How do States Deliver, Administer, and Integrate Behavioral Health Care? Findings from a Survey of State Medicaid Programs
Issue Brief
Increasing mental health challenges and growing opioid overdose deaths have heightened the focus on behavioral health issues and the need for improved delivery of services. Behavioral health conditions, including mental health and substance use disorders, are particularly prevalent among Medicaid enrollees, with approximately 39% living with such a disorder. Federal initiatives have aimed to increase access by addressing workforce shortages, improving school-based care delivery, and launching and funding crisis services.
Medicaid is the single largest payer of behavioral health services in the country, so state programs can help leverage changes in the system by implementing a range of policies that enhance the delivery, quality, and effectiveness of these services. Despite state and federal efforts to improve accessibility and quality, 35% of Medicaid-covered individuals with significant mental health concerns report not receiving treatment. States maintain flexibility in determining the coverage, delivery, and payment of behavioral health services, leading to variations in these areas.
KFF surveyed state Medicaid officials about behavioral health policies related to administration, delivery systems, integrated care, and data analytics. These questions were part of KFF’s Behavioral Health Survey of state Medicaid programs, fielded as a supplement to the 22nd annual budget survey of Medicaid officials conducted by KFF and Health Management Associates (HMA). A total of 44 states (including the District of Columbia) responded to the survey by December 2022, but response rates varied by question. Further policy context is available in a series of behavioral health briefs that can be accessed in the “Behavioral Health Supplemental Survey” section on this page.
This issue brief utilizes this survey data to answer four key questions:
- How do states administer and finance their behavioral health programs?
- What managed care arrangements do states use to deliver behavioral health care?
- How are states promoting the delivery of integrated behavioral and physical health care?
- How do states monitor behavioral health data?
Behavioral Health Administration and Spending
Medicaid covers a disproportionate share of adults with mental illness and/or SUD (22% vs. 18% of all non-elderly adults). In recent years, state Medicaid and behavioral health authorities are increasingly collaborating to fund, provide oversight, and develop policy for publicly-funded behavioral health services and supports. We asked states to describe the current organizational structure of their Medicaid and behavioral health authorities and to indicate any planned changes to this structure. We also asked states about growth of behavioral health spending in Medicaid.
States’ behavioral health administration structures vary, but in most states Medicaid and behavioral health authorities are different divisions under a single agency (Table 1). Only two states reported that Medicaid and behavioral health authorities were in the same division under a single agency. About one-third of states reported that Medicaid and behavioral health authorities were in separate agencies—either separate cabinet level agencies, separate social service agencies, or separate agencies for each of Medicaid, mental health, and SUD. Three states reported “other” administrative structures.1 While agency structure is not the only approach to coordination, operating Medicaid and behavioral health in a single agency may allow states to foster communication and data-sharing between these authorities. For example, one stated rationale for the 2015 merger of Arizona’s Medicaid and behavioral health authorities was to improve coordination of health care by integrating the management of health services for Medicaid enrollees.
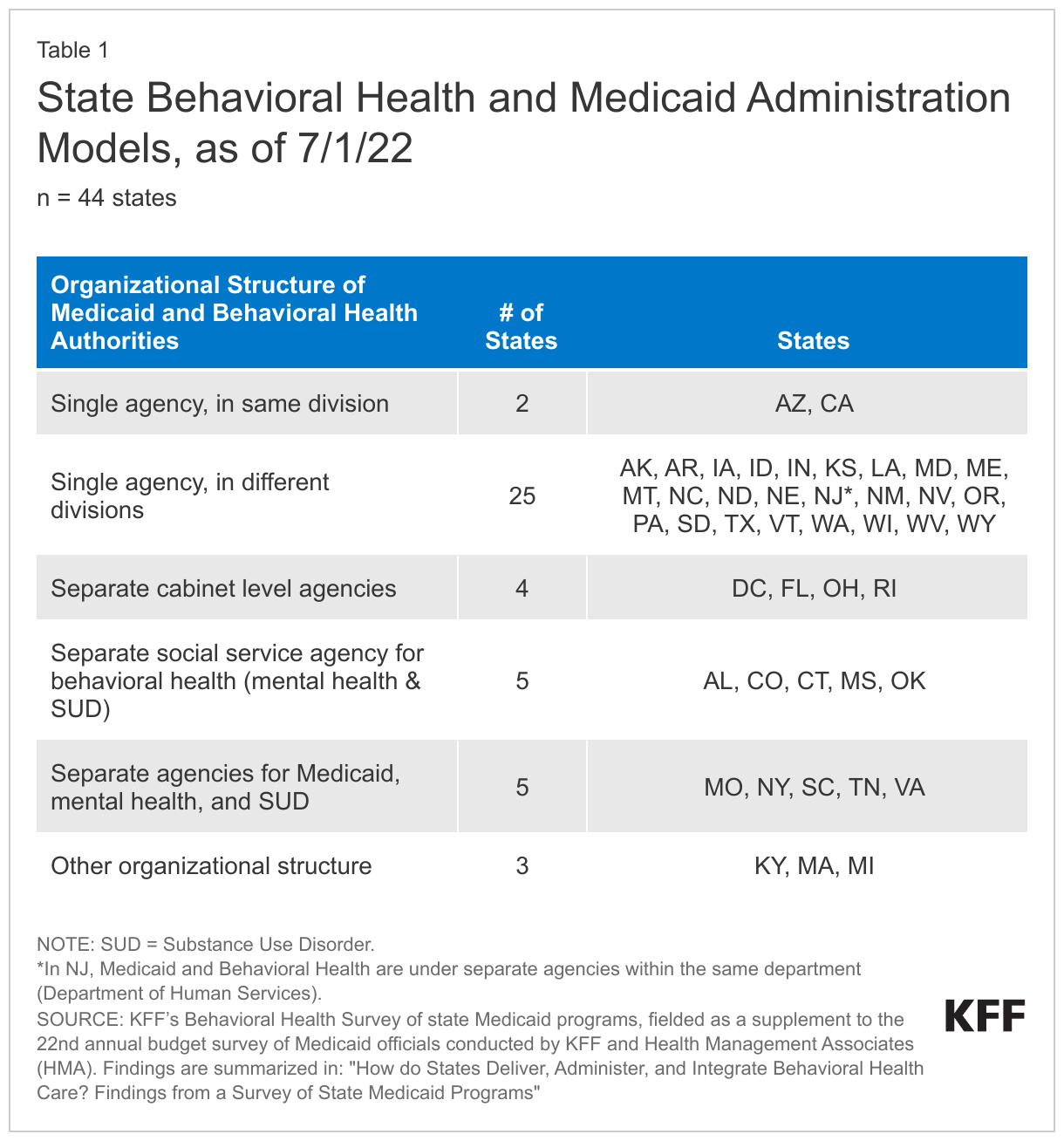
Of the 44 responding states, two reported plans to change the state administrative structure in FY 2023: Iowa reported that its Department of Human Services and Department of Public Health have aligned to form a single Department of Health and Human Services and that behavioral health and Medicaid will both be divisions within this larger agency. Idaho reported plans to transition behavioral health and Medicaid from different divisions under a single agency to a joint division under the agency, and to manage both Medicaid and non-Medicaid behavioral health services through a managed care organization (MCO).
Most states report that Medicaid spending on behavioral health services is growing faster or about the same as overall Medicaid spending growth. In particular, a plurality of responding states (18 of 43) reported faster growth in behavioral health spending, while only four states reported slower growth in behavioral health spending; of the remaining states, seven reported that growth was about the same and fourteen reported they did not know. Reasons reported for faster rates of behavioral health spending included increased utilization and expansion of telehealth, increased utilization of behavioral health services, rate increases for behavioral health services, and new or expanded services or eligibility criteria for those with behavioral health.
Delivery System Models and Managed Care Arrangements for Behavioral Health Services
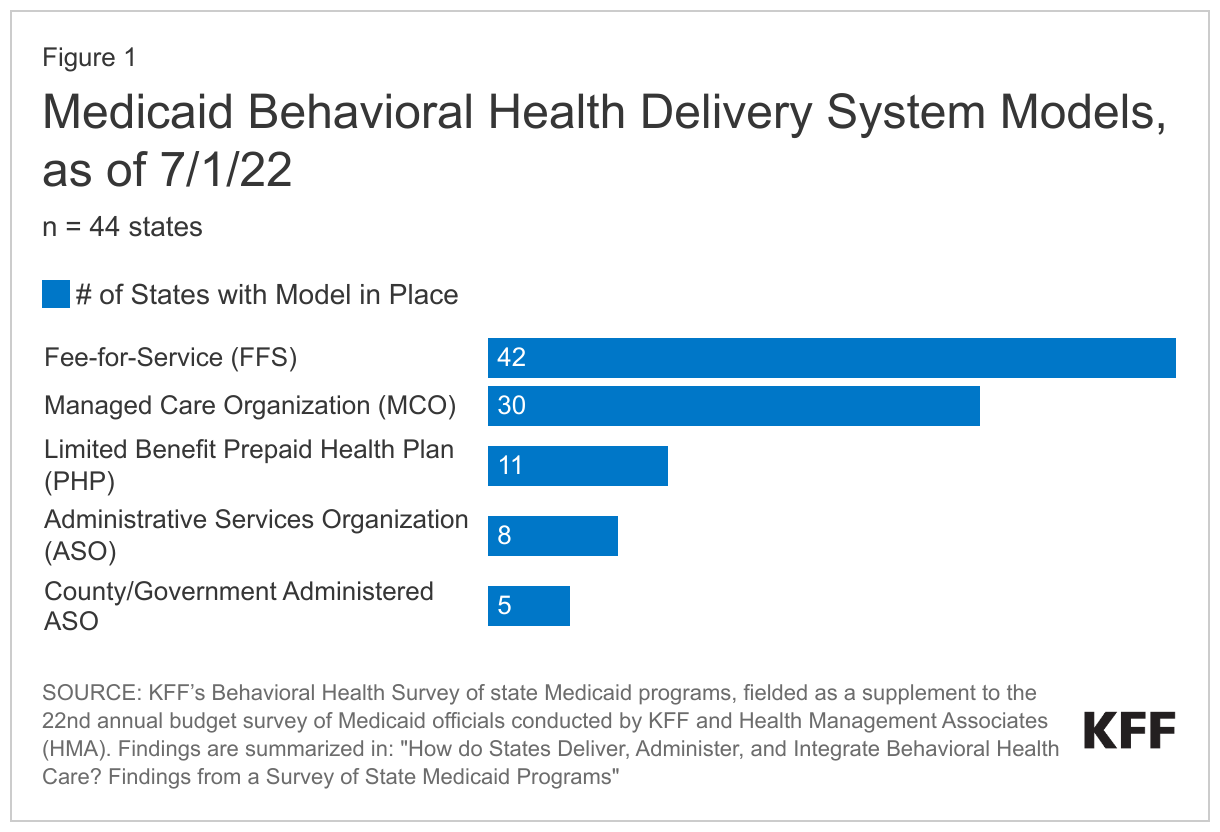
States use a combination of fee-for-service (FFS) and managed care arrangements to deliver behavioral health care to Medicaid beneficiaries, with these services increasingly being provided by managed care organizations (MCOs) in recent years. State movement toward managed care models has included carving behavioral health services into comprehensive, capitated MCO contracts or contracting with risk-based limited benefit prepaid health plans (PHPs). Other states have retained the FFS model but may contract with public or private Administrative Service Organizations (ASOs) to deliver behavioral services on a non-risk basis. We asked states to indicate behavioral health delivery system models in place and, if applicable, to report MCO provision of different behavioral health benefits. We also asked states to report any behavioral health quality incentives in place across delivery system models.
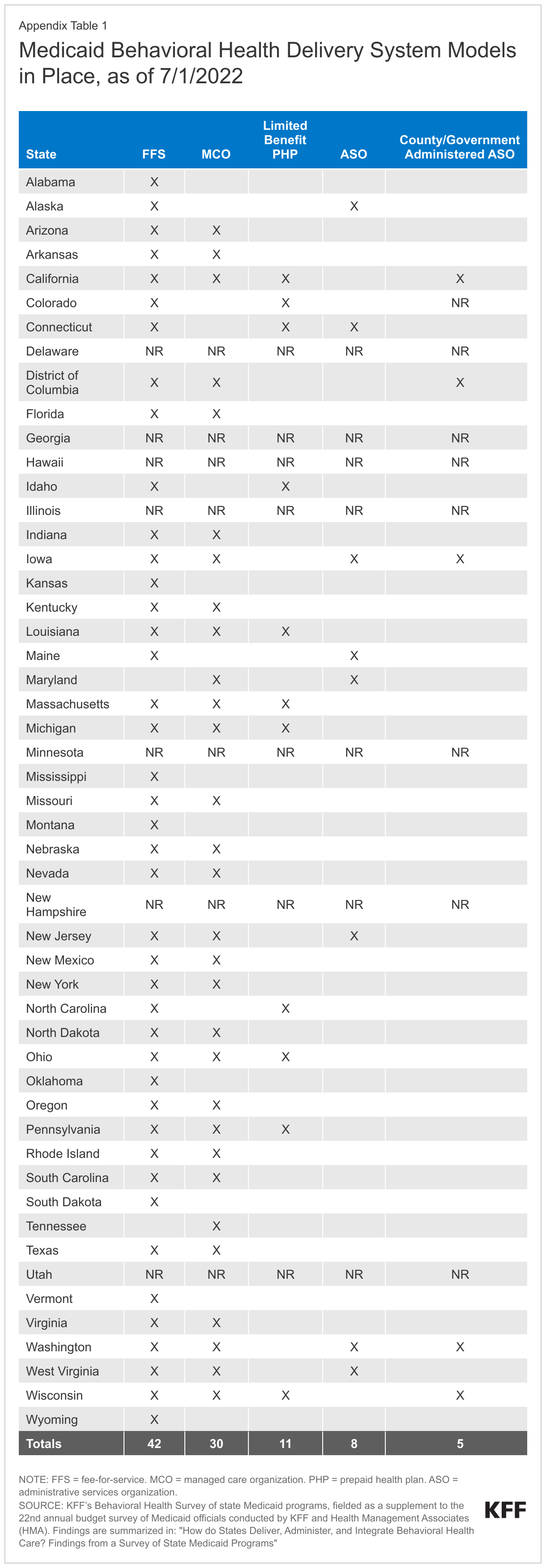
Nearly all responding states had multiple behavioral health delivery system models in place as of July 1, 2022; in particular, most states reported covering behavioral health services under both FFS and through MCOs (Figure 1 and Appendix Table 1). Almost all responding states (42 of 44) reported covering at least some behavioral health services under FFS; of these, 32 states also reported that some behavioral health services were included in a managed care arrangement (MCO and/or PHP). Only two states (Tennessee and Maryland) reported that they did not use any FFS arrangements to cover behavioral health services. Some states with FFS and/or managed care models reported that coverage of behavioral health services also included public or private behavioral health ASOs and/or county or government administered ASOs. While states may use different delivery models for certain behavioral health services, the increased complexity of the behavioral health delivery landscape could complicate access to needed care for enrollees.
Six states reported behavioral health delivery system changes planned for FY 2023:
- Three states (Missouri, North Carolina, and Oklahoma) reported plans to put in place new MCO arrangements for covering behavioral services.
- North Carolina and Arizona reported plans to eliminate their FFS models and transition all behavioral health benefits in to managed care.
- Iowa reported a plan to eliminate its county/government ASO model.
- Ohio implemented a new PHP model on July 1, 2022.
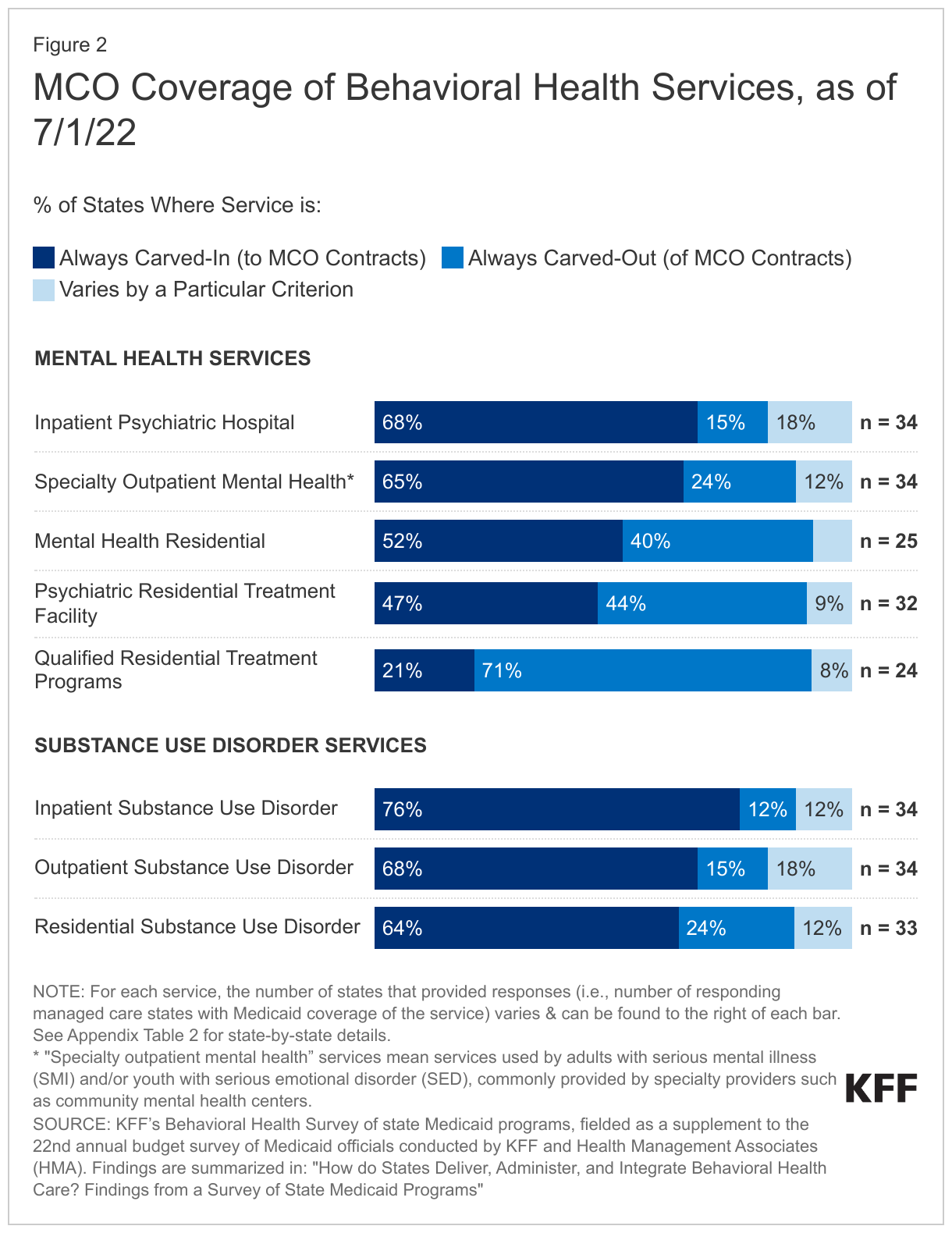
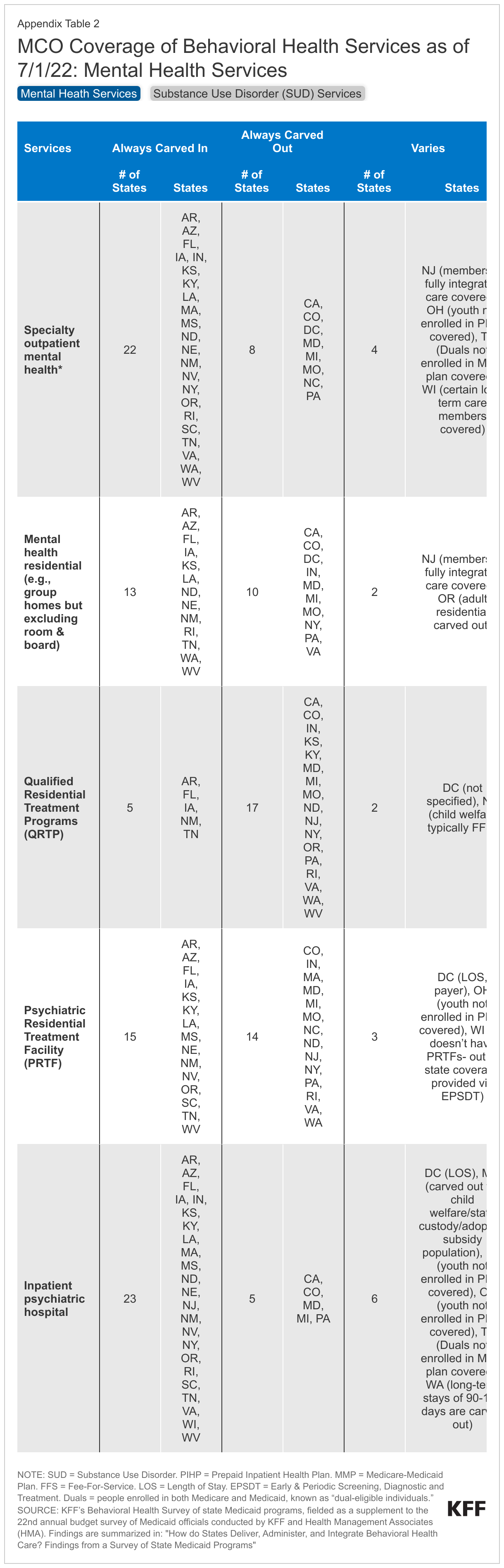
Most states continue to rely on MCOs to administer and manage inpatient and outpatient behavioral health services (Figure 2 and Appendix Table 2). States may carve specific services out of MCO contracts to FFS or PHPs; services frequently carved out include behavioral health, pharmacy, dental, and long-term services and supports (LTSS). However, significant movement has occurred across states to carve these services in to MCO contracts. Consistent with results from past years, the majority of MCO states reported that most specified behavioral health service types were always carved into their MCO contracts (i.e., virtually all services covered by the MCO); fewer states reported that services were always carved out (to PHP or FFS) or that carve-in status varies by geographic or other factors. Qualified Residential Treatment Programs (QRTPs)2 and mental health residential stays were the benefits most frequently carved-out. Some states reported that managed care coverage of specific behavioral health benefits varied by certain criterion, such as carve-outs for certain populations (see Appendix Table 2 for more information).
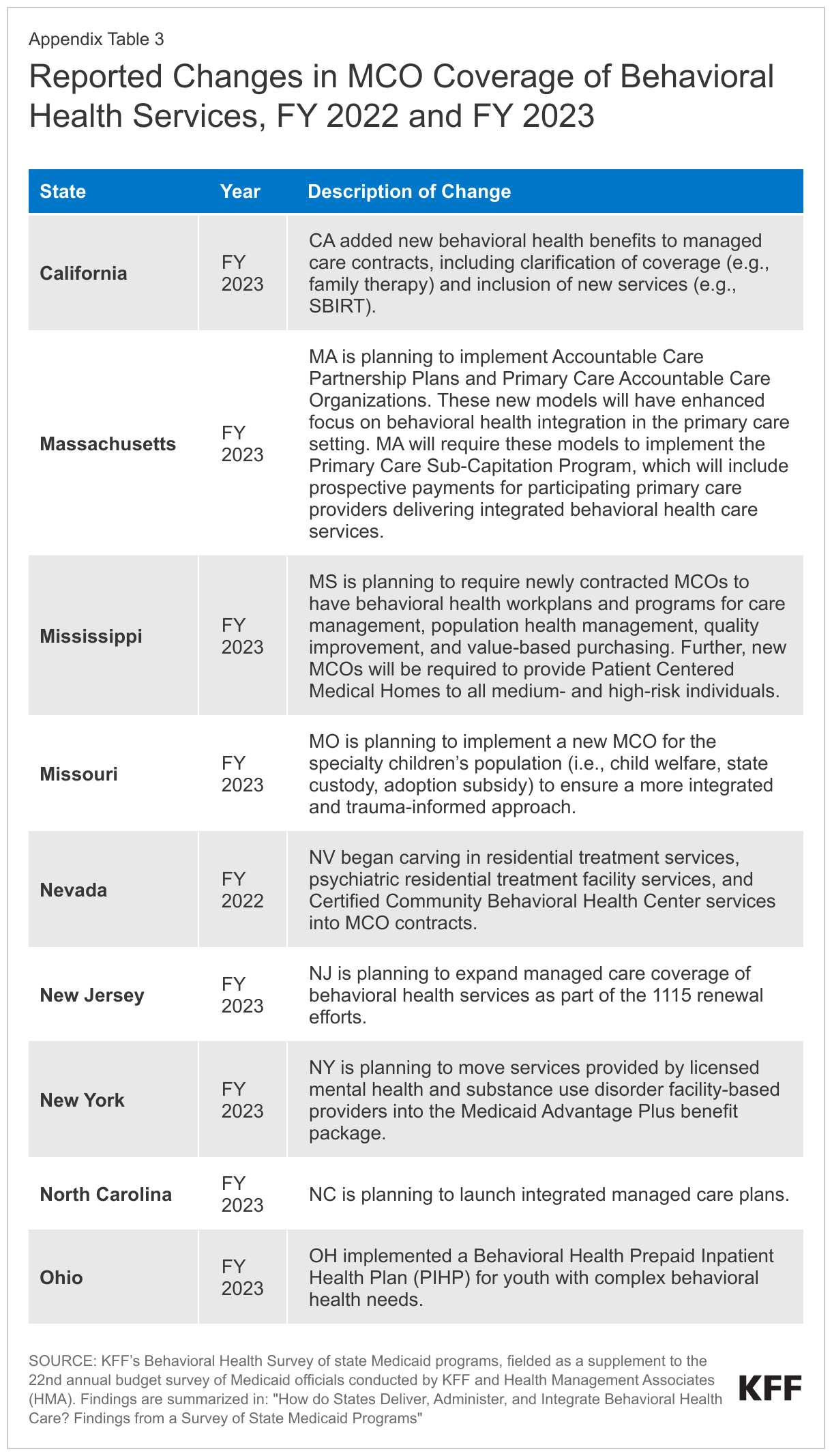
Nine responding states with MCO arrangements for acute care benefits reported changes to how behavioral health benefits were delivered under MCO contracts in FY 2022 or 2023. Changes to contracts fall into a few key policy domains, including:
- Revisions to support behavioral health integration. For example, North Carolina reported plans to launch integrated managed care plans.
- Changes to benefit design or coverage. For example, Ohio implemented a new prepaid inpatient health plan (PIHP) for youth with complex behavioral health needs
- Implementation of new payment models. For example, Massachusetts reported plans to implement prospective payments for participating primary care providers delivering integrated behavioral health care services.
See Appendix Table 3 for additional state-by-state detail on changes in MCO coverage of behavioral health services.
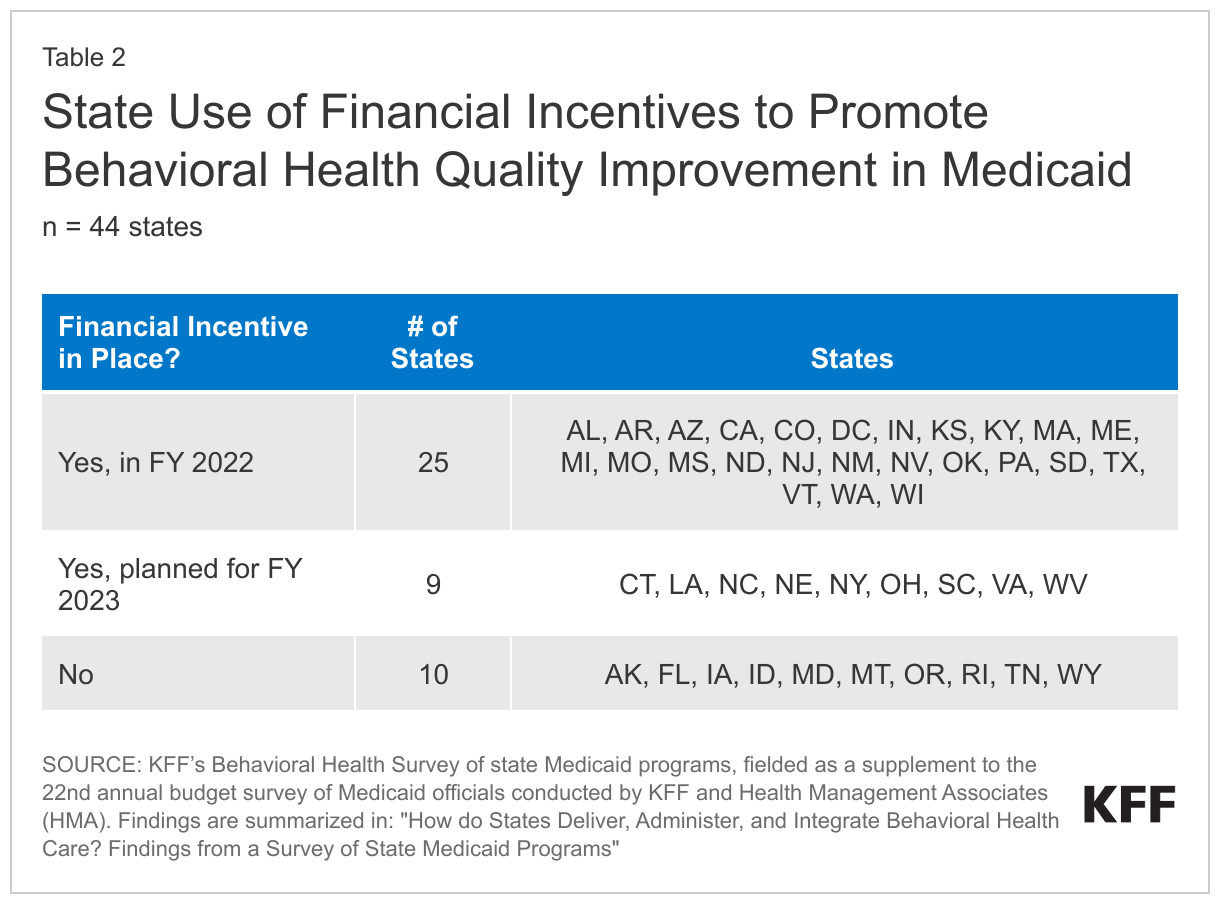
Three-quarters of responding states reported a financial quality incentive in place in FY 2022 or planned for FY 2023 to drive improvements in behavioral health care quality (Table 2). We asked states to report any financial incentives to promote behavioral health quality for MCOs, PHPs, and/or PCCMs or FFS. Of states with financial incentives in place or planned, states most commonly noted that they included behavioral health quality measures in an alternative or value-based payment program. States also reported withholding a percentage of managed care capitation payments or implementing performance bonuses or payments. Some states reported multiple kinds of financial incentives in place or planned. For example, Massachusetts noted that MCOs and Accountable Care Organizations (ACOs) participate in shared savings/losses programs tied to behavioral health quality performance indicators and that psychiatric and substance abuse treatment hospitals have a quality incentive payment structure.
Integrated Care
Many individuals receiving care for behavioral health conditions also have physical health conditions that require medical attention, and the inverse is also true. State Medicaid programs can adopt integrated care policies to address care fragmentation and better integrate physical and behavioral health care, such as by co-locating of both types of care at the same site or removing documentation requirements that may serve as barriers to integration. We asked states about whether they had implemented certain strategies to promote integrated care: Certified Community Behavioral Health Clinics, the psychiatric collaborative care model, and less extensive behavioral health documentation requirements.
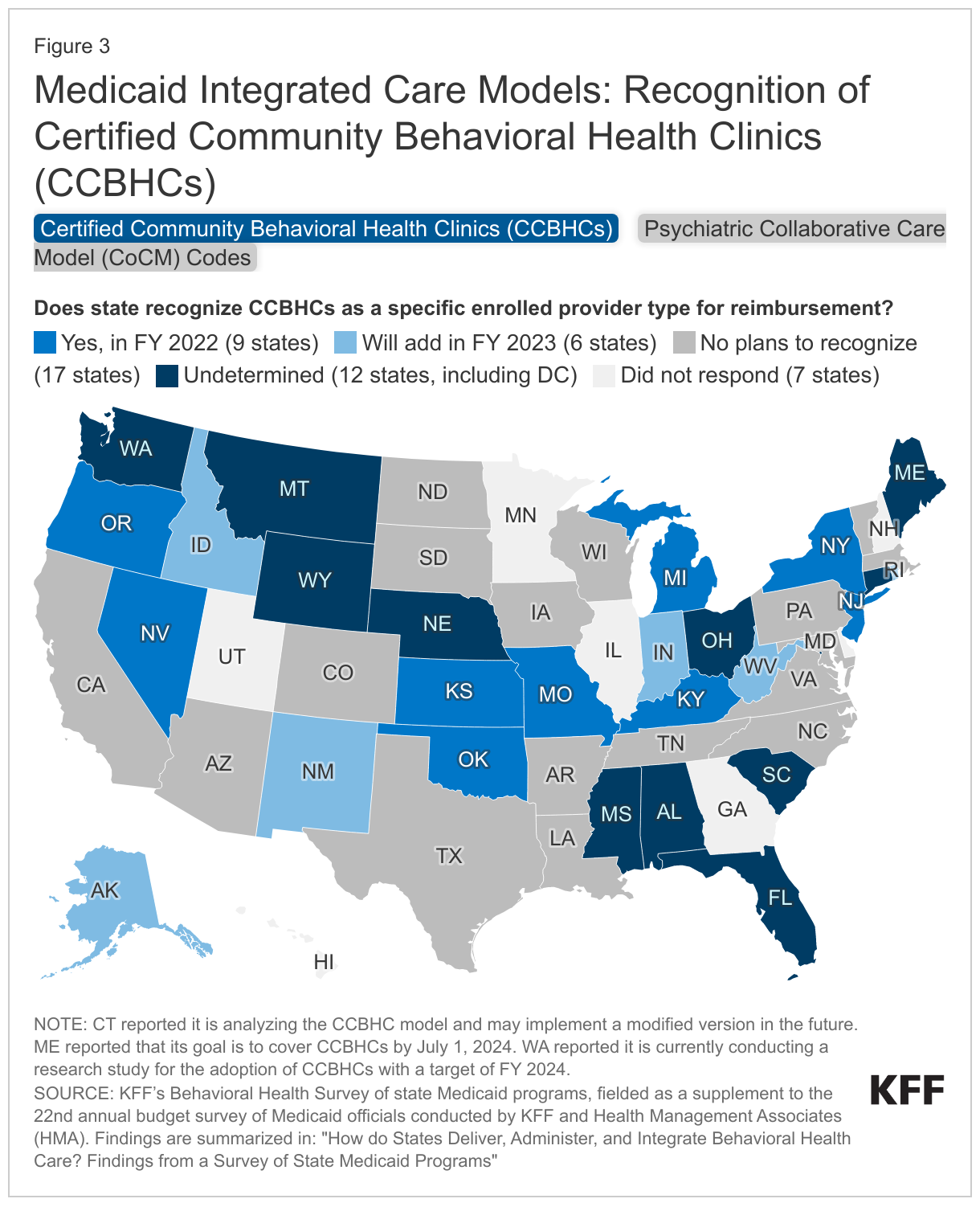
About one-third of responding states reported recognizing Certified Community Behavioral Health Clinics (CCBHCs) as a provider type for reimbursement in FY 2022 or FY 2023 (Figure 3). The CCBHC demonstration, established by Congress in 2014 and expanded in 2022, aims to improve the availability and quality of ambulatory behavioral health services and to provide coordinated care across behavioral and physical health.3 We asked states to report information on CCBHC coverage and experiences:
- CCBHC coverage: Nine states reported that they recognized CCBHCs as a specific enrolled provider type for Medicaid reimbursement in FY 2022, with an additional six states planning to do so in FY 2023. Most of the remaining states (17) reported no plans to recognize CCBHCs in FY 2023, while 12 states were undetermined.4 A few states reported reasons they did not currently plan to recognize CCBHCs, including concerns about payment methodology, budgetary impacts, or that the state had existing providers that served a similar function.
- CCBHC challenges: Among states that do or plan to reimburse CCBHCs, challenges to their adoption included cost efficiency, implementation of payment structure, and workforce challenges.
- CCBHC reimbursement structure: The most commonly reported CCBHC reimbursement methodology was a daily or monthly prospective payment system (PPS) (10 states). A handful of states reported using FFS, outlier/bonus payment, or another methodology.5 Finally, where applicable, states reported a range of approaches to managed care payment requirements for CCBHCs; some states require managed care entities (MCEs) to pay rates set by the state while others allow MCEs to negotiate rates
About one-third of responding states reimbursed psychiatric collaborative care model (CoCM) codes in FY 2022, with many states undetermined as to whether they will open such codes in the future (Figure 3). CoCM is a behavioral health integration model that enhances primary care by adding two services (and providers) to a primary care team: care management for patients receiving behavioral health treatment, and regular psychiatric inter-specialty consultation. CMS has developed specific CPT billing codes for COCM services. Fifteen states reported reimbursing these codes in FY 2022, with two more states planning to reimburse in FY 2023. An additional one-third of states (15) were undetermined about whether to reimburse these codes in the future,6 while the remaining 12 states reported no plans to open these codes.
A small number of states reported promoting integrated care by adopting less extensive documentation requirements for primary care settings as compared to specialty behavioral health settings. Four states reported they had less extensive requirements in place in FY 2022 (Arizona, California, Maryland, and Texas) and one state planned to adopt less extensive requirements in FY 2023 (Arkansas). For example, Arizona formally recognizes accredited patient centered medical homes with behavioral health distinction as meeting documentation requirements without the need for additional auditing and is working to do the same for behavioral health homes.
Behavioral Health Data and Health Information Exchanges
Data on behavioral health utilization can be used to understand areas such as care utilization patterns, access gaps, population trends, and health disparities. Health information exchanges (HIEs) can facilitate communication, which may result in more effective and timely linkages to behavioral health and other care, as well as improved coordination and quality. We asked states about initiatives to encourage and support behavioral health provider participation in HIEs, as well as any challenges encountered. In addition, we asked states whether they collected or analyzed data to better understand behavioral health utilization patterns, needs, or disparities.
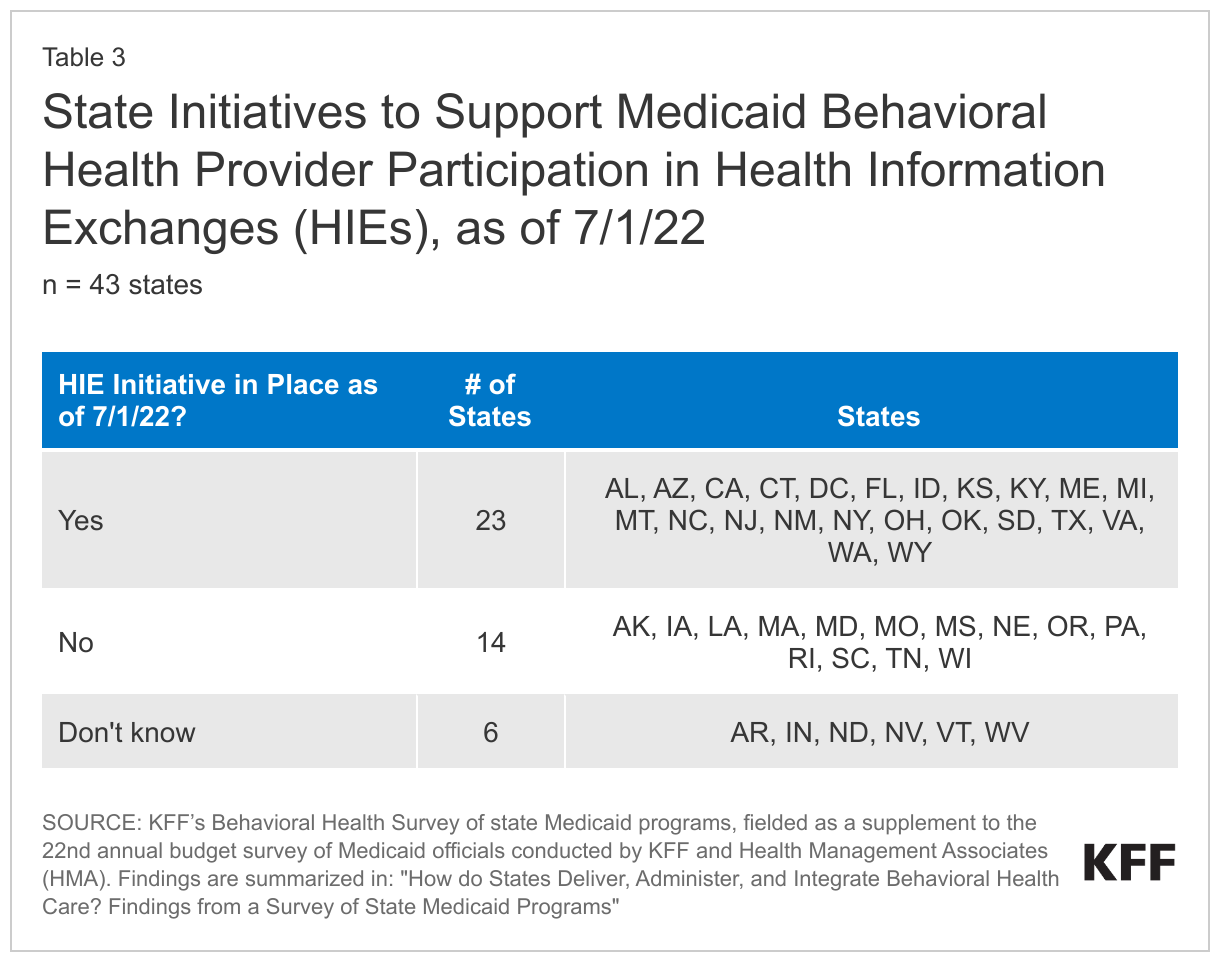
About half of responding states reported a state initiative to encourage or support Medicaid behavioral health provider network participation in health information exchanges (HIEs) (Table 3). Leadership buy-in, financial incentives, infrastructure assistance, and quality incentives are some of the methods states use to encourage behavioral health providers to utilize HIEs. Most states report HIEs are used to manage admission, discharge, and to transfer data during acute care or crisis situations. Behavioral health providers may also utilize HIEs for care coordination, referral services, and in some instances, social services referrals.
States reported that technology limitations, costs, and confidentiality concerns were primary barriers to use of HIEs in behavioral health. Some states point to a lack of trust among behavioral health providers regarding entering sensitive data into the HIE due to concerns about violating enhanced confidentiality requirements for some behavioral health populations. States report several financial barriers that may prevent behavioral health providers from participating in HIE, including limited access to technology, upgrades to existing IT infrastructure, integration costs across data systems, and changes in billing and administrative processes.
Nearly all responding states (40 of 44) reported using state-level data to better understand the needs of Medicaid behavioral health populations. States report analysis of claims data, newly collected data, or other data sources. These include data analyses conducted within state Medicaid agencies, often through demonstrations or waivers, and within MCO contracts.
Looking Ahead
As states continue to expand behavioral health services coverage to close access gaps and address the pandemic's impact on mental health and substance use disorders, they may face continued upward budget pressures in behavioral health services spending due to increased utilization. Improved data quality and access may prompt states and analysts to further examine the complex Medicaid behavioral health delivery system, examining access and outcomes associated with various delivery and financing mechanisms. While states are increasingly adopting integrated care initiatives and making efforts to reduce fragmentation across physical and mental health, behavioral health providers' difficulty participating in health information exchanges may hinder progress.
In addition, current discussions over proposed federal rule changes, such as privacy regulations for people with substance use disorders and telehealth prescribing for controlled substances, may affect how behavioral health systems and providers deliver and coordinate care. Numerous existing and proposed federal initiatives aim to employ strategic policies to enhance the accessibility, quality, and availability of behavioral health care. For example, the Consolidated Appropriations Act (CAA) passed workforce requirements that aim to increase the accessibility and availability of behavioral health care, including requirements for Medicaid provider network directories and funding for new psychiatry residency positions. Finally, recognizing Medicaid’s importance in covering and financing behavioral health care for children, recent legislation has utilized Medicaid as one pathway to expand school-based behavioral health services and additional federal and state efforts in this area are ongoing.
This work was supported in part by Well Being Trust. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
This brief draws on work done under contract with Health Management Associates (HMA) consultants Angela Bergefurd, Gina Eckart, Kathleen Gifford, Roxanne Kennedy, Gina Lasky, and Lauren Niles.
Appendix
Endnotes
- The three states are KY, MA, and MI: KY reported that both the State Medicaid Services (Department for Medicaid Services, DMS) and Behavioral Health (Department for Behavioral Health, Developmental and Intellectual Disabilities, DBHDID) are under the Kentucky Cabinet for Health and Family Services. MA reported that Medicaid and behavioral health were within the same executive office, under different agencies/programs. MI reported that adult behavioral health and Medicaid are in the same administration (the Behavioral and Physical Health and Aging Services Administration) within the Michigan Department of Health and Human Services (MDHHS), while children's behavioral health policy is administered by a separate area of MDHHS. ↩︎
- Qualified residential treatment programs (QRTPs) are child care institutions that provide trauma-informed therapeutic programming designed to address the needs, including clinical needs, of children with serious emotional or behavioral disorders or disturbances. QRTPs may receive federal foster care maintenance payments, but may be subject to the IMD exclusion for federal Medicaid payment. On KFF’s Behavioral Health survey, of 43 states responding, 16 states reported reimbursing for QRTPs in FY 2022 and an additional 5 states planned to add reimbursement in FY 2023. Two states reported a Section 1115 waiver in place to allow coverage of services provided to enrollees in QRTPs that meet IMD criteria, while 5 states planned to seek such a waiver. Of these 5 states, all planned to seek Section 1115 authority to exempt the limitations on lengths of stays under the waiver for foster care children residing in QRTPs. ↩︎
- The Protecting Access to Medicare Act of 2014 established a demonstration program to improve community mental health services by funding planning grants for states to implement Certified Community Behavioral Health Clinics (CCBHCs), and the 2022 Safer Communities Act expanded this program. In addition to setting requirements for CCBHCs, the 2014 Act directed CMS to issue guidance on a prospective payment system for mental health services furnished by CCBHCs to account for the total cost of comprehensive services they provide. The CCBHC demonstration aims to improve the availability and quality of ambulatory behavioral health services and to provide coordinated care across behavioral and physical health. CCBHCs provide nine types of services: crisis mental health services; screening, assessment, and diagnosis; patient-centered treatment planning; outpatient mental health and substance use services; outpatient clinic primary care screening and monitoring; targeted case management; psychiatric rehabilitation; peer support and counselor services and family supports; and intensive, community-based mental health care for members of the armed forces and veterans. CCBHCs may partner with designated collaborating organizations to provide some of these services. ↩︎
- Including CT (which reported it is analyzing the CCBHC model and may implement a modified version in the future), ME (which reported that its goal is to cover CCBHCs by July 1, 2024), and WA (which reported it is currently conducting a research study for the adoption of CCBHCs with a target of FY 2024). ↩︎
- Of the 15 states that reported recognizing CCBHCs in FY 2022 or 2023, 12 provided information on their current CCBHC reimbursement structure(s). Some of these states reported the use of multiple reimbursement strategies. PPS methodologies: On May 20, 2015, the Centers for Medicare and Medicaid Services (CMS) issued guidance to states specific to the development of a PPS to be tested under the Section 223 Demonstration Program for CCBHCs, and required in Section 223 of the Protecting Access to Medicare Act of 2014. CMS released proposed updates to that CCBHC PPS Guidance in May 2023 to coincide with an additional round of state CCBHC grantees. CMS developed two PPS methodologies for reimbursing CCBHCs: one that pays a fixed daily rate for all service rendered to a Medicaid enrollee (similar to the methodology used by Federally Qualified Health Centers) and one that pays a fixed monthly rate. 8 states reported using the daily PPS model (ID, KS, KY, MI, MO, NV, NY, and OR) and 2 states reported a monthly PPS model (NJ and OK). Other methodologies: 3 states reported using FFS (NJ, NM, and NV), 3 states reported using outlier or bonus payments (MI, NJ, and NV), and 2 states reported using another methodology (AK reported that CCBHs are grant-funded; NY reported using a PPS methodology but carved out of managed care and paid using a CCBHC-specific code with a provider-specific rate based on each agency's total cost of operations divided by total visits). ↩︎
- Including SC, which reported that it intended to cover these codes and hoped to do so in FY 2023, but a firm date had not been established. ↩︎