Lower Income Adults with Employer Sponsored Insurance Face Unique Challenges with Coverage Compared to Higher Income Adults
The KFF Consumer Survey assessed consumers’ experiences with their health insurance coverage, their understanding of their coverage, problems they may face with their insurance, and if they believe that their insurance coverage is adequately meeting their needs. This Data Note examines the experiences of lower income adults with their current employer sponsored insurance (ESI) — including their reported satisfaction with the costs, quality, and availability of network providers — in comparison to higher income adults with ESI coverage. Lower income adults in our survey were defined as adults with reported household incomes below 200% the federal poverty line (FPL). This is any income below $27,180 for a single adult or $46,060 for a family of three. Higher income adults are defined as those with household incomes at or above 200% of FPL. Lower income adults with ESI were as likely to report insurance problems as higher income adults with ESI. However, lower income adults with ESI were more likely to report problems paying for health care, delayed treatment, and a decline in health as a result of insurance problems. Lower income adults with ESI were also more likely to say the availability and quality of health care professionals covered by their insurance was fair or poor, and were more likely to report difficulty in signing up for coverage and comparing options.
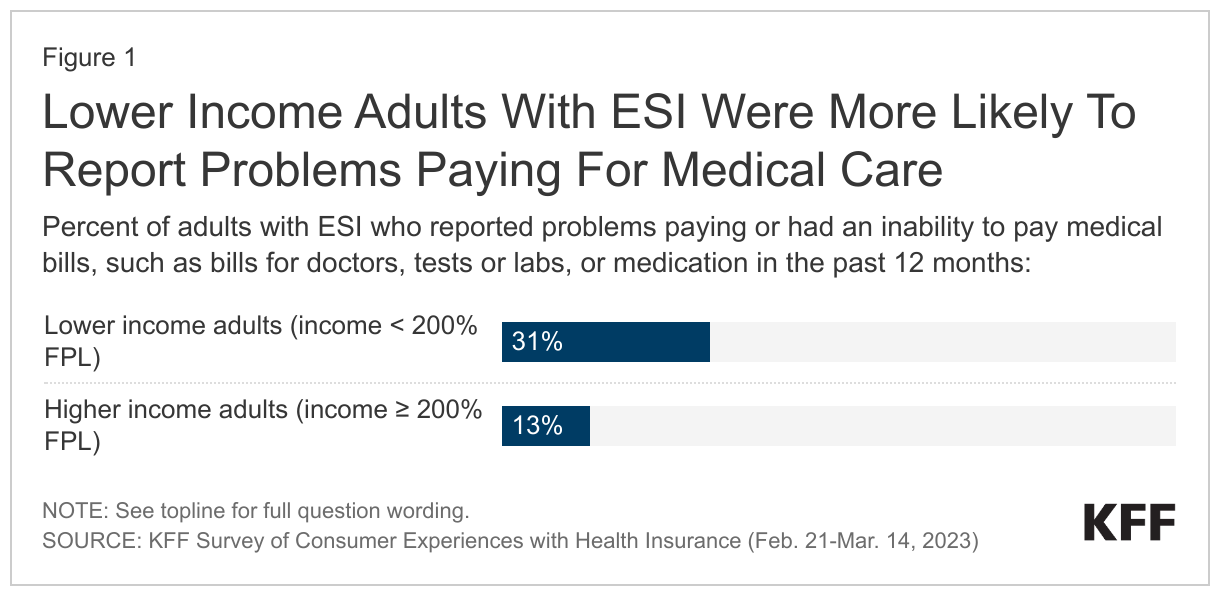
Lower income adults with ESI were more likely to report problems paying for health care services compared to higher income adults.
Among those with ESI coverage, lower income adults (31%) were over twice as likely to report trouble paying for medical bills compared to higher income adults (13%).
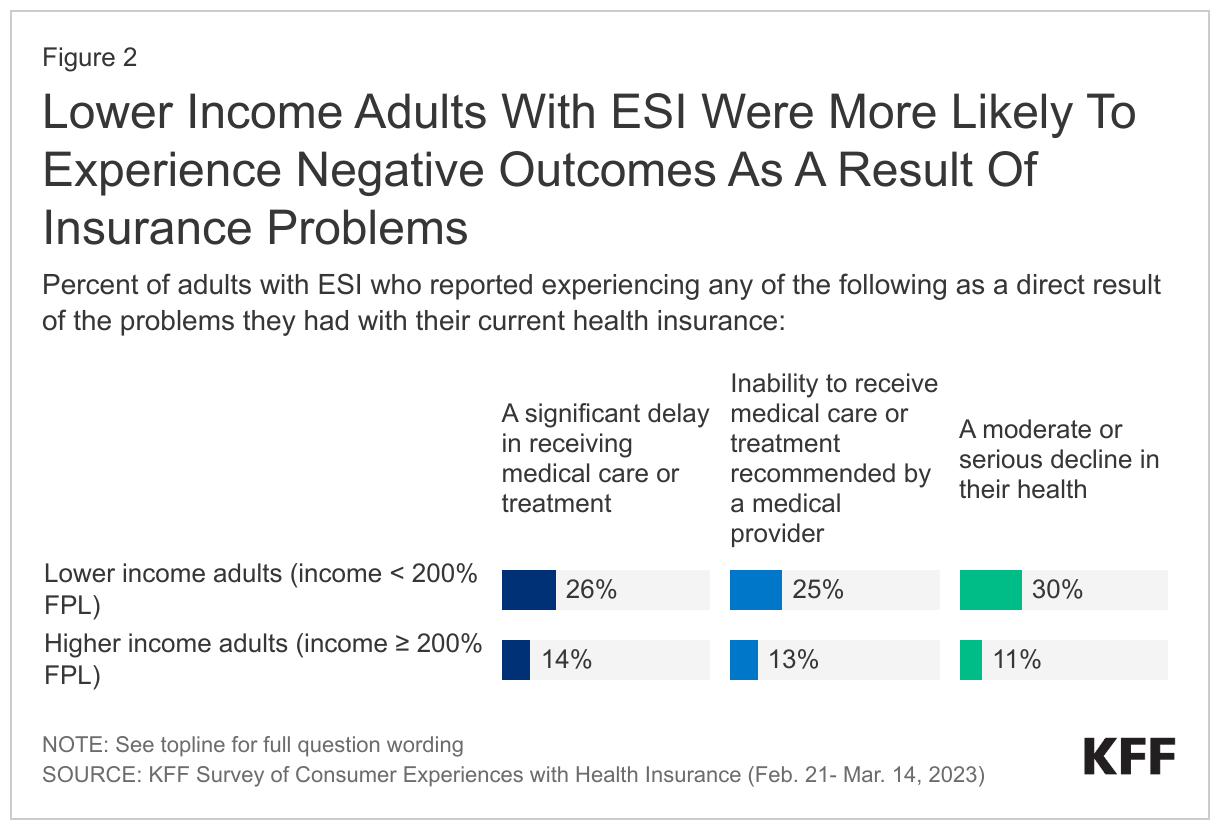
Lower income adults with ESI were just as likely to report insurance problems as higher income adults with ESI, but were more likely to delay treatment and report a decline in health as a result of insurance problems.
Lower income adults with ESI were as likely as higher income adults with ESI to report having common problems with their insurance over the past year, such as prior authorization issues (16% for lower income adults and 15% for higher income adults) and denied claims (22% for lower income adults and 21% for higher income adults). However, lower income adults were more likely than higher income adults to report negative outcomes as a result of experiencing insurance problems. Among those with ESI who had a problem with their current insurance in the past year, lower income adults were more likely to report a significant delay in treatment or care (26%) as a result of insurance problems compared to higher income adults (14%). Additionally, one in four lower income adults reported being unable to receive medical treatment recommended by a medical provider as a direct result of the problems they had with their current health insurance, compared to 13% of higher income adults. Lower income adults were also more likely to report a moderate to serious decline in health as a result of insurance problems compared to those with higher income. Over twice as many lower income adults (30%) reported a moderate or serious decline in health as a direct result of insurance problems compared to higher income adults (11%).
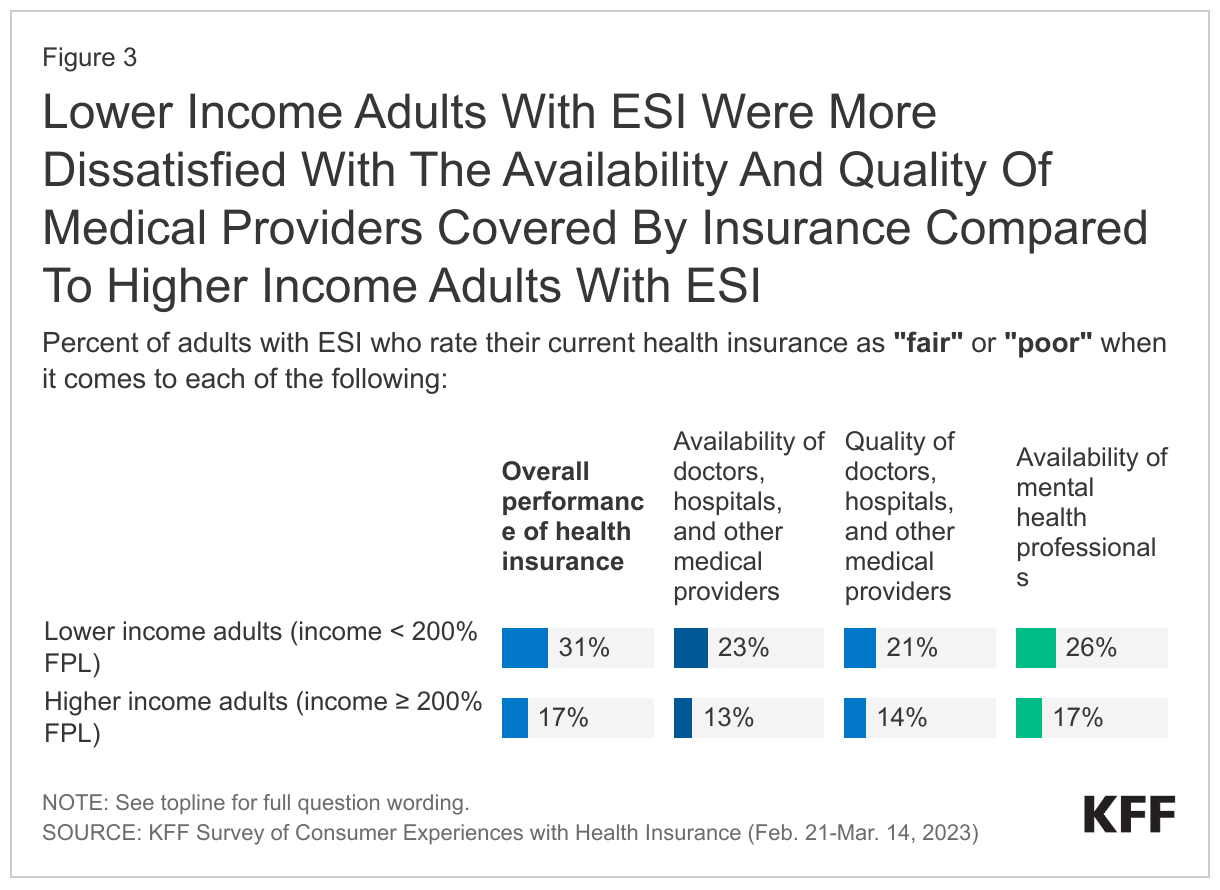
Lower income adults with ESI were more likely to rate the availability and quality of providers within their network as “fair or poor.”
Lower income adults with ESI were more likely to rate the overall performance of their current health insurance as “fair” or “poor” (31%) compared to higher income adults with ESI (17%). Additionally, lower income adults with ESI were more likely to grade the availability and quality of in-network providers within their health insurance as fair or poor overall compared to adults with higher incomes. About a quarter (23%) of lower income adults with ESI rated the availability of health care professionals covered by their insurance as “fair” or “poor,” compared to about one in eight (13%) of adults with higher incomes. In addition, one in five (21%) lower income adults rated the quality of health care professionals covered by their insurance as “fair” or “poor” compared to one in seven (14%) higher income adults. A quarter of lower income adults with ESI also gave fair or poor ratings on the availability of mental health professionals covered by their health insurance.
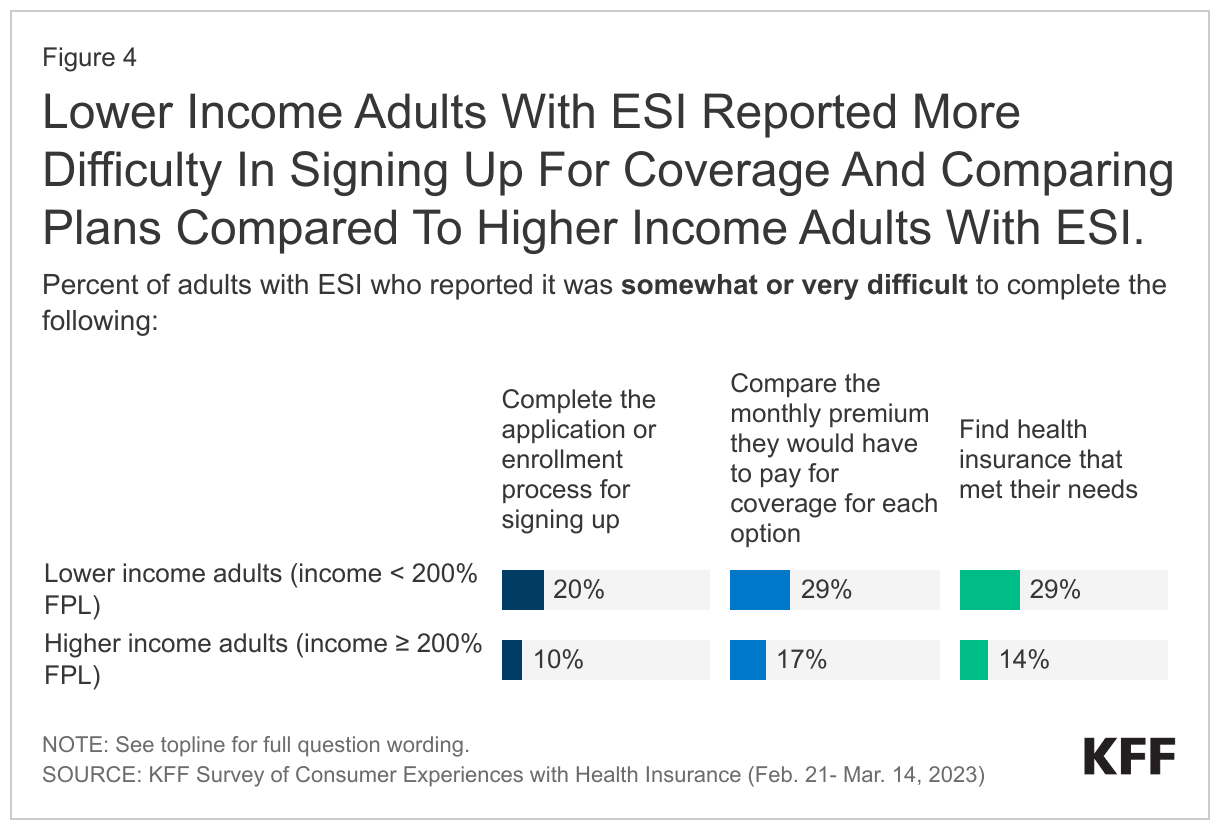
Lower income adults with ESI reported more difficulty in signing up for coverage and comparing plans compared to higher income adults with ESI.
Lower income adults with ESI (20%) were twice as likely to state that the application process for insurance was somewhat or very difficult compared to higher income adults (10%). Additionally, three in ten (29%) lower income adults reported more difficulty in comparing the monthly premium among insurance options, compared to 17% of those with higher incomes. Lower income adults were also twice as likely to report difficulty finding a health plan that met their needs (29%) than higher income adults (14%).
Discussion
Lower income adults face unique financial barriers to health care that could negatively affect their health outcomes. Lower income adults with ESI in our survey were much more likely to report financial difficulties in paying for medical bills, aligning with past research that shows lower income adults tend to spend a higher share of their income on health care costs compared to higher income adults. Many lower income adults do not have a safety net or savings to pay for medical costs and are disproportionately burdened by medical debt. High health care costs may deter lower income adults with ESI from seeking the medical care they need, leading to worse health outcomes. Lower income adults often cannot afford to lose income to see their health care provider if their job does not offer enough sick leave or paid time off, which could also lead to worse health outcomes down the line. Some lower income individuals are denied care due to outstanding medical bills, which could worsen any illness or condition that they have. Additionally, lower income adults are more likely to be exposed to occupational hazards within the workplace that can lead to injury or disease, which could also lead to unexpected, pricy medical costs or a reduction in wages.
Some lower income adults with ESI may end up paying more for “affordable” insurance through their employer than they would pay for other types of coverage. For example, some lower income adults are eligible for cost-sharing reductions and premium assistance that would greatly lower the percentage of monthly income they would be expected to contribute towards their monthly premium (as low as 0 to 2% for those with incomes less than 200% FPL) for a Marketplace plan, but cannot take advantage of this financial assistance if the employer plan they are being offered meets an affordability threshold under by the ACA (a premium contribution of 8.39% of income for 2024). Additionally, adults who are eligible for Medicaid or state premium assistance programs in their state would typically face lower out-of-pocket spending with these coverage types compared to if they enrolled in ESI coverage, although these options may not available to single adults who live in states that did not expand Medicaid or have not established a state premium assistance program.
Nearly six in ten employers reported that they have a moderate or high level of concern regarding cost-sharing for their employees. Some employers have attempted to reduce health care costs for adults with ESI, specifically for those with lower incomes, through use of different health care plan designs such as:
- Salary based premium programs: These are programs that base the monthly premium amount an enrollee is expected to pay on their annual salary. Salary-based premium programs lower monthly premium costs but may not contain costs for other out-of-pocket expenses like deductibles.
- Co-pay plans: These plans offer flat fees for routine doctor visits and typically have low deductibles. Co-pay plans may be beneficial for those who use insurance primarily for routine visits, but may also be financially burdensome for those who need care outside of routine health care services, as these may lead to higher health care costs.
- High deductible health plans (HDHPs): These are health plans that have higher deductibles but low premium costs. HDHPs are typically beneficial for those who can contribute or meet the deductible by enrolling in a Health Savings Account (HSA), a benefit sometimes offered to those enrolled in HDHPs where they can set aside money on a pre-tax basis to pay for out-of-pocket healthcare costs or a Health Reimbursement Account (HRA) where ESI enrollees can be reimbursed for paying for certain medical expenses. Lower income adults with ESI sometimes do not have enough money to meet the deductible, even when a savings option such as an HSA or HRA is available. In addition, tax-preferred HSAs and HRAs are of less value to lower income people in lower tax brackets.
Uptake of health plans designed to lower cost-sharing for ESI enrollees is unknown. Ten percent of large firms reported implementing a program that lowers premium costs for lower income enrollees, and five percent offered programs that help lower cost sharing for lower income enrollees overall. One brokerage firm survey found that 39% of employers surveyed offered co-pay plans to their enrollees, and 19% offered a salary based premium program.
Lower income adults with ESI reported more problems in accessing timely and quality behavioral health services compared to higher income adults with ESI. Ensuring timely and adequate access to behavioral health care is an issue for those with ESI coverage, but the survey findings indicate that this may be an even bigger problem for lower income adults with ESI, who are more likely than their higher income counterparts to rate their insurance coverage negatively in terms of the availability of mental health providers. It is not clear whether lower income adults with ESI are more challenged by time and distance to in-network providers, lack of available appointments, high demand, difficulties in accessing providers using public transportation or other issues, such as fewer providers regardless of in-network status who they trust with their care. Studies have shown that many individuals with employer coverage must access behavioral health care through out-of-network providers, paying the higher out-of-network rates or paying the entire cost of the care. This may simply not be an option for a lower income adult with the same ESI coverage. Also, lower income adults with ESI may be more likely to choose an ESI coverage option with a narrower network than other available plan options because it is the lowest cost option available. Proposed updates to the Mental Health Parity and Addiction Equity Act would require health plans, including employer-sponsored plans, to collect and evaluate information related to the status and breadth of their behavioral health networks, including utilization of out-of-network behavioral health.
Lower income adults reported that they were more likely to experience difficulty in signing up for coverage and this could lead to worse health outcomes and medical debt. Lower income respondents with ESI in our survey were more likely than those with higher incomes to report having a difficult time comparing plan options and signing up for coverage that best met their needs. This could be related to more complex needs, as well as lower levels of education. Signing up for coverage and comparing options can be complicated for consumers. While Human Resources (HR) departments can be helpful, HR professionals, especially those working in small firms, might not always have the time or expertise needed to assist employees. Also, signing up for coverage can also be especially challenging for those who are eligible for coverage options outside of ESI (e.g., adults who are eligible for Medicaid in their state) or for consumers who are switching to ESI coverage as a result of the unwinding of the Medicaid continuous enrollment requirement and must navigate complications that come with the ESI enrollment process, such as enrolling in coverage in alignment with special enrollment period deadlines.
It may be difficult for lower income adults with ESI to find assistance outside of Human Resources that will help them with the enrollment process, including comparing available choices between ESI and public programs. Insurance brokers might provide assistance for those eligible for Marketplace coverage, but, according to a 2022 KFF Assister survey, brokers were less likely than other assisters to provide help with Medicaid enrollment, and did not always have the same ability to work with those who needed language assistance. There is no longer any federally supported program that is designed to offer resources to those with ESI as there was under the Consumer Assistance Program (CAP). CAP was established under the ACA and offered federal funding for states to create programs to assist consumers with insurance problems and identify their best options for health coverage. Unlike the Navigator program that was specifically created to assist Marketplace, Medicaid, and CHIP consumers, the CAP program was able to assist consumers with ESI coverage as well as those with other types of coverage, for those states that chose to participate. 35 states and the District of Columbia signed up for CAP in 2010, but the grant was not renewed for federal funding, eliminating the only federally funded program that could assist those with ESI coverage. Many states have continued their CAP programs through their own funding, but others have discontinued their operations.
Methodology
This KFF Survey of Consumer Experiences with Health Insurance was designed and analyzed by public opinion researchers at KFF. The survey was designed to reach a representative sample of insured adults in the U.S. The survey was conducted February 21–March 14, 2023, online and by telephone among a nationally representative sample of 3,605 U.S. adults who have employer sponsored insurance plans (978), Medicaid (815), Medicare (885), Marketplace plans (880), or a Military plan (47).
The margin of sampling error for adults with employer-sponsored insurance is plus or minus 4 percentage points. For the 213 adults with employer-sponsored insurance with a household income under 200% of the federal poverty line the margin of error is plus or minus 8 percentage points. For the 758 adults with employer-sponsored plans and household incomes of 200% of the federal poverty line or greater, the margin of sampling error is plus or minus 4 percentage points.
The sample includes 2,595 insured adults reached through the SSRS Opinion Panel either online or over the phone (n=75 in Spanish). Another 504 respondents were reached online through the Ipsos Knowledge Panel. Another 289 (n=10 in Spanish) interviews were conducted from a random digit dial (RDD) of prepaid cell phone numbers (n=190) and landline telephone numbers (n=99). An additional 217 respondents were reached by calling back respondents who said they were insured in previous KFF probability-based polls.
Respondents were weighted separately to match each group’s demographics using data from the 2021 American Community Survey (ACS). Weighting parameters included gender, age, education, race/ethnicity, and region.
For full details on the survey methodology, see the Methodology tab of the KFF Survey of Consumer Experiences with Health Insurance.
This work was supported in part by a grant from the Robert Wood Johnson Foundation. The views and analysis contained here do not necessarily reflect the views of the Foundation. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.