Access and Coverage for Mental Health Care for Women
Mental health continues to be a growing area of health concern for people, with 90% of Americans saying there is a mental health crisis in the U.S. in a 2023 KFF-CNN poll. Women’s mental health often differs from men’s, with women experiencing some mental health symptoms more commonly than men but also conditions that are unique to women, such as perinatal and perimenopausal depression.
This brief analyzes data from the 2024 KFF Women’s Health Survey (WHS), a nationally representative survey of 6,246 adults ages 18 to 64, including 5,055 women and 1,191 men, conducted from May 15 to June 18, 2024. In addition to several topics related to reproductive health and well-being, the survey asked respondents about their mental health and their experiences accessing mental health services in the past year. This issue brief presents KFF WHS data on access to mental health services among women and men ages 18 to 64, and it also takes a closer look at mental health coverage among women. See the Methodology section for details.
Key Takeaways
- Nearly three in ten women ages 18 to 64 (28%) describe their mental health or emotional well-being as “fair” or “poor”, including higher shares of women with low incomes (38%) and those who identify as LGBT+ (45%). Nearly three quarters of those who say they have a mental health-related disability (73%) report having “fair/poor” mental well-being.
- Three in ten (29%) women say they received mental health services in the past 12 months. About half of women who describe their mental health as “fair/poor” say they received mental health care in the past year (48%). While eight in 10 ten women with a self-reported mental health-related disability (81%) say they received care, one in five did not.
- Among women who report receiving mental health services, the most commonly reported services are one-on-one care with a provider, in-person (60%) and/or via telehealth (55%). Just over half of this group report receiving a prescription for medication (52%). Few women say they received care through a mental health therapy app (7% of those who report receiving services) or other services like in-patient hospitalization or group therapy (8%).
- Four in ten women overall (38%) say it is difficult for women to get mental health services in their state. One-third (32%) of all women say they did not get mental health services despite needing them, citing barriers such as cost, stigma, or inability to get time off from work.
- Among women who were able to get mental health care, half (50%) say it is difficult for women to access mental health services in their state, and more than half say they experienced barriers during care-seeking (55%). These challenges include trouble finding a provider that was accepting new patients (25%) or one that accepted their insurance (21%). The large majority of women with Medicaid say their most recent mental health care visit was covered completely by Medicaid (85%), whereas most women with private insurance had to pay some (48%) or all (14%) costs out-of-pocket.
- Cost is a significant barrier to obtaining mental health services. More than one in ten women 18 to 64 (13%) say they did not get mental health care or could not continue to afford the mental health care they were receiving because of cost. More than twice as many women without insurance (29%) cite cost as a reason for not getting care.
Self-Described Mental Health
In general, slightly larger shares of women describe their mental health status as “fair” or “poor” compared to men (28% vs. 23%). Most women (72%) and men (77%) describe their mental health as either “good” or “excellent/very good” (Figure 1).
As other research has found, younger adults report mental health challenges at higher rates than older adults. Over one third of younger women ages 18 to 25 describe their mental health status as “fair” or “poor” (36%), compared to a smaller share of women ages 50 to 64 (21%). A higher share of 50 to 64 — about half (49%) – describe their mental well-being as “excellent” or “very good,” which is considerably higher than just three in ten (30%) younger women ages 18 to 25.
About 4 in 10 women (38%) who have low incomes (below 200% of the federal poverty level (FPL)) report fair or poor mental health status, nearly double the rate reported by those with higher incomes (21%). Nearly two times as many women who identify as LGBT+ (45%) say their mental health is “fair” or “poor” compared to those who do not identify as LGBT+ (24%). Not surprisingly, nearly three-quarters of women who identify as having a mental health-related disability (73%) say they have “fair” or “poor” mental health, three times the rate of those who do not identify as being disabled (24%) or who have another non-mental health disability (27%).

Mental Health Care Utilization
Not only do a slightly larger share of women than men report poorer mental health status, but compared to men, a somewhat larger share of women report receiving mental health care in the past 12 months (Figure 2). Roughly three in the ten women (29%) say they received mental health services from a mental health professional, compared to 22% of men.
Younger women are also more likely to use mental health services than older women. One in three women under the age of 50 say they received professional mental health care in the past year, compared to just 22% of women between age 50 and 64. Compared to their White counterparts (31%), smaller shares of Asian (19%) and Hispanic (24%) women say they received mental health care in the past year, consistent with previous mental health findings from KFF polling. Black (30%) and White women report obtaining mental health care at similar rates.
Consistent with the findings on self-described mental well-being, nearly twice as many women who identify as LGBT+ (45%) than those who do not (27%) say they received mental health care in the past 12 months. Similarly, eight in ten women who identify as having a mental health-related disability (81%) say they received mental health services, compared to 27% of women who identify as having another disability and 18% of women who do not identify as disabled.
Higher shares of women with lower incomes and those covered by Medicaid say they obtained mental health services compared to their higher income and privately insured counterparts. While mental health services can be very costly and private insurance coverage is often limited and associated with high out-of-pocket costs, Medicaid, a program designed for people with low incomes, typically has nominal or very low out-of-pocket costs for enrollees.
While use of mental health services is higher among many of the subpopulations that rate their mental health lower, still about half (48%) of women who rate their mental health as “fair” or “poor” say they obtained mental health care, suggesting that many women with “fair” or “poor” mental health who could benefit from care are not getting it. The survey also shows that mental health services are used by people across the mental health continuum. Three in ten (31%) women who rate their mental health as “good” and more than one in ten (13%) who describe it as “excellent” or “very good” say they received care in the past year.

When asked what kind of mental health services they received in the past 12 months, most women who say they received care say they received 1-on-1 care with a provider, either in-person (60%) or via telehealth (55%). About half of women who say they received mental health care in the past year report getting a prescription for a medication (52%).
Fewer than one in ten women who report receiving care (7%) say they received care through a mental health therapy app, like BetterHelp or Talkspace, which connect patients to a clinician for virtual appointments but outside of the traditional medical system, or through another avenue (8%) such as inpatient hospitalization or group therapy (Table 1).
The types of mental health services women use vary by demographics. While similar shares of women across all age groups say they received in-person 1-on-1 care with a provider, larger shares of women ages 26 to 35 compared to women ages 50 to 64 say they used digital services for care, such as telehealth services (59% vs. 49%, respectively) and care through a mental health therapy app (8% vs. 3%, respectively). One in ten women ages 18 to 25 who say they received care say they received care through a mental health therapy app. There were no statistically significant differences by age for prescription medications and other mental health services.
Among those who report receiving mental health services in the past year, nearly six in ten (59%) women who rate their mental health as “fair” or “poor” report receiving a prescription medication, as do half (50%) of women who describe their mental health as “good” and more than a third (37%) of those who rate it as “excellent/very good.”
Among those who report receiving mental health care, larger shares of women who identify as LGBT+ than those are not LGBT+ say they accessed mental health care through telehealth service (65% vs. 52%) or through a mental health therapy app (12% vs 6%). More women who identify as LGBT+ also say they received a prescription for a medication compared to their non-LGBT+ counterparts (60% vs. 50%).
Over half of women say they received more than one type of mental health service in the past 12 months (58%). Higher shares of women with “fair” or “poor” mental health (65%) and/or who identify as having a mental health-related disability (73%) say they received more than one type of service in the past year.

Coverage of Mental Health Services
While federal laws require parity for insurance coverage of mental health care, gaps in coverage remain. All state Medicaid programs provide coverage for mental health services for beneficiaries with low incomes, and the Affordable Care Act (ACA) requires most individual and small group insurance insurers to cover behavioral health care, which includes mental health services. However, the scope of coverage varies, provider networks are limited in many plans, and mental health providers may not accept all insurance plans or in some cases, any insurance.
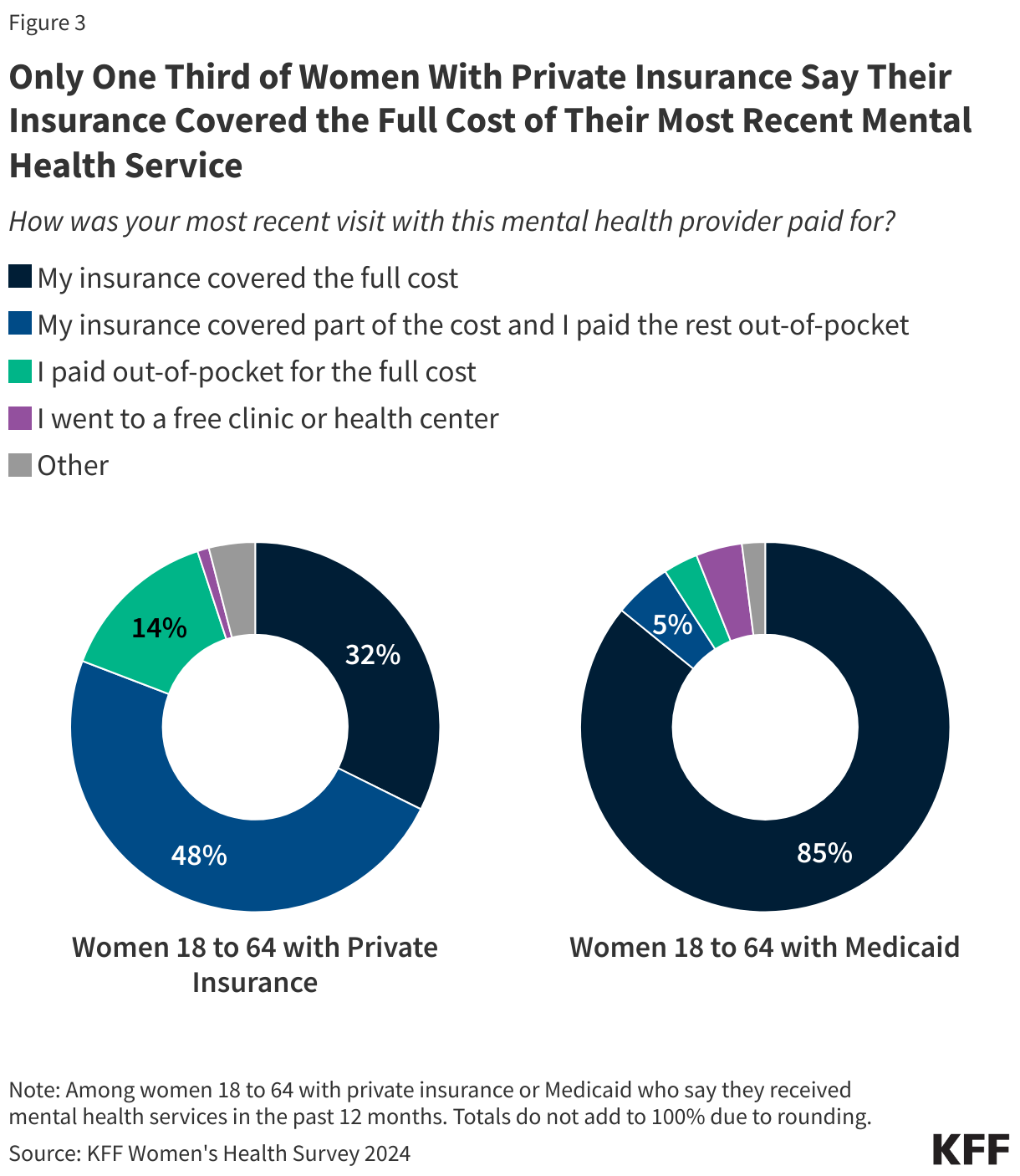
The large majority of women with Medicaid coverage who access care say their most recent visit was completely covered by Medicaid (85%) (Figure 3). Of the remaining 15%, 4% say they received free services at a clinic or health center. Medicaid is the single largest payer of behavioral health services, which includes mental health care and substance use services. By design, Medicaid charges very little cost-sharing.
Most women with private insurance say they had to pay at least some out-of-pocket costs for their most recent mental health care. Nearly half (48%) paid some of the cost out-of-pocket while their insurance covered part of the cost and 14% paid the full cost out-of-pocket. About one in three (32%) women with private insurance say their most recent visit was completely covered by their insurance plan.
Barriers to Accessing Mental Health Care
Overall, four in ten women (38%) say it is difficult to access mental health services in their state, but this share rises to half (49%) among women who say they recently received mental health care in the past year (Figure 4).

One in three women (32%) say they did not get mental health services in the past year even though they needed them (Figure 5). More than one third of women younger than 50 say they did not get the care they needed compared to 22% of women 50 to 64. Four in ten uninsured women (40%) say they needed mental health care but did not get it, compared to 31% of women with private insurance. Half of women who identify as LGBT+ (50%) say they needed mental health care but did not get it, compared to three in ten who do not identify as LGBT+ (29%). Similarly, nearly half of women with a mental health disability (47%) say they did not get mental health care even though they needed it. More than half of women with “fair” or “poor” mental health did not get the care they say they needed (55%).

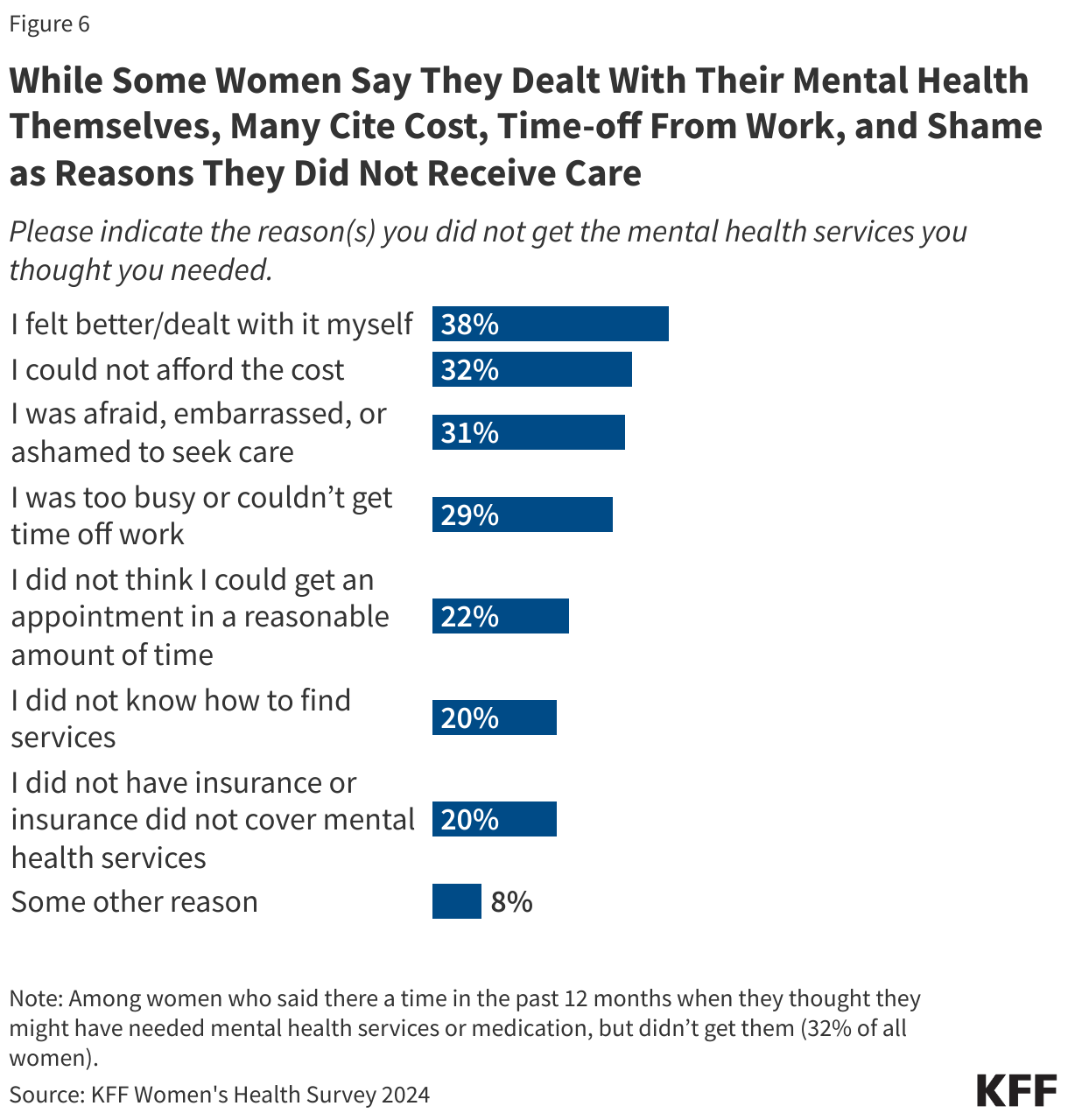
When asked to indicate the reason(s) why they did not get the care they needed, many women say they did not get care because they felt better or dealt with their mental health issues by themselves (38%) (Figure 6). However, three in ten women who say they did not get needed care cite cost (32%), being unable to take time off from work or being too busy (29%), or feeling afraid, embarrassed, or ashamed to seek care (31%). A small share of women cites some other reason (8%), such as transportation barriers or challenges with reaching providers to coordinate a visit.
It is not uncommon for those who receive care to also experience challenges while trying to find care. Among women who received mental health care in the past 12 months, more than half (55%) say they experienced a barrier during their care seeking journey (Figure 7). One in four women who say they received care say they had trouble finding a provider that was accepting new patients (25%) and about one in five had trouble finding a provider that accepted their insurance (21%). One in four women who received mental health care in the past year say they had trouble scheduling an appointment in a reasonable amount of time (24%).
There were few differences between women of different subgroup, with the exception of higher shares of LGBT+ women experienced challenges getting mental health services (66%) compared to 52% of women who do not identify as LGBT+, including trouble finding a provider, and affording the cost. These findings reflect well documented shortages, burnout, and high demand among clinicians in the mental health profession.

While only 5% of all women say they had difficulty finding a provider who spoke their language or one from a similar racial or ethnic background as themselves, these findings vary by race/ethnicity. Significantly larger shares of Hispanic (11%) and Black (8%) women report facing this challenge, compared to just 1% of White women (Figure 7). These findings are consistent with previous KFF polling, underscoring the additional and disproportionate challenges people of color face when accessing mental health care.

Cost continues to be a commonly reported barrier to mental health care. More than one in ten women 18 to 64 (13%) say they did not get mental health care or could not continue to afford the mental health care they were receiving because of cost (Figure 9). Thirteen percent (13%) of women with private insurance say they did not get care because of cost, and more than twice as many women without insurance (29%) cite cost as reason for not getting care. The share is lower among women with Medicaid, reflecting the program’s important role in providing access to mental health services, but still 8% cite cost as a barrier. The barriers are multi-pronged. Insurance networks can be very narrow for mental health care, and a significant portion of mental health clinicians do not participate in insurance networks. These findings on cost barriers underscore the ongoing challenges with affordable mental health care, especially among the uninsured, but even for those with coverage.
