How Might Federal Medicaid Cuts in the Enacted Reconciliation Package Affect Rural Areas?
Note: Originally published on July 2, this brief has been updated to reflect new CBO estimates of the reconciliation law’s impact.
 Approximately 66 million people – about 20% of the U.S. population – live in rural areas, where Medicaid covers 1 in 4 adults (a higher share than in urban areas) and plays a large part in financing health care services. In rural communities, Medicaid covers nearly half of all births and one fifth of inpatient discharges. The Congressional Budget Office (CBO) estimates that the enacted reconciliation package would reduce federal Medicaid spending by an estimated $911 billion over ten years, and result in 10 million more uninsured people nationwide. Senators from both parties have raised concerns about potential impacts on rural hospitals and other providers, particularly given the ongoing trend of rural hospital closures.
Approximately 66 million people – about 20% of the U.S. population – live in rural areas, where Medicaid covers 1 in 4 adults (a higher share than in urban areas) and plays a large part in financing health care services. In rural communities, Medicaid covers nearly half of all births and one fifth of inpatient discharges. The Congressional Budget Office (CBO) estimates that the enacted reconciliation package would reduce federal Medicaid spending by an estimated $911 billion over ten years, and result in 10 million more uninsured people nationwide. Senators from both parties have raised concerns about potential impacts on rural hospitals and other providers, particularly given the ongoing trend of rural hospital closures.
To address those concerns, the reconciliation package includes $50 billion in funding over five years (starting in fiscal year 2026) for state grants through a Rural Health Transformation Program (referred to here as the “rural health fund”). This policy watch estimates how the reconciliation package would affect federal Medicaid spending in rural areas and how that compares to the newly proposed funding for rural areas through the rural health fund. This analysis estimates the likely effects in rural areas by building on KFF’s estimated reductions in Medicaid spending across the states.
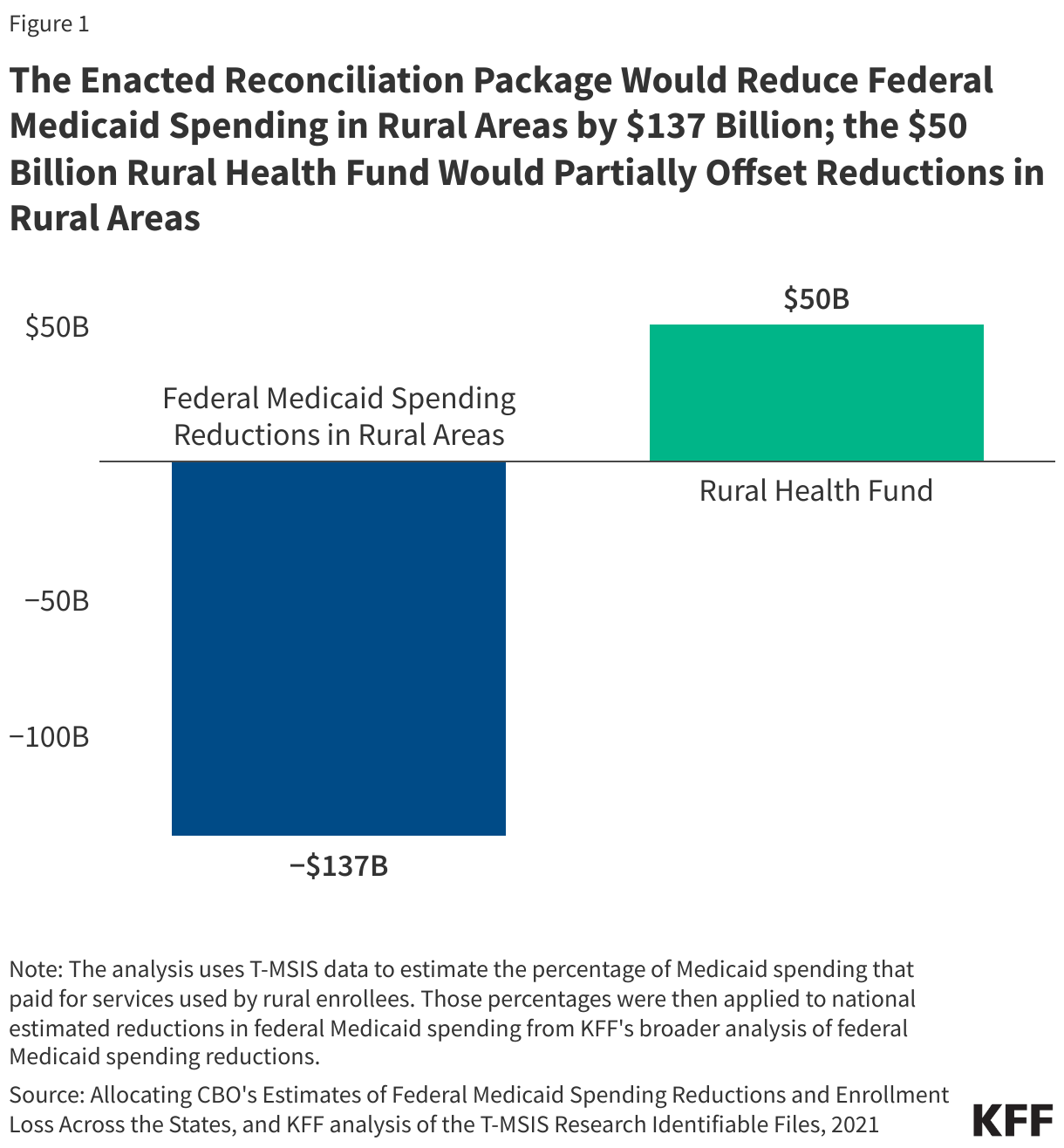
Under the reconciliation package, federal Medicaid spending in rural areas is estimated to decline by $137 billion, more than the $50 billion appropriated for the rural health fund (Figure 1). Building on separate KFF estimates of state-by-state Medicaid cuts, this analysis estimates that federal Medicaid spending in rural areas could decrease by $137 billion over 10 years—about $87 billion more than is appropriated for the rural health fund.
The analysis allocates each state’s estimated spending reductions from the KFF analysis of the reconciliation package to urban and rural areas using the percentage of Medicaid spending that paid for services used by rural enrollees within each state. The estimates may understate the effects on rural areas because they do not account for the full change in total Medicaid spending, which would include the federal spending reductions and the associated reduction in state Medicaid spending stemming from lower enrollment. The estimates also do not account for spending cuts related to Affordable Care Act (ACA) Marketplace coverage from the reconciliation bill, the expiration of enhanced ACA premium tax credits that were enacted during the COVID-19 pandemic, and the impact of proposed Marketplace integrity rules. Combined, the changes represent the “biggest rollback in federal support for health coverage ever.” Federal spending cuts and coverage losses could also have implications for rural hospitals and other providers, including increases in uncompensated care. While providers could potentially offset at least some of the cuts—including through the new rural health funding—any financial pressure on hospitals and other providers could lead to layoffs of staff, more limited investments in quality improvements, fewer services, or additional rural hospital closures.
Although this analysis provides state-by-state estimated reductions in Medicaid funding, it does not show estimated rural health funds by state because it is unclear how the rural health funds will be allocated across the states and how the Secretary may interpret the law. Fifty percent of the funding would be equally distributed among states with approved applications, while the remainder would be allocated by the Centers for Medicare and Medicaid Services (CMS) using a method that takes into account such factors as states’ rural populations within metropolitan areas, the share of rural health facilities nationwide that are in a state, and the situation of hospitals which serve a disproportionate number of low-income patients with special needs. The bill specifies that the funds could be used in a variety of ways, including promoting care interventions, paying for health care services, expanding the rural health workforce, and providing technical or operational assistance aimed at system transformation. It is unclear how the funds will be distributed across states and how states will allocate funding between hospitals, other providers, and various state initiatives.
Over half of the spending reductions in rural areas are among 12 states that have large rural populations and have expanded Medicaid under the ACA, 10 of which could see rural federal Medicaid spending decline by $5 billion or more over 10 years. Those 10 states include Kentucky, North Carolina, Illinois, Virginia, New York, Michigan, Ohio, Pennsylvania, Oklahoma, and Louisiana. Kentucky would experience the largest rural Medicaid spending reduction, with an estimated drop of nearly $11 billion over 10 years (Figure 2). Over half of the estimated federal spending cuts stem from provisions that only apply to states that have adopted the ACA expansions, including work requirements, more frequent eligibility determinations, and new cost sharing requirements. As a result, the effects of the reconciliation bill in rural areas will be larger for expansion than non-expansion states.
