
Medicaid Reforms to Expand Coverage, Control Costs and Improve Care: Results from a 50-State Medicaid Budget Survey for State Fiscal Years 2015 and 2016
Executive Summary
Medicaid plays a significant role in the U.S. health care system, now providing health insurance coverage to more than one in five Americans. The Medicaid program continues to evolve, responding to changes in the economy, the broader health system, state budgets and policy priorities, and in recent years, to requirements and opportunities in the Affordable Care Act (ACA).
This report provides an in-depth examination of the changes taking place in Medicaid programs across the country. The findings in this report are drawn from the 15th annual budget survey of Medicaid officials in all 50 states and the District of Columbia conducted by the Kaiser Commission on Medicaid and the Uninsured and Health Management Associates (HMA), in collaboration with the National Association of Medicaid Directors. This report highlights policy changes implemented in state Medicaid programs in FY 2015 and those planned for implementation in FY 2016 based on information provided by the nation’s state Medicaid directors.
Policy changes and initiatives described in this report include those in eligibility and enrollment, managed care, delivery and payment system reforms, provider payment rates, and covered benefits (including prescription drug policies). The report also looks at the key issues and challenges now facing Medicaid programs.
Eligibility and enrollment changes in the ACA are continuing to have major policy implications for states in FY 2015 and FY 2016. As of October 2015, 31 states (including DC) had adopted the ACA Medicaid expansion. This includes 26 states that implemented the expansion in FY 2014, three additional states in FY 2015 (New Hampshire, Pennsylvania and Indiana) and two additional states in FY 2016 (Alaska and Montana). Other eligibility changes adopted or planned for states in FY 2015 and FY 2016 were small and targeted to a limited number of beneficiaries. As a result of new coverage pathways, a number of states are eliminating coverage for beneficiaries with incomes above 138 percent of poverty, many of whom qualify for Marketplace subsidies, as well as eligibility pathways to more limited Medicaid coverage. A few states had received or were seeking waivers to implement changes to premiums that were primarily related to the ACA coverage expansions (Arkansas, Indiana, Iowa, Michigan and Montana).
Under the ACA, all states were required to implement enrollment changes including new streamlined application, enrollment, and renewal processes for individuals. Many states adopted new eligibility and enrollment systems. A number of states were still working through challenges in processing renewals at the start of FY 2016.
States remain focused on strategies and initiatives to improve the effectiveness and outcomes of care, and to slow the growth in the cost of care. As of July 2015, a total of 48 states used some form of managed care to serve the Medicaid population, including 39 states (including DC) that contracted with risk-based managed care organizations (MCOs) to serve their Medicaid enrollees. In 21 of these states, at least 75 percent of all Medicaid beneficiaries were enrolled in MCOs. In FYs 2015 and 2016, the trend toward increased use of MCOs continues, as five states (Florida, Indiana, Iowa, Louisiana and Rhode Island) end their primary care case management (PCCM) programs and transition populations to MCOs. Other states are moving more eligibility groups, geographic areas and benefits into MCOs. As more states rely on MCOs for acute physical health care, a growing number of states are focusing on integration of physical health, behavioral health and long-term services and supports (LTSS) under the umbrella of managed care as a priority policy direction.
With greater utilization of MCOs has come greater focus on quality performance. For FY 2015, a total of 21 states implemented new or expanded quality initiatives and 19 states planned to do so in FY 2016. (ES 1) These include MCO report cards and greater reporting of quality metrics, pay for performance, capitation withholds, performance bonuses or penalties, and special quality initiatives and performance improvement projects.
States are implementing and expanding alternative delivery system and payment models. Thirty-seven (37) states in either FY 2015 or FY 2016, including 27 states in FY 2015 and 28 states in FY 2016, reported adopting or expanding one or more initiatives that seek to control costs, reward quality and encourage integrated care. (ES 1) Initiatives include patient-centered medical homes (PCMHs), Health Homes, Accountable Care Organizations (ACOs) as well as other initiatives to coordinate physical and behavioral health care and better manage the care of persons with multiple chronic conditions. Nearly a quarter of states are implementing initiatives in FY 2015 or FY 2016 to coordinate care and financing for dually-eligible Medicare-Medicaid beneficiaries. A limited number of states are implementing episode of care and DSRIP initiatives.
States are implementing policies designed to “re-balance” care to allow more individuals to live in their homes and in the community. Nearly every state (46 states in both FY 2015 and FY 2016) took steps to expand care in the home and community. The ACA included some LTSS-related options intended to promote LTSS rebalancing including the Community First Choice Option and the 1915(i) HCBS State Plan Option. Thirteen (13) states reported having one or both of these options in place in FY 2014; an additional six states implemented at least one of these options in FY 2015 and eight states planned to do so in FY 2016.
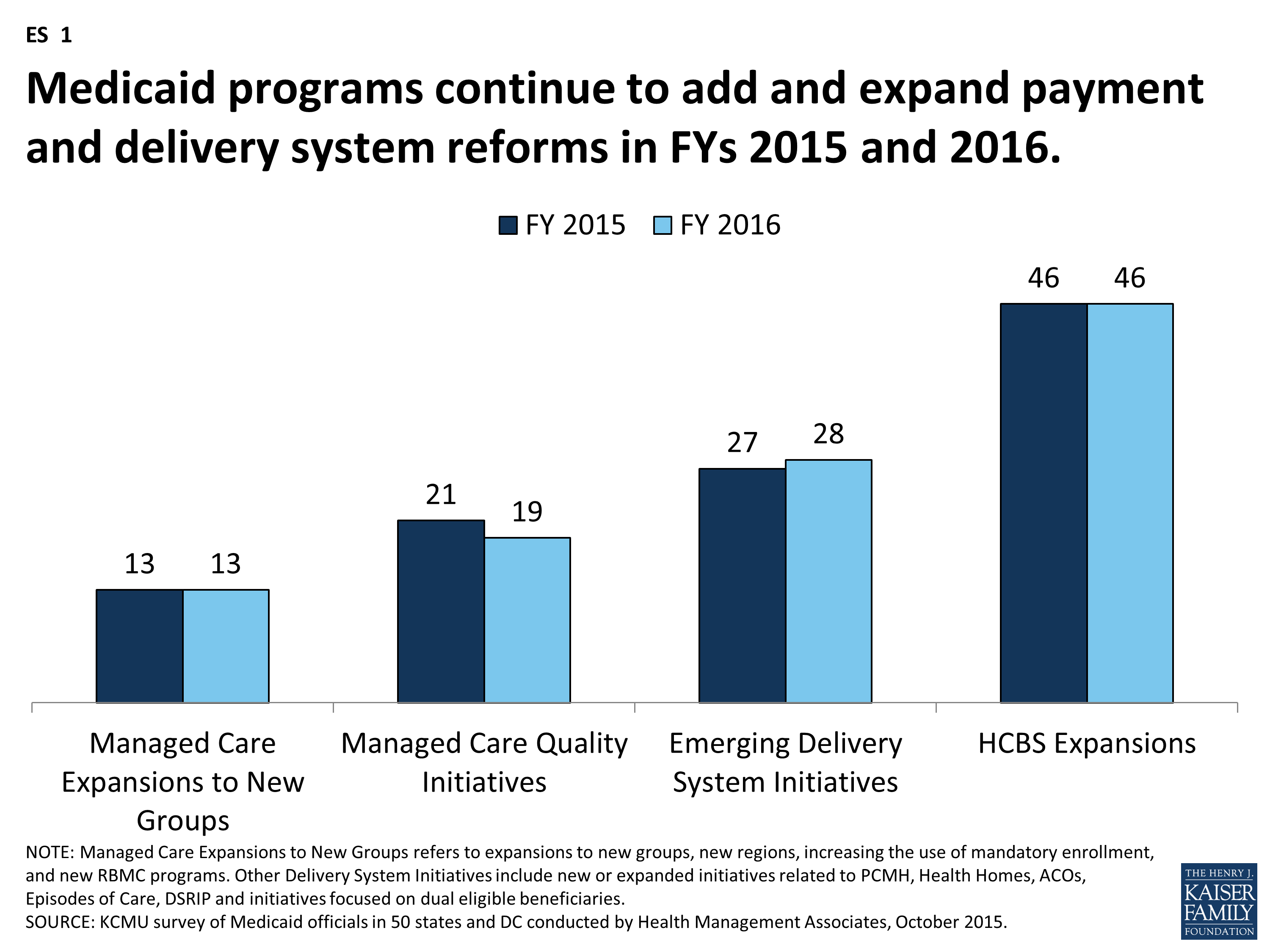
Figure ES-1: Medicaid programs continue to add and expand payment and delivery system reforms in FYs 2015 and 2016.
Given the size of Medicaid in state budgets, there is always pressure to control costs; however, improvements in the economy have allowed states to adopt more increases in reimbursement rates and benefits compared to restrictions. Medicaid provider payment rates and benefits are often adjusted in response to changes in the economy, with restrictions in times of economic downturns and state budget shortfalls, and restorations or enhancements when the economy and state revenues improve. In FY 2015 and FY 2016, more states implemented or planned for rate increases compared to restrictions (47 and 45 states increasing compared to 35 and 38 states restricting rates in those years). In this survey, a number of states reported that they have or are adopting reimbursement policies to reduce potentially preventable hospital readmissions and early elective deliveries.
All states (except Alaska) use at least one provider tax or fee to help finance Medicaid. Eighteen (18) states increased or planned to increase one or more provider taxes or fees in FYs 2015 and 2016. Seven (7) of the Medicaid expansion states (Arizona, California, Colorado, Indiana, Kentucky, Nevada and Ohio) reported plans to use increased provider taxes or fees to fund all or part of the costs of the ACA Medicaid expansion beginning in January 2017, when states must pay a small share of the costs of the expansion.
A total of 24 states expanded or enhanced covered benefits in FY 2015, and 18 states planned expansions in FY 2016. The most common benefit enhancements reported were for behavioral health and substance abuse services, HCBS and dental services for adults. Far fewer states reported benefit restrictions.
States have a renewed focus on controlling rising prescription drug costs. Since 2014, rising drug prices and increasing program costs have refocused state attention on pharmacy reimbursement and coverage policies. The majority of states identified high-cost and specialty drugs (e.g., hepatitis C antivirals among others) as a significant cost driver for state Medicaid programs as well as increased costs for generics among other factors. Over two-thirds of the states in FY 2015 and half in FY 2016 reported actions to refine and enhance their pharmacy programs in response to new and emerging specialty and high-cost drug therapies.
Medicaid directors reported a number of key priorities in FY 2016 and beyond. Medicaid is a large and complex program that provides health coverage for an increasing share of the population in each state. As the program continues to evolve, the key priorities for most directors are around implementing the ACA coverage provisions, controlling costs, implementing an array of complex delivery system reforms, and standing up new systems to support program operations related to enrollment, claims processing and delivery system reforms. Tackling this magnitude of change is a significant challenge, particularly given that most state Medicaid programs are operating within constrained resources, both in terms of staff and funding. Emerging priorities mentioned by Medicaid directors include population health and social determinants of health. (ES 2) State Medicaid programs are looking for opportunities to leverage other resources and stakeholders (such as state public health agencies and other payers) to improve the quality of care provided and ultimately affect health outcomes for the populations they serve. Pursuing these significant goals has caused Medicaid to evolve into a major player in transforming the overall health care system.
Figure ES-2: Medicaid directors reported many key priorities for FY 2016 and beyond.
Report
Introduction
This report provides an in-depth examination of the reforms, policy changes and initiatives taking place in state Medicaid programs across the country. The findings in this report are drawn from the 15th annual budget survey of Medicaid officials in all 50 states and the District of Columbia conducted by the Kaiser Commission on Medicaid and the Uninsured (KCMU) and Health Management Associates (HMA), in collaboration with the National Association of Medicaid Directors. This was the fifteenth annual survey, which has been conducted at the beginning of each state fiscal year from FY 2002 through FY 2016.1 (Copies of previous reports are archived here.)
The KCMU/HMA Medicaid survey on which this report is based was conducted from June through August 2015. Medicaid directors and staff provided data for this report in response to a written survey and a follow-up telephone interview. All 50 states and DC completed surveys and participated in telephone interview discussions between June and August 2015. The survey asked state officials to describe policy initiatives and changes that occurred in FY 2015 and those adopted for implementation for FY 2016 (which began for most states on July 1, 20152). The survey does not attempt to catalog all Medicaid policies. Experience has shown that adopted policies are sometimes delayed or not implemented for reasons related to legal, fiscal, administrative, systems or political considerations, or due to delays in approval from CMS. Not included in the survey are policy changes under consideration where a definite decision on implementation has not yet been made. A copy of the survey instrument is located in the appendix of this report.
Key findings of this survey, along with 50-state tables providing more detailed information, are described in the following sections of this report:
- Eligibility, Enrollment, Premiums and Cost-Sharing
- Managed Care Reforms
- Emerging Delivery System and Payment Reforms
- Long-Term Services and Supports
- Provider Rates, Taxes and Benefits
- Priorities for FY 2016 and Beyond Reported by Medicaid Directors
Eligibility, Enrollment, Premiums and Cost-Sharing
| Key Section Findings |
Tables 2, 3 and 4 at the end of this section include additional details on eligibility, premiums and cost-sharing policy changes in FYs 2015 and 2016. These tables are also available in a downloadable PDF. |
Changes to Eligibility Standards
The ACA included a number of significant changes to Medicaid eligibility and enrollment policies. One of the most significant changes was to extend Medicaid coverage to nearly all non-elderly adults with incomes up to 138 percent of the federal poverty level (FPL) ($16,242 per year for an individual in 2015), ending the historic exclusion of adults without dependent children, or childless adults, from the program. However, the June 2012 Supreme Court ruling on the constitutionality of the ACA effectively made the Medicaid expansion optional for states. Regardless of whether states implement the Medicaid expansion, all states were required to implement a range of other changes to eligibility and enrollment under the ACA. These changes included transitioning to use of Modified Adjusted Gross Income (MAGI) to determine financial eligibility for children, pregnant women, parents and low-income adults; eliminating asset limits for these same groups; establishing a new minimum eligibility limit of 138 percent FPL for children in Medicaid, which resulted in the transition of older children from the Children’s Health Insurance Program (CHIP) to Medicaid in some states; and providing new streamlined application, enrollment, and renewal processes for individuals. In addition, Medicaid agencies must coordinate eligibility determination and enrollment processes with the new Marketplaces. Altogether, the eligibility changes in 2014 represent historic program changes. Most of these changes occurred in FY 2014. As a result, very few changes in eligibility standards occurred for FY 2015 and FY 2016.
As of October 2015, 31 states (including DC) had adopted the Medicaid expansion. (Figure 1) In Utah, discussions continue about implementing the Medicaid expansion, and other states may re-visit the decision in the next legislative session. Most states that have adopted the ACA Medicaid expansion did so in FY 2014 (26 states). In FY 2015, three additional states adopted the ACA Medicaid expansion (Indiana, New Hampshire and Pennsylvania.) In FY 2016, two states to date have adopted the ACA Medicaid expansion; Alaska implemented in September 2015, and Montana plans to implement in January 2016 pending federal waiver approval.
Other eligibility changes in FY 2015 and FY 2016 were limited and targeted to small numbers of beneficiaries. For FY 2015, a total of eleven states made changes that expanded Medicaid eligibility and for FY 2016, five states plan to implement Medicaid eligibility expansions. (Figure 2) Only one state in FY 2015 and three states in FY 2016 made or are planning eligibility restrictions that were likely to leave individuals without other coverage options. A number of states are making changes to existing Medicaid eligibility pathways due to the availability of new coverage options; these changes are not counted as restrictions or expansions in this report.
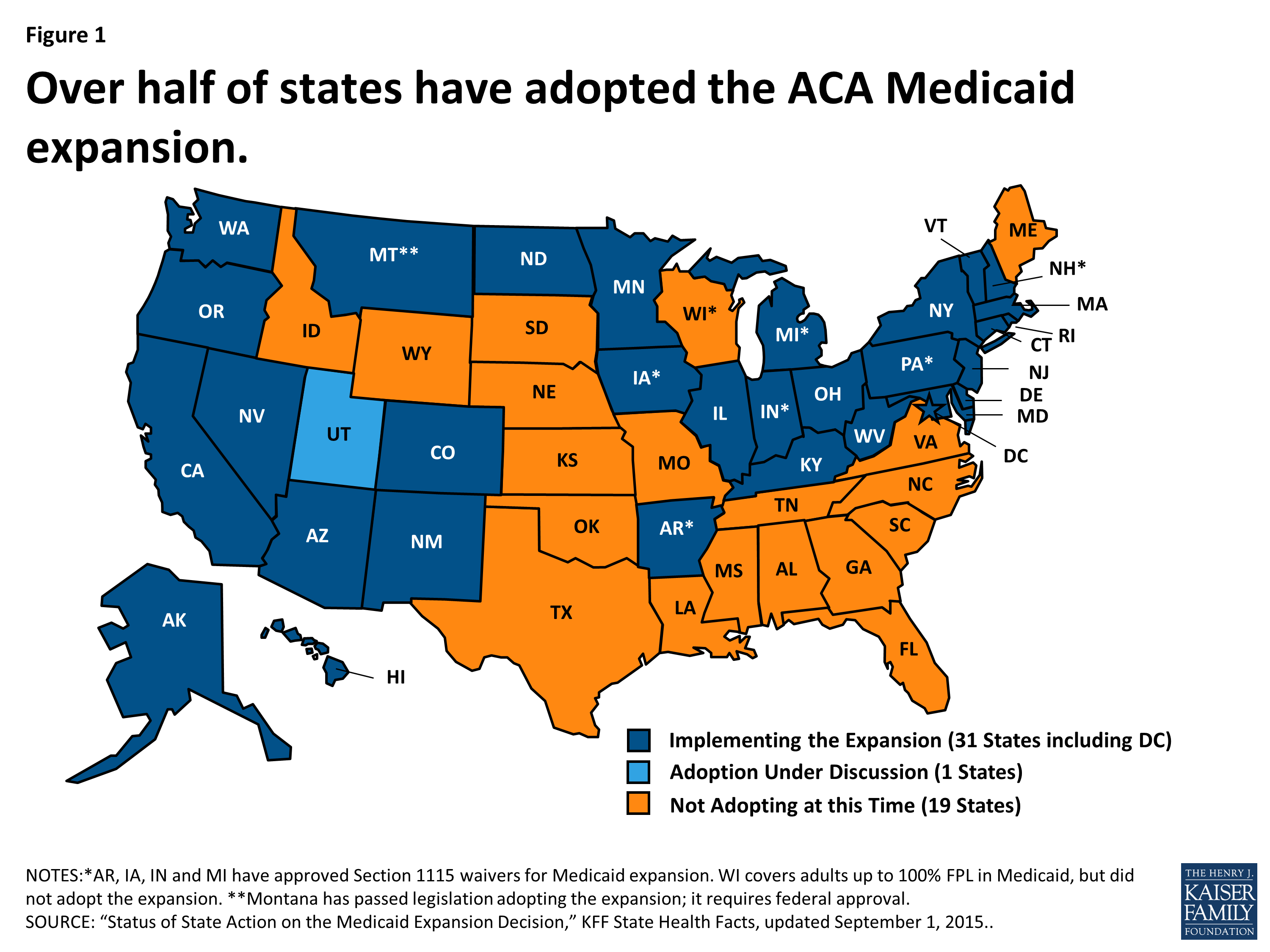
Figure 1: Over half of states have adopted the ACA Medicaid expansion.
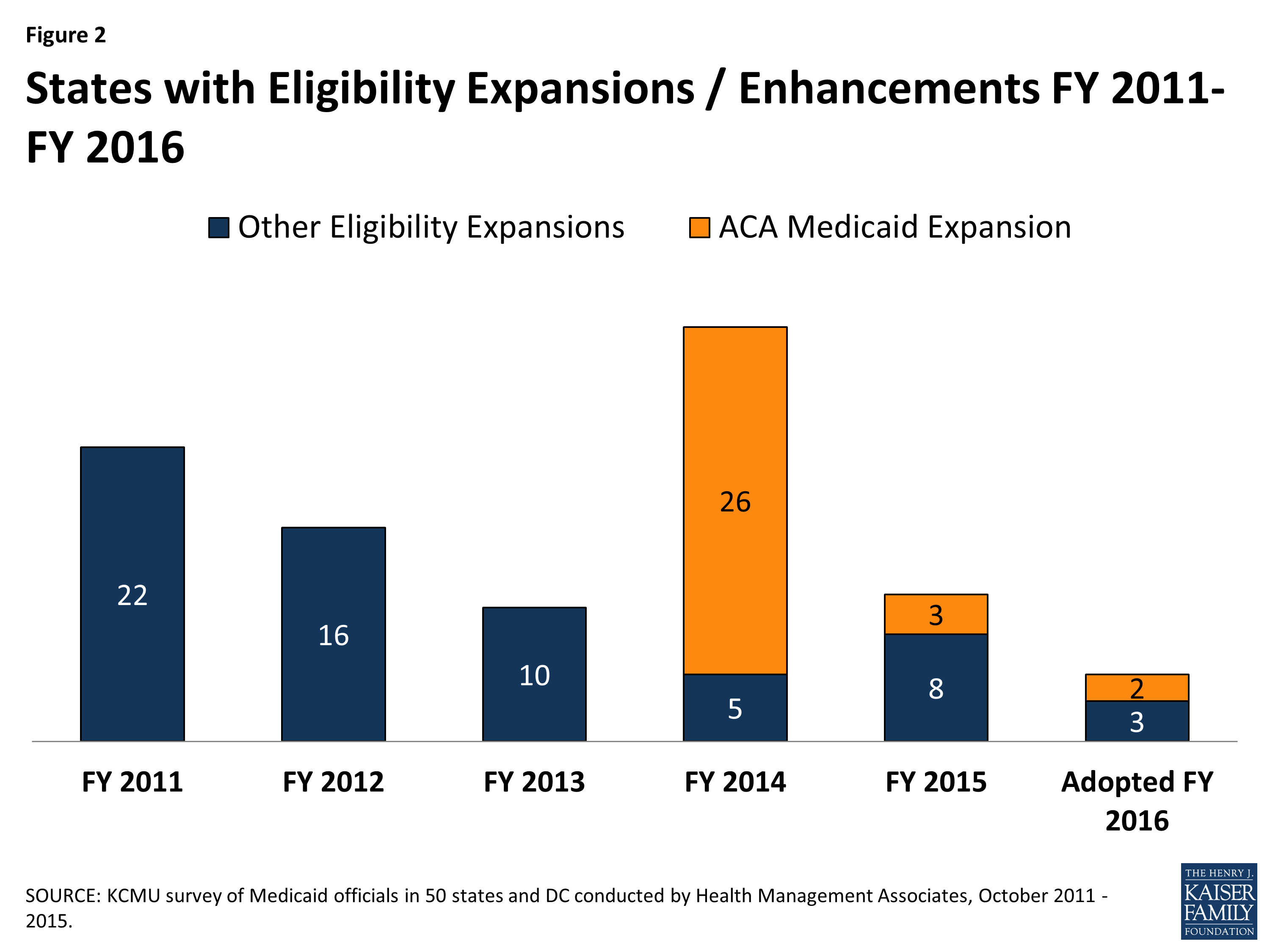
Figure 2: States with Eligibility Expansions / Enhancements FY 2011-FY 2016
Coverage Transitions
As reported last year, with more coverage options available across the income spectrum, some states made changes to existing Medicaid pathways. These changes are discussed below and are noted in Tables 2 and 3 as “(#)” meaning they are not counted as a positive or negative eligibility change.
Medicaid expansion states reducing eligibility for adults over 138 percent FPL. Both Minnesota and New York previously covered adults with incomes above traditional Medicaid eligibility levels through Medicaid waiver programs but have transferred those groups to their Basic Health Plans, discussed below. In addition, Connecticut reported plans to reduce Medicaid parent eligibility levels to 150 percent FPL in FY 2016; many parents previously eligible at the higher levels should be eligible for Marketplace subsidies.
| Basic Health Plan |
New York and Minnesota both implemented a Basic Health Plan (BHP) in FY 2015. Under the BHP provisions of the ACA, a state receives 95 percent of what the federal government would have spent on premium and cost-sharing subsidies in the Marketplace for the eligible population. The state then provides coverage through a state-managed BHP. While the BHP is not part of Medicaid, it affected Medicaid in these states.
|
States reducing or eliminating optional and limited Medicaid eligibility pathways. With new coverage options available either through the Medicaid expansion or the Marketplace, states have new options about how they treat some existing eligibility pathways for more limited Medicaid coverage, such as pregnancy related coverage, family planning-only programs, some spend-down programs, and the Breast and Cervical Cancer Treatment (BCCT) program.2 Prior to the implementation of the major ACA coverage changes, it was not clear if states would eliminate or scale back some of these programs in response to the new coverage options. While most states reported no current plans to change such pathways, many states indicated that enrollment in these groups has declined as more individuals are eligible under the adult Medicaid expansion group. However, a few states did note eligibility changes. (Table 1) In these cases, states generally plan to not allow new enrollment through these pathways but will continue coverage for those already enrolled.
| Table 1: States Eliminating Coverage for Optional and Limited Medicaid Eligibility Pathways | ||
| Program | In Place in 2013 (Prior to the ACA) | Eliminated or Plans to Eliminate |
| Breast and Cervical Cancer Treatment | 51 | Arkansas and Maryland (FY 2014), Illinois (FY 2016) |
| Medically Needy / Spend Down Adults | 36 | Hawaii and Illinois (FY 2014); Pennsylvania1 (FY 2015) |
| Pregnant Women Coverage > 138% FPL | 43 | Louisiana2 (FY 2014) |
| Family Planning Waivers or State Plan | 33 | Arizona, Arkansas, Delaware, Louisiana3 and Michigan4 (FY 2014); Illinois (FY 2015); Ohio and Pennsylvania5 (FY 2016) |
|
NOTES:
1 Pennsylvania eliminated spend-down for the disabled only; it is reinstating this coverage in FY 2016.
2 Louisiana reported that pregnant women with income above 133% FPL were eligible for coverage under CHIP. 3 Louisiana converted its family planning waiver to a SPA, but eligibility declined to 133% FPL. 4 Michigan closed its family planning waiver to new enrollment in April 2014. 5 Pennsylvania is converting its family planning wavier to a SPA but is no longer accepting new enrollment. |
||
Other Eligibility Changes
Other eligibility changes were more targeted or limited. These changes are noted in Table 2, but a few include:
- In FY 2016, Colorado is implementing the option to eliminate the five-year bar on Medicaid eligibility for lawfully-residing immigrant children.
- In FY 2015, Montana increased the cap on enrollment in its Mental Health Services Plan (MHSP) waiver from 2,000 to 6,000 adults with serious mental illness (before the state adopted the Medicaid expansion).
- Virginia implemented a Section 1115 waiver to provide limited benefits to some uninsured adults with serious mental illness as part of the Governor’s Action Plan in FY 2015. (State legislation later reduced eligibility for this waiver from 100 percent FPL to 60 percent FPL, effective July 1, 2015.)
- A number of states made changes to increase eligibility for the aged, blind and individuals with disabilities including eliminating the asset test (Vermont in FY 2015)and increasing income and asset limits for working individuals with disabilities (Virginia, New Jersey, Florida and Michigan).
Only one state in FY 2015 (Wisconsin) and three states in FY 2016 (Ohio, Tennessee and Virginia) made or plan to make eligibility restrictions that are likely to leave individuals without other coverage options. These are targeted restrictions that would affect small groups of beneficiaries.
In addition, California mentioned plans in FY 2016 to extend coverage to all undocumented children. This is a state-funded initiative and not funded through Medicaid; therefore, it is not counted as a Medicaid policy change in this report.
Enrollment Policies and Changes
Renewals
As of January 1, 2014, new streamlined renewal policies for Medicaid also went into effect under the ACA. However, many states were delayed in implementing new renewal procedures. Recognizing this delay, during 2014, CMS allowed states to suspend renewals for existing enrollees for specified periods of time in order to free up staff resources to process new applicants and continue to update eligibility systems to implement new streamlined renewal procedures based on MAGI rules. States were asked if, at the time of the survey, they were experiencing challenges processing MAGI-based renewals and to describe those challenges.
A number of states reported that they were experiencing challenges processing MAGI-based renewals at the time of the survey. Most of the issues reported were related to new eligibility systems, high volume of renewals, challenges matching data, and issues with pre-populated renewal forms. Most of these challenges were seen as temporary issues, but were not yet fully resolved in some states at the start of FY 2016.
Hospital Presumptive Eligibility (HPE)
Starting in January 2014, the ACA allowed qualified hospitals to make Medicaid presumptive eligibility determinations. States were asked to describe the level of participation among hospitals in their states. Thirty-three (33) states reported that they have implemented HPE and have at least one hospital participating in the initiative; the remaining states noted that either they were still working to implement HPE or that no hospitals had signed up to participate at the time of the survey.
Premiums and Cost-Sharing
In July 2013, CMS released final rules designed to streamline and simplify regulations around Medicaid premiums and cost-sharing, consolidate existing law and provide for individual market premium assistance. Under the new rules, CMS clarified that total Medicaid premiums and cost-sharing incurred by all individuals in a Medicaid household may not exceed an aggregate limit of five percent of the family’s income, applied on either a quarterly or monthly basis. To enforce this, the new rules also extended the requirement that states track aggregate premiums and cost-sharing and suspend such payments if the household reached the five percent cap.3 In this year’s survey, several states commented on the difficulty of implementing a process to track these limits. In some cases, this has resulted in delays or reversals of plans to increase beneficiary cost-sharing.
Premiums
With certain exceptions, Medicaid generally is not allowed to charge premiums to Medicaid beneficiaries with incomes at or below 150 percent FPL, although in limited cases certain populations may be charged premiums (sometimes referred to as “buy-in” programs) including: working individuals with disabilities eligible under the Ticket to Work and Work Incentives Improvement Act (TWWIIA) and children with disabilities in families with incomes that otherwise exceed Medicaid limits eligible under the Family Opportunity Act (FOA). States are also permitted under certain circumstances to impose premiums on parents receiving Transitional Medical Assistance (TMA) coverage. Prior to the ACA Medicaid expansion, a number of states also received Section 1115 waiver authority to expand coverage to higher income groups who were not otherwise eligible for Medicaid and to subject them to a premium requirement. Under the ACA, a few states have received federal waivers to impose premiums on their Medicaid expansion populations.
In this year’s survey, states identified very few changes to premiums. Six states reported premium changes, including some with multiple changes. Five states made or proposed changes related to ACA coverage expansions (Arkansas, Indiana, Iowa, Michigan and Montana) and are described following the next section. Two states (Michigan and Minnesota) increased premiums for working individuals with disabilities.4
Copayment Requirements
Most state Medicaid programs require beneficiary copayments, but to varying degrees. Six states reported new copayment requirements in either FY 2015 or FY 2016; each of these states reported new copayment requirements for their Medicaid expansion populations. Indiana reported new copayments in FY 2015 and FY 2016 aside from the new Medicaid expansion group. Only three states reported any other actual or planned copayment increases for either FY 2015 (one state) or FY 2016 (two states). Two states reported elimination of copayments in FY 2015 and three states reported reductions in copayments in either FY 2015 (two states) or FY 2016 (one state).
Increases for the ACA Expansion Population. Two states in FY 2015 (Indiana and Iowa) and four states in FY 2016 (Arizona, Montana, New Hampshire and New Mexico) adopted new copayments for their expansion populations. Four of these states (Arizona, Indiana, Iowa and New Mexico) noted changes in copayments related to non-emergent use of the Emergency Department (ED) for the expansion group; all but one (Indiana) planned to increase such copayments under existing state plan authority (up to $8). Indiana received a waiver under Section 1916(f) to test the effects of higher copayments ($8 for the first use of the ED and then $25 for subsequent use) than otherwise allowed under federal law (Section 1115 waiver authority does not extend to Medicaid cost-sharing requirements).5 Additionally, two states (New Hampshire and Michigan) reported plans to increase copayments for some expansion adults in FY 2016.
Pharmacy. A few states reported changes to pharmacy copayments in either FY 2015 or FY 2016. The nature and direction of these changes varied based on policy goals. New Mexico added pharmacy copayments for its expansion population. New Hampshire increased pharmacy copayments for its Medicaid expansion population, but eliminated pharmacy copayments for adults with incomes below 100 percent FPL. Two states reported decreased pharmacy copayments – an across the board reduction for working individuals with disabilities in New Mexico and a reduction in copayments for high value drugs (such as those for diabetes or mental illness) in South Carolina.
| ACA Medicaid Expansion Premium Waivers |
| Five states (Arkansas, Indiana, Iowa, Michigan and Montana) used or plan to use Section 1115 demonstration waiver authority to implement premium requirements for their expansion populations. (Pennsylvania also received waiver authority to implement premiums for this population beginning January 1, 2016, but Governor Wolf chose to transition its Medicaid expansion from a waiver to a state plan amendment by September 2015, without premiums.) Arkansas, Indiana, Iowa, Michigan and Montana all implemented or plan to implement changes to premiums for their expansion populations in FY 2015 or FY 2016.
Arkansas, in February 2015, added monthly contributions of $10 to $15 depending on income as part of Health Care Independence Accounts (HIA) available to newly eligible adults with incomes between 100 and 138 percent FPL in lieu of paying cost-sharing obligations. If individuals do not pay the HIA amounts, they would be assessed copayments at the point of service. Indiana’s Medicaid expansion waiver, Healthy Indiana Plan 2.0, requires most newly eligible adults with incomes from 0 to 138 percent FPL to contribute to a Personal Wellness and Responsibility (POWER) Account. Contributions range from $1 per month for individuals with incomes from zero to five percent FPL to $27 per month for individuals with incomes between 100 and 138 percent FPL. Payment is required before Medicaid enrollment is effective. Individuals have 90 days from the date of their invoice to make the required contributions without penalty. Failure to make contributions to the POWER accounts would result in a more limited benefits package and point of service copayments for those with incomes below 100 percent FPL and would result in a six month “lockout” from Medicaid eligibility for those with incomes above 100 percent FPL. Under Iowa’s Medicaid expansion waiver, enrollees with incomes over 50 percent FPL are required to make a monthly premium contribution, beginning in the second year of coverage (January 2015 at the earliest), which could be waived if the beneficiary completes specified wellness activities. Beneficiaries can also receive a hardship exemption if they cannot pay the premiums. In Iowa, there are no copayment requirements except for non-emergency use of the emergency department, which were waived during the first year of enrollment. This copayment was adopted under a SPA, not a waiver. The Healthy Michigan Plan requires contributions equal to two percent of annual income for persons between 100 and 138 percent FPL after they have been in the health plan for six months. (This is equivalent to the premiums that this population would face if they were enrolled in the Marketplace if the state had not expanded Medicaid). Total cost-sharing, including copayments (determined based on the past six months of services use) cannot exceed five percent of annual household income and is paid through the use of a dedicated health account called the “MI Health Account.” Enrollees can reduce their annual cost-sharing by participating in healthy behavior activities which include completing an annual health risk assessment. The imposition of these contributions began in FY 2015.6 Failure to pay premiums would not result in a loss of eligibility. Montana’s Medicaid expansion waiver request would impose a premium of two percent of income for the entire ACA expansion group (from 0 to 138 percent FPL) as of January 1, 2016. Montana proposes dis-enrolling beneficiaries from 100-138 percent FPL for failing to pay premiums and seeks waiver authority to lock-out these individuals until overdue premiums are paid, or there is an assessment from the Department of Revenue against income taxes. Additionally, the waiver mentions that participation in a wellness program could exempt a beneficiary from disenrollment, but details were not provided. While the state is not requesting waiver authority, the proposal would require copayments according to maximum state plan amounts and consistent with federal law for all newly eligible beneficiaries.7 |
Table 2: Changes to Eligibility Standards in all 50 States and DC, FY 2015 and 2016
|
Eligibility Standard Changes |
||||||
|
STATES |
FY 2015 |
FY 2016 |
||||
|
(+) |
(-) |
(#) |
(+) |
(-) |
(#) |
|
|
Alabama |
||||||
|
Alaska |
X – Medicaid Expansion |
|||||
|
Arizona |
||||||
|
Arkansas |
||||||
|
California |
||||||
|
Colorado |
X |
|||||
|
Connecticut |
X |
|||||
|
Delaware |
||||||
|
DC |
||||||
|
Florida |
X |
|||||
|
Georgia |
||||||
|
Hawaii |
||||||
|
Idaho |
||||||
|
Illinois |
X |
X |
||||
|
Indiana |
X – Medicaid Expansion |
|||||
|
Iowa |
||||||
|
Kansas |
X |
|||||
|
Kentucky |
||||||
|
Louisiana |
X |
X |
||||
|
Maine |
||||||
|
Maryland |
||||||
|
Massachusetts |
||||||
|
Michigan |
X |
|||||
|
Minnesota |
X |
|||||
|
Mississippi |
||||||
|
Missouri |
||||||
|
Montana |
X |
X – Medicaid Expansion |
||||
|
Nebraska |
X |
|||||
|
Nevada |
||||||
|
New Hampshire |
X – Medicaid Expansion |
|||||
|
New Jersey |
X |
|||||
|
New Mexico |
||||||
|
New York |
X |
|||||
|
North Carolina |
X |
|||||
|
North Dakota |
||||||
|
Ohio |
X |
X |
||||
|
Oklahoma |
||||||
|
Oregon |
||||||
|
Pennsylvania |
X – Medicaid Expansion |
X |
X |
|||
|
Rhode Island |
||||||
|
South Carolina |
||||||
|
South Dakota |
||||||
|
Tennessee |
X |
|||||
|
Texas |
||||||
|
Utah |
||||||
|
Vermont |
X |
|||||
|
Virginia |
X |
X |
X |
|||
|
Washington |
||||||
|
West Virginia |
||||||
|
Wisconsin |
X |
|||||
|
Wyoming |
||||||
|
Totals |
11 |
1 |
6 |
5 |
3 |
4 |
| NOTES: Positive changes from the beneficiary’s perspective that were counted in this report are denoted with (+). Negative changes from the beneficiary’s perspective that were counted in this report are denoted with (-). Several states made reductions to Medicaid eligibility pathways in response to either the availability of coverage through the Marketplaces and/or through the Medicaid expansion; these changes were denoted as (#) since most affected beneficiaries will have access to coverage through an alternative pathway.
SOURCE: Kaiser Commission on Medicaid and the Uninsured Survey of Medicaid Officials in 50 states and DC conducted by Health Management Associates, October 2015. |
||||||
Table 3: Eligibility Changes in all 50 States and DC, FY 2015 and FY 2016*
| State | Fiscal Year | Eligibility Changes |
| Alabama | 2015 | |
| 2016 | ||
| Alaska | 2015 | |
| 2016 | Adults (+): Medicaid expansion on September 1, 2015. (Estimated first year enrollment of 20,000) | |
| Arizona | 2015 | |
| 2016 | ||
| Arkansas | 2015 | |
| 2016 | ||
| California | 2015 | |
| 2016 | ||
| Colorado | 2015 | |
| 2016 | Other (+): Implement the option to eliminate the 5-year bar on eligibility for lawfully residing immigrant children. (Estimated to affect 1,699 individuals) | |
| Connecticut | 2015 | |
| 2016 | Adults (#): Reduction in income limits for parent/caretakers to 150% of FPL (with disregard, effectively 155%) (Estimated to affect 23,700 individuals, of whom 1,350 are not eligible for Transitional Medical Assistance and will lose Medicaid eligibility effective 9/1/2015) | |
| Delaware | 2015 | |
| 2016 | ||
| District of Columbia | 2015 | |
| 2016 | Adults (nc): Section 1115 waiver expires 12/31/2015. Plan to transition adults with incomes above 138% FPL from a Medicaid waiver to Medicaid state plan. (Estimated to affect 7,000 or more individuals) | |
| Florida | 2015 | Elderly and Disabled (+): Increased the minimum monthly maintenance income allowance and excess standard for community spouses of institutionalized people. (The number of nursing home residents eligible for Medicaid is also affected by 2015 cost of living adjustments and increases in the average private pay nursing home used to set LTSS policy.) |
| 2016 |
|
|
| Georgia | 2015 | |
| 2016 | ||
| Hawaii | 2015 | |
| 2016 | ||
| Idaho | 2015 | |
| 2016 |
|
|
| Illinois | 2015 | Adults (#): Family planning waiver expired December 31, 2014.
Adults (nc): The state’s previous 1115 waiver (Cook County Care) ended June 30, 2014; adults transitioned to the new Medicaid expansion adult group July 2014. |
| 2016 | Adults (#): Plan to eliminate Breast and Cervical Cancer Treatment Program, with the expectation that these individuals qualify under the ACA expansion. (current enrollment is about 1,200) | |
| Indiana | 2015 | Adults (+): Adult expansion under HIP 2.0. (Affects an estimated 357,000 individuals) |
| 2016 | ||
| Iowa | 2015 | |
| 2016 | ||
| Kansas | 2015 | Adults (+): Presumptive Eligibility for Pregnant Women. (Estimated fewer than 500) |
| 2016 | ||
| Kentucky | 2015 | |
| 2016 | ||
| Louisiana | 2015 | Adults (#): Eliminated Family Planning waiver for those over 138% FPL. Those with income below 133% FPL will move from waiver to state plan. (8,700 individuals)
Adults (+): Family Planning SPA includes more services and adds coverage for men. |
| 2016 | ||
| Maine | 2015 | |
| 2016 | ||
| Maryland | 2015 | |
| 2016 | ||
| Massachusetts | 2015 | |
| 2016 | ||
| Michigan | 2015 | |
| 2016 | Adults (+): Income and asset expansion for working disabled adults. | |
| Minnesota | 2015 | Adults (#): Eliminated MinnesotaCare coverage for those with incomes between 133% and 200% FPL. Change is neutral for enrollees because Minnesota implemented a Basic Health Plan for those with incomes between 133% and 200% FPL. |
| 2016 | ||
| Mississippi | 2015 | |
| 2016 | ||
| Missouri | 2015 | |
| 2016 | ||
| Montana | 2015 | Adults (+): Raised cap on 1115 Mental Health Services Plan (MHSP) waiver from 2,000 to 6,000 adults with SMI. |
| 2016 | Adults (+): Waiver request in process to implement ACA expansion, including request for 12 month continuous coverage. | |
| Nebraska | 2015 | |
| 2016 | Other (+): Individuals age 19-21 who entered into a subsidized guardianship or adoption at age 16 or older. (13 individuals) | |
| Nevada | 2015 | |
| 2016 | ||
| New Hampshire | 2015 | Adults (+): Implemented the Medicaid expansion as of July 1, 2014. Coverage became effective August 15, 2014. The expansion was originally implemented through existing managed care programs and transitioned to a waiver January 2016. (estimated 50,000 individuals) |
| 2016 | ||
| New Jersey | 2015 | Elderly and Disabled (+): New Jersey implemented the “Miller Trust” option. New applicants formerly eligible for the Medically Needy program will establish qualified income trust, resulting in an expanded benefit package (beyond just long-term care services). Individuals in the “Medically Needy Spend-Down Adults” group on November 30, 2014, were grandfathered into this program.8 (209 additional enrollees) |
| 2016 | ||
| New Mexico | 2015 | |
| 2016 | ||
| New York | 2015 | Adults (#): Transfer some Medicaid waiver coverage (parents with incomes from 138% FPL to 150% FPL that receive an additional premium wrap to purchase coverage in the Marketplace) to Essential Plan (New York’s BHP). |
| 2016 | ||
| North Carolina | 2015 | Adults (+): Income and resource disregard of payments from the Eugenics Compensation Program. |
| 2016 | ||
| North Dakota | 2015 | |
| 2016 | ||
| Ohio | 2015 | |
| 2016 | Adults (#): Ending Family Planning coverage group as of 1/1/16.
Other (-): Change in transitional Medicaid for families from 12 months of eligibility to six months of eligibility with possible coverage for two consecutive six-month reporting periods. (Affects estimated 50,000 individuals) |
|
| Oklahoma | 2015 | |
| 2016 | ||
| Oregon | 2015 | |
| 2016 | ||
| Pennsylvania | 2015 | Adults (+): Implemented the Healthy PA Section 1115 waiver January 1, 2015, which increased Medicaid eligibility for adults up to 138% FPL. (605,180 individuals) State converted this to a SPA starting in FY 2015 with completion in FY 2016.
Adults (#); Medically-Needy Spend-down disabled adult coverage was discontinued with the implementation of Healthy PA; however, it is scheduled for reinstatement in FY 2016. (Affects 3,346 individuals) |
| 2016 | Adults (nc): Family Planning waiver converted to a SPA. Review of family planning enrollees for possible eligibility for full health care. (90,000 individuals)
Adults (#): Reinstatement of medically needy spend-down for disabled adults. (3,346 individuals) Adults (nc): Converted all individuals enrolled in Medicaid expansion under the Healthy PA 1115 waiver to the Health Choices Medicaid expansion state plan as of September 1st. |
|
| Rhode Island | 2015 | |
| 2016 | ||
| South Carolina | 2015 | |
| 2016 | ||
| South Dakota | 2015 | |
| 2016 | ||
| Tennessee | 2015 | |
| 2016 | Elderly and Disabled (-): In FY 2016 (7/1/2015), will begin limiting new LTSS enrollment into a 1915(i)-like group (offered under 1115 authority) to those eligible for SSI only. People already enrolled in the group under institutional income standards will be grandfathered. (Affects estimated 915 individuals) | |
| Texas | 2015 | |
| 2016 | ||
| Utah | 2015 | |
| 2016 | ||
| Vermont | 2015 | Other (+): Submitted SPA to disregard asset tests for non-ABD medically needy. |
| 2016 | ||
| Virginia | 2015 | Adults (#): Restored income eligibility for Family Planning coverage to 200% FPL. (Limit had been cut to 100% FPL on 1/1/2014.)
Elderly and Disabled (+): For Ticket to Work disabled population, three changes: Adults (+): Implemented a Section 1115 waiver program to expand limited benefit coverage to uninsured adults with incomes up to 100% FPL with serious mental illness. |
| 2016 | Adults (-): Per state legislation, income eligibility for the Section 1115 waiver program that expanded limited benefit coverage to uninsured adults with serious mental illness was reduced from 100% FPL to 60% FPL. | |
| Washington | 2015 | |
| 2016 | ||
| West Virginia | 2015 | |
| 2016 | ||
| Wisconsin | 2015 | Elderly and Disabled (-): Treating promissory notes as an asset. (Estimate of 40 individuals) |
| 2016 | ||
| Wyoming | 2015 | |
| 2016 | ||
| * Positive changes from the beneficiary’s perspective that were counted in this report are denoted with (+). Negative changes from the beneficiary’s perspective that were counted in this report are denoted with (-). Several states made reductions to Medicaid eligibility pathways in response to either the availability of coverage through the Marketplaces and/or through the Medicaid expansion; these changes were denoted as (#) since most affected beneficiaries will have access to coverage through an alternative pathway. Other changes to Medicaid eligibility that are not likely to affect beneficiaries but were reported by states are denoted with (nc). | ||
Table 4: Premium and Copayment Actions Taken in all 50 States and DC, FY 2015 and 2016*
| State | Fiscal Year | Premium and Copayment Changes |
| Alabama | 2015 | |
| 2016 | ||
| Alaska | 2015 | |
| 2016 | ||
| Arizona | 2015 | |
| 2016 | Copays (New only for expansion group): Impose mandatory copays to federal statutory limits and an $8 copay for non-emergent use of the ER on expansion adults. (Upon CMS approval) | |
| Arkansas | 2015 | Premiums (New only for expansion group): Added monthly contributions as part of Health Independence Accounts available to newly eligible adults with incomes between 100-138% FPL. Contributions to the HIAs are in lieu of point of service copayments. (February 2015) |
| 2016 | ||
| California | 2015 | |
| 2016 | ||
| Colorado | 2015 | |
| 2016 | ||
| Connecticut | 2015 | |
| 2016 | ||
| Delaware | 2015 | |
| 2016 | ||
| District of Columbia | 2015 | |
| 2016 | ||
| Florida | 2015 | |
| 2016 | ||
| Georgia | 2015 | |
| 2016 | ||
| Hawaii | 2015 | |
| 2016 | ||
| Idaho | 2015 | |
| 2016 | ||
| Illinois | 2015 | |
| 2016 | ||
| Indiana | 2015 | Premiums (New only for expansion group): POWER Account Contributions under HIP 2.0 for all low-income parents/caretakers and the new adult group (0-138% FPL) on a sliding scale. Those that fail to pay premiums within a 60-day grace period with income at or below 100% FPL are moved to a more limited benefit package and those with income over 100% FPL will be dis-enrolled from coverage and barred from re-enrolling for 6 months. (Feb 2015)
Premiums (New): Non-expansion parent/caretaker relatives and those receiving TMA have the option of paying premiums to get additional benefits and in lieu of copays for services. Copays (New): Testing graduated copays ($8 then $25) for non-emergency use of the ER for non-expansion parent/caretakers and newly eligible adults under § 1916(f) authority. Copays (New for expansion group): Beneficiaries with income at or below 100% FPL who fail to pay premiums will be required to make copays in state plan amounts. Copays (Elimination): Remove copays for ABD enrollees in managed care. (April 2015) |
| 2016 | Copays (New): Restore copays for ABD enrollees in managed care (Jan 2016) | |
| Iowa | 2015 | Premiums (New only for expansion group): Under the Iowa Health and Wellness Plan (IHWP), enrollees with incomes over 50 percent FPL are required to make a monthly premium contribution, beginning in the second year of coverage, which could be waived if they complete specified wellness activities. Premium amounts are $5 per month for those with incomes between 50% to 100% FPL and $10 per month for those with incomes over 100% FPL. Individuals can file a hardship exemption if they are not able to pay. (Jan 2015)
Copays (New only for expansion group): All enrollees in the expansion group are be subject to $8 copay for non-emergent use of the ED. (Jan 2015) |
| 2016 | ||
| Kansas | 2015 | |
| 2016 | ||
| Kentucky | 2015 | |
| 2016 | ||
| Louisiana | 2015 | |
| 2016 | ||
| Maine | 2015 | |
| 2016 | ||
| Maryland | 2015 | |
| 2016 | ||
| Massachusetts | 2015 | |
| 2016 | ||
| Michigan | 2015 | Premiums (New only for expansion group): Healthy Michigan Plan requires MI Health Account contributions equal to 2% of annual income for persons between 100% and 133% FPL after they have been in the health plan for 6 months. (Oct 2014) |
| 2016 | Premiums (Increase): Legislation expanding the income and asset levels for Freedom to Work Medicaid (TWIIAA) included a revised premium schedule. (Oct 2015)
Copays (Increase): Increase in prescription, hospital, and office visit copays for Healthy Michigan Plan enrollees with incomes above 100% FPL. (Unknown date due to systems issues and CMS approval requirements.) |
|
| Minnesota | 2015 | Cost-Sharing (Neutral Effect): The family deductible for adults in Medicaid was decreased to $2.75 per month, retroactive to 1/1/2014. (MCOs can waive the deductible.) |
| 2016 | Premiums (Decreased): Minimum premium for Medical Assistance for Employed Persons with Disabilities (MA-EPD) reduced. (Sep 2015)
Copays (Decreased): Decreased copayment amounts for MA-EPD group. (Sep 2015) |
|
| Mississippi | 2015 | |
| 2016 | ||
| Missouri | 2015 | |
| 2016 | ||
| Montana | 2015 | |
| 2016 | Premiums (New only for expansion group): Waiver request to impose premiums (2% of income) for the entire ACA expansion group.
Copays (New only for expansion group): Individuals with incomes up to 138% FPL will be required to pay copayments up to the maximum allowable amount under federal law. |
|
| Nebraska | 2015 | |
| 2016 | ||
| Nevada | 2015 | |
| 2016 | ||
| New Hampshire | 2015 | Copays (Eliminated): Eliminating pharmacy copays for adults under 100% FPL. (July 2014) |
| 2016 | Copays (Increased): Pharmacy copays for the expansion group (those above 100% FPL) are being increased from $1/$4 (generic/brand) to $2/$8. (Jan 2016)
Copays (New only for expansion group): Expansion group will be subject to copays on some medical services. (Jan 2016) |
|
| New Jersey | 2015 | |
| 2016 | ||
| New Mexico | 2015 | Copays (Decreased): Pharmacy copayment decreased from $5.00 to $4.00 for working disabled Individuals. (FY 2015) |
| 2016 | Copays (New only for expansion group): Copays for non-emergency use of the emergency department and for brand-name prescriptions when there is a less expensive generic equivalent medicine available. (FY 2016) | |
| New York | 2015 | |
| 2016 | ||
| North Carolina | 2015 | |
| 2016 | ||
| North Dakota | 2015 | |
| 2016 | ||
| Ohio | 2015 | |
| 2016 | ||
| Oklahoma | 2015 | Copays (Increased): Most SoonerCare copays increased. (July 2014) |
| 2016 | ||
| Oregon | 2015 | |
| 2016 | ||
| Pennsylvania | 2015 | |
| 2016 | ||
| Rhode Island | 2015 | |
| 2016 | ||
| South Carolina | 2015 | |
| 2016 | Copays (Decrease): Exempting certain high value drugs (including maintenance and certain psychiatric drugs) from copay requirements for all full benefit Medicaid beneficiaries. (July 2015) | |
| South Dakota | 2015 | |
| 2016 | ||
| Tennessee | 2015 | |
| 2016 | ||
| Texas | 2015 | |
| 2016 | ||
| Utah | 2015 | |
| 2016 | ||
| Vermont | 2015 | |
| 2016 | ||
| Virginia | 2015 | |
| 2016 | ||
| Washington | 2015 | |
| 2016 | ||
| West Virginia | 2015 | |
| 2016 | ||
| Wisconsin | 2015 | |
| 2016 | ||
| Wyoming | 2015 | |
| 2016 | ||
| * New premiums or copays as well as new requirements (i.e. making copays enforceable) are noted as (NEW). Increases in existing premiums or copays are noted as (Increased), while decreases are noted as (Decreased) and eliminations are noted as (Eliminated). | ||
Managed Care Reforms
| Key Section Findings |
Tables 5 through 10 include more detail on the populations covered under managed care (Table 5), expansions to new groups (Table 6), selected benefits included in managed care contracts (Table 7), managed care quality initiatives (Table 8), and MLR (Table 9) and auto-enrollment policies (Table 10). These tables are also available in a downloadable PDF. |
Managed care is now the predominant delivery system for Medicaid in most states, as Medicaid programs increasingly have turned to managed care as a means to help ensure access, improve quality and achieve budget certainty. As of July 2015, all states (including DC) except three – Alaska, Connecticut and Wyoming– had in place some form of managed care. Across the 48 states with some form of managed care, a total of 39 states (including DC) had contracts with comprehensive risk-based managed care organizations (MCOs); 19 states administered a Primary Care Case Management (PCCM) program, a managed fee-for-service based system in which beneficiaries are enrolled with a primary care provider who are paid a small fee to provide case management services in addition to primary care. Of the 48 states that operate some form of managed care, a total of 10 states operate both MCOs and a PCCM program while 29 states (including DC) operate MCOs only and nine states operate PCCM programs only.1 (Figure 3) Wyoming, one of the three states without managed care (i.e., without an MCO or PCCM model), does operate a limited-benefit risk-based prepaid health plan (PHP). In total, 18 states (including Wyoming) contracted with one or more PHPs to provide behavioral health, dental care, maternity care, non-emergency medical transportation, or other benefits.
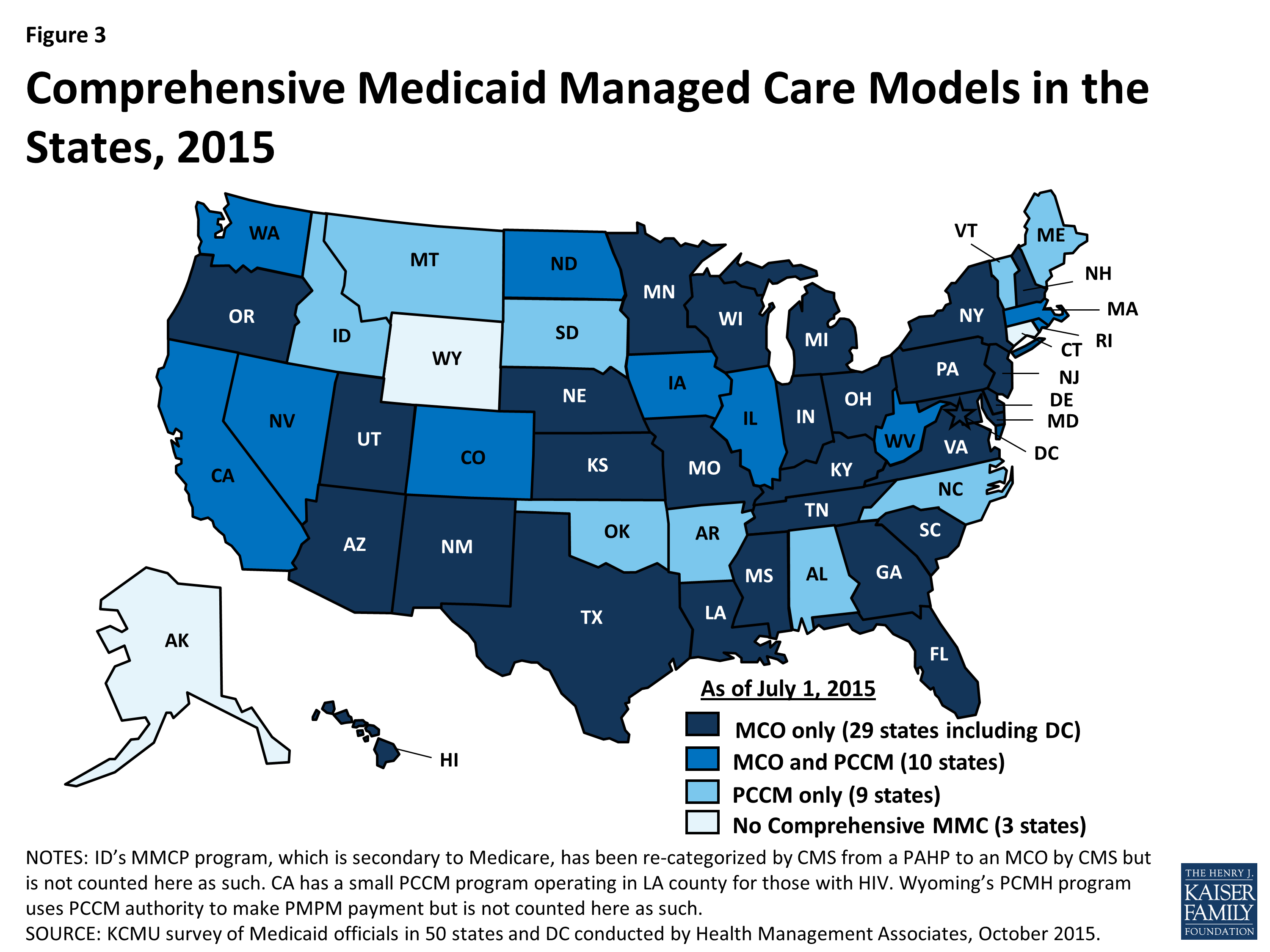
Figure 3: Comprehensive Medicaid Managed Care Models in the States, 2015
Populations Covered by Managed Care
The share of Medicaid beneficiaries enrolled in MCOs, PCCM programs or remaining in fee-for-service varies widely by state. However, the share of Medicaid beneficiaries enrolled in MCOs has steadily increased as states have expanded their managed care programs to new regions and new populations and made MCO enrollment mandatory for additional eligibility groups. In this year’s survey, states were asked to indicate the approximate share of specific Medicaid populations that were served by MCOs, PCCM programs and fee-for-service (FFS) for their acute care services. As shown in Table 5, among the 39 states (including DC) with MCOs, 21 states reported that 75 percent or more of their Medicaid beneficiaries were enrolled in MCOs as of July 1, 2015, including four of the five states with the largest total Medicaid enrollment, accounting for 4 out of every 10 Medicaid beneficiaries across the country (California, New York, Texas and Florida). (Figure 4 and Table 5)
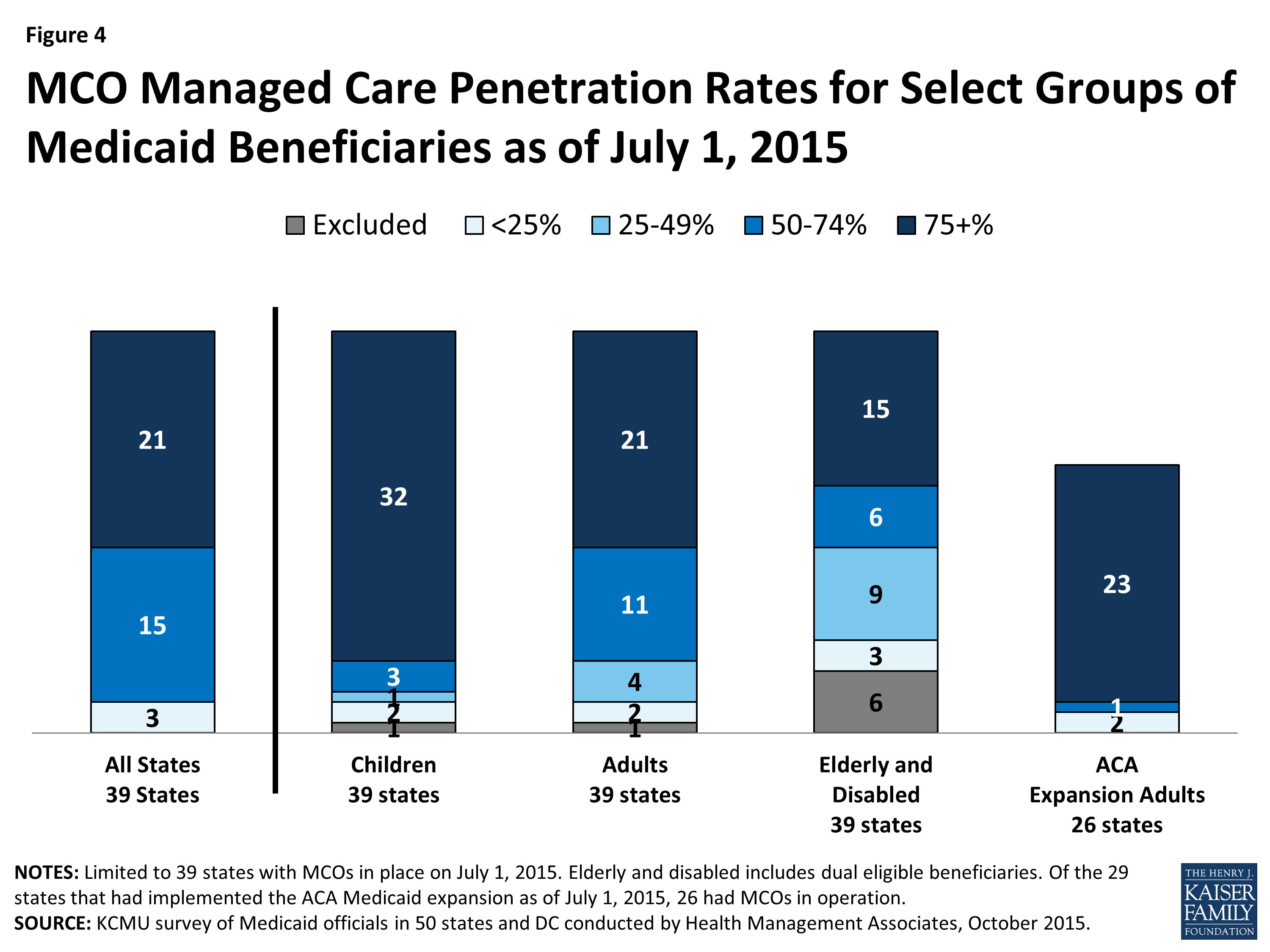
Figure 4: MCO Managed Care Penetration Rates for Select Groups of Medicaid Beneficiaries as of July 1, 2015
Children and adults (particularly those enrolled through the ACA Medicaid expansion) are much more likely to be enrolled in an MCO than elderly Medicaid beneficiaries or those with disabilities. Thirty-two (32) of the 39 MCO states covered 75 percent or more of children through MCOs. Twenty-one (21) of the 39 MCO states covered 75 percent or more of low-income adults (e.g., parents, pregnant women) through MCOs. The elderly and people with disabilities were the group least likely to be covered through managed care contracts, with only 15 of the 39 MCO states covering 75 percent or more such enrollees through MCOs. (Figure 4) With the exception of some states participating in the CMS Financial Alignment Demonstrations, most states were even less likely to include those dually eligible for Medicare and Medicaid through managed care contracts.
Of the 29 states that were implementing the ACA Medicaid expansion on July 1, 2015, 26 were using MCOs to cover newly eligible adults. (The three expansion states without risk-based managed care were Arkansas, Connecticut and Vermont.) The large majority (23) of these 26 states covered more the 75 percent of beneficiaries in this group through managed care. The three states with less than 75 percent MCO penetration for this group were Colorado, Illinois and Iowa (which each operate PCCM programs as well as MCOs.)
Ten (10) of the 19 states with PCCM programs also contract with MCOs. In most of these states, MCOs cover a larger share of beneficiaries than PCCM programs. However, Colorado, Iowa and North Dakota are exceptions: a majority of Colorado’s enrollees were in the PCCM program, which is the foundation of the state’s Accountable Care Collaboratives, and approximately four in ten enrollees in both Iowa and North Dakota were enrolled in those states’ PCCM programs as of July 1, 2015.
Managed Care Population Changes
In both FY 2015 and in FY 2016, states continued to take actions to increase enrollment in managed care, although fewer states reported doing so than in last year’s survey – likely reflecting full or nearly full MCO saturation in a growing number of states. Of the 39 states (including DC) with MCOs, a total of 20 states indicated that they made specific policy changes in either FY 2015 (13 states) or FY 2016 (13 states) to increase the number of enrollees in MCOs, compared to 34 in last year’s survey; no states with MCOs took any action to restrict MCO enrollment.
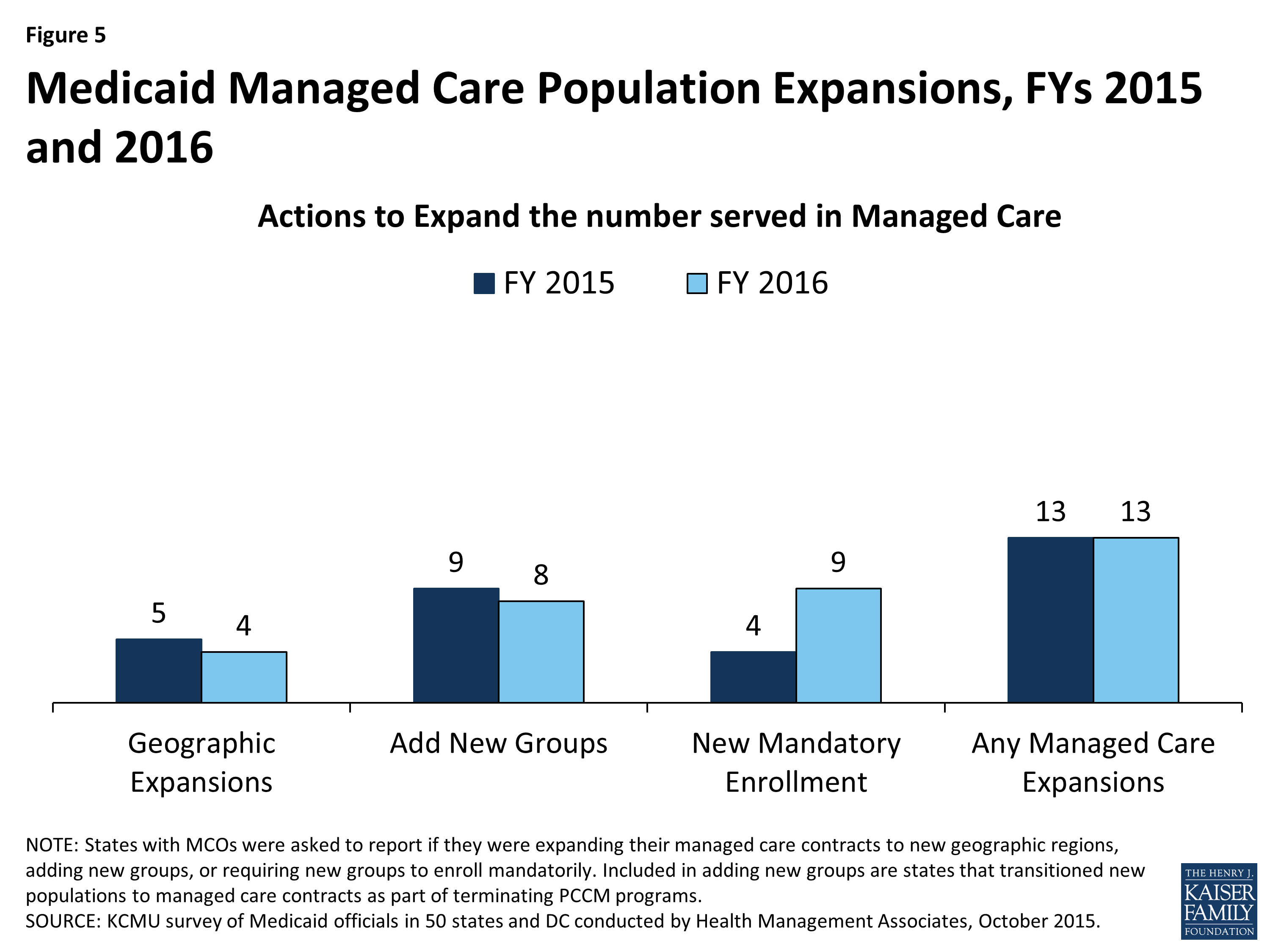
Figure 5: Medicaid Managed Care Population Expansions, FYs 2015 and 2016
The most common strategy was to expand voluntary or mandatory enrollment to additional eligibility groups (9 states in FY 2015 and 8 states in FY 2016). The eligibility group most commonly added to MCOs was persons eligible for LTSS (New Jersey, New Mexico, New York, Texas, Virginia and Washington), followed by the newly eligible adult group in states adopting the ACA Medicaid expansion (Illinois, Indiana, Pennsylvania and West Virginia). In addition, five states (Florida, Indiana, Iowa, Louisiana and Rhode Island) are terminating their PCCM programs in either FY 2015 or FY 2016 and shifting those populations into risk-based managed care (discussed below). Four states (Florida, Illinois, Louisiana and New York) made enrollment mandatory for specific eligibility groups in FY 2015, and nine states (Illinois, Iowa, Louisiana, New Hampshire, New York, Rhode Island, Utah, Virginia and Washington) are doing so in FY 2016. Expansions of MCO geographic service areas were reported in five states in FY 2015, and in four states for FY 2016. (Figure 5) In addition, California reported plans to enroll undocumented children into MCOs in FY 2015. This is predominantly a state-funded program and is therefore not counted as a Medicaid policy change in this report.
| Notable MCO Expansions Implemented or Planned |
| Florida transitioned nearly all Medicaid enrollees into MCOs on a phased-in schedule that was completed in August 2014. At that time, Florida’s PCCM, dental PHP and behavioral health PHP programs ended.
Indiana began enrolling aged, blind and disabled enrollees into the Hoosier Care Connect MCO program in April 2015 and ended the Care Select PCCM program on June 30, 2015. Iowa plans to implement statewide MCO coverage for almost all Medicaid enrollees on January 1, 2016 (pending federal waiver approval) and end its PCCM and behavioral health PHP programs. Louisiana discontinued its Bayou Health Shared Savings (enhanced PCCM) model on January 31, 2015 and transitioned enrollees to MCOs. Rhode Island reported plans to eliminate its PCCM program for adults with disabilities (Connect Care Choice) in FY 2016 and transition enrollees to MCOs. |
Primary Care Case Management (PCCM) Programs Changes
Of the 19 states with PCCM programs, six indicated they enacted policies to increase PCCM enrollment in FY 2015 or FY 2016. Four (Iowa, Massachusetts, Montana and Nevada) indicated that they would enroll new Medicaid expansion adults in their PCCM programs; Alabama expanded its Health Home program statewide in FY 2015; and Colorado reported increased PCCM enrollment of persons dually eligible for Medicare and Medicaid as part of its Financial Alignment Demonstration.
In contrast, seven states (Florida, Illinois, Indiana, Iowa, Louisiana, Oklahoma, and Rhode Island) have taken actions to decrease enrollment in their PCCM programs. Five of these states (Florida, Indiana, Iowa, Louisiana and Rhode Island) have ended or plan to end their PCCM programs and will transition PCCM enrollees to risk-based managed care. In June 2014, Illinois began transitioning 1.5 million PCCM enrollees to new care coordination models (including both risk-based managed care and PCCM models) in five mandatory enrollment regions. In Oklahoma, effective July 2014, individuals with creditable primary coverage are no longer eligible for the SoonerCare Choice PCCM program.
Limited-Benefit Prepaid Health Plans (PHP) Changes
Of the 18 states with one or more limited-benefit prepaid health plans (PHPs), six indicated they enacted policies to increase PHP enrollment in FY 2015 or FY 2016. California is planning to move coverage of substance abuse services from FFS to a PHP arrangement in FY 2016.2 Iowa reported that the benefit for its Medicaid expansion population includes a dental PHP program, and Pennsylvania reported that the Medicaid expansion would increase enrollment in its behavioral health PHP program. Michigan indicated that its dental PHP program was expanding to additional counties; Wisconsin noted that its LTSS PHP was expanding to additional counties; and Wyoming expanded a behavioral health PHP program for children statewide.
Four states reported actions that decreased enrollment in their PHP programs. Iowa and Florida folded, or will fold, PHP arrangements into their MCO programs (dental and behavioral health PHPs in Florida and a behavioral health PHP program in Iowa). Colorado ended a physical health PHP and replaced it with an MCO arrangement, and Washington is allowing “Early Adopter” counties to convert behavioral health PHPs to fully integrated MCO contracts.
Benefits Covered Under Managed Care Contracts
Although MCOs are at-risk financially for providing a comprehensive set of acute-care services, nearly all states elect to exclude or “carve-out” certain services from MCO contracts. These services may be delivered and financed through another contractual arrangement (e.g., through a limited benefit risk-based PHP) or in the FFS delivery system. In this year’s survey, states were asked to indicate the delivery system(s) used to provide the following benefits: prescription drugs, children’s dental services, adult dental services, outpatient and inpatient mental health services and substance abuse services.
The data presented shows this information only for populations enrolled under an MCO contract. Nearly all states exclude some populations from MCOs. For example, North Dakota does not cover children through its managed care contracts so North Dakota is not included in the “Dental (Children)” data. Ten states that operate MCOs do not cover dental services for adults (or only cover emergency dental), so these states are excluded from the “Dental (Adults)” counts.
“Carved-in” refers to the inclusion in MCO contracts of virtually all services in a given category (exceptions may exist, such as limited carve-outs for selected drugs). “Varies” refers to cases where the inclusion of benefits in MCO contracts may vary by population or region or the contract may cover some but not all services (e.g., states that carve-in some behavioral health services but carve-out specialized services for persons with serious mental illness). “Carved-out” means that the services are largely excluded from MCO contracts and are instead covered under either a FFS or PHP model. (Figure 6) States were also asked to describe any carve-in or carve-out changes for specific benefits in FY 2015 or planned for FY 2016. The most commonly reported benefit change was to carve-in behavioral health services and LTSS.
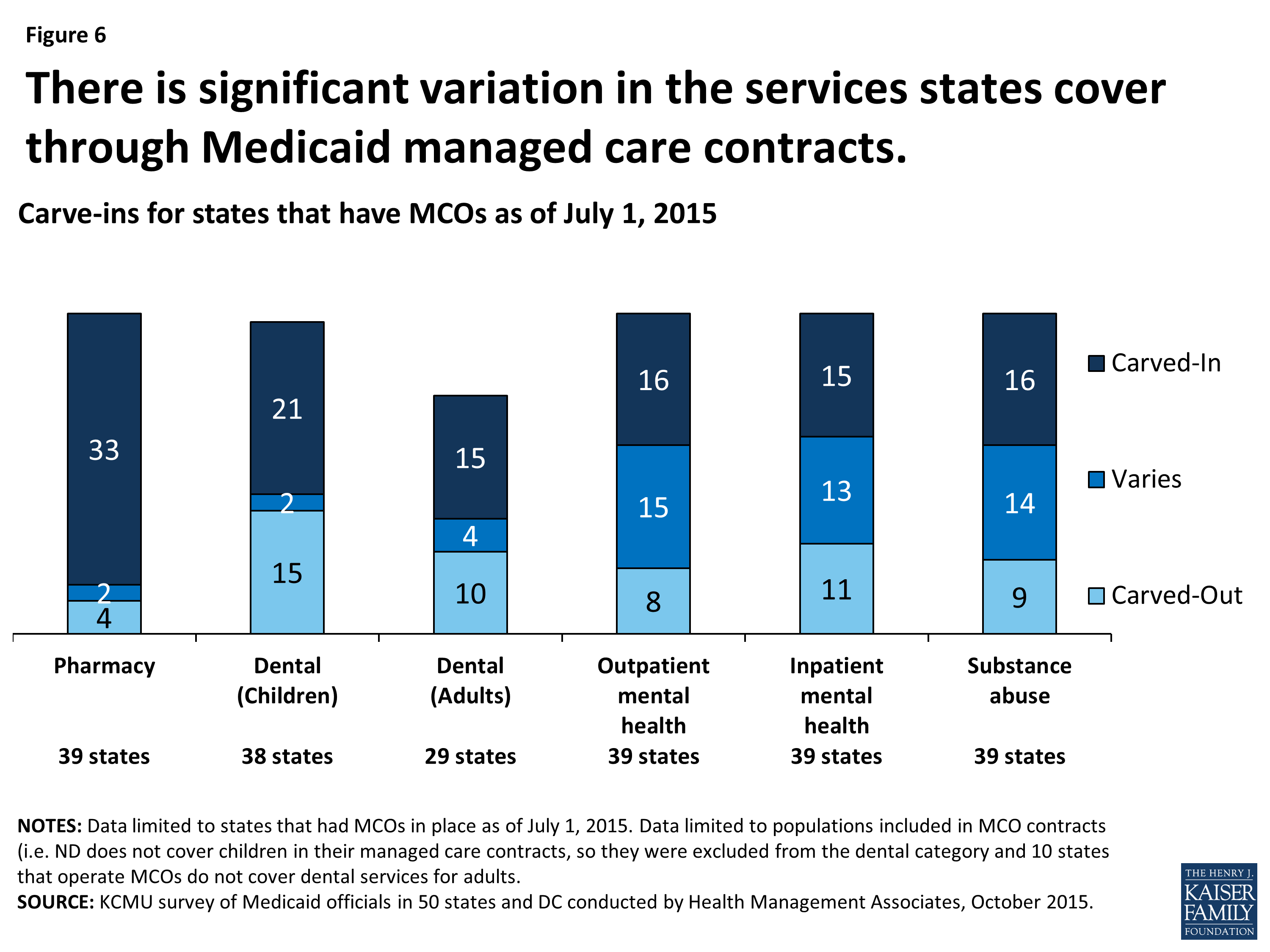
Figure 6: There is significant variation in the services states cover through Medicaid managed care contracts.
Pharmacy
Most MCO states (33 of 39 states) carve-in their pharmacy services for the populations covered by their MCO contracts. Some of these states have small carve-outs for certain drugs or drug classes (e.g., HIV/AIDS drugs, medications for hepatitis C, mental health drugs, etc.). Three states (Iowa, Missouri and Nebraska) carve-out pharmacy benefits entirely, delivering these benefits on a FFS basis. Additionally, Tennessee reported that all drugs – except for certain physician-administered drugs – are carved-out and delivered FFS through a contracted pharmacy benefit manager. Two states (Indiana and Wisconsin) reported that pharmacy benefits are carved-in under certain MCO programs but carved-out of others.
A number of states have carved pharmacy benefits into their managed care contracts in recent years. In this year’s survey, four states added or reported plans to add pharmacy benefits to their managed care contracts (Delaware, Iowa, Indiana and New York). Delaware reported carving pharmacy benefits into their MCO contracts in FY 2015. Iowa plans to carve the pharmacy benefit into its MCO contracts as it terminates its PCCM program and shifts this population to MCOs in FY 2016. Indiana implemented a new MCO program for the aged, blind and disabled population in FY 2015 that included pharmacy benefits; it also carved-in pharmacy benefits for the Healthy Indiana Plan (the state’s expansion group). New York, which had already carved most pharmacy benefits into managed care contracts, plans to carve-in hemophilia factor products and injectable antipsychotic drugs in FY 2016. In contrast, only one state (Maryland) reported carving some pharmacy benefits out of managed care contracts in FY 2016 (substance use disorder drugs).
Dental
Children’s Dental. More than half of MCO states that cover children under their managed care contracts3 generally carve-in children’s dental services (21 of 38 states). Fifteen (15) MCO states carve-out children’s dental services. The majority of these states cover children’s dental on a FFS basis, but two states (Louisiana and Rhode Island) carve-out these services to a PHP and two states (Michigan and Utah) use both PHP and FFS models, depending on geographic area. Two states (Indiana and Wisconsin) reported that children’s dental services are sometimes carved-in: Indiana’s coverage varies by MCO program and Wisconsin’s coverage varies by geographic region.
Adult Dental. Twenty-nine (29) of the 39 MCO states reported that they cover adult dental benefits; the other ten do not cover adult dental or only provide coverage for emergency dental services.4 Just over half of the MCO states that cover adult dental generally carve-in this benefit (15 of 29 states). Another four (Indiana, Massachusetts, Michigan and Wisconsin) sometimes carve-in adult dental services; in Indiana, Massachusetts and Michigan, the dental carve-in varies by MCO program while the dental carve-in in Wisconsin varies by geographic region. Eight of the remaining ten MCO states with adult dental benefits carve these services out5 to FFS, while two states (Iowa for expansion adults and Louisiana) carve-out adult dental services to PHPs.
Indiana reported carving dental services into managed care contracts for selected populations (children and adults) in FY 2015.
Behavioral Health
States cover behavioral health services (mental health and substance abuse services) through a wide array of delivery arrangements. Sixteen (16) MCO states generally cover outpatient mental health services through their MCO contracts; a similar number cover inpatient mental health services (15 states) and substance abuse services (16 states) through their MCO contracts. Of the remaining states, a number contract with PHPs to provide carved-out specialty behavioral health services.
Eight states reported planned changes for FY 2016: six states (Arizona, Iowa, Louisiana, New York, Washington and West Virginia) plan to carve inpatient and outpatient mental health services as well as substance abuse services into at least some of their MCO contracts. Arizona plans to carve-in these services for their dual-eligible beneficiaries under their acute care contracts; New York continues to phase in coverage of these services under managed care plans. Iowa and Louisiana plan to transition coverage from PHPs to their managed care contracts. Washington also reported plans to carve these services into managed care contracts in regions that elect to be “Early Adopters” as part of their effort to establish common purchasing regions for managed behavioral health and physical health. (Those that do not will contract separately for physical and behavioral health.) In addition, Mississippi plans to carve inpatient mental health services into its managed care contracts as part of its larger effort to carve-in inpatient services generally. Maryland reported carving substance abuse services out of managed care contracts in FY 2015.
Long-Term Care Services and Supports (LTSS)
In this survey, about half of the MCO states reported that institutional LTSS (17 states) and home and community-based services (HCBS) (18 states) were provided only under the FFS delivery system. However, the survey did not capture whether LTSS was carved out of the states’ MCO arrangements or whether, instead, persons receiving LTSS were entirely excluded from MCO arrangements for all of their care (primary, acute, and behavioral health services). Only a small number of states reported that most LTSS is provided by MCOs – five states for institutional LTSS (Arizona, Hawaii, Kansas, New Mexico and Tennessee) and four states for HCBS (Arizona, Kansas, New Jersey and Tennessee). In some of these states, however, persons with intellectual and developmental disabilities (IDD) are excluded from enrollment or IDD waiver services are carved-out. In addition, 17 other MCO states reported providing some HCBS and institutional LTSS through MCOs, often based on specific population characteristics and/or geographic region (for example, under a Financial Alignment Demonstration for dual eligible beneficiaries). A number of states also mentioned PACE programs,6 but this site-based form of managed care was not counted for purposes of this analysis.
Ten states reported changes for FY 2015 or planned for FY 2016. In FY 2015, six states (California, Michigan, New Jersey, New York, South Carolina and Texas) implemented MCO arrangements for institutional LTSS and HCBS for at least some populations; many of these states noted this change was in reference to the launch of dual eligible demonstrations (Michigan, New York, South Carolina and Texas). California implemented MCO contracts including both HCBS and institutional care services in some counties in FY 2015. New Jersey carved HCBS (services and beneficiaries) into managed care contracts as well as institutional services for new nursing facility entrants (those already in nursing facilities will remain in FFS). Texas also carved institutional LTSS into its non-dual managed LTSS program. Additionally, Idaho added institutional as well as HCBS to its Medicare-Medicaid Coordinated Plan (MMCP) in FY 2015.7
In FY 2016, five states will implement new LTSS MCO arrangements. Rhode Island will implement its dual eligible demonstration; Iowa will include both HCBS and institutional LTSS into new MCO contracts (pending federal waiver approval), and New Hampshire will add HCBS to its MCO contracts. New York and New Mexico will add additional LTSS (services and beneficiaries) to their MCO contracts (assisted living services in New York, waiver services for the medically frail in New Mexico).
Managed Care Quality Initiatives
All states with MCO programs track one or more quality measures and require other health plan quality activities to improve health care outcomes and plan performance. In this year’s survey, states were asked whether certain quality strategies were in place in FY 2014, or newly added or expanded in FY 2015 or FY 2016. Thirty-three (33) of the 39 MCO states (including DC) had one or more of these quality strategies in place in FY 2014. A majority (23 states) publicly reported or required MCOs to publicly report quality metrics (e.g., a “report card”), and over one-third had pay-for-performance provisions, capitation withholds, and performance bonuses or penalties in place in FY 2014 as well. (Figure 7) Four states mentioned other types of quality initiatives in place in 2014 including a requirement for some or all plans to be NCQA-accredited (Massachusetts and Tennessee), a requirement for MCOs to implement provider and member incentive plans (Missouri) and other reviews of performance, quality and network adequacy (Nevada).
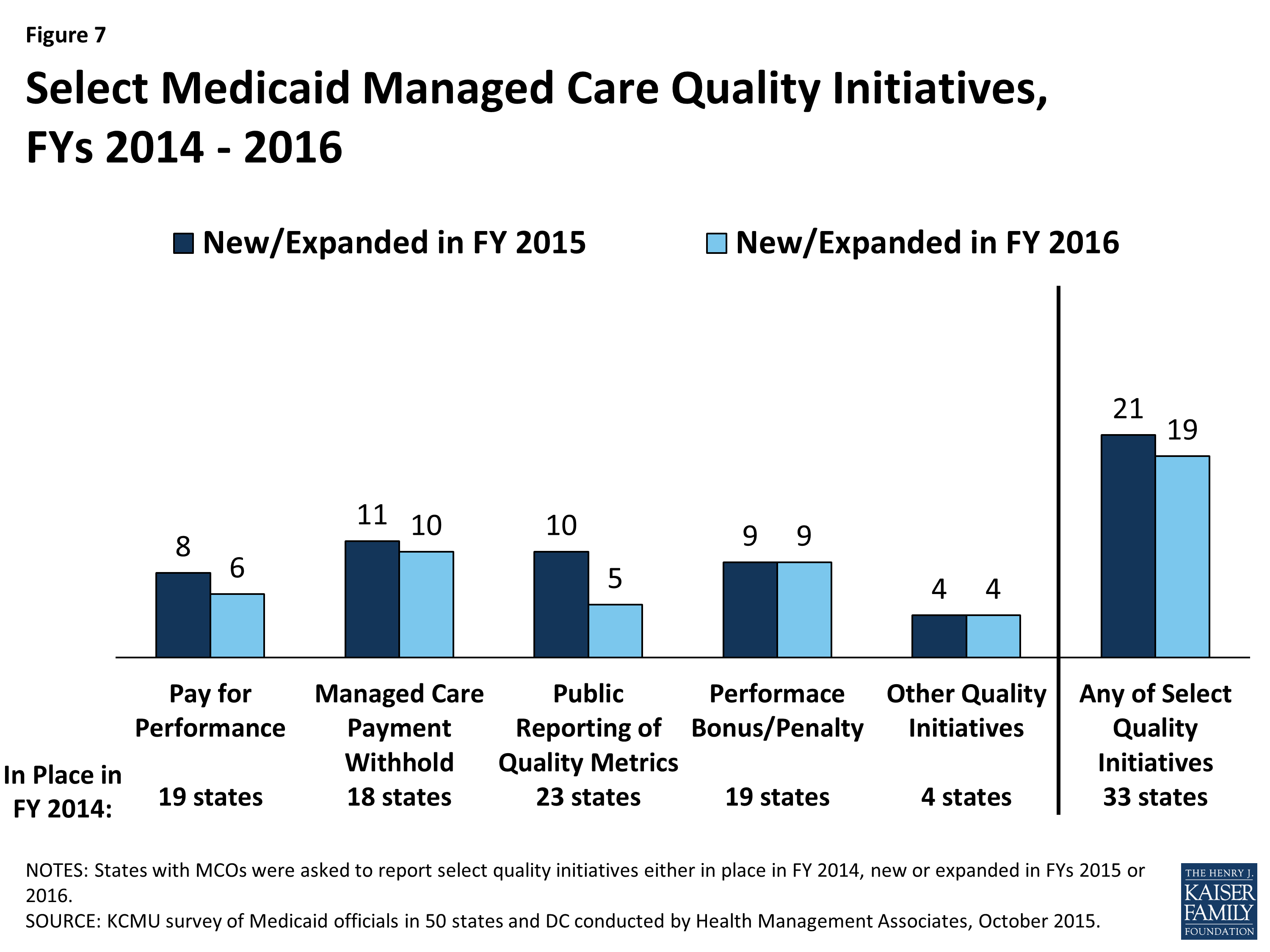
Figure 7: Select Medicaid Managed Care Quality Initiatives, FYs 2014 – 2016
In FY 2015, a total of 21 states implemented new or expanded quality initiatives and 19 states planned to do so in FY 2016. The most common initiative that was new or expanded in FY 2015 and 2016 was managed care payment withholds tied to quality performance. (Figure 7) Three of these states in FY 2015 (California, Texas and West Virginia) and two of these states in FY 2016 (DC and Iowa) added new withhold requirements. Withhold amounts ranged from 0.15 percent (Virginia) to five percent (West Virginia and Minnesota). Several states also reported expanding or adding new pay-for- performance requirements as well as performance bonus or penalties and initiatives to publicly report quality metrics.
A few states mentioned additional types of quality initiatives. Minnesota will require MCOs to participate in its ACO and value-based contracting initiatives in FY 2016, and Pennsylvania will require MCOs to participate in community-based care management programs in FY 2015 and plans to require MCOs to participate in physical health/behavioral health integration efforts in FY 2016.
Medicaid Managed Care Administrative Policies
Minimum Medical Loss Ratios
For an MCO, the proportion of total per member per month capitation payments that is spent on clinical services and for quality improvement is known as the Medical Loss Ratio (MLR). Thus, the MLR represents the share of dollars that MCOs spend on providing and improving patient care, rather than on administrative costs, which include executive salaries, overhead, and marketing and profits. State insurance regulators commonly set a minimum MLR for commercial health plans, and the ACA mandates a minimum MLR for Medicare Advantage plans and for qualified health plans (QHPs) participating in the health insurance Marketplaces. There is currently no federal minimum MLR for Medicaid MCOs, nor are state Medicaid programs currently required to set minimum MLRs, but states are allowed to establish minimum MLR requirements for Medicaid health plans.
As of July 1, 2015, 19 of the 39 states that contracted with comprehensive risk-based MCOs specified a minimum MLR for all or some plans, and 20 states did not have an MLR requirement. Seventeen (17) of the 19 states with a MLR requirement always applied it and two states applied it on a limited basis (e.g., for the new ACA Medicaid expansion population). State Medicaid MLRs vary, but are most commonly set at 85 percent. A few states noted that their minimum MLRs varied by type of plan or population.
Other states that do not require a minimum MLR did note other mechanisms to monitor administrative costs and profits among Medicaid MCOs. Four states without minimum MLRs (Massachusetts, New York, Pennsylvania and Virginia) reported having a cap on profits and/or administrative costs. Two states (California and Utah) reported using a target MLR in their rate-setting process. One state (Texas) reported requiring “experience rebates” from plans with profits above a specified level, and one state (Kansas) reported not requiring a minimum MLR but does track MLRs of its plans.
Auto-enrollment
Beneficiaries who are required to enroll in MCOs must be offered a choice of at least two plans. Those who do not select a plan are auto-enrolled in a plan by the state. Of the 39 states with comprehensive risk-based MCOs, all except one required some or all beneficiaries to enroll in an MCO. (The exception is North Dakota, which has only one health plan.) The proportion of beneficiaries who are auto-enrolled varies widely across states. Two states had auto-enrollment rates of 10 percent or less, while six states auto-enrolled over 75 percent of new MCO enrollees.8 States’ auto-enrollment algorithms also vary, but are usually designed to take into consideration previous plan or provider relationships, geographic location of the beneficiary, and/or plan enrollments of other family members. In addition, over half (23) of MCO states reported that their auto-enrollment algorithms were designed to balance enrollments among plans; 15 states considered plan capacity, and eight states took plan quality rankings into consideration. Other states noted plans to move toward including quality rankings in their auto-assignment algorithms in the future.
| Selected State Auto-Enrollment Quality Criteria |
| Minnesota: Enrollees who do not select a plan are defaulted (i.e., auto-enrolled) into plans in their area with the highest overall quality score.
Missouri: Auto-enrollment algorithm includes various factors including plan capacity, balancing enrollment among plans, certain performance criteria and consideration of the number of FQHCs, RHCs, CMHCs, and safety net hospitals in the plan. Washington: The auto-enrollment algorithm is based on an average of plan performance on two HEDIS measures as well as initial health screening rates. In May 2015, Washington’s Health Benefit Exchange implemented health plan selection online, enabling Medicaid beneficiaries to select a health plan online at the time of eligibility and recertification or at any time (as state does not currently have a “lock-in” policy). The state anticipates this change will reduce the number of auto-enrolled individuals. |
Using HEDIS measures for Plan Selection. In this year’s survey, states were asked if they used, or planned to use, HEDIS scores as criteria for selecting MCOs to contract with. Of the 39 states with MCOs, 14 answered “yes,” 22 answered “no,” and three states did not respond.
| Proposed Managed Care Rule |
| On May 26, 2015, CMS released a long-awaited proposal to revise and modernize the Medicaid managed care regulations.9 The proposed rule addresses changes that have occurred in state Medicaid managed care and other programs since the regulations were last revised in 2002, including the emergence of managed long-term services and supports (MLTSS) and other innovative payment and delivery system models. Among other things, the sweeping changes proposed are intended to strengthen the quality of care provided to Medicaid beneficiaries, promote more effective use of data in overseeing managed care, strengthen actuarial soundness and other payment requirements, ensure beneficiary protections, promote beneficiary access to care and strengthen program integrity safeguards. The proposed rule is also intended to promote better alignment with other coverage including Marketplace Qualified Health Plans and Medicare Advantage plans.10 A variety of other stakeholders, including state Medicaid agencies, health plans, providers and beneficiary advocates, commented on the proposed rule, expressing support for select provisions and raising concerns over others.11
In its lengthy and detailed comment letter to CMS submitted on July 27, 2015, the National Association of Medicaid Directors (NAMD) identified both the specific concerns of its members as well as those provisions of the proposed rule viewed as positive policy approaches.12 Three overarching concerns were identified: the new administrative costs that states would incur to implement the new requirements; the ability of CMS to carry out the new proposed oversight activities without resulting in problematic delays for states (e.g., approvals of capitation rates and contracts); and the apparent shift in the balance of regulatory authority for Medicaid managed care from the states to the federal government. Of particular concern is a requirement for states to provide a minimum 14-day period of FFS coverage before enrolling beneficiaries into managed care arrangements and the proposed capitation rate review process. In this survey, states were asked to identify the key issues, concerns or opportunities related to the proposed rule. A number of states indicated that the proposed rule was still under review and other states touched on many of the issues raised in the NAMD comment letter. The most frequently cited concerns related to the capitation rate review process and the 14 day FFS enrollment requirement. |
Table 5: Share of the Medicaid Population Covered Under Different Delivery Systems, as of July 2015
| States | Type(s) of Managed Care In Place | Share of Medicaid Population in Different Managed Care Systems | ||
| MCO | PCCM | Other / FFS | ||
| Alabama | PCCM | — | 64.3% | 35.7% |
| Alaska | FFS | — | — | 100.0% |
| Arizona | MCO | 87.3% | — | 12.7% |
| Arkansas | PCCM* | — | 57.6% | 42.4%* |
| California | MCO and PCCM* | 77.0% | <1% | 23.0% |
| Colorado | MCO and PCCM* | 8.5% | 64.9% | 26.6% |
| Connecticut | FFS* | — | — | 100.0% |
| DC | MCO | 72.0% | — | 28.0% |
| Delaware | MCO | 90.0% | — | 10.0% |
| Florida | MCO | 79.0% | — | 21.0% |
| Georgia | MCO | 66.4% | — | 33.6% |
| Hawaii | MCO | 99.9% | — | 0.1% |
| Idaho | PCCM* | — | NR | NR |
| Illinois | MCO and PCCM | 52.7% | 26.6% | 20.7% |
| Indiana | MCO* | 77.9% | 0.6%* | 21.5% |
| Iowa | MCO and PCCM | 12.0% | 37.0% | 51.0% |
| Kansas | MCO | 95.0% | — | 5.0% |
| Kentucky | MCO | 91.0% | — | 9.0% |
| Louisiana | MCO | 71.0% | — | 29.0% |
| Maine | PCCM | — | NR | NR |
| Maryland | MCO | 82.0% | — | 18.0% |
| Massachusetts | MCO and PCCM | 51.5% | 20.6% | 27.9% |
| Michigan | MCO | 77.0% | — | 23.0% |
| Minnesota | MCO | 73.0% | — | 27.0% |
| Mississippi | MCO* | 67.0% | — | 33.0% |
| Missouri | MCO | 50.5% | — | 49.5% |
| Montana | PCCM | — | 73.7% | 26.3% |
| Nebraska | MCO | 74.0% | — | 26.0% |
| Nevada | MCO and PCCM | 68.0% | 6.0% | 26.0% |
| New Hampshire | MCO | 89.8% | — | 10.2% |
| New Jersey | MCO | 93.0% | — | 7.0% |
| New Mexico | MCO | 87.5% | — | 12.5% |
| New York | MCO | 77.8% | — | 22.2% |
| North Carolina | PCCM | — | NR | NR |
| North Dakota | MCO and PCCM | 21.0% | 41.0% | 37.0% |
| Ohio | MCO | 78.3% | — | 21.7% |
| Oklahoma | PCCM | — | 69.9% | 30.1% |
| Oregon | MCO* | 93.0% | — | 7.0% |
| Pennsylvania | MCO | 70.0% | — | 30.0% |
| Rhode Island | MCO and PCCM | 87.7% | 1.6% | 10.7% |
| South Carolina | MCO | 75.0% | — | 25.0% |
| South Dakota | PCCM | — | 86.0% | 14.0% |
| Tennessee | MCO | 100.0% | — | — |
| Texas | MCO | 88.0% | — | 12.0% |
| Utah | MCO* | 62.8% | — | 37.2% |
| Vermont | PCCM | — | NR | NR |
| Virginia | MCO | 66.0% | — | 34.0% |
| Washington | MCO and PCCM | 79.0% | 1.0% | 20.0% |
| West Virginia | MCO and PCCM | 65.0% | 2.0% | 33.0% |
| Wisconsin | MCO | 67.0% | — | 33.0% |
| Wyoming | FFS* | — | — | 100.0% |
| NOTES: Share of Medicaid Population that is covered by different managed care systems. MCO refers to risk-based managed care; PCCM refers to Primary Care Case Management. Other/FFS refers to Medicaid beneficiaries that are not in MCOs or PCCM programs. *AR – included in “Other/FFS” include those receiving premium assistance through the Private Option (Medicaid Expansion). *CA – PCCM program operates in LA county for those with HIV. *CO – PCCM enrollees are part of the state’s Accountable Care Collaboratives (ACO). *CT – terminated its MCO contracts in 2012 and now operates its program on a fee-for-service basis using four administrative services only entities. *ID – The Medicaid-Medicare Coordinated Plan (MMCP) has been recategorized by CMS as an MCO but is not counted here as such since it is secondary to Medicare. *IN – state ended its PCCM program as of July 1, 2015. *MS – risk-based managed care program does not cover inpatient hospital services. *OR – MCO enrollees include those enrolled in the state’s Coordinated Care Organizations. *UT – MCO enrollees include those enrolled in the state’s Accountable Care Organizations. *WY – the state does not operate a traditional PCCM or MCO program, but does use PCCM authority to make PCMH payments.
SOURCE: Kaiser Commission on Medicaid and the Uninsured Survey of Medicaid Officials in 50 states and DC conducted by Health Management Associates, October 2015. |
||||
Table 6: Medicaid Managed Care Expansions to New Groups in all 50 States and DC, FY 2015 and 2016
| States | Geographic Expansions | Add New Groups | New Mandatory Enrollment | Any Managed Care Expansions | |||||
| 2015 | 2016 | 2015 | 2016 | 2015 | 2016 | 2015 | 2016 | Either Year | |
| Alabama | |||||||||
| Alaska | |||||||||
| Arizona | |||||||||
| Arkansas | |||||||||
| California | |||||||||
| Colorado | X | X | X | ||||||
| Connecticut | |||||||||
| Delaware | |||||||||
| DC | |||||||||
| Florida | X | X | X | ||||||
| Georgia | |||||||||
| Hawaii | |||||||||
| Idaho | |||||||||
| Illinois | X | X | X | X | X | X | X | X | X |
| Indiana | X | X | X | ||||||
| Iowa | X | X | X | X | X | ||||
| Kansas | |||||||||
| Kentucky | |||||||||
| Louisiana | X | X | X | X | X | ||||
| Maine | |||||||||
| Maryland | |||||||||
| Massachusetts | |||||||||
| Michigan | |||||||||
| Minnesota | |||||||||
| Mississippi | X | X | X | X | X | ||||
| Missouri | |||||||||
| Montana | |||||||||
| Nebraska | X | X | X | ||||||
| Nevada | |||||||||
| New Hampshire | X | X | X | ||||||
| New Jersey | X | X | X | ||||||
| New Mexico | X | X | X | ||||||
| New York | X | X | X | X | X | X | X | X | |
| North Carolina | |||||||||
| North Dakota | |||||||||
| Ohio | |||||||||
| Oklahoma | |||||||||
| Oregon | |||||||||
| Pennsylvania | X | X | X | ||||||
| Rhode Island | X | X | X | X | |||||
| South Carolina | |||||||||
| South Dakota | |||||||||
| Tennessee | |||||||||
| Texas | X | X | X | X | |||||
| Utah | X | X | X | X | |||||
| Vermont | |||||||||
| Virginia | X | X | X | X | X | ||||
| Washington | X | X | X | X | |||||
| West Virginia | X | X | X | ||||||
| Wisconsin | X | X | X | X | X | ||||
| Wyoming | |||||||||
| Totals | 5 | 4 | 9 | 8 | 4 | 9 | 13 | 13 | 20 |
| NOTES: States were asked if they expanded managed care (comprehensive risk-based managed care) to new regions, new populations, or increased the use of mandatory enrollment.
SOURCE: Kaiser Commission on Medicaid and the Uninsured Survey of Medicaid Officials in 50 states and DC conducted by Health Management Associates, October 2015. |
|||||||||
Table 7: Coverage of Select Benefits Under Medicaid Managed Care Contracts, as of July 2015
| State | Coverage of Select Benefits under MCO contracts | |||||
| Pharmacy | Dental | Behavioral Health | ||||
| Children | Adults | Outpatient Mental Health | Inpatient Mental Health | Substance Abuse | ||
| Alabama | — | — | — | — | — | — |
| Alaska | — | — | — | — | — | — |
| Arizona | carved-in | carved-in | carved-in | varies (region) | varies (region) | varies (region) |
| Arkansas | — | — | — | — | — | — |
| California | carved-in | carved-out | carved-out | varies (services) | carved-out | carved-out |
| Colorado | carved-in | carved-in | carved-in | carved-out | carved-out | carved-out |
| Connecticut | — | — | — | — | — | — |
| DC | carved-in | carved-in | carved-in | varies (services) | varies (services) | varies (services) |
| Delaware | carved-in | carved-out | not covered | varies (services) | varies (services) | varies (services) |
| Florida | carved-in | carved-in | carved-in | carved-in | carved-in | carved-in |
| Georgia | carved-in | carved-in | not covered | carved-in | carved-in | carved-in |
| Hawaii | carved-in | carved-out | not covered | varies (services) | varies (services) | varies (services) |
| Idaho | — | — | — | — | — | — |
| Illinois | carved-in | carved-in | carved-in | carved-in | carved-in | carved-in |
| Indiana | varies | varies | varies | carved-out | varies (services) | varies (services) |
| Iowa | carved-out | carved-out | carved-out | carved-out | carved-out | carved-out |
| Kansas | carved-in | carved-in | carved-out | carved-in | carved-in | carved-in |
| Kentucky | carved-in | carved-in | carved-in | carved-in | carved-in | carved-in |
| Louisiana | carved-in | carved-out | carved-out | carved-out | carved-out | carved-out |
| Maine | — | — | — | — | — | — |
| Maryland | carved-in | carved-out | carved-out | carved-out | carved-out | carved-out |
| Massachusetts | carved-in | carved-out | varies | carved-in | carved-in | carved-in |
| Michigan | carved-in | carved-out | varies | varies (services) | varies (services) | carved-out |
| Minnesota | carved-in | carved-in | carved-in | carved-in | carved-in | carved-in |
| Mississippi | carved-in | carved-in | carved-in | carved-in | carved-out | carved-in |
| Missouri | carved-out | carved-in | carved-in | varies (services) | carved-out | varies (services) |
| Montana | — | — | — | — | — | — |
| Nebraska | carved-out | carved-out | carved-out | carved-out | carved-out | carved-out |
| Nevada | carved-in | carved-in | not covered | carved-in | carved-in | carved-in |
| New Hampshire | carved-in | carved-out | not covered | carved-in | carved-in | carved-in |
| New Jersey | carved-in | carved-in | carved-in | varies (program, population) | varies (program, population) | varies (program, population) |
| New Mexico | carved-in | carved-in | carved-in | carved-in | carved-in | carved-in |
| New York | carved-in | carved-in | carved-in | varies (population, services) | varies (population, services) | varies (services) |
| North Carolina | — | — | — | — | — | — |
| North Dakota | carved-in | excluded | not covered | carved-in | carved-in | carved-in |
| Ohio | carved-in | carved-in | carved-in | varies (population) | carved-in | varies (population) |
| Oklahoma | — | — | — | — | — | — |
| Oregon | carved-in | carved-in | carved-in | carved-in | carved-out | carved-in |
| Pennsylvania | carved-in | carved-in | carved-in | carved-out | carved-out | carved-out |
| Rhode Island | carved-in | carved-out | carved-out | varies (services) | varies (services) | varies (services) |
| South Carolina | carved-in | carved-out | carved-out | varies (services) | varies (services) | varies (services) |
| South Dakota | — | — | — | — | — | — |
| Tennessee | carved-out | carved-in | not covered | carved-in | carved-in | carved-in |
| Texas | carved-in | carved-in | not covered | carved-in | carved-in | carved-in |
| Utah | carved-in | carved-out | carved-out | varies (services) | varies (services) | varies (services) |
| Vermont | — | — | — | — | — | — |
| Virginia | carved-in | carved-out | not covered | varies (services) | varies (services) | varies (services) |
| Washington | carved-in | carved-out | carved-out | carved-out | carved-out | carved-out |
| West Virginia | carved-in | carved-in | not covered | carved-in | carved-in | carved-in |
| Wisconsin | varies | varies | varies | varies (services) | varies (services) | varies (services) |
| Wyoming | — | — | — | — | — | — |
| Carved-in | 33 | 21 | 15 | 16 | 15 | 16 |
| Varies | 2 | 2 | 4 | 15 | 13 | 14 |
| Carved-out | 4 | 15 | 10 | 8 | 11 | 9 |
| NOTES: *– indicates there were no MCOs operating in that state’s Medicaid program in July 2015. Data limited to populations included in MCO contracts (e.g., ND does not cover children in their managed care contracts, so they were excluded from the dental (children) category and 10 states that operate MCOs do not cover dental services for adults, these states were excluded from dental (adults)). Carved-in refers to states that carve-in virtually all services (exceptions might relate to small carve-outs for select drugs for example). Varies refers to instances where services are carved in for some populations covered under MCOs but not for other MCO populations or some services are carved-in while others are not (e.g. more intensive mental health or behavioral health services are carved-out.) Carved-out means that the service is largely carved out of managed care and covered by either FFS or PHPs.
SOURCE: Kaiser Commission on Medicaid and the Uninsured Survey of Medicaid Officials in 50 states and DC conducted by Health Management Associates, October 2015. |
||||||
TABLE 8: MEDICAID MANAGED CARE QUALITY INITIATIES IN ALL 50 STATES AND DC, FY 2014 – 2016
|
States |
Pay for Performance |
Managed Care Payment Withhold |
Public Reporting of Quality Metrics |
Performance Bonus or Penalties |
Other Quality Initiatives |
Any Quality Initiatives |
||||||||||||
|
In Place |
New/ Expanded |
In Place |
New/ Expanded |
In Place |
New/ Expanded |
In Place |
New/ Expanded |
In Place |
New/ Expanded |
In Place |
New/ Expanded |
|||||||
|
2014 |
2015 |
2016 |
2014 |
2015 |
2016 |
2014 |
2015 |
2016 |
2014 |
2015 |
2016 |
2014 |
2015 |
2016 |
2014 |
2015 |
2016 |
|
|
Alabama |
||||||||||||||||||
|
Alaska |
||||||||||||||||||
|
Arizona |
X |
X |
X |
X |
X |
X |
X |
X |
X |
X |
||||||||
|
Arkansas |
||||||||||||||||||
|
California |
X |
X |
X |
X |
X |
X |
X |
X |
X |
|||||||||
|
Colorado |
X |
X |
X |
X |
||||||||||||||
|
Connecticut |
||||||||||||||||||
|
DC |
X |
X |
X |
X |
X |
X |
||||||||||||
|
Delaware |
X |
X |
X |
|||||||||||||||
|
Florida |
X |
X |
X |
X |
X |
X |
X |
X |
X |
|||||||||
|
Georgia |
X |
X |
X |
X |
X |
X |
||||||||||||
|
Hawaii |
X |
X |
X |
X |
||||||||||||||
|
Idaho |
||||||||||||||||||
|
Illinois |
X |
X |
X |
X |
X |
X |
X |
X |
X |
X |
||||||||
|
Indiana |
X |
X |
X |
X |
||||||||||||||
|
Iowa |
X |
X |
X |
|||||||||||||||
|
Kansas |
X |
X |
X |
X |
||||||||||||||
|
Kentucky |
X |
X |
X |
X |
||||||||||||||
|
Louisiana |
X |
X |
X |
X |
X |
X |
X |
X |
||||||||||
|
Maine |
||||||||||||||||||
|
Maryland |
X |
X |
X |
|||||||||||||||
|
Massachusetts |
X |
X |
X |
X |
X |
X |
X |
X |
||||||||||
|
Michigan |
X |
X |
X |
X |
X |
X |
X |
X |
||||||||||
|
Minnesota |
X |
X |
X |
X |
X |
X |
||||||||||||
|
Mississippi |
X |
X |
X |
X |
||||||||||||||
|
Missouri |
X |
X |
X |
X |
X |
X |
X |
X |
X |
X |
X |
X |
||||||
|
Montana |
||||||||||||||||||
|
Nebraska |
||||||||||||||||||
|
Nevada |
X |
X |
X |
X |
X |
X |
||||||||||||
|
New Hampshire |
X |
X |
X |
X |
||||||||||||||
|
New Jersey |
X |
X |
X |
X |
X |
X |
X |
X |
X |
|||||||||
|
New Mexico |
X |
X |
X |
X |
X |
|||||||||||||
|
New York |
X |
X |
X |
X |
||||||||||||||
|
North Carolina |
||||||||||||||||||
|
North Dakota |
||||||||||||||||||
|
Ohio |
X |
X |
X |
X |
X |
X |
X |
X |
X |
X |
X |
|||||||
|
Oklahoma |
||||||||||||||||||
|
Oregon |
X |
X |
X |
X |
X |
|||||||||||||
|
Pennsylvania |
X |
X |
X |
X |
X |
X |
X |
X |
X |
X |
X |
X |
||||||
|
Rhode Island |
X |
X |
X |
|||||||||||||||
|
South Carolina |
X |
X |
X |
X |
X |
|||||||||||||
|
South Dakota |
||||||||||||||||||
|
Tennessee |
X |
X |
X |
|||||||||||||||
|
Texas |
X |
X |
X |
X |
X |
X |
X |
|||||||||||
|
Utah |
X |
X |
||||||||||||||||
|
Vermont |
||||||||||||||||||
|
Virginia |
X |
X |
X |
X |
X |
X |
X |
X |
X |
X |
X |
X |
||||||
|
Washington |
X |
X |
X |
|||||||||||||||
|
West Virginia |
X |
X |
X |
X |
X |
X |
X |
|||||||||||
|
Wisconsin |
X |
X |
X |
X |
X |
X |
X |
X |
X |
|||||||||
|
Wyoming |
||||||||||||||||||
|
Totals |
19 |
8 |
6 |
18 |
11 |
10 |
23 |
10 |
5 |
19 |
9 |
9 |
4 |
4 |
4 |
33 |
21 |
19 |
|
NOTES: States with MCO contracts were asked to report if select quality initiatives were included in contracts in FY 2014, new or expanded in FY 2015 or in FY 2016. The table above does not reflect all quality initiatives states have included as part of MCO contracts. SOURCE: Kaiser Commission on Medicaid and the Uninsured Survey of Medicaid Officials in 50 states and DC conducted by Health Management Associates, October 2015. |
||||||||||||||||||
Table 9: Minimum Medical Loss Ratio Policies for Medicaid MCOs in all 50 States and DC, as of July 2015
| Minimum Medical Loss Ratio (MLR) | ||
| States | Require minimum MLR | % if required |
| Alabama | — | |
| Alaska | — | |
| Arizona | Yes — always | 85% |
| Arkansas | — | |
| California | Yes — sometimes* | 85%* (Expansion) |
| Colorado | Yes — always | 85% |
| Connecticut | — | |
| Delaware | No | |
| DC | Yes — always | 85% |
| Florida | Yes — always | 85% |
| Georgia | No | |
| Hawaii | Yes — always | ~90% |
| Idaho | — | |
| Illinois | Yes — always | 85% (aged, blind and disabled) 88% (MAGI-related populations) |
| Indiana | Yes — always | 85% (Hoosier Healthwise program) 87% (HIP 2.0 and Hoosier Care Connect) |
| Iowa | Yes — always | 85% |
| Kansas | No | |
| Kentucky | Yes — always | 85% |
| Louisiana | Yes — always | 85% |
| Maine | — | |
| Maryland | Yes — always | NR |
| Massachusetts | No* | |
| Michigan | No | |
| Minnesota | No | |
| Mississippi | Yes — always | 85% |
| Missouri | No | |
| Montana | — | |
| Nebraska | No | |
| Nevada | No | |
| New Hampshire | No | |
| New Jersey | Yes — always | 80% |
| New Mexico | Yes — always | 85% |
| New York | No* | |
| North Carolina | — | |
| North Dakota | No | |
| Ohio | Yes — always | 85% |
| Oklahoma | — | |
| Oregon | Yes — sometimes | 80% (Expansion) |
| Pennsylvania | No* | |
| Rhode Island | No | |
| South Carolina | No | |
| South Dakota | — | |
| Tennessee | No | |
| Texas | No* | |
| Utah | No* | |
| Vermont | — | |
| Virginia | No* | |
| Washington | Yes — always | 85-87%* |
| West Virginia | Yes — always | 85% |
| Wisconsin | No | |
| Wyoming | — | |
| Yes — always | 17 | |
| Yes — sometimes | 2 | |
| No | 20 | |
| N/A – No MCOs | 12 | |
| NOTES: MLR refers to the proportion of total per member per month capitation payments that is spent on clinical services and for quality improvement. “–” indicates states that do not have Medicaid MCOs. NR – not reported. CA (outside of their expansion population) and UT reported not requiring a minimum MLR but using a target MLR as part of their rate setting process. MA, NY, PA, VA reported no minimum MLR but do have administrative and/or profit caps. TX has experience rebates on plans above a certain profit level. VA – FY16 contract also requires MCOs to report MLRs to the state, but there is no minimum MLR. WA indicated that the minimum MLR varied by population.
SOURCE: Kaiser Commission on Medicaid and the Uninsured Survey of Medicaid Officials in 50 states and DC conducted by Health Management Associates, October 2015. |
||
Table 10: Auto-Enrollment Policies for Medicaid MCOs in all 50 States and DC, as of July 2015
|
Auto-Enrollment Practices |
Select Factors Used in State Auto-Enrollment Algorithms |
||||||
|
States |
Auto-Enrollment Process |
Share of Beneficiaries Auto-Enrolled |
Plan Capacity |
Plan Cost |
Balancing Enrollment |
Encouraging New Plan Entrants |
Plan Quality Rating |
|
Alabama |
|||||||
|
Alaska |
|||||||
|
Arizona |
Yes |
17% (Acute Care)* |
X |
||||
|
Arkansas |
|||||||
|
California |
Yes |
35-40% |
X |
X |
X |
X |
|
|
Colorado |
Yes |
94%* |
|||||
|
Connecticut |
|||||||
|
Delaware |
Yes |
45% |
X |
||||
|
DC |
Yes |
20% |
X |
X |
|||
|
Florida |
Yes |
52% – Acute Care (MMA) |
|||||
|
Georgia |
Yes |
NR |
X |
X |
|||
|
Hawaii |
Yes |
100%* |
X |
X |
X |
||
|
Idaho |
|||||||
|
Illinois |
Yes |
53% |
X |
X |
|||
|
Indiana |
Yes |
68% |
X |
||||
|
Iowa |
Yes |
80% |
|||||
|
Kansas |
Yes |
65% |
X |
||||
|
Kentucky |
Yes |
54% |
X |
X |
|||
|
Louisiana |
Yes |
50% |
X |
X |
|||
|
Maine |
|||||||
|
Maryland |
Yes |
32% |
X |
X |
|||
|
Massachusetts |
Yes |
30% |
X |
X |
|||
|
Michigan |
Yes |
24% |
X |
X |
X |
||
|
Minnesota |
Yes |
25% |
X |
||||
|
Mississippi |
Yes |
80% |
|||||
|
Missouri |
Yes |
13% |
X |
X |
|||
|
Montana |
|||||||
|
Nebraska |
Yes |
52% |
X |
||||
|
Nevada |
Yes |
30% |
X |
||||
|
New Hampshire |
Yes |
30% |
|||||
|
New Jersey |
Yes |
15% |
|||||
|
New Mexico |
Yes |
22% |
X |
||||
|
New York |
Yes |
4% (statewide) |
X |
X |
X |
||
|
North Carolina |
|||||||
|
North Dakota |
No |
||||||
|
Ohio |
Yes |
39% (CFC & ABD) |
|||||
|
Oklahoma |
|||||||
|
Oregon |
Yes |
5% |
X |
X |
|||
|
Pennsylvania |
Yes |
40% |
X |
||||
|
Rhode Island |
Yes |
20% |
|||||
|
South Carolina |
Yes |
60% |
X |
X |
|||
|
South Dakota |
|||||||
|
Tennessee |
Yes |
100%* |
X |
||||
|
Texas |
Yes |
30% |
X |
X |
|||
|
Utah |
Yes |
20% |
X |
||||
|
Vermont |
|||||||
|
Virginia |
Yes |
80% |
X |
||||
|
Washington |
Yes |
50% |
X |
||||
|
West Virginia |
Yes |
50% |
X |
||||
|
Wisconsin |
Yes |
60%* |
X |
X |
|||
|
Wyoming |
|||||||
|
Total |
38 |
15 |
2 |
23 |
3 |
8 |
|
|
NOTES: States with Medicaid MCOs were asked if they have an auto-enrollment process and to estimate the share of their population that is typically auto-enrolled (average monthly basis for FY 2015). NR – not reported. AZ – rate reported refers to acute care only. CO – the state only has one MCO plan; it uses a passive enrollment process since there isn’t a choice of plans. HI and TN both auto-enroll beneficiaries and then offer beneficiaries a period to change plans. WI – Long-term care does not have an auto-enrollment process; auto enrollment used only for HMOs. SOURCE: Kaiser Commission on Medicaid and the Uninsured Survey of Medicaid Officials in 50 states and DC conducted by Health Management Associates, October 2015. |
|||||||
Emerging Delivery System and Payment Reforms
| Key Section Findings |
Tables 11 and 12 contain more detailed information on emerging delivery system and payment reform initiatives in place in FY 2014, implemented in FY 2015 or planned for FY 2016. These tables are also available in a downloadable PDF. |
Interest in delivery system and payment reforms that hold the promise of improving health outcomes and constraining costs remains high among state Medicaid programs across the country. Twenty-seven (27) states in FY 2015 and 28 states in FY 2016 reported adopting or expanding one or more initiatives that seek to reward quality and encourage integrated care. Key initiatives include patient-centered medical homes (PCMHs), Health Homes, and Accountable Care Organizations (ACOs). States are also implementing initiatives to coordinate care and financing for dual eligible beneficiaries. Episode of care and DSRIP initiatives are emerging delivery system reforms. This year’s survey asked states to identify which delivery system and payment reform models were in place in FY 2014, and whether they had adopted or were enhancing such models in FY 2015 or FY 2016. (Figure 8)
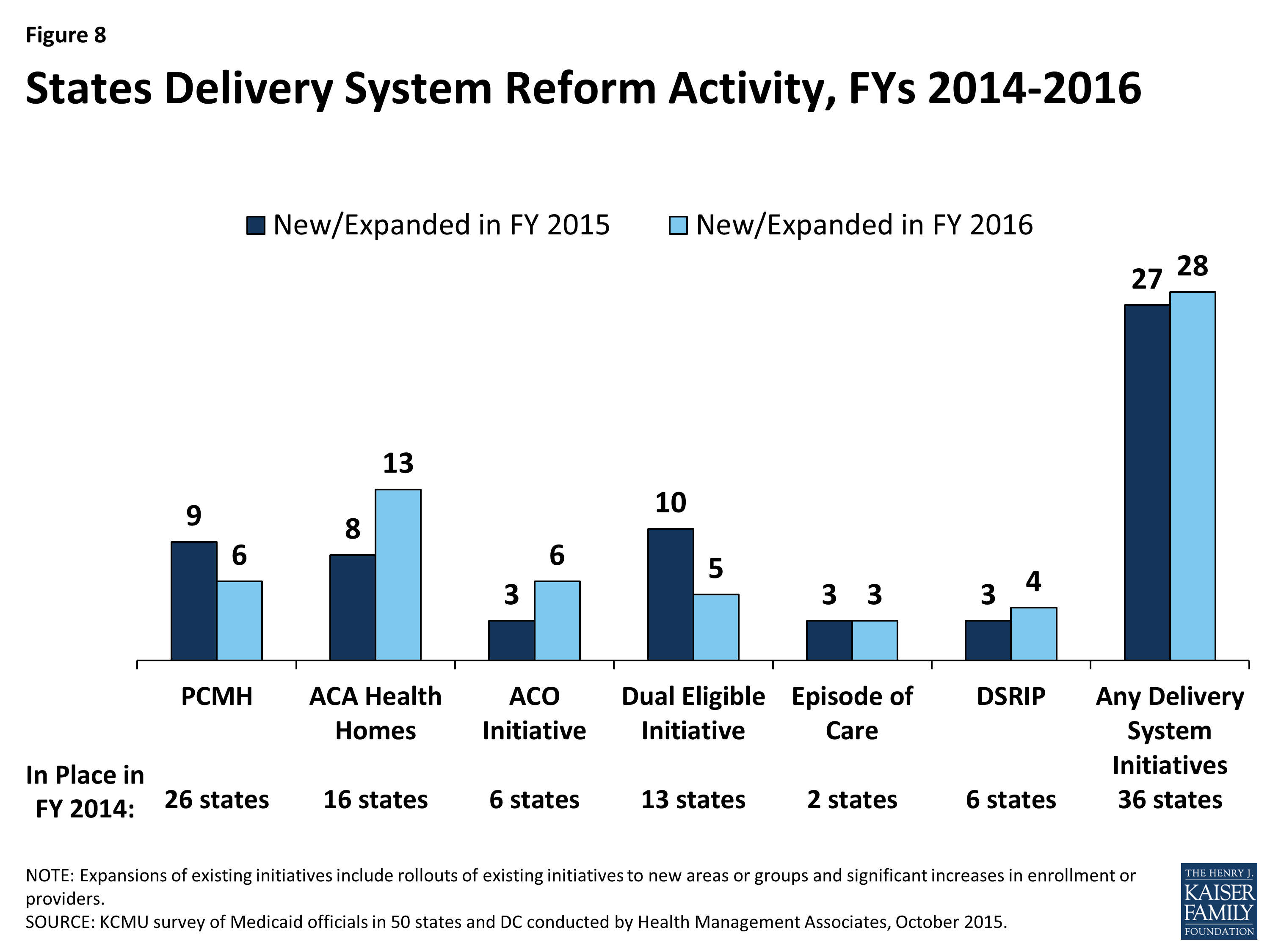
Figure 8: States Delivery System Reform Activity, FYs 2014-2016
Patient-Centered Medicaid Homes (PCMHs)
Patient-centered medical home initiatives operated in half (26) of Medicaid programs in FY 2014. Under a PCMH model, a physician-led, multi-disciplinary care team holistically manages the patient’s ongoing care, including recommended preventive services, care for chronic conditions and access to social services and supports. Generally, providers or provider organizations that operate as a PCMH seek recognition from organizations like the National Committee for Quality Assurance (NCQA).1 PCMHs are often paid (by state Medicaid agencies directly or through MCO contracts) a PMPM fee in addition to regular FFS payments for their Medicaid patients.2
In this year’s survey, nine states reported having adopted or expanded PCMHs in FY 2015 and six states indicated plans to do so in FY 2016. Several of these states reported significant expansions. For example, Connecticut has made significant investments in recent years to help primary care practices obtain NCQA PCMH recognition. Over one-third of Connecticut’s Medicaid beneficiaries are served by PCMHs and the state is considering expanding the model beyond primary care. Wyoming, a state without MCO or PCCM programs, implemented PCMHs in FY 2015; the state is expanding the number of large practices participating. Idaho also reported expanding the number of practices participating in the state’s PCMH program, with the goal of covering 80 percent of the state’s population over the next four years. Other states with well-established managed care programs reported harmonizing PCMH requirements across their MCOs (Tennessee) and requiring MCOs to establish pilot medical homes for behavioral health, targeting adults with serious mental illness (Virginia).
In contrast, Massachusetts reported that its PCMH demonstration ended in March 2014, but was followed by the launch of the state’s three-year Primary Care Payment Reform Demonstration covering nearly 90,000 lives. Also, Pennsylvania reported that one of its MCOs participated in the CMMI Multi-Payer Advanced Primary Care Practice demonstration (that included Medicaid) that ended in 2014, but is considering expanding PCMH payments under future managed care contracts.
ACA Health Homes
Nearly one-third of states (16) had at least one Health Home initiative in place in FY 2014. This option, created under Section 2703 of the ACA, builds on the PCMH concept. It requires states to target beneficiaries who have at least two chronic conditions (or one and risk of a second, or a serious and persistent mental health condition), and provide a person-centered system of care that facilitates access to and coordination of the full array of primary and acute physical health services, behavioral health care, and long-term services and supports. This includes services such as comprehensive care management, referrals to community and social support services and the use of Health Information Technology (HIT) to link services, among others. States receive a 90 percent federal match rate for qualified Health Home service expenditures for eight quarters under each Health Home state plan amendment; states can (and have) created more than one Health Home program to target different populations.
In this survey, eight states reported having adopted or expanded Health Homes in FY 2015 and 13 states reported plans to do so in FY 2016. Nearly all states noted that they were focusing their Health Home programs on populations with behavioral health conditions. States are also incorporating Health Homes into larger reform efforts related to integrating physical and behavioral health. For example, Tennessee is planning to implement Health Homes statewide for individuals with severe and persistent mental illness in 2016; this is part of a larger effort to develop a multi-payer PCMH program that the state plans to expand statewide by 2018.
Two states reported that they ended their Health Homes during this period. Oregon ended its Health Home initiative on September 30, 2013, when the enhanced federal payments ended, but the state continues to expand the use of PCMHs. Washington’s Health Home program, which provided additional coordination and other Health Home services for those dually-eligible for Medicare and Medicaid as well as other Medicaid beneficiaries with at least one chronic condition and at risk of developing another, is ending December 31, 2015. The state is working with beneficiaries to transition them to other care management services.
Accountable Care Organizations (ACOs)
States continue to experiment with accountable care organizations as the concept evolves. Six states reported having ACO models in place for at least some of their Medicaid beneficiaries in FY 2014. While there is currently no uniform, commonly accepted federal definition of an ACO, an ACO generally refers to a group of health care providers or, in some cases, a regional entity that contracts with providers and/or health plans, that agrees to share responsibility for the health care delivery and outcomes for a defined population.3 An ACO that meets quality performance standards that have been set by the payer and achieves savings relative to a benchmark can share in the savings. The organizational structure of ACOs varies, but ACOs generally include primary and specialty care physicians and at least one hospital. Virtually all states with ACO initiatives built on existing care delivery programs (e.g., PCCM, medical homes, MCOs) that already involved some degree of coordination among providers and likely had key infrastructure to facilitate coordination among ACO providers (e.g., electronic medical records). States use different terminology in referring to their Medicaid ACO initiatives, such as Coordinated Care Organizations (CCOs) in Oregon and Regional Care Collaborative Organizations (RCCOs) in Colorado.4
In this survey, three states reported adopting or expanding ACOs in FY 2015 and six states reported such activity in FY 2016. This includes states like Maine, Massachusetts, and New Jersey that have implemented or are planning to implement new ACO models. Utah reported plans to expand their ACO model to new counties. Other states reported ACO activity spurred by MCO contract requirements (Iowa, New Mexico and Minnesota) or as part of larger Section 1115 waiver proposals (California).
| New Jersey ACO Demonstration |
| In July 2015, New Jersey kicked off the Medicaid ACO Demonstration Project, which focuses on improving health outcomes, quality and access to care through regional collaboration, and shared accountability while reducing costs. The Medicaid ACO Demonstration Project provides the New Jersey Medicaid program an opportunity to explore innovative system re-design including: testing the ACO as an alternative to managed care; evaluating how care management and care coordination could be delivered to high-risk, high-cost utilizers; stretching the role of Medicaid beyond medical services to integrate social services; and testing payment reform models including pay for performance metrics and incentives. |
Care Coordination and Integration of Care for Dual Eligible Beneficiaries
Coordinating care for those dually eligible for Medicare and Medicaid (dual eligible beneficiaries) is a significant issue for Medicaid programs. These individuals tend to have significant health needs, a high prevalence of chronic conditions and substantial need for long-term services and supports. Prior to the ACA, coordination of care for individuals with dual enrollment in Medicaid and Medicare had been difficult to pursue for states in part because of misalignment between Medicare and Medicaid laws. In addition, when states did develop approaches to better coordinate care, any resulting savings from improvements in acute care (such as reduced inpatient admissions, readmissions and emergency room visits) accrued to Medicare and were not shared with state Medicaid programs. Under Section 2602 of the ACA, CMS established the Medicare-Medicaid Coordination Office (MMCO) and initiated Financial Alignment Demonstrations (FADs) with interested states seeking to coordinate and improve care and control costs for those dually eligible for Medicare and Medicaid.
In this survey, 13 states indicated that initiatives to coordinate care for dual eligible beneficiaries were in place in FY 2014, including seven with CMS FADs and seven with initiatives outside the CMS FAD that centered on enrolling this population in comprehensive MCOs or managed long-term care plans (one state had both a FAD and a non-FAD initiative). Ten states reported implementing or expanding an initiative to coordinate care for dual eligible beneficiaries in FY 2015, including six states with FADs, two of which (California and Texas) implemented or expanded other initiatives such as MLTSS outside of the FAD initiative. For FY 2016, five states are planning to implement or expand an initiative including one state planning a FAD. Initiatives outside of the FADs included alignment of Medicare Advantage Special Needs Plans for dual eligible beneficiaries (D-SNPs) with Medicaid MCOs and enrollment of dual eligible beneficiaries in comprehensive Medicaid MCOs (for acute care services) or managed long-term care.
| Selected Dual Eligible Care Coordination Initiatives (Outside of Financial Alignment Demonstrations) |
| Arizona is working to increase alignment and improve service delivery for dual eligible beneficiaries by contractually requiring its health plans to also serve as Medicare Dual Special Needs Plans (D-SNPs) and promoting enrollment of dual eligible beneficiaries into the same health plan for both Medicaid and Medicare to the greatest extent possible. Enrolling in specialized duals-only Medicare plans allows individuals to receive all of their health care, including the payment for prescriptions and benefits, from a single, integrated source.
Florida reported contracting with a specialty Medicaid managed care plan beginning in FY 2015 that caters to dual eligible beneficiaries with chronic conditions. |
Episode-of-Care Initiatives
Unlike fee-for-service (FFS) reimbursement where providers are paid separately for each service, or capitation where a health plan receives a per member per month (PMPM) payment intended to cover the costs for all covered services, an episode-of-care payment is linked to the care that a patient receives for a defined condition or health event (e.g., pregnancy and delivery, heart attack, or knee replacement). Episode-based payments usually involve payment for multiple services and providers and therefore create a financial incentive for physicians, hospitals and other providers to work together to improve patient care and manage costs. In this survey, two states (Arkansas and Tennessee) noted that an episode-of-care initiative was in place in FY 2014. Both states indicated that they continued to expand these initiatives in FY 2015 and FY 2016. New Mexico reported that a small pilot is being operated by some of the state’s MCOs in FY 2015 and Louisiana reported that one MCO planned a demonstration in partnership with a birthing hospital in FY 2016. Additionally, Ohio is currently in an episode-of-care reporting year; gain-sharing payments will begin in calendar year 2017.
Hospital Delivery System Reform Incentive Payment (DSRIP) Program
Delivery System Reform Incentive Payment (DSRIP) programs are another piece of the dynamic and evolving Medicaid delivery system reform landscape. DSRIP initiatives, which are part of broader Section 1115 demonstration waiver programs, provide states with significant funding to support hospitals and other providers in changing how they provide care to Medicaid beneficiaries. DSRIP waivers are not grant programs – they are performance-based incentive programs. Originally, DSRIP initiatives were more narrowly focused on funding for safety-net hospitals and often grew out of negotiations between states and HHS over the appropriate way to finance hospital care. Now, however, they are used to promote far more sweeping payment and delivery system reforms.
The first DSRIP initiatives were approved and implemented in California and Texas in 2010 and 2011, followed by New Jersey, Kansas and Massachusetts in 2012 and 2013. In this year’s survey, Massachusetts reported expanding its DSRIP program and New Mexico and New York reported implementing DSRIP programs in FY 2015. For FY 2016, California and New Mexico reported DSRIP enhancements while New Hampshire and Washington reported plans to seek approval for new DSRIP initiatives.
Other Initiatives
In addition to the initiatives discussed already, states reported other delivery system and payment reform initiatives. For example, some states reported including value-based purchasing requirements in their managed care contracts (Arizona, Iowa, Michigan, and Texas). Pennsylvania reported plans to include a “health-home like” program in its 2016 MCO contracts. Other states reported expanding telehealth services and use of community health workers (New Mexico), creating a coordinated point of entry for substance abuse disorder treatment services (New Jersey) and offering subsidies to enable ambulatory practices to access health information exchange services and achieve Meaningful Use (North Carolina).
| All-Payer Claims Database |
| All-payer claims database (APCD) systems are large-scale databases that systematically collect medical claims, pharmacy claims, dental claims (typically, but not always), and eligibility and provider files from both private and public payers. They can be a valuable tool for identifying areas to focus reform efforts and for other purposes. Ten states (Colorado, Massachusetts, Maine, Minnesota, Montana, New Hampshire, Oregon, Rhode Island, Tennessee and Virginia) reported having APCDs in place while two states (California and Washington) planned to implement APCDs in FY 2016. |
Table 11: Delivery System and Payment Reform Initiatives in Place in all 50 States and DC in FY 2014
| States | Patient-Centered Medical Homes (PCMH) |
ACA Health Homes | Accountable Care Organizations (ACO) | Dual Eligible Initiatives | Episode of Care Payments | Delivery System Reform Incentive Payment Program (DSRIP) | Other Initiatives | Any of these Initiatives in Place in FY 2014 |
| Alabama | X | X | X | |||||
| Alaska | ||||||||
| Arizona | X | X | X | |||||
| Arkansas | X | X | X | |||||
| California | X* | X | X | |||||
| Colorado | X | X | X* | X | ||||
| Connecticut | X | X | ||||||
| Delaware | ||||||||
| DC | ||||||||
| Florida | ||||||||
| Georgia | ||||||||
| Hawaii | X | X | ||||||
| Idaho | X | X | X | X | ||||
| Illinois | X* | X | ||||||
| Indiana | ||||||||
| Iowa | X | X | X | |||||
| Kansas | X | X | X | |||||
| Kentucky | ||||||||
| Louisiana | ||||||||
| Maine | X | X | X | |||||
| Maryland | X | X | X | |||||
| Massachusetts | X | X* | X | X | ||||
| Michigan | X | X | X | |||||
| Minnesota | X | X | X | X | ||||
| Mississippi | ||||||||
| Missouri | X | X | ||||||
| Montana | ||||||||
| Nebraska | X | X | ||||||
| Nevada | ||||||||
| New Hampshire | ||||||||
| New Jersey | X | X | X | X | ||||
| New Mexico | X | X | X | X | ||||
| New York | X | X | X | |||||
| North Carolina | X | X | ||||||
| North Dakota | ||||||||
| Ohio | X | X* | X | |||||
| Oklahoma | X | X | ||||||
| Oregon | X | X | X | X | X | |||
| Pennsylvania | X | X | ||||||
| Rhode Island | X | X | X | X | ||||
| South Carolina | X | X | ||||||
| South Dakota | X | X | ||||||
| Tennessee | X | X | X | |||||
| Texas | X | X | X | X | ||||
| Utah | X | X | ||||||
| Vermont | X | X | X | X | ||||
| Virginia | X | X* | X | |||||
| Washington | X | X* | X | |||||
| West Virginia | ||||||||
| Wisconsin | X | X | X | |||||
| Wyoming | ||||||||
| Totals | 26 | 16 | 6 | 13 | 2 | 6 | 3 | 36 |
| NOTES: Dually Eligible Initiatives: X* = State is pursuing a Financial Alignment Demonstration. CA reported another dual initiative in place outside of the demonstration.
SOURCE: Kaiser Commission on Medicaid and the Uninsured Survey of Medicaid Officials in 50 states and DC conducted by Health Management Associates, October 2015. |
||||||||
Table 12: Delivery System and Payment Reform Actions Taken in all 50 States and DC, FY 2015 and 2016
| States | Patient-Centered Medical Homes (PCMH) |
ACA Health Homes | Accountable Care Organizations (ACO) | Dual Eligible Initiatives | Episode of Care Payments | Delivery System Reform Incentive Payment Program (DSRIP) |
Other Initiatives | Any New or Expanded Initiative | ||||||||
| 2015 | 2016 | 2015 | 2016 | 2015 | 2016 | 2015 | 2016 | 2015 | 2016 | 2015 | 2016 | 2015 | 2016 | 2015 | 2016 | |
| Alabama | X | X | ||||||||||||||
| Alaska | ||||||||||||||||
| Arizona | X | X | X | X | X | X | ||||||||||
| Arkansas | X | X | X | X | ||||||||||||
| California | X | X | X* | X | X | X | ||||||||||
| Colorado | ||||||||||||||||
| Connecticut | X | X | X | X | ||||||||||||
| Delaware | X | X | X | X | ||||||||||||
| DC | X | X | ||||||||||||||
| Florida | X | X | ||||||||||||||
| Georgia | ||||||||||||||||
| Hawaii | ||||||||||||||||
| Idaho | X | X | ||||||||||||||
| Illinois | X | X | ||||||||||||||
| Indiana | ||||||||||||||||
| Iowa | X | X | X | X | X | X | ||||||||||
| Kansas | ||||||||||||||||
| Kentucky | X | X | ||||||||||||||
| Louisiana | X | X | X | |||||||||||||
| Maine | X | X | X | |||||||||||||
| Maryland | ||||||||||||||||
| Massachusetts | X | X | X | X | X | |||||||||||
| Michigan | X | X | X* | X | X | X | ||||||||||
| Minnesota | X | X | ||||||||||||||
| Mississippi | ||||||||||||||||
| Missouri | X | X | X | X | ||||||||||||
| Montana | X | X | X | X | ||||||||||||
| Nebraska | ||||||||||||||||
| Nevada | ||||||||||||||||
| New Hampshire | X | X | ||||||||||||||
| New Jersey | X | X | X | X | X | X | X | X | ||||||||
| New Mexico | X | X | X | X | X | X | X | X | X | X | ||||||
| New York | X | X | X* | X | X | X | ||||||||||
| North Carolina | X | X | ||||||||||||||
| North Dakota | ||||||||||||||||
| Ohio | X* | X | ||||||||||||||
| Oklahoma | X | X | X | |||||||||||||
| Oregon | X | X | X | X | ||||||||||||
| Pennsylvania | X | X | ||||||||||||||
| Rhode Island | X* | X | ||||||||||||||
| South Carolina | X* | X | ||||||||||||||
| South Dakota | ||||||||||||||||
| Tennessee | X | X | X | X | X | X | X | |||||||||
| Texas | X* | X | ||||||||||||||
| Utah | X | X | ||||||||||||||
| Vermont | ||||||||||||||||
| Virginia | X | X | X | X | ||||||||||||
| Washington | X | X | ||||||||||||||
| West Virginia | X | X | X | X | ||||||||||||
| Wisconsin | ||||||||||||||||
| Wyoming | X | X | X | X | ||||||||||||
| Totals | 9 | 6 | 8 | 13 | 3 | 6 | 10 | 5 | 3 | 3 | 3 | 4 | 3 | 6 | 27 | 28 |
| NOTES: Expansions of existing initiatives include rollouts of existing initiatives to new areas or groups and significant increases in enrollment or providers. Dually Eligible Intiatives: X* = State is pursuing a Financial Alignment Demonstration. CA and TX reported other FY 2015 initiatives outside of the demonstration.
SOURCE: Kaiser Commission on Medicaid and the Uninsured Survey of Medicaid Officials in 50 states and DC conducted by Health Management Associates, October 2015. |
||||||||||||||||
Long-Term Services and Supports Reforms
| Key Section Findings |
Additional information on LTSS expansions implemented in FY 2015 or planned for FY 2016 can be found in Tables 13 and 14. These tables are also available in a downloadable PDF. |
Medicaid is the nation’s primary payer for long-term services and supports (LTSS) covering a continuum of services ranging from home and community-based services (HCBS) that allow persons to live independently in their own homes or in the community, to institutional care provided in nursing facilities and intermediate care facilities for individuals with intellectual disabilities (ICF-ID). Long-term services and supports represent at least one-third of Medicaid spending and are an important focus for state policymakers.1 This year’s survey shows that almost all states are employing a variety of tools and strategies to expand HCBS options including traditional Section 1915(c) HCBS waivers, PACE programs,2 and managed LTSS.
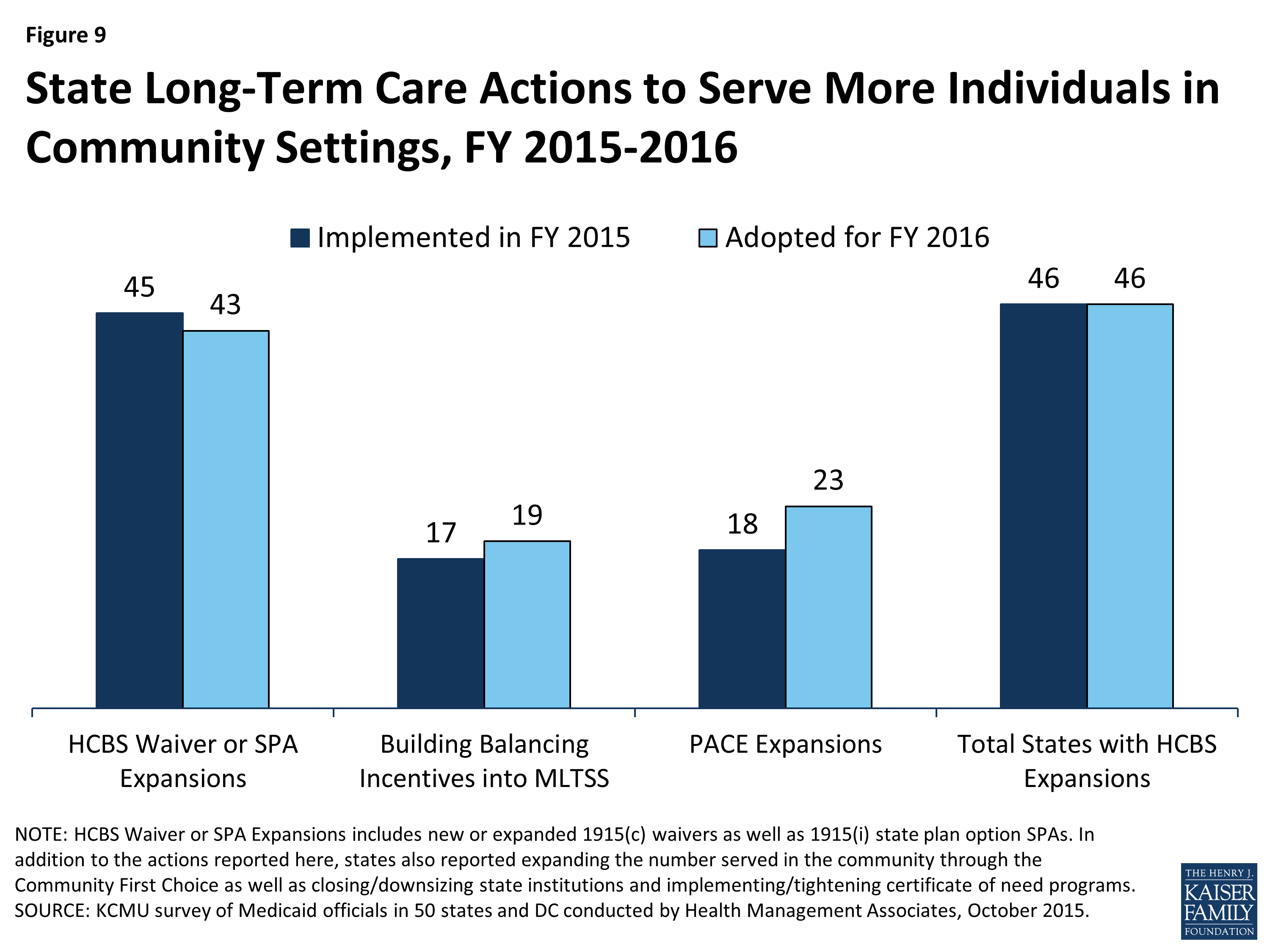
Figure 9: State Long-Term Care Actions to Serve More Individuals in Community Settings, FY 2015-2016
Nearly every state reported actions to expand the number of persons served in community settings in both years (46 states in FY 2015 and in FY 2016). The number of states taking such actions has increased since FY 2012 (26 states) and FY 2013 (22 states). While virtually every state reported using Section 1915(c) waivers or Section 1915(i) state plan authority to expand HCBS, a significant number of states (17 in FY 2015 and 19 in FY 2016) also reported that the incentives built into their managed care programs were expected to increase the availability of HCBS. Also, 18 states in FY 2015 and 23 states in FY 2016 reported implementing or expanding PACE programs. (Figure 9) A number of states (15 states in FY 2015 and 15 in FY 2016) reported closing or downsizing institutions that led to more community placements and several states (four states in FY 2015 and three states in FY 2016) reported implementing or tightening a Certificate of Need program or imposing a moratorium on construction of new institutional beds. States also reported increased take up of ACA options to expand community-based LTSS (discussed below).
Several states reported on a number of other rebalancing initiatives. California reported that its Department of Health Care Services will collaborate with its Department of Housing and Community Development to award rental subsidies to developers and Medi-Cal community-based organizations (CBOs) using grant awards received from the U.S. Department of Housing and Urban Development. The CBOs will use the subsidies to transition institutionalized or homeless Medi-Cal beneficiaries into private independent living settings partnered with home and community-based services.3 Connecticut reported that it was continuing to implement its Strategic Plan to Rebalance Long-Term Services and Supports including a second round of rebalancing grant awards, announced by Governor Malloy in May 2015, to help the state’s nursing home industry diversify services to meet the changing needs of older adults and other people with disabilities. Several states also noted the implementation of conflict-free case management and single points of entry4 and one state commented that it was in the process of developing and testing a uniform assessment tool that, in the future, should have a positive impact on rebalancing the LTSS system.
Three states (Iowa, Illinois and Tennessee) reported new HCBS restrictions or limitations in FY 2015 or FY 2016: Iowa reported that its HCBS waiver for persons with intellectual and developmental disabilities (IDD) had reached its federally approved enrollment cap causing the state to implement a waiting list in FY 2015; Illinois reported that it is planning to change its Level of Care criteria for nursing homes as part of a legislative mandate which will also reduce the number of persons eligible for Section 1915(c) waiver services; and in FY 2016, Tennessee will also begin limiting new enrollment into a Section 1915(i)-like group (offered under Section 1115 authority) to SSI eligible beneficiaries only. People already enrolled in the group under institutional income standards will be grandfathered.5
Long-Term Services and Supports Options in the ACA
The ACA created and expanded several LTSS-related options intended to promote LTSS rebalancing. This year’s survey asked about two LTSS-related options intended to promote LTSS rebalancing that were created or expanded by the ACA: the Community First Choice Option and the Section 1915(i) HCBS State Plan Option. Thirteen (13) states reported having at least one of these options in place in FY 2014; six states reported implementing at least one of these options in FY 2015 and eight reported plans to do so in FY 2016. (Figure 10) State utilization of each of these options is discussed below.
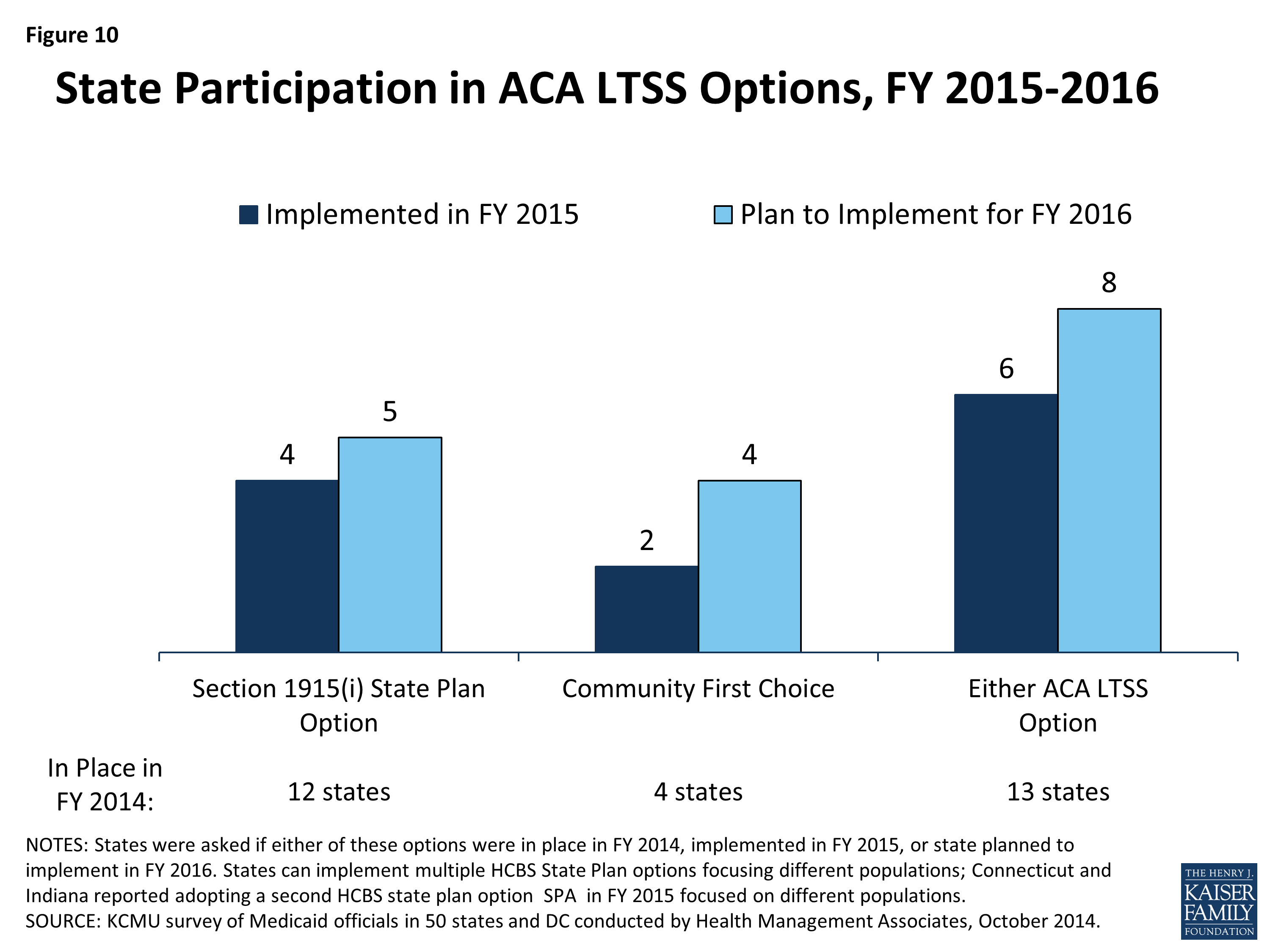
Figure 10: State Participation in ACA LTSS Options, FY 2015-2016
An additional program, the Balancing Incentive Program (BIP) was created under the ACA to provide enhanced Medicaid matching funds to certain states that meet requirements for expanding the share of LTSS spending for HCBS (and reducing the share of LTSS spending for institutional services). The enhanced funding ended in September 2015. For more information on the impact of this program, please see the following brief.6
Section 1915(i) HCBS State Plan Option
This option allows states to offer HCBS through a Medicaid state plan amendment (SPA) rather than through a Section 1915(c) waiver. As a result of changes made in the ACA, income eligibility for this option was extended up to 300 percent of the maximum SSI federal benefit rate and states were permitted to target benefits to specific populations and offer the same range of HCBS under Section 1915(i) as are available under Section 1915(c) waivers. Unlike Section 1915(c) waivers, however, states are not permitted to cap enrollment or maintain a waiting list and, if offered, the benefit must be available statewide. If enrollment exceeds the state’s projections, the state may tighten their Section 1915(i) needs-based eligibility criteria, subject to advance notice and grandfathering of existing beneficiaries. Twelve states reported having an HCBS state plan option in place in FY 2014. Four states (Connecticut, Delaware, DC and Indiana) reported implementing in FY 2015; Connecticut and Indiana already had 1915(i) SPAs in place but implemented additional ones in FY 2015. Five states (Maryland, Minnesota, Mississippi, New York and Texas) reported plans to implement in FY 2016.
States were also asked to describe the target populations for their Section 1915(i) SPAs. Adults with significant mental health needs were identified by the largest number of states (7) followed by persons with intellectual and developmental disabilities (5), children with significant mental health needs (4), the elderly (3) and persons with vision impairments or physical disabilities (1). For some states, the target population included more than one of these categories. Also, two states (Connecticut and Idaho) have two Section 1915(i) SPAs in place, while Indiana implemented a third Section 1915(i) SPA in FY 2015 for adults diagnosed with mental health conditions and have incomes below 300 percent of the supplemental security income benefit rate (SSI), including persons who lost Medicaid coverage when the state’s spend-down program was eliminated.7
Community First Choice (CFC) State Plan Option
States electing this State Plan option to provide Medicaid-funded home and community-based attendant services and supports receive an FMAP increase of six percentage points for CFC services. In this year’s survey, four states (California, Maryland, Montana and Oregon) reported having CFC in place in FY 2014. Two states reported implementing this option in FY 2015 (New York8 and Texas), and four states reported plans to implement in FY 2016 (Connecticut, Delaware, Minnesota and Washington).
| Texas LTSS Transformation Initiatives |
|
In the last two years, Texas has implemented a number of initiatives to transform delivery of long-term care services and supports. Through managed care, the state has expanded its managed LTSS program statewide, carved nursing facility services into its managed care contracts and shifted acute care health services for individuals in its Section 1915(c) ICF/IDD waivers into managed care. Texas has also nearly completed implementation of the structural changes required under the Balancing Incentive Program (e.g., statewide expansion of the Aging and Disability Resource Centers and the automated LTSS Screening and Referral System) and implemented the Community First Choice Option. These initiatives combined with implementation of the Department of Labor rule on minimum wage and overtime for direct care workers and the HCBS settings final rule amount to the state undergoing an unprecedented transformation in a short timeframe. Texas is planning additional initiatives to further transform its delivery of long-term care services and supports. For example, the state is planning to implement the STAR Kids managed care program for children with disabilities, to do a pilot program for serving individuals with IDD in managed care, and eventually to carve into managed care long-term care services for those in the state’s IDD waiver. As part of the nursing facility carve-in initiative, Texas is also developing performance measures to monitor admissions and readmissions to nursing facilities with the goal of ensuring appropriate utilization of nursing facility services and reducing unnecessary institutionalizations. |
| HCBS Settings Rule |
| In January 2014, CMS issued a new HCBS regulation (the “HCBS Rule”) making a number of significant program changes including the addition of new requirements that define the qualities of settings that are eligible for Medicaid reimbursement under Section 1915(c) waivers, the Section 1915(i) HCBS State Plan Option and the Community First Choice Option.9 The HCBS Rule includes a transitional process for states to ensure that their waivers and state plans meet the HCBS settings requirements including a requirement for each state to submit a Statewide Transition Plan. In this year’s survey, states were asked to comment on significant issues, concerns or opportunities that have emerged to date related to the implementation of their HCBS Statewide Transition Plans.
States expressed concerns around the administrative cost and staffing challenges associated with implementation of the Statewide Transition Plan as well as evaluating and completing on-site provider assessments and validating provider self-assessments. States also highlighted challenges in terms of provider compliance and consumer impact concerns including loss of providers and services valued by consumers and the potential for service disruptions when consumers are transitioned to compliant settings. A few states commented on delays in CMS feedback on submitted plans while three states indicated that more CMS guidance would be helpful. A few states also expressed concerns about the challenges faced in rural areas and those associated with specific sub-populations (e.g. beneficiaries with behavioral issues that pose a risk to the public). On the other hand, some states cited opportunities presented by the HCBS Rule for increasing consumer choice and autonomy, increasing HCBS quality, ensuring more person-centered and person-directed service planning and provision, and providing new opportunities to work across state agencies and divisions. |
Table 13: Long-Term Care Expansions in all 50 States and DC, FY 2015 and 2016
| HCBS Waiver or SPA Expansions | Building Balancing Incentives in MLTSS | PACE Expansions | Total States with HCBS Expansions | |||||
| 2015 | 2016 | 2015 | 2016 | 2015 | 2016 | 2015 | 2016 | |
| Alabama | X | X | X | X | ||||
| Alaska | ||||||||
| Arizona | ||||||||
| Arkansas | X | X | ||||||
| California | X | X | X | X | X | X | X | X |
| Colorado | X | X | X | X | X | |||
| Connecticut | X | X | X | X | ||||
| Delaware | X | X | X | X | X | X | X | |
| DC | X | X | X | X | X | |||
| Florida | X | X | X | X | X | X | X | X |
| Georgia | X | X | ||||||
| Hawaii | X | X | X | X | ||||
| Idaho | X | X | X | X | ||||
| Illinois | X | X | X | X | X | X | ||
| Indiana | X | X | X | X | X | X | ||
| Iowa | X | X | X | X | X | |||
| Kansas | X | X | X | X | ||||
| Kentucky | X | X | X | X | ||||
| Louisiana | X | X | X | X | X | X | ||
| Maine | X | X | X | X | ||||
| Maryland | X | X | ||||||
| Massachusetts | X | X | X | X | X | X | X | X |
| Michigan | X | X | X | X | X | X | X | X |
| Minnesota | X | X | X | X | X | X | ||
| Mississippi | X | X | X | X | ||||
| Missouri | X | X | X | X | ||||
| Montana | X | X | X | X | ||||
| Nebraska | X | X | X | X | X | |||
| Nevada | X | X | X | X | ||||
| New Hampshire | X | X | X | X | ||||
| New Jersey | X | X | X | X | X | X | X | X |
| New Mexico | X | X | X | X | X | X | ||
| New York | X | X | X | X | X | X | X | X |
| North Carolina | X | X | ||||||
| North Dakota | X | X | X | |||||
| Ohio | X | X | X | X | X | X | ||
| Oklahoma | X | X | X | X | X | X | ||
| Oregon | X | X | X | X | X | X | ||
| Pennsylvania | X | X | X | X | X | X | ||
| Rhode Island | X | X | X | X | X | X | X | X |
| South Carolina | X | X | X | X | X | X | X | |
| South Dakota | X | X | X | X | ||||
| Tennessee | X | X | X | X | X | X | ||
| Texas | X | X | X | X | X | X | X | X |
| Utah | X | X | X | X | ||||
| Vermont | X | X | X | X | ||||
| Virginia | X | X | X | X | X | X | X | X |
| Washington | X | X | X | X | X | X | ||
| West Virginia | X | X | ||||||
| Wisconsin | X | X | X | X | X | X | ||
| Wyoming | X | X | X | X | X | X | ||
| Totals | 45 | 43 | 17 | 19 | 18 | 23 | 46 | 46 |
| NOTES: “HCBS Expansion” includes both expansions of 1915(c) waivers as well as 1915(i) State Plan Options SPAs. In addition to the actions reported here, states also reported expanding the number served in the community through the ACA Community First Choice Option as well as closing/downsizing state institutions and implementing/tightening certificate of need programs.
SOURCE: Kaiser Commission on Medicaid and the Uninsured Survey of Medicaid Officials in 50 states and DC conducted by Health Management Associates, October 2015. |
||||||||
Table 14: State Adoption of ACA LTSS Options in all 50 States and DC, FY 2014 – 2016
| 1915(i) State Plan Option | Community First Choice | Any ACA LTC Option | |||||||
| In Place | New in: | In Place | New in: | In Place | New in: | ||||
| 2014 | 2015 | 2016 | 2014 | 2015 | 2016 | 2014 | 2015 | 2016 | |
| Alabama | |||||||||
| Alaska | |||||||||
| Arizona | |||||||||
| Arkansas | |||||||||
| California | X | X | X | ||||||
| Colorado | X | X | |||||||
| Connecticut | X | X | X | X | X | X | |||
| Delaware | X | X | X | X | |||||
| DC | X | X | |||||||
| Florida | X | X | |||||||
| Georgia | |||||||||
| Hawaii | |||||||||
| Idaho | X | X | |||||||
| Illinois | |||||||||
| Indiana | X | X | X | X | |||||
| Iowa | X | X | |||||||
| Kansas | |||||||||
| Kentucky | |||||||||
| Louisiana | X | X | |||||||
| Maine | |||||||||
| Maryland | X | X | X | X | |||||
| Massachusetts | |||||||||
| Michigan | |||||||||
| Minnesota | X | X | X | ||||||
| Mississippi | X | X | |||||||
| Missouri | |||||||||
| Montana | X | X | X | ||||||
| Nebraska | |||||||||
| Nevada | X | X | |||||||
| New Hampshire | |||||||||
| New Jersey | |||||||||
| New Mexico | |||||||||
| New York | X | X | X | X | |||||
| North Carolina | |||||||||
| North Dakota | |||||||||
| Ohio | |||||||||
| Oklahoma | |||||||||
| Oregon | X | X | X | ||||||
| Pennsylvania | |||||||||
| Rhode Island | |||||||||
| South Carolina | |||||||||
| South Dakota | |||||||||
| Tennessee | |||||||||
| Texas | X | X | X | X | |||||
| Utah | |||||||||
| Vermont | |||||||||
| Virginia | |||||||||
| Washington | X | X | |||||||
| West Virginia | |||||||||
| Wisconsin | X | X | |||||||
| Wyoming | |||||||||
| Totals | 12 | 4 | 5 | 4 | 2 | 4 | 13 | 6 | 8 |
| NOTES: States were asked if each of these options were in place in FY 2014, implemented in FY 2015, or state planned to implement in FY 2016. States can implement multiple HCBS State Plan options focusing different populations. New York reported implementing the Community First Choice option in FY 2015, but was awaiting final SPA approval at the time of the survey.
SOURCE: Kaiser Commission on Medicaid and the Uninsured Survey of Medicaid Officials in 50 states and DC conducted by Health Management Associates, October 2015. |
|||||||||
Provider Rates, Taxes and Benefits
| Key Section Findings |
Tables 15 through 17 provide a complete listing of Medicaid provider rate changes and provider taxes and fees in place in FY 2015 and FY 2016; Tables 19 through 21 provide a complete listing of Medicaid benefit and pharmacy changes for FY 2015 and FY 2016. These tables are also available in a downloadable PDF. |
Provider Rates
State fiscal conditions have a direct impact on Medicaid provider rates. During economic downturns, states often turn to provider rate cuts to control costs. Improving state finances in recent years have resulted in more states restoring or enhancing rates than restricting rates overall. In both FY 2015 and FY 2016, more states implemented or planned rate increases (47 and 45 states) compared to rate restrictions (35 states and 38 states) in those years. (Figure 11) Data for FY 2016 was not available for Illinois as budget deliberations were in process in September 2015.1 The number of states with rate increases exceeded the number of states with restrictions in FY 2015 and FY 2016 across all major categories of providers (physicians, MCOs and nursing homes) except for inpatient rates for hospitals.2
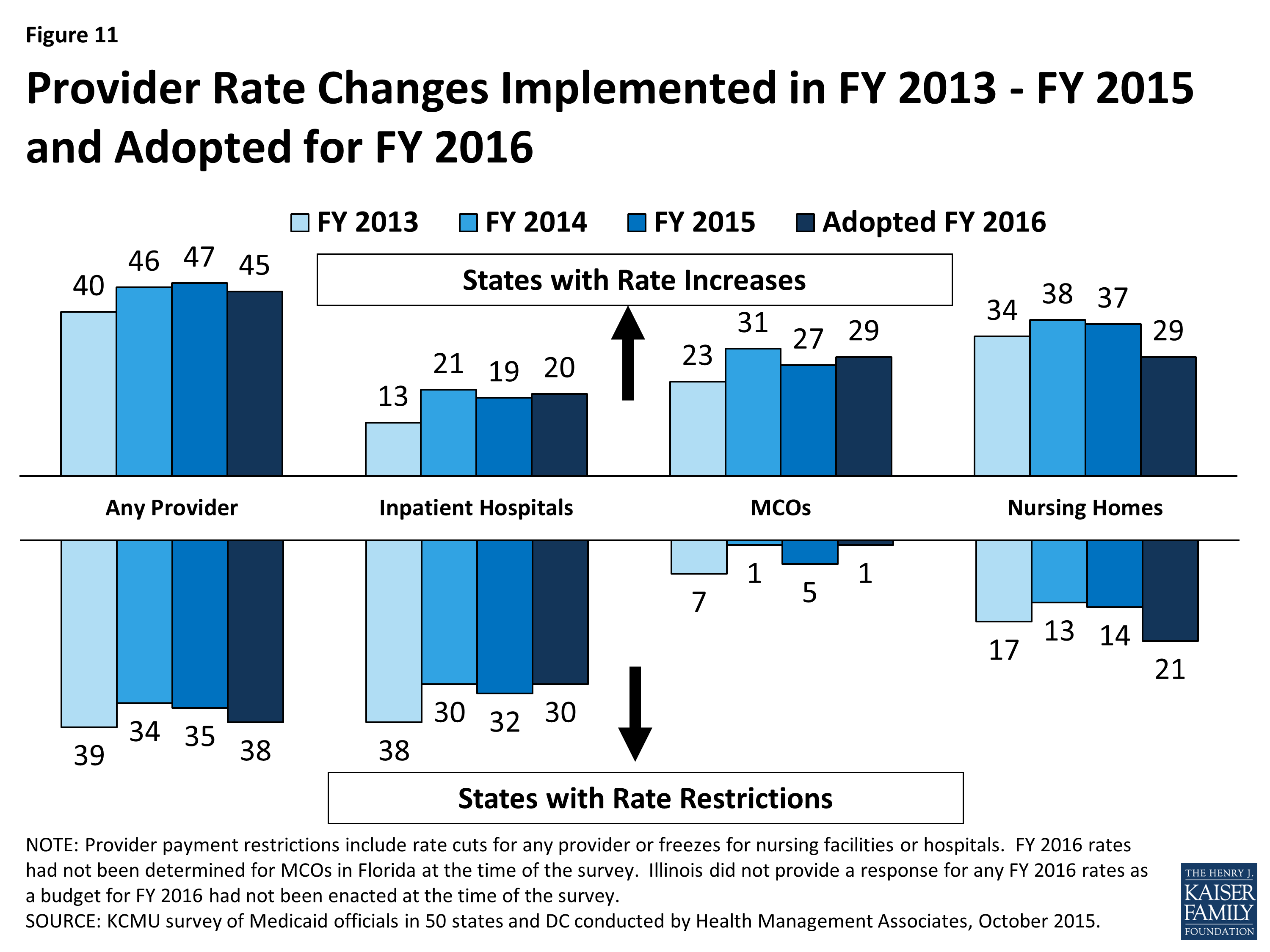
Figure 11: Provider Rate Changes Implemented in FY 2013 – FY 2015 and Adopted for FY 2016
For the purposes of this report, provider rate restrictions include cuts to fee-for-service rates for physicians, dentists, outpatient hospitals, and to capitation rates for managed care organizations, as well as cuts or freezes in rates for inpatient hospitals and nursing homes. States were asked to report aggregate changes for each major provider category. The ultimate impact of some rate changes may differ across states depending on the delivery system. For example, the effect of fee-for-service rate restrictions for hospitals, physicians, and nursing facilities rates may have less impact on providers in states that rely heavily on managed care than in states that have little or no managed care presence.
Only three states in FY 2015 and five states in FY 2016 had implemented or planned inpatient hospital rate reductions; the vast majority of hospital rate restrictions were freezes in rates. A few states noted that restrictions to inpatient hospital rates were a reflection of shifting some funding from inpatient to outpatient hospital rates. The number of states increasing nursing home rates dropped sharply in FY 2016. One state (Illinois3) cut nursing home rates in FY 2015 and four states indicated plans to cut nursing home rates in FY 2016. The other nursing home rate restrictions are rate freezes. (Figure 11)
Capitation payments for Medicaid Managed Care Organizations (MCOs) are generally bolstered by the federal requirement that states pay actuarially sound rates. In FY 2015 and FY 2016, the majority of the 39 states with Medicaid MCOs implemented or planned increases in MCO rates. Only five states reported MCO rate cuts in 2015, and only one state plans to cut MCO rates in FY 2016. To meet the federally required test of actuarial soundness, reductions to MCO rates may occur as a correction to previous rates that were set too high or to reflect reductions in fee-for-service rates or competitive price bids.
| Primary Care Payments |
The ACA included a provision to increase Medicaid payment rates for primary care services to Medicare rates from January 1, 2013 through December 31, 2014. The federal government funded 100 percent of the difference between Medicaid rates that were in effect as of July 1, 2009 and the full Medicare rates for these two years. States were asked about their plans to extend this provision for FY 2016 (at regular FMAP rates). The significance of this rate differential varies greatly across states; a 2012 survey of Medicaid physician fees showed that in a small number of states, Medicaid rates for physician services were already at or close to 100 percent of Medicare rates while other states paid sixty percent or less of Medicare rates.4
Among the states that did not continue the ACA primary care rate increase in FY 2015, seven states (Indiana, Missouri, New Jersey, New York, Ohio, South Dakota and Vermont) reported plans to increase primary care physician rates in FY 2016 from FY 2015 levels. |
In addition to primary care providers, the survey also asked about rates for specialist physicians, dentists and for outpatient services. For each of these categories, states reported more rate increases than rate cuts, particularly in FY 2015 and FY 2016. (Figure 12)
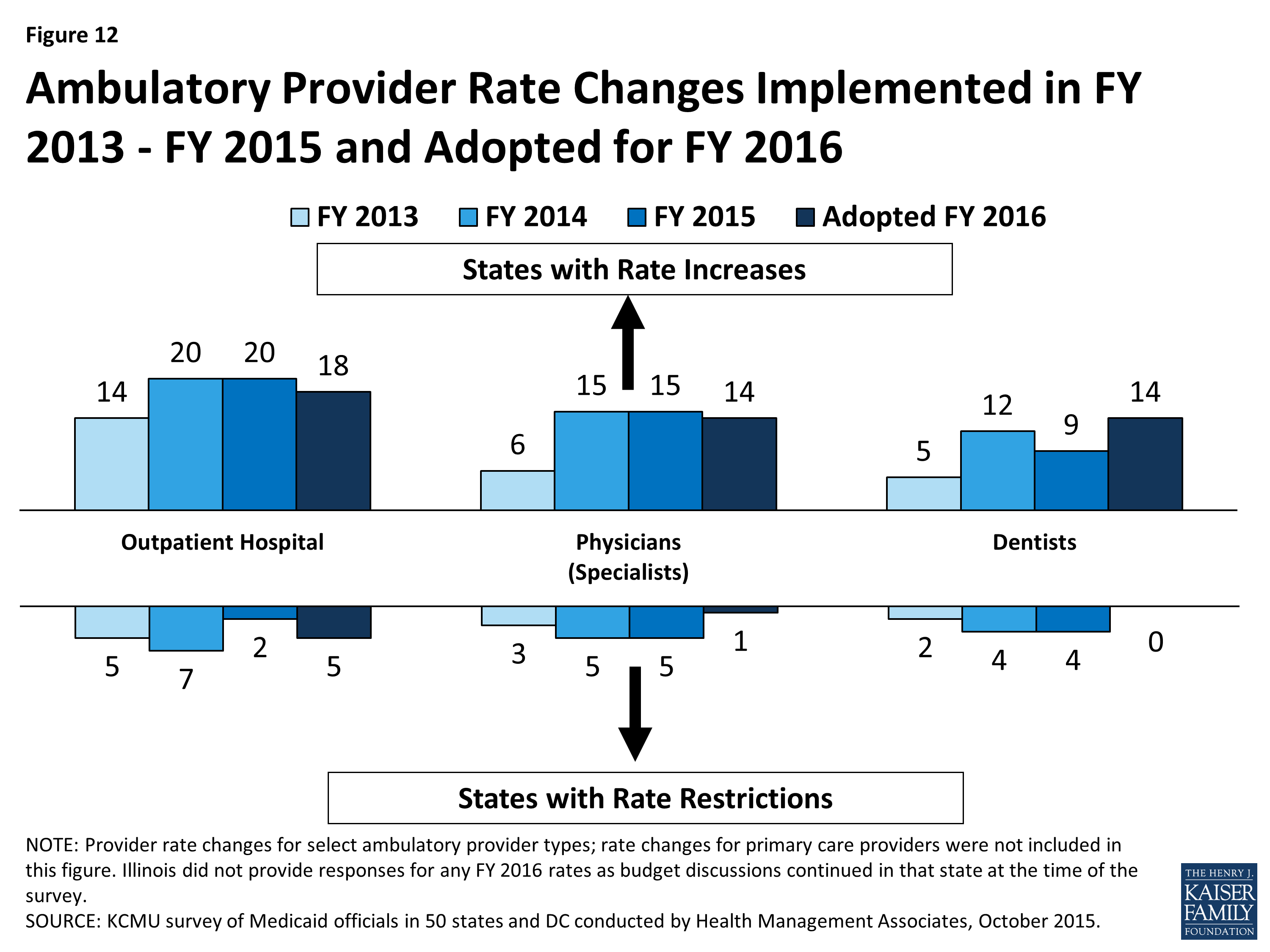
Figure 12: Ambulatory Provider Rate Changes Implemented in FY 2013 – FY 2015 and Adopted for FY 2016
Potentially Preventable Readmissions
States were asked if they had or planned to implement an inpatient hospital reimbursement incentive/policy for potentially preventable readmissions. Fifteen (15) states indicated that they had such policies in place in FY 2014 and two more states implemented such policies in FY 2015. Six states indicated that they have plans to implement in FY 2016 and an additional four states plan to implement after FY 2016.
Early Elective Deliveries
States were asked about reimbursement policies designed to reduce the number of early elective deliveries. Twenty (20) states had a policy in place in FY 2015 and six additional states plan to adopt such a policy in FY 2016. Some of the states that do not have such a policy indicated that their managed care organizations can elect to have such a policy. The most common policy was reduced payment (paying for a Cesarean-Section at the rate of a vaginal delivery) for any Cesarean-Section before 39 weeks gestational age unless there was documentation of medical necessity. States are also implementing incentive programs that reward providers for reducing the rate of early elective deliveries.
Provider Taxes and Fees
States continue to rely on provider taxes and fees to provide a portion of the non-federal share of the costs of Medicaid. At the beginning of FY 2003, a total of 21 states had at least one provider tax in place. Over the next decade, a majority of states imposed new taxes or fees and increased existing tax rates and fees to raise revenue to support Medicaid. By FY 2013, all but one state (Alaska) had at least one provider tax or fee in place.5 In FY 2015, 32 states had three or more provider taxes in place. (Figure 13)
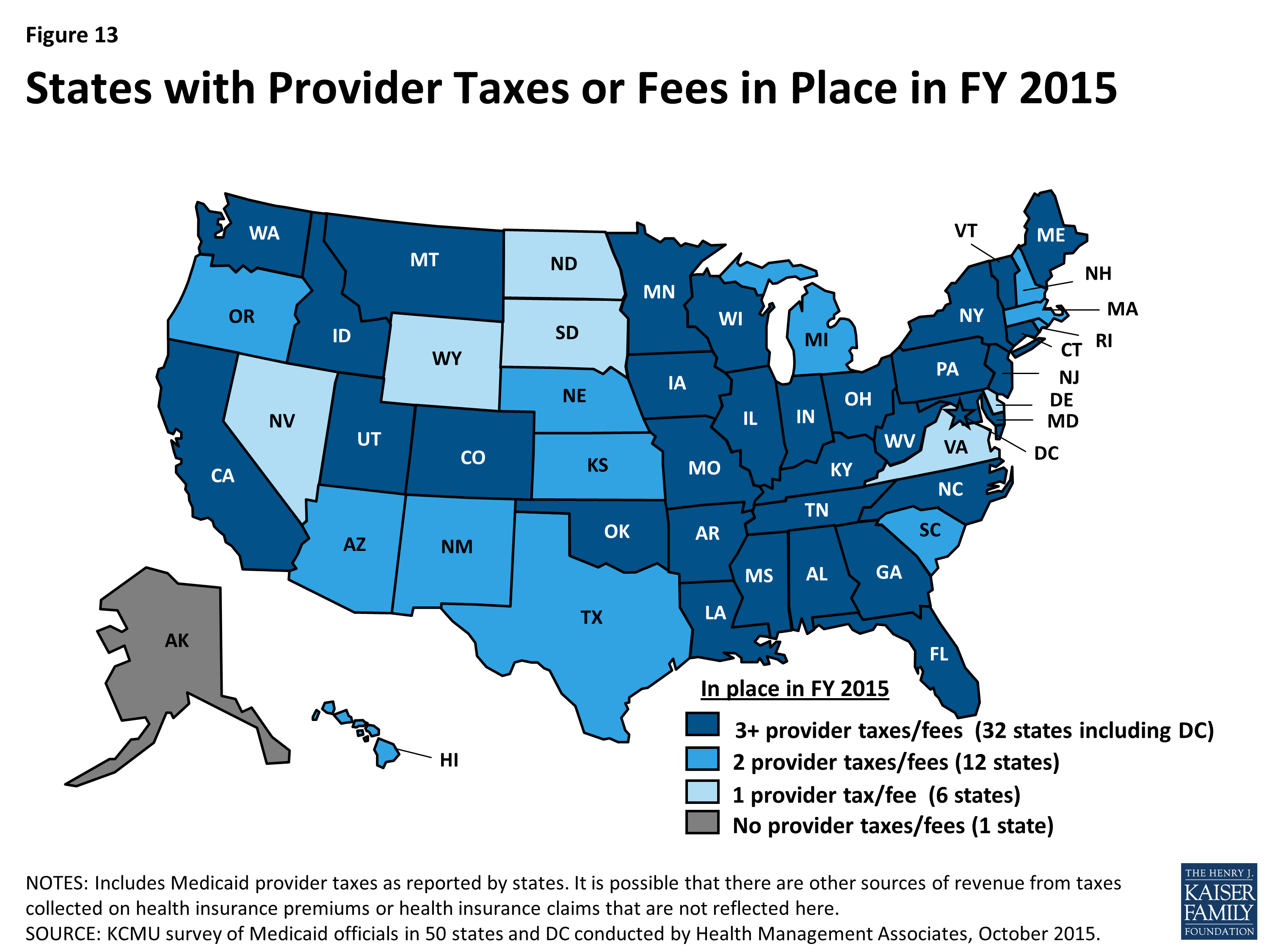
Figure 13: States with Provider Taxes or Fees in Place in FY 2015
The most common provider taxes in place in FY 2015 were taxes on nursing facilities (44 states), followed by taxes on hospitals (39 states) and intermediate care facilities (37 states). In recent years, states have made very few changes to the number of provider taxes. Minor changes for FY 2015 and FY 2016 include the following:
- In FY 2015, two states eliminated provider taxes (a hospital tax in DC and a cosmetic surgery tax in New Jersey).
- For FY 2016, three states and DC reported plans to add provider taxes. DC has a new hospital tax. Connecticut is adding a tax on ambulatory surgery centers. Michigan and Utah are adding taxes on ambulance providers.
Several states reported changes to tax rates in FY 2015 and FY 2016. Most notable were increases to rates for hospital taxes and fees (ten states in FY 2015 and six states in FY 2016) as well as increases to rates for nursing home taxes and fees (six states in FY 2015 and eight states in FY 2016). Some states also reported reducing tax rates, again mostly for hospitals (one state in FY 2015 and four states in FY 2016) and nursing home taxes and fees (two states in FY 2015 and one state in FY 2016).
States were asked whether in the future they planned to use increased provider taxes or fees to fund all or part of the costs of the ACA Medicaid expansion that will occur in calendar year 2017 and beyond when the 100 percent federal match rate for expansion costs starts to decline. Seven of the expansion states (Arizona, California, Colorado, Indiana, Kentucky, Nevada and Ohio) responded that they had such plans. Other expansion states are studying provider taxes and fees.
Table 15: Provider Rate Changes in all 50 States and DC, FY 2015
|
States |
Inpatient Hospital |
Outpatient Hospital |
Specialists |
Dentists |
Managed Care Organizations |
Nursing Facilities |
Total |
|||||||
|
Rate Change |
Increase |
Restrict |
Increase |
Restrict |
Increase |
Restrict |
Increase |
Restrict |
Increase |
Restrict |
Increase |
Restrict |
Increase |
Restrict |
|
Alabama |
X |
— |
— |
X |
X |
X |
||||||||
|
Alaska |
X |
X |
X |
— |
— |
X |
X |
|||||||
|
Arizona |
X |
X |
X |
X |
X |
|||||||||
|
Arkansas |
X |
— |
— |
X |
X |
X |
||||||||
|
California |
X |
X |
X |
X |
X |
|||||||||
|
Colorado |
X |
X |
X |
X |
X |
X |
||||||||
|
Connecticut |
X |
X |
— |
— |
X |
X |
||||||||
|
DC |
X |
X |
X |
X |
X |
X |
||||||||
|
Delaware |
X |
X |
X |
X |
X |
X |
X |
X |
||||||
|
Florida |
X |
X |
X |
X |
X |
X |
||||||||
|
Georgia |
X |
X |
X |
X |
X |
|||||||||
|
Hawaii |
X |
X |
X |
X |
X |
|||||||||
|
Idaho |
X |
X |
X |
— |
— |
X |
X |
X |
||||||
|
Illinois |
X |
X |
X |
X |
X |
X |
X |
X |
||||||
|
Indiana |
X |
X |
X |
X |
X |
|||||||||
|
Iowa |
X |
X |
X |
X |
X |
|||||||||
|
Kansas |
X |
X |
X |
X |
X |
|||||||||
|
Kentucky |
X |
X |
X |
|||||||||||
|
Louisiana |
X |
X |
X |
X |
X |
X |
||||||||
|
Maine |
X |
— |
— |
X |
X |
X |
||||||||
|
Maryland |
X |
X |
X |
X |
X |
X |
X |
|||||||
|
Massachusetts |
X |
X |
X |
X |
X |
|||||||||
|
Michigan |
X |
X |
X |
X |
X |
X |
||||||||
|
Minnesota |
X |
X |
X |
X |
||||||||||
|
Mississippi |
X |
X |
X |
X |
X |
X |
||||||||
|
Missouri |
X |
X |
X |
X |
X |
|||||||||
|
Montana |
X |
X |
X |
X |
— |
— |
X |
X |
X |
|||||
|
Nebraska |
X |
X |
X |
X |
X |
X |
||||||||
|
Nevada |
X |
X |
X |
X |
X |
|||||||||
|
New |
X |
X |
X |
X |
X |
|||||||||
|
New Jersey |
X |
X |
X |
X |
X |
|||||||||
|
New Mexico |
X |
X |
X |
X |
X |
|||||||||
|
New York |
X |
X |
X |
X |
X |
|||||||||
|
North Carolina |
X |
X |
X |
— |
— |
X |
|
X |
X |
|||||
|
North Dakota |
X |
X |
X |
X |
X |
X |
X |
|||||||
|
Ohio |
X |
X |
X |
X |
X |
|||||||||
|
Oklahoma |
X |
X |
X |
X |
— |
— |
X |
X |
||||||
|
Oregon |
X |
X |
X |
X |
||||||||||
|
Pennsylvania |
X |
X |
X |
X |
X |
|||||||||
|
Rhode Island |
X |
X |
X |
X |
X |
|||||||||
|
South Carolina |
X |
X |
X |
X |
X |
|||||||||
|
South Dakota |
X |
X |
X |
X |
— |
— |
X |
X |
||||||
|
Tennessee |
X |
X |
X |
X |
X |
|||||||||
|
Texas |
X |
X |
X |
X |
X |
|||||||||
|
Utah |
X |
X |
X |
X |
X |
X |
X |
|||||||
|
Vermont |
X |
X |
X |
X |
— |
— |
X |
X |
||||||
|
Virginia |
X |
X |
X |
X |
X |
X |
||||||||
|
Washington |
X |
X |
X |
X |
X |
|||||||||
|
West Virginia |
X |
X |
X |
X |
||||||||||
|
Wisconsin |
X |
X |
X |
X |
X |
|||||||||
|
Wyoming |
X |
— |
— |
X |
X |
|||||||||
|
Totals |
19 |
32 |
20 |
2 |
15 |
5 |
9 |
4 |
27 |
5 |
37 |
14 |
47 |
35 |
|
NOTES: For the purposes of this report, provider rate restrictions include cuts to rates for physicians, dentists, outpatient hospitals, and managed SOURCE: Kaiser Commission on Medicaid and the Uninsured Survey of Medicaid Officials in 50 states and DC conducted by Health Management |
||||||||||||||
Table 16: Provider Rate Changes in all 50 States and DC, FY 2016
|
States |
Inpatient Hospital |
Outpatient Hospital |
Specialists |
Dentists |
Managed Care Organizations |
Nursing Facilities |
Total |
|||||||
|
Rate Change |
Increase |
Restrict |
Increase |
Restrict |
Increase |
Restrict |
Increase |
Restrict |
Increase |
Restrict |
Increase |
Restrict |
Increase |
Restrict |
|
Alabama |
X |
— |
— |
X |
X |
X |
||||||||
|
Alaska |
X |
X |
— |
— |
X |
X |
X |
|||||||
|
Arizona |
X |
X |
X |
X |
X |
|||||||||
|
Arkansas |
X |
— |
— |
X |
X |
X |
||||||||
|
California |
X |
X |
X |
X |
X |
X |
||||||||
|
Colorado |
X |
X |
X |
X |
X |
X |
||||||||
|
Connecticut |
X |
— |
— |
X |
X |
X |
||||||||
|
DC |
X |
X |
X |
X |
X |
X |
||||||||
|
Delaware |
X |
X |
X |
X |
X |
X |
X |
X |
||||||
|
Florida |
X |
X |
TBD |
X |
X |
X |
||||||||
|
Georgia |
X |
X |
X |
X |
X |
|||||||||
|
Hawaii |
X |
X |
X |
X |
X |
|||||||||
|
Idaho |
X |
X |
— |
— |
X |
X |
X |
|||||||
|
Illinois |
TBD |
TBD |
TBD |
TBD |
TBD |
TBD |
TBD |
|||||||
|
Indiana |
X |
X |
X |
X |
X |
|||||||||
|
Iowa |
X |
X |
X |
X |
X |
|||||||||
|
Kansas |
X |
X |
X |
X |
X |
|||||||||
|
Kentucky |
X |
X |
X |
|||||||||||
|
Louisiana |
X |
X |
X |
X |
X |
|||||||||
|
Maine |
X |
— |
— |
X |
X |
X |
||||||||
|
Maryland |
X |
X |
X |
X |
X |
X |
X |
X |
||||||
|
Massachusetts |
X |
X |
X |
X |
X |
|||||||||
|
Michigan |
X |
X |
X |
X |
X |
|||||||||
|
Minnesota |
X |
X |
X |
X |
X |
X |
X |
|||||||
|
Mississippi |
X |
X |
X |
X |
X |
X |
||||||||
|
Missouri |
X |
X |
X |
X |
X |
X |
X |
X |
||||||
|
Montana |
X |
X |
X |
X |
— |
— |
X |
X |
||||||
|
Nebraska |
X |
X |
X |
X |
X |
X |
X |
|||||||
|
Nevada |
X |
X |
X |
X |
X |
|||||||||
|
New Hampshire |
X |
X |
X |
|||||||||||
|
New Jersey |
X |
X |
X |
X |
X |
X |
||||||||
|
New Mexico |
X |
X |
X |
X |
X |
|||||||||
|
New York |
X |
X |
X |
X |
X |
X |
X |
|||||||
|
North Carolina |
X |
— |
— |
X |
X |
|||||||||
|
North Dakota |
X |
X |
X |
X |
X |
X |
X |
|||||||
|
Ohio |
X |
X |
X |
X |
X |
X |
X |
X |
||||||
|
Oklahoma |
X |
— |
— |
X |
X |
|||||||||
|
Oregon |
X |
X |
X |
X |
||||||||||
|
Pennsylvania |
X |
X |
X |
X |
X |
|||||||||
|
Rhode Island |
X |
X |
X |
X |
X |
X |
||||||||
|
South Carolina |
X |
X |
X |
X |
X |
|||||||||
|
South Dakota |
X |
X |
X |
X |
— |
— |
X |
X |
||||||
|
Tennessee |
X |
X |
X |
|||||||||||
|
Texas |
X |
X |
X |
X |
X |
X |
||||||||
|
Utah |
X |
X |
X |
X |
X |
X |
X |
|||||||
|
Vermont |
X |
— |
— |
X |
X |
X |
||||||||
|
Virginia |
X |
X |
X |
X |
X |
X |
||||||||
|
Washington |
X |
X |
X |
X |
X |
|||||||||
|
West Virginia |
X |
X |
X |
X |
||||||||||
|
Wisconsin |
X |
X |
X |
X |
X |
X |
||||||||
|
Wyoming |
X |
— |
— |
X |
X |
X |
||||||||
|
Totals |
20 |
30 |
18 |
5 |
14 |
1 |
14 |
0 |
29 |
1 |
29 |
21 |
45 |
38 |
|
NOTES: For the purposes of this report, provider rate restrictions include cuts to rates for physicians, dentists, outpatient hospitals, and managed care organizations as well as both cuts or freezes in rates for inpatient hospitals and nursing facilities. Changes to primary care rates were asked about separately for FY 2016 and are not included in this table. There are 12 states that did not have Medicaid MCOs in operation in FY 2015; they are denoted as ‘–‘ in the MCO column. TBD – At the time of the survey, some rates for a few states were still being determined; these are denoted as TBD. SOURCE: Kaiser Commission on Medicaid and the Uninsured Survey of Medicaid Officials in 50 states and DC conducted by Health Management Associates, October 2015. |
||||||||||||||
Table 17: Provider Taxes in Place in the 50 States and DC, FY 2015 and 2016
|
States |
Hospitals |
Intermediate Care Facilities |
Nursing Facilities |
Other |
Any Provider Tax |
|||||
|
2015 |
2016 |
2015 |
2016 |
2015 |
2016 |
2015 |
2016 |
2015 |
2016 |
|
|
Alabama |
X |
X |
X |
X |
X |
X |
X |
X |
||
|
Alaska |
||||||||||
|
Arizona |
X |
X |
X |
X |
X |
X |
||||
|
Arkansas |
X |
X |
X |
X |
X |
X |
X |
X |
||
|
California |
X |
X |
X |
X |
X |
X |
X |
X |
X |
X |
|
Colorado |
X |
X |
X |
X |
X |
X |
X |
X |
||
|
Connecticut |
X |
X |
X |
X |
X |
X |
X |
X |
X |
|
|
Delaware |
X |
X |
X |
X |
||||||
|
DC |
X |
X |
X |
X |
X |
X |
X |
X |
X |
|
|
Florida |
X |
X |
X |
X |
X |
X |
X |
X |
||
|
Georgia |
X |
X |
X |
X |
X |
X |
X |
X |
||
|
Hawaii |
X |
X |
X |
X |
X |
X |
||||
|
Idaho |
X |
X |
X |
X |
X |
X |
X |
X |
||
|
Illinois |
X |
X |
X |
X |
X |
X |
X |
X |
||
|
Indiana |
X |
X |
X |
X |
X |
X |
X |
X |
||
|
Iowa |
X |
X |
X |
X |
X |
X |
X |
X |
||
|
Kansas |
X |
X |
X |
X |
X |
X |
||||
|
Kentucky |
X |
X |
X |
X |
X |
X |
X* |
X* |
X |
X |
|
Louisiana |
X |
X |
X |
X |
X |
X |
X |
X |
||
|
Maine |
X |
X |
X |
X |
X |
X |
X |
X |
X |
X |
|
Maryland |
X |
X |
X |
X |
X |
X |
X |
X |
X |
X |
|
Massachusetts |
X |
X |
X |
X |
X |
X |
||||
|
Michigan |
X |
X |
X |
X |
X |
X |
X |
|||
|
Minnesota |
X |
X |
X |
X |
X |
X |
X |
X |
X |
X |
|
Mississippi |
X |
X |
X |
X |
X |
X |
X |
X |
X |
X |
|
Missouri |
X |
X |
X |
X |
X |
X |
X* |
X* |
X |
X |
|
Montana |
X |
X |
X |
X |
X |
X |
X |
X |
||
|
Nebraska |
X |
X |
X |
X |
X |
X |
||||
|
Nevada |
X |
X |
X |
X |
||||||
|
New Hampshire |
X |
X |
X |
X |
X |
X |
||||
|
New Jersey |
X |
X |
X |
X |
X |
X |
X* |
X* |
X |
X |
|
New Mexico |
X* |
X* |
X |
X |
||||||
|
New York |
X |
X |
X |
X |
X |
X |
X* |
X* |
X |
X |
|
North Carolina |
X |
X |
X |
X |
X |
X |
X |
X |
||
|
North Dakota |
X |
X |
X |
X |
||||||
|
Ohio |
X |
X |
X |
X |
X |
X |
X |
X |
||
|
Oklahoma |
X |
X |
X |
X |
X |
X |
X |
X |
||
|
Oregon |
X |
X |
X |
X |
X |
X |
||||
|
Pennsylvania |
X |
X |
X |
X |
X |
X |
X* |
X* |
X |
X |
|
Rhode Island |
X |
X |
X |
X |
X |
X |
||||
|
South Carolina |
X |
X |
X |
X |
X |
X |
||||
|
South Dakota |
X |
X |
X |
X |
||||||
|
Tennessee |
X |
X |
X |
X |
X |
X |
X |
X |
X |
X |
|
Texas |
X |
X |
X |
X |
X |
X |
||||
|
Utah |
X |
X |
X |
X |
X |
X |
X |
X |
X |
|
|
Vermont |
X |
X |
X |
X |
X |
X |
X* |
X* |
X |
X |
|
Virginia |
X |
X |
X |
X |
||||||
|
Washington |
X |
X |
X |
X |
X |
X |
X |
X |
||
|
West Virginia |
X |
X |
X |
X |
X |
X |
X* |
X* |
X |
X |
|
Wisconsin |
X |
X |
X |
X |
X |
X |
X |
X |
X |
X |
|
Wyoming |
X |
X |
X |
X |
||||||
|
Totals |
39 |
40 |
37 |
37 |
44 |
44 |
19 |
22 |
50 |
50 |
|
NOTES: This table includes Medicaid provider taxes as reported by states. Some states also have premium or claims taxes that apply to managed care organizations and other insurers. Since this type of tax is not considered a provider tax by CMS, these taxes are not counted as provider taxes in this report. (*) has been used to denote states with multiple “other” provider taxes. SOURCE: Kaiser Commission on Medicaid and the Uninsured Survey of Medicaid Officials in 50 states and DC conducted by Health Management Associates, October 2015. |
||||||||||
Benefits Changes
In this year’s survey, the number of states reporting benefit cuts or restrictions – one in FY 2015 and five in FY 2016 – remains far below the number seen during the economic downturn. (Figure 14) A far larger number of states, 24 states in FY 2015 and 18 in FY 2016, reported enhancing or adding new benefits.
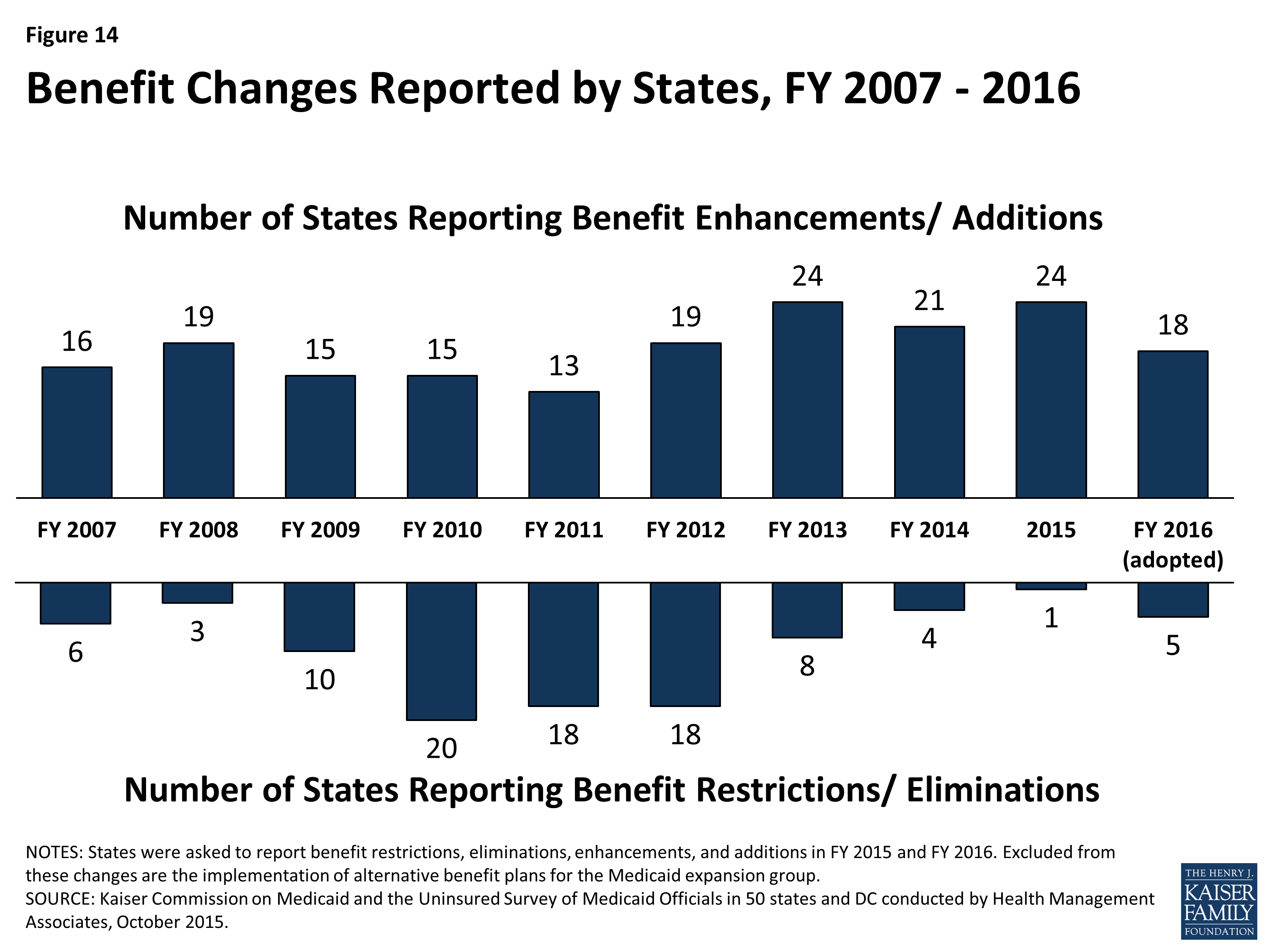
Figure 14: Benefit Changes Reported by States, FY 2007 – 2016
One of the most common benefit enhancements or additions reported was for behavioral health and substance abuse services. For example, Ohio is redesigning its behavioral health benefits to include coverage of additional services such as Assertive Community Treatment and Intensive Home Based Treatment. Other common benefit enhancements reported include home and community-based services including changes to 1915(c) waivers, new 1915(i) HCBS State Plan Option implementations and implementation of the Community First Choice State Plan Option. Also common were enhancements to dental services and telemedicine and tele-monitoring. (Table 18)
| Table 18: Benefit Enhancements or Additions | ||
| Benefit | FY 2015 | FY 2016 |
| Behavioral Health | CT, DE, IN, MD, MO, NH, SC, VA, WY | DC, MD, NY, OH, SC, TX, VT, WY |
| HCBS | CA, CT, DC, DE, MA, ND, NJ, NY, TX, WI | CA, CT, DC, DE, GA, MS, WA |
| Dental Services | CO, IL, MA, SC, VA | MO, OR |
| Telemedicine / Tele-monitoring | MD, VT | NE, VT |
For its Medicaid expansion population, Pennsylvania reported replacing its Healthy PA waiver benefits plan (that included a number of physical and behavioral health service limits) with its traditional Medicaid benefit plan resulting in the elimination of those limits in FY 2015. Also, California is planning a notable benefit expansion for pregnant women in FY 2016; the state is planning to provide the full Medicaid benefit package to pregnant women up to 138 percent FPL in place of the current, more limited pregnancy-related benefit package.
Benefit restrictions reflect the elimination of a covered benefit or the application of utilization controls for existing benefits. In FY 2015, Arkansas imposed limits to non-emergency transportation for non-medically frail adults. For FY 2016, four states reported narrowly targeted benefit eliminations (Connecticut, New York, Oklahoma and Vermont) and one state (West Virginia) reported plans to apply a number of service limitations in its home and community-based services waiver serving persons with Intellectual and Developmental Disabilities to enable the waiver to operate within its budget while also serving more people on the waiting list.
| Autism Services |
| On July 7, 2014, CMS issued an Informational Bulletin6 describing approaches and Medicaid authorities available to cover Autism Spectrum Disorder (ASD) services. The bulletin also clarified state obligations under the Early and Periodic Screening, Diagnostic and Treatment (EPSDT) benefit to cover all medically necessary services for children, including ASD services. In this year’s survey, two states in FY 2015 and eight states in FY 2016 reported adding coverage for ASD services. These policy changes have not been counted as positive or negative as they were required changes. |
Table 19: Benefit Changes in the 50 States and DC, FY 2015 and 2016
|
Benefit Changes |
||||
|
STATES |
FY 2015 |
FY 2016 |
||
|
Enhancements/ Additions |
Restrictions/ Eliminations |
Enhancements/ Additions |
Restrictions/ Eliminations |
|
|
Alabama |
||||
|
Alaska |
||||
|
Arizona |
X |
X |
||
|
Arkansas |
X |
|||
|
California |
X |
X |
||
|
Colorado |
X |
|||
|
Connecticut |
X |
X |
X |
|
|
Delaware |
X |
X |
||
|
DC |
X |
X |
||
|
Florida |
||||
|
Georgia |
X |
|||
|
Hawaii |
||||
|
Idaho |
||||
|
Illinois |
X |
|||
|
Indiana |
X |
|||
|
Iowa |
||||
|
Kansas |
||||
|
Kentucky |
||||
|
Louisiana |
||||
|
Maine |
||||
|
Maryland |
X |
X |
||
|
Massachusetts |
X |
|||
|
Michigan |
||||
|
Minnesota |
X |
|||
|
Mississippi |
X |
X |
||
|
Missouri |
X |
X |
||
|
Montana |
||||
|
Nebraska |
X |
|||
|
Nevada |
||||
|
New Hampshire |
X |
|||
|
New Jersey |
X |
|||
|
New Mexico |
||||
|
New York |
X |
X |
X |
|
|
North Carolina |
||||
|
North Dakota |
X |
|||
|
Ohio |
X |
|||
|
Oklahoma |
X |
|||
|
Oregon |
X |
|||
|
Pennsylvania |
X |
|||
|
Rhode Island |
||||
|
South Carolina |
X |
X |
||
|
South Dakota |
||||
|
Tennessee |
||||
|
Texas |
X |
X |
||
|
Utah |
||||
|
Vermont |
X |
X |
X |
|
|
Virginia |
X |
|||
|
Washington |
X |
|||
|
West Virginia |
X |
|||
|
Wisconsin |
X |
|||
|
Wyoming |
X |
X |
||
|
Totals |
24 |
1 |
18 |
5 |
|
NOTES: States were asked to report benefit restrictions, eliminations, enhancements, and additions in FY 2015 and FY 2016. Excluded from these changes are the implementation of alternative benefit plans for the Medicaid expansion group. SOURCE: Kaiser Commission on Medicaid and the Uninsured Survey of Medicaid Officials in 50 states and DC conducted by Health Management Associates, October 2015. |
||||
Table 20: Benefit Actions Taken in all 50 States and DC, FY 2015 and 2016*
|
State |
Fiscal Year |
Benefit Changes |
|
Alabama |
2015 |
|
|
2016 |
||
|
Alaska |
2015 |
|
|
2016 |
||
|
Arizona |
2015 |
Adults (+) Eliminated 25-day inpatient hospital limit. (October 1, 2014) |
|
2016 |
Adults (+): Restoring coverage for orthotics. (August 1, 2015) |
|
|
Arkansas |
2015 |
Expansion Adults (-): Applied limits to non-emergency medical transportation benefits for non-medically frail expansion adults. (February 1, 2015) |
|
2016 |
Aged & Disabled (nc): Combining the ElderChoices 1915(c) and the Adults with Physical Disabilities 1915(c) waivers into a new 1915(c) waiver which ensures all benefits of both waivers to both groups. (January 1, 2016) |
|
|
California |
2015 |
Children (nc): Added coverage for Behavioral Health Treatment for children with autism spectrum disorder to meet federal requirements. (September 2014) Aged & Disabled (+): Partially restored FY 2014 in-home supportive services hour reduction. (July 1, 2014) |
|
2016 |
Aged & Disabled (+): Restored remaining FY 2014 in-home supportive services hour reduction. (July 1, 2015) Pregnant Women (+): Expansion to full-scope coverage to pregnant women 60-133% FPL. (Upon CMS approval) |
|
|
Colorado |
2015 |
Adults (+): Completed adding adult dental coverage. (July 1, 2014) |
|
2016 |
Children (nc): Increased expenditure cap as part of Autism Waiver expansion. (July 1, 2015) |
|
|
Connecticut |
2015 |
Adults (+): Expanded coverage for licensed behavioral health clinician services provided by independent practitioners (licensed psychologists, licensed clinical social workers, licensed marital and family therapists, licensed alcohol and drug counselors, and licensed professional counselors). (July 1, 2014) Aged & Disabled (+): Implemented new HCBS services under 1915(i) authority for Medicaid eligible elders who do not meet nursing home level of care. |
|
2016 |
Adults (+): Added coverage of select over the counter drugs. (July 1, 2015) Aged & Disabled (+): Implemented the Community First Choice Option. (July 2015) Pregnant Women (+): Added coverage of low dose aspirin. (July 1, 2015) Adults (-): Eliminated coverage of Part D copays for non-institutionalized dual eligible beneficiaries. (July 1, 2015) |
|
|
Delaware |
2015 |
Aged & Disabled (+): Added 1915(i) supported employment services for individuals with disabilities (Pathways Program). (January 1, 2015) |
|
Aged & Disabled (+): Enhancing behavioral health and substance use disorder services through the PROMISE Program. (January 1, 2015) |
||
|
2016 |
Aged & Disabled (+): Planning to implement the Community First Choice Option. |
|
|
District of Columbia |
2015 |
Children (+): Added coverage for school based health services when delivered in nonpublic school settings. (October 1, 2014) |
|
Children (nc): Personal care aide removed from coverage as school-based service. (Oct 2014) |
||
|
All (+): Expanding transplant services. (October 1, 2014) |
||
|
Aged & Disabled (+): Added adult day health services under 1915(i) authority for persons aged 55+ with a chronic medical condition. |
||
|
2016 |
Children (+): Adding reimbursement for adolescent substance abuse treatment. (Jan. 1, 2016) |
|
|
LTSS Adults (+): Amending the IDD and Elderly and Physically Disabled 1915(c) waivers to increase person-centered thinking, planning, and service coordination. Examples are the addition of Individualized Day Programs and Supported Living with Transportation to community activities for people with IDD. Key EPD Waiver amendments include the addition of a new provider type suitable to the delivery of Homemaker and Chore Services and revisions to the Environmental Accessibility Adaptation service that will make services more accessible. |
||
|
Florida |
2015 |
|
|
2016 |
||
|
Georgia |
2015 |
|
|
2016 |
Adults (+): Added coverage for medically necessary emergency transportation by rotary wing air ambulance. (July 1, 2015) LTSS Adults (+): Added hourly skilled nursing to Independent Care Waiver Program. (July 1, 2015) |
|
|
Hawaii |
2015 |
|
|
2016 |
||
|
Idaho |
2015 |
|
|
2016 |
||
|
Illinois |
2015 |
Adults (+): Restored coverage for adult dental services. (July 1, 2014) |
|
Adults (+): Restored coverage for adult podiatry services. (October 1, 2014) |
||
|
2016 |
||
|
Indiana |
2015 |
Aged & Disabled (+): Added habilitation services for adults with serious mental illness under 1915(i) authority. |
|
2016 |
Children (nc): Adding coverage for Applied Behavioral Analysis services for children with autism spectrum disorder to meet federal requirements. (October 1, 2015) |
|
|
Iowa |
2015 |
|
|
2016 |
||
|
Kansas |
2015 |
|
|
2016 |
||
|
Kentucky |
2015 |
|
|
2016 |
Aged & Disabled (nc): Modifying and adding new HCBS waiver services to better align beneficiary needs with services available and to comply with new HCBS federal requirements. |
|
|
Louisiana |
2015 |
|
|
2016 |
||
|
Maine |
2015 |
|
|
2016 |
||
|
Maryland |
2015 |
All (+): Expanded telemedicine services from rural to urban areas. (October 1, 2014) |
|
All (+): Added coverage for certain Substance Use Disorder services. (January 1, 2015) |
||
|
2016 |
All (+): Added Physician Assistants as a new provider type. (July 1, 2015) Children (+): Plan to implement services under 1915(i) authority for children and youth with serious emotional disturbances and serious and persistent mental illness. |
|
|
Massachusetts |
2015 |
Adults (+): Added coverage for treatment of gender dysphoria. Adults (+): Restored coverage for dentures. (May 15, 2015) Aged & Disabled (+): Added a shared living benefit to the TBI 1915(c) waiver. |
|
2016 |
||
|
Michigan |
2015 |
|
|
2016 |
||
|
Minnesota |
2015 |
Pregnant Women (+): Adding coverage for services provided by certified doulas. (July 1, 2014) |
|
2016 |
Children (nc): Added coverage for treatment of autism spectrum disorder to meet federal requirements. (July 1, 2015) Aged & Disabled (nc): Plan to convert the personal care assistance benefit to the Community First Choice Option under 1915(i) and Section 1115 waiver authority. (Upon CMS approval) |
|
|
Mississippi |
2015 |
Aged & Disabled Children (+): Added coverage for Prescribed Pediatric Extended Care Centers (a new provider type). (July 1, 2014) |
|
2016 |
Aged & Disabled (+): Plan to implement HCBS services under 1915(i) authority for persons with intellectual and developmental disabilities. |
|
|
Missouri |
2015 |
All (+): Added coverage for SBIRT (Screening, Brief Intervention, Referral and Treatment) and HBAI (Health Behavior Assessment and Intervention services). (January 2015) |
|
2016 |
Children (+): Adding coverage for asthma education and environmental assessment services. (Upon CMS approval) Adults (+): Restoring coverage for preventive dental services and fillings. (January 2016) |
|
|
Montana |
2015 |
|
|
2016 |
||
|
Nebraska |
2015 |
|
|
2016 |
All (+): Adding coverage for telehealth and tele-monitoring services. (January 2016). Children (nc): Adding coverage for intensive behavioral intervention services for treatment of autism spectrum disorder to meet federal requirements. |
|
|
Nevada |
2015 |
|
|
2016 |
||
|
New Hampshire |
2015 |
All (+): Removed service limits on psychotherapy, X-ray and outpatient hospital (to harmonize with Alternative Benefit Plan for the expansion population). Expansion Adults (+): Added coverage for chiropractic and Substance Use Disorder services. (August 15, 2014) |
|
2016 |
||
|
New Jersey |
2015 |
Aged & Disabled (+): Implemented managed long-term services and supports and consolidating 1915(c) waivers into state’s Section 1115 which provides LTSS beneficiaries with a greater array of LTSS services. (July 1, 2014) |
|
2016 |
||
|
New Mexico |
2015 |
Pregnant Women (nc): Added coverage for birthing centers to meet federal requirements. (December 1, 2014) Children (nc): Added coverage for treatment of autism spectrum disorder to meet federal requirements. (July 1, 2015) |
|
2016 |
||
|
New York |
2015 |
Aged & Disabled (+): Implemented the Community First Choice Option. (SPA still pending; plan to implement retroactively.7) |
|
2016 |
All (-): Discontinued coverage for viscosupplementation of the knee for an enrollee with a diagnosis of osteoarthritis of the knee. (April 1, 2015 for FFS and July 1, 2015 for managed care) All (+): Expanded smoking cessation counseling providers to include dental practitioners. (April 1, 2015 for FFS and July 1, 2015 for managed care) All (-): Limited coverage of DEXA Scans for Screening to one time every 2 years for Women Over Age 65 and Men Over Age 70. (April 1, 2015 for FFS and July 1, 2015 for managed care) Aged & Disabled (+):Plan to add services for adults with serious mental illness services under 1915(i) authority as part of the state’s Health and Recovery Plans (HARP) managed care program. |
|
|
North Carolina |
2015 |
|
|
2016 |
||
|
North Dakota |
2015 |
Aged & Disabled (+): Added personal care with supervision to the Home and Community Based waiver to allow individuals with a primary diagnosis of dementia or traumatic brain injury to receive 24 hour supervision with a daily rate. (January 2015) |
|
2016 |
||
|
Ohio |
2015 |
|
|
2016 |
Aged & Disabled (+): Planning to implement a redesign of behavioral health benefits to include coverage of additional services for persons with high intensity service and support needs (e.g., Assertive Community Treatment for SPMI adults, Intensive Home Based Treatment for SED children and residential treatment for substance use disorders). (January 1, 2016) |
|
|
Oklahoma |
2015 |
|
|
2016 |
Adults (-): Eliminated coverage for sleep studies. (July 1, 2015) |
|
|
Oregon |
2015 |
|
|
2016 |
Adults (+): Restoring previously cut adult restorative dental benefits (relaxed limitation criteria for dentures; coverage for crowns; scaling and planning). (January 1, 2016) |
|
|
Pennsylvania |
2015 |
Expansion Adults (+): Conformed Alternative Benefit Package (originally implemented on January 1, 2015) to the traditional Medicaid benefit package which resulted in an elimination of service limits on physical and behavioral health services. (April 27, 2015) |
|
2016 |
||
|
Rhode Island |
2015 |
|
|
2016 |
||
|
South Carolina |
2015 |
Dual Eligibles (+): Added inpatient psychiatric coverage. (July 1, 2014) Family Planning Adults (+): Added additional preventive services including diabetes screening, health and behavioral assessments, cholesterol abnormalities and HIV screening. (Aug 2014) Adults (+): Added a preventative adult dental benefit. (December 1, 2014) |
|
2016 |
Children (nc): Added autism spectrum disorder treatment to meet federal requirement. (Oct 2015) Children (+): Expanded coverage for treatment of eating disorders ages 0-21. (October 2015) |
|
|
South Dakota |
2015 |
|
|
2016 |
||
|
Tennessee |
2015 |
|
|
2016 |
||
|
Texas |
2015 |
LTSS Adults (+): Implemented Community First Choice Option (CFCO) services for eligible individuals meeting institutional level of care and delivered through both the FFS and managed care delivery systems. (September 1, 2014) MLTSS Adults (+): Added supported employment and employment assistance to the HCBS waiver service array in the STAR+PLUS program. (September 1, 2014) Aged & Disabled (nc): Allowed providers other than Local Mental Health Authorities (LMHAs) to provide Mental Health Targeted Case Management and Mental Health Rehabilitative services already available through STAR Health. (September 1, 2014) |
|
2016 |
Aged & Disabled (+): Implementing an array of HCBS designed to support long-term recovery from mental illness for SMI adults who are former long-term residents of inpatient facilities under a 1915(i) SPA. (Upon CMS approval) |
|
|
Utah |
2015 |
|
|
2016 |
Children (nc): Added autism spectrum disorder treatment to meet federal requirement. (July 2015) |
|
|
Vermont |
2015 |
All (+): Added a tele-monitoring benefit. (August 1, 2014) |
|
2016 |
Aged & Disabled (-): Eliminating Enhanced Residential Care and Adult Family Care Case Management. All (+): Adding coverage for Licensed Alcohol and Drug Counselors. (October 2015) All (+): Adding coverage for primary care telemedicine outside of a facility. (October 1, 2015) Children (nc): Added coverage for Applied Behavior Analysis for treatment of autism spectrum disorder to meet federal requirements. (July 1, 2015) |
|
|
Virginia |
2015 |
Aged & Disabled (+): Added nutrition counseling and inpatient substance abuse services for Medicaid Works (working disabled eligibility group). (July 1, 2014) |
|
Pregnant Women (+): Expanded comprehensive dental benefits to pregnant women. (March 2015) |
||
|
2016 |
||
|
Washington |
2015 |
|
|
2016 |
LTSS Adults (+): Adding skills acquisition training and assistive technology under Community First Choice (CFC) for persons meeting nursing facility level of care. (Upon CMS approval) All (+): Added coverage for gender reassignment surgery. (August 6, 2015) |
|
|
West Virginia |
2015 |
|
|
2016 |
Aged & Disabled (-): Amending IDD HCBS waiver (as part of five year renewal) to impose service limitations that will allow waiver to operate within its budget and serve more persons on the waiting list. Service limitations include reductions in respite hours, person centered support services, non-emergency transportation, and other reductions. (Upon CMS approval) |
|
|
Wisconsin |
2015 |
Aged & Disabled (+): Added the following HCBS waiver services for persons meeting nursing facility level of care: Consultative Clinical and Therapeutic Services for Caregivers and Training Services for Unpaid Caregivers. (January 1, 2015) |
|
2016 |
Children (nc): Added State Plan coverage (to replace HCBS waiver coverage) for behavioral health services for treatment of autism spectrum disorder to meet federal requirements. (January 1, 2016) |
|
|
Aged & Disabled (nc): A psychosocial rehabilitation program under 1915(i) along with two other such programs under other Medicaid authorities are being replaced with a single comprehensive psychosocial rehabilitation program under 1905 authority that will cover all the services provided by the prior programs. |
||
|
Wyoming |
2015 |
All (+): Added coverage for additional licensed MH provider types. (July 2014) |
|
2016 |
All (+): Added chiropractic benefit. (July 1, 2015) All (+): Adding coverage for additional provisionally licensed MH provider types. (July 1, 2015) |
|
|
* Benefit enhancements counted in this report are denoted with (+). Benefit restrictions or eliminations counted in this report are denoted with (-). Changes that were not counted as positive or negative in this report, but were mentioned by states in their responses, are denoted with (nc). |
||
Prescription Drug Utilization and Cost Control Initiatives
Just over a decade ago, between 2001 and 2005, the vast majority of states aggressively implemented policies designed to slow the growth in Medicaid spending for prescription drugs. In January 2006, the implementation of the Medicare prescription drug benefit reduced total state Medicaid drug expenditures by almost half, the rate of growth in the cost of prescription drugs abated, and the intense Medicaid focus on pharmacy cost containment began to diminish. Since 2014, however, a combination of rising drug prices and increasing enrollments (as a result of ACA coverage expansions) have refocused state attention on pharmacy reimbursement and coverage policies. In this year’s survey, over two-thirds of the states in FY 2015 and half in FY 2016 reported actions to refine and enhance their pharmacy programs and to react to new and emerging specialty and high-cost drug therapies.
This year’s survey asked states to comment on the most significant factors affecting the trend in total Medicaid pharmacy expenditures (federal and state) between FY 2014 and projected for FY 2016. Responding to this open-ended question, the vast majority of states identified specialty and other high-cost drugs as a significant cost driver including a number of states identifying specific drug classes: hepatitis C antivirals, oncology drugs, cystic fibrosis agents and hemophilia factor. A few states also identified recently approved cholesterol drugs called “PCSK9 inhibitors” as likely cost drivers for FY 2016. In addition to specialty and other high-cost drugs, a number of states identified generic drugs as a significant cost driver, referencing large price increases for existing generics and higher than expected prices for new generics entering the market in addition to inflation and general drug price increases. Increased enrollment was also identified as a factor (including both ACA Medicaid expansion states and non-expansion states). A few states also identified factors that helped to moderate or reduce expenditure growth trends including higher rebates, drugs coming off patent and increased prior authorization and step therapy requirements. A number of states also commented that because pharmacy benefits for many enrollees were delivered under a capitated MCO arrangement, the growth in pharmacy expenditures could not be isolated.
Pharmacy Management Policies in Place and New in FY 2015 and FY 2016
At the start of FY 2015, a total of 45 states indicated that they had already in place a Preferred Drug List (PDL) and were already obtaining supplemental rebates.8 Two states (Arizona and Massachusetts) reported collecting supplemental rebates for the first time during FY 2015; one state (North Dakota) reported plans to adopt a PDL and collect supplemental rebates in FY 2016. The number of states with limits on the number of prescriptions that Medicaid will pay for each month decreased to 14 states in FY 2015, down from 16 states in FY 2014 and 18 states in FY 2013. One state (Pennsylvania) reported eliminating their prescription cap for adults in FY 2015. (Kentucky reported eliminating their monthly prescription limit in January 2014.)
Summary of FY 2015 and FY 2016 Pharmacy Policy Changes and Cost Containment Efforts
Thirty-five states (35) in FY 2015 and 25 states in FY 2016 implemented cost-containment initiatives in the area of prescription drugs, comparable to the number of states taking such actions in FY 2014 (28), FY 2013 (24), and FY 2012 (33). As PDL and related supplemental rebate programs have matured in most states and as more states have carved the pharmacy benefit into capitated managed care arrangements, the number of states reporting PDL or supplemental rebate changes (e.g., adding new PDL drug classes or joining a multi-state rebate pool) has dropped significantly (three states planning changes to PDL and five states planning changes to supplemental rebates in FY 2016) compared to 24 and 28 states in FY 2009. A small number of states reported reductions in ingredient cost reimbursement (5 states in FY 2015 and 6 states in FY 2016) often associated with adopting an actual acquisition cost methodology (discussed below), and a small number reported dispensing fee reductions (4 states in FY 2015 and 1 state in FY 2016). No state reported imposing new limits on the number of monthly prescriptions in either FY 2015 or FY 2016. The most significant restriction reported related to applying clinical management protocols for specialty/high-cost drugs.
| Medicaid Covered Outpatient Drug Rule |
| State Medicaid programs reimburse pharmacies for the “ingredient cost” of each prescription using an Estimated Acquisition Cost (EAC), plus a dispensing fee.9 A proposed rule released in February 2012,10 replaces the term EAC with the term “Actual Acquisition Cost” (AAC) and also requires states to align their dispensing fees to be consistent with their ingredient cost reimbursement. States can define their own AAC prices or use the pricing files published and updated weekly by CMS – the “National Average Drug Acquisition Costs” (NADACs) – which are derived from outpatient drug acquisition cost surveys of retail community pharmacies.11 Some states have already transitioned to an AAC methodology. In this year’s survey, one state in FY 2015 (Alaska) and five states in FY 2016 (Maryland, Nevada, North Carolina, Texas and Virginia) reported adopting, or plans to adopt, an AAC (e.g., NADAC) ingredient cost methodology. A number of other states reported that they were holding off making any changes to their pharmacy reimbursement methodologies until the proposed rule is finalized which is expected to occur in late CY 2015.12 |
High-Cost Specialty Drugs
While there is no universally accepted definition of specialty drugs and Medicaid programs use varying definitions, products designated as specialty drugs tend to require either difficult or unusual medication delivery, or complex treatment maintenance. Price is also frequently considered an indicator of specialty drugs.13 According to pharmacy benefit manager, Express Scripts, overall U.S. drug spending increased by 13.1 percent in 2014 driven by a 30.9 percent increase in spending on specialty drugs, the highest specialty drug trend ever reported.14 Specialty drugs also grew as a share of total drug spending from 27.7 percent in 2013 to 31.8 percent in 2014 and are expected to reach 44 percent in the next three years with annual increases of 21 – 22 percent.15 Much of the 2014 growth was driven by the launch of three new hepatitis C treatments – Sovaldi, Olysio and Harvoni. As noted above, however, other new and emerging specialty drugs for cancer, cystic fibrosis, cholesterol management and other conditions are, or are expected to become, significant cost drivers.
In this year’s survey, states were asked to comment on whether their state had adopted or planned to adopt coverage, reimbursement or managed care policies targeting specialty or high-cost drugs in FYs 2015 or 2016.
- Nineteen (19) states reported implementing new clinical prior authorization requirements and 11 states indicated that they were standardizing clinical criteria across both fee-for-service and managed care;
- Four states (Connecticut, DC, Idaho and South Carolina) reported negotiating lower prices for certain drugs or more aggressive supplemental rebates;
- Two states (Tennessee, Texas) reported reimbursement changes that effectively lower specialty drug prices;
- One state (New York) reported plans to implement a specialty pharmacy program, and
- One state (Wyoming) reported adding case managements with high drug costs and plans to implement a medication therapy program.
In contrast, in FY 2016, two states (California and Connecticut) reported plans to liberalize their previously more restrictive prior authorization polices for hepatitis C drugs, making them more widely available.
Several states also reported other managed care policies specifically related to reimbursement of hepatitis C drugs in FY 2015: California and Florida pay “kick” payments to MCOs, Kansas pays a “case rate,” and Maryland makes supplemental payments to MCOs that follow the state’s hepatitis C clinical guidelines. New Mexico reported using risk corridors and Rhode Island reported stop-loss payments, and five states (DC, New Hampshire, South Carolina, Texas and Washington) reported carving these drugs out of the capitation payment. In some cases, these policies were reported as “temporary” to allow the state time to collect enough utilization data so that the cost of these drugs could be included in future capitation rates. Oregon also expressed the concern that the coverage of specialty and high-cost drugs could put its Section 1115 Demonstration Waiver budget neutrality ceiling at risk.
Other Pharmacy Policy Changes
Other pharmacy actions counted as cost containment measures for FY 2015 and FY 2016 included: Medication Therapy Management programs including efforts to better manage opiates and behavioral health drugs (Indiana, Massachusetts, North Carolina, North Dakota, Washington and Wyoming), new or expanded 340B programs (Arizona and Oklahoma), a common formulary across FFS and MCOs (Michigan and Mississippi), hemophilia management program (Arkansas), restructured physician administered drug program (Kentucky), expanded step therapy or prior authorization programs (Louisiana), new enrollee lock-in program (North Carolina), reductions in over-the-counter (OTC) coverage for cough and cold medications for children (New Mexico), management of compound prescriptions and limits on Buprenorphine – a medication used to treat opioid addiction (Tennessee).
In addition, several states reported other pharmacy-related actions that were not included in the count of cost containment actions. Connecticut is allowing non-controlled prescriptions to remain valid for a full year (rather than six months) and is also implementing select OTC coverage for adults. DC, New York, Ohio and Vermont are awarding new administrative contracts for pharmacy benefit management and related services. Delaware, Indiana and Iowa are transitioning the pharmacy benefit to MCOs and Kansas is moving select vaccines to the pharmacy benefit under managed care. New York plans to carve in hemophilia factor products and injectable antipsychotic drugs into managed care contracts in FY 2016. Maryland carved-out substance use disorder drugs from managed care. Michigan is allowing behavioral health and other select physician injectables to be billed under the pharmacy benefit. Nebraska implemented Indian Health Service pharmacy reimbursement at an encounter rate. Texas is requiring MCO prior authorization policies to be reviewed and approved by its Drug Utilization Review Board.
Finally, a few states reported pharmacy-related expansions or reversals of previous pharmacy cost containment actions. Three states increased dispensing fees in FY 2015 (Alaska, Iowa and Montana) and six states planned to increase dispensing fees in FY 2016 (Maryland, Montana, Nevada, North Carolina, Texas and Virginia). In six of these states (Alaska, Maryland, Nevada, North Carolina, Texas and Virginia), dispensing fee increases were expected to partially offset reimbursement decreases resulting from the adoption of the AAC/NADAC ingredient cost reimbursement methodology. In addition to expansions or reversals of cost containment noted previously (Pennsylvania eliminated its monthly prescription cap for adults; California and Connecticut reported plans to liberalize their prior authorization policies for hepatitis C drugs) Illinois reported exempting antipsychotic medications from its monthly prescription cap, as well as exempting children with complex medical needs enrolled in a care coordination entity from its monthly prescription cap requirements.
Table 21: Pharmacy Cost Containment Actions Taken in all 50 States and DC, FY 2015 and 2016
|
States |
Reduce Dispensing Fee |
Reduce Ingredient Costs |
Preferred Drug List Changes |
Supplemental Rebate Changes |
Specialty Rx Actions |
Other Pharmacy Actions |
Total Pharmacy Actions Taken |
|||||||
|
2015 |
2016 |
2015 |
2016 |
2015 |
2016 |
2015 |
2016 |
2015 |
2016 |
2015 |
2016 |
2015 |
2016 |
|
|
Alabama |
||||||||||||||
|
Alaska |
X |
X |
||||||||||||
|
Arizona |
X |
X |
X |
X |
X |
|||||||||
|
Arkansas |
X |
X |
X |
X |
X |
X |
X |
|||||||
|
California |
X |
X |
||||||||||||
|
Colorado |
||||||||||||||
|
Connecticut |
X |
X |
X |
X |
X |
X |
X |
X |
X |
|||||
|
Delaware |
||||||||||||||
|
DC |
X |
X |
X |
X |
||||||||||
|
Florida |
X |
X |
||||||||||||
|
Georgia |
||||||||||||||
|
Hawaii |
X |
X |
||||||||||||
|
Idaho |
X |
X |
X |
|||||||||||
|
Illinois |
X |
X |
X |
X |
X |
|||||||||
|
Indiana |
X |
X |
X |
X |
X |
X |
||||||||
|
Iowa |
||||||||||||||
|
Kansas |
||||||||||||||
|
Kentucky |
X |
X |
||||||||||||
|
Louisiana |
X |
X |
X |
X |
X |
X |
||||||||
|
Maine |
X |
X |
||||||||||||
|
Maryland |
X |
X |
X |
X |
||||||||||
|
Massachusetts |
X |
X |
X |
X |
X |
|||||||||
|
Michigan |
X |
X |
||||||||||||
|
Minnesota |
||||||||||||||
|
Mississippi |
X |
X |
X |
X |
X |
|||||||||
|
Missouri |
||||||||||||||
|
Montana |
X |
X |
X |
|||||||||||
|
Nebraska |
X |
X |
X |
X |
||||||||||
|
Nevada |
X |
X |
X |
X |
X |
|||||||||
|
New Hampshire |
X |
X |
||||||||||||
|
New Jersey |
||||||||||||||
|
New Mexico |
X |
X |
X |
X |
||||||||||
|
New York |
X |
X |
X |
X |
X |
|||||||||
|
North Carolina |
X |
X |
X |
X |
X |
X |
X |
|||||||
|
North Dakota |
X |
X |
X |
X |
X |
|||||||||
|
Ohio |
||||||||||||||
|
Oklahoma |
X |
X |
X |
|||||||||||
|
Oregon |
X |
X |
X |
X |
X |
|||||||||
|
Pennsylvania |
X |
X |
||||||||||||
|
Rhode Island |
X |
X |
X |
X |
||||||||||
|
South Carolina |
X |
X |
||||||||||||
|
South Dakota |
||||||||||||||
|
Tennessee |
X |
X |
X |
X |
X |
X |
X |
|||||||
|
Texas |
X |
X |
X |
X |
X |
X |
X |
|||||||
|
Utah |
||||||||||||||
|
Vermont |
||||||||||||||
|
Virginia |
X |
X |
X |
X |
||||||||||
|
Washington |
X |
X |
X |
X |
||||||||||
|
West Virginia |
||||||||||||||
|
Wisconsin |
X |
X |
||||||||||||
|
Wyoming |
X |
X |
X |
X |
||||||||||
|
Totals |
4 |
1 |
5 |
6 |
6 |
3 |
6 |
5 |
26 |
13 |
6 |
11 |
35 |
25 |
|
SOURCE: Kaiser Commission on Medicaid and the Uninsured Survey of Medicaid Officials in 50 states and DC conducted by Health Management Associates, October 2015. |
||||||||||||||
Priorities for FY 2016 and Beyond Reported by Medicaid Directors
Medicaid is a large and complex program that provides health coverage for an increasing share of the population in each state. As the program continues to evolve, key priorities for most directors center around implementing the Medicaid expansion, controlling costs, implementing an array of complex delivery system reforms, and standing up new information technology systems related to eligibility, enrollment, claims processing and delivery system reform. Emerging priorities are focused on population health and social determinants of health. Tackling these major issues is a significant challenge for Medicaid directors, especially since administrative resources (both in terms of staff and funding) are often constrained. Key priorities for Medicaid directors identified in this year’s survey are described below.
Implementing the myriad provisions of the ACA. All states continue to focus on eligibility and enrollment changes, and 31 states (including DC) have adopted the ACA Medicaid expansion. Many directors reported that implementing the Medicaid expansion and expanding access to care for residents who have not had insurance continues to be a key priority.
Controlling costs. While not as acute as during the recession, states still report that controlling costs and spending is a top priority. Given the size of the Medicaid program as a share of state budgets, ensuring high quality and cost effective care is a perennial issue. Several expansion states indicated that as the overall program grows, maintaining or reducing state Medicaid spending or achieving other state budget savings (such as those related to behavioral health or corrections) has been key. More broadly, many states mentioned the growing costs of specialty drugs and improving program integrity as areas of focus. In addition, a number of states noted that while the economy has been improving, state revenues may not have kept pace, which has implications for all state programs including Medicaid. Looking ahead to FY 2017, a few states implementing the Medicaid expansion reported that finding general funds for the state share of Medicaid spending beginning in January 2017 is an upcoming challenge.
Implementing a wide range of payment and delivery system reform initiatives. Medicaid programs have embarked on a range of initiatives designed to better coordinate and integrate care. These initiatives often utilize reimbursement approaches that incentivize high quality care and reward optimal outcomes. These are complex initiatives to design, adopt and implement. States also continue to prioritize efforts to “rebalance” the delivery of LTSS toward greater use of home and community-based services. Some of these Medicaid reforms may have effects that ripple throughout the entire health system.
A number of Medicaid payment and delivery system reforms rely on managed care. With the increasing reliance on MCOs to manage physical health care, a growing number of states are focusing on the integration of physical health, behavioral health and long-term services and supports under the umbrella of managed care. States mentioned that expanding the scope of managed care involves a number of specific challenges, including the procurement and contracting for Medicaid health plans, the need for effective oversight of MCO contracts and performance and the new potential challenges from the recently proposed CMS rules for Medicaid managed care.
Ensuring that information technology systems are in place to support program operations with constrained administrative resources. In almost half of states, systems and administrative initiatives were listed as a top priority for FY 2016. These priorities include procurement or implementation of new Medicaid Management Information Systems (MMIS), ongoing work on upgrades or replacement of eligibility systems, and other information technology or system projects designed to improve administrative efficiency and to achieve program goals. Development data analytics capability for is one example of using systems technology to develop information that can help a program run more effectively. Technology systems initiatives take several years to procure and often present major administrative challenges, especially since workload and demands on staff continue to increase while resources remain constrained in most states. Medicaid directors noted continued strain on administrative resources, in particular staff, as Medicaid programs are working to implement a number of major initiatives across multiple arenas (delivery system and payment reform, coverage expansions and information technology.)
Improving population health and addressing the social determinants of health. Expanding access to coverage and needed care was highlighted as a key element in addressing population health, especially among states implementing the ACA Medicaid expansion. However, broader efforts to improve population health are emerging priorities for Medicaid directors. State Medicaid programs are looking for opportunities to leverage other resources and stakeholders (such as state public health agencies and other payers) to improve the quality of care provided and ultimately affect health outcomes for the populations they serve. Pursuing these significant goals, however, has caused Medicaid to evolve into a major player in transforming the overall health care system.
Methodology
Methods
The Kaiser Commission on Medicaid and the Uninsured (KCMU) commissioned Health Management Associates (HMA) to survey Medicaid directors in all 50 states and the District of Columbia to identify and track trends in Medicaid spending, enrollment and policy making. This is the 15th annual survey, each conducted at the beginning of the state fiscal year from FY 2002 through FY 2016. Additionally, eight mid-fiscal year surveys were conducted during state fiscal years 2002-2004 and 2009-2013, when a large share of states were considering mid-year Medicaid policy changes due to state budget and revenue shortfalls. Findings from previous surveys are referenced in this report when they help to highlight current trends. Archived copies of past reports are available on the following page.
The KCMU/HMA Medicaid survey on which this report is based was conducted from June through August 2015. The survey instrument (in the Appendix) was designed to document policy actions states implemented in FY 2015 and adopted for FY 2016 (which began for most states on July 1, 2015.1) Each survey is designed to capture information consistent with previous surveys, particularly for eligibility, provider payment rates, benefits, long-term care and managed care. Each year, questions are added to address current issues, such as state actions to address rising costs for specialty prescription drugs.
Medicaid directors and staff provided data for this report in response to a written survey and a follow-up telephone interview. The survey was sent to each Medicaid director in June 2015. All 50 states and DC completed surveys and participated in telephone interview discussions in July and August 2015. The telephone discussions are an integral part of the survey to ensure complete and accurate responses and to record the complexities of state actions. At the time the survey and telephone discussion was completed, the Medicaid budget for FY 2016 had not been adopted in Illinois and Pennsylvania. For Pennsylvania, FY 2016 responses were generally based on the Executive Recommended Budget. FY 2016 information was incomplete for Illinois.
The survey does not attempt to catalog all Medicaid policies in place for each state. The focus is on changes in Medicaid policy and new initiatives that are implemented in FY 2015 and those adopted and planned for implementation in FY 2016. Experience has shown that adopted policies are sometimes delayed or not implemented, for reasons related to legal, fiscal, administrative, systems or political considerations, or due to delays in approval from CMS. Policy changes under consideration without a definite decision to implement are not included in the survey.
Appendix
Appendix: Survey Instrument
Endnotes
Report
Introduction
An archive of previous survey reports is available at: “50-State Medicaid Budget Survey Archives,” Kaiser Commission on Medicaid and the Uninsured, accessed October 1, 2015, https://www.kff.org/medicaid/report/medicaid-budget-survey-archives/.
State fiscal years begin on July 1 except for these states: NY on April 1; TX on September 1; AL, MI and DC on October 1.
Eligibility, Enrollment, Premiums and Cost-Sharing
New York transitioned parents with incomes between 138 percent FPL to 150 percent FPL who received an additional Medicaid-funded premium wrap to purchase coverage in the Marketplace to the BHP.
Family planning waivers and SPAs offer limited benefits while the breast and cervical cancer treatment program and the medically needy spend-down programs offer full Medicaid benefits but are limited to those with either a specific condition or after meeting spend-down requirements. Medicaid for Pregnant Women varies in scope of services. Some states only cover services very directly related to the pregnancy while other states deem that any health care issue could possibly affect a pregnancy.
Previously this requirement had applied to states that applied alternative cost-sharing arrangements under 42 U.S.C. § 1396o-1.
David Machledt and Jane Perkins, Medicaid Premiums and Cost Sharing (Washington, DC: National Health Law Program, March 25, 2014), http://www.healthlaw.org/publications/browse-all-publications/Medicaid-Premiums-Cost-Sharing#.Vg1KQ_lVhBe.
Since the survey was fielded, two states (AZ and MI) have submitted waiver requests that include premium and cost-sharing proposals. Each of these waiver proposals must be approved by CMS before the states could implement such changes. Additionally, state legislation in Ohio requires the state to seek a waiver to implement Health Savings Accounts (HSAs) for non-disabled adults in Ohio Medicaid. The state is still developing such a proposal; at the time of this report, no proposal had been publicly released.
- Arizona released a waiver proposal in August 2015 based on state legislation calling for the establishment of HSAs with contributions of up to 2 percent of income for new adults and copayments of up to $25 for non-emergent use of the emergency room.
Arizona Health Care Cost Containment System, Arizona’s Application for a New Section 1115 Demonstration (Arizona: Arizona Health Care Cost Containment System, September 2015), http://www.azahcccs.gov/shared/Downloads/AZWaiverPackage9-30-15RealFinal.pdf.
Nick Lyon, Amendment to Michigan’s Section 1115 Demonstration Known as the “Healthy Michigan Plan” Submitted Under Authority of Section 1115 of the Social Security Act (Michigan: Michigan Department of Health and Human Services, September 1, 2015), http://www.michigan.gov/documents/mdch/CMS_HMP_1115_Waiver_Amendment_Submission_498740_7.pdf.
“FY 2016- 2017 State Budget – Health Savings Accounts,” Ohio Department of Medicaid, accessed October 1, 2015, http://medicaid.ohio.gov/INITIATIVES/StateBudget.aspx.
In order to impose higher cost sharing than otherwise allowed under federal law, a state needs to meet separate cost sharing waiver requirements under Section 1916(f) of the Social Security Act. Section 1916(f) permits a state to seek a demonstration waiver to charge cost sharing above otherwise allowable amounts if the state meets specific requirements and criteria, including testing a unique and previously untested use of copayments and limiting the demonstration to no longer than two years.
Robin Rudowitz, Samantha Artiga and MaryBeth Musumeci, The ACA and Medicaid Expansion Waivers (Washington, DC: Kaiser Commission on Medicaid and the Uninsured, February 2015), https://www.kff.org/report-section/the-aca-and-medicaid-expansion-waivers-issue-brief/.
Michigan released a waiver proposal in September 2015 based on state legislation calling for those with incomes between 100 and 138% FPL who have had coverage through the Healthy Michigan Plan for 48 cumulative months to be given the choice of either purchasing private insurance through the Marketplace with eligibility for advanced premium tax credits and cost-sharing reductions or remain in Healthy Michigan Plan but with increased cost-sharing and premiums capped at 7% of income (instead of federal maximum of 5%.) Such beneficiaries would also have increased monthly contributions (up to 3.5%) that could be reduced if they complete healthy behavior activities. If approved, this change would not go into effect until April 1, 2018. If this waiver is not approved, state law requires that the Healthy Michigan Plan ends as of April 30, 2016.
Nick Lyon, Amendment to Michigan’s Section 1115 Demonstration Known as the “Healthy Michigan Plan” Submitted Under Authority of Section 1115 of the Social Security Act (Michigan: Michigan Department of Health and Human Services, September 1, 2015), http://www.michigan.gov/documents/mdch/CMS_HMP_1115_Waiver_Amendment_Submission_498740_7.pdf.
Kaiser Commission on Medicaid and the Uninsured, Proposed Medicaid Expansion in Montana (Washington, DC: Kaiser Commission on Medicaid and the Uninsured, September 2015), https://www.kff.org/medicaid/fact-sheet/proposed-medicaid-expansion-in-montana/.
This is in lieu of the “217-like option” which had been approved by CMS as part of the state’s comprehensive waiver, but proved challenging to implement.
Managed Care Reforms
Mississippi is included in the counts for states operating MCOs; however, its risk-based managed care program as of July 1, 2015 did not cover inpatient hospital services. Idaho’s MMCP program, which is secondary to Medicare, has been re-categorized by CMS from a PAHP to an MCO by CMS but is not counted here as such. California has a small PCCM program operating in LA County for those with HIV. Wyoming’s Patient Centered Medical Home program uses PCCM authority to make PMPM payments but is not counted here as such.
California notes that the delivery of substance abuse services is moving to an “Organized Delivery System operated by counties” in FY 2016. For purposes of this report, this new arrangement is treated as a PHP as it is recognized at the federal level.
One MCO state (North Dakota) had no children enrolled in its MCO which is limited to Medicaid expansion adults; they are therefore excluded from this count.
There are 10 MCO states (DE, GA, HI, ND, NH, NV, TN, TX, VA and WV) that either do not cover adult dental services or only cover emergency dental services for adults. Georgia and Tennessee indicated that MCOs could offer adult dental services as a value-added benefit or cost effective alternative.
Maryland indicated that MCOs could offer add-on adult dental plans for non-covered populations.
The “Program of all All-Inclusive Care for the Elderly” (PACE) is a capitated managed care benefit for the frail elderly provided by a not-for-profit or public entity that features a comprehensive medical and social service delivery system. It uses a multidisciplinary team approach in an adult day health center supplemented by in-home and referral services in accordance with participants' needs.
For purposes of this survey, Idaho Medicare Medicaid Coordinated Plan is considered a PHP rather than an MCO as Medicare provides primary coverage for primary and acute care including inpatient hospital services.
Hawaii and Tennessee auto assign all new members to a health plan and then offer them a choice.
80 Fed. Reg. 31097-31297 (June 1, 2015), available at https://federalregister.gov/a/2015-12965.
Julia Paradise and MaryBeth Musumeci, Proposed Rule on Medicaid Managed Care: A Summary of Major Provisions (Washington, DC: Kaiser Commission on Medicaid and the Uninsured, July 23, 2015), https://www.kff.org/medicaid/issue-brief/proposed-rule-on-medicaid-managed-care-a-summary-of-major-provisions/.
Julia Paradise and MaryBeth Musumeci, Awaiting New Medicaid Managed Care Rules: Key Issues to Watch (Washington, DC: Kaiser Commission on Medicaid and the Uninsured, March 24, 2015), https://www.kff.org/medicaid/issue-brief/awaiting-new-medicaid-managed-care-rules-key-issues-to-watch/.
National Association of Medicaid Directors, Comments on Medicaid and Children’s Health Insurance Programs; Medicaid Managed Care, CHIP Delivered in Managed Care, Medicaid and CHIP Comprehensive Quality Strategies and Revisions Related to Third Party Liability (CMS-2390-P) (Washington, DC: National Association of Medicaid Directors, July 27, 2015), http://medicaiddirectors.org/node/1241.
Emerging Delivery System and Payment Reforms
“Patient-Centered Medical Home Recognition,” National Committee on Quality Assurance, accessed October 1, 2015, http://www.ncqa.org/Programs/Recognition/Practices/PatientCenteredMedicalHomePCMH.aspx.
Kaiser Commission on Medicaid and the Uninsured, Medicaid Delivery System and Payment Reform: A Guide to Key Terms and Concept, (Washington, DC: Kaiser Commission on Medicaid and the Uninsured,) June 2015 Fact Sheet. http://files.kff.org/attachment/issue-brief-medicaid-delivery-system-and-payment-reform-a-guide-to-key-terms-and-concepts.
Kaiser Commission on Medicaid and the Uninsured, Medicaid Delivery System and Payment Reform: A Guide to Key Terms and Concept (Washington, DC: Kaiser Commission on Medicaid and the Uninsured, June 2015), http://files.kff.org/attachment/issue-brief-medicaid-delivery-system-and-payment-reform-a-guide-to-key-terms-and-concepts.
Ibid.
Long-Term Services and Supports Reforms
Steve Eiken, Kate Sredl, Brian Burwell and Paul Saucier, Medicaid Expenditures for Long-Term Services and Supports (LTSS) in FY 2013 (Truven Health Analytics, June 30, 2015), http://www.medicaid.gov/medicaid-chip-program-information/by-topics/long-term-services-and-supports/downloads/ltss-expenditures-fy2013.pdf.
The “Program of all All-Inclusive Care for the Elderly” (PACE) is a capitated managed care benefit for the frail elderly provided by a not-for-profit or public entity that features a comprehensive medical and social service delivery system. It uses a multidisciplinary team approach in an adult day health center supplemented by in-home and referral services in accordance with participants' needs.
California Department of Health Care Services, DHCS Issues Statement Regarding the Section 811 Project Rental Assistance Demonstration Program (California: Department of Health Care Services, February 2013), http://www.dhcs.ca.gov/Documents/13-1%20Section%20811%20Demo.pdf.
“Conflict-free case management” assures, in part, that the person or entity that conducts the functional assessment and/or case management services for a member does not also provide services to that individual.
Single points of entry (SPOE) systems offer consumers one-stop access to information, support, and linkages to local care services thereby reducing service fragmentation and simplifying access to long-term supports and services.
Tennessee also reported implementing an individual cost cap in one of its IDD HCBS waivers in FY 2015, but noted that persons whose services exceeded the cap were transitioned to another waiver with an aggregate cost cap so that their services would not be reduced. Also South Carolina) reported temporarily suspending its Certificate of Need program during parts of FY 2014 and FY 2015, but noted that the state did not experience any increases in institutional capacity during that period.
Molly O’Malley Watts, Erica L Reaves and MaryBeth Musumeci, Medicaid Balancing Incentive Program: A Survey of Participating States (Washington, DC: Kaiser Commission on Medicaid and the Uninsured, June 2015), https://www.kff.org/medicaid/report/medicaid-balancing-incentive-program-a-survey-of-participating-states/.
Until June 2014, Indiana operated as a Section 209(b) state; under Section 209(b) of the Social Security Act, states may develop their own disability determination methods for determining eligibility for aged, blind, and disabled groups. As part of this option, states must operate a spend-down program. In June 2014, Indiana switched to operate as a Section 1634 state, which relies on disability determinations by the Social Security Administration. As a Section 1634 state, Indiana no longer had to operate a spend-down program.
New York reported implementing this option in FY 2015, but was awaiting final SPA approval at the time of the survey. The SPA calls for retroactive implementation. New York State Department of Health, State Plan Amendment #13-35 Community First Choice Option (New York: New York State Department of Health, December 30, 2013), https://www.health.ny.gov/regulations/state_plans/status/non-inst/original/docs/os_2013-12-30_spa_13-35.pdf.
Centers for Medicare and Medicaid Services, Fact Sheet: Summary of Key Provisions of the Home and Community-Based Services (HCBS) Settings Final Rule (CMS 2249-F/2296-F) (Washington, DC: Centers for Medicare and Medicaid Services, January 10, 2014), http://www.medicaid.gov/Medicaid-CHIP-Program-Information/By-Topics/Long-Term-Services-and-Supports/Home-and-Community-Based-Services/Downloads/HCBS-setting-fact-sheet.pdf
Provider Rates, Taxes and Benefits
An additional state (Pennsylvania) had also not enacted a budget at the time of the survey. The state reported current plans but indicated that final actions depended on the final budget approved by state lawmakers.
Rates for FY 2016 not yet determined at the time of the survey included MCO rates for Florida and all rates for Illinois.
Illinois indicated that the rate restriction reported for nursing facilities in FY 2015 reflects a composite of a 10 month increase in rates and a two month decrease in rates.
Stephen Zuckerman and Dana Goin, How Much Will Medicaid Physician Fees for Primary Care Rise in 2013? Evidence from a 2012 Survey of Medicaid Physician Fees (Washington, DC: Kaiser Commission on Medicaid and the Uninsured, December 2012), https://www.kff.org/medicaid/issue-brief/how-much-will-medicaid-physician-fees-for/.
Some states also have premium or claims taxes that apply to managed care organizations and other insurers. Since this type of tax is not considered a provider tax by CMS, these taxes are not counted as provider taxes in this report.
Centers for Medicare and Medicaid Services, CMCS Informational Bulletin: Clarification of Medicaid Coverage of Services to Children with Autism (Washington, DC: Centers for Medicare and Medicaid Services, July 2014), http://www.medicaid.gov/Federal-Policy-Guidance/Downloads/CIB-07-07-14.pdf.
New York State Department of Health, State Plan Amendment #13-35 Community First Choice Option (New York: New York State Department of Health, December 30, 2013), https://www.health.ny.gov/regulations/state_plans/status/non-inst/original/docs/os_2013-12-30_spa_13-35.pdf.
In years past, New Mexico was reported as having a PDL. In this year’s survey, the state clarified that while the Medicaid MCOs have their own PDLs, the state does not have its own PDL.
In accordance with federal and state law, states pay the lower of (a) the ingredient cost rate plus a dispensing fee; (b) the Federal Upper Limit (FUL) or State Maximum Allowable Cost rate, if applicable, plus a dispensing fee; or (c) the pharmacy’s Usual and Customary Charge.
77 Fed. Reg. 5318-5367 (February 2, 2012), available at http://www.gpo.gov/fdsys/pkg/FR-2012-02-02/pdf/2012-2014.pdf.
Centers for Medicare and Medicaid Services, CMCS Informational Bulletin: Medicaid Pharmacy – Survey of Retail Prices (Washington, DC: Centers for Medicare and Medicaid Services, May 31, 2012), http://www.medicaid.gov/Federal-Policy-Guidance/Downloads/CIB-05-31-12.pdf.
“Medicaid Covered Outpatient Drug Rule Currently under OMB Review,” National Association of Medicaid Directors Newsletter, accessed August 18, 2015, http://medicaiddirectors.org/node/1249.
Brian Bruen and Katherine Young, What Drives Spending and Utilization on Medicaid Drug Benefits in States? (Washington, DC: Kaiser Commission on Medicaid and the Uninsured, December 2014), http://files.kff.org/attachment/brief-what-drives-spending-and-utilization-on-medicaid-drug-benefits.
The Express Scripts Lab, The 2014 Drug Trend Report (Saint Louis, Missouri: The Express Scripts Lab, March 2015), http://lab.express-scripts.com/drug-trend-report/.
Ibid. According to Express Scripts, roughly half of specialty drug expenditures are billed through the medical benefit (rather than the pharmacy benefit) and are not included in its trend calculations.
Methodology
Methods
State fiscal years begin July 1 except for these states: NY on April 1; TX on September 1; AL, MI and DC on October 1.