How OBGYNs Adapted Provision of Sexual and Reproductive Health Care During the COVID-19 Pandemic
Summary
The 2020 KFF National Physician Survey on Reproductive Health obtained responses from a nationally representative sample of OBGYNs practicing in the United States who provide sexual and reproductive health care to patients in office-based settings. The survey was designed and analyzed by researchers at KFF (the Kaiser Family Foundation). An independent research company, SSRS, carried out the fieldwork and collaborated on questionnaire design, pretesting, sample design, and weighting. KFF paid for all costs associated with the survey. Survey responses were collected via paper and online questionnaires from March 18 and September 1, 2020, from a random sample of 1,210 OBGYNs. All OBGYNs included in the sample were sent an invitation letter encouraging them to participate as well as an incentive, described below. The initial sample release in March 2020 corresponded with the emergence of the COVID-19 pandemic. As such, after the initial sample release, additional questions were added related to how the COVID-19 pandemic impacted providers. Among the 1,210 OBGYNs, 855 OBGYNs completed the additional questions related to COIVD-19. The samples were weighted to match known demographics. Taking into account the design effect, the margin of sampling error for the total sample is +/-4 percentage points at the 95% confidence level. The margin of error for the sample who completed the COVID-19 supplemental section +/-6 percentage points. All statistical significance testing was set at p <0.05.
Sample Design
The sample of OBGYNs was procured from IQVIA via their OneKey Database. The OneKey database integrates provider information from various sources (e.g., IMS Health, SK&A, and Healthcare Data Solutions) and is continually updated through telephone and desktop research. The IQVIA OBGYN population universe is about 46,815 and a sample of 6,288 records were selected for this study. Using the survey questionnaire, the sample was then further screened to include only those who are board certified, spend at least 60% of their time providing direct patient care, and provide sexual and reproductive health care to at least 10% of their patients in an office-based setting.
A two-wave sample release design was used for this study to enable adjustments to the sample release and improve representativeness as a result of non-response. In Wave 1, the sample included an oversample of OBGYNs who work in rural areas, work in a public setting and those that had 25% or more of their patients covered by Medicaid, in order to obtain a reliable sample of these key groups of interest. ZIP code of the office, profit status of the facility and median income of the practice location were used as proxies to target these groups respectively. After the initial sample release, SSRS reviewed the productivity of the sample to model the second release. The number of OBGYNs working in a public setting was lower than anticipated, therefore Wave 2 again included an oversample of OBGYNs in public practice.
Contact Design
In an effort to maximize the survey completion rate, OBGYNs were contacted by multiple modes (mail, email) and offered the opportunity to complete the questionnaire either on paper or online. Those who completed the paper survey mailed back their responses using a prepaid reply envelope. OBGYNs were sent an up-front cash $2 bill incentive as well as an incentive check for $75 in the first two mailings to encourage respondents to complete the survey. Respondents received up to five communications for the main survey, four postal mailings and one email. The Wave 1 release corresponded with the emergence of the COVID-19 pandemic. As such, after the initial sample release, additional questions were added related to how the COVID-19 pandemic impacted providers. Wave 1 completes were recontacted and asked to complete these questions, with up to two additional communications, one postal and one email. The Wave 2 release was sent the main survey as well as the COVID-19 questions to complete.
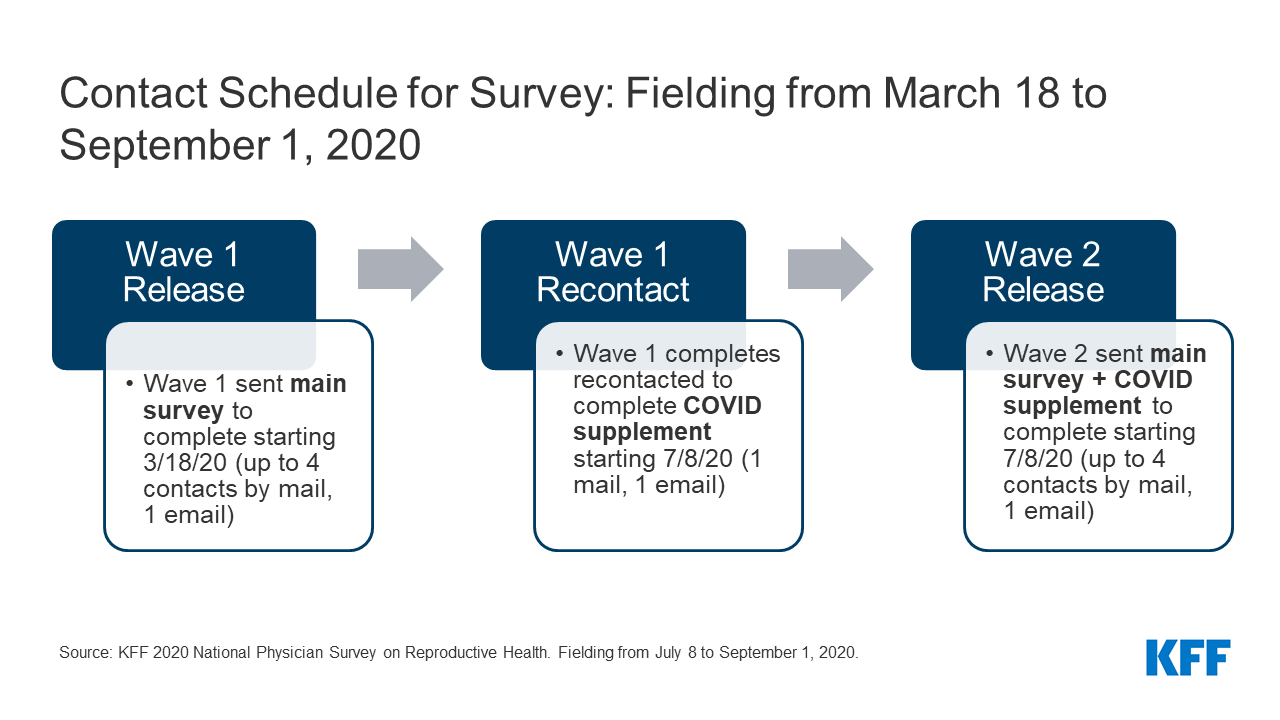
Contact Schedule for Survey: Fielding from March 18 to September 1, 2020
Response Rate
The response rate for the OBGYNs was 22.1% and was calculated using AAPOR’s RR3 (53% completes by web, 47% by mail).
Weighting
The sample was weighted in stages. The first stage of the weighting was the application of a base weight to account for the disproportionately-stratified samples and response rates across sample strata. In the second stage of weighting, the OBGYN sample was post-stratified to match the IQVIA frame on key variables. In the final stage, self-reported sample demographics were matched to population parameters from the AMA database. Qualified respondents’ weights were then rebalanced to the total complete sample size. Because a selection of questions about COVID-19 were added to the survey after the first wave of sample had been released, a second weight was calculated based on respondents who received the supplement and was used for analyses of those questions.
Analysis
A series of data quality checks were run, including removing duplicate cases (n = 32). We compared survey responses by key physician and practice demographics. Gender, age and race were determined by physician self-report. Practice type was determined by physician self-report; those who indicated they work in private practice or a health maintenance organization were classified as “private,” while those who indicated they work in a community health center, a family planning clinic or a government operated health department were classified as “public.” Practice size was determined by the number of full-time equivalent (FTE) physicians or advance practice clinicians (small ≤ 3, medium 4-10, large >10). Urbanicity and region were determined by the ZIP code of the practice, using U.S. census definitions and breaks.
Demographics of Survey Respondents for the COVID-19 Supplement
| Demographics of Survey Respondents for COVID-19 Supplement | ||
| Characteristic | Weighted n (%) | |
| Overall OBGYNs | 855 (100%) | |
| Gender | Female | 552 (65%) |
| Male | 294 (34%) | |
| Age | <45 | 312 (37%) |
| 45-54 | 214 (26%) | |
| 55-64 | 174 (21%) | |
| 65+ | 136 (16%) | |
| Race | White | 587 (69%) |
| Black | 84 (10%) | |
| Asian | 115 (13%) | |
| Other | 67 (8%) | |
| Practice type | Public | 133 (16%) |
| Private | 704 (82%) | |
| Practice size | Large (>10 FTE) | 176 (21%) |
| Medium (4-10 FTE) | 423 (49%) | |
| Small (≤ 3 FTE) | 241 (28%) | |
| Urbanicity | Urban | 488 (57%) |
| Suburban | 166 (19%) | |
| Rural | 136 (16%) | |
| Region | West | 199 (23%) |
| Northeast | 168 (20%) | |
| Midwest | 178 (21%) | |
| South | 305 (36%) | |
| A small percentage of respondents left demographic questions blank or their responses were unspecified, including n= 8 (1%) for gender, 18 (2%) for age, 3 (<1%) for race, 18 (2%) for practice type, 15 (2%) for practice size, 65 (8%) for urbanicity and 5 (1%) for region. | ||