Early Impacts of the Medicaid Expansion for the Homeless Population
Executive Summary
The Affordable Care Act (ACA) Medicaid expansion offers a significant opportunity to increase coverage and improve access to care for individuals experiencing homelessness, who historically have had high uninsured rates and often have multiple, complex physical and mental health needs. This analysis provides an early look at the impact of the expansion for homeless providers and the patients they serve, building on an earlier brief examining the potential role of Medicaid expansion for this population. It is based on focus groups conducted with administrators, providers, and enrollment workers at four sites serving homeless individuals in states that have expanded Medicaid (Albuquerque, NM; Baltimore, MD; Chicago, IL; and Portland, OR) and one site in a state that has not expanded (Jacksonville, FL), as well as administrative data collected from the sites. It finds:
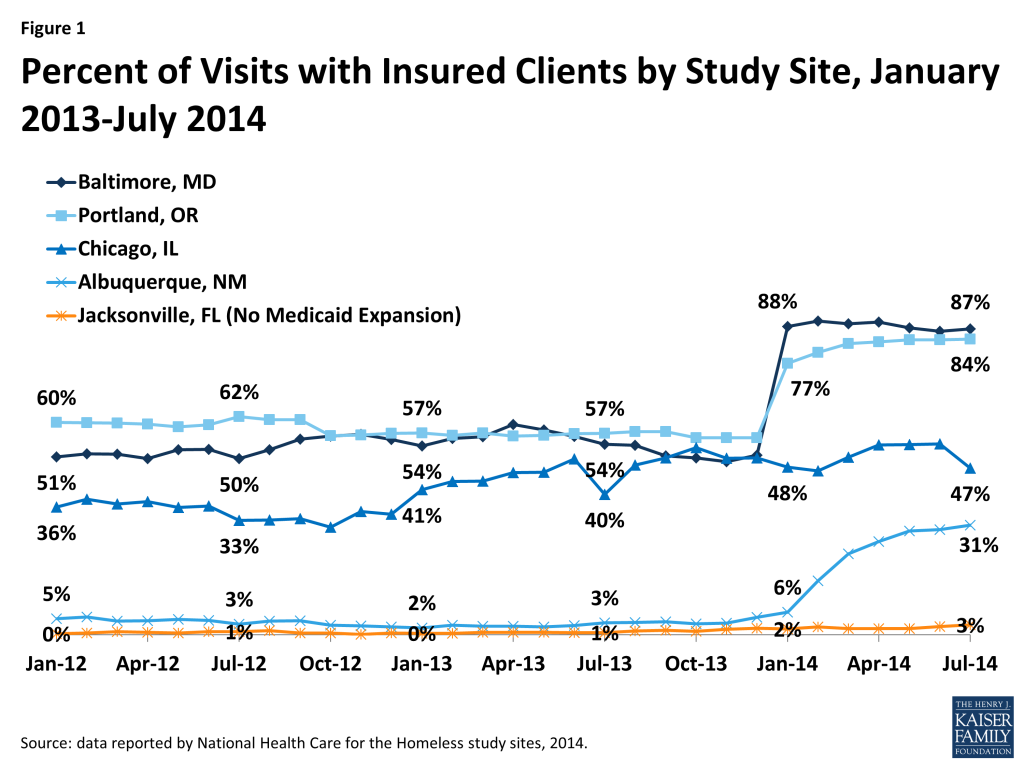
The Medicaid expansion has led to significant increases in coverage that are contributing to improved access to care and broader benefits for homeless individuals. Participants and data from the study sites indicate that the Medicaid expansion has led to significant gains in coverage among the individuals they serve (Figure 1). Providers reported that these coverage gains have enabled patients to access many services that they could not obtain while uninsured, including some life-saving or life-changing surgeries or treatments. Participants also identified other broader benefits for homeless individuals stemming from Medicaid coverage gains. For example, providers noted improvements in individuals’ ability to work and maintain stable housing due to better management of health conditions. In addition, participants said individuals have reduced financial stress and improved access to other services and programs, including disability benefits.
“A couple of my patients have had surgeries that have allowed them to return to work and now that they have a regular paycheck, they are able to get housed,” Provider, Baltimore
Providers reported having access to a broader array of treatment options as a result of Medicaid coverage gains among their patients. With these increased options, providers said they are better able to provide care based on the best courses of treatment rather than based on the availability of charity or discounted resources.
“It’s easier now if I say, take your insurance and go to the pharmacy…instead of me or the nurse having to fill out a bunch of paperwork and apply to the drug company or see what we have in samples and if we’re going to have enough for next time.” Provider, Portland
Gains in Medicaid revenue are facilitating strategic and operational improvements focused on quality, care coordination, and information technology. In addition, administrators indicated that Medicaid revenue gains supported staff increases and led to changing staff roles to meet increased administrative and billing needs. However, participants emphasized that, even with Medicaid revenue gains, other funding sources remain vital for supporting the full range of services needed by the homeless population.
Participants from the non-expansion site indicated that their patients remain uninsured and are continuing to face significant gaps in care that contribute to poor health outcomes. Participants also said they are facing an increasingly challenging financial situation because they are missing out on Medicaid expansion revenue gains and other funding sources are declining.
“A lot of it is just outright begging for care for these patients. You just miss that opportunity to pick it up in a more treatable stage.” Provider, Jacksonville (non-expansion site)
As homeless patients gain Medicaid coverage and are enrolled in managed care, some challenges are emerging. Participants commented that some patients are being auto-assigned to providers with whom they do not have an existing relationship and/or they may have difficulty accessing due to lack of transportation. Additionally, working within provider networks can be difficult given the complex needs of individuals, lack of transportation, and the limited experience among other providers in serving this population. Lastly, participants emphasized that prior authorization requirements and limited and/or changing drug formularies are leading to delays in care for individuals and creating substantial administrative burdens for providers.
Looking ahead, participants identified a number of priorities for meeting the health care needs of the homeless population. It was noted that maintaining coverage and educating individuals on how to use coverage will be key for shifting care patterns and reducing emergency room use. Further, maintaining other sources of funding will be key for supporting the full range of services they need. As homeless individuals are increasingly enrolled into managed care, it will be important to address their specific needs to minimize barriers to care and administrative burdens. Amid the shifting financial and delivery environment, maintaining supportive and case management services, addressing social determinants of health, and building upon interdisciplinary team-based models of care developed by homeless providers all will be key for engaging individuals in care. Finally, as broader payment and delivery reforms are implemented, it will be important for them to reflect the poorer health status and more complex health needs of the homeless population.
Introduction
One of the key goals of the ACA is to expand coverage and reduce the number of uninsured. A primary way the ACA seeks to reduce the number of uninsured is by expanding Medicaid to low-income adults (with incomes at or below 138% of the federal poverty level or $16,105 for an individual or $27,310 for a family of three as of 2014) who were historically ineligible for the program. As enacted, this expansion would occur in all states as of January 1, 2014. However, the Supreme Court ruling on the ACA effectively made the expansion a state option. As of November 2014, 28 states, including DC, are implementing the expansion.
The Medicaid expansion offers a particularly significant opportunity to increase coverage and improve access to care for individuals experiencing homelessness, who historically have had very high uninsured rates and often have multiple, complex physical and mental health needs. A prior brief examined how homeless health care providers were preparing for the Medicaid expansion and their anticipated impacts of the expansion.1 This brief builds on that previous work to identify early impacts of the expansion for homeless providers and the patients they serve as well as key priorities for meeting the health care needs of the homeless population looking ahead. While the findings are focused on the homeless community, they offer insights that may help inform understanding of how coverage gains are impacting the broader low-income population.
Overview of the Homeless Population
Each year, millions of people experience homelessness in the U.S. Though the total number is unknown, the U.S. Department of Housing and Urban Development (HUD) found that 1.48 million people stayed in emergency shelters or transitional housing in 2012.2 However, this estimate excluded individuals who avoided the shelter system, used privately funded shelters not part of HUD’s Continuum of Care network, or who stayed with friends and families to avoid the streets. On a single night in January 2013, HUD estimated 610,042 people were homeless in the U.S., of which 64% were individuals and 36% were part of families.3 This estimate also undercounts the number of people who are homeless, but represents the best attempt to collect national data across all states.
People who are homeless have high rates of both chronic disease and acute illnesses, with many of these conditions associated with and/or exacerbated by their living situations. There is a wide body of literature on the health status and conditions of homeless persons, which shows that they have a broad range of mental health and substance use needs that often are co-occurring with physical conditions.4 ,5 Higher exposure to violence, malnutrition, and extreme weather are additional risk factors for poor health and premature death.6 , 7 Often because of poor health and lack of housing, this population also frequents emergency rooms and hospitals more often than the general public, and has high rates of readmissions.8
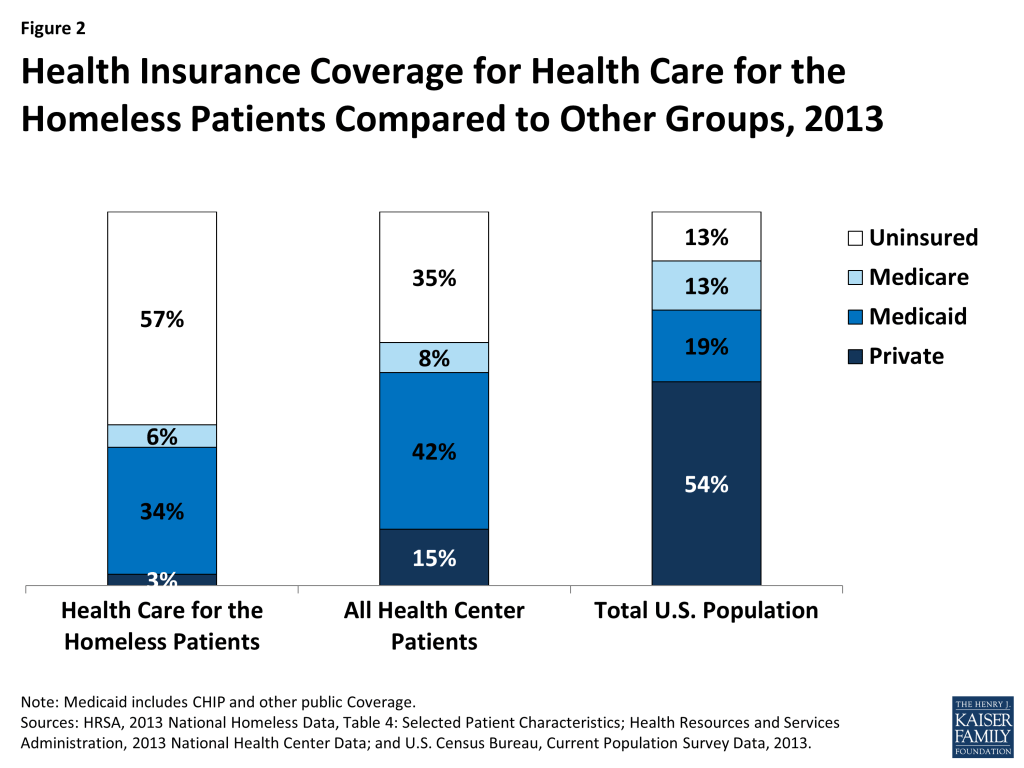
Prior to Medicaid expansion, homeless individuals were uninsured at high rates even when compared to other low-income groups. Of the 851,641 patients served by Health Care for the Homeless grantees in 2013,9 57% were uninsured, compared to 35% uninsured patients served at all health centers and over four times the rate of the general population (Figure 2).10 ,11 Despite having access to outpatient primary care and behavioral health services at health centers and other safety net venues, lack of health insurance has prevented this population from accessing the broader range of services needed to address their health conditions, such as specialty care, residential treatment, and surgeries. Being uninsured has also prevented a more systemic analysis of their utilization and cost of care given the lack of coordinated data available through insurers. Finally, connecting this particularly vulnerable group to health insurance is important for the providers who serve them, as they have traditionally relied on unpredictable grant funding and limited pro bono services in the community.
Methodology
To gain insight into the early impacts of the Medicaid expansion for the homeless community, the National Health Care for the Homeless Council and the Kaiser Commission on Medicaid and the Uninsured conducted focus group discussions with staff and community partners at federally qualified health centers that serve individuals experiencing homelessness at four sites in states that have expanded Medicaid (Albuquerque, NM; Baltimore, MD; Chicago, IL; and Portland, OR). Focus groups were also conducted at a site in Jacksonville, FL to gain insight into experiences in a state that has not expanded. In addition, health coverage and administrative data were collected from each of the sites to supplement the focus group findings. See Appendix Table 1 for and overview of the data.
Overall, a total of 118 professionals participated in 14 focus groups held between July and September 2014. Three focus groups were held in each of the four expansion sites—one composed of frontline outreach and enrollment workers, another composed of administrators and finance staff, and the third consisting of clinicians, case managers and other service providers. In Jacksonville, Florida, two focus groups were held—one with administrators, finance staff and clinicians, and another with frontline outreach and enrollment staff.
Key Findings
Enrollment
Changes in Coverage
Participants in the Medicaid expansion sites reported significant gains in health insurance among patients, while there were no reported coverage changes in the non-expansion site. Participants noted that the Medicaid expansion provided a new coverage pathway for many of their previously uninsured patients. In three of the sites, they indicated that state initiatives to facilitate enrollment supported rapid coverage gains under the expansion. Specifically, in Chicago, the state adopted an option to get an early start on the expansion in Cook County. In Baltimore, individuals enrolled in a pre-existing limited benefit program for adults (Primary Adult Coverage program) were automatically transitioned to the Medicaid expansion when it took effect on January 1st. Finally, in Portland, the state took up an option to utilize data from its Supplemental Nutritional Assistance Program (SNAP) to expedite enrollment into the Medicaid expansion. In contrast to coverage gains at sites in states that expanded Medicaid, participants in Jacksonville said that they have seen no significant changes in coverage. The majority of their patients remain uninsured and ineligible for Medicaid in the absence of the expansion.
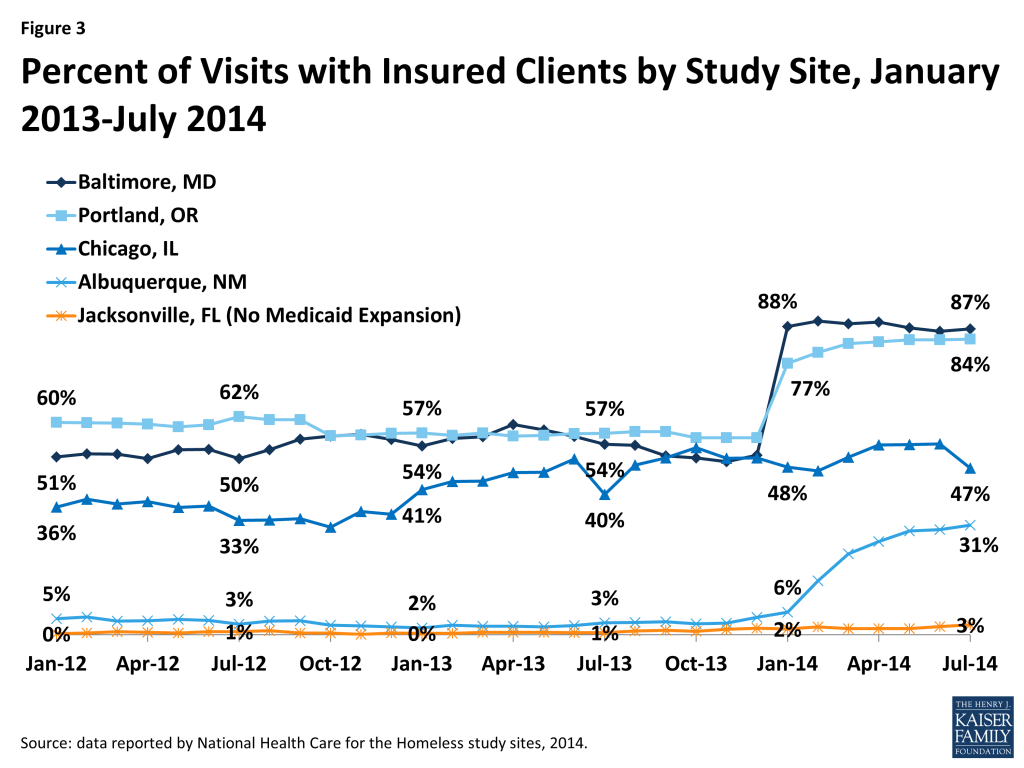
Coverage data from the sites are consistent with participants’ reported coverage changes. As shown in Figure 3, in Baltimore and Portland, the share of site visits with clients who have health insurance rose sharply as of January 2014, reflecting rapid coverage gains from the transition of the existing adult coverage program to the expansion in Maryland and the SNAP facilitated enrollment initiative in Oregon. Albuquerque also shows gains in the share of patients with insurance beginning in January 2014, although the increase is not as sharp. In Chicago, the rise in the share of visits with patients who have insurance begins earlier, at the end of 2012, reflecting the early expansion in Cook County, and then there are periods of decline that reflect some losses in coverage at renewal periods. In contrast, in Jacksonville, where Medicaid was not expanded, there is no notable increase in the share of visits with insured patients over the period.
Looking ahead, outreach workers are focused on maintaining coverage. Although policies are intended to facilitate auto-renewal for eligible individuals, outreach workers expressed significant concerns that individuals may lose coverage at renewal, particularly if systems are unable to automatically verify income for individuals. In two of the sites, all individuals will have to re-enroll at redetermination because the state is transitioning to a new enrollment system. Overall, outreach workers were confused about renewal processes and wanted more information to be able to support continuous coverage for individuals.
Outreach and Enrollment Experiences
Outreach through a broad range of settings was successful in reaching and enrolling individuals experiencing homelessness, who were generally eager to enroll and access services. Frontline outreach and enrollment workers noted that, in addition to conducting in-reach to enroll patients at their clinic sites, they conducted outreach in a wide range of community locations, including emergency shelters, encampments, under bridges, at parole and probation offices, day programs/drop-in centers, hospital emergency rooms, churches, and food pantries or soup kitchens. Participants agreed that having regular outreach schedules and developing trusting relationships with clients was a crucial step in engaging clients, particularly since they had broader goals beyond enrollment of engaging individuals in services. Participants found that individuals were usually interested in enrolling in coverage, although they sometimes had doubts about whether they would qualify or concerns about sharing their information with the government. In particular, individuals were most excited about potentially gaining access to prescription drugs, mental health and substance use services, and dental and vision care. Participants also said that individuals wanted the peace of mind of financial protection from large medical bills. To facilitate enrollment, assisters spent a considerable amount of time explaining to individuals why health insurance was important, the benefits of enrolling in coverage, and how the ACA had broadened eligibility for Medicaid compared to when individuals may have previously tried to enroll.
“….We go anywhere that we feel like they need help in our community.” Outreach Worker, Baltimore
“A lot of people haven’t been covered for years; they are just happy that they could get some medical treatment.” Outreach Worker, Portland
“…they’d say ‘oh, so I won’t get all these bills?’ No, you won’t. And so that was a big motivator….” Outreach Worker, Albuquerque
Outreach workers in the Medicaid expansion sites found that nearly all homeless individuals they assisted were eligible for Medicaid, while those in the non-expansion site found that most of the homeless population remained ineligible for coverage. In the expansion sites, outreach workers reported that nearly all individuals they assisted within the homeless population were eligible for Medicaid, although they did work with some individuals who were not eligible due to immigration status. They also encountered a few cases in which a homeless individual had a job and was just above the income limit for Medicaid. In these cases, coverage through the Marketplace was unaffordable, even with the premium subsidies. In Jacksonville, where the state did not expand Medicaid, outreach workers reported that most individuals were not eligible for Medicaid and did not have enough income to qualify for premium tax credits for Marketplace coverage. Enrollment workers in Jacksonville said that many individuals were confused about why they were not eligible for coverage because marketing campaigns were encouraging everyone to enroll, and some were fearful of being fined for not having insurance. They noted that clients were disappointed, angry, and frustrated when learning they were not eligible for coverage. Assisters tried to help connect individuals to available care by creating resource sheets that listed free or low-cost service sites, but, overall, felt it was difficult to conduct outreach and enrollment efforts when many people do not qualify for coverage.
Individuals within the homeless population needed substantial assistance with the application and enrollment process. Outreach and enrollment workers stressed that one-on-one assistance with the application process was key for enrolling individuals, particularly given their limited experience with health insurance and other enrollment barriers, including limited literacy, lack of access to the internet, language barriers, and confusion about coverage options. They further noted that enrollment was hampered by problems with online enrollment systems, particularly at the outset of open enrollment. Although systems problems impacted the broader population, there were some challenges that particularly impacted the homeless population including difficulty verifying identity for individuals without a credit history and verifying income for people with no income as well as systems failing to recognize when an individual is no longer incarcerated. Outreach and enrollment workers were hopeful that these system-related issues were short-term and that there would be a smoother enrollment process going forward. Participants said they often tracked the status of applications until a final eligibility determination was received since individuals may have difficulty obtaining communications from the state without a fixed address and/or trouble understanding notices. Moreover, in the expansion study sites, after an individual is determined eligible for Medicaid, he or she must then enroll in a managed care plan. Outreach and enrollment workers noted that individuals needed assistance selecting and enrolling in a plan. However, they said it was challenging to determine the differences between plans and explain them to individuals.
“If you didn’t have significant credit history or things like that, it couldn’t verify people’s identity, which just added an extra barrier to getting folks enrolled.” Outreach worker, Baltimore
“We keep a spreadsheet of everybody that we enroll and we keep going back to look if they’ve been approved.” Outreach worker, Albuquerque.
“The paperwork was confusing that they would get in the mail.” Outreach worker, Albuquerque
Homeless individuals need significant education and assistance to learn how to utilize their health coverage. Participants stressed that many of the homeless individuals who have gained Medicaid coverage have limited or no prior experience with health insurance and have typically delayed and/or gone without needed care and relied on the emergency room as a primary source of care. As such, they indicated that individuals need education and assistance to establish a relationship with a primary care provider and understand how to receive care and services within their provider network.
“There needs to be an educational piece, because a lot of people haven’t had primary care maybe ever and don’t even really know what it means to have a routine visit with a provider to get those preventative services.” Provider, Baltimore
Impacts of Coverage Gains for the Homeless Population
Participants reported that gains in Medicaid coverage have led to improved access to care for the patients they serve. Providers noted that gains in Medicaid coverage have enabled their patients to access many services that they could not previously obtain while uninsured, particularly specialty services, behavioral health services, medications, and medical supplies and equipment. They said they are able to get individuals referred for specialty services and screenings such as mammograms and colorectal screenings more quickly and able to make referrals to orthopedists, oncologists, physical therapists, podiatrists, and other specialists that they often were unable to refer to when their patients were uninsured. Some described instances of individuals receiving life-saving or life-changing surgeries or treatments that they could not obtain while uninsured. In particular, providers indicated that coverage has opened up access to mental health services and medications, which are important for this this population. It also was pointed out that coverage of non-emergency transportation helps individuals access needed services, especially from referral providers who may be located in another part of town. Some participants did note challenges finding certain specialists, although they indicated this was reflective of larger provider capacity limits, particularly for mental health and primary care providers. Participants also said that they are beginning to face backlogs in referrals for some services given the large surge in demand for care as people gain coverage. Further, some participants commented that even though Medicaid copayments are often very limited, they can serve as a barrier to care for this population, particularly if an individual is facing copays for multiple prescription medications.
“We had a gentleman who literally was waiting until January 1st and he had an appointment on the second to get oncology testing that he wasn’t able to access in the past.” Provider, Baltimore
“A lot more people are going to get the services that they’ve been needing.” Provider, Portland
“Now, we can just send them over to [the hospital] which is two, three blocks away. They can get in that day.” Provider, Chicago
“Any medicated-assisted therapy for substance use, it’s covered now and without that, my clients would have never been able to be successful in recovery.” Outreach worker, Albuquerque
Participants also identified broader benefits for individuals stemming from gains in Medicaid coverage. For example, providers said individuals have obtained surgeries and treatments that will resolve medical conditions and improve their ability to work and maintain stable housing. Additionally, participants commented that individuals have less stress about incurring unpaid medical bills or debt. Moreover, they indicated that reductions in medical debt improve individuals’ ability to access housing and employment program opportunities, since their credit is not negatively impacted by medical debt. Participants also said that obtaining Medicaid coverage helps individuals qualify for disability benefits by facilitating better documentation of their needs. Similarly, in one site, participants noted that Medicaid coverage gains have enabled individuals to get tested for Traumatic Brain Injuries (TBI), which supports their ability to apply for a TBI Waiver program that provides access to housing.
“A couple of my patients have had surgeries that have allowed them to return to work and now that they have a regular paycheck they are able to get housed.” Provider, Baltimore
“That’s something we’re going to start seeing less of—these large hospital bills that are going to negatively impact credit.” Provider, Baltimore
“I feel like they have a much stronger application that we’re turning into Social Security. More medical evidence, for sure.” Outreach worker, Albuquerque
Participants said that individuals are more empowered to manage their health and participate in decisions related to their health care as a result of gaining coverage. Providers and enrollment workers described how gaining health coverage and having a choice of plans and providers opened up new personal interest in health care among individuals. Participants recognized that some of this initial excitement may diminish over time, but nonetheless felt that this response provides an important new opportunity for engagement with a population that often has limited choice and control over the options available to them.
“The other thing that is a little bit more intangible is the excitement that patients feel in the choices that they have. They’re feeling quite empowered, they’re extraordinarily excited when they hear the types of things that they now have access to.” Provider, Albuquerque
Participants in the non-expansion site described a contrasting experience with individuals continuing to face significant barriers to care and poor health outcomes. Participants in Jacksonville noted that, without insurance, individuals continue to rely on limited pro bono services, have difficulty accessing needed treatments and specialty services, and utilize the emergency room for dental emergencies and acute mental health stabilization. As such, overall, they experience ongoing poor health, worsening of conditions, and, in some cases, preventable deaths.
“A lot of it is just outright begging for care for these patients. You just miss that opportunity to pick it up in a more treatable stage.” Provider, Jacksonville (non-expansion site)
“It really is people getting care in all the wrong places at all the wrong times in the most expensive way that they can, and that cost just gets shifted around.” Provider, Jacksonville (non-expansion site)
Impacts of Coverage Gains for Providers
Providers indicated that they have wider treatment options available to care for their patients as a result of coverage gains. In particular, providers noted that they have much wider choices of medications, since they are no longer limited to medications available through discounted or free pharmaceutical programs. They provided specific examples, such as being able to prescribe steroid inhalers for asthma or to give monthly injectable mental health medications (rather than daily pills, which have lower compliance rates). With these broader treatment options, providers said they can provide care based on the best course of treatment rather than based on what services or medications they can access through free or discounted programs. They also noted that they have greater ability to provide a stable and consistent treatment plan over time. In contrast, providers in Jacksonville, where Medicaid was not expanded, reported continuing to rely on charity, discounted, and pro-bono services and noted that their treatment choices remained constrained by available resources.
“It’s easier now, if I say, take your insurance and go to the pharmacy and they’ll give you a bottle of pills, instead of me or the nurse having to fill out a bunch of paperwork and apply to the drug company or see what we have in samples and see if we’re going to have enough for the next time.” Provider, Portland
“So it helps not only them, but it helps the primary provider not to feel like we’re practicing frontier medicine, in that we’re actually being helped by the people trained to provide the specialty care that the patients need. It’s been good for us and for them.” Provider, Baltimore
The study sites in Medicaid expansion states are experiencing increases in third-party payments as their patients are enrolled in Medicaid. Because the homeless patient population has largely been uninsured, providers serving the population have traditionally relied on a diverse range of public and private grants and donations as the bulk of their revenue. Third-party payments from insurers previously represented a very small percentage of their revenue. Administrators reported that gains in Medicaid coverage are now leading to an increased share of revenue coming from third-party payments, but indicated that other sources of funding, including public and private grants and donations, are declining at the same time. Administrators in Jacksonville, where Medicaid was not expanded, said they are missing out on potential Medicaid revenue gains without the expansion. However, they have experienced some increase in Medicaid revenues by amplifying efforts bill for reimbursable services. Overall, however, administrators in Jacksonville said they are facing an increasingly challenging financial situation due to declining grant dollars and donations and missed funding opportunities because their state has not expanded Medicaid.
Administrators indicated that gains in Medicaid revenue are facilitating longer-term strategic and operational improvements. Administrators noted that their historic reliance on fluctuating and unpredictable grant funding made it difficult to invest in structural improvements and plan for growth over the long-term. They commented that the shifts to Medicaid revenue are allowing them to implement longer-term performance improvements because they can plan based on patient volume and need rather than around varying short-term grant requirements. As a result of more stable revenue, they reported engaging in new initiatives focused on improving quality of care, care coordination, and information technology infrastructure. They also cited opportunities to allow clinicians to dedicate some portion of their time to administrative functions, such as care team management and leadership.
“What it’s allowed us to do is to think about growth, organizational growth as driven by volume and not driven by our ability to get another grant.” Administrator, Baltimore
Administrators reported increasing staffing levels and/or shifting staff responsibilities in response to Medicaid coverage gains. Administrators indicated that gains in Medicaid revenue have created new opportunities to add staff to meet existing needs and expand services. However, they also noted that staffing needs have changed as a result of increased need for billing managers, data specialists, and care coordination staff. As such, they reported hiring both clinical and administrative staff and/or shifting responsibilities of existing staff. In addition, participants at some of the sites indicated that there is a high level of burn-out among existing staff and significant competition for providers in the community, which has increased the importance of strong recruitment and retention policies.
“We believe that, by the end of the year, if we’re hiring all the positions that we have budgeted for, we’ll have 170 staff members up from about 140 last year.” Administrator, Baltimore
“We’ve certainly had to add more providers and behavioral health clinicians to meet increased demand.” Administrator, Portland
“We’ve added…some referrals staff and care coordination staff and also some staff specifically dedicated to managed care.” Administrator, Chicago
Participants emphasized that, even with Medicaid coverage gains, other funding sources remain vital for supporting the full range of services needed by the homeless population. Administrators stressed that Medicaid does not cover the full range of supportive services provided to patients. In particular, they noted that outreach, case management, nursing visits, some behavioral services, and housing and other support services are often not billable services. While they recognized that these services are included in the bundled Medicaid reimbursement health centers receive, participants indicated that the homeless population requires a more intensive level of care than covered by that rate, and pointed out that these services are typically not billable when provided outside a medical visit or by a non-billable provider. They also commented that the state’s Medicaid reimbursement rates rarely cover the full cost of care, particularly for behavioral health and dental care. As such, participants stressed that other sources of funding, including federal, state, and local grants as well as private philanthropy, remain vital to maintaining operations and services even with gains in Medicaid coverage. Participants were concerned that decreases in these other funding sources may make it difficult to maintain supportive services going forward and limit resources available for individuals who remain uninsured, including undocumented immigrants.
“The navigation piece and the additional hand-holding and helping them to figure out where they’re supposed to go and that they actually get there is a big piece of work that is unreimbursed.” Administrator, Baltimore
“There’s a sense that oh, you have a windfall of Medicaid now, we don’t need to give you these other funding streams that we gave you that supported your operation.” Administrator, Albuquerque
“The additional needs aren’t reimbursable.” Provider, Chicago
ACCESS TO AND DELIVERY OF CARE
Supporting Access to Care for the Homeless Population
Participants emphasized that case management and supportive services as well as an open, trusting, and integrated care environment are key for engaging homeless individuals in care. All participants referenced the need for dedicated staff to help patients navigate the system, fill out paperwork, make phone calls, work with managed care plans, obtain necessary paperwork and documentation, conduct needs assessments, assist with transportation to appointments, help refill medications, connect individuals to other programs and benefits, and many other activities. Participants also noted that providing an open-access and non-judgmental environment is important. For example, health centers serving this population typically have no copays or out-of-pocket costs, do not issue penalties for late or missed appointments, and emphasize a trusting relationship with patients. Moreover, they described how homeless providers utilize a team-based approach to provide integrated care to address individuals’ physical, behavioral, and social needs.
“It’s very much just open access.” Provider, Baltimore
“It’s not only about making sure that we have the appointment, the important part is making sure they get to the appointment.” Provider, Portland
“We have lots and lots of warm handoffs within the agency and so a person could walk in our door and the same day would have a behavioral health provider and a medical provider, who are crossing over one to the other….” Provider, Albuquerque
Participants pointed to the importance of addressing social determinants of health like poverty, hunger, lack of housing, and unemployment to support improved access to care and health outcomes and reduce health costs. Participants stressed that lack of housing is a key impediment to care and improved health for individuals and commented that permanent supportive housing is an effective model for supporting individuals with significant health conditions. Participants noted that Medicaid cannot pay for housing, but that support for housing would reduce costs by preventing repeat hospitalizations and emergency room visits. Participants also pointed out that lack of housing has implications for hospitals who incur longer lengths of stay and higher readmissions when patients have no safe discharge options. In these cases, medical respite programs can provide patients a place to rest and recuperate after surgeries or illnesses, while allowing some time to connect to other resources.12 In addition, hunger and lack of appropriate food were mentioned as challenges for this population, who generally have no place to store food and eat at soup kitchens, which tend to serve high-salt, high-starch diets that exacerbate medical conditions such as hypertension and diabetes.
“If they have some housing or something under their feet, then a lot of the other things can fall into place. It’s really hard to heal somebody’s wound if they’re lying on the street and if they don’t have a place where their medication can be safe.” Provider, Portland
“We can write prescriptions, we can send referrals, get people into specialty services, but if we were actually able to house people that’s the best way to improve their health.” Administrator, Baltimore
Although patients have increased choice of providers after gaining Medicaid coverage, most individuals are continuing to rely on providers who serve the homeless population. Participants described some instances of patients seeking care from alternative providers, but then returning to the homeless provider because they felt like they were not treated with respect and did not have a good patient experience at the other provider. Even so, administrators noted that, with the gains in Medicaid coverage, it is increasingly important for safety-net providers to establish themselves as a provider of choice, rather than a provider of last resort. As such, they are focusing on patient satisfaction, care coordination, and quality to provide a first choice medical home for their patients.
“They were treated like they shouldn’t have been there… they said that it actually started from the front desk all the way to the end of the appointment.” Administrator, Albuquerque
“We’ve had kind of a public image of being a place you go when you can’t go anywhere else. Now, we strive to provide great care and we would like to believe our care is as good as anybody else’s.” Administrator, Portland
Challenges Providing Care to the Homeless Population through Managed Care
In the expansion study sites, individuals gaining Medicaid coverage are enrolled into Medicaid managed care plans. Participants commented that this is leading to some new barriers to care for individuals and administrative burdens for providers as discussed below.
Participants noted that some individuals are being automatically enrolled into plans and assigned to a provider but are having difficulty accessing care through the assigned provider. Participants commented that individuals may have difficulty accessing care through their assigned provider if they do not have an established relationship with the provider, lack transportation, or if the provider’s practice does not accommodate the needs of homeless individuals. Participants have found that it is sometimes challenging for patients to switch providers and that, in some cases, by the time an individual realizes he or she has been auto-assigned to a plan and provider, they are outside the window of time in which they are allowed to make a plan change. As a result, participants reported instances of patients being auto-assigned to a provider, being unable to change their provider back to the health center, and then continuing to utilize the health center as their primary provider. In these cases, the patient may be insured, but the provider remains unable to bill for the services they provide.
“When they were enrolled, a lot of them got assigned to places without their choosing and then to straighten that out was difficult.” Administrator, Portland
“…if they don’t have us listed as their primary care physician and we don’t have a referral on file then we will not be reimbursed for those services.” Administrator, Chicago
Obtaining care through provider networks is posing some specific challenges for homeless individuals. Participants indicated it is sometimes difficult to find a network that includes all providers caring for a patient, particularly given the complex needs of the individuals they serve. Participants also noted that as a result of working within provider networks, there have been shifts in which specialists and hospitals they use to refer patients. In some cases, these shifts are leading to access barriers due to transportation limitations. Further, some patients have found the change difficult because they would prefer to rely on hospitals and providers that they already have experience using. Participants also commented that when individuals receive care from providers who do not have experience serving the homeless population, they sometimes prescribe treatment plans or medications that are not feasible for individuals who are homeless.
“Having only certain providers taking insurance is not specific to Medicaid, but it’s a big barrier to our patients because of transportation.” Provider, Baltimore
“…they’ll get sent back to us with stuff they obviously can’t do… The other providers are not really having an understanding of the special needs of the population.” Provider, Baltimore
Participants stressed that prior authorization requirements and drug formularies are leading to delays in care for individuals and creating substantial new administrative burdens. Specifically, providers said prior authorization requirements delay patients’ access to services, particularly substance abuse treatment, leading to missed opportunities to connect people to care. Providers noted that prior authorization requirements and drug formularies are different for each managed care plan, and that it is difficult to stay informed about these differences because they change frequently. Providers described cases of writing prescriptions for drugs they thought would be covered and then the patient finding out it is not covered when seeking to fill it. Overall, participants reported substantial time and effort is going toward addressing these requirements, which is taking away from clinical time for providers. Administrators noted that they are hiring staff or shifting existing staff roles to focus solely on these administrative requirements.
“The administrative burden of prior authorizations and the different requirements that all the MCOs have…I don’t think we quantified it, but I think we’ve seen that administrative burden go up and it’s a challenge for the providers for sure.” Administrator, Baltimore
“If you say, okay, well, this referral we have to do, we have to develop this form, we have to call this number, we have to wait three days, whatever it might be—next thing you know, they’re just saying forget it, and then they’re not getting that need met.” Provider, Chicago
Becoming credentialed providers with the managed care plans has been challenging. The study sites in states that expanded Medicaid were seeking to get credentialed with all or most of the Medicaid managed care plans in their area. Participants said the credentialing process has been very challenging and taken a substantial amount of time and administrative resources, particularly since each managed care plan has a separate process and different requirements.
“We’re also run into some problems credentialing… and it’s been somewhere between difficult and a nightmare.” Administrator, Chicago
Participants said that managed care plans are still developing resources, capacity, and experience to coordinate and manage care for the homeless population. Because the majority of homeless individuals have been ineligible for coverage in the past, Medicaid managed care plans have limited experience serving this population. Participants noted that most plans are not familiar with programs and supportive services, including housing, that are key for managing health care utilization and costs for this population. In one site, participants indicated that plans are required to complete in-person health assessments, which are creating significant challenges for homeless individuals, since it is difficult for them to complete the assessment and they are disenrolled if it is not completed. Overall, participants felt some plans have recognized that the homeless population is making up a larger share of their enrollees and are working to increase their understanding of how to manage and support care for this population. However, others have not yet recognized some of the unique challenges and needs of the population. It was noted that obtaining and analyzing utilization, cost, and outcome data and increased collaboration between homeless providers and plans will be key for improving care coordination moving forward.
Delivery and Payment Reform and Data Sharing
Beyond the Medicaid expansion, broader delivery system changes are impacting homeless providers and patients. Three of the study sites (Chicago, Portland, and Albuquerque) are in states that are implementing new care coordination models within their Medicaid programs that are focused on integrating behavioral and physical services. Further, participants in Baltimore noted that the state is reorganizing its behavioral health system. Participants commented that new coordinated care models are leading to shifts in reimbursements that are tied to outcomes rather than utilization. They stressed that as new delivery and payment models emerge, it will be important for payments to reflect and accommodate the poorer health status and more complex health needs of the homeless population to prevent disincentives for serving high-need individuals.
“A homeless population shouldn’t be judged in an outcome based, value based payment structure like me. I’ve been involved in preventative healthcare and good healthcare my entire life. …That’s a very unfair equation for providers and creates a real disincentive to serve a very needy population.” Administrator, Chicago
The study sites all have good internal data sharing, but there remain gaps in data sharing with external providers. Participants noted that their health centers have internal electronic health records systems that facilitate providers’ ability to share information and coordinate across primary care, behavioral health and case management services. However, they commented that data sharing with providers outside the health center remains limited. Some are able to view data from multiple hospitals and emergency departments within their communities, while others are only connected to data at one hospital. However, they are only able to view data and do not have the ability to enter data, make changes, or insert notes. As such, coordinating and sharing information with external providers generally still requires phone calls or faxing of reports. Participants felt that increased data sharing would support better care management and continuity of care, particularly among this high-need population and as they begin utilizing care from a wider array of providers.
Conclusion and Implications
Overall, these findings show that the Medicaid expansion has already contributed to key benefits for individuals and providers within the homeless community (Figure 4). Sites in states that expanded Medicaid have experienced significant gains in coverage among their homeless patients. Participants report that these coverage gains have led to improved access to care and other broader benefits, including improved ability to work and maintain housing. Providers feel they have a wider array of treatment options available and that they are better able to provide care based on the best courses of treatment rather than on the availability of charity or discounted services. Administrators note that gains in Medicaid coverage are leading to increases in Medicaid revenue that are supporting longer-term strategic and operational improvements focused on quality, care coordination, and information technology. Increased Medicaid coverage also has supported increases in clinical and administrative staff and led to changing staff roles to meet larger billing and administrative needs. However, even with increased Medicaid revenue, participants stress that other funding sources remain vital for supporting services that are not reimbursable and supporting care for individuals who remain uninsured.
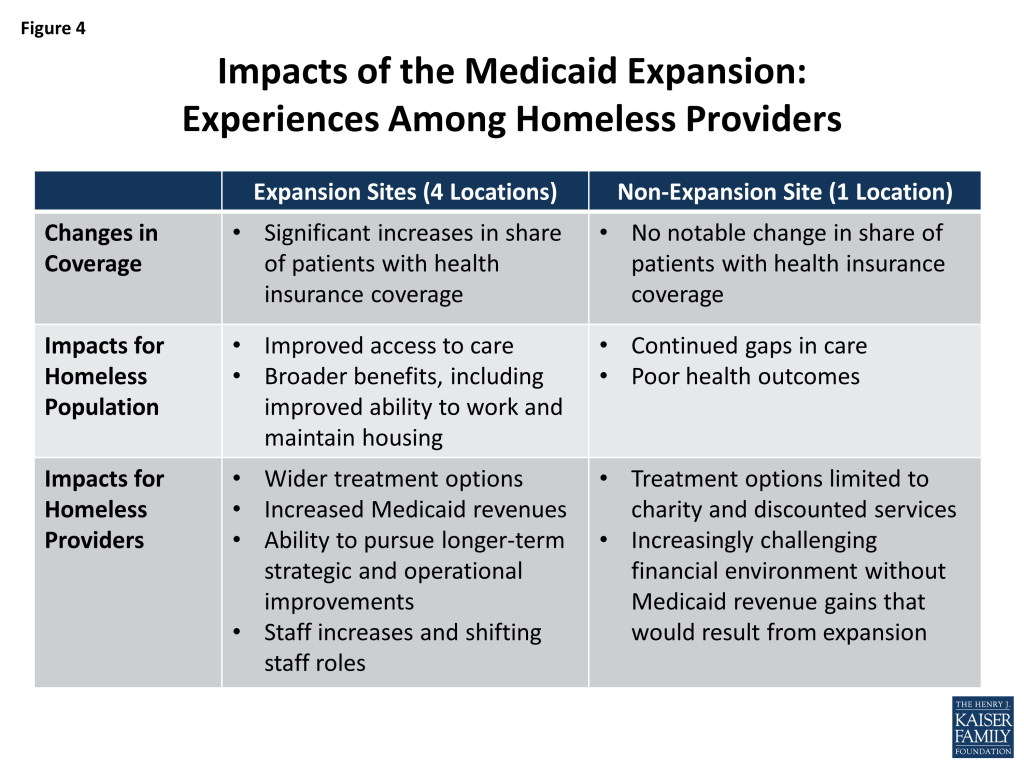
There were sharp contrasts in the experiences of the site where Medicaid was not expanded. Within the non-expansion site, homeless patients remained uninsured. Participants noted that patients continue to face significant gaps in care that contribute to poor health outcomes. Providers reported that their treatment options remain largely constrained to pro-bono, charity, and discounted services. Administrators described an increasingly challenging financial situation, noting that the site is not benefiting from gains in Medicaid revenue that would stem from the coverage expansion and is facing declines in other funding sources.
Looking ahead, participants identified a range of priorities for addressing the health care needs of the homeless population. They suggested that maintaining stable coverage for individuals and educating individuals on how to use their coverage will be key for shifting care patterns and reducing emergency room use. With regard to financing, it will be important to maintain other funding sources outside of Medicaid to support the full range of services that are important serving the population. Further, as homeless individuals are increasingly enrolled into managed care, addressing their specific needs will be key for minimizing barriers to care and administrative burdens. Amid the shifting financial and delivery environment, maintaining supportive and case management services, incorporating social determinants of health into care models, and building upon the interdisciplinary team-based models of care developed by homeless providers all will be key for engaging individuals in care. Finally, as broader payment and delivery reforms are implemented, it will be important for them to reflect the poorer health status and more complex health needs of the homeless population.
This brief was prepared by Barbara DiPietro of the National Health Care for the Homeless (HCH) Council and Samantha Artiga and Alexandra Gates with the Kaiser Family Foundation’s Commission on Medicaid and the Uninsured. The authors extend their deep appreciation to the individuals and organizations who so generously shared their time and efforts to coordinate and participant in the focus group discussions. Staff time of the National HCH Council author is supported by a Cooperative Agreement with the Health Resources and Services Administration(HRSA), Bureau of Primary Health Care, grant number U30CS09746. The publication’s contents are solely the responsibility of the authors and do not necessarily represent the official views of HRSA.
Appendix
| Appendix Table 1: Selected Administrative Data from Study Sites | |||||
| Study Site | Albuquerque, NM | Baltimore,MD | Chicago,IL | Portland,OR | Jacksonville, FL |
| Number of Patients (2013) | 4,348 | 10,072 | 8,570 | 7,159 | 5,237 |
| 2014 Budgeted Revenue | $6,217,575 | $15,995,409 | $23,084,922 | $41,709,430 | $3,887,217 |
| Share of Patients with Selected Health Conditions (2013) | |||||
| Hypertension | 18% | 25% | 21% | 31% | 30% |
| Diabetes | 9% | 8% | 9% | 18% | 16% |
| Asthma | 7% | 10% | 9% | 7% | 10% |
| HIV | <1% | 3% | 18% | 1% | <1% |
| Alcohol-related disorders | 13% | 12% | 5% | 32% | 4% |
| Hepatitis C | 5% | 6% | 2% | 6% | 1% |
| Depression/mood disorders | 28% | 18% | 26% | 25% | 10% |
| Other mental health issues | 15% | 9% | 12% | 16% | 2% |
| Percentage of Visits with Clients Who have Health Insurance, January 2012-July 2014 | |||||
| Jan-12 | 5% | 51% | 36% | 60% | 0% |
| Feb-12 | 5% | 52% | 39% | 60% | 0% |
| Mar-12 | 4% | 51% | 37% | 60% | 1% |
| Apr-12 | 4% | 50% | 38% | 60% | 1% |
| May-12 | 4% | 53% | 36% | 59% | 0% |
| Jun-12 | 4% | 53% | 37% | 60% | 1% |
| Jul-12 | 3% | 50% | 33% | 62% | 1% |
| Aug-12 | 4% | 53% | 33% | 61% | 1% |
| Sep-12 | 4% | 56% | 33% | 61% | 0% |
| Oct-12 | 3% | 57% | 31% | 57% | 0% |
| Nov-12 | 2% | 57% | 35% | 57% | 0% |
| Dec-12 | 2% | 56% | 34% | 57% | 0% |
| Jan-13 | 2% | 54% | 41% | 57% | 0% |
| Feb-13 | 3% | 56% | 44% | 57% | 0% |
| Mar-13 | 2% | 56% | 44% | 57% | 1% |
| Apr-13 | 2% | 60% | 46% | 57% | 1% |
| May-13 | 2% | 58% | 46% | 57% | 1% |
| Jun-13 | 3% | 56% | 50% | 57% | 1% |
| Jul-13 | 3% | 54% | 40% | 57% | 1% |
| Aug-13 | 3% | 54% | 48% | 58% | 1% |
| Sep-13 | 4% | 51% | 50% | 58% | 1% |
| Oct-13 | 3% | 50% | 53% | 56% | 1% |
| Nov-13 | 3% | 49% | 50% | 56% | 2% |
| Dec-13 | 5% | 51% | 50% | 56% | 2% |
| Jan-14 | 6% | 88% | 48% | 77% | 2% |
| Feb-14 | 15% | 89% | 47% | 80% | 2% |
| Mar-14 | 23% | 89% | 51% | 83% | 2% |
| Apr-14 | 27% | 89% | 54% | 83% | 2% |
| May-14 | 30% | 87% | 54% | 84% | 2% |
| Jun-14 | 30% | 86% | 54% | 84% | 2% |
| Jul-14 | 31% | 87% | 47% | 84% | 3% |
| SOURCE: Data collected from National Health Care for the Homeless study sites, 2014.*The prevalence of health conditions will vary widely from site to site based on numerous factors, to include specialized grants/programming aimed at specific conditions, the extent of screening and testing available, and the presence of other targeted community resources. | |||||
Endnotes
- Kaiser Family Foundation. (September 2012.) Medicaid Coverage and Care for the Homeless Population: Key Lessons to Consider for the 2014 Medicaid Expansion. Available at: https://modern.kff.org/health-reform/report/medicaid-coverage-and-care-for-the-homeless/. ↩︎
- U.S. Department of Housing and Urban Development (HUD), Office of Community Planning and Development. (September 2013.) The 2012 Annual Homeless Assessment Report (AHAR) to Congress. Available at: https://www.hudexchange.info/resources/documents/2012-AHAR-Volume-2.pdf. ↩︎
- U.S. Department of Housing and Urban Development (HUD). (November 2013.) The 2013 Annual Homeless Assessment Report (AHAR) to Congress, Part 1, Point-in-Time Estimates of Homelessness. Available at: https://www.hudexchange.info/resources/documents/AHAR-2013-Part1.pdf. ↩︎
- U.S. Department of Substance Abuse and Mental Health Services Administration (SAMHSA). (July 2011.) Current Statistics on the Prevalence and Characteristics of People Experiencing Homelessness in the United States. Available at: http://homeless.samhsa.gov/ResourceFiles/hrc_factsheet.pdf. ↩︎
- Fazel, S., Geddes, JR, Kushel, M. (October 2104.) “The health of homeless people in high-income countries: descriptive epidemiology, health consequences, and clinical and policy recommendations.” The Lancet 384 (9953), 1529 – 1540. Available at: http://www.thelancet.com/journals/lancet/article/PIIS0140-6736(14)61132-6/abstract ↩︎
- O’Connell, J.J. (Ed.) (2004.) “The health care of homeless persons: A manual of communicable diseases and common problems in shelters and on the streets.” The Boston Heath Care for the Homeless Program. Available at: http://www.bhchp.org/BHCHP%20Manual/pages/chapters_sections.html. ↩︎
- Morrison, D.S. (2009.) “Homelessness as an independent risk factor for mortality: Results from a retrospective cohort study.” International Journal of Epidemiology, 28(3), 877-883. ↩︎
- Ku. B, et al. (May-June 2010.) Factors Associated with Use of Urban Emergency Departments by the U.S. Homeless Population. Public Health Reports 125: 398-405. Available at: http://www.publichealthreports.org/issueopen.cfm?articleID=2402. ↩︎
- Known as “Health Care for the Homeless” grantees, these health centers are a special populations category of the health center program, administered by the Health Resources and Services Administration (HRSA). More information about HCH grantees can be found at http://bphc.hrsa.gov/about/specialpopulations/index.html. ↩︎
- U.S. Department of Health and Human Services, Health Resources and Services Administration. (2013.) Table 4: Selected Patient Characteristics, 2013 National Homeless Data. Available at: http://bphc.hrsa.gov/uds/datacenter.aspx?q=t4&year=2013&state=&fd=ho. ↩︎
- U.S. Department of Health and Human Services, Health Resources and Services Administration. (2013.) Table 4: Selected Patient Characteristics, 2013 National Data. Available at: http://bphc.hrsa.gov/uds/datacenter.aspx?q=t4&year=2013&state. ↩︎
- Medical respite care is acute and post-acute medical care for homeless persons who are too ill or frail to recover on the street from a physical illness or injury. Unlike “respite” for caregivers, “medical respite” is short-term residential care that allows homeless individuals the opportunity to rest in a safe environment while accessing medical care and other supportive services. Medical respite care is offered in a variety of settings, to include freestanding facilities, homeless shelters, nursing homes and transitional housing. More information is available at https://www.nhchc.org/resources/clinical/medical-respite/. ↩︎