Introduction
In the wake of COVID-19, the world has a new global health, multilateral financing mechanism known as the Pandemic Fund. Based at the World Bank, and officially launched in November 2022, it is the first mechanism with the specific purpose of providing sustained financing to help countries build their capacity to prevent, prepare for, and respond to epidemics and pandemics. While there had been discussions for years about increasing the amount of multilateral financing (i.e., donor funding channeled through an intergovernmental entity) directed to pandemic preparedness, it wasn’t until COVID-19 that policymakers and donors were spurred into action to create a formal mechanism for this purpose. The U.S. government has been a key champion of the Pandemic Fund since President Biden came into office in 2021 and the U.S. has provided more funding than any other donor up to this point.
Given how nascent the fund is, there are still many unknowns and unanswered questions about how it will be implemented, the scope and duration of its work, and how it fits into the broader set of global health efforts. To help shed light on these topics, this brief reviews the evolution and establishment of the Pandemic Fund, describes the Fund’s governance and operations, and discusses key issues and challenges for the Fund – particularly related to U.S. engagement – as it continues to make its transition from concept to implementation.
History and Development
There have long been calls for increased global cooperation and more international funding for building pandemic preparedness and response (PPR) capabilities worldwide. In 2005, World Health Organization (WHO) member states agreed to a revised set of rules for prevention of and response to international health crises, known as the International Health Regulations (IHRs) and, among other things, committed to build up core capacities for PPR. However, progress toward meeting established capacity benchmarks was slow and led to efforts to direct more attention and funding to PPR, such as the establishment of the Global Health Security Agenda in early 2014, just before the emergence of the largest Ebola outbreak in history. As a result, numerous expert commissions, panels, and international institutions pointed again to significant weaknesses in global PPR capabilities and recommended greater international coordination and increased funding. While a few incremental changes were enacted post-Ebola, it was clear that major gaps in PPR capabilities worldwide remained and funding was limited compared to estimated need. Even before COVID-19 emerged, some experts were already calling for increased multilateral funding for PPR including through multilateral development banks like the World Bank.
Box 1: Selected Timeline in the Lead up to the Pandemic Fund
- 2014: West African Ebola Epidemic begins
- 2017: World Bank International Working Group on Pandemic Preparedness Financing report calls for greater funding for global pandemic preparedness and response (PPR) capacity building
- 2019: Center for Strategic and International Studies report recommends new multilateral PPR financing; the Center for Global Development and the Nuclear Threat Initiative propose a new Global Health Challenge Fund
- January 2020: World Health Organization (WHO) declares COVID-19 a public health emergency of international concern (PHEIC)
- January 2021: G20 nations establish a High-Level Panel on Pandemic Financing
- January 2021: Biden White House releases National Strategy for COVID-19 Response and Pandemic Preparedness, calling for the Treasury Department to develop a strategy on how the U.S. can promote additional PPR financing through international financial institutions including the World Bank
- September 2021: The First Global COVID-19 Summit convened by President Biden, at which the US announces support for a multilateral PPR financing mechanism and commits $250 million
- May 2021: Independent Panel for PPR releases report calling for the creation of a “Pandemic Financing Facility” that would direct $5 to 10 billion annually for pandemic preparedness activities worldwide
- June 2021: G20 High Level Independent Panel releases report on Financing the Global Commons for PPR, including a recommendation to create a Global Health Threats Fund structured as a Financial Intermediary Fund (FIF) at the World Bank, which mobilizes at least $10 billion annually for global PPR efforts
- September 2021: Biden White House calls for creation of a pandemic FIF housed at the World Bank
- March 2022: WHO and World Bank’s G20 Joint Finance & Health Task Force analysis of PPR architecture, financing needs, gaps and mechanisms released, calling for $10 billion in external PPR financing annually over the next five years
- April 2022: G20 finance ministers agree to support the establishment of a Pandemic FIF at the World Bank
- May 2022: Second Global COVID-19 Summit held, donors pledge support to a Pandemic FIF, including an additional $200 million from the U.S. (for a total U.S. commitment of $450 million at this point)
- May 2022: World Bank “White Paper” on a proposed Pandemic FIF released
- June 2022: World Bank Board of Directors approves creation of a Pandemic FIF, forms Governing Board
- September 2022: Pandemic FIF formally established at the World Bank
- November 2022: Pandemic FIF re-named the “Pandemic Fund” and officially launched by G20 countries
- Jan-Feb 2023: An estimated 650 expressions of interest for funding submitted by countries, regional bodies and global health organizations in advance of the first call for proposals
- March 2023: First Pandemic Fund Call for Proposals is released, with the Fund making $300 million available; over subsequent months reportedly over 100 countries submit proposals for funding requests totaling over $7 billion
- May 2023: G7 leaders communique re-iterates support for the Pandemic Fund and encourages increased contributions; the White House announces an additional $250 million contribution to the Fund (pending Congressional notification), raising total U.S. pledges to $700 million
When COVID-19 precipitated a worldwide crisis starting in 2020, broader interest in multilateral PPR funding was re-ignited. Reports from high level international panels and expert commissions such as the G20 Joint Task Force and the Independent Panel for Pandemic Preparedness and Response recommended increased funding and using multilateral development banks to channel additional support for PPR. Endorsements and support for the idea of a “financial intermediary fund” (FIF) for PPR came from the Biden White House, the WHO Director-General, the European Union, and many other policymakers, organizations, and experts. In April 2022, G20 finance ministers agreed to establish such a fund and in June 2022, the World Bank approved the creation of a “financial intermediary fund for pandemic preparedness and response (FIF).” The FIF was formally established in September 2022, and officially launched as the renamed “Pandemic Fund” in November 2022 (see Box 1 for a fuller timeline of events in the development of the Pandemic Fund).
The decision to house the Fund at the World Bank reflected the Bank’s role in hosting similar mechanisms. While the Pandemic Fund is the first FIF focused on PPR specifically, there are at least two dozen other FIFs hosted by the World Bank, including a number of other global health-focused FIFs such as the Coalition for Epidemic Preparedness Innovations (CEPI), the Global Fund to Fight HIV/AIDS, Tuberculosis and Malaria, and the Global Finance Facility for Women, Children and Adolescents. Each FIF has its own unique rules and approaches to governance, financing, implementation, funding amounts, and other characteristics.
Mission, Governance, and Operations
The Fund has only recently been officially launched, and details of how it is governed and how it operates have had to be crafted over a relatively compressed time period. Stakeholders including donors, beneficiary governments, international agencies such as the WHO and World Bank, and civil society groups have all helped shape these details since mid-2022, and some aspects continue to evolve as the Fund moves further into its implementation phase. Several documents have been released by the World Bank and the Fund to describe how it works, including: a Board paper on establishing the Fund, a Governance Framework, and an Operations Manual. The Fund also released its first Call for Proposals, which outlines in more detail the process for submission, review, and distribution of funding.
This section summarizes publicly available information about the Fund’s governance and operations, and reviews key issues and debates that emerged as policies were developed.
Mission
According to the Governance Framework, the primary objective of the Fund is to “provide a dedicated stream of additional, long-term funding for critical pandemic PPR functions” to support and reinforce existing capacity building efforts. More specifically, the Fund is designed to add value by: 1) mobilizing additional sources of financing, including philanthropic and private sector funding more broadly, 2) leveraging its resources to incentivize more spending via matching domestic resources, co-financing and/or “concessional” lending, and 3) harmonizing spending for PPR and health systems by bringing actors together and linking financing with country level planning and prioritization processes.
As the Fund was being developed, the importance of this additionality was emphasized frequently. Rather than being another vehicle to re-direct existing government donor financing to global health security, the Fund is meant to draw in funding that would not otherwise be available and use its funding in such a way to encourage more spending by domestic governments and the private sector on pandemic preparedness activities.
Financial Status
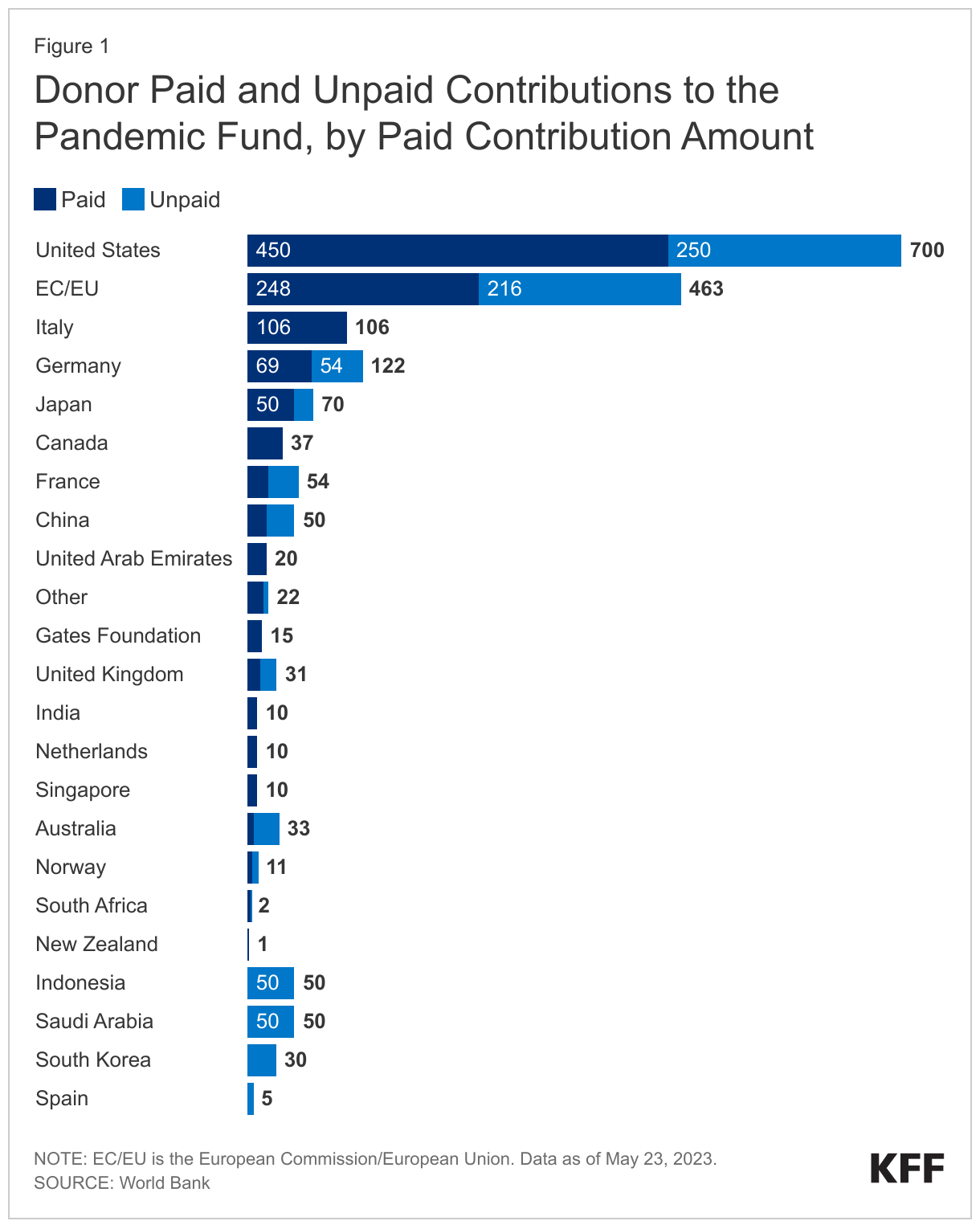
As of May 22, 2023, 26 donors (including countries, philanthropic foundations, and non-profit organizations) had pledged an estimated total of $1.9 billion in support of the Pandemic Fund, some of which consists of future commitments. The total amount received from donors and available for use (as of May 22, 2023) is reported as $1.1 billion, $300 million of which is dedicated to funding projects resulting from the first call for proposals.
The three largest donors to date by total amount committed (including paid and unpaid funds) are: the U.S. ($700 million), European Commission/European Union (EU/EC, $464 million), and Germany ($123 million). Counting only amounts paid in, the three largest donors so far are the United States ($450 million), the EU/EC ($248 million), and Italy ($106 million). Figure 1 shows a list of donor paid and unpaid contributions, by paid in amounts.
Governance
Policymakers faced many questions and debates about how to structure the Fund’s governing bodies to ensure some balance in decision-making and oversight between donors, international agencies, governments, private sector and civil society, and other stakeholders. In particular, there was a push from some low- and middle-income governments, advocates, and civil society representatives for their inclusion in Fund governance, a position supported by the United States. Ultimately, a decision was made to incorporate a broad set of stakeholders into the Fund’s governance structure, as follows:
- A Governing Board (the “Board”) is the principal decision-making body for the Fund, responsible for discussing and approving plans, priorities, principles, budgets, changes to governance and operations, and more. The Board has a total of 21 voting seats (with an equal number of alternates) divided among several constituencies as follows (members as of March 2023 listed here):
- Nine for “Contributors” (i.e., representatives from donor governments such as the U.S.)
- Nine for “Co-investors” (i.e., representatives from Fund-eligible country governments)
- One for philanthropic/foundation contributors
- Two for representatives from civil society/community groups (one for the “Global North” and one for the “Global South”).
- There are also non-voting members on the Board, including a representative from the G20, the Chair and Vice-Chair of the Technical Advisory Panel (see below), plus any other representatives from entities as approved by the Board. There are additional Observer seats as well, including representatives from the Trustee, Implementing Agencies, and the Secretariat (more on these below).
- A Technical Advisory Panel (TAP) is the principal advisory body to the Board, comprised of up to 20 experts drawn from a range of PPR-relevant fields and practice areas. The TAP has responsibilities for advising the Board on technical, financial, and other matters, including review, analysis, and recommendations related to proposals for funding. A senior WHO official (currently Mike Ryan) is the TAP Chair, and a “non-WHO” expert (currently Joy St. John from the Caribbean Public Health Agency) is the Vice Chair. Beyond these 20 (membership shown here), additional experts may be called to contribute on an as-needed basis. TAP members serve for two years, up to two consecutive terms.
- The Secretariat is the office responsible for day-to-day FIF operations and performs duties including convening Board and TAP meetings, developing the calls for proposals, compiling progress and evaluation reports, liaising with external partners, and other activities. Located at the World Bank, the Secretariat is comprised of a small staff of “professional and administrative staff employed by the World Bank or seconded to the World Bank from WHO.”
- The Trustee for the pandemic FIF is the World Bank, which is responsible for receiving and holding funds from contributors, providing financial oversight and agreements, reviewing financial reports, and other tasks.
The current Board is comprised of interim members put in place as the Fund was first established. A “Board reset,” which may result in turnover of some individuals currently occupying Board seats, is scheduled for May 2023.
Operations
The Fund’s Operations Manual describes key current operational aspects as follows:
Funding modalities, eligibility, and implementing agencies
The Fund can receive donor funding from governments, intergovernmental organizations, as well as approved non-governmental entities such as foundations/philanthropies. Any donor to the Fund enters an agreement with the Trustee (the World Bank), and contributions from non-governmental entities are subject to review and approval by the Governing Board. Contributions can be made as one-time payments or installments for up to eight years. All contributions are pooled for subsequent allocation by the Governing Board (more on this below). No donor contributions can be earmarked in advance for specific projects or recipients.
Pooled donor funds are to be directed in support of relevant capacity building activities at national, regional, and/or global levels. Countries that are eligible to receive World Bank funding (i.e., the World Bank-defined IBRD and/or IDA countries) are eligible to receive Pandemic Fund support. Regional entities that are specialized technical institutions supporting public health and/or strengthening preparedness capacity and established by governments of one or more eligible countries, as well as regional development communities and economic organizations, are also eligible for funding. Governments and entities that receive funding are known as Beneficiaries.
Funding is not provided directly to Beneficiaries, however. Instead, the Pandemic Fund channels funding through a pre-determined set of “Implementing Agencies” that partner with Beneficiaries to carry out activities that advance the Fund’s mission. The Pandemic Fund cannot provide grants for projects that do not involve an Implementing Agency. Currently, the Fund has named the following 13 Implementing Agencies as eligible:
- Multilateral Development Banks: African Development Bank, Asian Development Bank, Asian Infrastructure Investment Bank, European Investment Bank, Inter-American Development Bank, International Finance Corporation, World Bank
- United Nations Institutions: Food and Agriculture Organization, UNICEF, World Health Organization
- Other Multilateral & Global Health Organizations: Coalition for Epidemic and Preparedness Innovations (CEPI), Gavi the Vaccine Alliance (Gavi), the Global Fund to Fight AIDS, Tuberculosis and Malaria (Global Fund).
The Governing Board can approve additional Implementing Agencies, subject to a review and accreditation process.
Funding Proposal Review and Approval
Pandemic Fund grants will be allocated via a process of proposal submissions, review, and Board approval. The Secretariat will issue periodic calls for proposals and associated funding envelopes, asking for proposals from eligible parties for investments in specific PPR focus areas. Proposals may be submitted by one or more countries and/or regional entities, and must identify at least one approved Implementing Agency to support project implementation. The Secretariat receives and screens proposals to ensure compliance with the Fund’s governance and operations framework. Among other requirements, each proposal must include a description of its monitoring and evaluation approach, and these results must be tied to a specific results framework that measures progress in raising preparedness scores according to standard evaluation measures such as the WHO’s Joint External Evaluation (JEE) or State Party Self-Assessment Report (SPAR) and the World Organization for Animal Health’s Performance of Veterinary Services (PVS) Pathway tool.
Each proposal that meets compliance standards will be sent to the TAP for review and scoring. The TAP will review submissions for adherence to the criteria in the request for proposals, as well as other aspects such as technical soundness, cost efficiency, fit within the broader context of PPR and health financing, impact, and equity. Each proposal will be scored according to specific criteria and a system developed and approved in advance by the Governing Board. The TAP will submit its written assessments and scores to the Governing Board via the Secretariat, for final review and approval. The Governing Board then decides on allocations for approved proposals based on their assessed merit and resources available for distribution.
In January 2023, the Pandemic Fund asked potential Beneficiaries to submit preliminary expressions of interest for funding and through February had received a reported 650 such submissions. On March 3, 2023 the Fund released its first official call for proposals, which focuses on one or more of the following technical areas: 1) disease surveillance systems, 2) laboratory systems, and/or 3) strengthening human resources/public health workforce capacity. The Fund is making available $300 million for this round of proposals, with submissions required by May 2023 and final funding decisions expected by July 2023.
U.S. Engagement
The U.S. has publicly and actively supported the effort to direct additional multilateral financing for COVID-19 and PPR efforts more broadly since President Biden took office in January 2021. Soon after his inauguration the President released a National Strategy for the COVID-19 Response and Pandemic Preparedness that emphasized the need for more funding for PPR, and called on the U.S. Treasury to work with the World Bank and others to promote additional financing through multilateral financial institutions. At the U.S.-hosted first Global COVID-19 Summit in September 2021, the White House specifically called for the creation of a pandemic financial intermediary fund to be housed at the World Bank, and committed the first funding toward the mechanism. The U.S. Treasury, as the lead government agency for engagement with multilateral financing institutions, has played an ongoing role in advocating for and advancing the development of the Pandemic Fund, with U.S. Treasury Secretary Janet Yellen frequently voicing support and calling for more donor engagement and financing for this mechanism. The U.S. currently occupies one of nine “Contributor” (donor country) seats on the Pandemic Fund Board.
As the Fund as evolved, the U.S. government has sought to shape its governance and operational aspects according U.S. priorities. Many U.S. priorities for the Fund, as expressed by U.S. officials in response to initial World Bank proposals, have been implemented in the current Fund approach. For example, the U.S. pushed for a more inclusive Board and governance structure that includes recipient country and civil society representation, and sought to expand the set of implementing partners to include existing global health institutions such as Gavi, CEPI, and the Global Fund.
To date, the U.S. has both pledged and paid in more funding to the mechanism than any other single donor. The U.S. made an initial commitment of $250 million for the Fund in September 2021, and in May 2022 announced it was increasing its commitment to $450 million. In May 2023, the U.S. announced it would direct an additional $250 million to the Fund (pending Congressional notification), which brings the total of pledged U.S. contributions to $700 million. This would represent 37% of all donor commitments made so far. As of May 2023, the amount the U.S. has paid in ($450 million) represents about 40% of all financing received by the Fund to date. U.S. contributions have been drawn from a mix of COVID emergency supplemental funding and funding provided to USAID for global health security.”
For its part, Congress has drafted bills in support of more multilateral financing for pandemic preparedness, including through a new fund. The House passed a global health security bill in 2021 that, among other actions, authorized U.S. engagement with and contributions to a new multilateral fund for pandemic preparedness. While that bill was not passed by Congress in 2021, much of the language and expression of support for the Fund was eventually incorporated into the 2023 National Defense Authorization Act, which passed into law in December 2022. That legislation authorizes up to $5 billion in U.S. contributions to the Pandemic Fund over five years ($1 billion per year), and outlines requirements such as that U.S. contributions to the Fund are to not exceed one-third of all donor contributions to the mechanism. White House budget requests in FY 2023 and FY 2024 each asked Congress to provide $500 million for the Fund, but so far Congress has not appropriated any additional funding (beyond already existing COVID-19 emergency funding). Still, in final appropriations bills for FY 2022 and FY 2023, Congress provided the administration with the authority to transfer funding for global health programs more generally to the Pandemic Fund.
Policy Issues
The Pandemic Fund is still quite new, having launched only last year and just now readying its first round of funding. As such, many of the details about its policies, procedures, and operations are still being negotiated and fleshed out, with some changes and clarifications sure to come in the future. Still, enough is known at this point to identify key challenges and issues the Fund faces, now and going forward. These include:
- Limited donor funding to date and uncertain future support. Donors have promised over $1.9 billion to the Fund (including commitments made for future years) and paid in over $1.1 billion so far. However, these funding amounts fall far short of the $10 billion or more each year recommended by the World Bank, WHO, and other groups. It remains unclear whether and how this funding gap can be filled as attention to COVID-19 fades, and as donors and health systems face funding constraints and competing priorities. While there appears to be strong demand for Pandemic Fund grants – the first call for proposals generated submissions from more than 100 countries requesting funding totaling over $7 billion – the longer-term sustainability of the Fund remains in question without more financing, and its reliance on the generosity of donors in the coming years places it in a potentially precarious financial situation.
- Approach and ability to catalyze co-financing is unclear. As the Pandemic Fund’s Governance Framework makes clear, a key objective for the mechanism is to use its resources to leverage additional investments for pandemic preparedness and response from philanthropies and the private sector, as well as by country governments. However, only a limited amount of funding has been committed by philanthropies to date, including from the Gates Foundation ($15 million), Wellcome Trust (about $12 million), and Rockefeller Foundation ($15 million), which together comprise around 2 percent of all commitments to the Fund. In addition, it is still unclear how the Fund will “crowd in” additional PPR financing from domestic governments, particularly given the challenging fiscal environments faced by many low and middle income countries. A Board working group recommended against strict co-financing requirements linked to grants but did recommend co-financing be pursued when possible. The first call for proposals includes a set of principles for co-investments, making clear that mobilizing additional government spending is encouraged but not an absolute requirement. While rules and regulations may evolve for future funding rounds, it will be important to observe if and how much co-financing is mobilized in the first round of funding without specific requirements for it, and how successful the Fund can be in crowding in additional funds from other sources.
- Differing views on priorities by geography, activity, income level, and other aspects of project funding. The Fund has to choose how to spend a limited amount of funding across a broad set of potential projects, which could encompass preparedness and response, animal and human health, local and global capacities, early-stage research and last-mile delivery, and more. For its initial round, the Fund has focused on certain country and regional-level technical areas such as laboratory systems and public health workforce, but that leaves out other areas in need of investment. Going forward, decisions to focus in some areas but not others are likely to be contentious. For example, what the right split between funding country-level, regional-level, and global capacities is. Some advocates have argued for setting a specific target such as 70/20/10 across these three levels, respectively, but no hard and fast rule yet applies. In addition, the Board will have to choose how to balance financing across a range of country income levels, and disparate needs.
- Questions about governance processes and ensuring representative decision-making. At less than a year old, many of the Fund’s governance procedures and norms are still being negotiated and developed, but already there are questions about how it will navigate decision-making processes and ensuring equity and representation, such as:
- While some steps have been taken toward inclusive governance such as having civil society and recipient country representation on the Board, as sought by the U.S. and global health advocates, it’s not yet clear the extent to which decision-making will be influenced by these stakeholders as opposed to donor governments. There are the same number of Board seats (nine each) for “Co-investor” and “Contributor” countries plus two seats for civil society, but power imbalances can still exist in such situations in practice. Further, the two civil society representatives (one from the Global North and one from the Global South) have been tasked with representing large, diverse international constituencies, and keeping informed of and adequately representing the full array of issues and concerns of their constituencies is a major challenge.
- Concerns about potential conflicts of interest have also been raised, such as that “Co-investor” countries have a level of influence over funding decisions and also stand to benefit from funding decisions. The Board has been developing a set of guidelines to manage this and other potential conflicts of interest, but it remains to be seen how the Fund rolls out and implements the guidelines, and how robust they turn out to be. As it stands, the Fund’s Operations Manual states all individuals associated with decision-making and/or implementation “must disclose to the Secretariat any actual or potential conflicts of interest…and recuse themselves from decision-making or deliberations in relations to matters where conflicts arise.” Other global health financing mechanisms (including Gavi and Global Fund) have had to navigate this issue to some extent but it will be particularly important for the Fund as it establishes itself, builds trust and seeks legitimacy for its work.
- Ensuring transparency of decision-making and operations for the Fund will be important. Some notable steps toward greater transparency have already been taken, including having the Secretariat organize (occasional) open meetings with external stakeholders such as civil society representatives to provide information and accept input, posting Board meeting minutes detailing decisions and other important information, and creating a website with updated donor funding information, news, and other resources. As the review process for grants begins and funding begins to be awarded, transparency about how decisions are made, along with amounts, recipients, and projects funded, are likely to help maintain trust among interested parties. To this end, the Board released the instrument and scoring approach that will be used by the TAP to rank and score proposals in the first round of funding. It is expected that results from the reviews will be made public to an extent, along with posting and sharing of the Fund’s overall results and outcomes.
- Level of integration and coordination with existing global health and PPR efforts remains to be seen. The Fund was designed to be additive and build upon ongoing PPR and global health efforts. Among its key principles are that it “complements the work of existing institutions” and that it will “serve as an integrator rather than become a new silo that only furthers fragmentation.” One way it seeks to do this is by requiring its funding be channeled through existing institutions (i.e., “Implementing Agencies”) rather than building a new vertical funding structure. The Fund also requires that proposals address how their projects would integrate with and build upon existing plans and PPR frameworks Joint External Evaluations (JEEs), the International Health Regulations (IHR), and country-level National Action Plans for Health Security (NAPHS) or other plans, and proposals must outline how different key actors will coordinate their efforts. Still, as the Fund moves from concept to implementation it will be worth monitoring how effective these principles are and how closely it adheres to this vision. Depending on the focus and scope of projects, countries could have to integrate across many disparate and fragmented actors, including other multilateral efforts, bilateral programs, and overlapping (but potentially separately funded) primary health care, universal health coverage or health system strengthening efforts. Already, this challenge has emerged. The Global Fund, one of the Pandemic Fund’s 13 approved implementing entities, submitted an expression of interest to the Fund, but has since decided not to formally apply for funding in round one, while it continues to assess coordination and synergies between the two organizations.
- Demonstrating impact in the next few years will be important but challenging. As a new entity, the Fund does not yet have a track record it can point to and likely faces a relatively short time window to demonstrate its effectiveness to donors, partners, and communities. Setting ambitious but attainable goals and objectives will be important, especially ones that can be measured, quantified and progress tracked against. To this end, the Fund’s Results Framework outlines monitoring and evaluation requirements for funding recipients, with each implementing agency required to report annually to the Secretariat on progress according to standard metrics like the JEE and SPAR. The Secretariat will then provide an annual, overall results report for the Board. The challenges may come with definitively demonstrating impact, especially if metrics are hard to interpret and/or could take time (perhaps years) to improve. There will be a balance between making quick progress to show donors that funds are having an impact, and allowing enough time for chosen projects to be implemented. In addition, given that the ultimate goal is to help countries prevent epidemics and pandemics, it will be difficult to measure such an effect beyond these intermediary metrics.
- Future U.S. funding for the Pandemic Fund, as well as coordination of this support within the context of existing global health programs, remains to be determined. The future of U.S. funding for the Fund is unknown, as the Biden Administration has so far been able to primarily tap pre-existing funds from COVID-19 emergency appropriations, along with global health security funds. Additional amounts, specifically appropriated by Congress for the Fund, are not a given. In the current period of divided government and budget constraints, in advance of a Presidential election year, it is not clear there is a bipartisan consensus on more U.S. support for the Fund – let alone the $1 billion annually that the White House supports and Congress has authorized for this purpose. Also, given the already long-standing U.S. support for bilateral and multilateral global health efforts such as PEPFAR and the Global Fund, as well as a number of dedicated bilateral global health security programs, it remains to be seen how the U.S. will balance its support for the Pandemic Fund with that for its other programs. Any further U.S. contributions to the new mechanism might come in addition to discretionary funding amounts Congress provides for other U.S. global health programs, potentially leading to tension about the right balance. Further, in places where U.S.-funded global health programs and Pandemic Fund supported projects occur together geographically, U.S. programs might have to consider how best to coordinate and, where appropriate, integrate efforts.