Key Elements of the Biden Administration’s Proposed Title X Regulation
Issue Brief
Introduction
On April 15, 2021, the Department of Health and Human Services (HHS) published a notice of proposed rulemaking (NPRM) in the Federal Register entitled “Ensuring Access to Equitable, Affordable, Client-Centered, Quality Family Planning Services”, which proposed to replace the Trump Administration rules published on March 4, 2019. The Trump regulations made many programmatic changes to the Title X family planning program, notably adding restrictions to federal funding for abortion counseling and referral, as well as bans on federally-funded Title X sites from being co-located with abortion services. The Biden HHS is proposing to revise the Trump Administration rules by essentially re-instating prior regulations that are very similar to those that were in effect from 1993-2019 with several revisions that focus on “ensuring access to equitable, affordable, client-centered, quality family planning services” for all clients, especially for low-income clients. This brief provides an overview of the key elements of the Biden Administrations proposed regulations for the federal Title X family planning program.
Impact of the Trump Administration Title X Regulations
In the proposed rules, HHS outlines the substantial impact the Trump Administration regulations have had on the network over the time that the regulations have been in effect. The number of clients served by the program dropped from 3,939,749 clients in 2018 to 3,095,666 clients in 2019 (a 21% decrease), and then further decreased to 1,536,744 clients in 2020 which is a 60% decrease in clients served from 2018 (Figure 1). This dramatic drop is likely due to a combination of the impact of the pandemic with fewer people seeking care and the significant reduction in Title X sites serving clients due to the Trump Administration regulations.
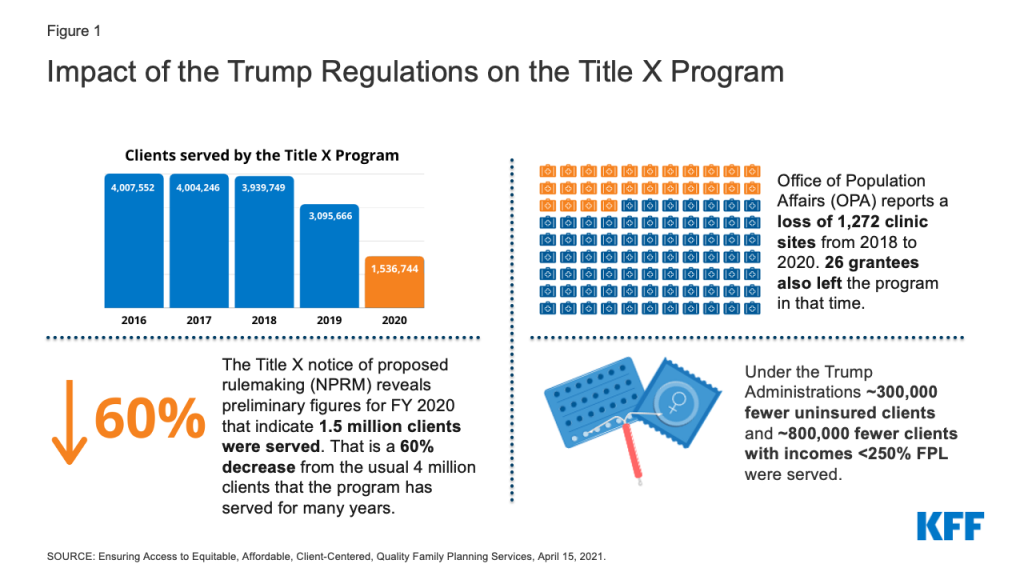
From 2018 to 2020, HHS reports a loss of 26 grantees (26%) who receive Title X funding and then distribute funds to the Title X clinic sites within their networks, as well as a loss of 1,272 clinic sites. There are currently six states without any Title X-funded services (HI, ME, OR, UT, VT, WA) and Office of Population Affairs (OPA) has been unable to find new grantees to fill most of the gaps that the Trump Administration rule created. There are an additional eight states that lost over half of their Title X network (AK, CT, IL, MA, MD, MN, NY, NH).
The Trump Administration regulations have had a substantial impact on low-income and uninsured clients that have relied on these services. Compared to 2018, there was a decrease in over 800,000 low-income clients (incomes < 250% of the Federal Poverty Level (FPL)) and over 300,000 uninsured clients. There has also been a substantial decrease in the number of sexual and reproductive health services provided from 2018 to 2019. There was a decrease of close to 400,000 women who received contraception through the Title X program from 2018 to 2019, about 300,000 fewer cancer screenings, and over one million fewer sexual transmitted infection (STI) tests.
Key Elements of the Biden Notice of Proposed Rule Making
1. Title X Clinics Will Be Able to Refer for Abortion Services and Have Co-located Abortion Services
The Biden HHS proposed Title X regulations are similar to the regulations that were in place from 1993 to 2019. They again allow Title X funded sites and providers to discuss and refer clients to abortion services when they wish to terminate a pregnancy and permit family planning services to be co-located with abortion services, but maintain the longstanding prohibition on the use of Title X funds to pay for abortions. The proposed regulations once again require, “upon request of the client, nondirective counseling and referral, regarding any option requested: (1) prenatal care and delivery; (2) infant care, foster care, or adoption; and (3) pregnancy termination.”
2. Quality Family Planning Guidelines Will Be Used as a Standard of Care
The proposed regulations will again base the standards of care for the Title X program on Providing Quality Family Planning Services (QFP) guidelines. They also incorporate several of the QFP’s recommendations into the regulations, including providing a range of Food and Drug Administration (FDA)- approved contraceptive methods onsite or a referral if necessary, using a client-centered approach to care provision and delivering high-quality care to all clients equitably. First published in 2014 by the Office of Population Affairs and the Centers for Disease Control (CDC), QFP recommendations are based on rigorous systematic reviews of the scientific evidence and reference other clinical guidelines from federal agencies and professional medical associations.
3. Contraceptive Services Include FDA-approved Contraceptives and Natural Family Planning
The proposed regulations revert to the previous definition of family planning services, which includes FDA-approved contraceptive services, and natural family planning services. The Trump Administration had dropped the requirement for “FDA-approved” and required a broad range of “acceptable and effective” family planning methods (including contraceptives, natural family planning or other fertility awareness-based methods).” This opened the path for organizations to qualify for federal Title X support even though they only offered a single method such as fertility awareness-based approaches or one, like abstinence, which is not an FDA-approved method. Ensuring that women have access to a broad range of FDA-approved contraceptive methods is significant because on average, women use 3.4 methods through their lifetime and women’s contraceptive preferences change across their reproductive years (Table 1).
4. Clinic Sites That Do Not Provide a Broad Range of Contraceptive Methods Must Provide Referrals to a Provider That Does
If a clinic does not provide a broad range of contraceptive methods or the method that a client seeks, referrals can assure access to their preferred method of contraception. In the proposed regulations, clinic sites that do not provide a broad range of contraceptive methods on-site must be able to provide clients with a referral to a provider who does offer the client’s method of choice. The regulations specify that the referral provided must not unduly limit access to the client’s method of choice, such as excessive distance or travel time to the referral location or referral to services that are cost-prohibitive for the client. Other Title X clinics and U.S. Health Resources & Services Administration (HRSA) Section 330-funded Federally Qualified Health Centers could both provide services on a sliding fee scale, but services at non-federally funded clinics or other sites may not be affordable without insurance or offered on a sliding scale. However, it is unclear in the proposed regulations whether this referral has to be another Title X-funded site, or if it can be outside of the Title X network, and if so, how the client will be able to afford that service or method.
The KFF Women’s Health Survey found that one in five women is not using their preferred method of contraception and this share is higher among uninsured (27%) and low-income women (25%) and women of color compared to white women (Figure 2). Among women who say they are not using their preferred method of contraception, a quarter of women say it is because they cannot afford it (Figure 3). Women using their preferred contraceptive method are more likely to consistently use their method and intend to continue using it compared to women not using their preferred method and Title X clinics can make contraception more affordable.
5. Clinic Sites Will Be Required to Assess Clients’ Family Income Before Determining Payment
One of the goals of the Title X program is to ensure cost is not a barrier to family planning services. The Title X program uses a sliding fee scale that bases the amount a client has to pay on their income. Clients with incomes at or below 100% of the Federal Poverty Level are not to be charged for their services, while clients with incomes between 101% and 250% FPL receive discounted services based on their ability to pay. Recognizing that a client’s income cannot always be verified, the proposed regulations state that charges can be based on the client’s self-reported income if verification is too burdensome. Clinics are still required to make efforts to bill third party payors for clients with coverage, regardless of their income.
A new addition to the proposed regulations specifically addresses insured clients whose family income is at or below 250% FPL and requires that they do not pay more (in copayments or additional fees) than what they would otherwise pay without insurance when the sliding fee scale is applied. This ensures that clients with insurance are not paying more than what they would pay without insurance for their family planning services. There is a sizable share of low-income women with insurance that still rely on these public programs (16%) to pay for their contraceptive care (Figure 4).
6. Advancing Health Equity as a Criterion for Awarding Grant Funds
Family planning care has a long history of inequitable care with people of color and low-income people disproportionately receiving coercive and non-client centered care. When asked to rate their contraceptive care provider on four items of client-centered contraceptive counseling — respecting me as a person, letting me say what mattered to me about my birth control, taking my preferences about my birth control seriously, and gave me enough information to make the best decision about my birth control — less than half of women and even smaller shares of Black and Hispanic women, low-income women, and uninsured women rated their contraceptive counseling as excellent on all four items (Figure 5).
In their 2011 report, the Institute of Medicine (now the National Academy of Medicine), defines quality health care as health care that is provided using a client-centered approach and is equitable, among other attributes. These attributes of quality care are added to the new proposed regulation with a specific focus on services that are client-centered, culturally and linguistically appropriate, inclusive, trauma-informed, and ensure equitable and quality service delivery. HHS is proposing to add the ability to advance health equity as a new criterion for awarding grant funds. These additions would help to ensure care is more equitable, particularly by incorporating the evidence-based Quality Family Planning Guidelines. However, it is unclear how all of these additions to the program will be actualized in the provision of care by clinics across grantee networks. There are few evidence-based tools for clinics to use to assess whether their provision of family planning services is culturally and linguistically appropriate, inclusive, trauma-informed, and equitable. However, this is one area where OPA could provide more guidance to clinics through program guidelines or through the development and dissemination of tools for assessing and implementing these attributes in family planning.
Rebuilding the Title X Network
The Biden HHS regulations were published on April 15, 2021, with a 30-day public comment period and public comments are due Monday, May 17, 2021. HHS will then address the public comments and issue a final regulation. Regulations usually become effective 60 days after publication of the Final Regulations, but the agency could make them effective sooner if it has good cause. Currently funded grantees could begin bringing clinic sites who have left the program back into their networks immediately after the effective date, but in order to receive new funds for services, grantees that left the Title X program will have to wait to apply to the program when the Funding Opportunity Announcement is released, which is anticipated in December 2021.
HHS estimates that it will likely take at least two years for program participation and clients served to reach previous numbers. This assumes that most of the service sites that withdrew from the Title X program have remained open and would be able to rejoin under the proposed rule. The pandemic plus the regulations resulted in significantly lower numbers of clients served in 2020 (~1.5 million clients). HHS anticipates that the number of clients would increase to about 3.2 million by 2022 and then by 2023 be back to the ~4 million clients the program has historically served (Figure 6). While the reduction in Title X funded sites and clients has been well documented, there is less known about whether clinics have had to close, reduce hours, or lay off staff. The pandemic has also significantly reshaped many elements of the health care delivery system from telemedicine to workforce that has also likely impacted the family planning network in the US. One aspect of the regulation that could make it easier for sites to expand their workforce is a change that acknowledges that consultation for medical services related to family planning can be provided by healthcare providers beyond physicians. Historically, the Title X regulations have required that all clients must have access to a consultation overseen by a physician. The proposed regulations expand the types of providers who can provide consultations for medical services related to family planning to include physician assistants and nurse practitioners, which could help with staffing and restructuring.
Grantees and Individuals with Conscience Objections
The preamble to the proposed regulations states that “individuals and grantees with conscience objections will not be required to follow the proposed rule’s requirements regarding abortion counseling and referral.” Although, this exemption predates the Trump regulations, the Trump Administration was the first to actively encourage faith-based organizations to apply to become grantees even if they included sites that limited their family planning offerings to abstinence and fertility awareness methods. However, the regulation does not specify how the Biden Administration will address this allowance to ensure that Title X clients receive all the family planning counseling and referrals they seek, especially when it comes to abortion care counseling and referrals. How will OPA ensure that clients who seek services from grantees with objections to abortion and certain methods of contraception have a choice to go to a provider that offers a full range of counseling and referrals? The regulation is also unclear regarding the responsibility of the grantees with conscience objections to providing some contraceptive methods to refer clients to another provider who offers these methods.
Looking Forward
HHS is accepting public comments on the proposed Title X regulations until May 17, 2021. Current and former Title X grantees and clinic sites and other interested parties can comment on how any of these changes will impact the provision of services to family planning clients. There are elements of the regulations that are ambiguous and inconsistent, and commenters are encouraged to ask for more clarification. HHS estimates that these new regulations will bring many of the previous grantees back into the Title X program that left due to restrictions on abortion referrals and the ban on co-location of abortion services. It is unknown, however, how many will return, and if so, how long it will take to restore the network. While the Biden Administration’s regulations will allow the program to operate largely under the same rules that it had been operating since 1993, unless Congress specifies otherwise, a future administration could again revise the regulations and reinstate the types of policies that triggered the dramatic reduction in the Title X network of providers and the sizable drop of federally funded family planning services across the nation.
Appendix
..