Key Facts on Health Coverage of Immigrants
Editorial Note
This brief was updated on June 12, 2026 to include additional details on fully state-funded coverage in Washington.
Summary
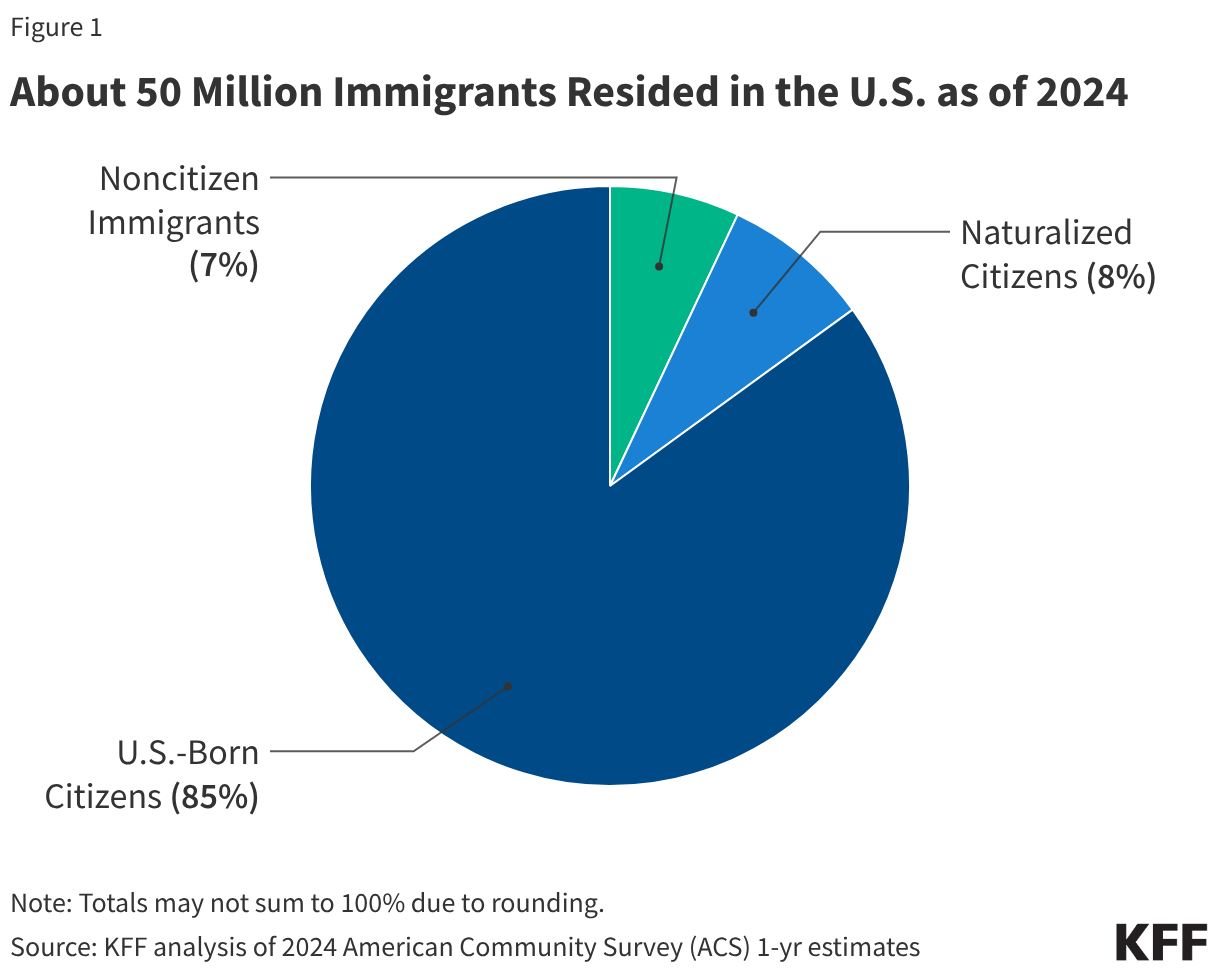
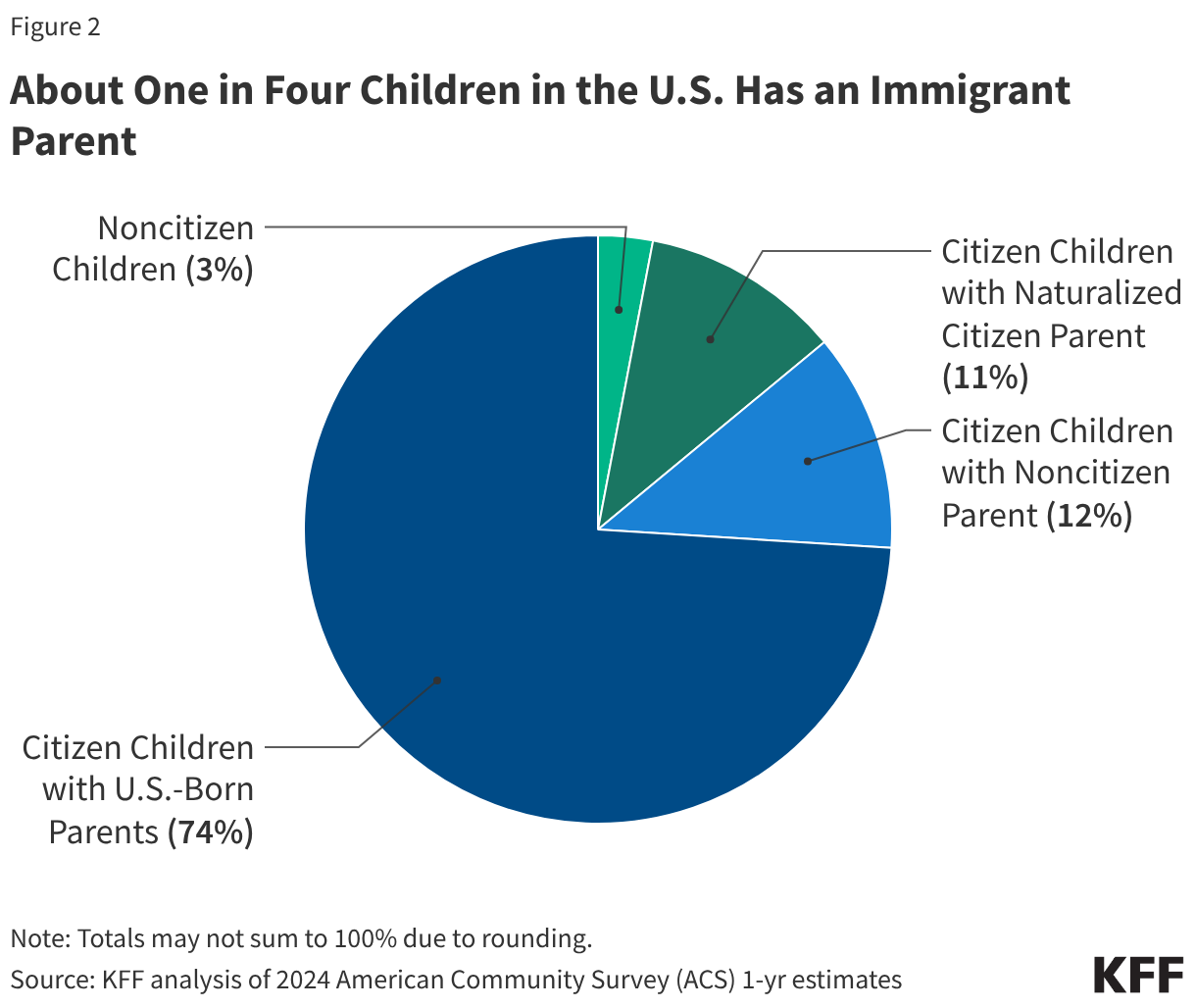
As of 2024, there were about 50 million immigrants residing in the U.S., including 24 million noncitizen immigrants and 26 million naturalized citizens, who each accounted for about 7% and 8% of the total population, respectively. Noncitizens include lawfully present and undocumented immigrants. Many individuals live in mixed immigration status families that may include lawfully present immigrants, undocumented immigrants, and/or citizens. One in four (26%) children has an immigrant parent, including over one in ten (12%) who are citizen children with at least one noncitizen parent.
This fact sheet provides an overview of health coverage for immigrants based on data from the KFF/New York Times 2025 Survey of Immigrants and discusses implications of the current policy and immigration enforcement environment for their health and health care. It shows:
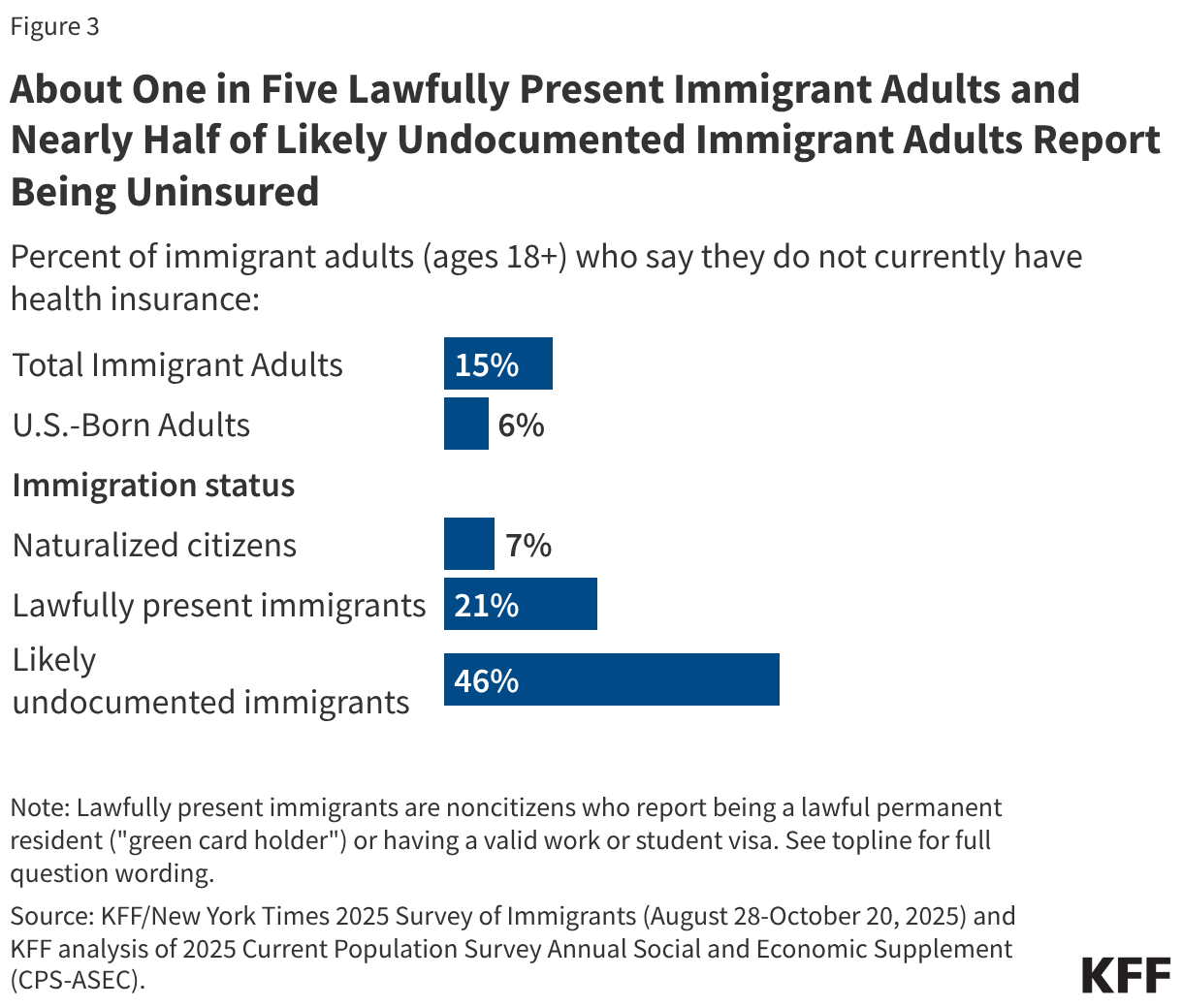
- Although the majority of uninsured people are citizens, noncitizen immigrant adults, particularly likely undocumented immigrants, are significantly more likely to report being uninsured than citizens. As of 2025, almost half (46%) of likely undocumented immigrant adults and one in five (21%) lawfully present immigrant adults reported being uninsured compared to less than one in ten naturalized citizen (7%) and U.S.-born citizen (6%) adults. These higher uninsured rates reflect a combination of more limited access to private coverage due to working in jobs less likely to offer health coverage and exclusions and limitations on eligibility for federally funded coverage options, including Medicaid, Affordable Care Act (ACA) Marketplace, and Medicare coverage.
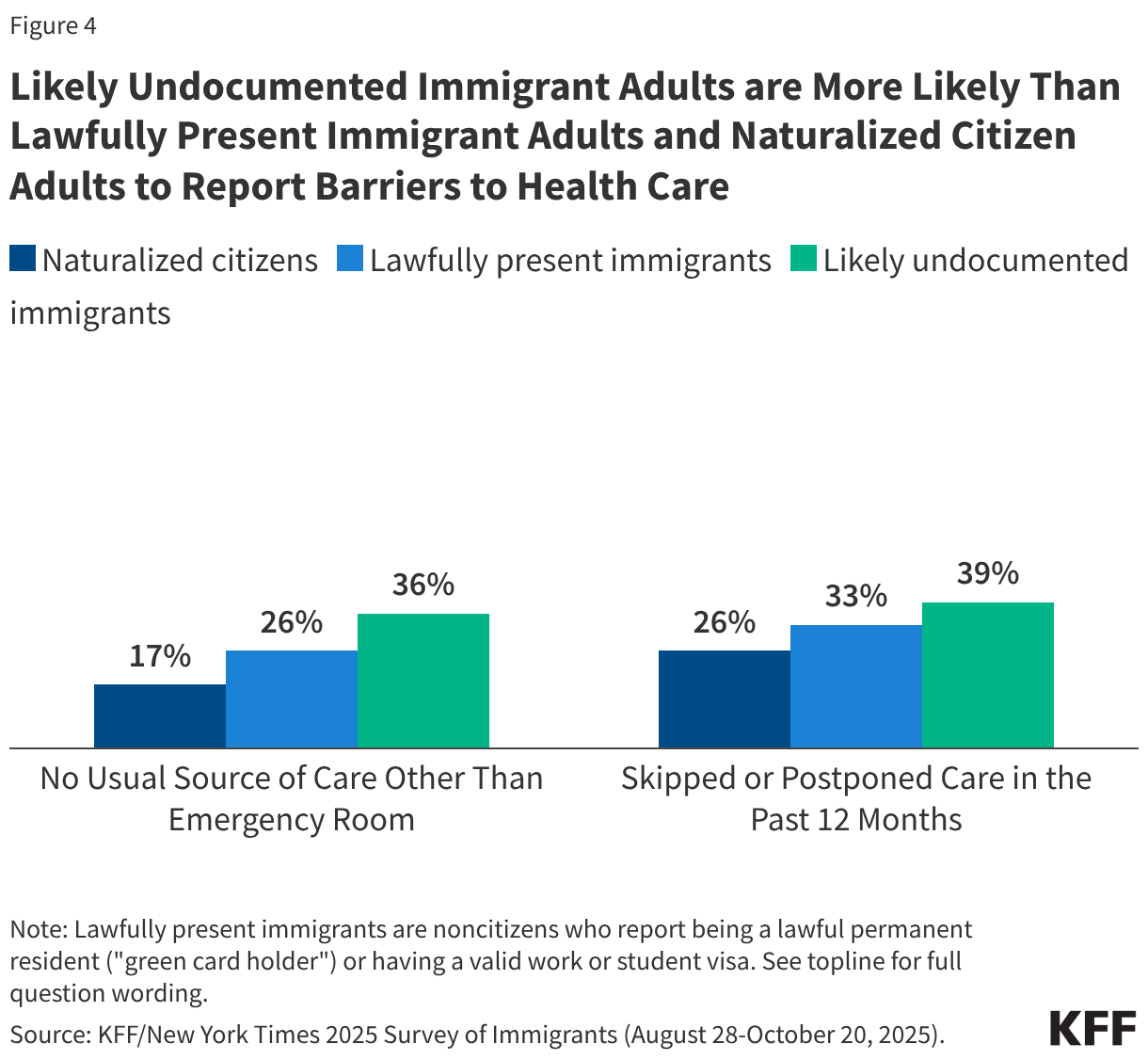
- Reflecting their higher uninsured rate, noncitizen immigrants are more likely than citizens to report barriers to accessing health care and skipping or postponing care. Immigrants have lower health care expenditures than their U.S.-born counterparts reflecting lower use of care due to a combination of them being younger and healthier and facing more barriers to accessing care.
- Some states have expanded access to health coverage for immigrants through Medicaid options for lawfully residing immigrant children and pregnant people and fully state-funded programs, but some states have rolled back this coverage since 2025.
- Recent policy changes will further restrict lawfully present immigrants’ access to health coverage, and immigrants across all statuses have become more fearful about accessing health coverage and care due to increased immigration enforcement actions under the Trump Administration.
Overview of Immigrants
Based on federal survey data, as of 2024, there were about 50 million immigrants residing in the U.S., including 24 million noncitizen immigrants and 26 million naturalized citizens, who each accounted for about 7% and 8% of the total population, respectively (Figure 1). More recent estimates show that the number of immigrants in the U.S. has since been declining, with the population declining by about 1.4 million immigrants between January 2025 and June 2025. KFF estimates for this analysis are based on the American Community Survey, the latest year of data for which is 2024, and thereby don’t reflect population changes since 2025. Estimates suggest that about half of noncitizens were lawfully present immigrants, such as lawful permanent residents (“green card” holders) and those with a valid work or student visa, while the remaining half were undocumented immigrants, who may include individuals who entered the country without authorization, individuals who entered the country lawfully and stayed after their visa or status expired, or individuals who lost their lawful status due to recent policy changes like immigrants with temporary protected status (TPS) from certain countries.1 The underlying estimates used in this analysis also include some immigrants with temporary deportation protections in the undocumented immigrant population. Many individuals live in mixed immigration status families that may include lawfully present immigrants, undocumented immigrants, and/or citizens. Close to 20 million, or one in four (26%), children living in the U.S. had an immigrant parent as of 2024, and the majority of these children were citizens (Figure 2). About 9 million, or 12%, were citizen children with at least one noncitizen parent.
Uninsured Rates by Immigration Status
The KFF/New York Times 2025 Survey of Immigrants, a nationally representative survey of immigrants, provides data on health coverage of immigrant adults and experiences accessing health care, including by immigration status.
Although the majority of uninsured people are citizens, noncitizen immigrant adults, particularly likely undocumented immigrants, are significantly more likely to report being uninsured than citizens. As of 2025, almost half (46%) of likely undocumented immigrant adults and one in five (21%) lawfully present immigrant adults reported being uninsured compared to less than one in ten naturalized citizen (7%) and U.S.-born citizen (6%) adults (Figure 3).
Reflecting their higher uninsured rates, noncitizen immigrants, especially those who are likely undocumented, are more likely than citizens to report barriers to accessing health care and skipping or postponing care. Research shows that having insurance makes a difference in whether and when people access needed care. Those who are uninsured often delay or go without needed care, which can lead to worse health outcomes over the long-term that may ultimately be more complex and expensive to treat. Overall, likely undocumented immigrant adults are more likely than lawfully present immigrant adults and naturalized citizen adults to report not having a usual source of care other than an emergency room and skipping or postponing care in the past 12 months (Figure 4).
Research also shows that immigrants have lower health care use and expenditures than their U.S.-born counterparts and help to subsidize health care for U.S.-born citizens. Overall, research shows that immigrants, including lawfully present and undocumented immigrants, use less health care than U.S.-born citizens. Lower use of health care among immigrants likely reflects a combination of them being younger and healthier than their U.S.-born counterparts as well as them facing increased barriers to care including a higher uninsured rate, language access challenges, confusion, and immigration-related fears. Reflecting their lower use of health care, immigrants have lower health care expenditures than their U.S.-born counterparts. 2023 Medical Expenditure Panel Survey data show that, on average, annual per capita health care expenditures for immigrants are about 30% lower than those for U.S.-born citizens ($5,453 vs. $7,838).2 Research further finds that, because immigrants, especially undocumented immigrants, have lower health care use despite contributing billions of dollars in insurance premiums and taxes, they help subsidize the U.S. health care system and offset the costs of care incurred by U.S.-born citizens.
Access to Health Coverage Among Immigrants
Private Coverage
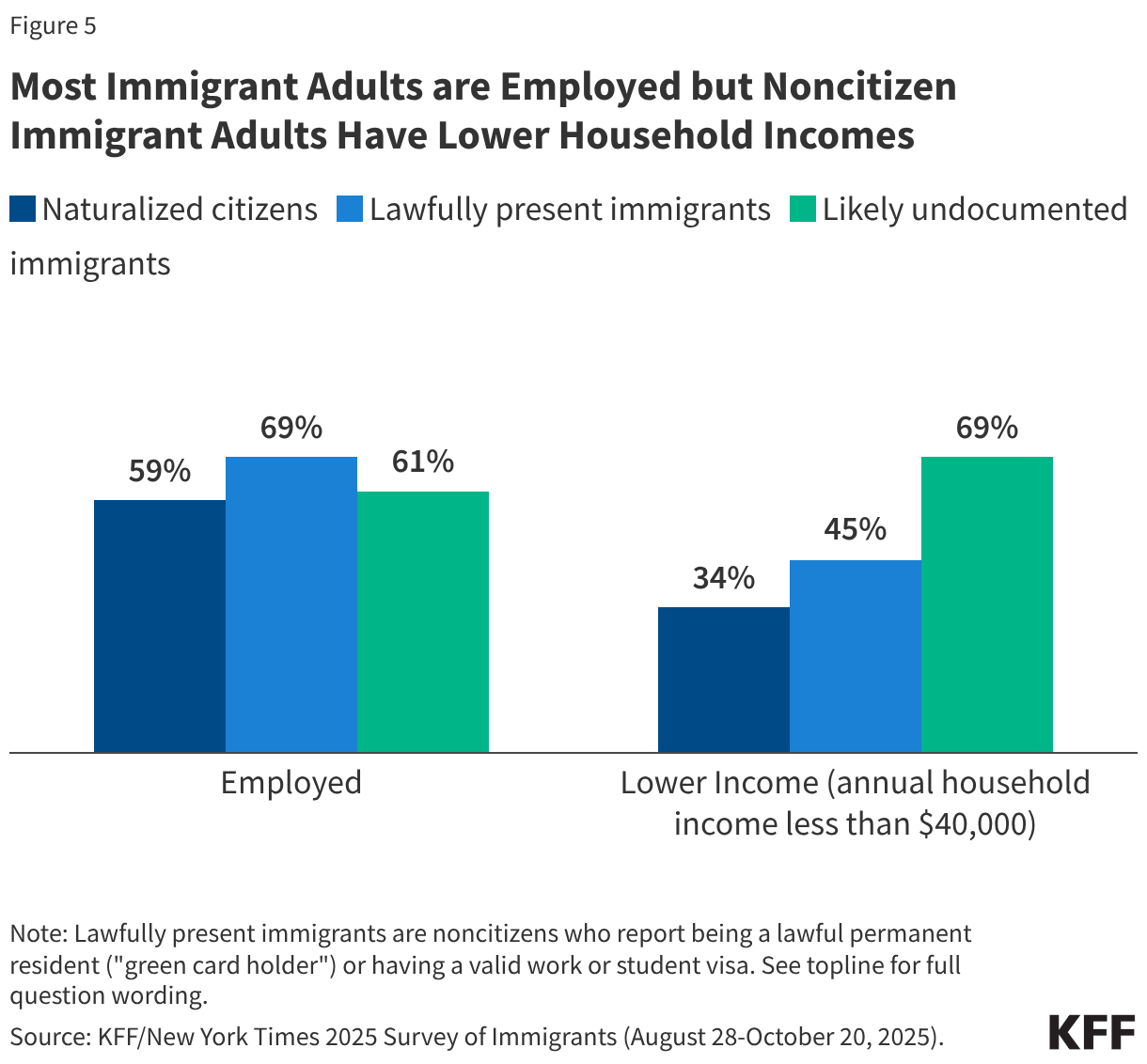
Despite high rates of employment, noncitizen immigrants have limited access to employer-sponsored coverage. Although most noncitizen immigrant adults report being employed, they are significantly more likely than citizens to report being lower income (household income less than $40,000) (Figure 5). This pattern reflects disproportionate employment of noncitizen immigrants in low-wage jobs and industries that are less likely to offer employer-sponsored coverage. Given their lower incomes, noncitizen immigrants also face challenges affording employer-sponsored coverage when it is available or through the individual market.
Federally Funded Coverage
Some lawfully present immigrants may qualify for Medicaid and the Children’s Health Insurance Program (CHIP) subject to eligibility restrictions. Prior to the 2025 reconciliation law, lawfully present immigrants who have a “qualified” immigration status have been eligible for Medicaid or CHIP if they meet other eligibility requirements such as income. Qualified immigrants are a subset of lawfully present immigrants and generally include lawful permanent residents, refugees, asylees, survivors of trafficking, Compact of Free Association (COFA) migrants, Cuban/Haitian entrants, members of federally recognized tribes, and some parolees (Appendix A). Many immigrants with qualified status, including most lawful permanent residents or “green card” holders, must wait five years after obtaining qualified status before they may enroll. Some immigrants with qualified status, such as refugees and asylees, as well as citizens of COFA nations, do not have to wait five years before enrolling. Some immigrants, such as those with temporary protected status, are lawfully present but do not have a qualified status and are not eligible to enroll in Medicaid or CHIP regardless of their length of time in the country (Appendix A). Once changes in the 2025 reconciliation law go into effect, fewer qualified immigrants will be eligible for Medicaid and CHIP (see below).
For children and pregnant people, states can eliminate the five-year wait and extend coverage to some lawfully present immigrants without a qualified status. As of April 2026, 38 states, including DC, have taken up this option for children and 32 states, including DC, have elected the option for pregnant individuals. A total of 25 states, including DC, have also extended coverage to pregnant people regardless of immigration status through the CHIP From-Conception-to-End-of-Pregnancy (FCEP) option. States have the option in CHIP to provide prenatal care and pregnancy related benefits to eligible low-income children beginning from conception to end of pregnancy regardless of their parent’s citizenship or immigration status. While other pregnancy-related coverage in Medicaid and CHIP requires 60 days of postpartum coverage, the CHIP FCEP option does not include this coverage. However, some states that took up this option provide postpartum coverage through a CHIP health services initiative or using state-only funding. Eleven of the states that have implemented the FCEP option (California, Colorado, Connecticut, Illinois, Maine, Massachusetts, Minnesota, New York, Oregon, Rhode Island, and Washington) have used state funding or CHIP health services initiatives to extend postpartum coverage to 12 months to align with the Medicaid extension established by the American Rescue Plan Act. Maryland extends coverage for four months postpartum, and Alabama, Texas, Virginia, and DC extend coverage for 60 days postpartum using CHIP health services initiatives.
Lawfully present immigrants can purchase coverage through the ACA Marketplace and, like citizens, may receive tax credits to help pay for premiums and cost sharing that vary on a sliding scale based on income. Generally, these tax credits are available to people with incomes starting from 100% of the federal poverty level (FPL) who are not eligible for other affordable coverage. In addition, lawfully present immigrants with incomes below 100% FPL had been eligible to receive tax credits if they were ineligible for Medicaid based on immigration status, for example due to being in the five-year waiting period for Medicaid or CHIP or because they did not have a “qualified” status. However, this coverage was eliminated effective January 1, 2026, under the 2025 reconciliation law (see below).
Individuals with Deferred Action for Childhood Arrivals (DACA) status are not considered lawfully present for purposes of health coverage eligibility and remain ineligible despite having a deferred action status, which is otherwise considered a lawfully present status. The Biden administration published regulations in 2024 that changed the definition of lawfully present to include DACA recipients for purposes of eligibility to purchase coverage through the ACA Marketplace and to receive tax credits to help pay for premiums and cost sharing, but this change faced legal challenges. The Trump administration published regulations in June 2025 that once again made DACA recipients in all states and DC ineligible for ACA Marketplace coverage. Most states terminated coverage for enrolled DACA recipients on September 30, 2025.
Lawfully present immigrants also can qualify for Medicare subject to certain restrictions. Specifically, lawfully present immigrants must have sufficient work history to qualify for premium-free Medicare Part A. If they do not have sufficient work history, they may qualify if they are lawful permanent residents and have resided in the U.S. for five years immediately prior to enrolling in Medicare, although they must pay premiums to enroll in Part A. Once changes in the 2025 reconciliation law go into effect, fewer lawfully present immigrants will be eligible for Medicare (see below).
Undocumented immigrants are not eligible to enroll in federally funded coverage including Medicaid, CHIP, or Medicare or to purchase coverage through the ACA Marketplaces. Medicaid payments for emergency services may be made to hospitals on behalf of individuals who are otherwise eligible for Medicaid but for their immigration status. These include lawfully present immigrants who are subject to a five-year waiting period for Medicaid, lawfully present immigrants who are not eligible for Medicaid, and undocumented immigrants. These payments may help cover the costs for emergency care provided to immigrants who remain ineligible for Medicaid but are not coverage for individuals. Much of Emergency Medicaid spending goes towards labor and delivery costs and Emergency Medicaid spending represented less than 1% of total Medicaid spending in fiscal year 2023.
Eligibility Restrictions for Immigrants Under the 2025 Reconciliation Law
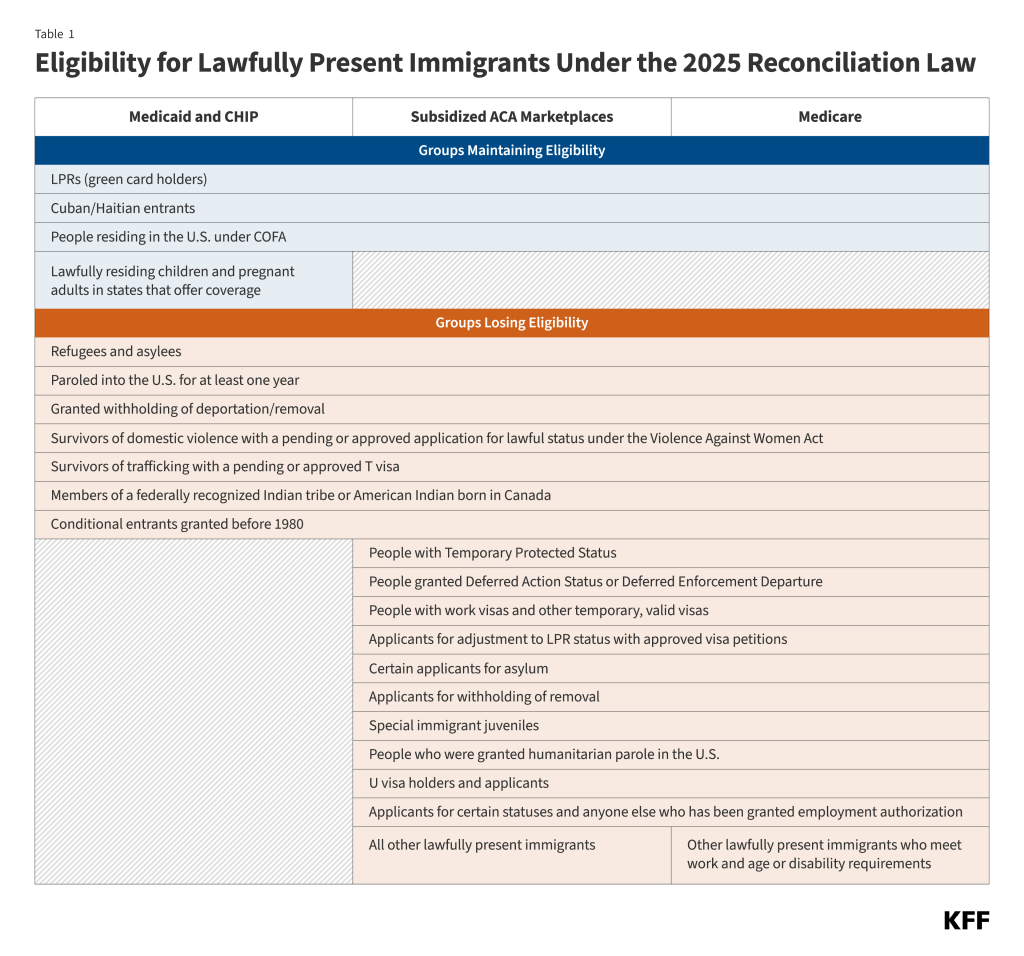
The 2025 reconciliation law will further limit the groups of lawfully present immigrants who may qualify for federally funded coverage, including Medicaid and CHIP, the ACA Marketplace, and Medicare. Specifically, effective October 1, 2026, Medicaid and CHIP eligibility will be limited to lawful permanent residents (LPRs or “green card” holders), Cuban and Haitian entrants, people residing in the U.S. under COFA, and lawfully residing children and pregnant immigrants in states that cover them under the Medicaid and/or CHIP option (Table 1). This will result in some groups of lawfully present immigrants losing eligibility, including refugees and asylees without green cards. The law also eliminates ACA Marketplace coverage for lawfully present immigrants with incomes less than 100% FPL effective January 1, 2026, and limits subsidized ACA Marketplace coverage to lawfully present immigrants who are LPRs, Cuban and Haitian entrants, and people residing in the U.S. under COFA beginning January 1, 2027. As a result, a broader group of lawfully present immigrants will lose access to subsidized Marketplace coverage, including refugees and asylees without green cards, people with TPS, and individuals on work visas, among others. Medicare eligibility also will be limited to lawfully present immigrants who are LPRs, Cuban and Haitian entrants, and people residing in the U.S. under COFA, eliminating eligibility for similar groups. Current beneficiaries subject to the new restrictions will lose coverage no later than 18 months from the enactment of the legislation (January 4, 2027).
The Congressional Budget Office (CBO) estimates that the health coverage eligibility restrictions for lawfully present immigrants in the 2025 reconciliation law will result in 1.4 million lawfully present immigrants becoming uninsured by 2034. This includes 100,000 who will lose coverage due to eligibility restrictions for Medicaid and CHIP, 1.2 million who will lose coverage due to eligibility restrictions for ACA Marketplace coverage, and another 100,000 who will lose coverage due to eligibility restrictions in Medicare by 2034. The CBO also estimates that these coverage restrictions will result in $131 billion in reduced federal spending and $4.8 billion in increased federal revenues by 2034.
State-Funded Coverage
Some states have established fully state-funded programs to provide health coverage to some groups of low-income immigrants who remain ineligible for federally funded coverage options. This coverage is sometimes limited to certain groups, such as children, and varies in scope. While some programs offer benefits similar to Medicaid coverage, these programs are separate state programs that are not part of the Medicaid program. Several states have recently scaled back their state-funded coverage due to budget pressures.
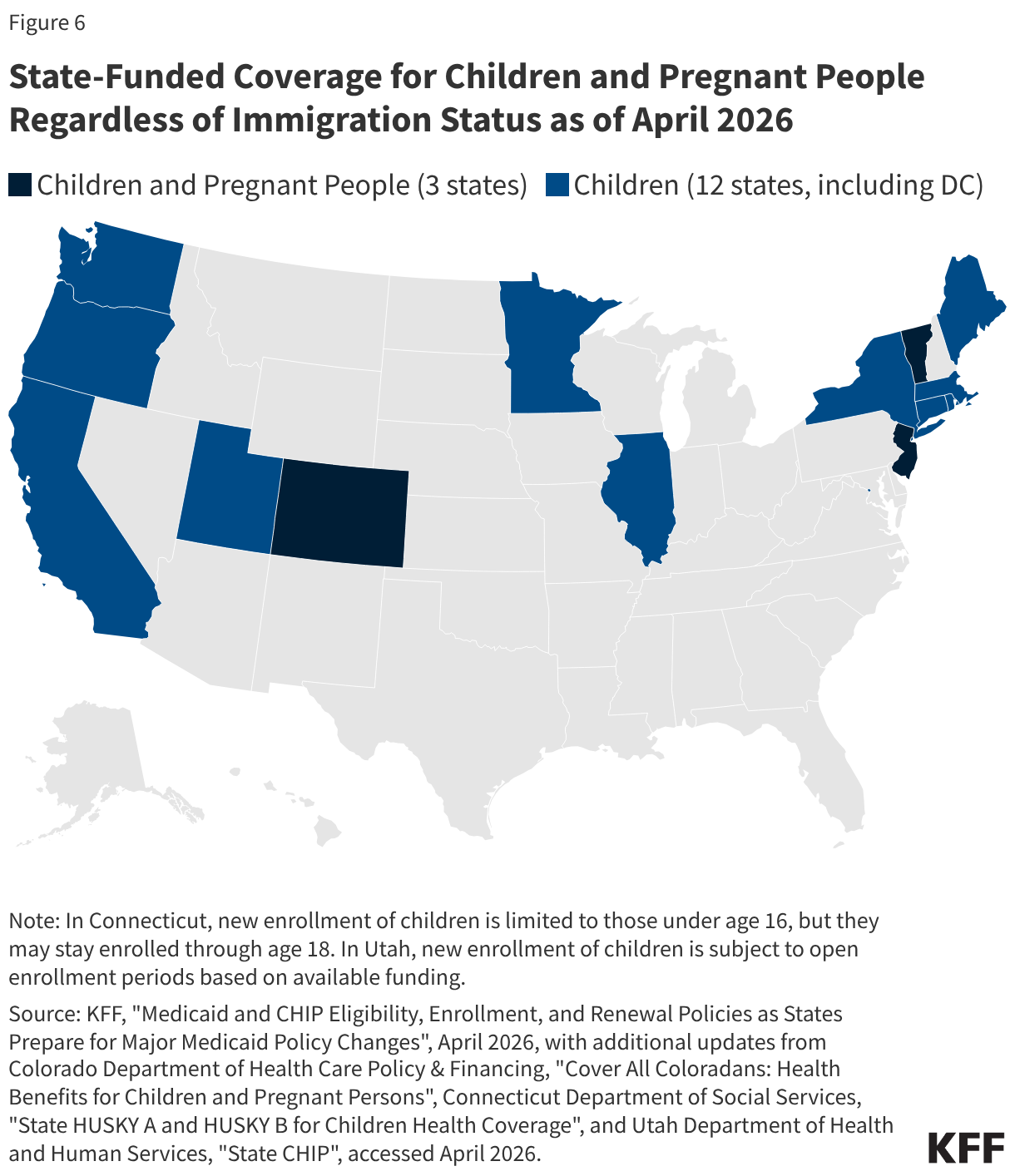
As of April 2026, 15 states, including DC, provide comprehensive state-funded coverage to children regardless of immigration status, with one state (Colorado) planning to scale back coverage due to budget pressures (Figure 6). These states include California, Colorado, Connecticut, Illinois, Maine, Massachusetts, Minnesota, New Jersey, New York, Oregon, Rhode Island, Utah, Vermont, Washington, and DC. Three of these states (Colorado, New Jersey, and Vermont) also provide state-funded coverage to income-eligible pregnant people regardless of immigration status, with Vermont extending this coverage for 12 months postpartum. Colorado plans to implement rollbacks to their state-funded coverage program for children and pregnant people, including capping enrollment and limiting certain benefits, starting January 2027 due to funding constraints.
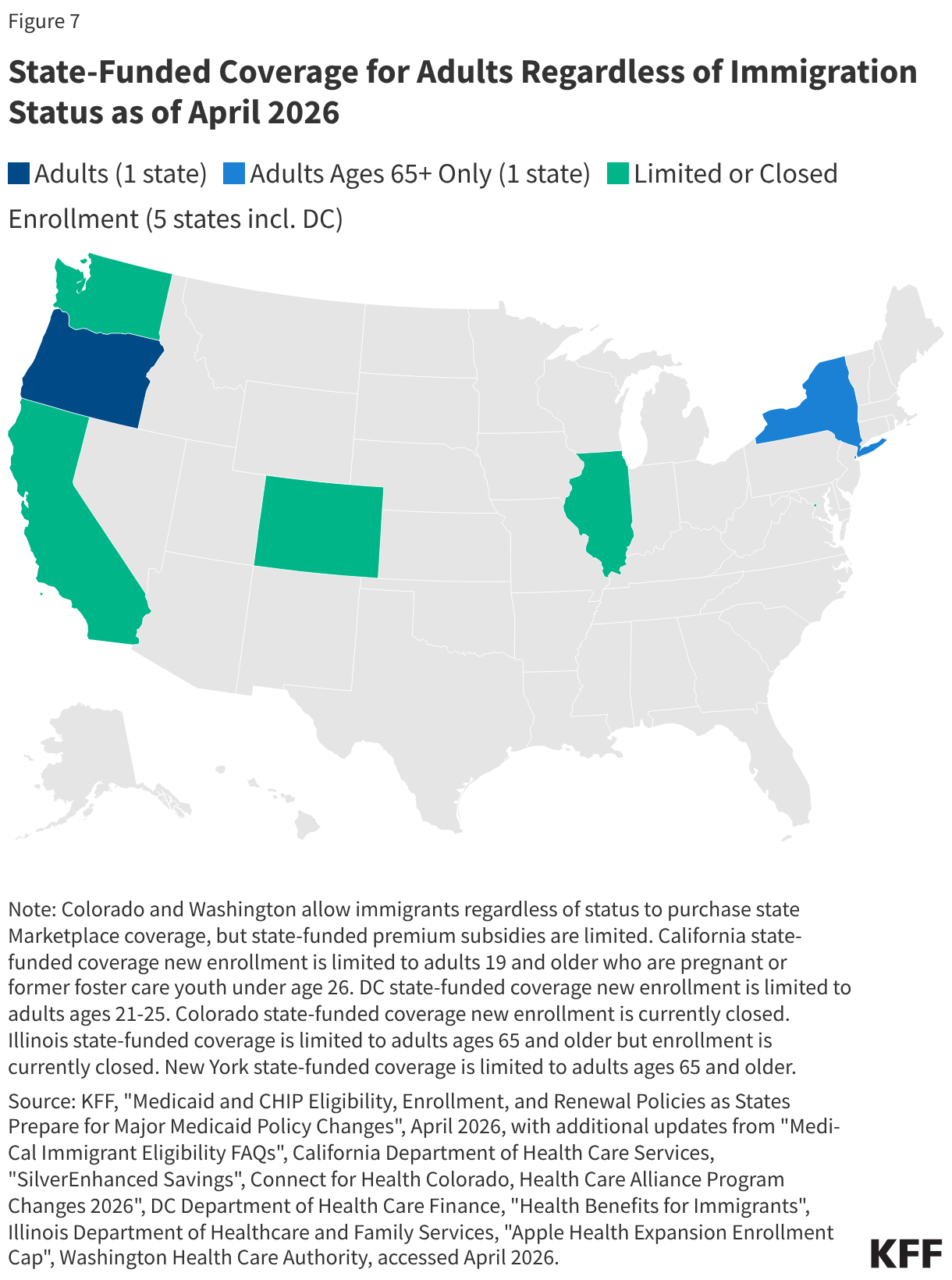
As of April 2026, seven states, including DC, have also expanded fully state-funded coverage to some income-eligible adults regardless of immigration status (Figure 7). These states include California, Colorado, DC, Illinois, New York, Oregon, and Washington. In some cases, coverage is limited to certain age groups, and several states have closed new enrollment. Some additional states cover some income-eligible adults who are not otherwise eligible due to immigration status using state-only funds but limit coverage to specific groups, such as lawfully present immigrants who are in the five-year waiting period for Medicaid coverage, or provide more limited benefits.
Six states, including DC, have recently eliminated or reduced or plan to scale back state-funded coverage due to budget pressures.
- California previously extended state-funded coverage to all income-eligible adults regardless of immigration status but implemented coverage reductions for adults 19 and older who are not pregnant or former foster youth under age 26 due to funding constraints, including: closing enrollment starting January 2026, ending dental benefits starting July 2026, and charging $30 monthly premiums for adults ages 19-59 starting July 2027. The California governor’s 2026-27 budget also proposes applying Medicaid policy changes included in the 2025 reconciliation law (work requirements and more frequent six-month renewals) to adults enrolled in the state-funded coverage program.
- Colorado allows adults regardless of immigration status to obtain Marketplace coverage through OmniSalud using a section 1332 waiver. Colorado uses state funds to provide plans with $0 premiums through SilverEnhanced Savings. The state reduced the enrollment cap for the program from 12,000 in 2025 to 6,700 people due to funding constraints. As noted above, the state also plans to cap enrollment and limit benefits for children and pregnant people beginning in January 2027 due to funding constraints.
- DC provides health coverage to low-income adults 21 and older regardless of immigration status through its longstanding locally funded Healthcare Alliance program. However, DC closed enrollment to adults ages 26 and older and reduced income limits for adults 21 and older starting October 2025. DC plans to end coverage for all adults ages 21 and older by October 2027.
- Illinois extended state-funded coverage to low-income individuals ages 65 and older regardless of immigration status through its Health Benefits for Immigrant Seniors (HBIS) program in December 2020 but new enrollment has been paused since 2023. Illinois previously extended coverage to low-income immigrants ages 42 to 64 regardless of immigration status through the Health Benefits for Immigrant Adults (HBIA) program in 2022, but ended HBIA coverage on July 2025 due to funding constraints.
- Minnesota extended state-funded health coverage to income-eligible adults 18 and older regardless of immigration status in January 2025 but ended this coverage starting January 2026 due to funding constraints.
- Washington uses state funds to provide Marketplace coverage with premium subsidies to individuals with incomes up to 250% FPL regardless of immigration status through Cascade Care using a section 1332 waiver, but funding is limited. In July 2024, Washington extended state-funded health coverage to individuals with incomes up to 138% FPL who are not eligible for either federal Medicaid or federal advance premium tax credits, but the state closed enrollment due to funding constraints and moves current and future enrollees to a fee-for-service program.
In addition to these states, Maryland also delayed plans to allow income-eligible individuals to purchase Marketplace coverage without subsidies regardless of immigration status to 2028 due to changes in the 2025 reconciliation law that will require additional administrative resources to implement.
Two states (New Mexico and New York) are planning to provide fully state-funded coverage to lawfully present immigrants that will lose Medicaid and ACA Marketplace coverage due to eligibility restrictions in the 2025 reconciliation law. New Mexico plans to use state funds to cover lawfully present immigrants losing Medicaid and ACA Marketplace Coverage in addition to DACA recipients. The New York governor’s 2026-27 budget proposes using state funds to cover lawfully present immigrants losing Medicaid coverage. The state will also use state funds to cover income-eligible lawfully present immigrants losing federally-subsidized health coverage through the Essential Plan. Under a longstanding court ruling, New York is required to provide state-funded coverage to lawfully present immigrants who would be eligible for Medicaid if not for their immigration status. Legislation introduced in New York and several other states, including California, Illinois, and Washington, would expand state-funded health coverage for immigrants to help fill gaps created by the reconciliation law; however, it is uncertain these bills will be enacted.
Data suggest that state coverage expansions for immigrants make a difference in their health coverage and health care access and use. The KFF/New York Times 2025 Survey of Immigrants shows that immigrant adults residing in states with more expansive coverage policies for immigrants are less likely to be uninsured compared to their counterparts living in states with less expansive coverage policies. Other research shows that coverage expansions for immigrant children increase access to health care and are associated with improved health outcomes. A study found that eliminating the five-year wait for Medicaid or CHIP was associated with a decline in uninsured rates among lawfully present foreign-born children in states without state-funded health care programs. California’s 2016 expansion to low-income children regardless of immigration status was associated with a 34% decline in uninsurance rates, and the state’s expansion to all adults was associated with an increase in health coverage among immigrant adults ages 50 and older. Similarly, a study found that children who reside in states that have expanded coverage to all children regardless of immigration status were less likely to be uninsured, to forgo medical or dental care, and to go without a preventive health visit than children residing in states that have not expanded coverage. Another study found that immigrant children residing in states with more expansive health coverage policies were more likely to have uninterrupted health coverage and a usual source of primary care than those residing in states with less expansive health coverage policies. Research has also found that expanding Medicaid coverage to pregnant people regardless of immigration status is associated with higher rates of prenatal care and improved birth outcomes, while more restrictive state coverage policies were associated with reduced postpartum care utilization.
Enrollment Barriers
Among immigrants who are eligible for coverage, many remain uninsured because of a range of enrollment barriers, including fears around immigration-status and data privacy. Trump administration immigration policy changes and increased enforcement efforts are contributing to growing fears among immigrant families and increased reluctance to access health coverage and care for themselves and/or their children. The share of immigrant adults who say they personally worry that they or a family member could be detained or deported has increased significantly in 2025 (41%) as compared to 2023 (26%). As of 2025, over one in ten (12%) immigrant adults also report avoiding applying for government assistance as compared to 8% in 2023 and 29% report skipping or postponing health care as compared to 22% in 2023. Further, about half (51%) of immigrant adults overall and about eight in ten (78%) of those who are likely undocumented say they are “somewhat” or “very” concerned about health care providers sharing information about immigration status with immigration enforcement officials, a fear that could be further exacerbated following the public notice of CMS’s new Medicaid data sharing policy with ICE.
Appendix
Appendix Table A
| Lawfully Present Immigrants by Qualified Status as of April 2026 | |
|---|---|
Qualified Immigrant Category | Other Lawfully Present Immigrants |
Lawful permanent resident (LPR or green card holder) | Granted Withholding of Deportation or Withholding of Removal, under the immigration laws or under the Convention against Torture (CAT) |
Refugee | Individual with Non-Immigrant Status, includes worker visas, student visas, U-visa, and other visas, and citizens of Micronesia, the Marshall Islands, and Palau |
Asylee | Temporary Protected Status (TPS) |
Cuban/Haitian entrant | Deferred Enforced Departure (DED) |
Paroled into the U.S. for at least one year | Deferred Action Status |
Conditional entrant granted before 1980 | Lawful Temporary Resident |
Granted withholding of deportation | Administrative order staying removal issued by the Department of Homeland Security |
Battered noncitizen, spouse, child, or parent | Resident of American Samoa |
Victims of trafficking and their spouse, child, sibling, or parent or individuals with pending application for a victim of trafficking visa | Applicants for certain statuses |
Member of a federally recognized Indian tribe or American Indian born in Canada | People with certain statuses who have employment authorization |
Citizens of the Marshall Islands, Micronesia, and Palau who are living in one of the U.S. states or territories (referred to as Compact of Free Association or COFA migrants) | People with certain statuses who have employment authorization |
Endnotes
- The estimate of the total number of noncitizens in the U.S. is based on the 2024 American Community Survey (ACS) 1-year Public Use Microdata Sample (PUMS). The ACS data do not directly indicate whether an immigrant is lawfully present or not. KFF draws on the methods underlying the 2013 analysis by the State Health Access Data Assistance Center (SHADAC) and the recommendations made by Van Hook et. al. This approach uses the Survey of Income and Program Participation (SIPP) to develop a model that predicts immigration status; it then applies the model to ACS, controlling to state-level estimates of total undocumented population from Pew Research Center. For more detail on the immigration imputation used in this analysis, see Technical Appendix B. ↩︎
- KFF analysis of 2023 Medical Expenditure Panel Survey full-year consolidated data file. ↩︎
