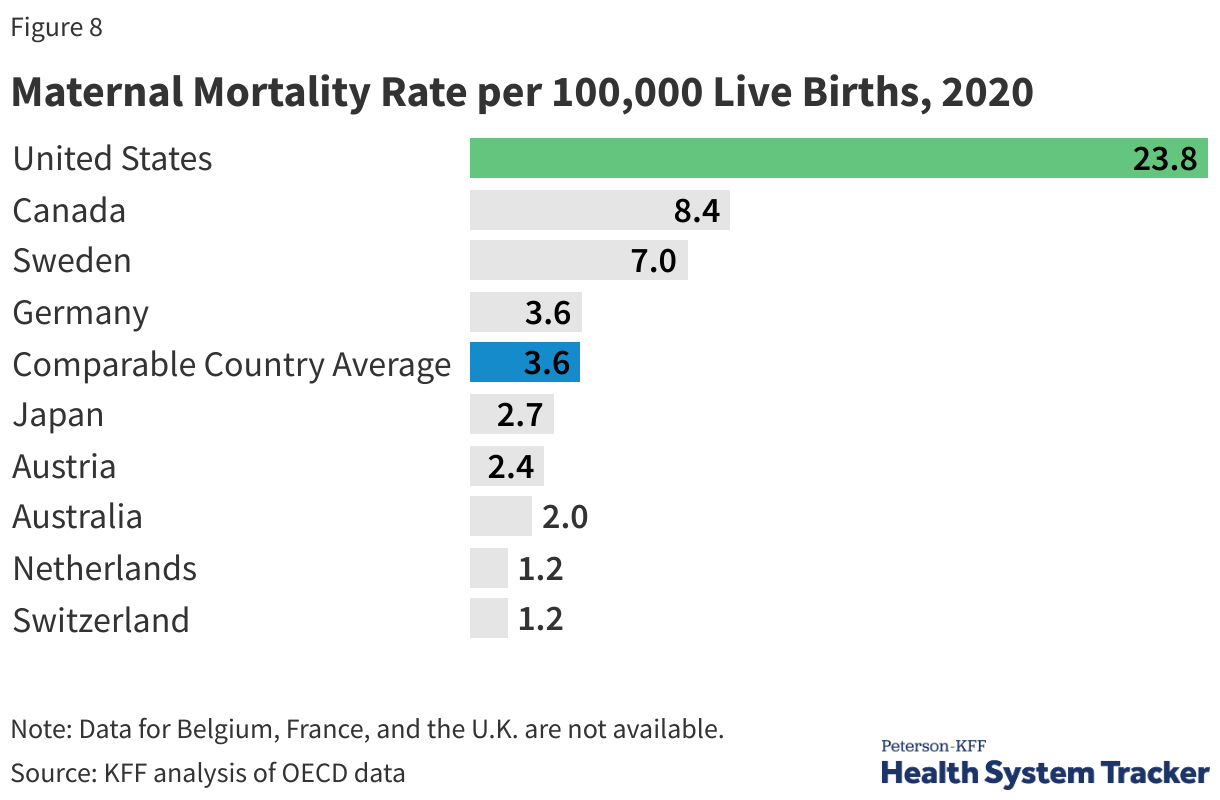
While wealth and economic prosperity are highly correlated with lower maternal mortality rates, the U.S. is an outlier with the highest rate of pregnancy-related deaths (23.8 deaths per 100,000 live births in 2020) when compared to similar countries (3.6 deaths per 100,000 live births).
Within the U.S., there are significant racial disparities in maternal mortality rates. The maternal mortality rate for Black mothers is about three times the rate for White mothers — a disparity that persists across age and socioeconomic groups. Every race and ethnicity, socioeconomic, and age group in the United States sees higher maternal mortality rates than the average in comparable countries. Maternal mortality in the U.S. has risen in recent years, sparking concern from the medical community and policymakers.
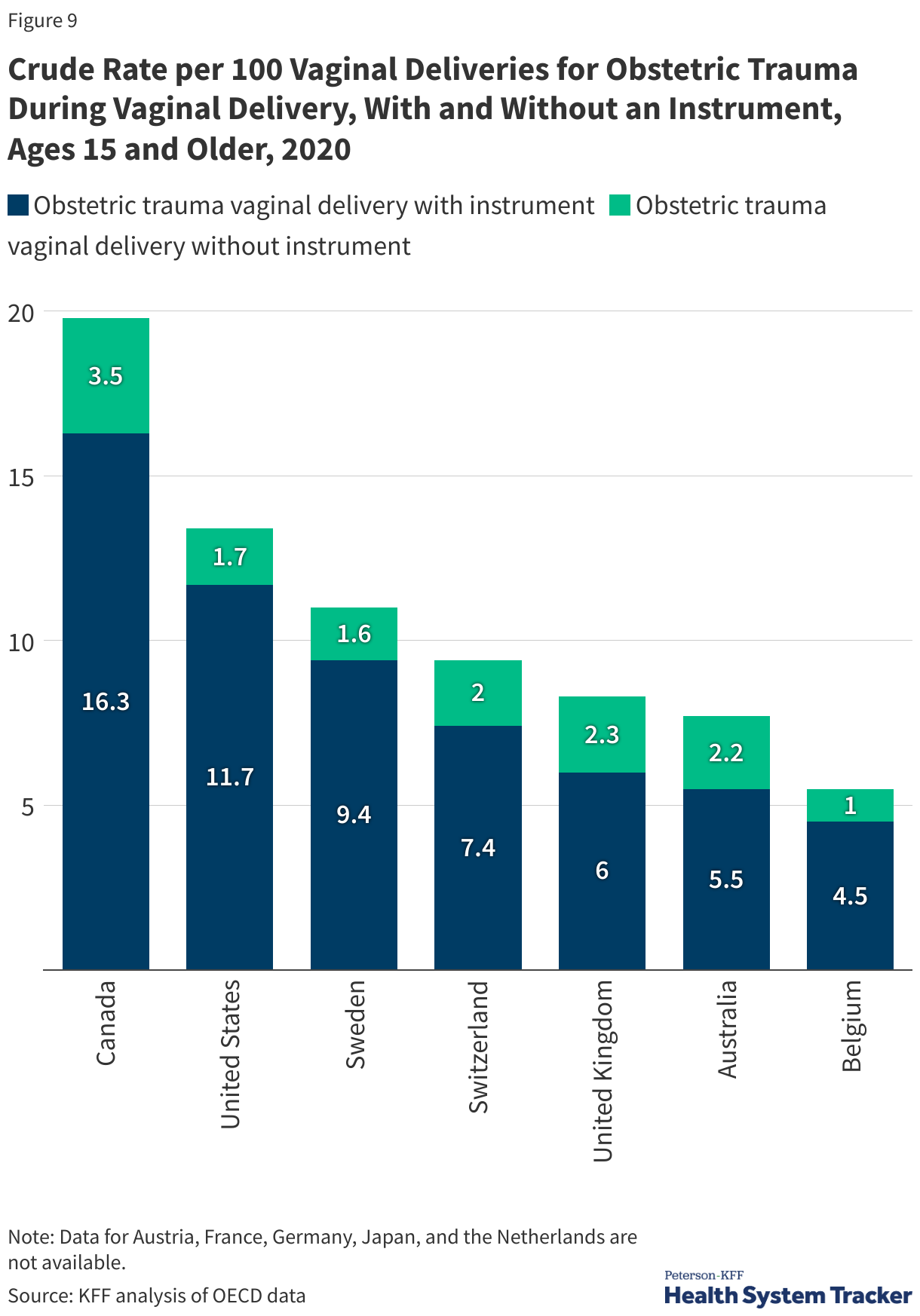
Obstetric trauma is more likely to occur in deliveries where instruments are utilized (i.e., forceps). The rate of obstetric trauma during deliveries with an instrument in the U.S. was 11.7 per 100 vaginal deliveries in 2020, higher than most comparable countries with available data. The rate of obstetric trauma during deliveries without an instrument in the U.S. was 1.7 per 100 vaginal deliveries in 2020, on the lower end among comparable countries with available data.
Hospital Admissions
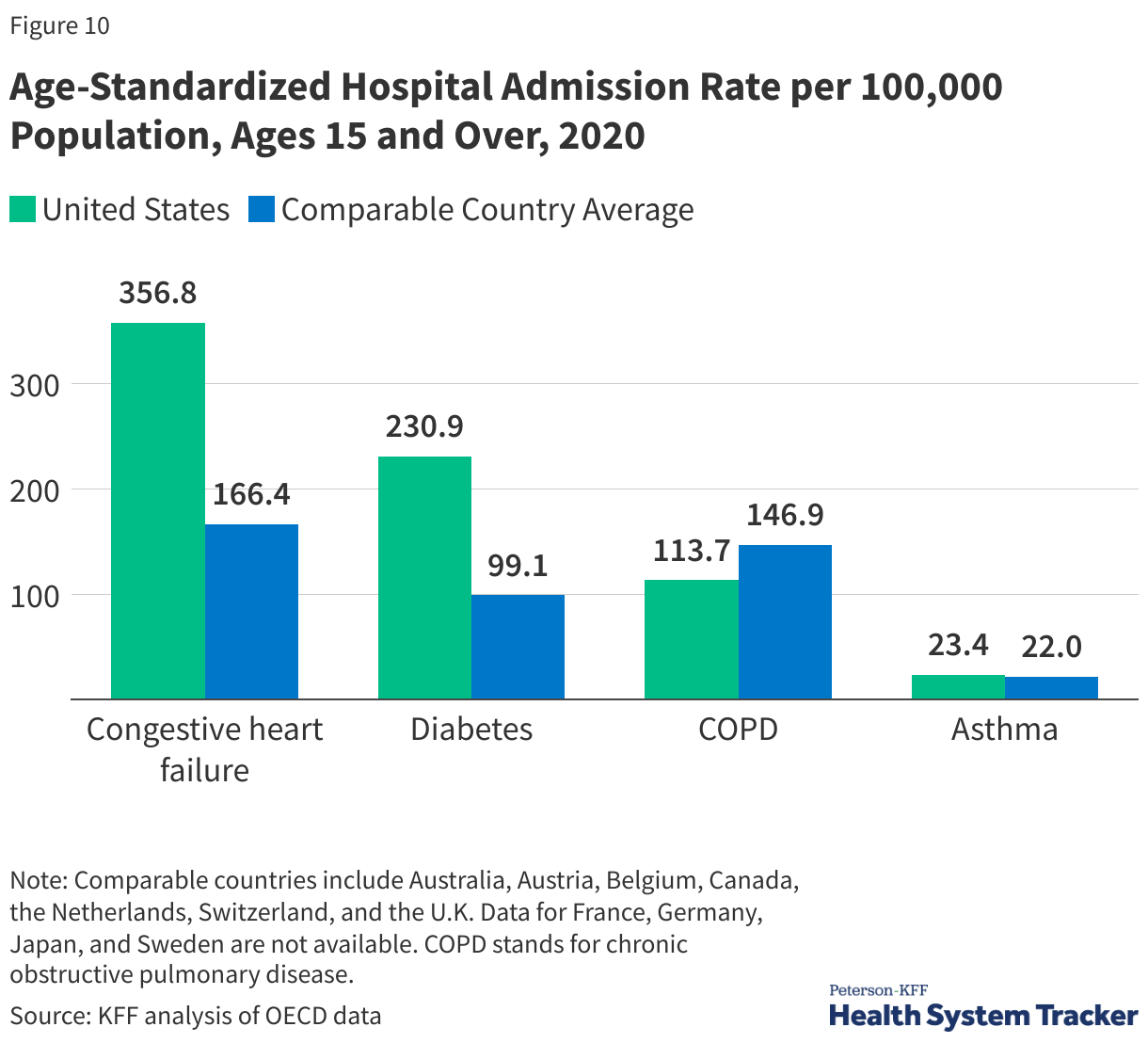
Hospital admissions for certain chronic diseases, such as cardiac conditions, chronic obstructive pulmonary diseases (COPD), asthma, and diabetes, can arise for a variety of reasons, but preventive services — or lack thereof — play a large role. Hospital admission rates in the U.S. are higher than in comparable countries for congestive heart failure and complications due to diabetes, and some admissions for these chronic conditions could be minimized with adequate primary care. Admission rates in 2020 are likely impacted by the COVID-19 pandemic—patients were less likely to seek hospital treatment, and hospitals were at times overwhelmed and unable to admit patients who would have been admitted in a different year.
Post-Operative Complications
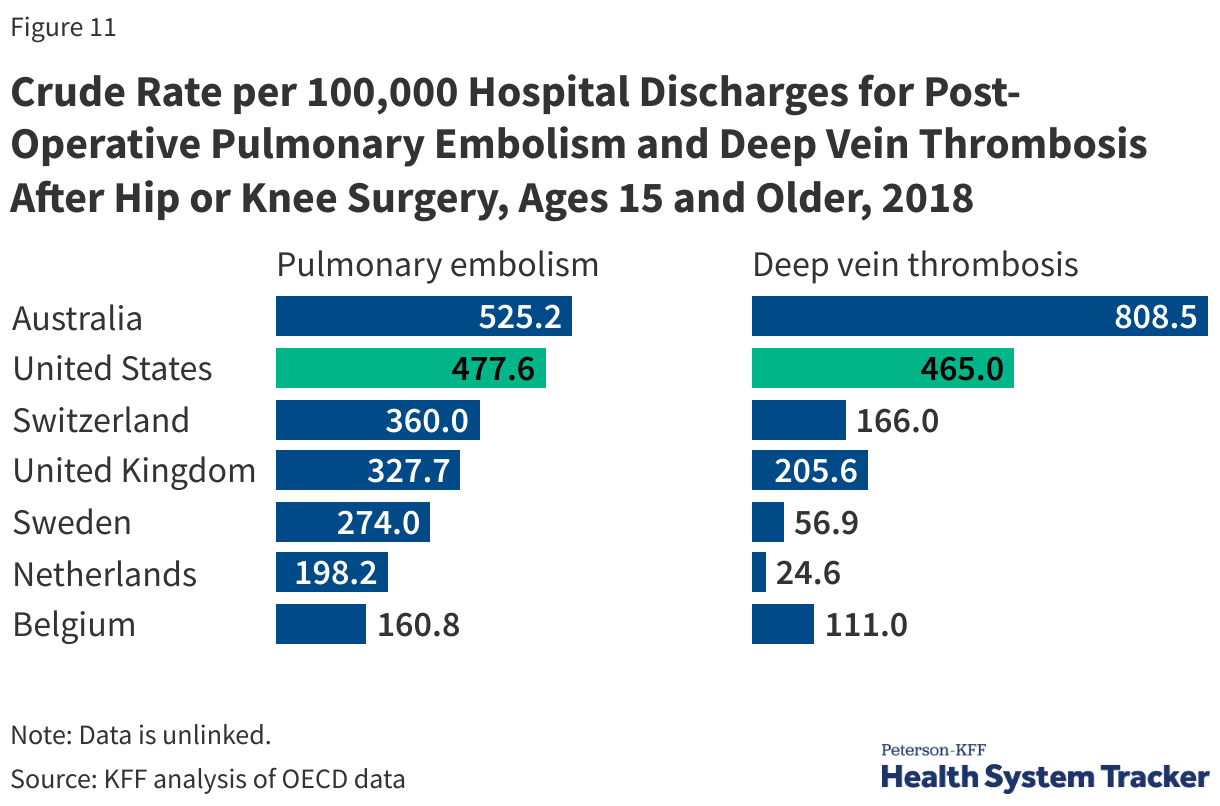
Rates of post-operative complications are an important measure of hospital safety. Pulmonary embolisms and deep vein thrombosis are common complications after major surgeries, such as hip or knee replacement. The prevalence of post-operative clots for these procedures is higher in the U.S. than in the U.K., Sweden, Belgium, and the Netherlands, but lower than in Australia.
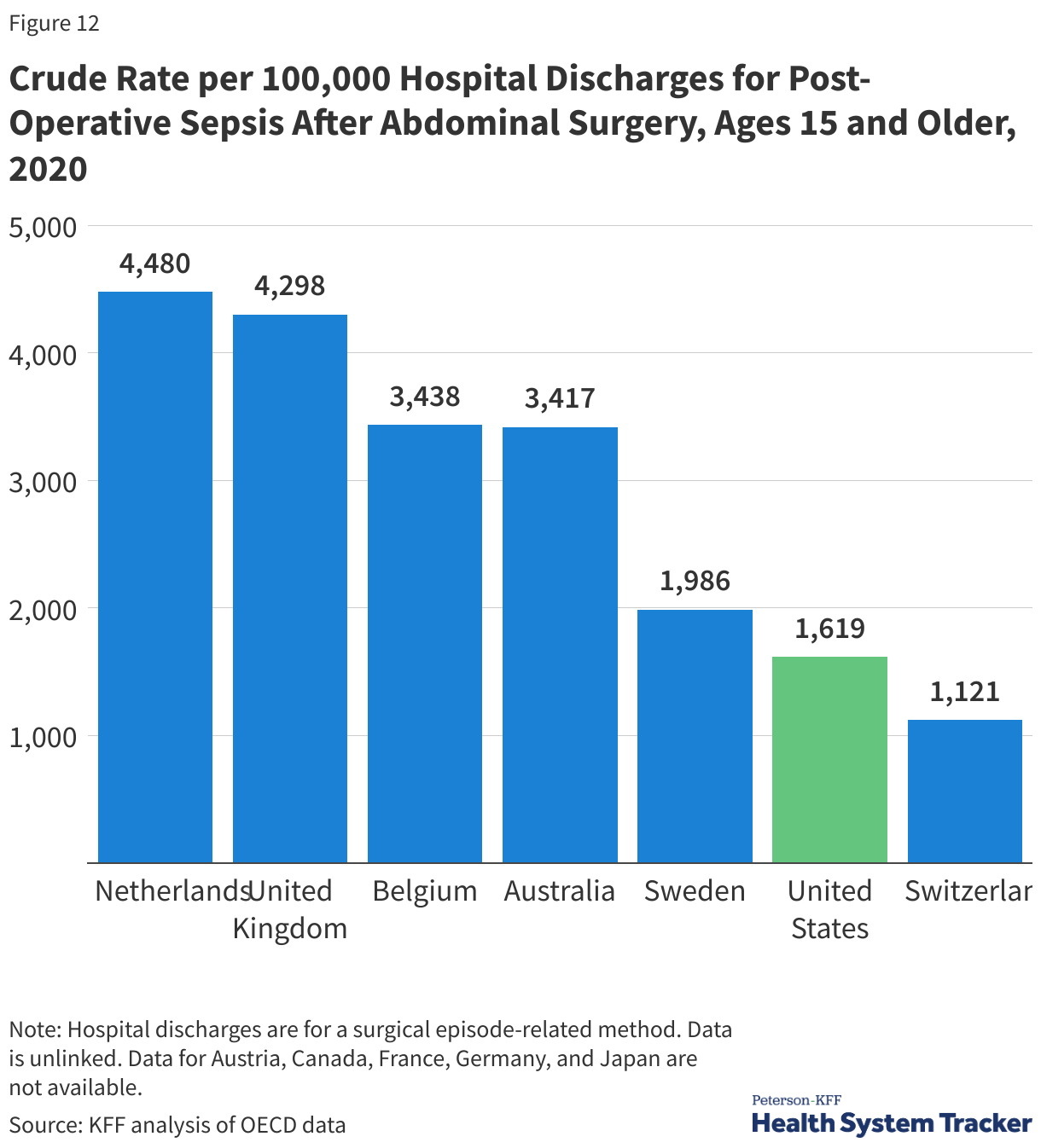
Sepsis is a serious complication for patients with infections, and effects can range from organ failure and shock to death in severe cases. Rates of post-operative infections and sepsis are an important marker of care quality for patients undergoing surgery, because this is a major source of morbidity and mortality that can sometimes be prevented. Prevention is multifactorial and can involve proper operative techniques and training, hygiene and safety protocols, and antibiotic utilization, amongst other things. The rate of post-operative sepsis following abdominal surgery is just under 2% in the U.S., lower than in most peer countries that report data.