Women’s Experiences with Intimate Partner Violence
Introduction
Intimate partner violence (IPV) is a persistent public health crisis that affects many women in the United States. IPV affects disproportionately affects women but also affects people of all genders. It has a wide range of negative effects on women’s physical and mental health, such as physical injuries, pregnancy complications, and substance use. IPV also has psychosocial impacts, affecting women’s safety, economic security and freedom, isolation, and ability to care for themselves and their children.
The 2024 KFF Women’s Health Survey provides data on women experiencing IPV in the past five years. This group includes women who said that in the past five years a current or former partner did at least one of the following: made them fear for their or their family’s safety, tried to control most or all of their daily activities, hurt them physically, forced them into sexual activity. However, this population does not include those who had experiences with IPV at earlier points in their lives or other forms of IPV and should not be used as an estimate of overall lifetime IPV prevalence Many women, particularly those who are older, may have experienced IPV prior to the last five years.
This analysis reports on a range of health topics affecting women who experienced IPV in the past five years, including their health care needs and use, barriers, and mental health. The impact on women who have been historically marginalized by society and health care systems, including those who are LGBTQ+, experience physical and mental disabilities, and those who are low-income is also examined. The survey was conducted from May 13 – June 18, 2024, online and by telephone among a nationally representative sample of 5,055 women ages 18 to 64.
Key Takeaways
- One in five (19%) women ages 18 to 64 say they have experienced intimate partner violence (IPV) in the last five years. Higher shares of women with lower incomes, LGBT+ women, and those who identify as disabled report recent IPV.
- Many women who have experienced IPV in the past five years contend with health challenges. Large shares characterize their physical (27%) and mental (46%) health as fair or poor. One in four say that a health condition keeps them from fully participating in work or other activities. Almost half of women who have experienced IPV in the past five years incurred a physical injury as a result.
- Over one in ten (14%) women who have experienced IPV in the past five years say that at some point they did not receive health care services they needed related to IPV. Privacy concerns, fear, and intimidation are leading reasons why people experiencing IPV do not obtain health care.
- There are differences in where women affected by IPV usually get health care. More than a third (35%) say their usual site of care is a clinic or health center. One in ten (9%) say it is the emergency room.
- IPV is a major concern during women’s reproductive years. Among women who experienced IPV in past five years, four in ten said they experienced violence during their most recent pregnancy or in the year before or after the pregnancy.
- Emergency contraception is an important back-up contraceptive for reproductive age women affected by IPV. One in five report using emergency contraception in the past year. One in ten also say they have obtained it since the Dobbs ruling in case they need it. These shares are approximately double the rates reported by women who have not experienced IPV in past five years.
Rates of IPV
One in five women ages 18 to 64 say they have experienced IPV in the past five years.
IPV presents in many forms, including physical, sexual, emotional, coercion, and online. The KFF Women’s Health Survey asked about a subset of IPV experiences that women have reported experiencing in the past five years. Approximately one in ten women say that in the past five years, a current or former partner has made them fear for their or their family’s safety (11%), tried to control most or all of their daily activities (11%), hurt them physically (9%), or forced them into sexual activity (9%) (Figure 1). In total, one in five (19%) women ages 18 to 64 said they have experienced at least one of these forms of IPV in the past five years.
Throughout this brief, this is the group referenced when discussing women who have experienced IPV.

Larger shares of women who are younger and have lower incomes consistently report experiencing IPV compared to those who are older and have higher incomes. Conversely, women who are Asian American or Pacific Islander report lower rates of IPV compared to women of other racial and ethnic groups. While women of all subpopulations experience IPV, rates are higher among some groups (Figure 2). More than one in four (27%) women who have lower incomes say they have experienced IPV in the past five years, about twice the share of those with higher incomes (14%). One in ten (9%) AAPI women report IPV in the past five years, which is lower than women of other racial/ethnic backgrounds.
One-third of women who are LGBT+ and one in four who identify as disabled report experiencing IPV in the past five years. Rates of all the IPV questions in the survey are higher among LGBT+ women compared to those who are not LGBT+ (Figure 2). Approximately one in five LGBT+ women said that in the past five years a current or former partner has made them fear for their or family’s safety (19%), tried to control most or all of their daily activities (20%), hurt them physically (18%), or forced them into sexual activity (18%). In total, twice as many LGBT+ women (32%) said they have experienced one of these forms of IPV in the past five years compared to non-LGBT+ women (16%). One in five women with a disability say they have feared for their or their family’s safety at the hands of a current or former partner (19%). Overall, one in four (27%) women who identifies as disabled reports experiencing at least one form of IPV in the past five years.

On average, women who have experienced IPV in the past five years have lower incomes and lower rates of private health insurance.
More than half (54%) of women affected by IPV in the past five years have low incomes, compared to one-third of those who have not (Figure 3). Insurance profiles also differ between women affected by IPV and those who have not, with a lower rate of private insurance coverage and higher rate of Medicaid coverage among those who have experienced IPV in the past five years compared to those who have not. Almost half (45%) of women who have experienced IPV in the past five years have young children, and half (54%) are not married. This is in part a reflection of the fact that many women experience IPV at young ages.

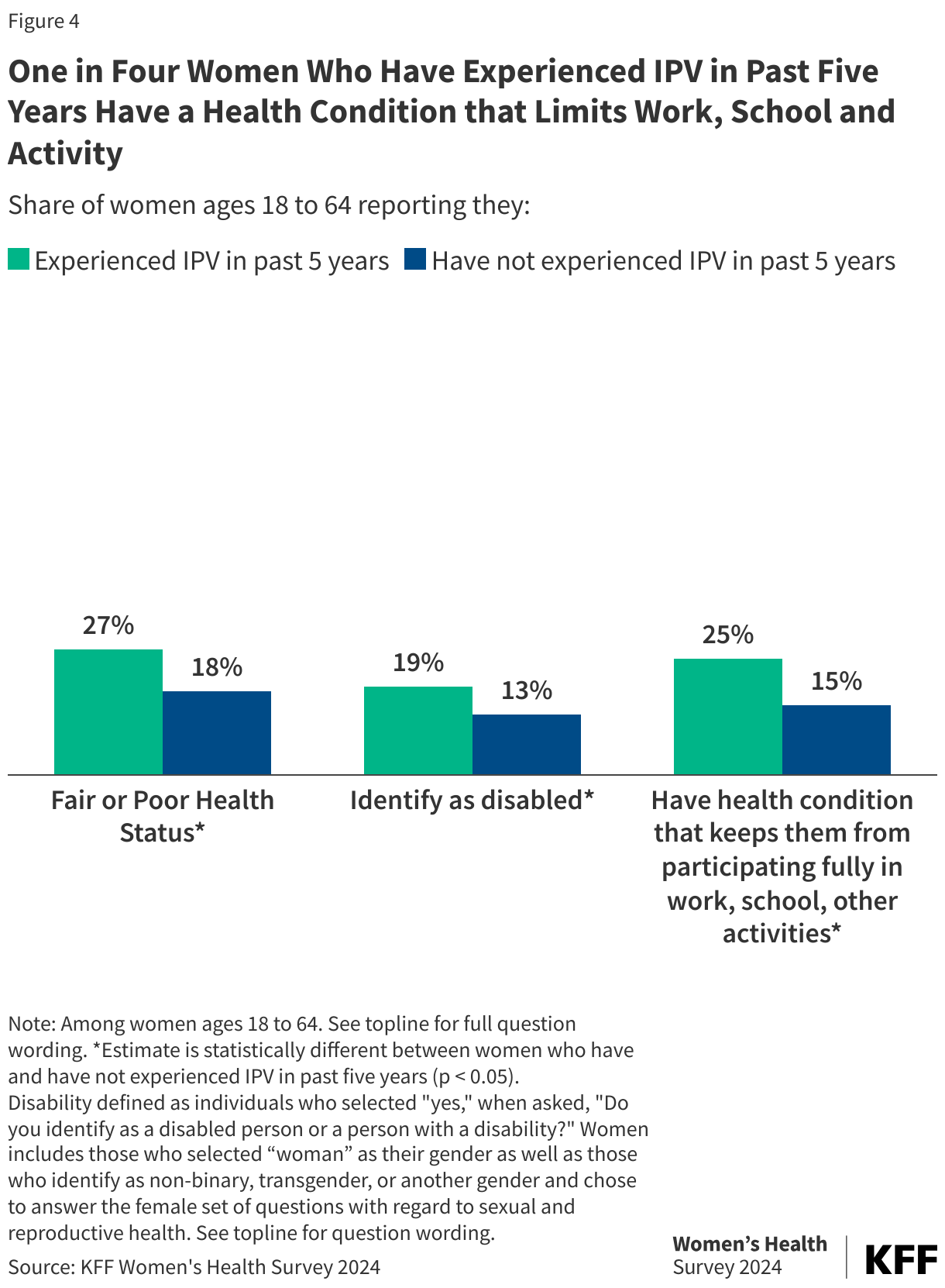
Women who have experienced IPV report higher rates of some health challenges, including disability and poorer health status. One in four women who have experienced IPV in the past five years rates their health as “fair” or “poor” (Figure 4). One in four (25%) also report having a chronic condition that keeps them from participating fully in work, school, or other activities. One in five (19%) say they identify as disabled. IPV may be a cause or contributor to these conditions or could exacerbate any of them.
Health Care Access and Barriers
Women who have experienced IPV in the past five years have heavier reliance on clinics and emergency rooms for their health care. Just under half (47%) of women who have experienced IPV in the past five years say they usually get health care in a private doctor’s office, whereas this is the site of care for the majority (62%) of those who have not experienced IPV recently (Figure 5). Three in ten (31%) women who have experienced IPV in the past five years say they usually obtain health care at a neighborhood clinic or health center, and one in ten (9%) usually get care at an emergency room. These differences in site of care may be driven by income, given that women who have experienced IPV are disproportionately lower-income.

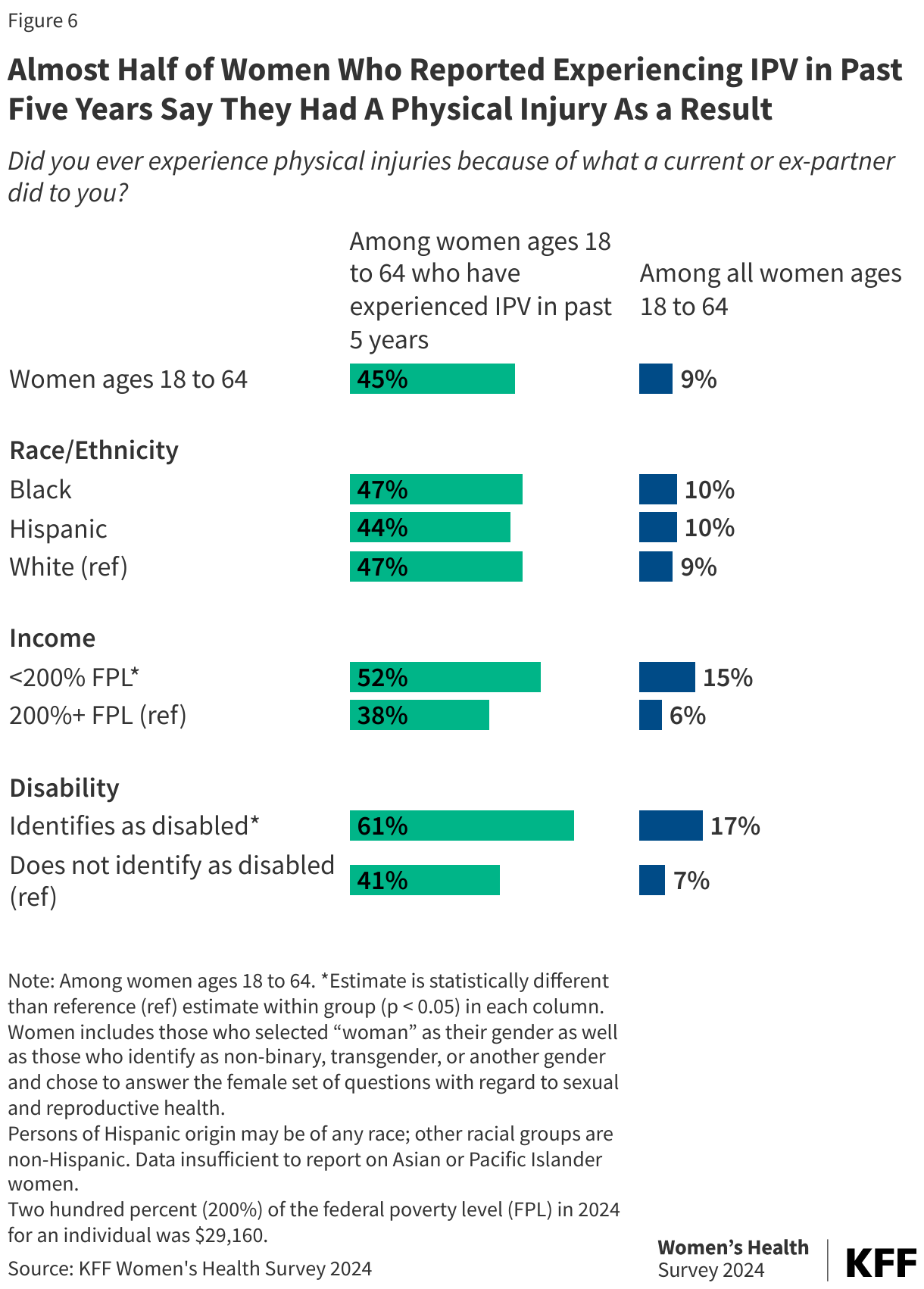
Almost half of women who have experienced IPV in the past five years incurred a physical injury as a result. Some of the most common injuries reported by people who experience IPV include head trauma, gynecologic conditions, and fractures. Overall, 45% of women who experienced IPV in the past five years say that their IPV experience resulted in physical injury, which translates to about one in ten (9%) among all women ages 18 to 64 (Figure 6). Among women who experienced IPV in the past five years, majorities of those who identify as having a disability (61%) and have lower incomes (52%) report having physical injuries from IPV. The shares are similar across White, Black, and Hispanic women.
Over one in ten (14%) women who have experienced IPV in the past five years did not receive health care services they needed. Women who experience IPV may need a wide range of health care services related to the impact of IPV. However, 14% of women who recently experienced IPV were not able to get medical or mental health care services related to IPV (Figure 7). Three in ten women say they needed health care services and did obtain them, and more than half (56%) of women who experienced IPV in the past five years say they did not need health services related to their IPV experience.

Privacy concerns, fear, and intimidation are leading reasons why women experiencing IPV do not get care. People who experience IPV are typically dealing with multiple, complicated circumstances that can affect whether, when, and if they can disclose IPV and seek and obtain care. Among women who experienced IPV in the past five years and did not receive care that they needed, nearly six in ten (58%) say it is because they did not want anyone to find out (Figure 8). For some, fear of retribution from a partner is too high to seek care. Almost four in ten (37%) women who did not receive care say they feared the police or child protective services would get involved. Prior research finds that some women affected by IPV report that involvement of police authorities can backfire on them because they lose care of their children or are accused of crimes they did not commit. Health system barriers affect women experiencing IPV too. Almost four in ten (38%) say they could not afford to get care and one in ten (12%) say services were unavailable, which may be tied to their higher rates of uninsurance. Medical billing practices can make confidentiality challenging as violent partners may get a hold of billing statements and patient records.

IPV and Mental Health Care
Violence, control, and coercion have severe negative effects on an individual’s mental health and well-being. IPV is associated with higher rates of depression, anxiety, and substance use. Mental health care has been identified as one of the essential health services needed for women affected by IPV.
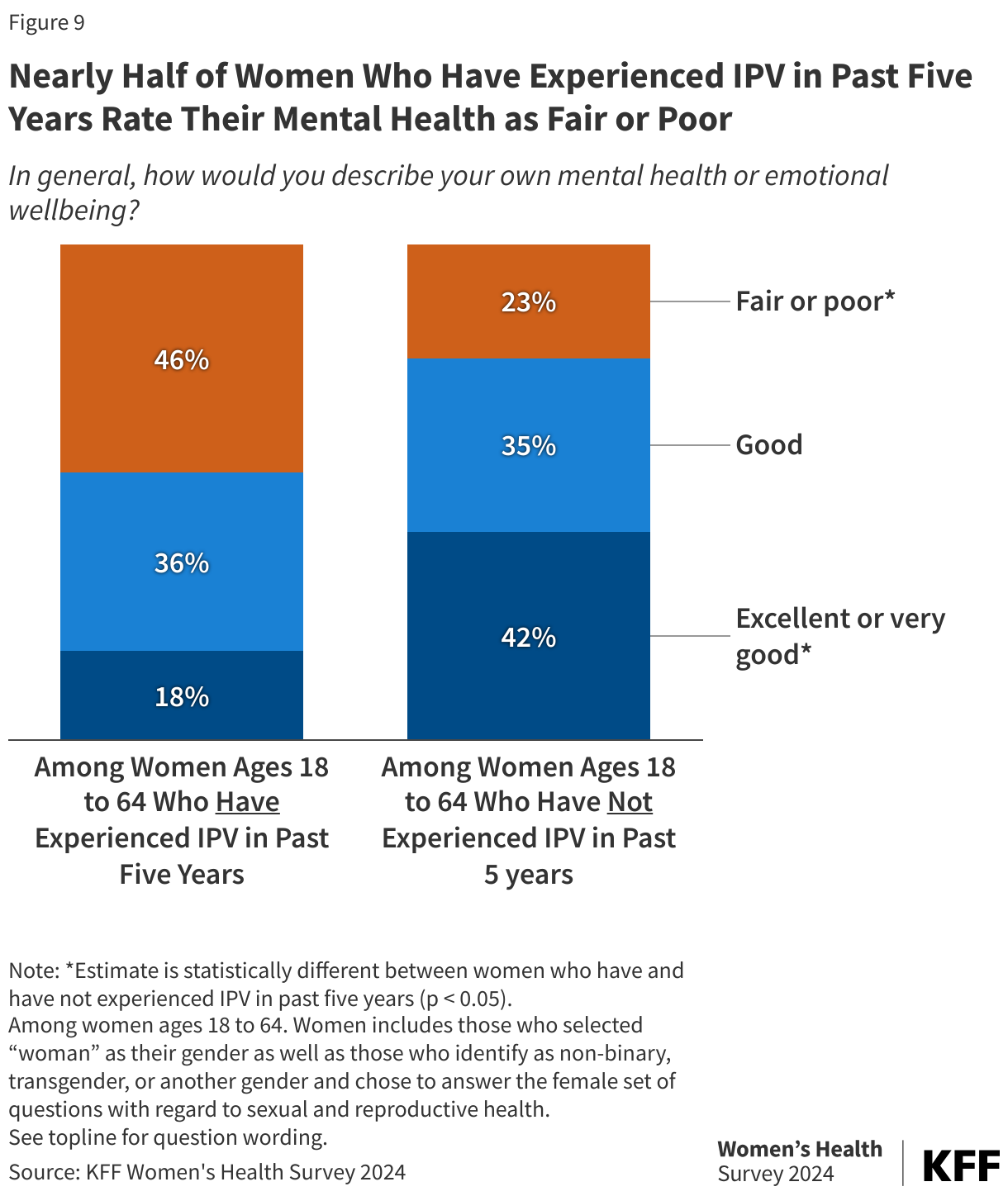
Women who have been affected by IPV in the past five years have poorer self-reported mental health status and emotional well-being than those who have not. Almost half (46%) of women who have experienced IPV in the past five years describe their mental health and emotional well-being as “fair” or “poor,” twice the share of those who have not (Figure 9). Conversely, 42% of women who have not been affected by IPV in the past five years describe their mental health as “excellent” or “very good,” over twice the share of women affected by IPV (18%). Just over one-third of each group rates their health as “good.”
Many women encounter barriers to mental health care, particularly those affected by IPV. Among women who have experienced IPV in the past five year who rate their health as fair or poor, two-thirds (66%) say that in the past year they did not obtain mental health care they thought they needed. This is also the case for half (50%) of women with fair or poor mental health who have not experienced IPV recently.
IPV and Reproductive Health
IPV often begins during women’s reproductive years, and research has documented associations between IPV and several sexual and reproductive health challenges, including higher risk for sexually transmitted infections, inconsistent use of contraception, and high rate of unplanned pregnancies.
Among reproductive age women who experienced IPV and were pregnant in the past five years, four in ten say they experienced violence around the time of pregnancy. Pregnancy can be a risky period for people experiencing IPV, as some people report that violence increases or intensifies during and after pregnancy. Experiences with IPV have been linked with greater risk for negative maternal and fetal health complications, including preterm birth, low birthweight, as well as maternal and fetal death in the most severe cases. Among women of reproductive age (18 to 49 years old) who were pregnant and experienced IPV in the past five years, one in five say they experienced IPV in the year prior to their last pregnancy (21%), during their most recent pregnancy (22%), and in the year after (20%). Overall, four in ten women of reproductive age who have experienced IPV say they experienced IPV during one of these periods (Figure 10).

Among women who were pregnant in the past five years, a higher share of those who also experienced IPV (65%) said they needed mental health services during or within the first year after pregnancy, compared to those who were not affected by IPV (44%).
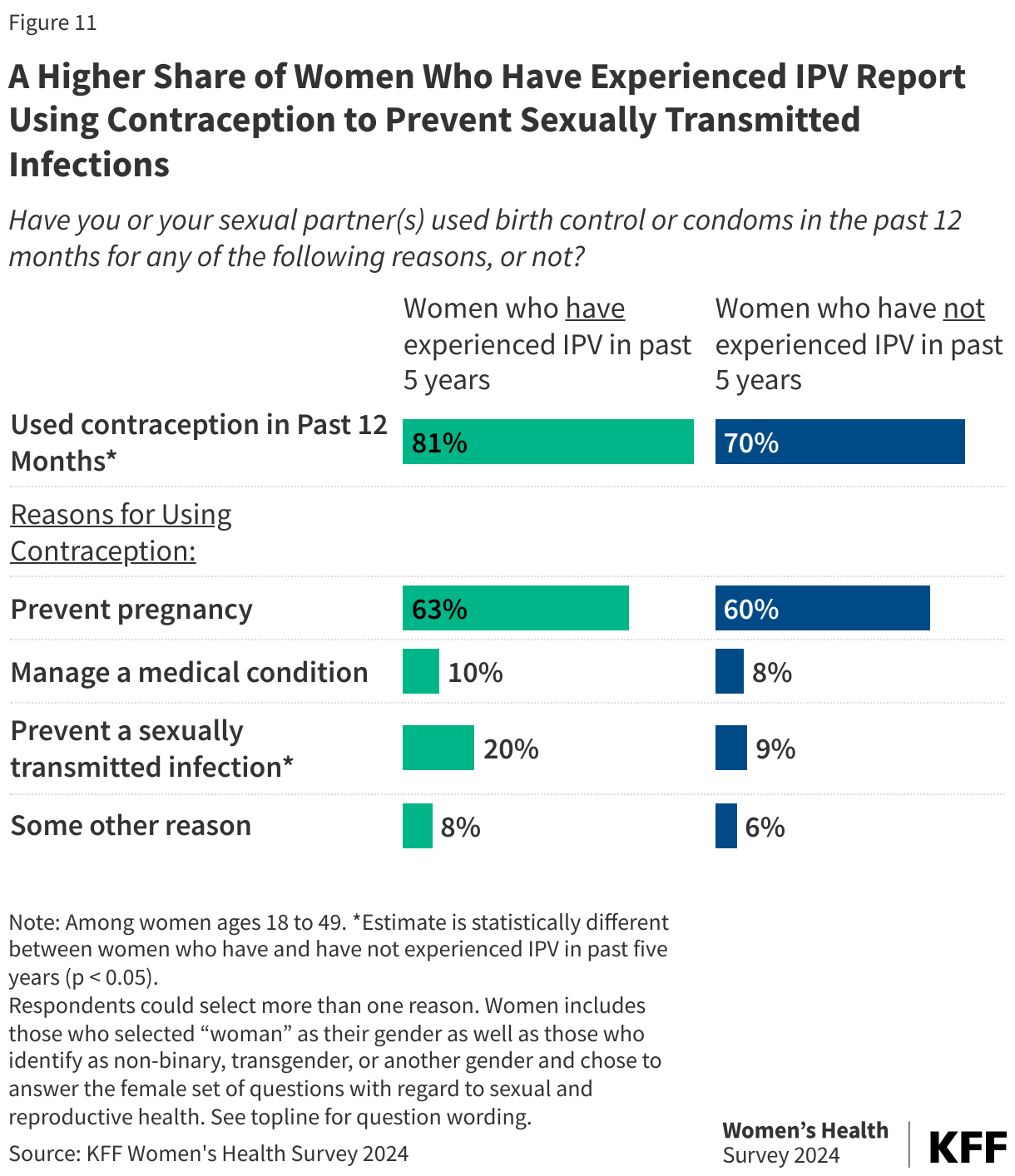
Eight in ten women of reproductive age who have experienced IPV in the past five years report using contraception in the past year. Preventing pregnancy is the leading reason for using contraception for this group, but one in five women who have experienced IPV in the past five years use it to prevent an STI.
The majority of reproductive age women who have experienced IPV, as well as those who have not, used contraception in the past year (Figure 11). For most contraceptive methods, rates of use are similar between women who have experienced IPV in the past five years and those who have not. However, more women affected by IPV report using condoms (38%, 33% respectively) and withdrawal (32%, 21%) compared to those not affected by IPV, which is surprising given that these methods are controlled by men. One in four women affected by IPV report they have had a sterilization procedure, one in five use IUDs and one in five say they used EC. One notable difference is why women use contraception. One in five women who have experienced IPV in the past five years say they use it to prevent an STI, twice the share among women who have not experienced IPV in the past five years (9%).
Reproductive coercion, control by an intimate partner over reproductive health issues such as use of contraception or an abortion, is also a form of IPV. More than one in ten (13%) women who have experienced other forms of IPV in the past five years also report that a partner has tried to stop them from using contraception so they would become pregnant against their will (data not shown).
One in four reproductive age women who have experienced IPV in past five years says they or their partner made a change in contraception practices because of the overturning of Roe v. Wade. Since the 2022 Supreme Court ruling that overturned Roe v. Wade, many states have banned or severely restricted abortion access, which has prompted some people to make changes in their use of contraception. Overall, nearly twice as many women affected by IPV (26%) say they’ve made a change than those who have not recently experienced IPV (14%). In particular, 10% of reproductive age women who have experienced IPV in the past five year has obtained EC to have on hand in case they need it. Almost one in ten (8%) report starting contraception or switching to a more effective method (Figure 12).
