How Does Use of Medicaid Wraparound Services by Dual-Eligible Individuals Vary by Service, State, and Enrollees’ Demographics?
Issue Brief
In 2021, 12.9 million people received health coverage through both the Medicare and Medicaid programs. For those “dual-eligible individuals,” Medicare is the primary payer and covers medical acute and post-acute care, including skilled nursing facility services and home health care. Medicaid wraps around Medicare coverage by paying Medicare premiums and in most cases, cost sharing. Most dual-eligible individuals (9.5 million people in 2021) are also eligible for Medicaid benefits that are not otherwise covered by Medicare, including long-term services and supports (LTSS), vision, and dental care (referred to here as Medicaid “wraparound services” for dual-eligible individuals).
Dual-eligible individuals tend to have low incomes, high rates of long-term disabilities, and multiple chronic conditions. Without coverage of wraparound services under Medicaid, some dual-eligible individuals might be unable to obtain services such as eye exams, treatment for cavities, help bathing and moving to avoid bedsores; or they may have to make difficult choices between paying out-of-pocket for those types of services and paying for their groceries. But Medicaid coverage of these services varies widely across states, potentially leading to variation in access and use among dual-eligible individuals.
This issue brief describes the share of dual-eligible individuals with full Medicaid benefits who use wraparound services, including institutional LTSS, home- and community-based services (HCBS), vision services, dental care, and non-emergency medical transportation (NEMT); and how use of these services varies by state and select demographic characteristics of enrollees. The analysis includes 7.2 million individuals with at least 10 months of full Medicaid coverage in 2019 Medicaid claims data from T-MSIS (see Methods). The analysis presents data from 2019, which are expected to be more representative of non-pandemic utilization trends than data from 2020, the most recent year of data available when the analysis was conducted. Key takeaways include:
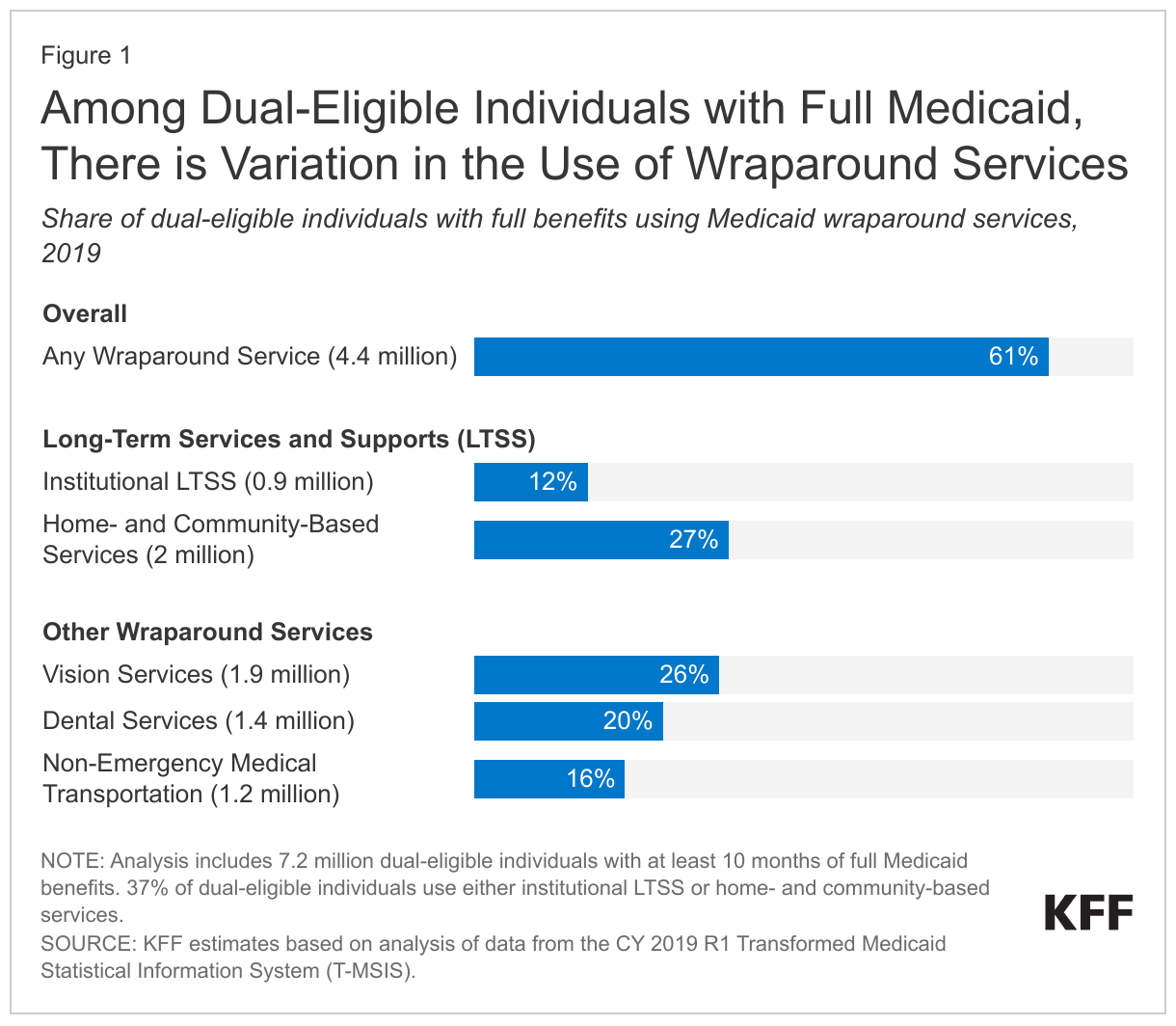
- Just over 6 in 10 (61%) of the 7.2 million dual-eligible individuals with at least 10 months of full Medicaid coverage (4.4 million people) use at least one Medicaid wraparound service.
- Around one-fourth of full-benefit dual-eligible individuals use home- and community-based services (27%) or vision services (26%), while rates of use are lower for dental care (20%), NEMT (16%), and institutional LTSS (12%). Over one-third of dual-eligible individuals (37%) use some type of LTSS—either institutional care or HCBS.
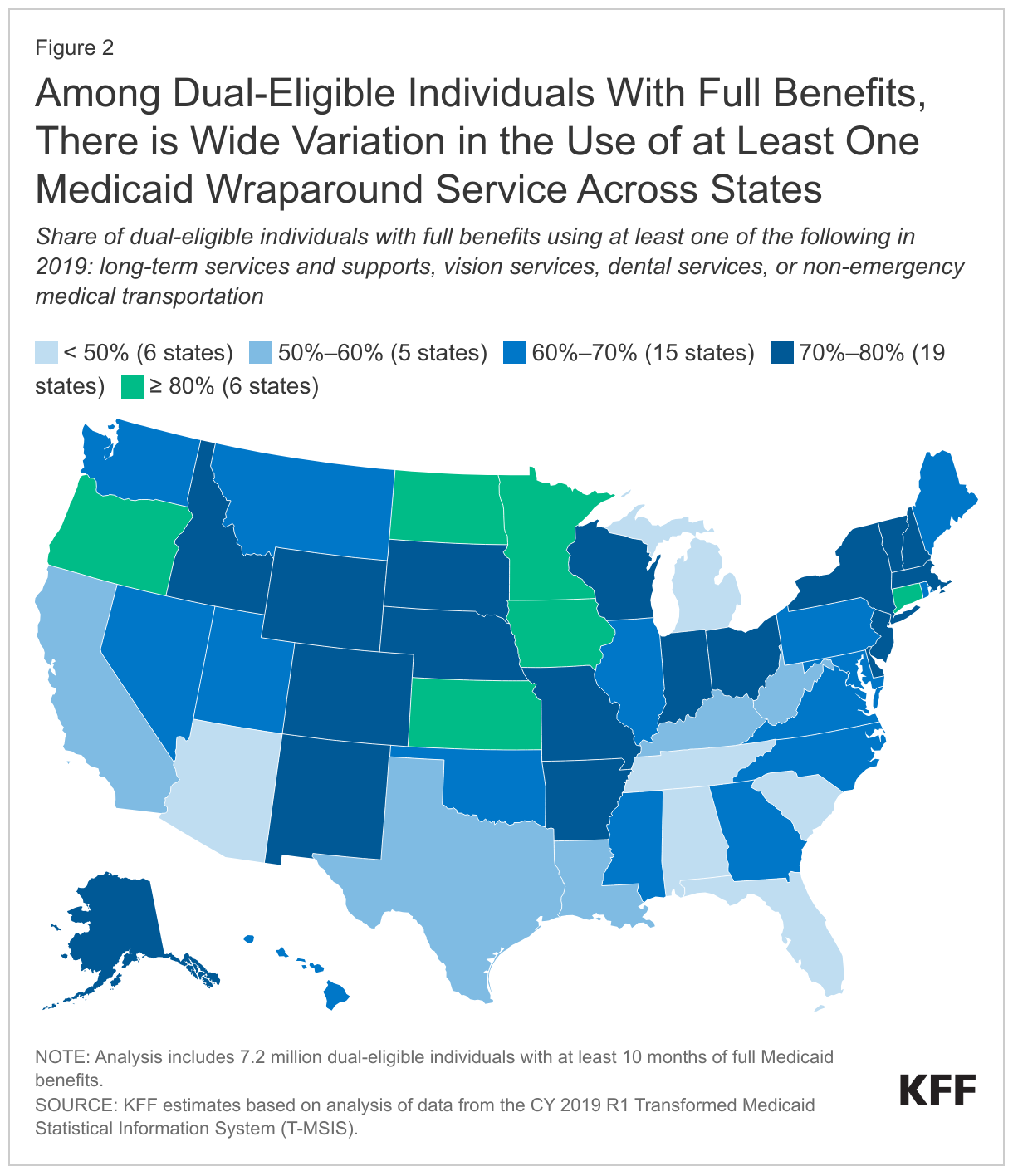
- The percentage of full-benefit dual-eligible individuals that use at least one Medicaid wraparound service in 2019 ranges from 32% in Florida to 88% in Minnesota. That variation stems from variation in rates of use for all specific services included in the analysis.
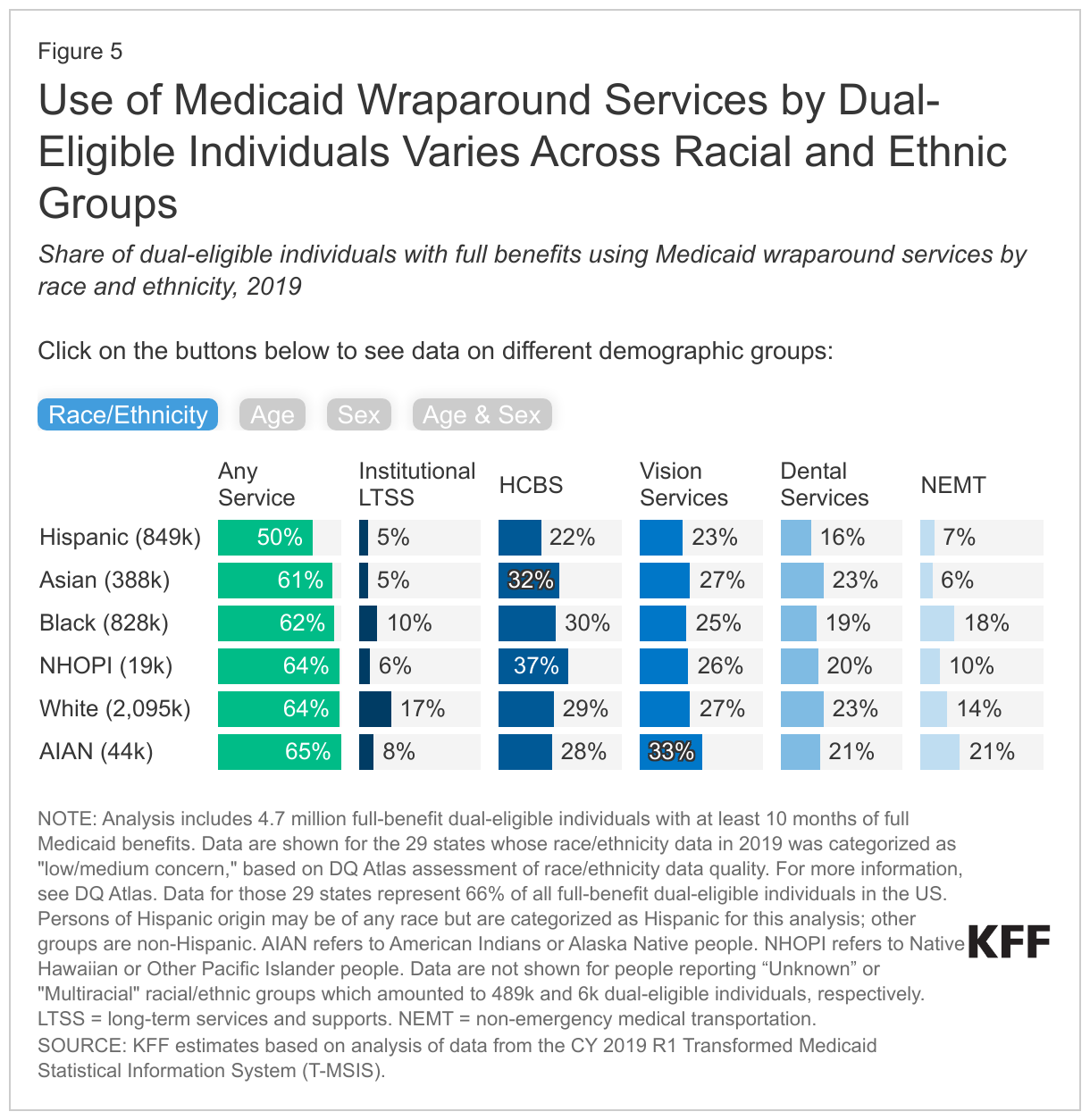
- Dual-eligible individuals who are Hispanic use Medicaid wraparound services at lower rates than those who are not Hispanic (50% use one or more wraparound service compared with 61%-65% among other racial and ethnic groups).
- Dual-eligible individuals who are ages 65 and older have higher rates of use of institutional LTSS and vision services than those who are younger and qualify for coverage based on a disability (16% vs. 5%, and 28% vs. 24%).
- Variation in rates of Medicaid wraparound service use may stem from differences in peoples’ health status, demographic characteristics, states’ coverage of various services, enrollees’ awareness of Medicaid’s benefits, type of Medicare coverage, and other factors that affect people’s need for and access to care.
How many dual-eligible individuals use Medicaid wraparound services and how does the use of services vary across service types?
Among the 7.2 million dual-eligible individuals with at least 10 months of full Medicaid, roughly 61% (4.4 million) of dual-eligible individuals with full Medicaid benefits use at least one Medicaid wraparound service, but rates of use for individual services are lower (Figure 1). The wraparound services in this analysis include services that states are required to cover and services that states may elect to cover. Required services include nursing facility care (which is part of institutional LTSS), home health care (which is part of HCBS), and NEMT. Optional services include dental care, vision care, and all HCBS other than home health. Rates of use by dual-eligible individuals for Medicaid wraparound services by type of service are:
- 27% for HCBS (2 million dual-eligible individuals),
- 26% for vision care (1.9 million),
- 20% for dental care (1.4 million),
- 16% for NEMT (1.2 million), and
- 12% for institutional LTSS (0.9 million) (Figure 1).
Rates of use for wraparound services among dual-eligible individuals differ from rates for Medicaid enrollees who are eligible because they have a disability or are ages 65 and older but don’t have Medicare. Such enrollees tend to be younger than dual-eligible individuals because most people ages 65 and older do have Medicare. As a result, they have lower rates of use of institutional LTSS and HCBS, but relatively similar rates of use for other wraparound services (Appendix Figure 1).
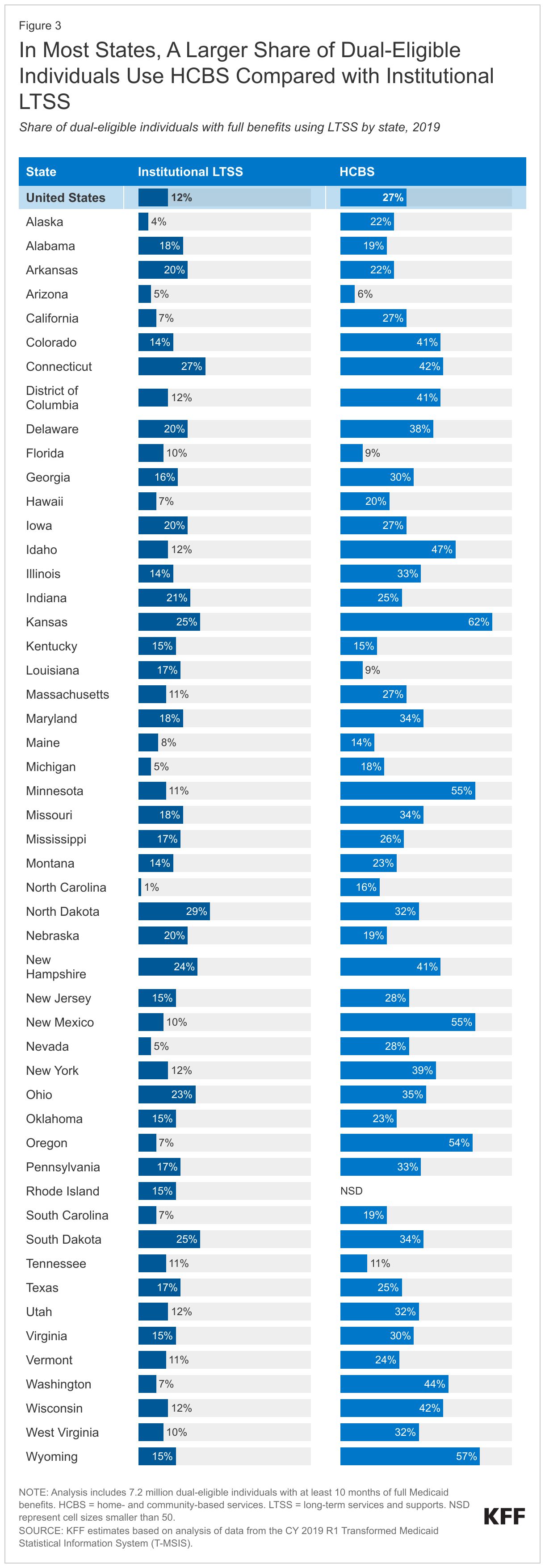
For LTSS wraparound services, a larger share of dual-eligible individuals with full Medicaid benefits use HCBS than institutional LTSS (Figure 1). LTSS are generally provided either in institutional settings, such as a nursing facility or an intermediate care facility for people with intellectual disabilities, or in home- and community-based settings. HCBS include a broad range of benefits, such as access to personal care, adult day care, and senior centers, which are all optional benefits, except for home health care (which is also covered by Medicare). Within Medicaid in 2020, more Medicaid enrollees use HCBS than institutional LTSS and in this analysis, over twice as many dual-eligible individuals use HCBS compared with institutional LTSS (27% compared with 12% respectively). In 2020, dual-eligible individuals who used any Medicaid wraparound LTSS accounted for nearly two-thirds of all people who used Medicaid LTSS that year.
For non-LTSS wraparound services, rates of use were highest for vision care, followed by dental care, and NEMT (Figure 1). For the purposes of this analysis, vision care is defined to exclude services that are covered by traditional Medicare such as treatment for cataracts and glaucoma. Vision care includes eye exams and eyewear (contacts or eyeglasses) and dental care includes oral exams, routine cleanings, and more extensive services such as fillings, extractions, and root canals (see Methods for more details). NEMT provides those in need with assistance getting to and from non-emergency medical appointments and covers a broad range of modes of transportation including taxis, buses, vans, and personal vehicles. Wraparound vision and dental services are generally not covered by traditional Medicare but are often covered by Medicare Advantage plans as supplemental benefits.
How does the use of wraparound services vary across states?
The percentage of full-benefit dual-eligible individuals using at least one Medicaid wraparound service ranges from 32% in Florida to 88% in Minnesota (Figure 2). In Alabama, Arizona, Florida, Michigan, South Carolina, and Tennessee, fewer than half of dual-eligible individuals use any Medicaid wraparound services. Among those states, Alabama and Florida have relatively low rates of use for all specific services. More than 8 in 10 use one or more wraparound services in Connecticut, Iowa, Kansas, Minnesota, North Dakota, and Oregon, with Minnesota having high rates of each of the services except institutional LTSS.
In 45 states, more dual-eligible individuals with full benefits use HCBS than institutional LTSS, but there is wide variation in rates of HCBS use across states (Figure 3). Higher rates of HCBS use stem from initiatives to remove what has been referred to as the “institutional bias” in Medicaid. The percentage of full-benefit dual-eligible individuals who use HCBS ranges from less than 10% in Arizona, Florida, and Louisiana to over 50% in Kansas, Minnesota, New Mexico, Oregon, and Wyoming. However, some of those low rates of HCBS use may reflect states’ difficulty reporting HCBS service use in the Medicaid claims data: For example, a prior KFF analysis noted that HCBS users were likely undercounted in Rhode Island on account of missing HCBS records. States with high rates of HCBS use among dual-eligible individuals also tend to have high rates of HCBS use among other Medicaid enrollees (Appendix Figure 2).
The percentage of dual-eligible individuals who use institutional LTSS ranges from fewer than 5% in Alaska and North Carolina to more than 25% in Connecticut and North Dakota. Beyond states’ coverage policies, the age and health status of dual-eligible individuals is a determinant for LTSS use: KFF analyses find that overall, Medicaid enrollees who use LTSS tend to be older and have long-term health conditions.
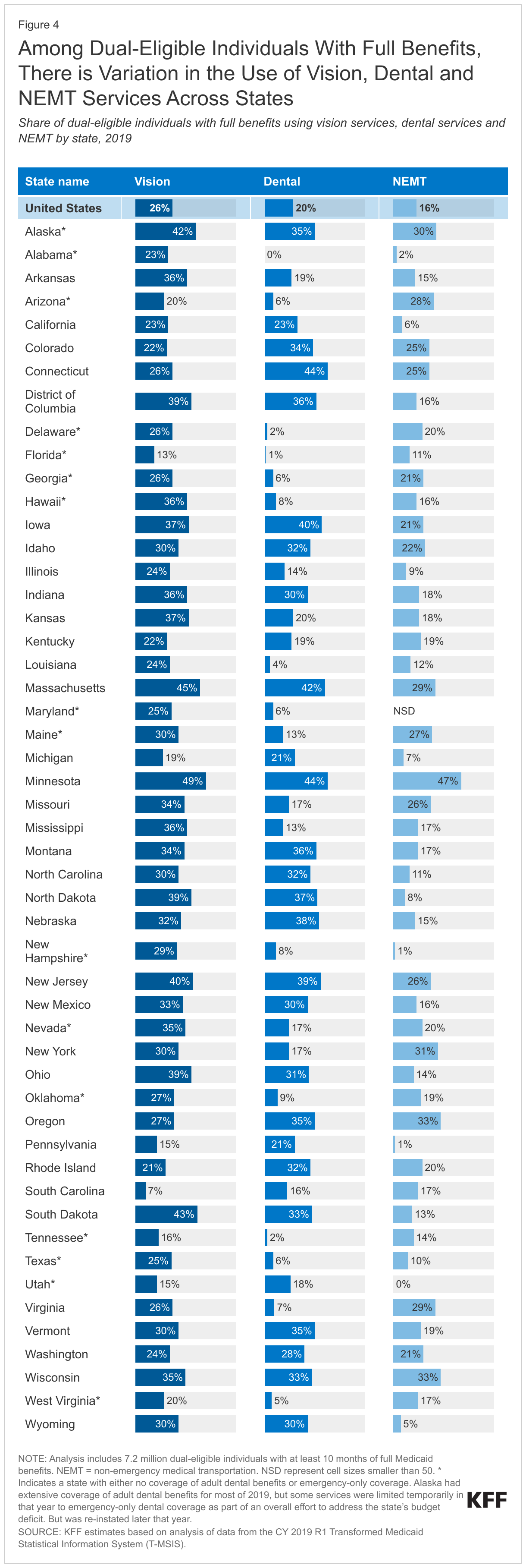
Across states, the percentage of dual-eligible individuals that use the non-LTSS wraparound services, vision, dental, and NEMT, ranges from the low single digits to nearly half (Figure 4). Such variation may stem from Medicaid coverage and administrative policies as states with higher rates of use among dual-eligible individuals also have higher rates of use among other Medicaid enrollees (Appendix Figure 2).
- Vision. The percentage of full-benefit dual-eligible individuals who use Medicaid wraparound vision services ranges from 7% in South Carolina to almost 50% in Minnesota, which may reflect, in part, differences in Medicaid coverage of vision services.
- Dental. The percentage of dual-eligible individuals who used Medicaid wraparound dental services ranges from 1% or fewer in Florida and Alabama to 44% in Connecticut and Minnesota, also reflecting, in part, differences in coverage of adult dental benefits. Among the 14 states with fewer than 10% of dual-eligible individuals using dental services, all but one state had either no coverage of adult dental benefits or emergency-only coverage.
- Non-Emergency Medical Transportation. The percentage of full-benefit dual-eligible individuals who use NEMT ranges from 1% or fewer of dual-eligible individuals in Utah, New Hampshire, and Pennsylvania to 47% in Minnesota. Other studies have found that there is significant variation in NEMT access across states, but also significant variation in states’ reporting of NEMT use.
Variation across states in the use of wraparound services reflects a host of factors including factors that are common across all Medicaid enrollees regardless of whether they have Medicare, but also including factors that are unique to dual-eligible individuals. States that have higher percentages of dual-eligible individuals using wraparound services often have higher use rates among Medicaid-only enrollees who are eligible because they have a disability or are ages 65 and older (Appendix Figure 2). Similarities in the variation of use rates between dual-eligible individuals and Medicaid-only enrollees highlight the role of Medicaid-specific factors in determining how readily people access wraparound services. Some of the factors that are common across all Medicaid enrollees regardless of whether they have Medicare include:
- States’ coverage of each wraparound service,
- States’ administrative policies that make it easier or harder for people to access the services,
- The number of providers of each service and their appointment availability (which reflects states’ payment rates among other factors), and
- The extent to which records of services are completely and properly reported in the data.
Other factors affect rates of service use that are unique to dual-eligible individuals including:
- People’s need for services such as LTSS, dental and vision services (which reflects the characteristics of states’ dual-eligible individuals),
- Dual-eligible individuals’ awareness of Medicaid wraparound service availability and coverage, and
- Dual-eligible individuals’ access to wraparound services in programs other than Medicaid (such as Medicare Advantage plans).
How does the use of wraparound services vary across dual-eligible individuals with different demographic characteristics?
Full-benefit dual-eligible individuals who are Hispanic use Medicaid wraparound services at lower rates than other racial and ethnic groups (Figure 5, Race/Ethnicity tab). Only half of dual-eligible individuals who are Hispanic access one or more wraparound services whereas over 60% of all other groups do. The overall disparity reflects differences in use rates for all specific service types, which are below 10% for institutional LTSS and NEMT, 16% for dental care, and below 25% for HCBS and vision services. Dual-eligible individuals who are Asian also have low use rates for institutional LTSS (5%) and NEMT (6%), but 23% use dental services, 27% use vision services, and nearly one-third use HCBS. The highest rates of service use are among dual eligible individuals who are American Indian or Alaskan Native (65% overall which reflects high rates of vision service use), White (64% overall which reflects high rates of institutional LTSS use), and Native Hawaiian or Other Pacific Islander (64% which reflects high rates of HCBS use). (These rates are among the 29 states that reported “low/medium concern” with the quality of their race and ethnicity data in 2019; these 29 states account for 66% of the dual-eligible population; see Methods for additional details).
Dual-eligible individuals ages 65 and older use institutional LTSS at a rate that is over three times higher than the rate for those under age 65 (16% compared with 5%), but they use dental services at a lower rate (Figure 5, Age tab). The percentage of dual-eligible individuals who use one or more wraparound services is 63% for those ages 65 and older and 59% for those under age 65. Differences in use rates are small for HCBS, vision services, and NEMT, but larger for dental services: 24% of those under age 65 use dental services compared with 17% of those ages 65 and older.
Among all dual-eligible individuals with full Medicaid, females use wraparound services at higher rates than males, but among those under age 65, rates of LTSS use are slightly higher for males (Figure 5, Sex and Age & Sex tabs). When age is not accounted for, males and females use individual services at similar rates, but a higher percentage of females use one or more service (64% compared with 58%). When males and females are grouped by age, males under age 65 have slightly higher rates of LTSS use (both institutional and HCBS), but lower rates of use for other services and lower rates of use overall.
What are the policy implications of variation in use of Medicaid wraparound services?
Medicaid provides wraparound services such as long-term services and supports, vision and dental care, and non-emergency medical transportation for dual-eligible individuals who tend to have low incomes, high rates of long-term disabilities, and chronic conditions. Among the 7.2 million dual-eligible individuals with at least 10 months of full Medicaid, 61% (4.4 million people) use at least one Medicaid wraparound service; however, use varies considerably by type of service and across states. The variation across states may be due to a number of factors, including differences in peoples’ health status, demographic characteristics, states’ coverage of various services, enrollees’ awareness of Medicaid’s benefits, and type of Medicare coverage among dual-eligible beneficiaries.
What do rates of wraparound service use suggest regarding the health and wellbeing of dual-eligible individuals and potential disparities among various groups? Dual-eligible individuals who are Hispanic have lower rates of use for all wraparound services as do people living in certain states, but it is unknown whether those lower rates reflect limited access to care, difficulty in navigating care and benefits across the two programs, or lower levels of need between different groups. For most services, the variation across states in rates of use is similar among dual-eligible individuals and Medicaid enrollees without Medicare who are eligible because of their age or disability. Those similarities suggest that specific features of state Medicaid programs—such as coverage levels, the availability of providers that take Medicaid, and the ease of accessing Medicaid services—may play some role in determining what share of dual-eligible individuals access wraparound services within a given state.
What are the implications of variation in the use of Medicaid wraparound services across states for dual-eligible individuals who are enrolled in traditional Medicare? According to a separate KFF analysis, 55% of dual-eligible individuals with full Medicaid benefits were in traditional Medicare in 2020, and the remaining 45% were in Medicare Advantage plans. For full-benefit dual-eligible individuals in traditional Medicare, Medicaid would provide the wraparound services included in this analysis. Dual-eligible individuals in traditional Medicare may have less access to these services if they live in states that do not offer these benefits or where Medicaid coverage of wraparound benefits is more limited than in other states with more generous benefits.
What are the implications of the availability of Medicaid wraparound services for dual-eligible individuals in Medicare Advantage plans? According to a separate KFF analysis, Medicare Advantage plans offer some of the wraparound services analyzed here, such as dental and vision, but typically not LTSS. Potential overlap between Medicare Advantage supplemental benefits and Medicaid wraparound services has prompted concerns among advocates and policymakers that enrollees in these plans may not be getting the full complement of wraparound benefits if benefits are not well coordinated between Medicare Advantage plans and Medicaid. Further, there is some concern that Medicare Advantage plans may be marketing these supplemental benefits to attract dual-eligible individuals, even though these beneficiaries may already have access to these benefits covered under their state Medicaid program. (Note that this analysis is not able to analyze how use of Medicaid wraparound services by dual-eligible individuals differs for people with traditional Medicare or Medicare Advantage.)
What does variation in Medicaid coverage across states suggest for ongoing policy proposals to create new Medicare dental, vision, or HCBS benefits? In recent years, policymakers have proposed adding new benefits to the Medicare benefit package including:
- HCBS in the Choose Home Care Act of 2021 (R. 5514 and S.2562), and Expanding Care in the Home Act (H.R. 2853)
- Dental and vision care in the Medicare and Medicaid, Dental, Vision and Hearing Benefit Act of 2023 (S.842 and H.R.33) and the Medicare Dental Benefit Act of 2023 (H.R. 4146).
New Medicare benefits could increase access to these services for Medicare beneficiaries overall, but the effects on dual-eligible individuals would depend on the generosity of coverage in their state’s Medicaid program and whether states reduced their coverage of wraparound services in response to Medicare benefit changes.
This work was supported in part by Arnold Ventures. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Methods
Data: Monthly enrollment and eligibility information come from the 2019 T-MSIS Research Identifiable Demographic-Eligibility Files and service use come from the 2019 T-MSIS other services (OT) and long-term (LT) claims files. Data from the 50 states and DC are included in this analysis. The District of Columbia is considered a state for the purposes of this report, but the U.S. territories are excluded on account of differences in the way Medicaid operates in the territories.
Definition of Full-Benefit Dual-Eligible Individuals: Full-benefit dual-eligible individuals include anyone with one or more months of Medicare coverage defined as DUAL_ELGBL_CD_LTST values of 01, 02, 03, 04, 05, 06, 08; and 10 or more months of full Medicaid defined as RSTRCTD_BNFTS_CD_LTST values of 1,A,D,4,5,7.
Definition of Medicaid Enrollees Without Medicaid coverage: Full benefit Medicaid enrollees include anyone with 10 or more months of full Medicaid defined as RSTRCTD_BNFTS_CD values of 1,A,D,4,5,7; and eligibility for Medicaid based on age 65 or over, blindness, or disability , which includes ELGBLTY_GRP_CD_LTST values of 11, 12, 13, 15-26, 37-60 or if age is greater than 64.
Medicaid enrollees are categorized as follows:
- Under age 65 or ages 65 and older using the Age variable in years;
- Male or female using the SEX_CD variable; and
- Into race and ethnicity groups using the RACE_ETHNCTY_CD from the 29 states that reported “low/medium concern” data quality levels with their race and ethnicity data in 2019. For more information, see DQ Atlas. Data for those 29 states represent 66% of all full-benefit dual-eligible individuals in the US. The 29 states include: AK, CA, DE, FL, GA, ID, IL, IN, KY, ME, MI, MN, MS, NC, ND, NE, NH, NJ, NM, NV, OH, OK, PA, SD, TX, VA, VT, WA, WI. Persons of Hispanic origin may be of any race but are categorized as Hispanic for this analysis; other groups are non-Hispanic. Data are not shown for people reporting “Unknown” or "Multiracial" racial/ethnic groups which amounted to 489k and 6k dual-eligible individuals, respectively.
Use of LTSS: Medicaid enrollees who use LTSS are identified using the methods described in the issue brief “How Many People Use Medicaid Long-Term Services and Supports and How Much Does Medicaid Spend on Those People?” Methods box.
Use of other wraparound services: Medicaid enrollees who use each service include anyone with one or more fee-for-service claim or managed care encounter for each service type. The specific codes used include the following.
- NEMT services were identified as records with HCPC codes A0080, A0090, A0100, A0110, A0120, A0130, A0140, A0160, A0170, A0180, A0190, A0200, A0210, S0209, S0215, T2001, T2002, T2003, T2004, T2005, T2007, Z2713, W7274, W7275, W7276, M0372, M0419, M0373, M0374, M0418, M0420 as described in MACPAC Mandated Report on Non-emergency Medical Transportation.
- Vision services include eye exams with CPT/HCPC codes 92002, 92004, 92012, 92014 provided by any provider type and evaluation and management codes 99201, 99202, 99203, 99204, 99205, 99212, 99213, 99214, 99215, 99241, 99242, 99243, 99244, 99245, 99341, 99342, 99343, 99344, 99345, 99347, 99348, 99349, 99350 if the procedure provided by an ophthalmologist, optometrist and optician using provider type codes 41, 18, 96 or related provider taxonomy codes; eye glasses with procedure codes V2020, V2025, V2100, V2101, V2102, V2103, V2104, V2105, V2106, V2107, V2108, V2109, V2110, V2111, V2112, V2113, V2114, V2115, V2118, V2121, V2199, V2200, V2201, V2202, V2203, V2204, V2205, V2206, V2207, V2208, V2209, V2210, V2211, V2212, V2213, V2214, V2215, V2218, V2219, V2220, V2221, V2299, V2300, V2301, V2302, V2303, V2304, V2305, V2306, V2307, V2410, V2430, V2499; contact lenses with CPT/procedure codes 92310, 92325, 92326, 92071, 92072, V2510, V2511, V2512, V2513, V2520, V2521, V2522, V2523, V2531, V2599; and low vision aids with procedure codes V2600, V2610, V2615, Z460.
- This methodology uses the CDC’s Vision and Eye Health Surveillance System classifications for Eye exams and/or glasses/contacts. Any treatment, imaging, diagnostic, or screening services were excluded to avoid overlap with Medicare covered services.
- Dental services include any claims with a dental-related procedure code (D0100-D9999) including diagnostic, preventive, restorative, endodontics, periodontics, implant services and prosthodontics, oral and maxillofacial surgery, orthodontics and adjustive general service as described by the American Dental Association.
The analysis presents data from 2019 data, which are expected to be more representative of non-pandemic utilization trends than data from 2020, the most recent year of data available when the analysis was conducted. Use of many health care and wraparound services declined during the pandemic as outpatient and elective services were cancelled, delayed, or avoided among all people. Deferrals and avoidance of care also affected the use of Medicaid wraparound services (Appendix Figure 3).
The most significant limitations of this analysis stem from the fact that the data do not account for the use of Medicare services or type of enrollment in Medicare. Specifically, the analysis does not distinguish between dual-eligible individuals based on whether they were enrolled in different types of Medicare Advantage (MA) plans, which usually cover supplemental benefits. The analysis is also unable to identify whether dual-eligible individuals are using Medicare-covered services, which in some cases may overlap with Medicaid supplemental benefits.
This analysis does not examine if rates of use for wraparound services are associated with different rates of need (medical condition or functional status) or different rates of access to services. This analysis includes the share of dual-eligible individuals who use a particular wraparound service among all dual-eligible individuals, but among those who do not use the services, it is unknown whether the lack of use reflects lack of need or lack of access.
Appendix


