KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
Vaccine Misinformation Spreads as Children Head Back to School
This is Irving Washington and Hagere Yilma. We direct KFF’s Health Misinformation and Trust Initiative and on behalf of all of our colleagues across KFF who work on misinformation and trust we are pleased to bring you this edition of our bi-weekly Monitor.
Addressing Vaccine Hesitancy Around MMR and Childhood Immunizations as Measles Resurges
FG Trade / Getty Images
As students return to school, state health departments have urged families to make sure their children are up to date on recommended vaccinations. Without these immunizations, children risk contracting preventable diseases such as measles, which has seen a resurgence in several states. However, a KFF analysis highlights that routine immunization rates for kindergarteners have not returned to pre-pandemic levels, in part due to vaccine hesitancy fueled by misinformation and partisan politics. Persistent false claims include the debunked link between vaccines and autism, which has falsely led some to believe that vaccines are more harmful than the diseases they prevent. These claims downplay the severity of measles and dismiss it as rare or harmless. They also commonly suggest delaying or skipping vaccines for children to avoid unfounded risks, despite the CDC’s evidence-based schedule. These misleading narratives erode public confidence in vaccines, fueling larger and faster outbreaks.
Polling Insights:
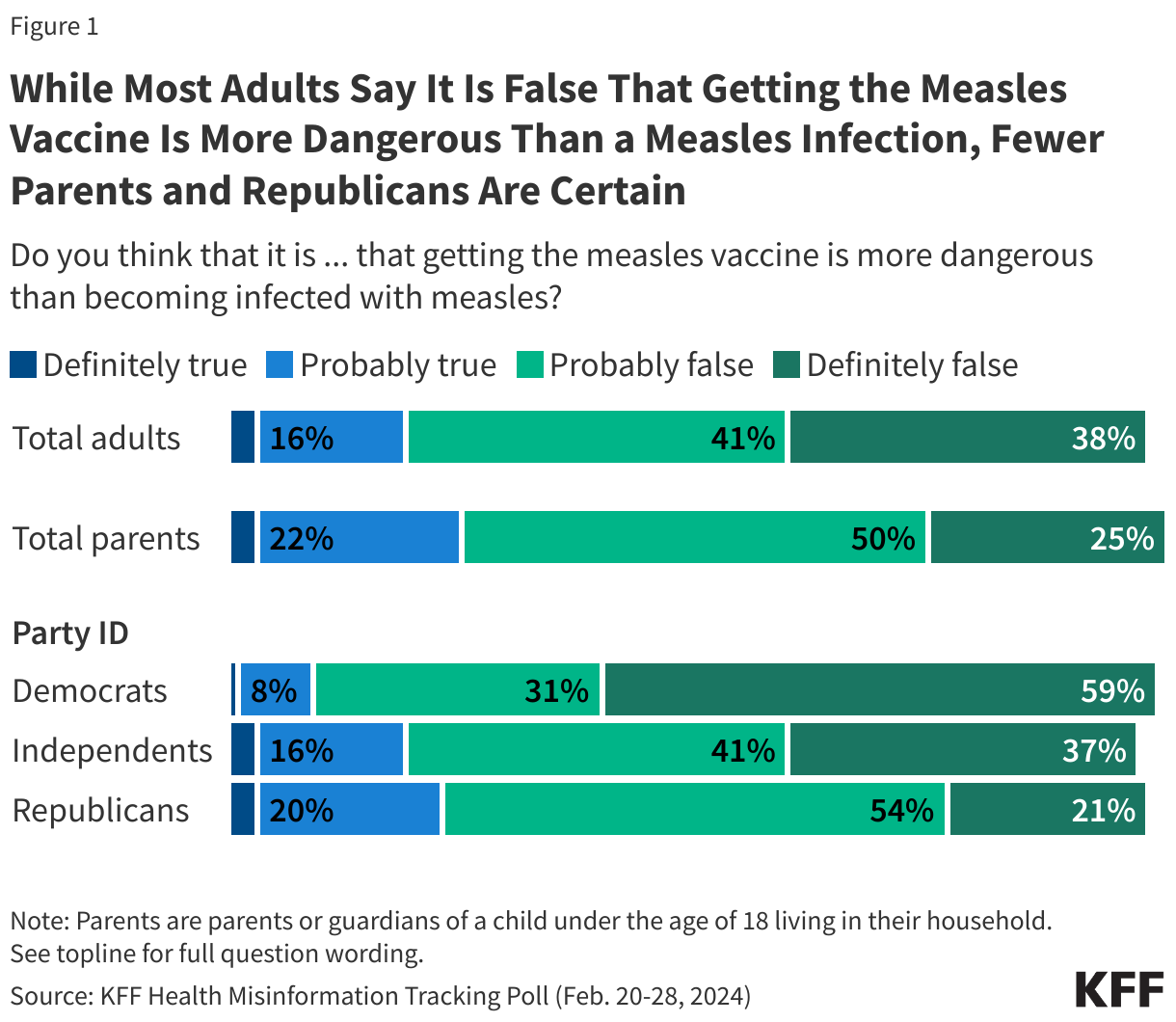
While a large share of the public correctly views the false claim that “the measles vaccine is more dangerous than the disease itself” as definitely false, KFF polling from February 2024 finds that most adults express some uncertainty when it comes to this claim. More than half of U.S. adults say this claim is either “probably false” (41%) or “probably true” (16%). Few (3%) believe it is “definitely true,” while about four in ten (38%) are confident that the claim is “definitely false.” (Figure 1). Additionally, there are partisan divides when it comes to definitively identifying the claim as false, with Republicans being less likely to do so. Notably, a quarter of parents of children under the age of 18 say that the false claim that the measles vaccine is more dangerous than the measles infection is definitely or probably true.
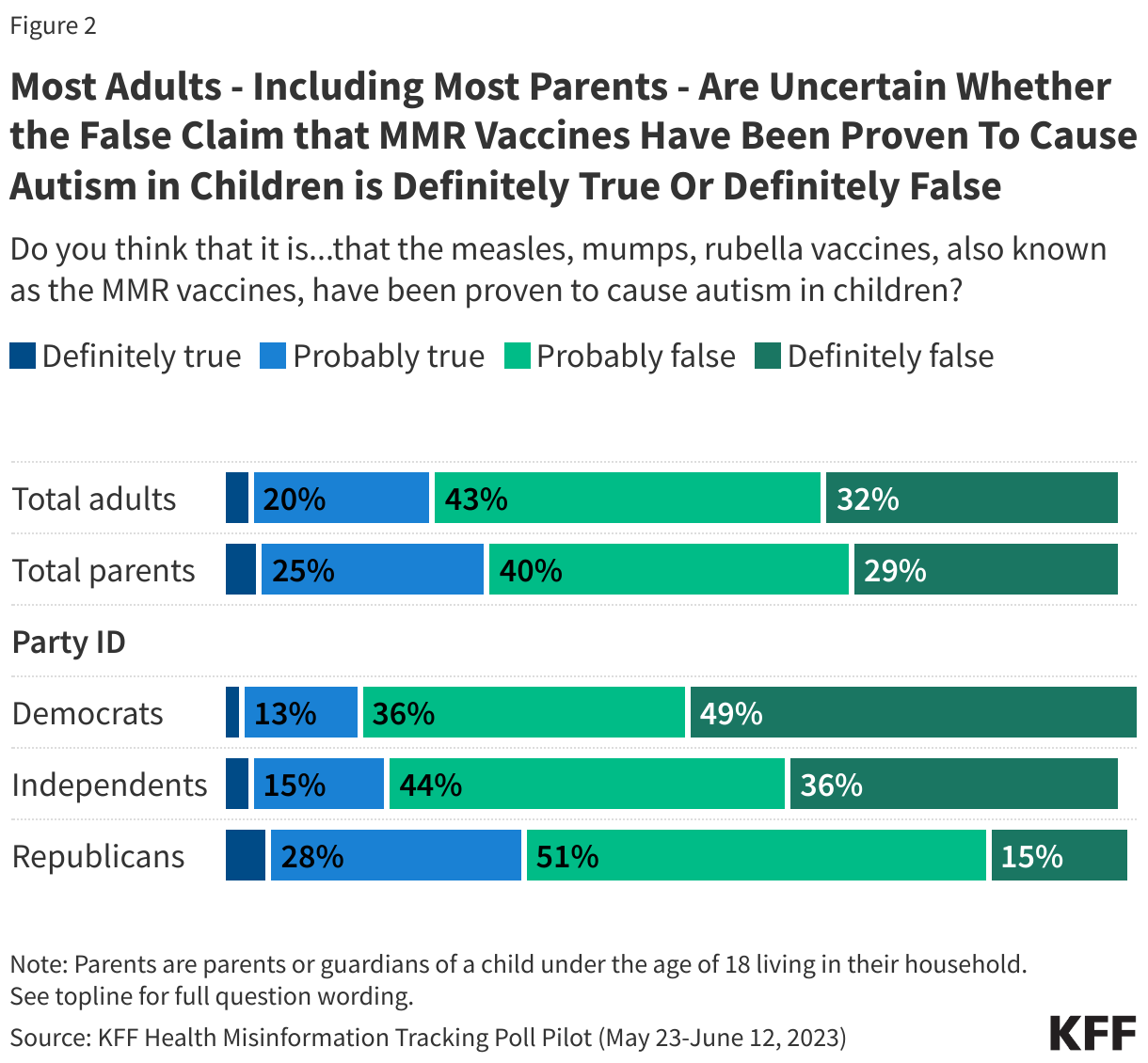
The 2023 KFF Health Misinformation Tracking Poll Pilot found similar results for the claim that “The measles, mumps, rubella vaccines, also known as the MMR vaccines, have been proven to cause autism in children.” While most Americans do not believe the statement, the bulk of the public is uncertain, with 43% saying it is “probably false” and 20% saying it is “probably true.” About a third of the public (32%) identify the claim as being “definitely false.” This highlights the ongoing confusion and hesitancy many people face when navigating vaccine misinformation. Partisan differences also emerged on this question with Republicans (33%) being more likely than independents (18%) and Democrats (15%) to say that this statement is definitely or probably true.
Large shares of parents also express uncertainty about whether MMR vaccines have been proven to cause autism in children with a quarter of parents (25%) saying that claim is “probably true” while four in ten parents say it is “probably false.” (Figure 2).
To combat misinformation about the MMR vaccine, health professionals and media outlets can address and debunk common misconceptions like the narratives listed above. Health media resources like The Harvard Kennedy School’s The Journalist’s Resource provide guidance for reporters covering MMR vaccination rates and hesitancy. These resources emphasize the importance of clearly distinguishing between vaccine hesitancy and anti-vaccine beliefs, highlighting the high vaccination rates among U.S. students, and exploring reasons for delayed or incomplete vaccinations.
Emerging Misinformation Narratives
Reemergence of COVID-19 Vaccine Misinformation Following FDA Booster Approval
Thanasis / Getty Images
In addition to the required back-to-school vaccines for children, health officials are recommending that everyone 6 months of age and older receive the updated COVID-19 vaccines this fall. However, misinformation in online conversations indicate that vaccine hesitancy and misinformation may hinder uptake for some. In the days after the FDA approved the booster vaccines, more than half of posts, articles, comments on articles and videos mentioning the COVID-19 vaccines included terms associated with false claims. Many social media posts recycled debunked narratives that emerged during the initial approval of the COVID-19 vaccines, such as claims that the vaccines contain the SV40 virus, cause “turbo cancer,” were designed to only profit the government and pharmaceutical companies or were approved too quickly to be safe.
Misinformation has also emerged around specific vaccine types. Online discussions leading up to the FDA’s approval reflected some people’s frustration over the delayed approval of Novavax’s non-mRNA COVID-19 vaccine. Some falsely claimed the Novavax COVID-19 vaccine is “over 40% more effective” than other vaccines and that the FDA is “intentionally withholding” it, deepening distrust in the FDA approval process and mRNA vaccines. One post that made this claim had approximately 89,700 views, 3,000 likes, 1,000 reposts, and 50 comments as of August 27th. At the same time, there are also examples of support for the updated boosters. One doctor said, “I’ll get the updated COVID vaccine as soon as it’s available, and I’ll urge my patients to do the same. Getting COVID over and over again is not a great plan.” a post garnering 85,300 views, 3,300 likes, 620 reposts, and 470 comments by August 27th. These examples illustrate that both misinformation and accurate information can circulate on social media and receive comparable levels of engagement.
Recent political statements have further complicated the vaccine discussion. Presidential candidate Donald Trump has pledged to defund schools that mandate COVID-19 vaccines, a move that could exacerbate vaccine hesitancy and negatively impact public health efforts. While Trump previously supported the development and promotion of vaccines, his current stance has raised concerns among health experts about the potential for increased vaccine misinformation and declining vaccination rates. Trump’s rhetoric against vaccine mandates could undermine public trust in vaccination programs and jeopardize progress made in controlling preventable diseases.
False Claims Linking Mpox to COVID-19 Vaccines and Lockdowns
Marina Demidiuk / Getty Images
Misinformation about the public health response to mpox (formerly known as monkeypox) appeared online after the World Health Organization (WHO) declared the disease a public health emergency. Most of the misinformation falsely claims that the WHO had ordered nations to prepare for “mega lockdowns” because of mpox. Similar misinformation has fueled fears of school closures, despite experts clarifying that mpox spreads primarily through close skin contact, making such drastic measures highly unlikely. Some have also falsely claimed that the WHO has reversed its decision, often using an old video from May 2023 showing the WHO Director General announcing the end of a previous mpox emergency.
Simultaneously, the WHO’s declaration sparked a wave of claims linking mpox to COVID-19 vaccines. Several popular posts in English and Spanish falsely claimed that mpox is a side effect of mRNA COVID-19 vaccines, with some recycling the debunked myth that mpox is an autoimmune skin disease triggered by vaccination. An X post in Spanish shared on August 15 read, “No, there was never any COVID, but rather pneumonia. And no, there is no monkeypox, or bird flu, or anything like that. What there are the after-effects of the ‘vaccines.’” In just 12 days, the post had received approximately 275,200 views, 4,000 likes, 2,500 reposts, and 170 comments.
Research Updates
Research Review Highlights Strategies to Combat MMR Vaccine Hesitancy
FluxFactory / Getty Images
A review published earlier this year in Vaccines explored why some people are hesitant to receive the MMR vaccine by examining the role of misinformation and the changing landscape of online communication. The review explains how communities and the way vaccines are presented can influence people’s attitudes. Based on these factors, the authors shared evidence-based strategies to address hesitancy, including improving communication between health care providers and patients, developing personalized approaches, and implementing effective public information campaigns.
Source: Higgins, D. M., & O’Leary, S. T. (2024). A World without Measles and Rubella: Addressing the Challenge of Vaccine Hesitancy. Vaccines, 12(6), 694.
AI and Emerging Technologies
Undisclosed Use of AI in Academic Papers
AndreyPopov / Getty Images
The rise of AI-generated fake scientific papers has the potential to erode public trust in science and contribute to the spread of misinformation, particularly in areas such as health and environmental policy. Often disseminated through platforms like Google Scholar, these papers go undetected by readers and can influence evidence-based decision-making. A recent analysis found that about two-thirds of the papers examined were created, at least in part, using artificial intelligence (AI) without proper disclosure, making it difficult to identify and correct the misinformation. As these fraudulent studies circulate online, they risk distorting public understanding and undermining the integrity of scientific research.
About The Health Information and Trust Initiative: the Health Information and Trust Initiative is a KFF program aimed at tracking health misinformation in the U.S., analyzing its impact on the American people, and mobilizing media to address the problem. Our goal is to be of service to everyone working on health misinformation, strengthen efforts to counter misinformation, and build trust.
The Monitor is a report from KFF’s Health Information and Trust initiative that focuses on recent developments in health information. It’s free and published twice a month.
Support for the Health Information and Trust initiative is provided by the Robert Wood Johnson Foundation (RWJF). The views expressed do not necessarily reflect the views of RWJF and KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities. The Public Good Projects (PGP) provides media monitoring data KFF uses in producing the Monitor.
Poll Finding
KFF Health Tracking Poll September 2024: Harris v. Trump on Key Health Care Issues
Note: The third bullet in the key findings was updated on Sept. 17, 2024, to correct a typographical error, where former President Trump had been misidentified as President Biden.
Key Takeaways
Four in ten voters (38%) choose the economy and inflation as the most important issue determining their vote this fall from a list of national issues, including several health care issues. As the economy looms large in the 2024 election, voters from both parties want their candidates to talk about health care costs. When voters are asked to offer in their own words what health care issue they most want to hear the candidates talk about, about four in ten voters across partisanship mention issues related to the cost of health care. Democratic and Democratic-leaning independent voters say they would like Vice President Harris to talk about general health care costs (20%), prescription drug costs (15%), and the cost of insurance or reducing their monthly premiums (6%). About one in seven offered abortion as the one health care issue they want to hear about from Harris and 13% mentioned universal health care – an issue that was largely debated during the 2020 Democratic primaries. Similarly, nearly half (45%) of Republican voters and Republican-leaning independent voters say they would most like to hear former President Trump talk about health care costs. This is followed by one in eight (12%) who say they want to hear him talk about Medicare, Medicaid, or Social Security.
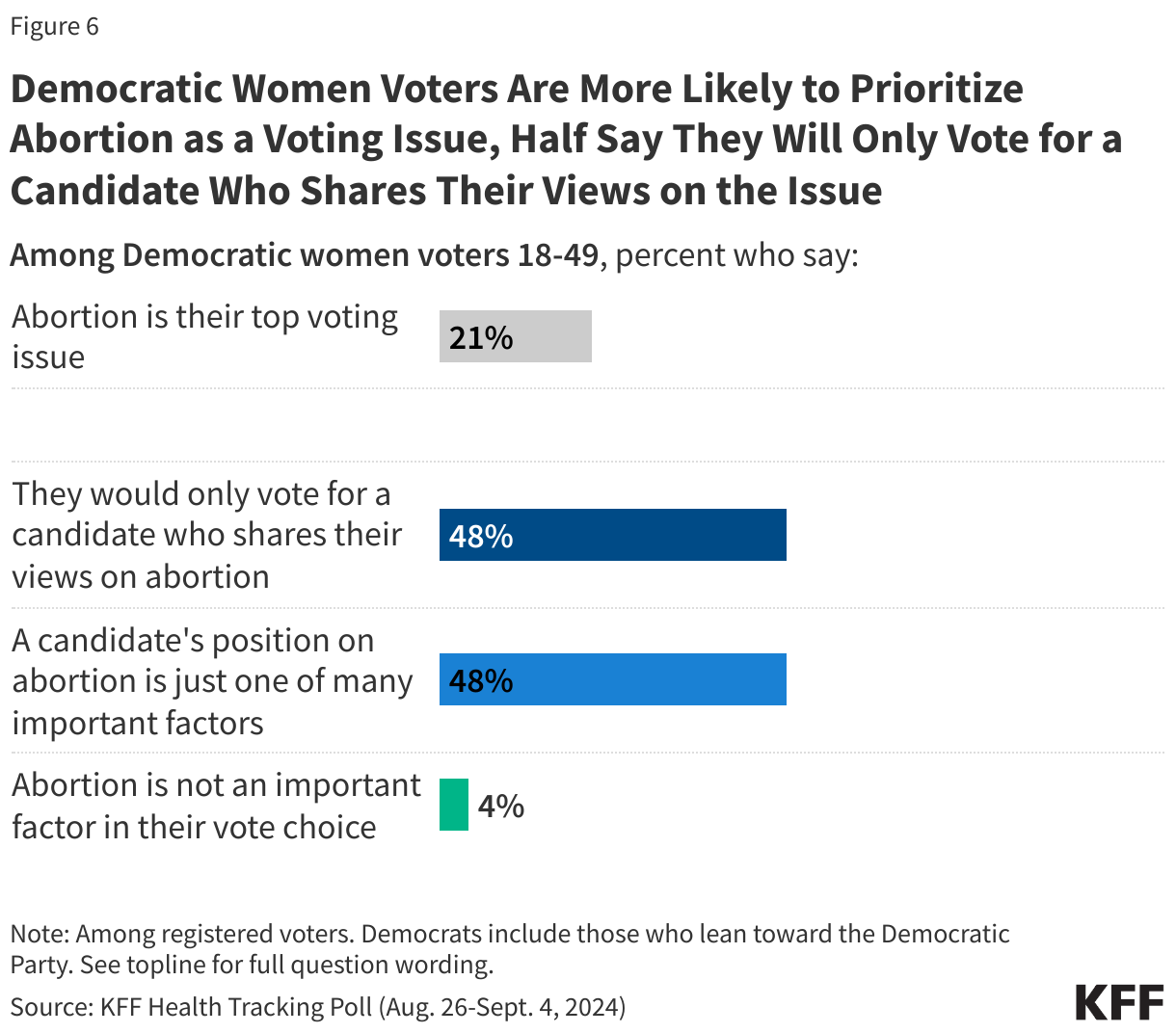
Abortion continues to motivate a small group of voters, mainly Democratic and Democratic-leaning independent women voters of reproductive age (ages 18-49). About a fifth of this voting bloc say abortion is their most important voting issue and half say they will only vote for a candidate who shares their views on abortion. Overall, this group of voters wants abortion to be legal and the vast majority (90%) say they want a federal law restoring a nationwide right to abortion similar to what was protected by Roe v. Wade. The share of Democratic-leaning women of reproductive age who say they think the presidential election will have a major impact on abortion access has increased 31 percentage points in the past six months (90% v. 59%), a time in which Vice President Harris became the Democratic presidential nominee and began highlighting the issue in her campaign.
A majority of all voters now say they trust the Democratic nominee more to handle the issue of abortion compared to former President Trump (53% v. 34%), widening a much smaller advantage that President Biden had over Trump earlier this year (38% v. 29%), a sign of Harris’s relative strength with Democratic voters on this issue.
Voters largely prefer a federal law restoring a nationwide right to abortion, similar to what was protected by Roe v. Wade (61%), rather than leaving it up to the states to decide whether abortion is legal or not (39%). Majorities of both Democratic voters (87%) and independent voters (68%) would prefer a federal law restoring the nationwide right to an abortion, the policy position of the Democratic presidential candidate V.P. Harris, while seven in ten Republican voters would prefer leaving abortion laws up to the states, the position advocated by former President Trump. Notably, while the vast majority of Democratic and Democratic-leaning women voters of reproductive age support restoring a federal law for a nationwide right to abortion, this policy proposal is also preferred by half of Republican women voters of reproductive age.
How Voters Are Prioritizing Health Care Issues in 2024
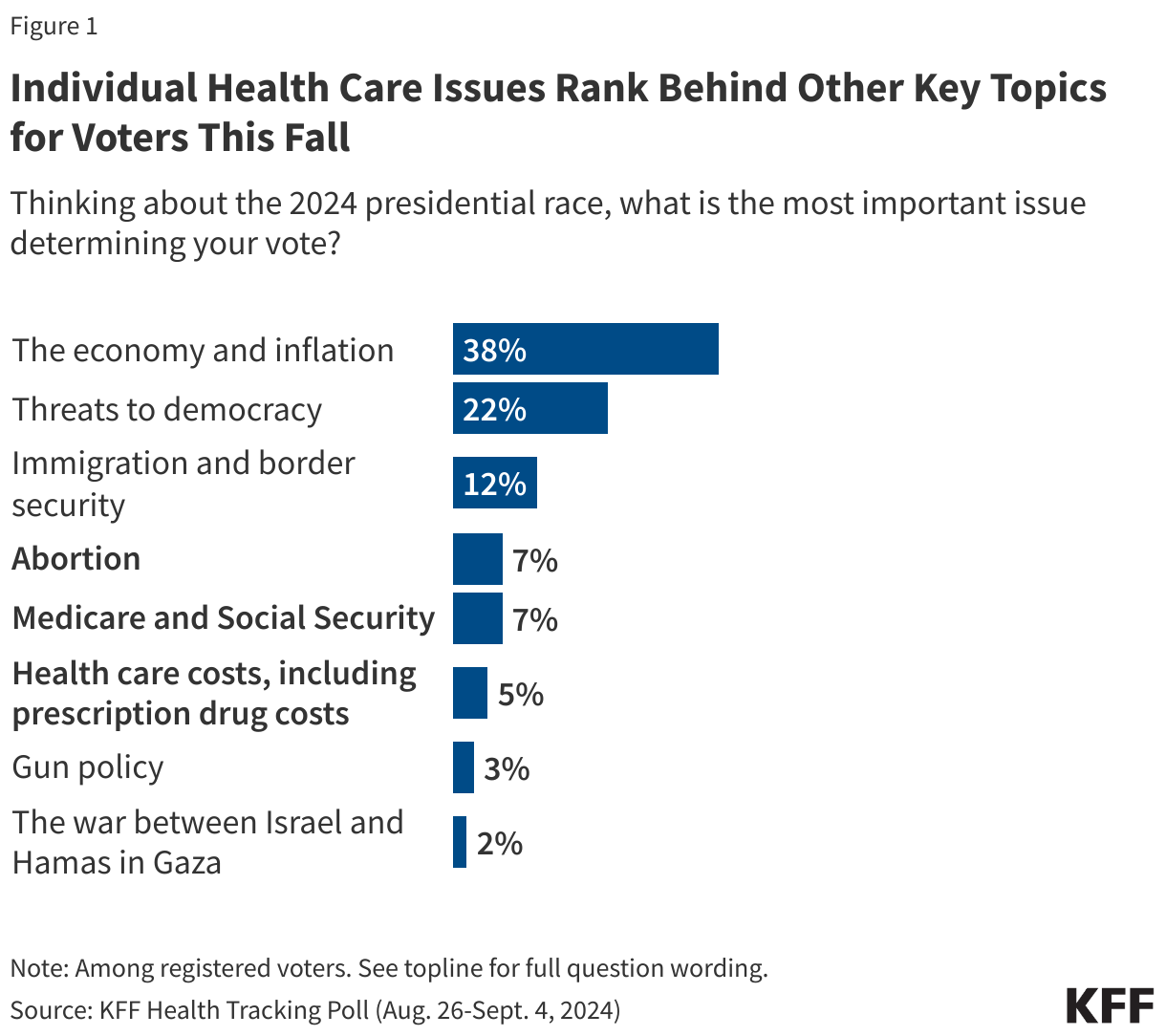
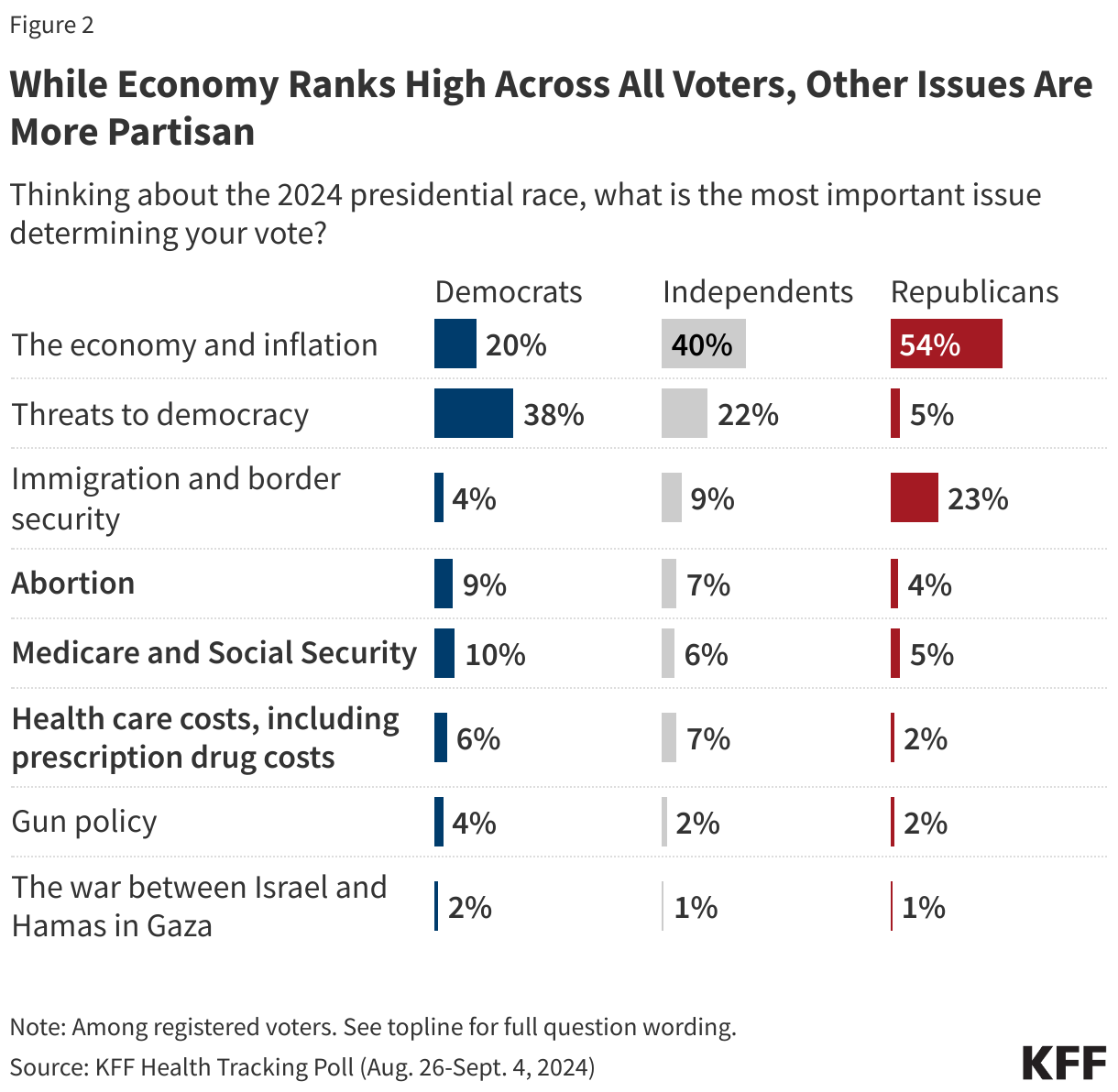
The economy and inflation continue to dominate the list of issues that voters are focusing on during this year’s presidential election with four in ten voters (38%) saying it is the most important issue determining their vote in the 2024 presidential race. Following the economy is threats to democracy (22%), immigration and border security (12%), then several individual health care issues including abortion (7%), Medicare and Social Security (7%), and health care costs, including prescription drug costs (5%). Altogether, health care issues are seen as the most important issue by about one in five voters (19%). Gun policy (3%) and the war between Israel and Hamas in Gaza (2%) rank the lowest among the issues included in the list provided to voters.
While substantial shares of voters across partisanship say the economy and inflation is their most important voting issue including more than half (54%) of Republican voters, the ranking of other issues are more partisan. For example, Republican voters are much more likely to prioritize immigration as a voting issue with nearly a quarter (23%) saying it is the most important issue to their vote compared to one in ten independent voters (9%) and few Democratic voters (4%). On the other hand, threats to democracy is the top voting issue for Democratic voters with four in ten (38%) saying it is their most important issue, compared to one in five independent voters (22%) and 5% of Republican voters who say the same.
Voters Want to Hear Candidates Talk About Lowering Health Care Costs
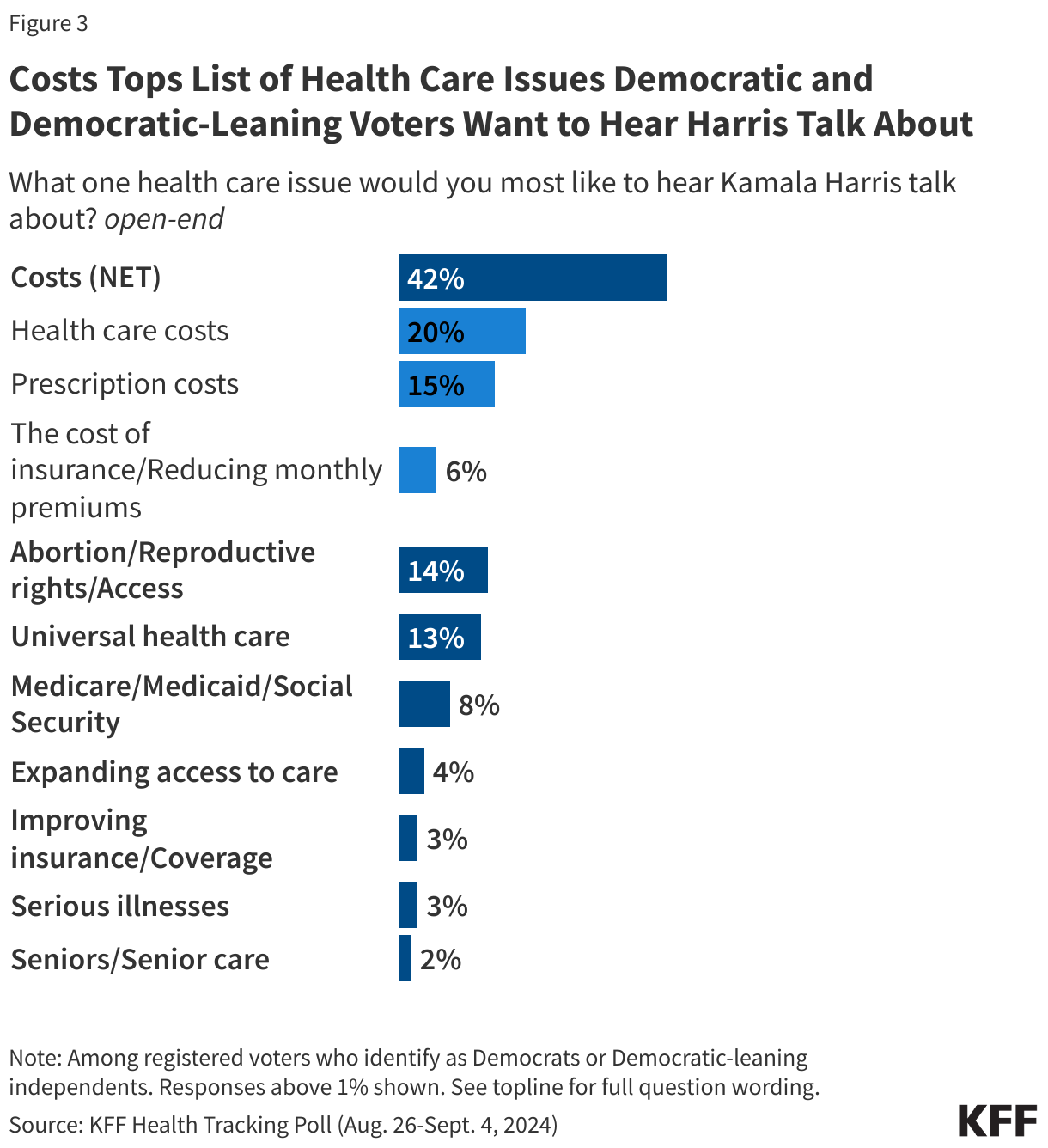
An indication of how the economy and health care consistently overlap for voters, economic concerns also rear up when voters are asked what health care issue they most want to hear the candidates talk about. Across partisans, the recurring theme is costs. Responses related to health care costs are offered by four in ten (42%) Democratic and Democratic-leaning independent voters when asked to say in their own words what is the one health care issue they would most like Vice President Harris to talk about. This includes voters who mentioned general health care costs (20%), prescription drug costs (15%), and the cost of insurance or reducing their monthly premiums (6%). About one in seven offered abortion as the one health care issue they want Harris to talk about and 13% mentioned universal health care – an issue that was largely debated during the 2020 Democratic primaries.
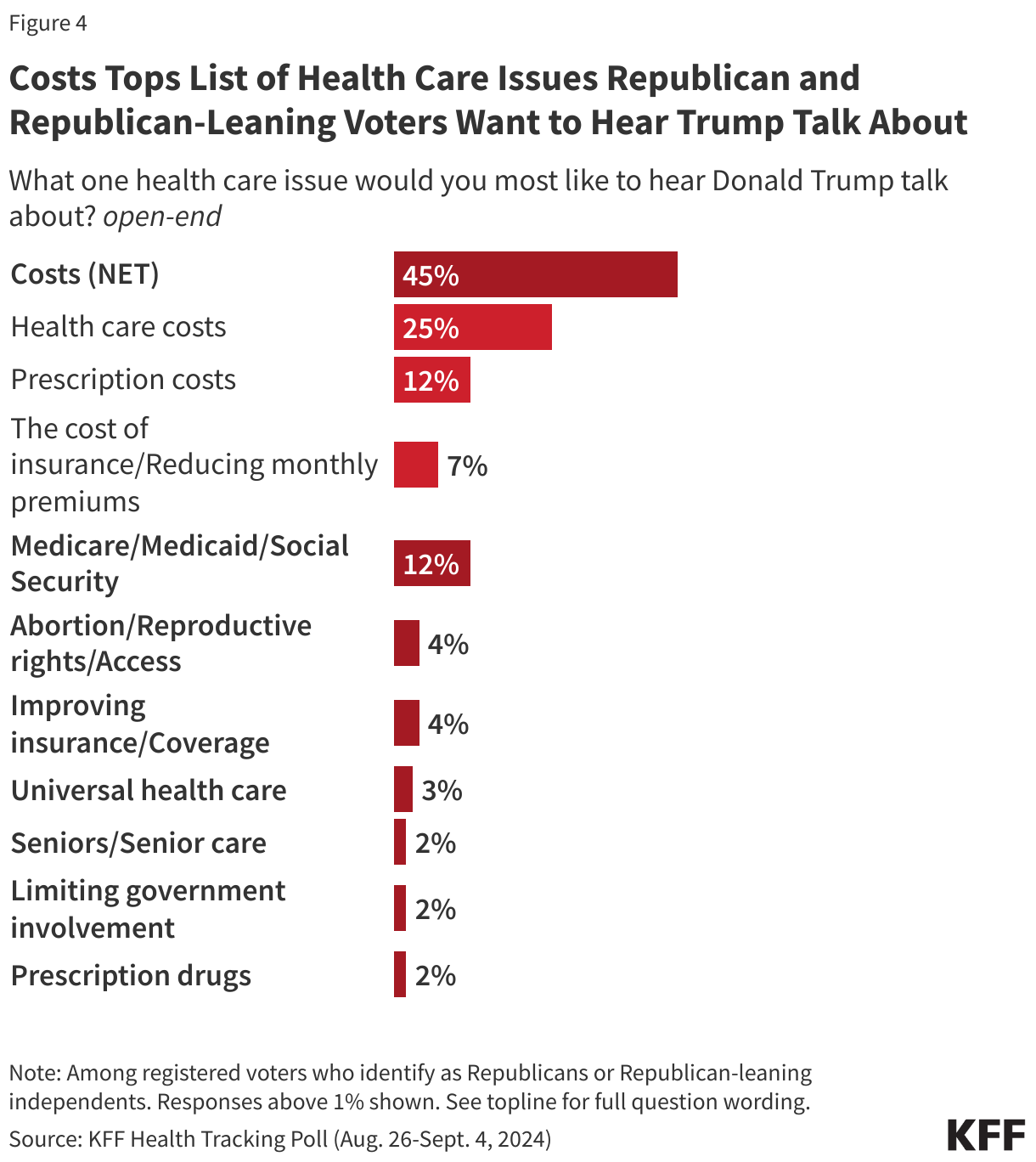
Similarly, nearly half (45%) of Republican voters and Republican-leaning independent voters say they would most like to hear former President Trump talk about health care costs. This is followed by one in eight voters who say they want to hear him talk about Medicare, Medicaid, or Social Security.
Health Care Issues, Including Abortion, Resonate Highest With Certain Voters
Overall, the individual health care issues included in the list loom larger for Democratic voters, as they are more than twice as likely as Republican voters to select abortion, Medicare and Social Security, or health care costs as their most important voting issue (25% v. 11%). One in five independent voters also chose a health care issue as their most important voting issue. In addition, women voters are about twice as likely as men to choose a health care issue as their most important voting issue this fall (25% vs. 12%). Democratic voters and women voters have long been more likely to prioritize health care issues than their counterparts, except for Republican voters’ focus on repealing the ACA, but this election cycle is slightly different. In the first presidential election since the Supreme Court Dobbs decision that overturned Roe v. Wade, abortion is now a top voting issue for about one in ten Democratic voters and a similar share of overall women voters.
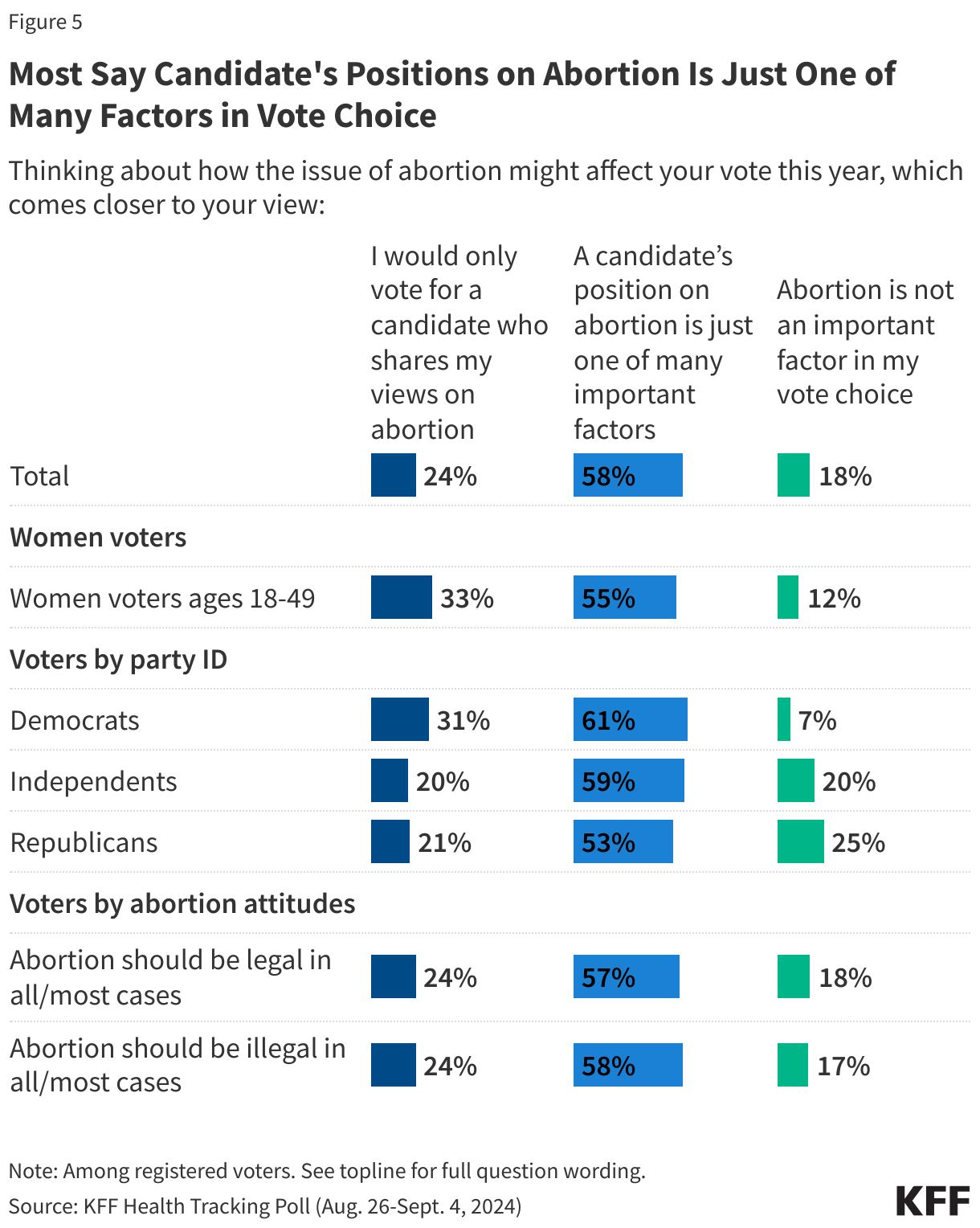
Overall, most voters (58%) say a candidate’s position on abortion is just one of many factors that might affect their vote this year while about a quarter of voters say they will only vote for a candidate who shares their views on abortion. About one in five (18%) voters say abortion isn’t an important factor in their vote choice.
Democratic voters are more likely to say they will only vote for a candidate who shares their view on abortion (31%), but still most say it is just one of many factors (61%). The same is true among all women of reproductive age, with one in three saying they would only vote for a candidate who shares their view on abortion.
Abortion Is an Important Voting Issue for Democratic Women of Reproductive Age
While abortion may not resonate as a top voting issue for all voters, for a key group of voters – Democratic women voters of reproductive age – abortion is among the most important voting issues.
Abortion ranks as a top voting issue for Democratic and Democratic-leaning women of reproductive age (between the ages of 18 and 49), with 21% saying it is their most important issue, ranking alongside the economy (23%) and threats to democracy (25%) as their top voting issue.
Half of Democratic women of reproductive age, the group that is most likely to prioritize abortion as a voting issue, say they will only vote for a candidate who shares their view on abortion (48%), a position they hold more often than any other group. A similar share (48%) say abortion is one of many important factors, while few say abortion is not an important factor in their vote choice (4%). This group is largely in support of abortion access with nine in ten (93%) Democratic women of reproductive age saying they think abortion should be legal in all or most cases.
Vice President Harris Has Strong Advantage on Abortion, Former President Trump Leads on Economy and Immigration
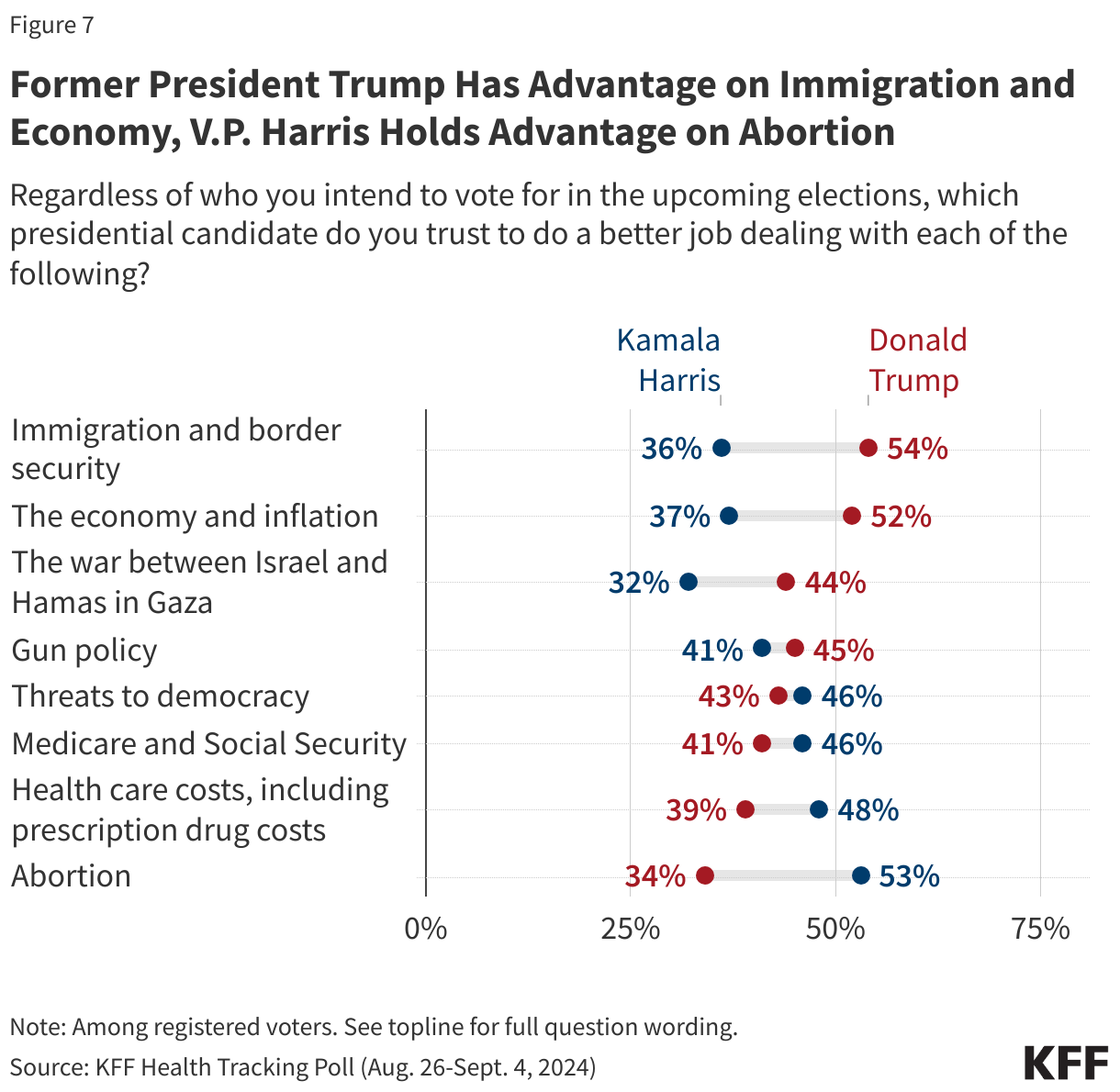
Former President Trump has a clear advantage over Vice President Harris on who voters trust to do a better job dealing with two key issues: economy and inflation (52% vs. 37%) and immigration and border security (54% vs. 36%). On the other hand, Vice President Harris has nearly a similar advantage on the issue of abortion (53% vs. 34%). A KFF Tracking Poll conducted earlier this year when President Biden was still the Democratic nominee found that Biden had a smaller advantage over Trump on abortion (38% v. 29%), a sign of Harris’s relative strength with Democratic voters on this issue.
Neither candidate has a majority of voters saying they trust them more to do a better job on any of the other key voting issues asked about including Medicare and Social Security or health care costs. However, V.P. Harris does have the advantage on the issue of health care costs. Former President Trump garners more trust on the issue of the war between Israel and Hamas in Gaza, but a substantial share of voters say they trust neither candidate to do a better job of handling this issue.
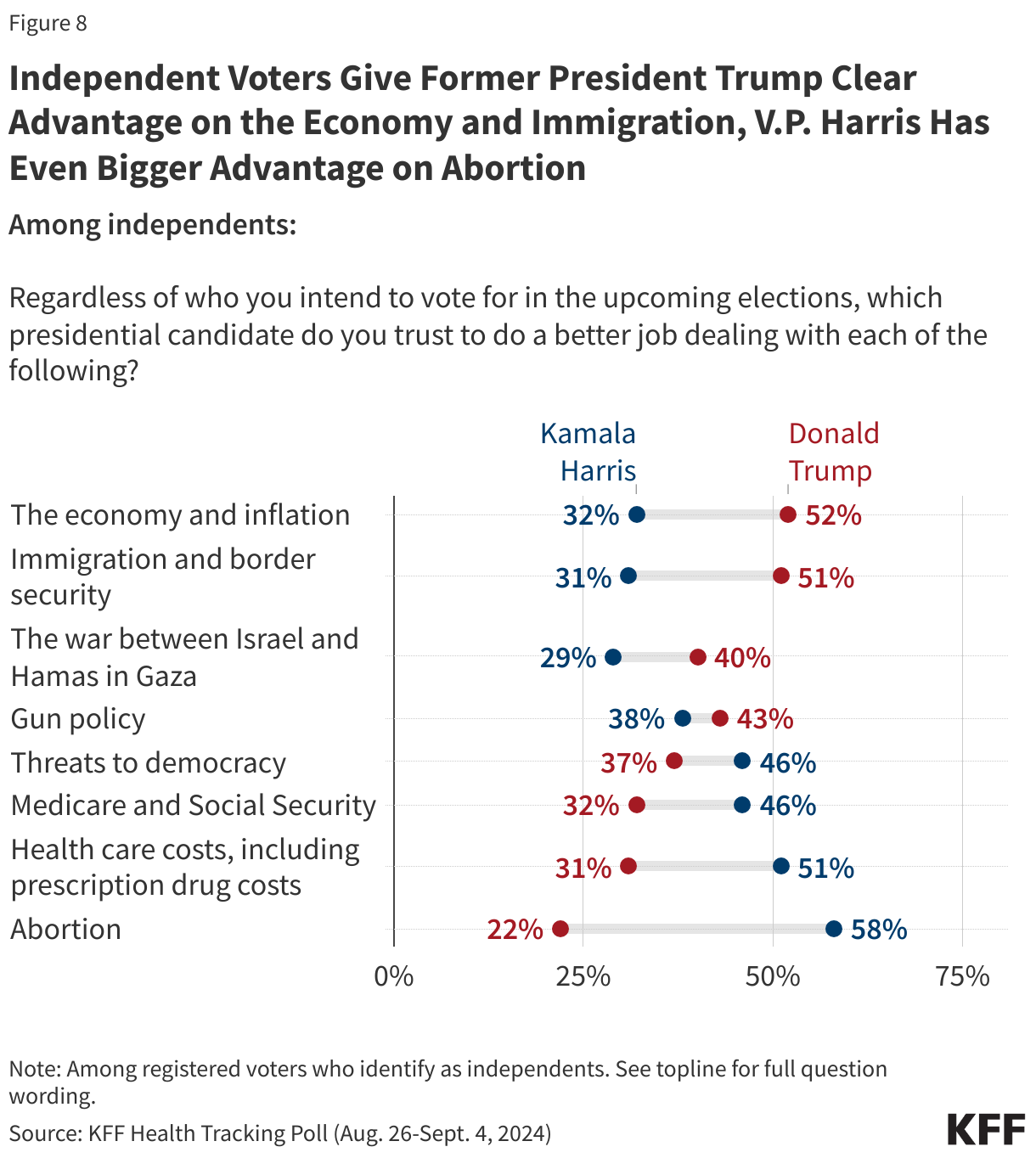
Both presidential candidates are trying to garner support from independent voters and these voters give former President Trump the advantage on their top voting issue – the economy and inflation. About half of independent voters (52%) say they trust former President Trump to do a better job dealing with the economy and inflation, while a third (32%) of independent voters say they trust V.P. Harris to do a better job. V.P. Harris holds a much smaller advantage on their second most important voting issue – threats to democracy (46% vs. 37%). Across the three health care issues, V.P. Harris has a strong advantage over former President Trump among independent voters including a 36-point advantage on the issue of abortion. On the other hand, former President Trump holds a 20-point advantage on the issue of immigration and border security.
Most Voters Expect Presidential Election to Have Major Impact on Abortion Policy
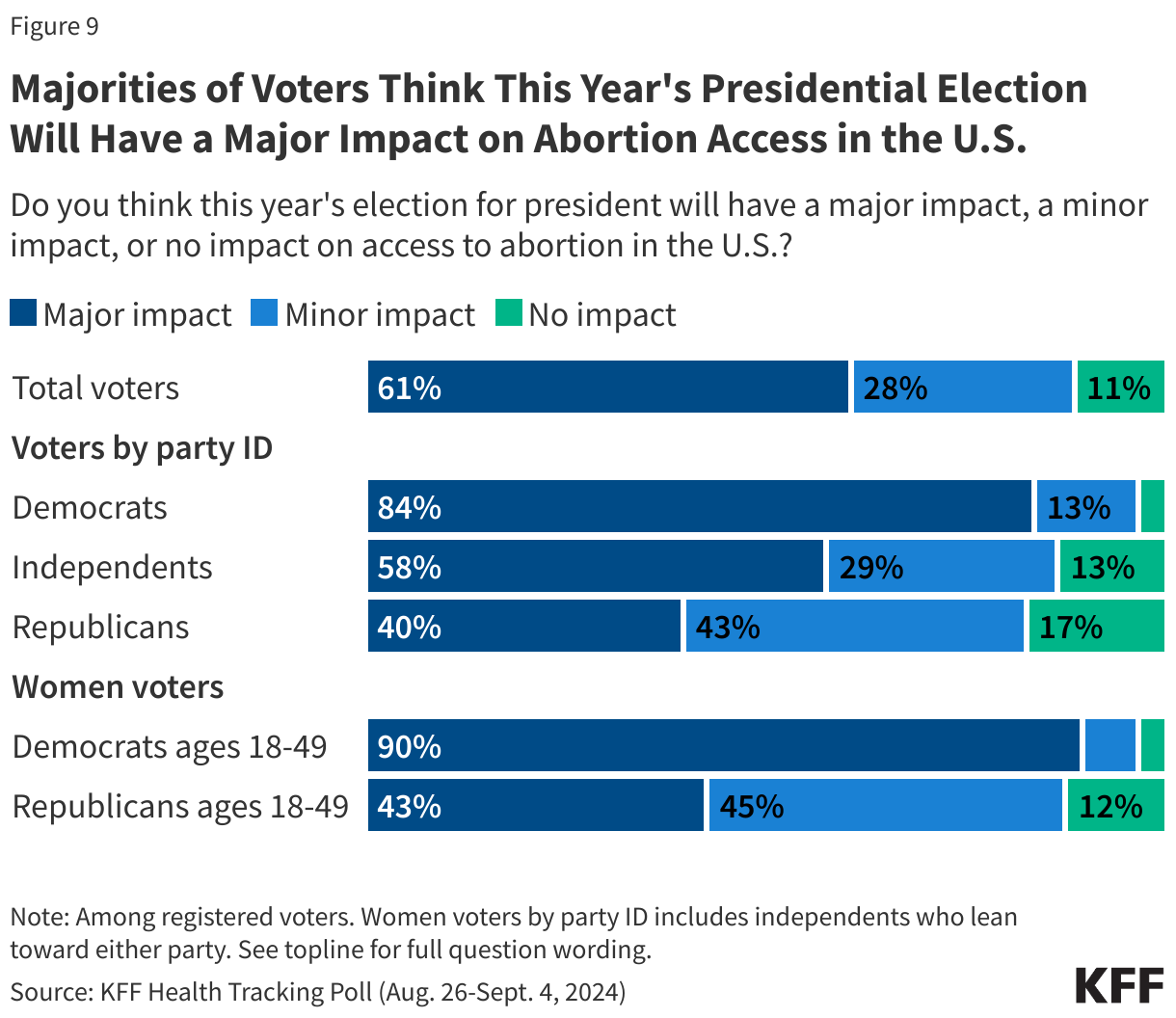
Nine in ten (89%) voters say this year’s elections for president will have an impact on abortion access in the U.S., including six in ten (61%) voters who say it will have a “major impact.” One in ten (11%) voters think the election will not have any impact on access to abortion in the U.S.
Democratic voters are more than twice as likely as Republican voters (84% vs. 40%) to say the election will have a major impact on abortion access. Three-fourths (72%) of women voters of reproductive age, those most directly impacted by abortion policy in the U.S., say the presidential election will have a major impact on abortion access, rising to nine in ten Democratic and Democratic-leaning independent women voters ages 18-49. On the other hand, four in ten (43%) Republican and Republican-leaning independent women voters of reproductive age say the same.
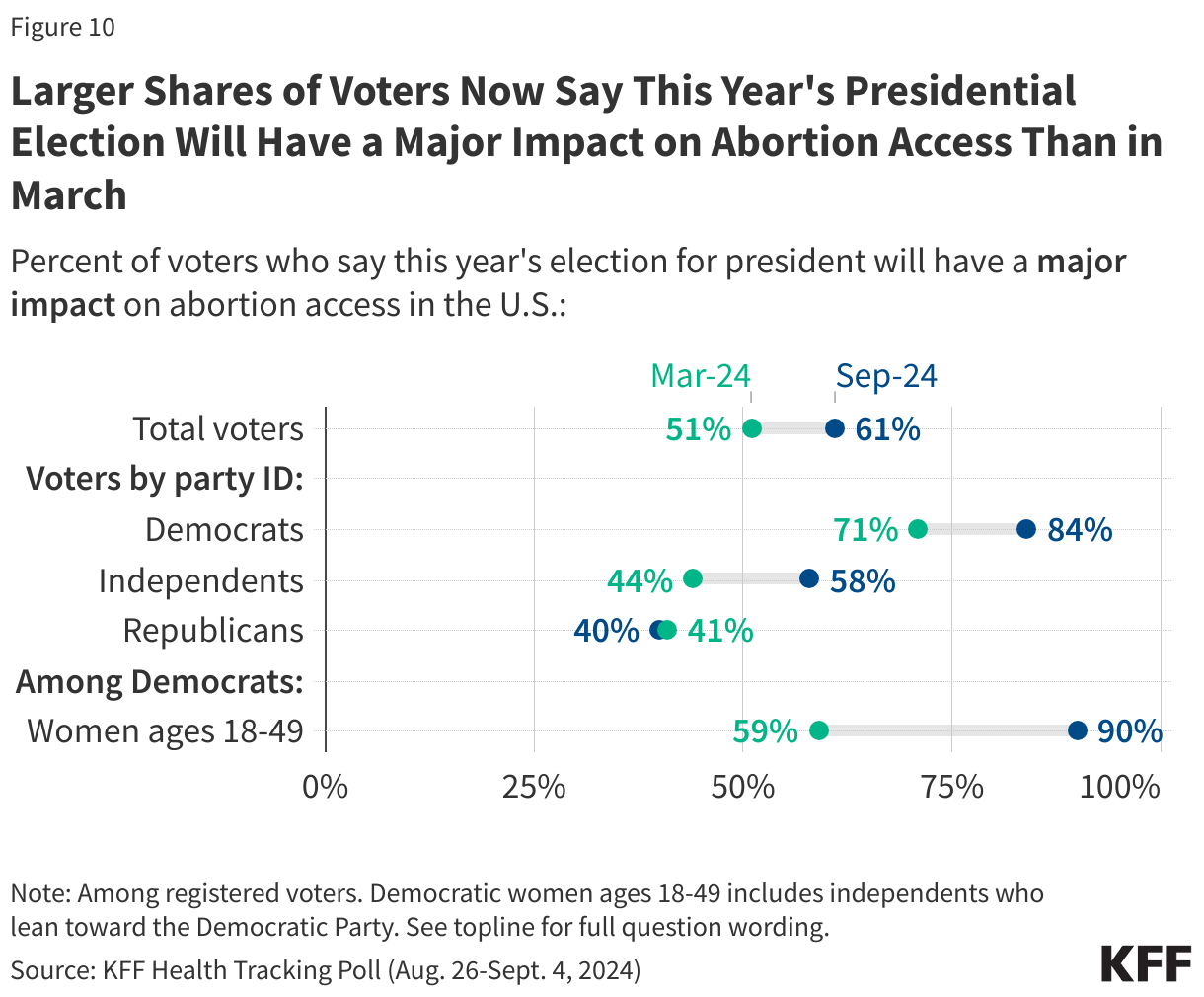
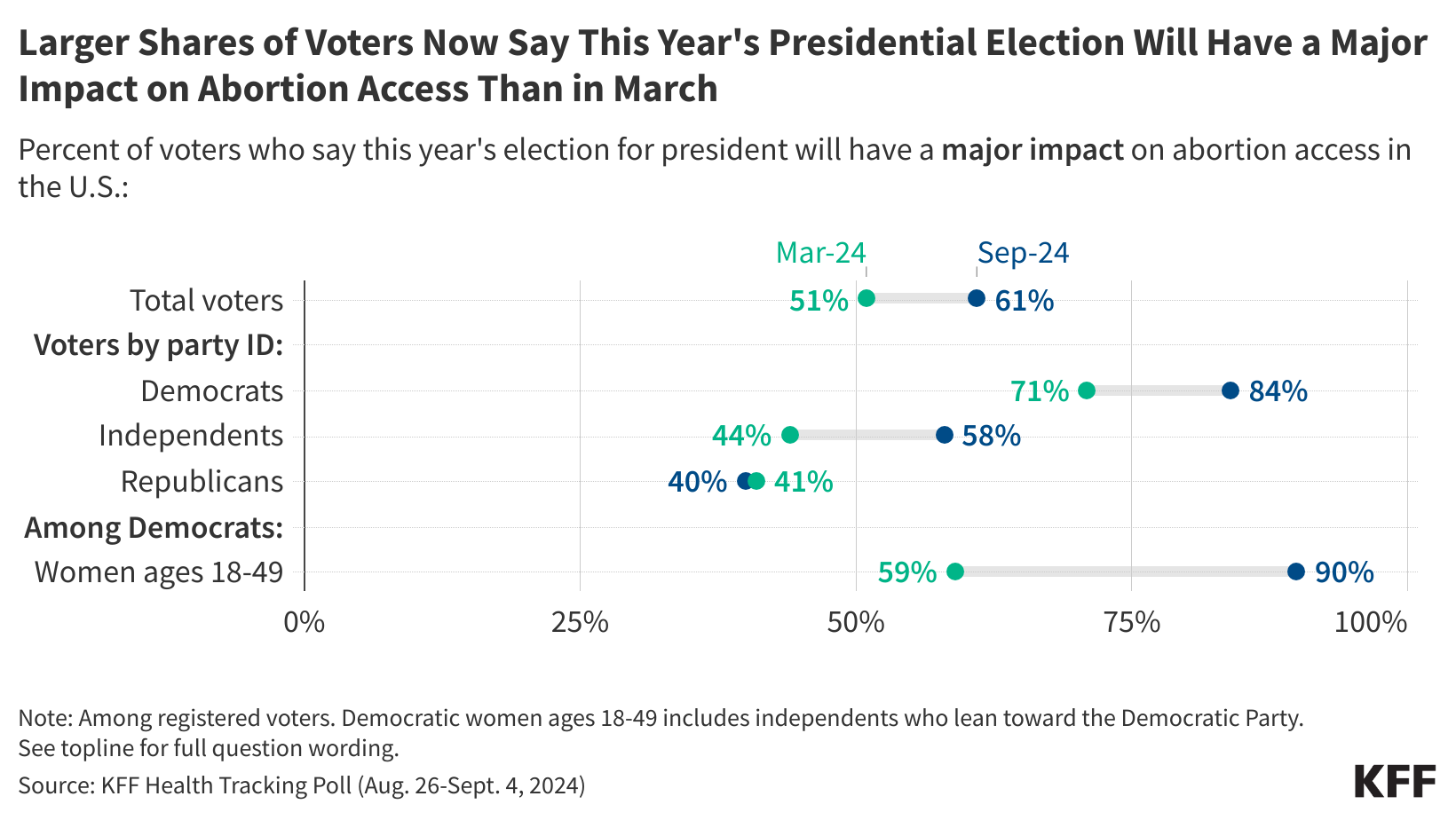
A larger share of voters now say that this election will have a “major” impact on abortion access than the share who said so in March of this year when President Biden was still on the ballot, perhaps reflecting the current president’s uneasiness with the issue. Currently, six in ten (61%) voters think this election will have a “major” impact, compared to about half (51%) in March. Some of the largest changes have been among independent voters and Democratic voters, with 84% of Democratic voters now saying the presidential election will have a major impact on abortion access, up from 71% in March. Similarly, 58% of independent voters say the same, a 14-percentage point increase from 44% in March. The share of Republican voters who say the election will have a major impact has remain unchanged.
Democratic and Democratic-leaning independent women voters of reproductive age (ages 18-49) are also now placing a higher emphasis on this election’s impact on abortion access. In the most recent tracking poll, nine in ten Democratic women under age 50 now say this year’s presidential election will have a major impact on abortion access in the U.S., compared to just 59% who said the same in March of this year.
Six In Ten Voters Want Roe Protections Restored
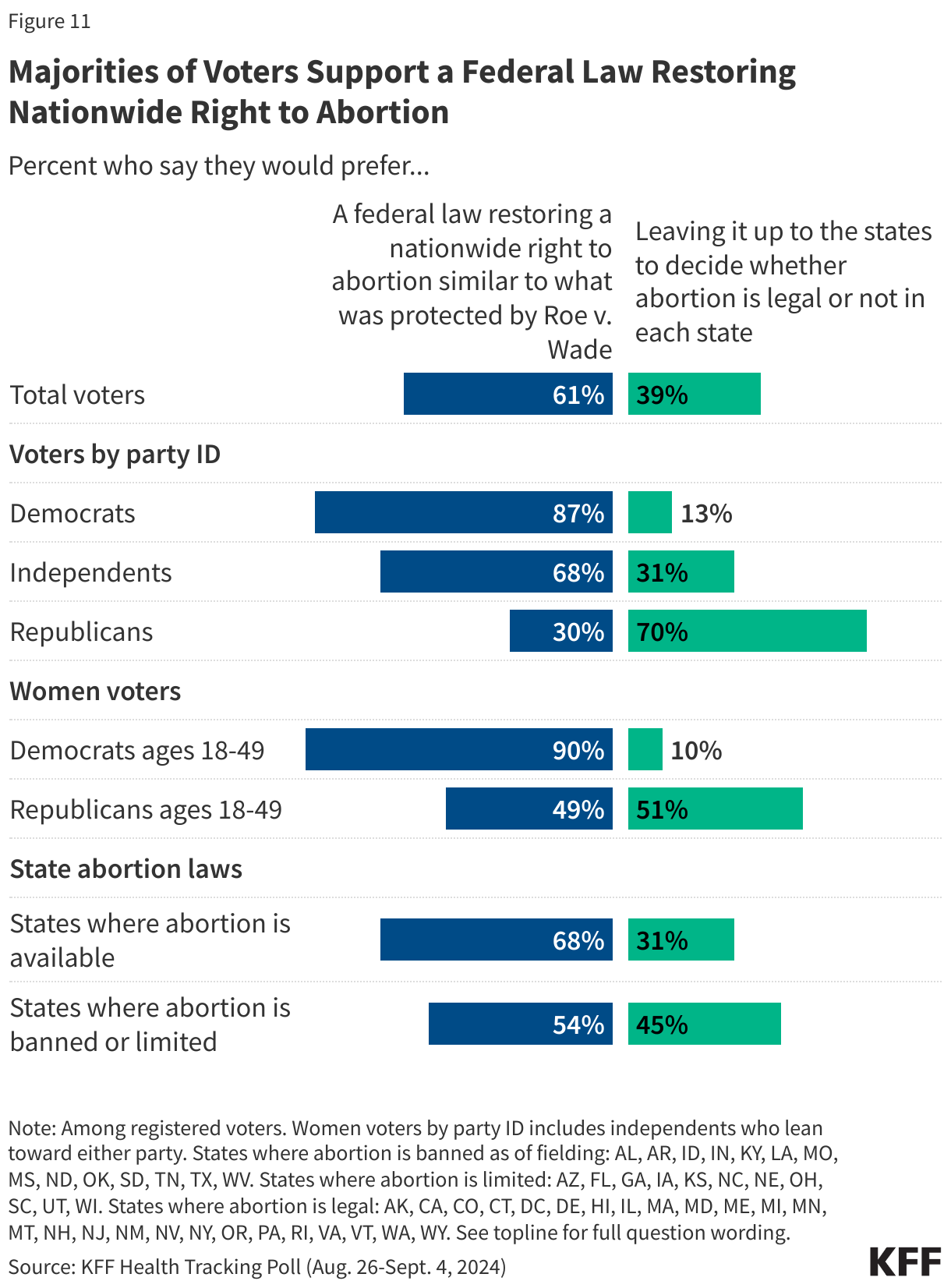
Six in ten (61%) voters would prefer a federal law restoring a nationwide right to abortion, similar to what was protected by Roe v. Wade, while four in ten (39%) would prefer to leave it up to the states to decide whether abortion is legal or not in each state.
Majorities of both Democratic voters and independent voters would prefer a federal law restoring a nationwide right to abortion, with nearly nine in ten (87%) Democratic voters and two-thirds (68%) of independent voters who say so. Seven in ten Republican voters would prefer leaving abortion laws up to the states.
Nine in ten Democratic and Democratic-leaning women voters who are of reproductive age support restoring a federal law for a nationwide right to abortion, while Republican women voters of reproductive age are more divided with similar shares saying they would prefer a federal law restoring a nationwide right to abortion (49%) or leaving it up to the states (51%).
Nearly seven in ten voters who live in states where abortion is legal and available support a federal law restoring a nationwide right to abortion (68%), as do a majority of voters living in states where abortion is banned or limited (54%).
This is especially important as ten states are set to have voters cast ballots on abortion-related measures in the 2024 election. In those states, 62% of voters say they would prefer to have a federal law restoring a nationwide right to abortion similar to what was protected by Roe.
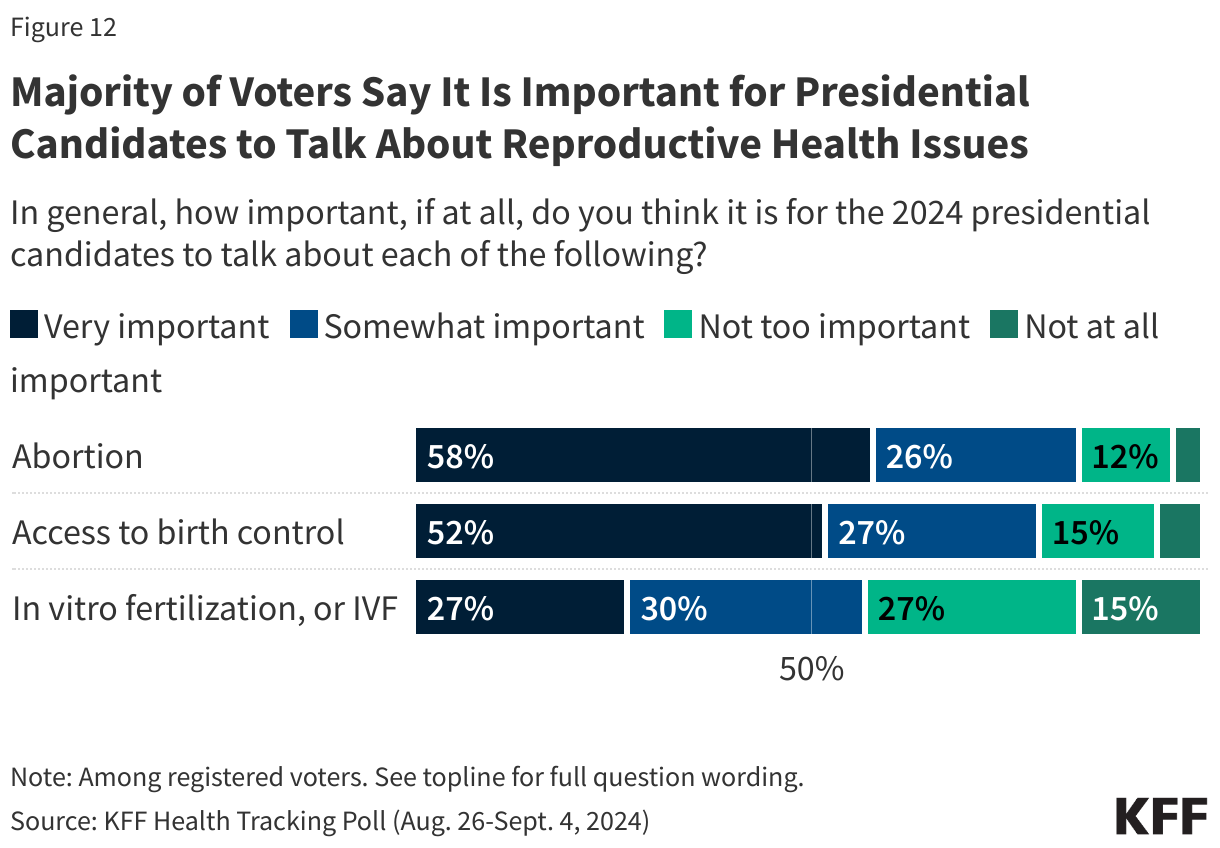
As the presidential campaigns continue, a majority of voters say it is important for the 2024 presidential candidates to talk about abortion (84%), access to birth control (79%), and in vitro fertilization, or IVF, (57%) on the campaign trail.
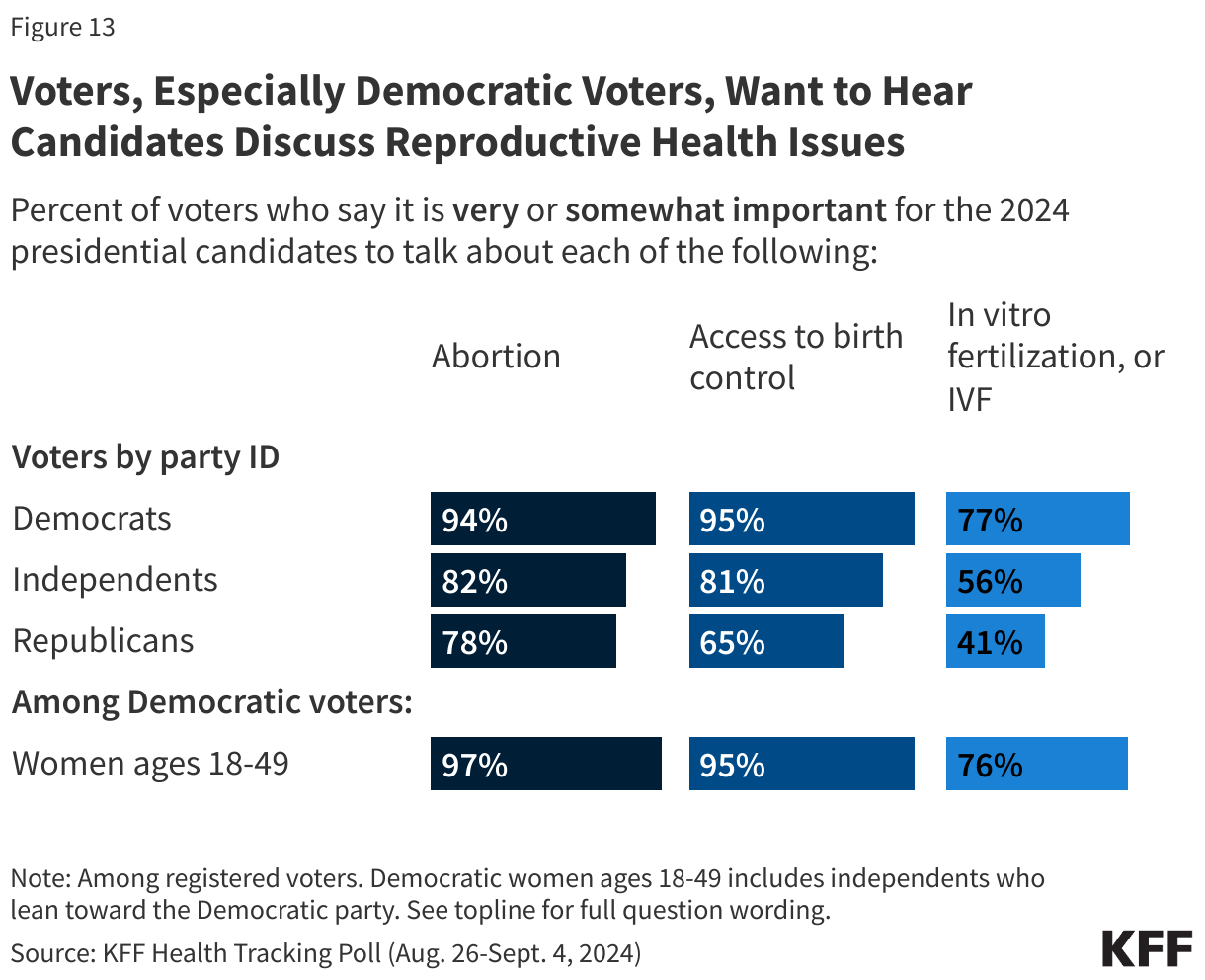
At least three-quarters of Democratic voters say it is either “very important” or “somewhat important” for the candidates to talk about each of these issues, as do a majority of independent voters. A majority of Republican voters agree, albeit to a lesser degree, that it is important for the presidential candidates to discuss abortion and birth control access, but less than half say the same about IVF.
At least nine in ten Democratic and Democratic-leaning women of reproductive age say it is important for the candidates to discuss abortion (97%) and access to birth control (95%) on the campaign trail, and three quarters (76%) say it is important for the candidates to talk about IVF.
Methodology
This KFF Health Tracking Poll/Health Misinformation Tracking Poll was designed and analyzed by public opinion researchers at KFF. The survey was conducted August 26-September 4, 2024, online and by telephone among a nationally representative sample of 1,312 U.S. adults in English (1,244) and in Spanish (68). The sample includes 1,028 adults (n=53 in Spanish) reached through the SSRS Opinion Panel either online (n=1,018) or over the phone (n=18). The SSRS Opinion Panel is a nationally representative probability-based panel where panel members are recruited randomly in one of two ways: (a) Through invitations mailed to respondents randomly sampled from an Address-Based Sample (ABS) provided by Marketing Systems Groups (MSG) through the U.S. Postal Service’s Computerized Delivery Sequence (CDS); (b) from a dual-frame random digit dial (RDD) sample provided by MSG. For the online panel component, invitations were sent to panel members by email followed by up to three reminder emails.
Another 284 (n=15 in Spanish) interviews were conducted from a random digit dial telephone sample of prepaid cell phone numbers obtained through MSG. Phone numbers used for the prepaid cell phone component were randomly generated from a cell phone sampling frame with disproportionate stratification aimed at reaching Hispanic and non-Hispanic Black respondents. Stratification was based on incidence of the race/ethnicity groups within each frame.
Respondents in the phone samples received a $15 incentive via a check received by mail, and web respondents received a $5 electronic gift card incentive (some harder-to-reach groups received a $10 electronic gift card). In order to ensure data quality, cases were removed if they failed two or more quality checks: (1) attention check questions in the online version of the questionnaire, (2) had over 30% item non-response, or (3) had a length less than one quarter of the mean length by mode. Based on this criterion, no cases were removed.
The combined cell phone and panel samples were weighted to match the sample’s demographics to the national U.S. adult population using data from the Census Bureau’s 2022 Current Population Survey (CPS), September 2021 Volunteering and Civic Life Supplement data from the CPS, and the 2024 KFF Benchmarking Survey with ABS and prepaid cell phone samples. The demographic variables included in weighting for the general population sample are gender, age, education, race/ethnicity, region, civic engagement, frequency of internet use, political party identification by race/ethnicity, and education. The sample of registered voters was weighted separately to match the U.S. registered voter population using the same parameters above derived from the 2024 KFF Benchmarking Survey. Both weights account for differences in the probability of selection for each sample type (prepaid cell phone and panel). This includes adjustment for the sample design and geographic stratification of the cell phone sample, within household probability of selection, and the design of the panel-recruitment procedure.
The margin of sampling error including the design effect for the full sample is plus or minus 4 percentage points and is plus or minus 4 percentage points for registered voters. Numbers of respondents and margins of sampling error for key subgroups are shown in the table below. For results based on other subgroups, the margin of sampling error may be higher. Sample sizes and margins of sampling error for other subgroups are available by request. Sampling error is only one of many potential sources of error and there may be other unmeasured error in this or any other public opinion poll. KFF public opinion and survey research is a charter member of the Transparency Initiative of the American Association for Public Opinion Research.
Most voters (61%) now say that the outcome of this year’s presidential election will have a major impact on access to abortion in this country – up 10 percentage points from March, a new KFF Health Tracking Poll finds.
The shift has occurred mainly among Democratic and independent voters over a period of time that saw Vice President Harris become the Democratic presidential nominee and make protecting abortion access a key component of her campaign.
Abortion resonates most with Democratic women voters of reproductive age (under age 50). About one in five (21%) in this group name abortion as their top voting issue.
Democratic women voters of reproductive age overwhelmingly (90%) say the presidential election will have a major impact on abortion access – up 31 percentage points from six months ago. The vast majority (93%) of this group of voters say that abortion should be legal in all or most cases.
Among all voters, Vice President Harris holds a large advantage over former President Trump on who they trust to do a better job on the abortion issue (53% vs. 34%). That’s a bigger lead on the issue than President Biden enjoyed earlier this year on a similar question before he dropped out of the race.
Vice President Harris also holds a narrower lead on trust to handle health care costs (48% vs. 39%). Independent voters give Harris an even bigger edge on health costs.
Meanwhile, former President Trump holds a large trust advantage among all voters on two major non-health issues: the economy and inflation (52% vs. 37%) and immigration and border security (54% vs. 36%). Independents also give the edge to former President Trump on these issues.
Among Health Issues, Voters Are Most Eager to Hear the Candidates Address Costs
Ahead of tonight’s presidential debate, voters identify costs as the health care issue that they most want former President Trump and Vice President Harris to talk about, likely reflecting broader concerns about the economy and inflation, which remains voters’ top overall issue.
Among Republicans and Republican-leaning independents, nearly half (45%) say they most want former President Trump to talk about health costs, offering responses like prescription drug costs and insurance premiums. A similar share of Democrats and Democratic-leaning independents (42%) say they most want Vice President Harris to talk about health care costs.
Other findings include:
Among all voters, six in ten (61%) say they would prefer a federal law restoring a national right to abortion similar to what existed under Roe v. Wade than leaving it up to the states to decide whether abortion is legal or not (39%). In the 10 states where voters could decide abortion ballot initiatives, voters prefer a federal law to leaving it up to the states by a similar margin (62% vs. 38%).
Among Democratic women voters under age 50, the vast majority (90%) say they favor a federal law restoring a nationwide right to abortion similar to what existed prior to the Supreme Court’s 2022 decision overturning its Roe v. Wade precedent.
When asked directly about these issues, voters say it is important for the presidential candidates to talk about abortion (84%), access to birth control (79%), and In vitro fertilization, or IVF, (57%) on the campaign trail. At least three-quarters of Democratic voters say it is important for the candidates to talk about each of these issues, as do most independent voters. Most Republican voters also say it is important for the candidates to discuss abortion and birth control access, but less than half say the same about IVF.
Designed and analyzed by public opinion researchers at KFF, the survey was conducted August 26-Sept. 4, 2024, online and by telephone among a nationally representative sample of 1,312 U.S. adults, including 1,084 registered voters, in English and in Spanish. The margin of sampling error is plus or minus 4 percentage points for the full sample and among registered voters. For results based on other subgroups, the margin of sampling error may be higher.
This report, based on analysis of KFF’s 2023 Racism, Discrimination, and Health Survey, focuses on the experiences of people who have been previously incarcerated and examines their social and economic circumstances as well as their physical and mental health and access to health care. The findings aim to fill in a gap in publicly available data on the experiences of people who were previously incarcerated. The goal is to provide increased understanding of the health and other basic needs of people who were previously incarcerated, rather than identifying the role incarceration plays in driving these and other outcomes.
The analysis shows that people with previous experience with incarceration have significant health needs and limited access to resources, including health care, and experience more social isolation. Some key findings include:
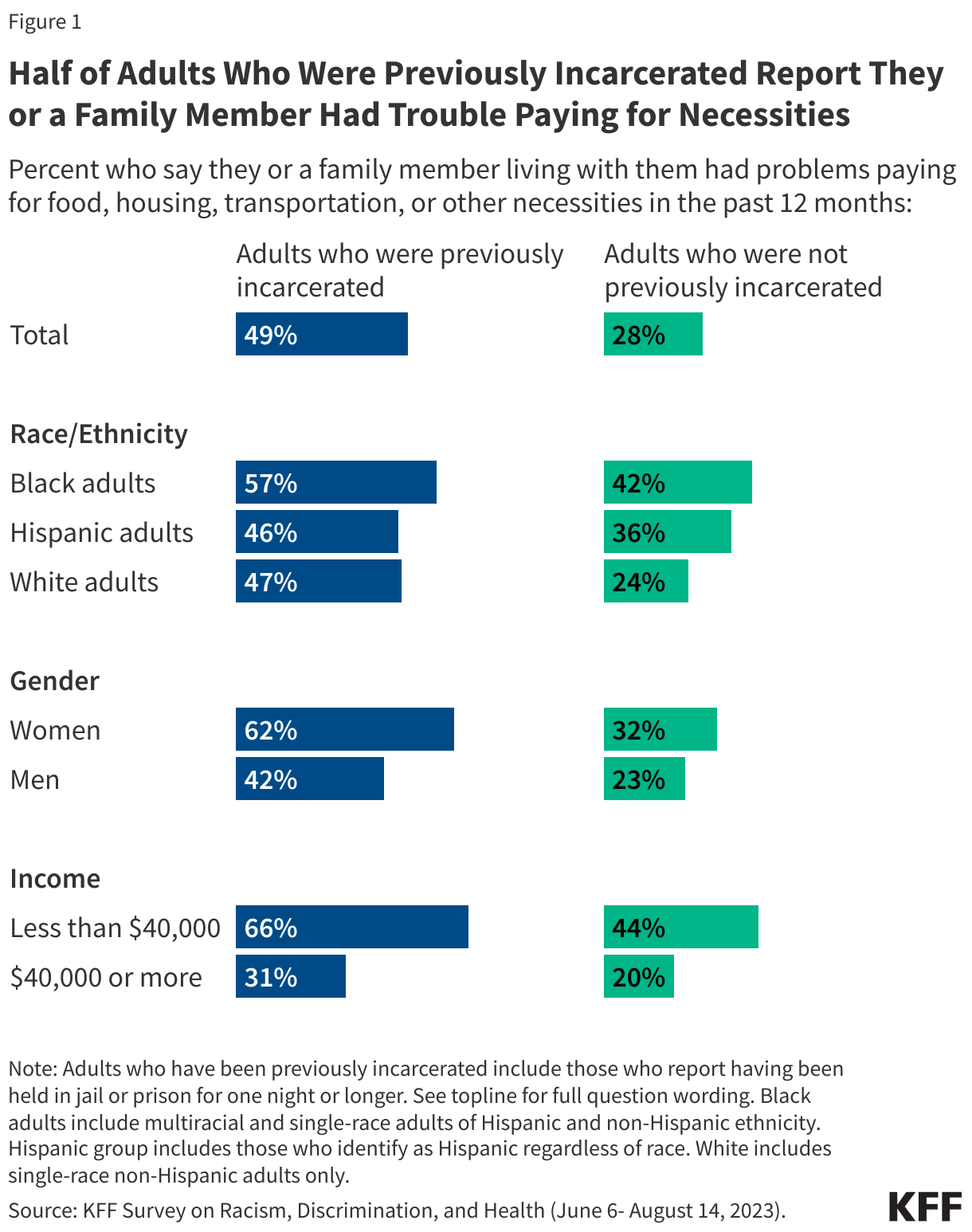
Adults with prior incarceration experience report many financial challenges, including half who say they have problems affording basic living expenses. These financial hardships are particularly pronounced among previously incarcerated adults who are lower income (household incomes below $40,000) (66%), women (62%), or Black (57%). Yet, the experiences are not solely explained by the fact that many previously incarcerated adults have lower household incomes than their counterparts. When comparing the experiences among the lowest income individuals in both groups, previously incarcerated adults are more likely than those with similar incomes but no incarceration experience to report difficulty affording expenses.
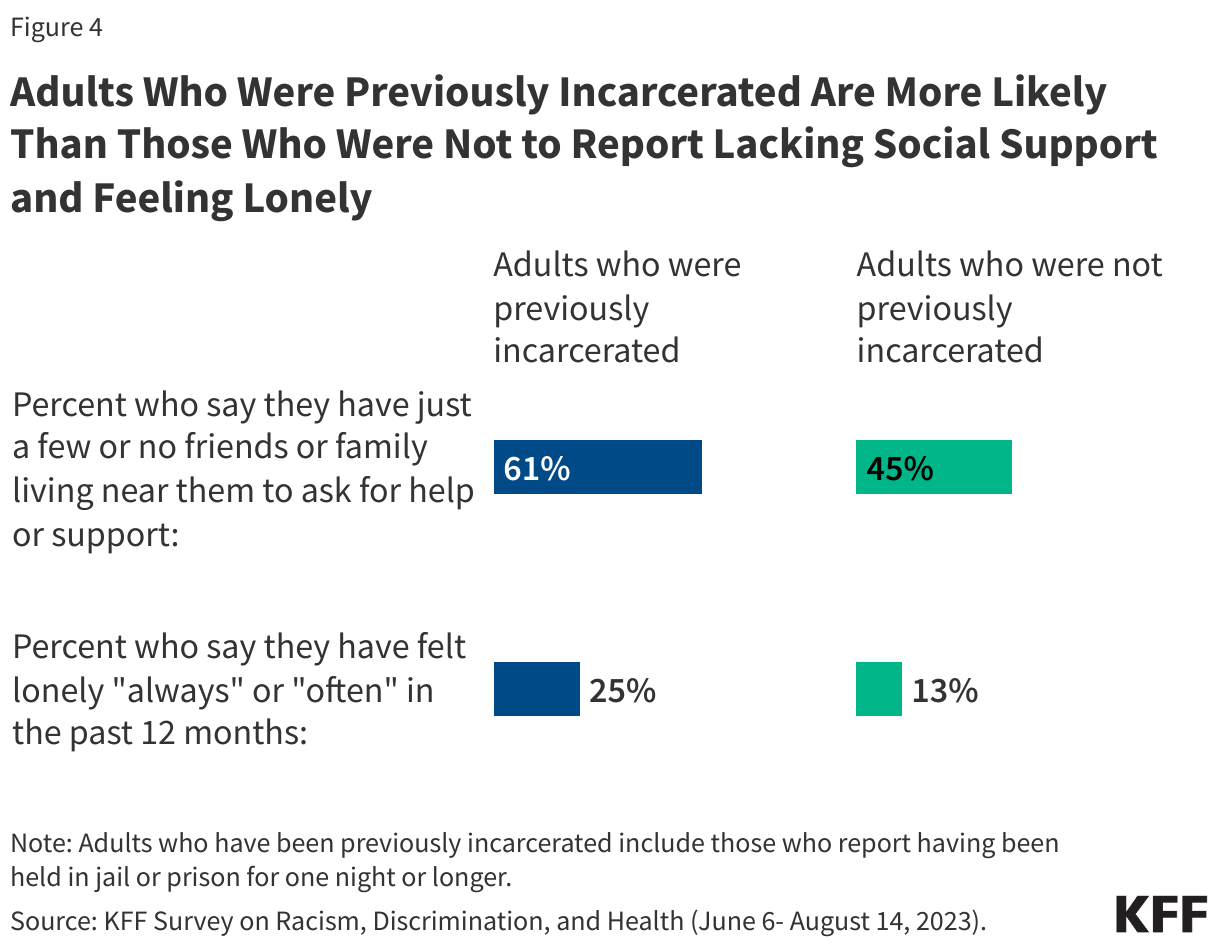
Social support networks may be particularly important for people who have interactions with the criminal justice system, yet six in ten (61%) of those with prior incarceration experience say they have just a few or no friends or family living near them to ask for help or support. In addition, a quarter of previously incarcerated individuals say they have felt lonely either “always” or “often” in the past twelve months, almost twice the share among those without previous incarceration experience (13%).
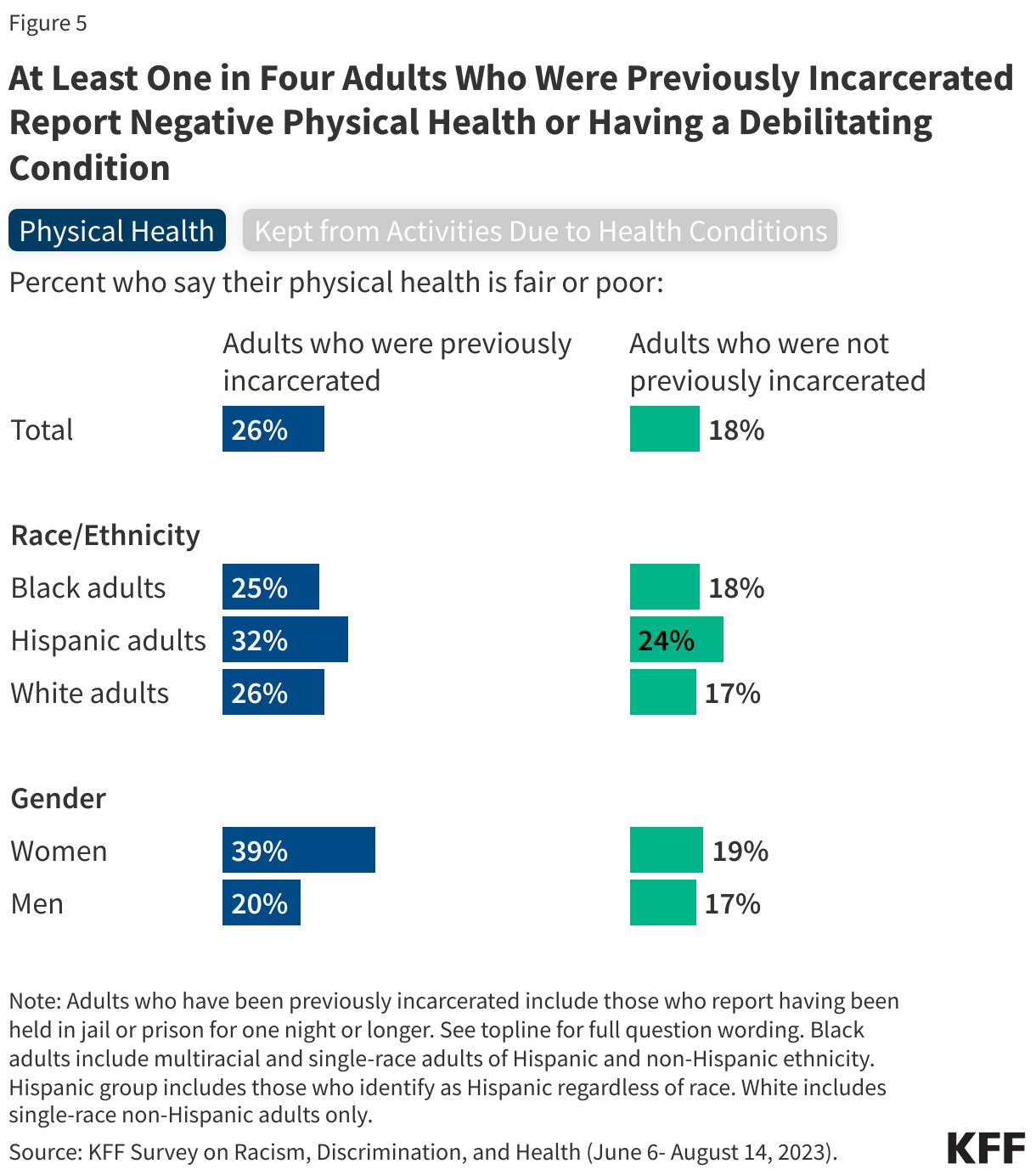
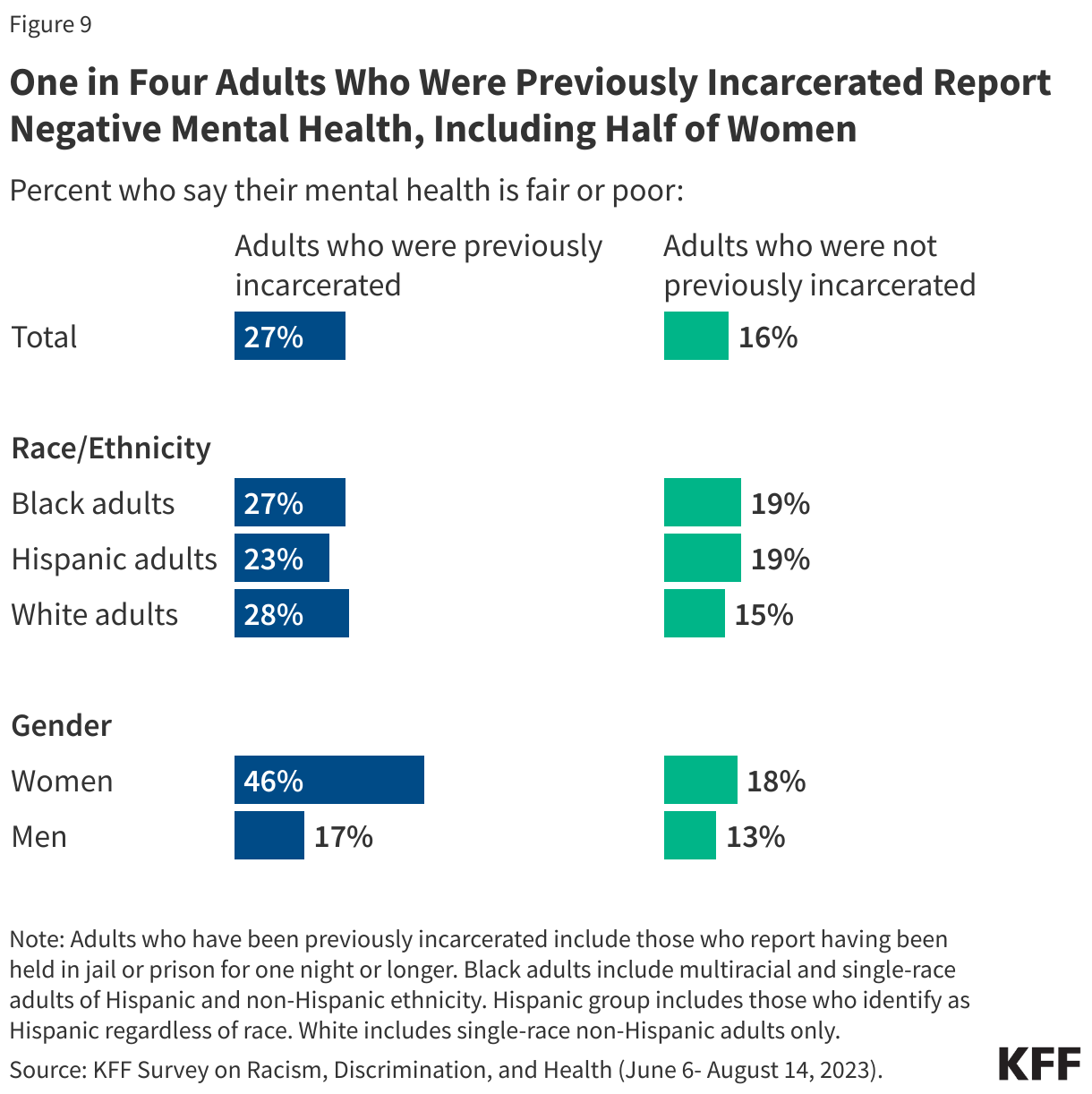
A substantial share of adults who have been previously incarcerated report “fair” or “poor” physical health and mental health, and the disparity between those with incarceration experience and those without is even more pronounced among women. Overall, a quarter of those who have been incarcerated say their physical health is “fair” or “poor,” increasing to four in ten (39%) among women who have spent a night in jail or prison. One in four (27%) previously incarcerated adults say their mental health is “fair” or “poor,” increasing to almost half (46%) of women who have been previously incarcerated.
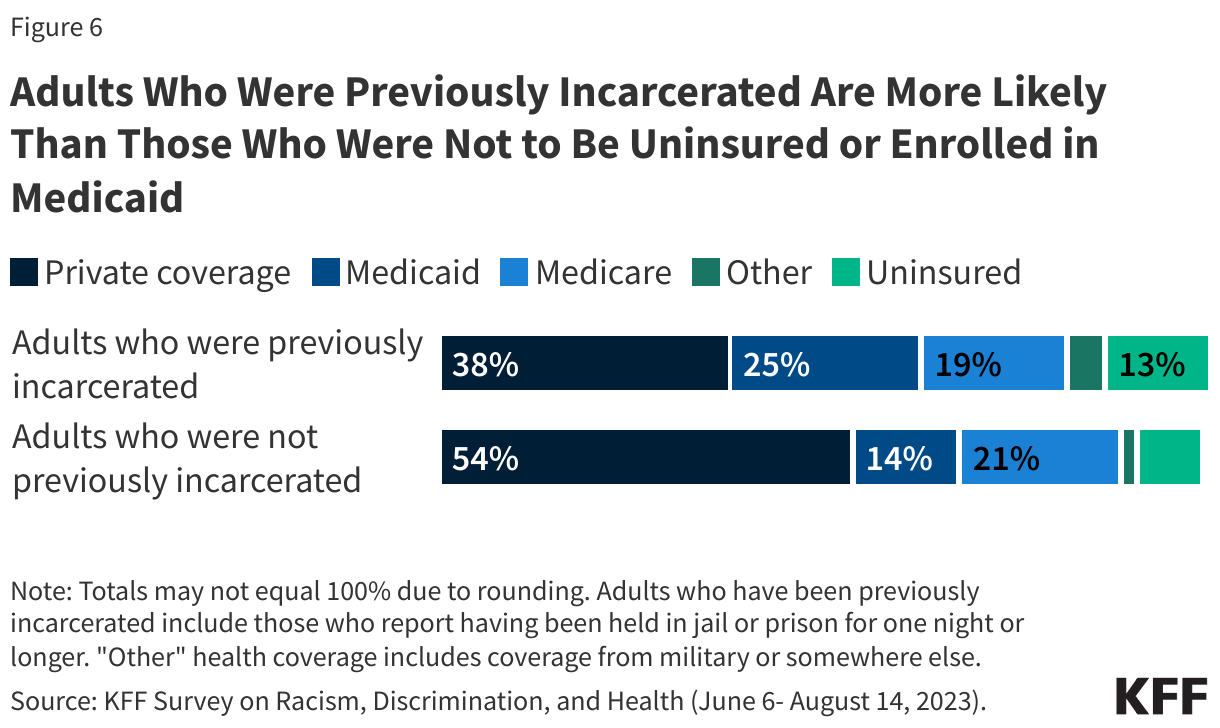
Reflecting their lower income levels, Medicaid covers about a quarter (25%) of previously incarcerated adults compared with 14% of adults without previous incarceration experience. Although Medicaid coverage helps to fill gaps in private coverage for previously incarcerated adults, they also remain more likely than adults without incarceration experience to report being uninsured (13% vs. 8%).
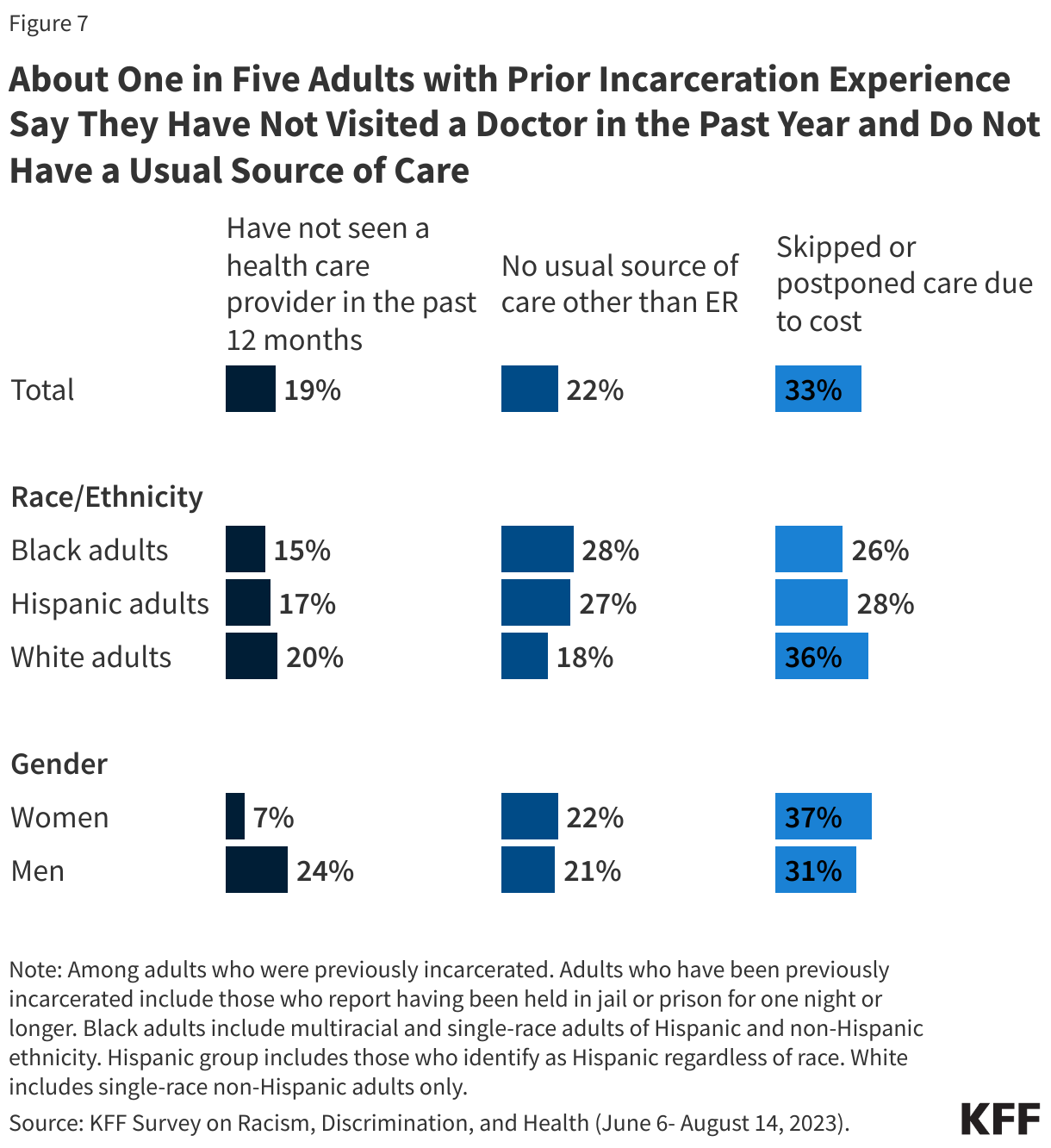
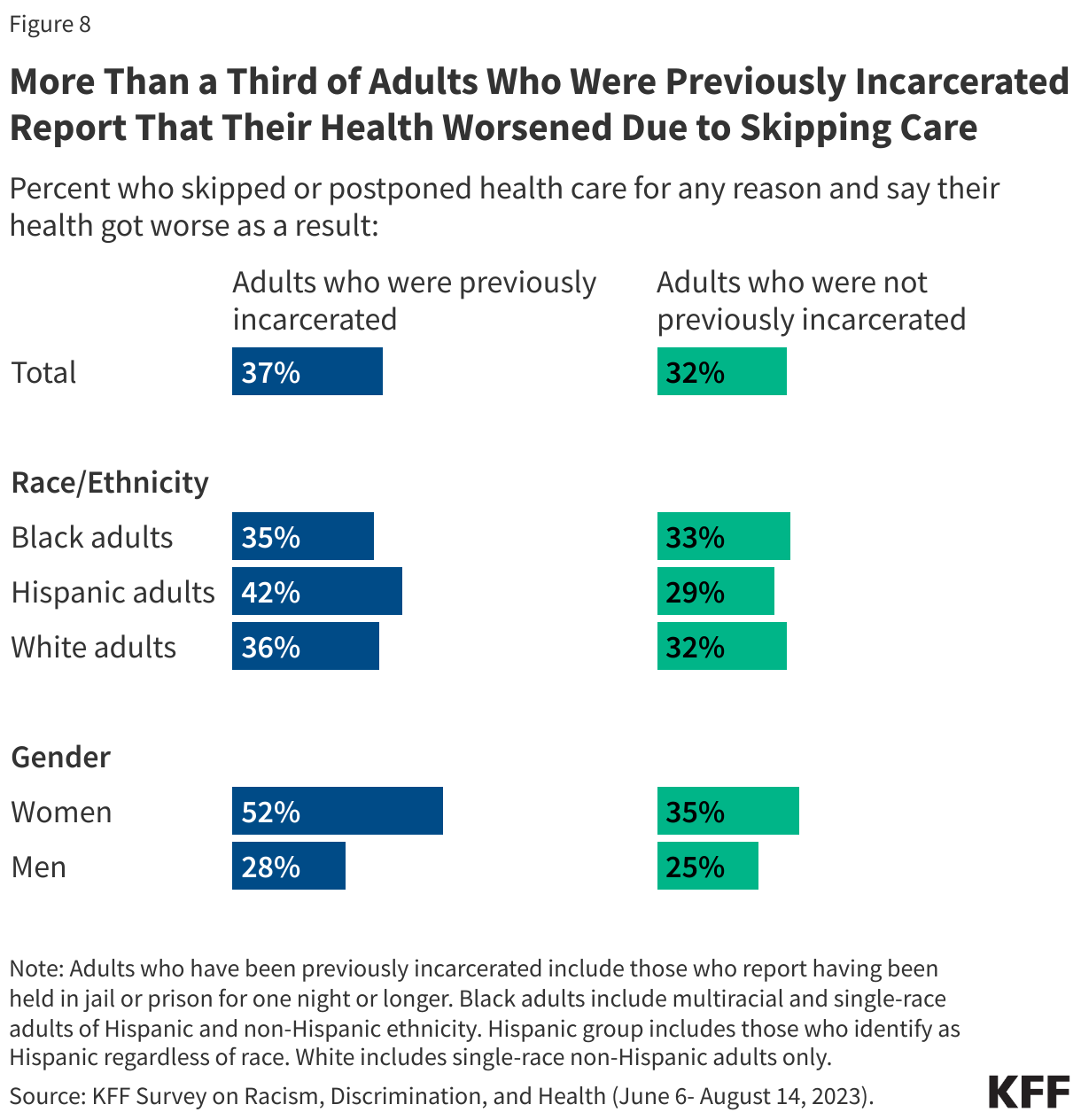
Despite significant health needs, one in five (22%) adults with previous incarceration experience say they do not have a usual source of care or go to the emergency room when they are sick or need advice about their health. One in three of those with previous incarceration experience say they skipped or postponed health care because of costs in the past year. This includes nearly four in ten (37%) women with prior incarceration experience.
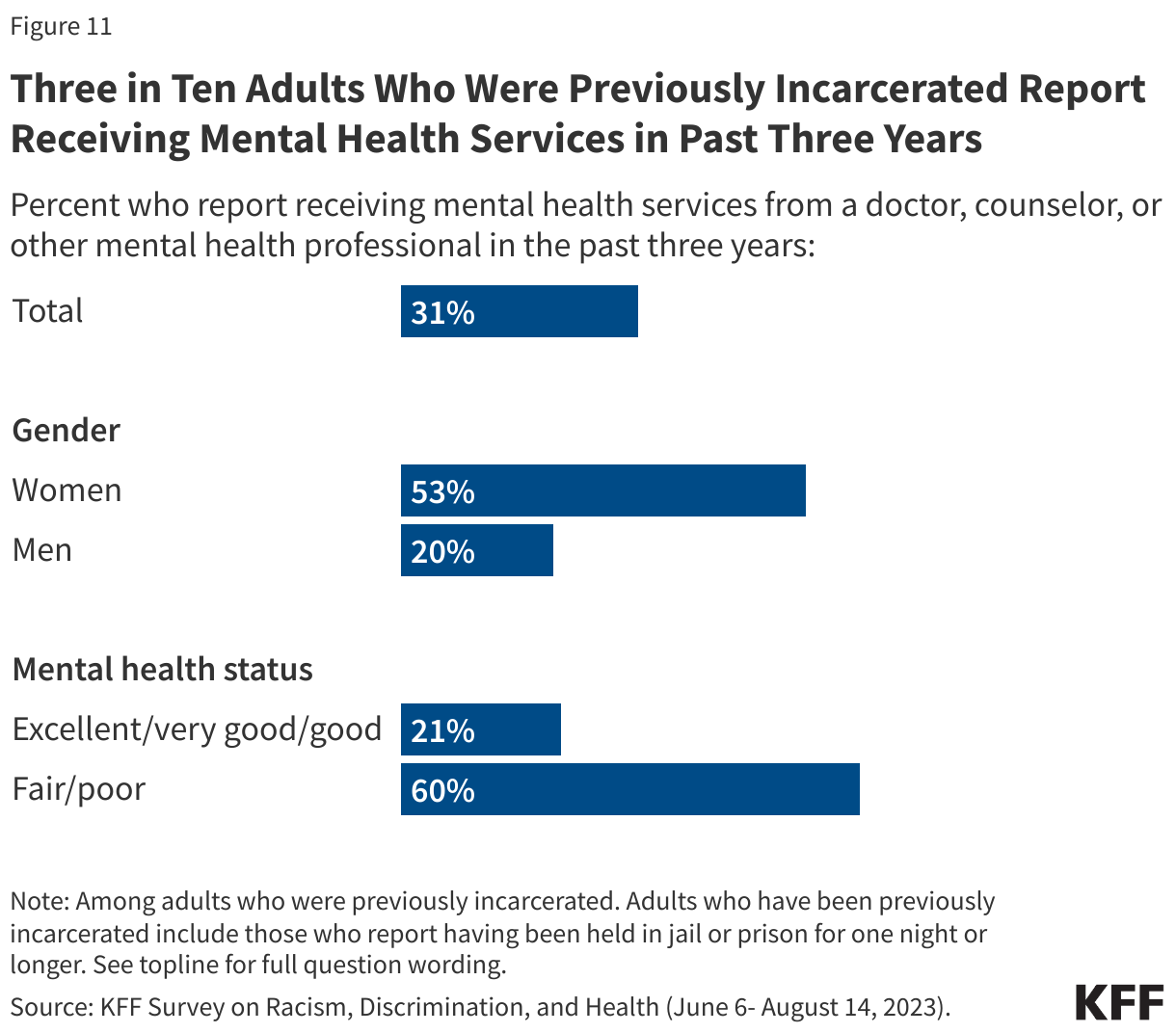
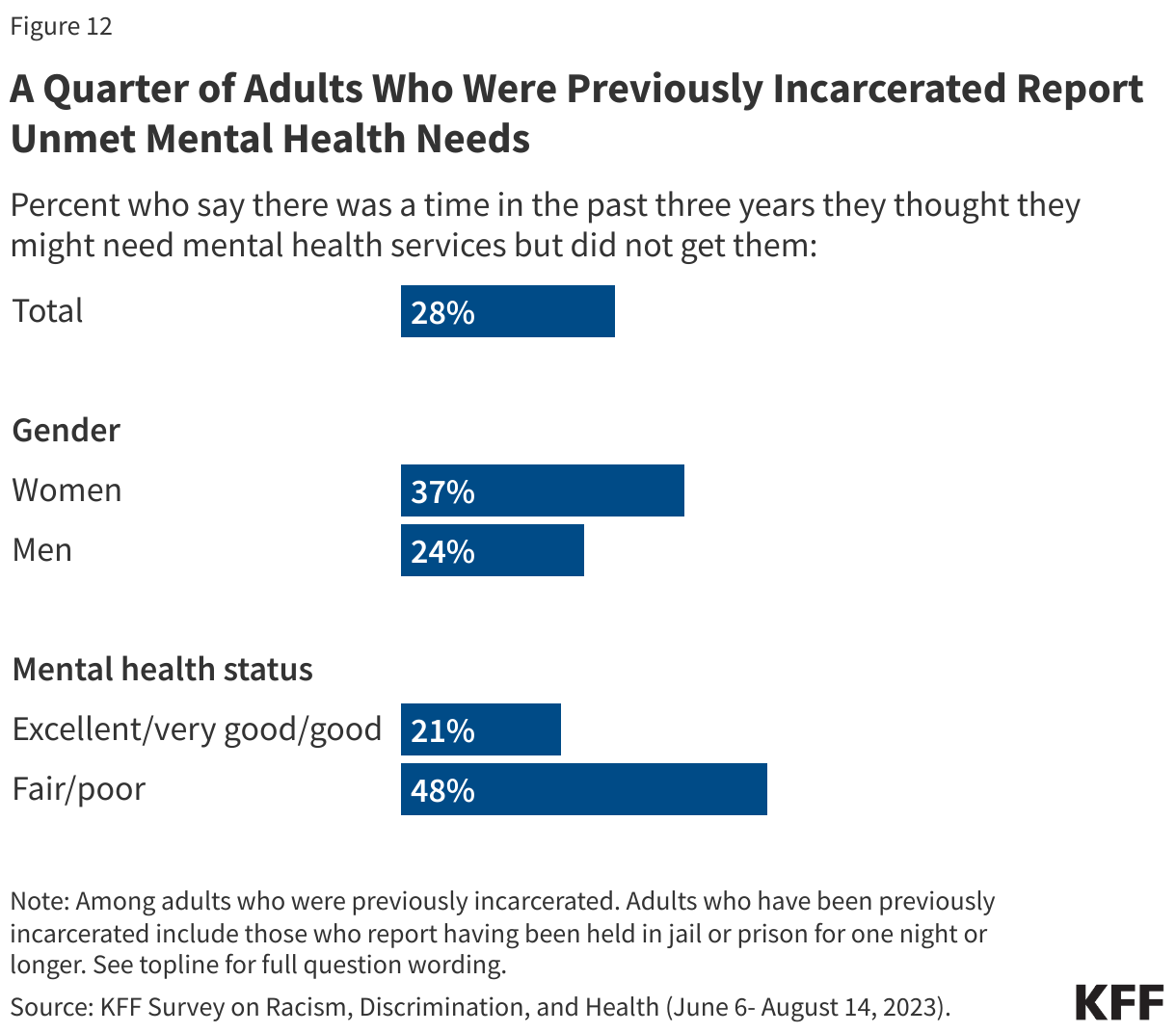
About three in ten (31%) adults with previous incarceration experience say they have received mental health services from a doctor, counselor, or other mental health professional in the last 3 years. Among those with incarceration experience, women are more than twice as likely as men to say they have received such services (53% vs. 20%), likely reflecting the higher share of women in this group who report mental health challenges. But there are still unmet needs, with almost half of those previously incarcerated who report having fair or poor mental health saying there was a time in the past three years when they needed mental health services or medication but didn’t get them.
Who Are Previously Incarcerated Adults?
One in seven (14%) U.S. adults say they have ever been held in jail or prison for one night or longer. This broad definition of previously incarcerated adults encompasses a range of experiences, including variations in how long people were incarcerated (from a single night to months or even years) and variations in how recently this experience occurred. Notably, it excludes adults who are currently incarcerated and should not be interpreted as representative of that population.
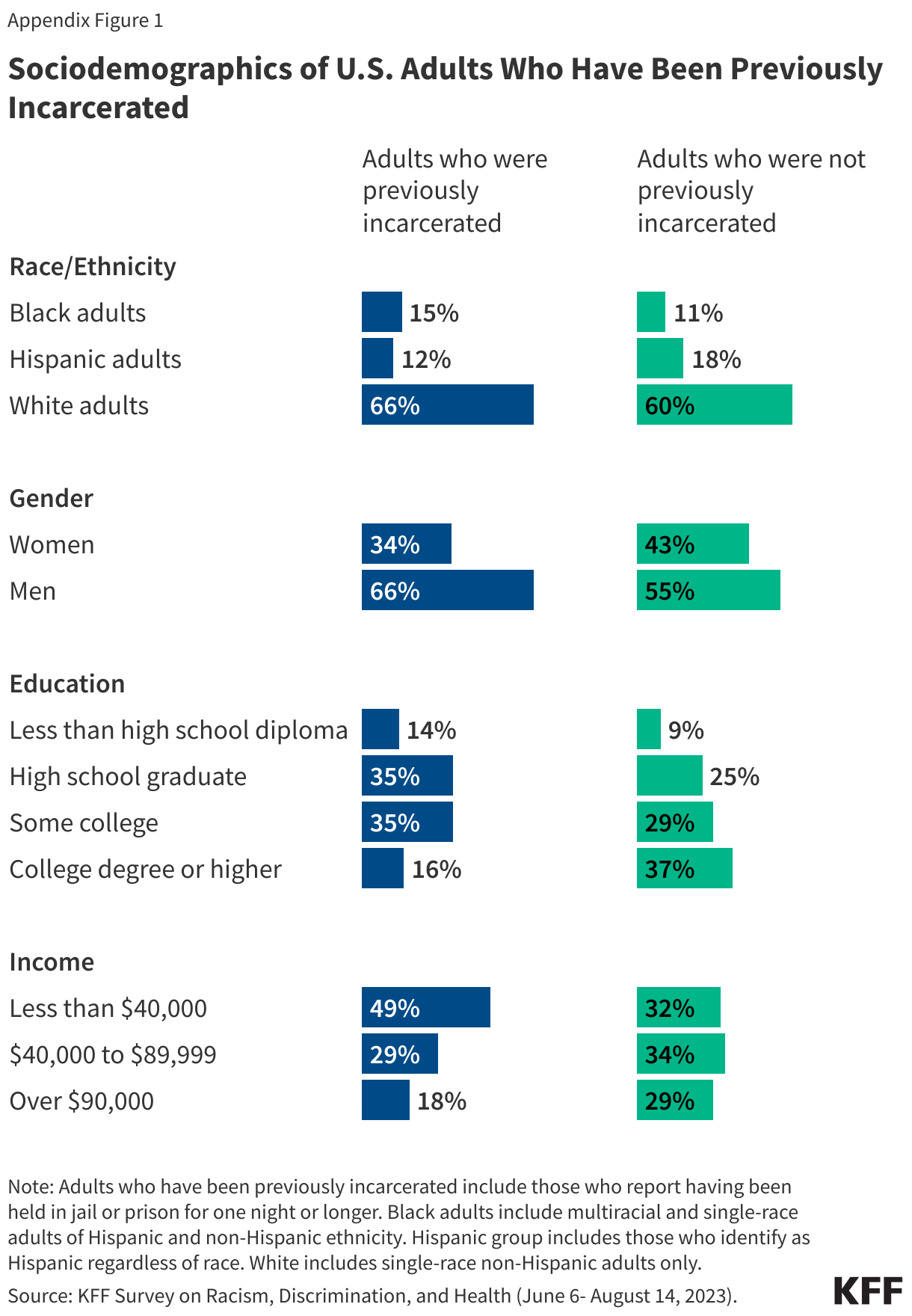
People with previous incarceration experience are more likely to identify as Black and/or American Indian and less likely to identify as Asian compared to those with no incarceration experience. While Black and Hispanic people make up disproportionate shares of the currently incarcerated population, these patterns are less pronounced among the group with any previous incarceration experience. This may be due to racial and ethnic disparities in federal sentencing.
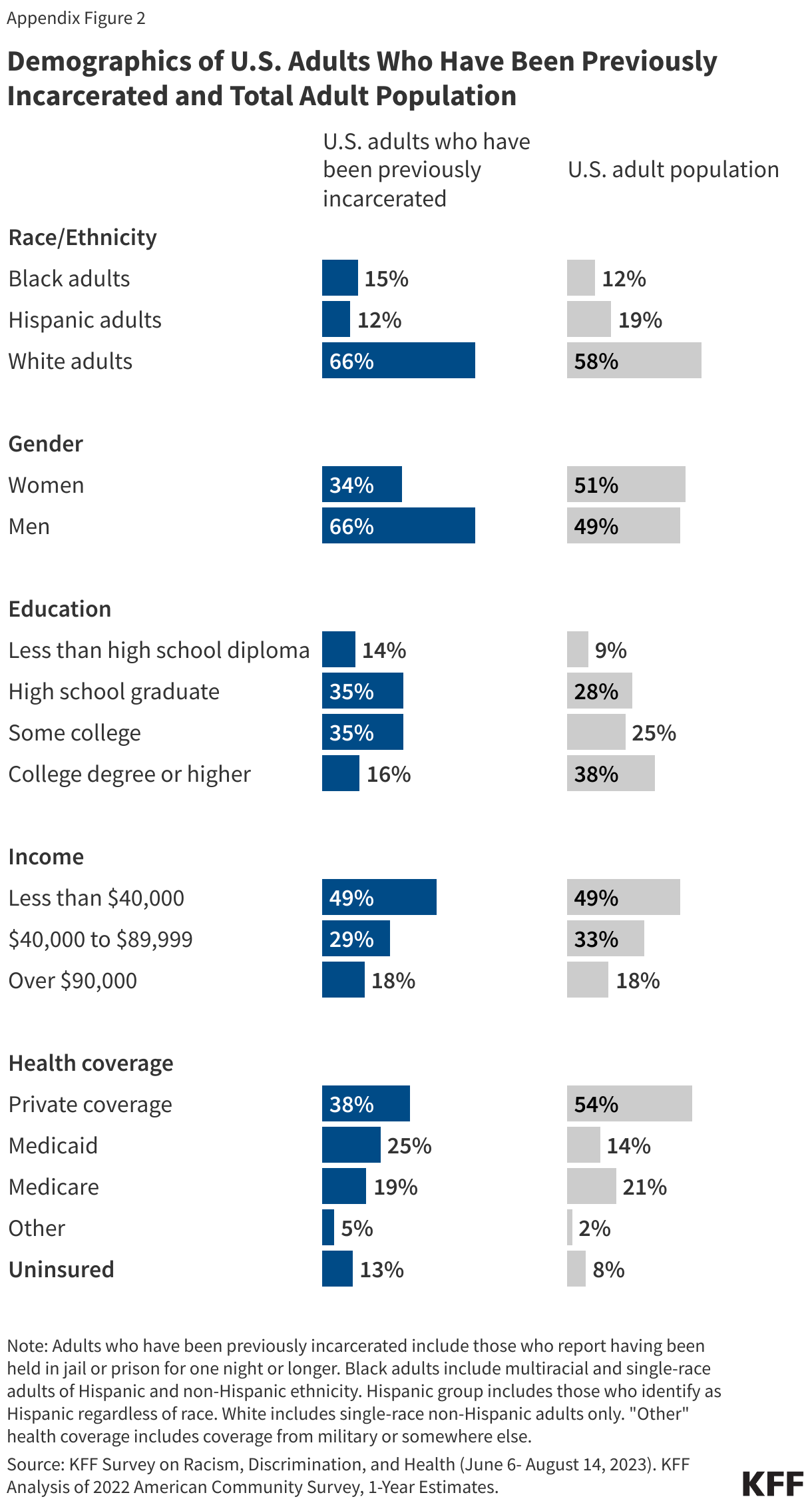
People who have been incarcerated are disproportionately male (66%), without a college degree (84%), and have incomes under $40,000 (49%). See Appendix Figure 1 for more details on the demographic profile of the population included in this analysis. Appendix Figure 2 compares estimates of this previously incarcerated definition across key demographic groups.
Economic and Social Challenges
Many adults with prior incarceration experience report facing financial challenges, including difficulty affording basic needs and paying their monthly bills. These challenges are particularly pronounced among certain groups of adults who previously incarcerated including those with lower incomes, those who are Black adults, and those who are women.
Half of adults who have been previously incarcerated say they or a family member living with them have had problems paying for food, housing, transportation, or other necessities in the past 12 months. The share rises to 57% of Black adults and 62% of women with prior incarceration experience. Overall, adults who have previously been incarcerated are more likely than those who have not to report problems paying for basic needs. While this in part reflects their lower incomes, even among adults with household incomes of less than $40,000, those who have been incarcerated are more likely to report problems paying for basic necessities than those who have not (66% vs. 44%).
Lower-income adults and women with previous experience with being incarcerated report difficulties affording expenses and securing housing.
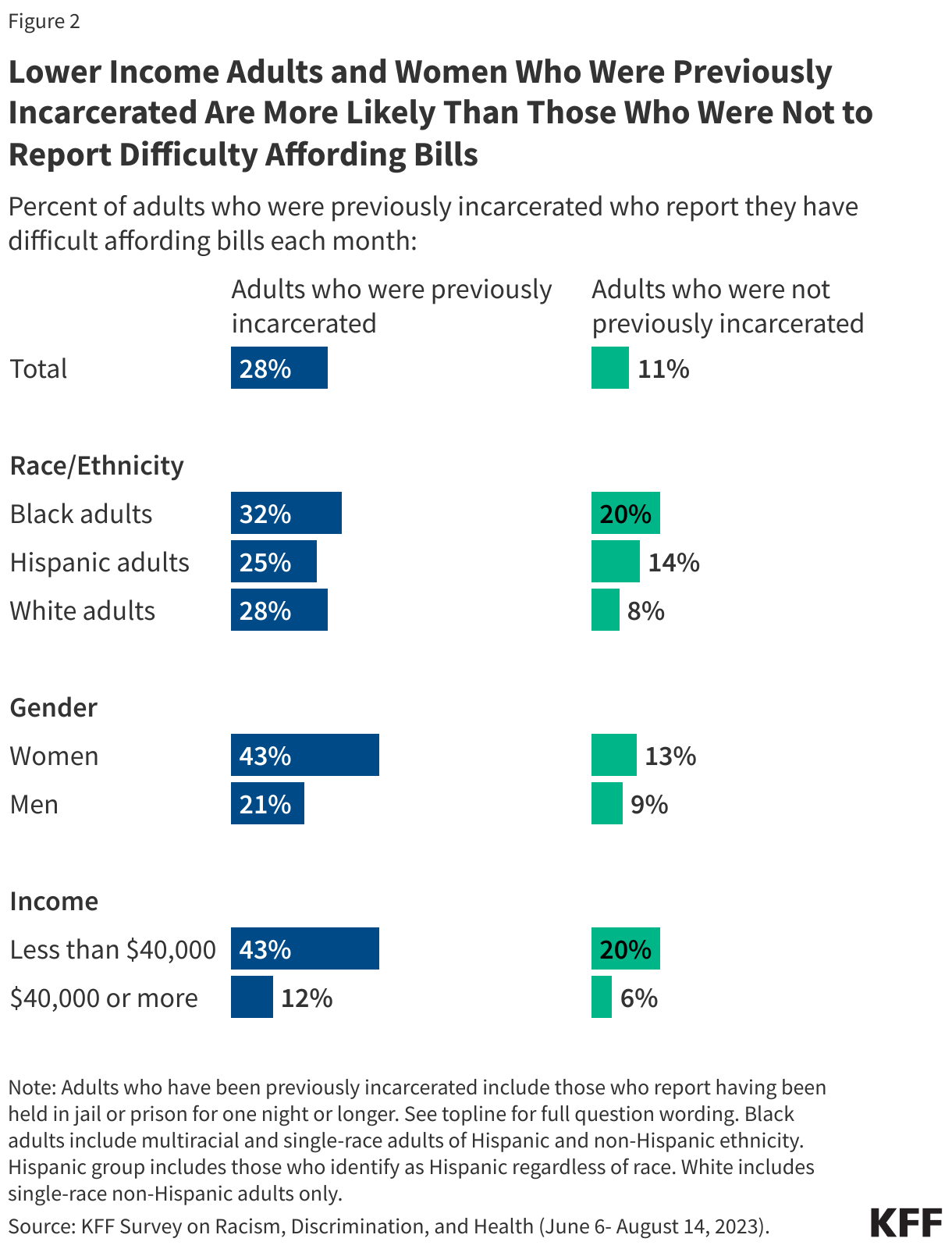
More than one in four adults who have been previously incarcerated say they have difficulty affording their bills each month rising to more than four in ten (43%) of those who have been previously incarcerated and have household incomes under $40,000. One in five (20%) of those earning similar incomes without incarceration experience say the same.
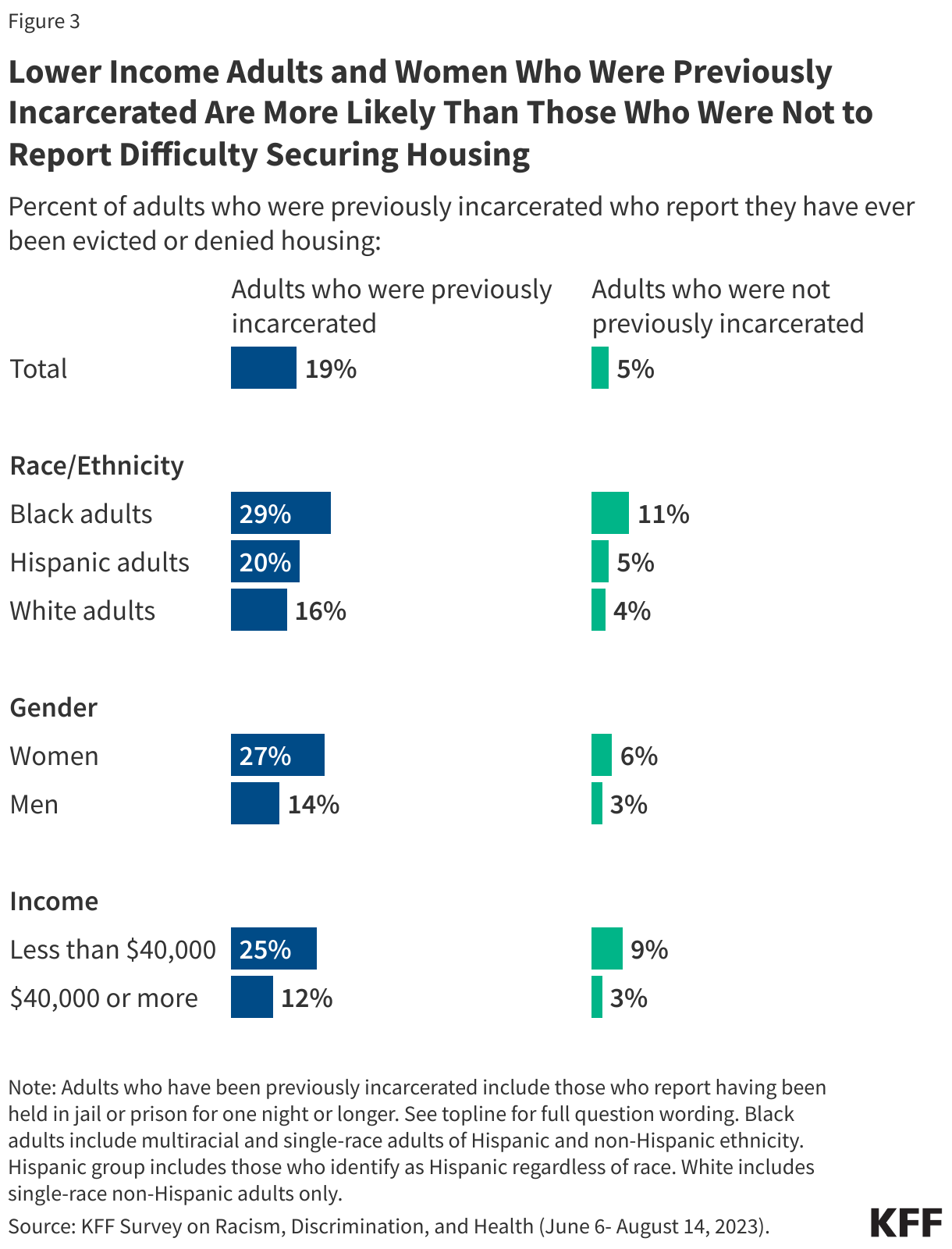
About one in five adults with previous experience being incarcerated report they have been evicted or denied housing, nearly four times the share of those without incarceration experience (19% v. 5%). This share rises among those with lower incomes, with one in four of those with household incomes under $40,000 saying they have been evicted or denied housing (compared to one in ten of those with similar income levels but without previous incarceration experience).
More than four in ten women with previous experience being incarcerated report difficulty affording their monthly bills and more than a quarter say they have ever been evicted or denied housing. The share of women who report such experiences is higher than the share of men with incarceration experience who report the same.
At least a quarter of previously incarcerated adults across race and ethnicity groups said they had difficulty affording bills each month (25% of Hispanic adults, 28% of White adults, and 32% of Black adults). About three in ten Black adults who were previously incarcerated also reported ever being evicted or denied housing as did one in five Hispanic adults and 16% of White adults.
Difficulty affording monthly bills or getting housing may reflect problems getting or keeping a job. One in four of those who have been previously incarcerated say in the past 12 months they or a family member living with them have had problems getting or keeping a job and 14% say they are currently unemployed.
Social Supports
Social support networks may be particularly important for people who have interactions with the criminal justice system, yet six in ten (61%) of those with prior incarceration experience say they have just a few or no friends or family living near them to ask for help or support. In addition, a quarter of previously incarcerated individuals say they have felt lonely either “always” or “often” in the past twelve months, almost twice the share among those without previous incarceration experience (13%). The share who report feeling lonely at least often increases to 42% of Black women who were previously incarcerated (compared to 20% of Black women with no incarceration experience).
Health and Health Care Access
One in four adults with previous incarceration experience report being in fair or poor physical health, and three in ten report having a disability or condition that prevents them from participating fully in work or other activities, including much higher shares among women than men.
About a quarter of those who have been incarcerated say their physical health is “fair” or “poor.” The share of previously incarcerated adults who report negative physical health increases to four in ten (39%) among women, twice the share of women without such experience who say the same (19%). About one in five men, regardless of their experience being incarcerated, report the same. Similarly, while three in ten of those who have been previously incarcerated report having a physical or mental health condition or disability that keeps them from participating fully in work, school housework or other activities, it rises to four in ten among women who have been previously incarcerated.
Reflecting their lower incomes, adults with prior incarceration experience are disproportionately likely to be covered by Medicaid or uninsured. Medicaid covers a quarter (25%) of previously incarcerated adults compared with 14% of adults without previous incarceration experience. Although Medicaid coverage helps to fill gaps in private coverage for previously incarcerated adults, they remain more likely than other adults to report being uninsured (13% vs. 8%).
Despite their reported health care needs, about one in five (19%) people with experience being incarcerated say they have not gone to a doctor or any other health care provider about their own health in the past 12 months.
In addition, one in five adults (22%) with previous incarceration experience say they do not have a usual source of care or go to the emergency room when they are sick or need advice about their health. One in three of those with previous incarceration experience say they skipped or postponed health care because of costs in the past year. This includes nearly four in ten (37%) women and nearly a third of men (31%).
In all, 37% previously incarcerated individuals say they skipped or postponed care for any reason and their health got worse because of it, rising to half (52%) of women with previous incarceration experience.
While previously incarcerated individuals are less likely to report using health care compared to those with no incarceration experience, this does not necessarily reflect a lack of concern about their health. One in five previously incarcerated individuals say they experienced worry or stress related to their health almost every day or even more often than that in the past 30 days, including one in ten (10%) who say they experienced it every day.
Mental Health Care
A substantial share of previously incarcerated adults, including even larger shares of women, report difficulties with their mental health and barriers to accessing mental health care.
One in four (27%) previously incarcerated adults say that their mental health is “fair” or “poor,” increasing to almost half (46%) of women who have been previously incarcerated. That includes about a quarter of previously incarcerated adults across and racial and ethnic groups.
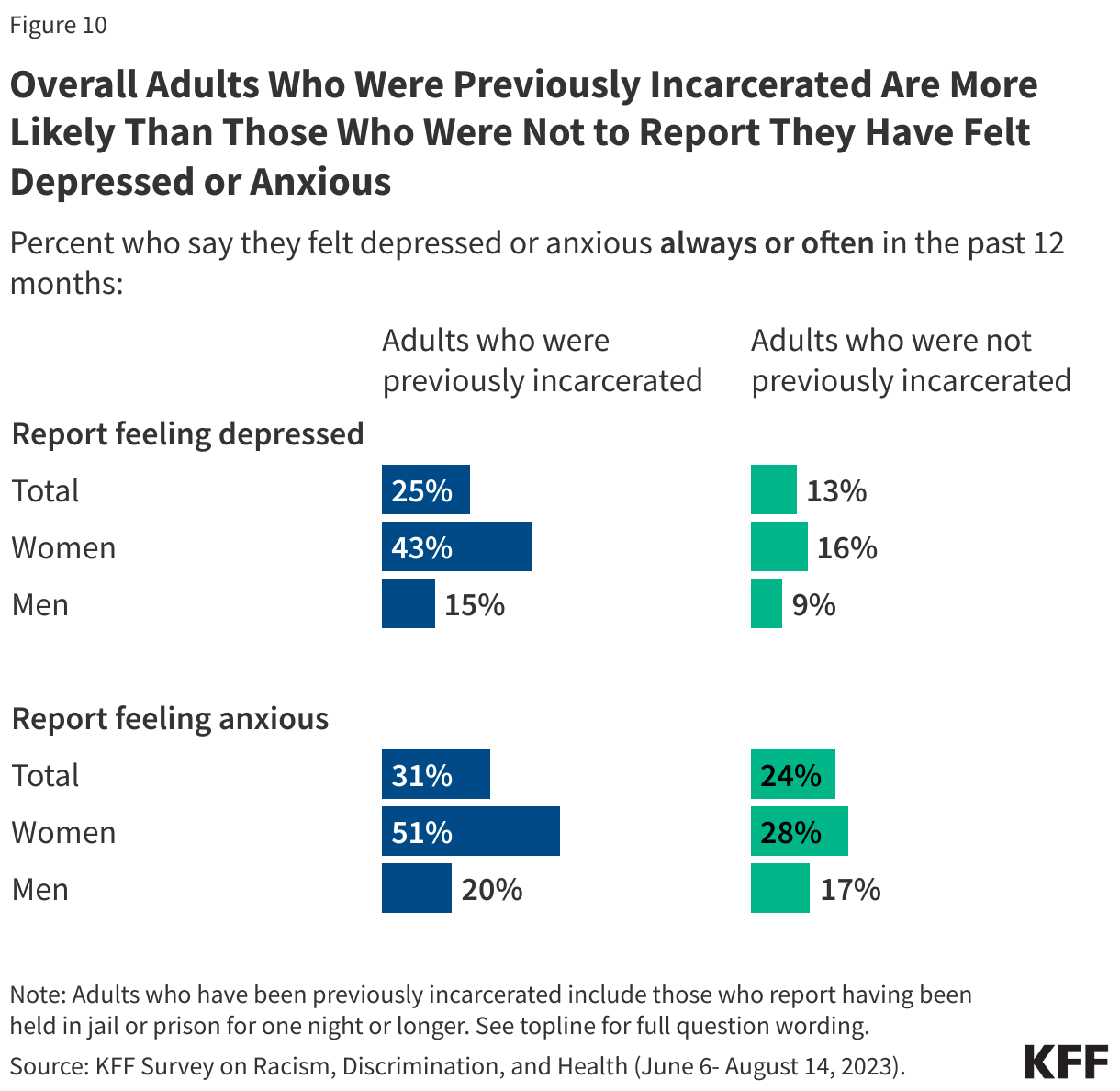
In addition, one in four previously incarcerated individuals say they have felt depressed always or often in the past 12 months, increasing to 43% of previously incarcerated women. Nearly one in three say they have felt anxious always or often in the past 12 months, once again increasing to half of previously incarcerated women.
About three in ten (31%) adults with previous incarceration experience say they have received mental health services from a doctor, counselor, or other mental health professional in the last 3 years. Among those with incarceration experience, women are more than twice as likely as men to say they have received such services, likely reflecting the higher share of women in this group who report mental health challenges. In addition, six in ten previously incarcerated adults who report having fair or poor mental health say they have received mental health care services in the past three years.
But there are still unmet needs with about a quarter saying they didn’t receive mental health services or medications they needed in the past three years. The share who report this increases to nearly half (48%) of those previously incarcerated who report having fair or poor mental health and women (37%).
Methodology
The Survey on Racism, Discrimination, and Health was designed and analyzed by researchers at KFF. The survey was conducted June 6 – August 14, 2023, online and by telephone among a nationally representative sample of 6,292 U.S. adults in English (5,706), Spanish (520), Chinese (37), Korean (16), and Vietnamese (13).
The sample includes 5,073 adults who were reached through an address-based sample (ABS) and completed the survey online (4,529) or over the phone (544). An additional 1,219 adults were reached through a random digit dial telephone (RDD) sample of prepaid (pay-as-you-go) cell phone numbers. Marketing Systems Groups (MSG) provided both the ABS and RDD sample. All fieldwork was managed by SSRS of Glen Mills, PA; sampling design and weighting was done in collaboration with KFF.
Sampling strategy:
The project was designed to reach a large sample of Black adults, Hispanic adults, and Asian adults. To accomplish this, the sampling strategy included increased efforts to reach geographic areas with larger shares of the population having less than a college education and larger shares of households with a Hispanic, Black, and/or Asian resident within the ABS sample, and geographic areas with larger shares of Hispanic and non-Hispanic Black adults within the RDD sample.
The ABS was divided into areas (strata) based on the share of households with a Hispanic, Black, and/or Asian resident, as well as the share of the population with a college degree within each Census block group. To increase the likelihood of reaching the populations of interest, strata with higher incidence of Hispanic, Black, and Asian households, and with lower educational attainment, were oversampled in the ABS design. The RDD sample of prepaid (pay-as-you-go) cell phone numbers was disproportionately stratified to reach Hispanic and non-Hispanic Black respondents based on incidence of these populations at the county level.
Incentives:Respondents received a $10 incentive for their participation, with interviews completed by phone receiving a mailed check and web respondents receiving a $10 electronic gift card incentive to their choice of six companies, a Visa gift card, or a CharityChoice donation.
Community and expert input:Input from organizations and individuals that directly serve or have expertise in issues facing historically underserved or marginalized populations helped shape the questionnaire and reporting. These community representatives were offered a modest honorarium for their time and effort to provide input, attend meetings, and offer their expertise on dissemination of findings.
Translation:After the content of the questionnaire was largely finalized, SSRS conducted a telephone pretest in English and adjustments were made to the questionnaire. Following the English pretest, Cetra Language Solutions translated the survey instrument from English into the four languages outlined above and checked the CATI and web programming to ensure translations were properly overlayed. Additionally, phone interviewing supervisors fluent in each language reviewed the final programmed survey to ensure all translations were accurate and reflected the same meaning as the English version of the survey.
Data quality check:A series of data quality checks were run on the final data. The online questionnaire included two questions designed to establish that respondents were paying attention and cases were monitored for data quality including item non-response, mean length, and straight lining. Cases were removed from the data if they failed two or more of these quality checks. Based on this criterion, 4 cases were removed.
Weighting:The combined cell phone and ABS samples were weighted to match the sample’s demographics to the national U.S. adult population using data from the Census Bureau’s 2021 Current Population Survey (CPS). The combined sample was divided into five groups based on race or ethnicity (White alone, non-Hispanic; Hispanic; Black alone, non-Hispanic; Asian alone, non-Hispanic; and other race or multi-racial, non-Hispanic) and each group was weighted separately. Within each group, the weighting parameters included sex, age, education, nativity, citizenship, census region, urbanicity, and household tenure. For the Hispanic and Asian groups, English language proficiency and country of origin were also included in the weighting adjustment. The general population weight combines the five groups and weights them proportionally to their population size.
A separate weight was created for the American Indian and Alaska Native (AIAN) sample using data from the Census Bureau’s 2022 American Community Survey (ACS). The weighting parameters for this group included sex, education, race and ethnicity, region, nativity, and citizenship. For more information on the AIAN sample including some limitations, adjustments made to make the sample more representative, and considerations for data interpretation, see Appendix 2.
All weights also take into account differences in the probability of selection for each sample type (ABS and prepaid cell phone). This includes adjustment for the sample design and geographic stratification of the samples, and within household probability of selection.
The margin of sampling error including the design effect for the full sample is plus or minus 2 percentage points. Numbers of respondents and margins of sampling error for key subgroups are shown in the table below. Appendix 1 provides more detail on how race and ethnicity was measured in this survey and the coding of the analysis groups. For results based on other subgroups, the margin of sampling error may be higher. All tests of statistical significance account for the design effect due to weighting. Dependent t-tests were used to test for statistical significance across the overlapping groups.
Sample sizes and margins of sampling error for other subgroups are available by request. Sampling error is only one of many potential sources of error and there may be other unmeasured error in this or any other public opinion poll. KFF public opinion and survey research is a charter member of the Transparency Initiative of the American Association for Public Opinion Research.
Group
N (unweighted)
M.O.S.E.
Total
6,292
± 2 percentage points
Race/Ethnicity
White, non-Hispanic (alone)
1,725
± 3 percentage points
Black (alone or in combination)
1,991
± 3 percentage points
Hispanic
1,775
± 3 percentage points
Asian (alone or in combination)
693
± 5 percentage points
American Indian and Alaska Native (alone or in combination)
Black people in the U.S. have been disproportionately affected by HIV since the epidemic’s beginning, and that disparity has deepened over time.
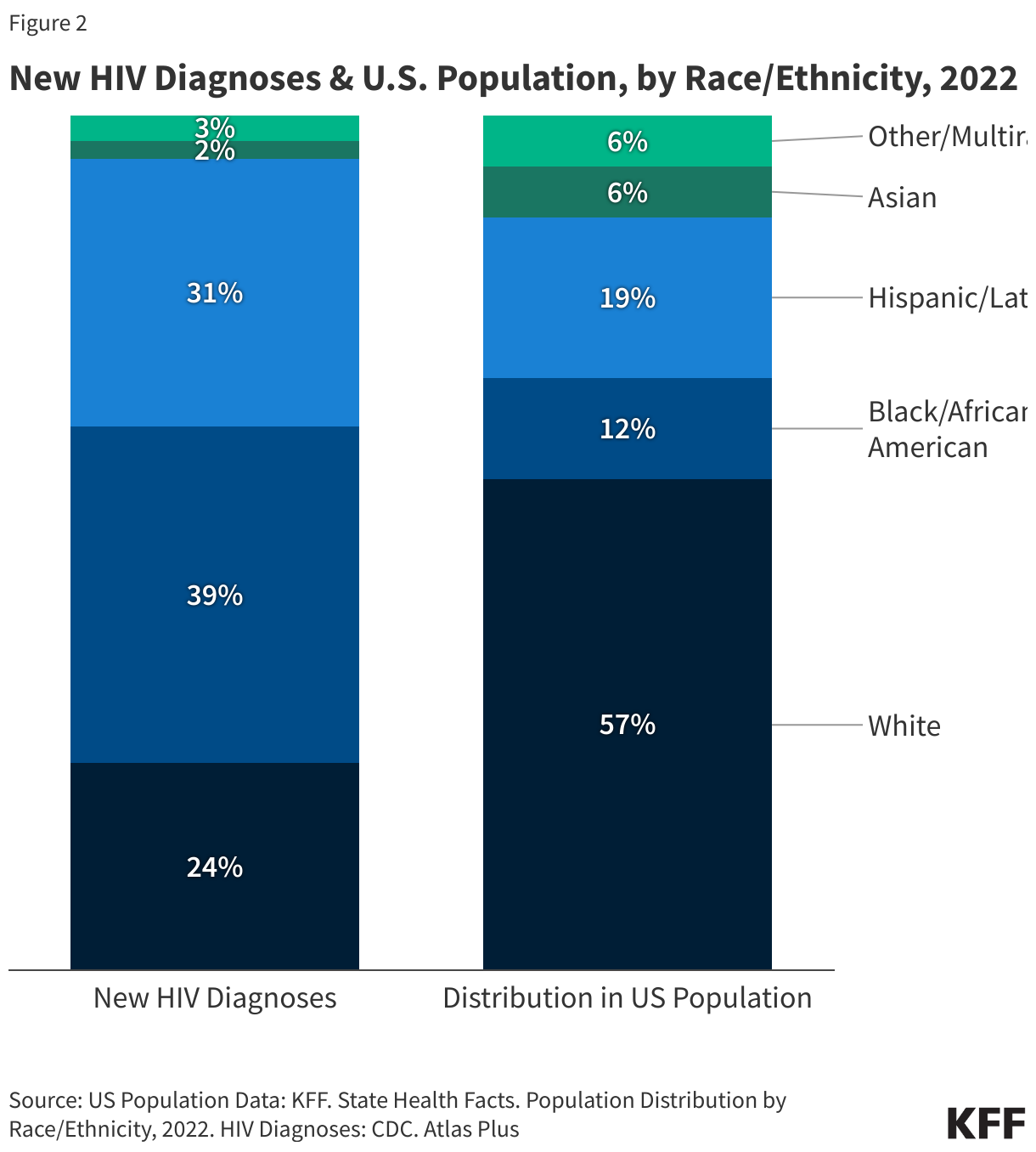
Although they represent only 12% of the U.S. population, Black people account for a much larger share of HIV diagnoses (39%), people living with HIV (40%), and deaths among people with HIV (43%) than any other racial/ethnic group in the U.S.
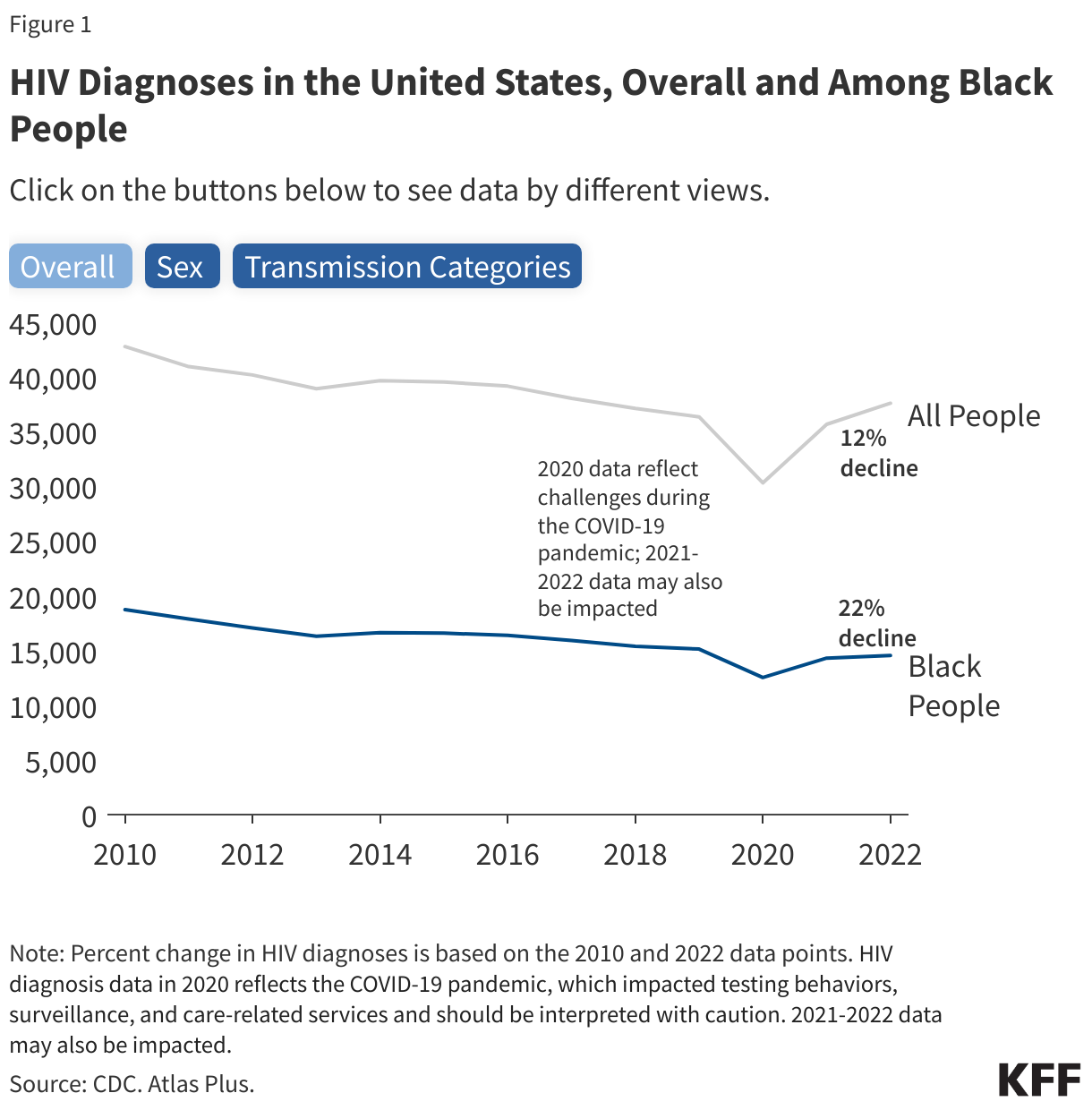
Recent data indicate some encouraging trends, including declining new HIV diagnoses among Black people overall, especially among women, and a leveling off of new diagnoses among Black gay and bisexual men (see Figure 1). However, given the epidemic’s continued and disproportionate impact on Black people, continued focus on this population is key to addressing HIV in the United States.
Overview
Today, there are more than 1.2 million people living with HIV in the U.S., 40% of whom (489,200) are Black.
The latest data indicate declines in both the number and rate of annual new diagnoses among Black people in recent years, including among both men and women (see Figure 1). However disparities persist in HIV prevention, treatment, and outcomes.
Although Black people represent only 12% of the U.S. population, they accounted for 39% of new HIV diagnoses in 2022 (see Figure 2).
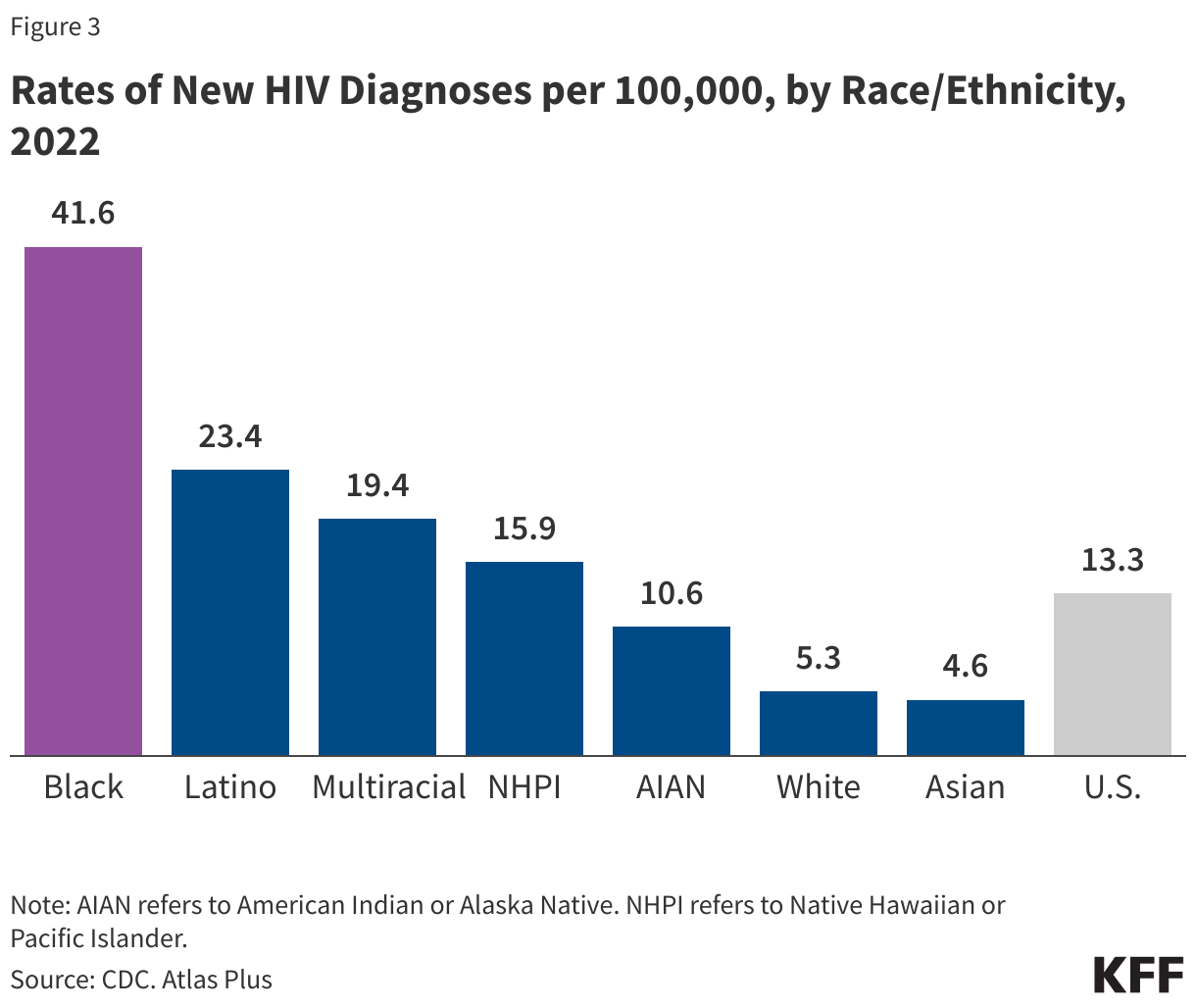
The rate of new HIV diagnoses per 100,000 among Black adults/adolescents (41.6) was about 8 times that of White people (5.3) and twice that of Latinos (23.4) in 2022 (see Figure 3). The rate for Black men (66.3) was the highest of any race/ethnicity and gender, followed by Latino men (40.8), the second highest group. Black women (19.2) had the highest rate among women.
Black people accounted for more than 4 in 10 (43%) deaths among people with an HIV diagnosis (deaths may be due to any cause) in 2022. The number of deaths among Black individuals with an HIV diagnosis decreased 13% between 2010 and 2018 but then increased more recently, by 15% between 2018 and 2022.
HIV death rates (deaths for which HIV was indicated as the leading cause of death) are highest among Black people compared to people of other race/ethnicities. In 2022, Black people had the highest age-adjusted HIV death rate per 100,000 – 5.9, compared to 0.6 per 100,000 White persons.
In addition, in 2021 HIV was the 8th leading cause of death for Black men and for Black women ages 25-34.
Transmission
Transmission patterns vary by race/ethnicity. While male-to-male sexual contact accounts for the largest share of HIV cases among both Black and White people, proportionately, fewer Black people contract HIV this way. Heterosexual sex accounts for a greater proportion of HIV cases among Black people than White people.
Among Black people, 63% of HIV diagnoses in 2022 were attributable to male-to-male sexual contact and 32% were attributable to heterosexual sex; among White people, 70% of new HIV diagnoses in 2022 were attributable to male-to-male sexual contact and 16% were attributable to heterosexual sex. The remainder of HIV diagnoses in each group were attributable to other causes, including injection drug use.
Most HIV positive Black women acquired HIV through heterosexual transmission and a smaller share of HIV infections are attributable to injection drug use among Black women compared to White women (15% v 32%).
Geography
Although HIV diagnoses among Black people have been reported throughout the country, the impact of the epidemic is not uniformly distributed.
Regionally, the South accounts for both the majority of Black people newly diagnosed with HIV (52% in 2022) and the majority living with HIV at the end of 2022 (46%).
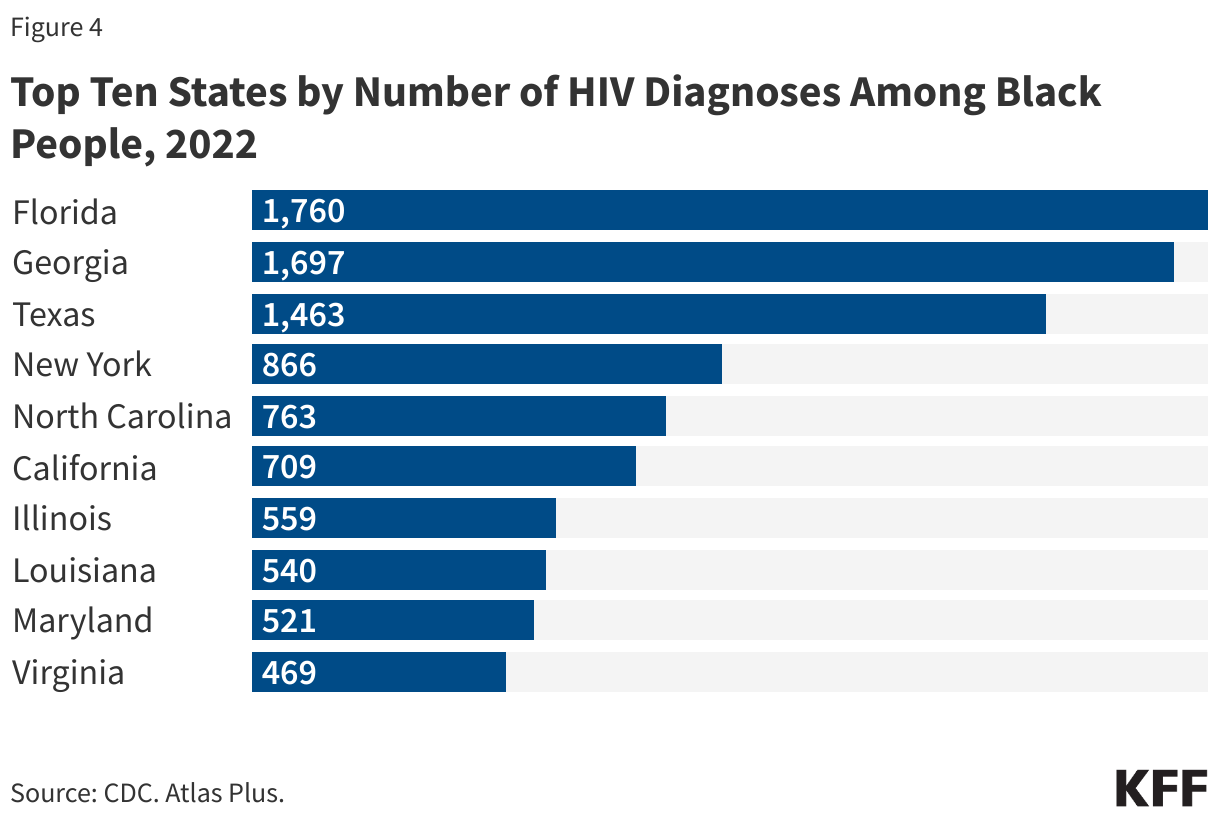
HIV diagnoses among Black people are concentrated in a handful of states. The top 10 states, 7 of which are in the South, account for 64% of all HIV diagnoses among Black people (see Figure 4).
Women
Black women account for the largest share of new HIV diagnoses among women (3,523 or 50% in 2022) as well as the largest share of all women living with HIV. The rate of new diagnoses among Black women (19.2) is 10 times the rate among White women (1.9) and 3 times the rate among Latinas (5.5).
Although new HIV diagnoses continue to occur disproportionately among Black women, data show a 39% decrease in new diagnoses for Black women between 2010 and 2022. More recently though, from 2018 to 2022, new HIV diagnoses among Black women were essentially flat, decreasing by just 1%.
In 2022, Black women represented about one quarter (24%) of new HIV diagnoses among all Black people – a higher share than Latinas and White women (who represented 12% and 18% of new diagnoses among their respective racial/ethnic groups).
Young People
In 2022, half (50%) of HIV diagnoses among all young people ages 13-24 were among Black people.
More than half (53%) of gay and bisexual teens and young adults with HIV were Black in 2022.
In 2023, 10% of Black high school students report having ever been tested for HIV compared to 5% of White students but that share is down from 20% of Black students in 2013.
Gay and Bisexual Men
Black gay and bisexual men accounted for almost half (49%) of Black people living with HIV and 30% of gay and bisexual men living with HIV.
Among Black people, male-to-male sexual contact accounted for more than half (63%) of HIV diagnoses in 2022 and a majority (82%) of diagnoses among Black men.
Young Black gay and bisexual men are particularly affected. Black gay and bisexual men are younger than their White counterparts, with those ages 13-24 accounting for 32% of new HIV diagnoses among Black gay and bisexual men in 2022, compared to 12% among White gay and bisexual men.
HIV Testing and Access to Prevention & Care
In 2022, over half (57%) of Black adults reported ever having been tested for HIV, a greater share than among Latino or White adults (44% and 32%, respectively).
One-in-five (20%) Black people with HIV tested positive late in their illness – that is, were diagnosed with AIDS at the time of testing positive for HIV; similar to the share among White (21%) and Latino (21%) people.
Looking across the care continuum, Black people face disparities related to linkage to care and viral suppression. At the end of 2022, 88% of Black people with HIV were diagnosed, 64% were linked to care, and 53% were virally suppressed. In comparison, 89% of White people with HIV were diagnosed, 70% were linked to care, and 63% were virally suppressed.
More than two in five (42%) or 57.4 million adults under 65 with private insurance could be eligible under clinical criteria for GLP-1 drugs used to treat people with type 2 diabetes, obesity, or excess weight and weight-related health issues, according to a new KFF analysis.
Though only about 3% of adults with employer coverage had a prescription in 2022, demand for and spending on GLP-1 drugs has grown and could continue to grow. Given the steep costs and high demand for these drugs, employers and insurers may continue to impose more restrictive eligibility standards for coverage than the clinical indications set by the Food and Drug Administration.
The full analysis and other data on health costs are available on the Peterson-KFF Health System Tracker, an online information hub dedicated to monitoring and assessing the performance of the U.S. health system.
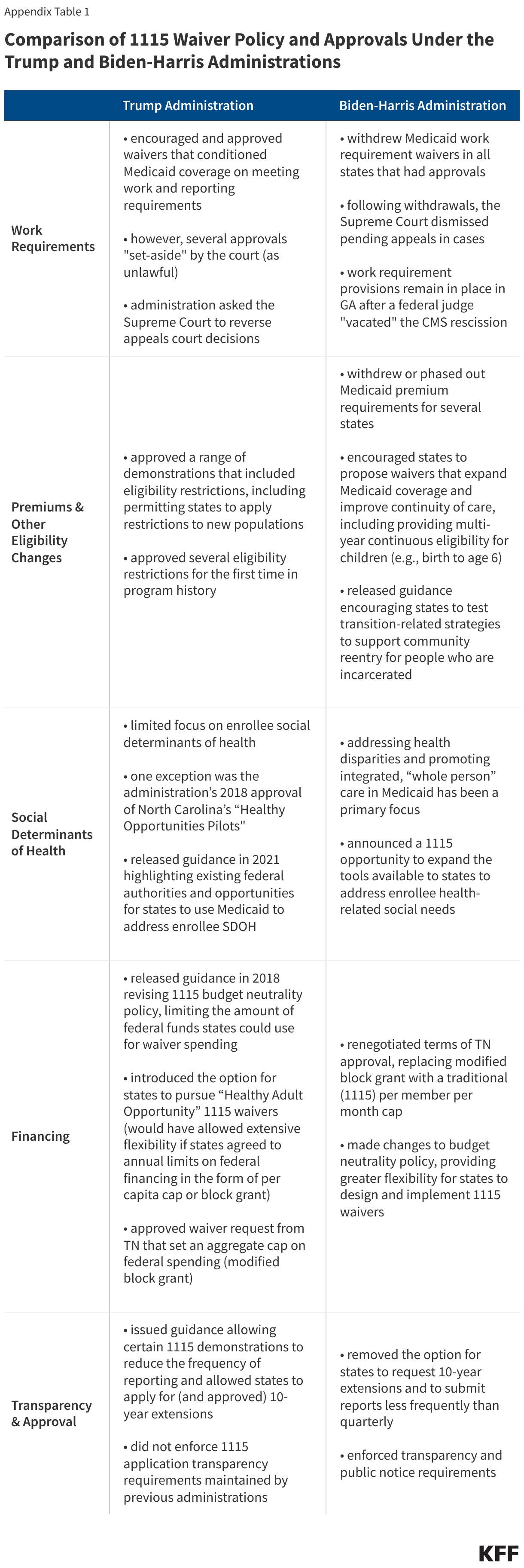
Section 1115 Medicaid demonstration waivers offer states an avenue to test new approaches in Medicaid that differ from what is required by federal statute, so long as the approach is likely to “promote the objectives of the Medicaid program.” Waivers generally reflect priorities identified by states as well as changing priorities from one presidential administration to another. Each administration has some discretion over which waivers to approve and encourage, but that discretion is not unlimited. The Trump administration’s Section 1115 waiver policy emphasized work requirements – which were challenged in court – and other eligibility restrictions and capped financing. In contrast, the Biden-Harris administration has encouraged states to propose waivers that expand coverage, reduce health disparities, and advance whole-person care. Both administrations prioritized improving access to behavioral health services.
As with broader Medicaid policy, the future landscape of Section 1115 waivers depends on the outcome of the November 2024 presidential election as a new administration could focus on different priorities, rescind existing guidance, or withdraw already-approved waivers. This waiver watch summarizes five key areas of difference in 1115 waiver policy and waiver approvals under the Trump and Biden-Harris administrations (Figure 1, also see Appendix Table 1).
Work Requirements. For the first time in the history of the Medicaid program, the Trump administration encouraged and approved Section 1115 waivers that conditioned Medicaid coverage on meeting work and reporting requirements, approving 13 state work requirement waivers. The Biden-Harris administration withdrew Medicaid work requirement waivers in all states that had approvals, concluding that these provisions do not promote the objectives of the Medicaid program.
Premiums and Eligibility Changes. Under the Trump administration, CMS approved a range of demonstrations that included eligibility restrictions, including permitting states to apply restrictions (e.g., charging premiums, locking out enrollees disenrolled for unpaid premiums, and eliminating retroactive eligibility) to new populations (beyond ACA expansion adults) and approving several eligibility restrictions for the first time in program history. The Biden-Harris administration took steps to withdraw or phase out Medicaid premium requirements for several states and has encouraged states to propose waivers that expand Medicaid coverage and improve continuity of care.
Social Determinants of Health. The Trump administration generally had a limited focus on enrollee social determinants of health. In contrast, addressing health disparities and promoting integrated (“whole person”) care has been a primary focus of the Biden-Harris administration. In 2022, CMS announced a new 1115 demonstration opportunity that expands flexibility for states to leverage Medicaid to help address enrollee health-related social needs (HRSN) (including housing instability, homelessness, and nutrition insecurity).
Financing and Budget Neutrality. The Centers for Medicare and Medicaid Services (CMS) made changes to 1115 waiver budget neutrality policy in 2018, limiting the amount of federal funds that could be used for waiver spending. The Trump administration also introduced a demonstration opportunity that would have allowed states “extensive flexibility” to use Medicaid funds to cover certain adults without being bound by many federal standards (related to eligibility, benefits, delivery systems, and oversight) if states agreed to annual limits on federal financing (no state took up this option). The Biden-Harris administration made changes to Section 1115 budget neutrality policies that may provide greater flexibility for states to design and implement 1115 demonstration programs, including HRSN initiatives.
Transparency and Approval Process. Under the Trump administration, in a departure from prior policy, CMS approved waiver extension requests for up to 10 years, signaled an interest in reducing the frequency of required state reporting on 1115 waivers, and did not enforce state-level public notice and comment procedures for certain new/renewal 1115 waiver requests. Under the Biden-Harris administration, CMS removed the option for 10-year extensions and for less frequent state reporting and has enforced transparency and public notice requirements.
Work Requirements
Current Law/Context. Data show most Medicaid adults are working or face barriers to work. Current law prohibits conditioning Medicaid eligibility on meeting a work or reporting requirement. Prior to the Trump administration, no states had received Section 1115 waiver approval to condition Medicaid coverage on work and reporting requirements, and legislativeattempts to incorporate work requirements into Medicaid statute failed. Medicaid can support employment by providing health coverage and access to care and medications that enable people to work, and it can also provide voluntary employment referral and/or work support programs. A central question in the debate over work requirements in Medicaid is whether such policies promote health. A review of research on the relationship between work and health found that although there is strong evidence of an association between unemployment and poorer health outcomes, there is limited evidence on the effect of employment on health (studies have found job quality and stability are key factors in work-health relationship). While work requirements were the subject of litigation during the Trump and Biden-Harris administrations, the Supreme Court never ruled on the issue leaving it open for future administrations; however, any future waivers with work requirements would likely face legal challenges. Several states continue to pursue work requirement waivers, often tied to Medicaid expansion efforts.
Trump. The Trump administration encouraged and approved Section 1115 waivers that conditioned Medicaid coverage on meeting work and reporting requirements, approving 13 state work requirement waivers. Only Arkansas implemented work and reporting requirements with consequences for noncompliance, which resulted in over 18,000 people losing coverage before the court deemed the work requirement unlawful. While the vast majority of enrollees were working or qualified for exemptions, barriers with meeting reporting requirements led to people getting dropped from the program. Other states with approvals for work requirements paused implementation due to litigation and/or the COVID-19 pandemic. Plans from some Republican and conservative groups continue to support federal legislation to allow or require work requirements in Medicaid. A Congressional Budget Office analysis of a recent work requirement proposal shows that the policy would reduce federal spending due to reductions in enrollment but would not increase employment.
Biden-Harris. The Biden-Harris administration withdrew Medicaid work requirement waivers in all states that had approvals, concluding that these provisions do not promote the objectives of the Medicaid program. Although CMS withdrew work and premium requirements in Georgia’s “Pathways” waiver, these provisions remain in place after a federal judge vacated the CMS rescission. Georgia’s waiver expands eligibility to 100% of the federal poverty level (FPL) for parents and childless adults (not a full Medicaid expansion under the ACA that does not qualify for enhanced federal matching funds), with initial and continued enrollment conditioned on meeting work and premium requirements. The waiver was implemented in July 2023. A year into the demonstration, enrollment remains low—as of June 2024, the state had only enrolled about 4,300 adults.
Premiums and Eligibility Changes
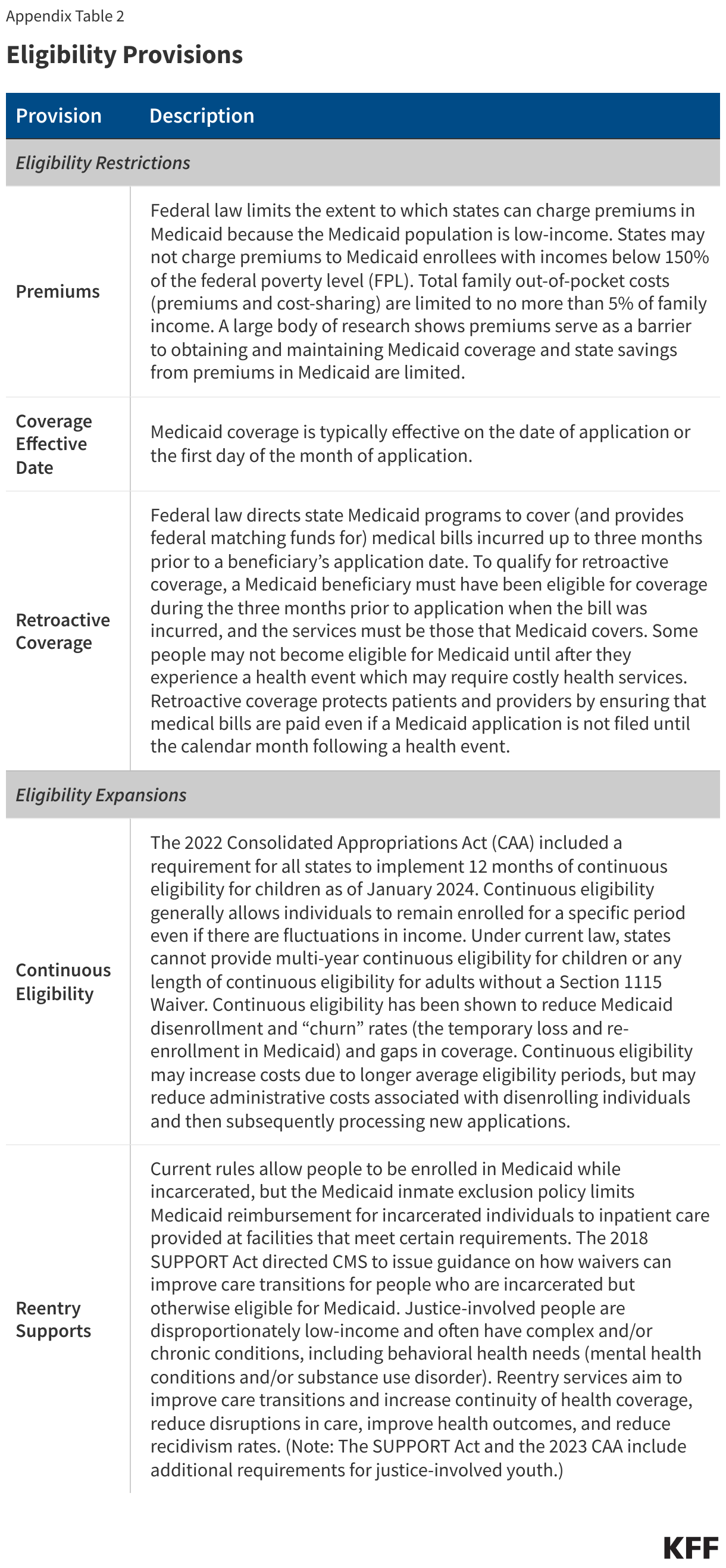
Current Law/Context. Given that people covered by Medicaid have low-incomes, federal rules limit states’ ability to charge premiums. States may not charge premiums to Medicaid enrollees with incomes below 150% of the FPL ($22,590 for an individual in 2024). Total family out-of-pocket costs (premiums and cost-sharing) are limited to no more than 5% of family income. Some states have received 1115 waiver approval to charge premiums or monthly contributions that are not otherwise allowed. States can also request 1115 authority to implement other eligibility and enrollment restrictions or to implement eligibility expansions, not otherwise allowed under current law (see Appendix Table 2).
Trump. Under the Trump administration, CMS approved a range of demonstrations that included eligibility restrictions. The administration approved some eligibility- and enrollment-related waiver provisions that had been approved under previous administrations (e.g., charging premiums, eliminating retroactive eligibility, making coverage effective on the date of the first premium payment (instead of the date of application), and locking out enrollees disenrolled for unpaid premiums); however, the Trump administration permitted states to apply these restrictions to new populations beyond ACA expansion adults (e.g., low-income parent/caretakers). The Trump administration also approved several eligibility restrictions for the first time, including:
Coverage lock-outs for failure to timely renew coverage or report changes affecting eligibility
Authority to charge premiums up to 5% of family income and to impose a premium surcharge for tobacco users
Eligibility conditioned on the completion of a health risk assessment
Biden-Harris. The Biden-Harris administration has taken steps to withdraw or phase out Medicaid premium requirements for several states, indicating the research evidence shows imposing premiums reduces access to coverage and care and is not likely to promote the objectives of the Medicaid program. The Biden-Harris administration also withdrew or phased out the authority for states to condition Medicaid eligibility on the completion of a health risk assessment.
The Biden-Harris administration has encouraged states to propose waivers that expand Medicaid coverage and improve continuity of care. For example, the Biden-Harris administration has encouraged states to adopt strategies to promote continuity of coverage, including providing multi-year continuous eligibility for children (e.g., birth to age 6) through Section 1115. In April 2023, CMS released guidance encouraging states to apply for a new Section 1115 demonstration opportunity to test transition-related strategies to support community reentry for people who are incarcerated. This demonstration allows states a partial waiver of the inmate exclusion policy, which prohibits Medicaid from paying for services provided during incarceration (except for inpatient services). CMS has developed a standard demonstration application and special terms and conditions for reentry waivers to expedite approval.
Social Determinants of Health
Current Law/Context. Social determinants of health (SDOH) are the conditions in which people are born, grow, live, work and age. SDOH include but are not limited to housing, food, education, employment, healthy behaviors, transportation, and personal safety. While there are limits, states can use Medicaid – which, by design, serves a primarily low-income population with greater social needs – to address social determinants of health. States can use a range of state plan and waiver authorities to add certain non-clinical services to the Medicaid benefit package including case management, housing supports, employment supports, and peer support services.
Trump. The Trump administration generally had a limited focus on enrollee social determinants of health. One exception was the administration’s 2018 approval of North Carolina’s “Healthy Opportunities Pilots,” allowing the state to cover certain non-medical services that target social needs, including housing, nutrition, transportation, and interpersonal relationship supports. The Trump administration later released guidance in 2021 highlighting existing federal authorities and opportunities for states to use Medicaid to address enrollee social determinants of health, including under Section 1115 authority.
Biden-Harris. Addressing health disparities and promoting integrated, “whole person” care in Medicaid has been a primary focus of the Biden-Harris administration. In 2022, CMS announced a Section 1115 demonstration waiver opportunity to expand the tools available to states to address enrollee health-related social needs (or “HRSN”). In 2023, CMS released a detailed Medicaid and CHIP HRSN Framework accompanied by an Informational Bulletin. The new demonstration opportunity includes federal guardrails and requirements including expenditure limits, service delivery requirements, and monitoring and evaluation requirements. CMS has stressed new HRSN initiatives are not designed to replace other federal, state, and local social service programs but rather to complement and coordinate with these efforts. HRSN demonstration approvals to date include coverage of rent/temporary housing and utilities for up to six months and meal support up to three meals per day, departing from longstanding prohibitions on payment of “room and board” in Medicaid.
Financing and Budget Neutrality
Current Law/Context. Medicaid financing is shared by states and the federal government with a guarantee to states for federal matching payments with no pre-set limit. The federal Medicaid match rate is an area that may not be changed under Section 1115 waiver authority. Under long-standing policy and practice (although not required by statute), waivers must also be “budget neutral” to the federal government over the course of the waiver (usually five years). In other words, federal costs under an 1115 waiver may not exceed what they would have been for that state without the waiver. Typically, budget neutrality calculations are determined on a per enrollee basis—so, per enrollee spending over the course of the waiver cannot exceed the projected per enrollee spending calculated in the “without-waiver baseline.” Waiver budget neutrality—measured against the estimated without-waiver baseline over the entire demonstration period—is not the same as a federal per enrollee limit on spending set at rates lower than expected under current law to generate federal savings. These broader limits on federal spending have been and continue to be part of plans supported by Trump and other Republicans.
Trump. CMS released guidance in 2018 revising Section 1115 budget neutrality policy. The guidance established new rules for calculating the “without-waiver” baseline to require “rebasing” every five years and to limit the trend to historical state spending rates or the President’s Budget trend rate (whichever rate was lower). These changes were designed to limit the “without-waiver” baseline and thereby limit the amount of federal funds that could be used for waiver spending.
After major legislative attempts to restructure Medicaid financing (into a block grant or per capita cap) as part of the 2017 ACA repeal debate failed, in January 2020 the Trump administration introduced the option for states to pursue “Healthy Adult Opportunity” (HAO) Section 1115 demonstrations. This demonstration opportunity would have allowed states “extensive flexibility” to use Medicaid funds to cover certain adults (including ACA expansion adults) without being bound by many federal Medicaid standards related to eligibility, benefits, delivery systems, and program oversight. In exchange, states would agree to a limit on federal financing in the form of a per capita or aggregate cap (with methods that differed from those used to determine budget neutrality). Only one state (Oklahoma) submitted an HAO demonstration request, which included a work requirement and other eligibility and benefit restrictions that would have applied to a new ACA expansion adult population. However, the state withdrew its application following a successful ballot measure adopting a traditional Medicaid expansion (in June 2020).
In January 2021, CMS approved a waiver request from Tennessee (not part the HAO initiative) that set an aggregate cap on federal spending and provided an opportunity for the state to keep a portion of any unspent federal dollars up to the cap without putting up the state match, as is required under current law. Unlike legislative block grant proposals designed to reduce federal spending, aggregate caps proposed In the Tennessee waiver were designed to be adjusted to reflect expected growth in federal Medicaid spending in the President’s budget and adjusted for changes in enrollment, posing less fiscal risk to the state.
Biden-Harris. The Biden-Harris administration renegotiated Tennessee’s waiver approval, replacing the aggregate cap with a traditional (i.e., 1115 waiver / budget neutral) per member per month cap. The Biden-Harris administration has also made changes to Section 1115 budget neutrality policies that may provide greater flexibility for states to design and implement 1115 demonstration programs (including “HRSN” initiatives). Republican members of the US House and Energy Commerce Committee have raised concerns about changes to Section 1115 budget neutrality requirements made by the Biden-Harris administration.
Transparency and Approval Process
Current Law/Context. Waivers are generally approved for a five-year period and can be extended, typically for three-to-five-year periods. The ACA made Section 1115 waivers subject to new rules about transparency, public input, and evaluation. In February 2012, HHS issued regulations that require public notice and comment periods to occur at the state and federal levels before CMS approves new Section 1115 waivers and extensions of existing waivers. Although the final regulations on public notice do not require a state-level public comment period for amendments to existing/ongoing demonstrations, CMS historically applied these regulations to amendments as well. The ACA also implemented new evaluation requirements for Section 1115 waivers, including that states must have a publicly available, CMS-approved evaluation strategy. States have traditionally been required to submit quarterly reports as well as an annual report to HHS that describes the changes occurring under the waiver and the impact on access, quality, and outcomes.
Trump. CMS released an Informational Bulletin in November 2017 signaling an interest in reducing the frequency of required state reporting from quarterly to semi-annual or annual for certain demonstrations. In the November 2017 bulletin, CMS also indicated that it would consider approving “routine, successful, non-complex” 1115 waiver extension requests for up to 10 years. The administration approved several 10-year waiver extension requests (e.g., most notably Florida, Indiana, Tennessee, and Texas as well as several family planning waivers). CMS, under the Trump administration, did not enforce state-level public notice and comment procedures for certain new 1115 waivers or extension requests (e.g., Indiana and Kentucky),1 including waivers that proposed significant changes (e.g., work requirements).
Biden-Harris. In 2022, CMS reinstated guidance from 2015, removing the option for 10-year extensions and for less frequent state reporting; however, the Biden-Harris administration has not rescinded any of the 10-year approvals. Additionally, under the Biden-Harris administration, CMS has enforced transparency and public notice requirements, returning incomplete 1115 applications submitted for federal review back to states to remedy (e.g., when an application failed to provide sufficient detail summarizing state-level public comments, including how the state considered the comments in developing the application).
CMS deemed an amendment request (to a pending renewal application) from Indiana as complete in June 2017, opening the federal comment period while the state comment period was ongoing. This “amendment” request included a work requirement. In July 2017, Kentucky submitted an amendment (to a pending new waiver application) without holding a state-level public comment period prior to submission. The request included premium requirements (including disenrollment and lock-out for failure to pay), disenrollment and lock-out for failure to timely report income / employment changes, removal of non-emergency medical transportation (NEMT) for certain adults, among other changes. ↩︎
While Medicaid policy may not be a central issue candidates are talking about, the outcome of the election could have major implications for Medicaid, the primary program providing comprehensive coverage for over one in five low-income Americans. Medicaid is jointly financed by the federal government and states and administered by states within broad federal guidelines. Medicaid represents nearly one in five dollars spent on health and disproportionately finances safety-net hospitals and clinics, behavioral health care, and long-term services and supports (LTSS) in the community and nursing homes for seniors and people with disabilities. Medicaid has become a major part of our health care system, with two-thirds of Americans having a connection to Medicaid. Public opinion polling shows Medicaid has broad support across political parties.
This brief highlights major policy differences under the Biden-Harris Administration and the Trump Administration on key Medicaid topic areas. The brief examines the records and proposed budgets under President Biden and Vice President Harris and former President Trump as well as major legislative proposals that former President Trump supported. Budget proposals often include policy proposals that would require Congressional action to enact. The 2024 Republican Party platform calls for new affordable health care and prescription drug options with protections for Medicare and seniors but does not include any details about Medicaid policy. To help inform the range of options that could be considered under a Trump presidency, this brief also examines Medicaid policies included in the Republican Study Committee (RSC) FY 2025 budget and the Heritage Foundation’s Project 2025. Former President Trump has not endorsed these proposals, though there would likely be a push for them from conservative groups and Republicans in Congress if Trump wins the election. Policy differences are highlighted across the following key Medicaid topic areas, with more detail about candidate records and specific sources in the Appendix.
The analysis finds that Vice President Harris and former President Trump have vastly different records, views on, and policy proposals for Medicaid (Figure 1). More broadly, as KFF President and CEO Drew Altman recently wrote, “Republicans and Democrats have fundamentally different world views of the program.”
Biden-Harris Administration policy proposals have generally focused on efforts to “protect and strengthen Medicaid and the Affordable Care Act (ACA)” by expanding health coverage and improving continuity of coverage, reducing the rate and number of uninsured, expanding access to care, and reducing health disparities. These policies generally maintain or increase federal Medicaid spending.
Former President Trump has not talked specifically about Medicaid in the current campaign, but his record as president and proposals from Republican groups include plans to repeal or weaken the ACA, cap and reduce Medicaid financing, and restrict Medicaid eligibility, with the overarching goal of reducing federal spending on Medicaid. Estimates of savings range widely, from a $4.5 trillion reduction over 10 years (over a 50% reduction) under the RSC FY 2025 budget proposal, to earlier Congressional Republican proposals that would have reduced Medicaid spending by 25% or one-third, to other proposals with smaller overall reductions but large shifts in spending across states. Reductions in federal spending generally shift risk and costs to states as well as enrollees and would likely increase the number of uninsured people.
Key Takeaways
Vice President Harris inherits the record of the current administration but has also independently focused on reproductive rights and policies aimed at reducing maternal mortality and morbidity. Major Biden-Harris Administration efforts across key Medicaid topic areas include:
ACA Medicaid Expansion: The Biden-Harris Administration implemented policies to strengthen the ACA, including enacting legislation with an additional fiscal incentive for states to adopt Medicaid expansion. The administration also proposed a plan to close the coverage gap in states that have not expanded Medicaid, but it did not pass Congress.
Financing: The administration built on the existing Medicaid financing framework by expanding federal matching funds for priority areas, such as incentivizing states to expand Medicaid home and community-based services (HCBS).
Eligibility, Benefits, and Cost-Sharing: The Biden-Harris Administration enacted legislation to expand access to health insurance coverage by requiring 12-month continuous eligibility for children and creating an option for states to extend postpartum coverage to 12 months as well as cover certain justice-involved youth. During the unwinding of the Medicaid continuous enrollment provision, the administration issued guidance and provided states with additional waiver flexibilities to help eligible enrollees retain coverage.
Prescription Drugs: The Inflation Reduction Act (IRA), enacted during the Biden-Harris Administration, included several provisions to lower prescription drug costs and reduce drug spending by the federal government, including allowing the federal government to negotiate prices for some drugs in Medicare and requiring that drug manufacturers pay rebates for price increases above inflation in Medicare. Within Medicaid specifically, the administration has enacted policies (as well as proposed additional policies that did not pass) to expand and strengthen the Medicaid drug rebate program (MDRP).
Long-Term Services and Supports: The administration enacted legislation to increase federal funding for Medicaid HCBS and issued regulations to increase access to Medicaid HCBS, promote higher payment rates for home care workers, and establish minimum staffing requirements in nursing facilities. President Biden and Vice President Harris have called for additional, permanent federal funding for HCBS, which did not pass.
Managed Care: The Biden-Harris Administration issued updated Medicaid managed care regulations aimed at improving access to care, quality, health outcomes, and health equity as well as took action to improve Medicaid managed care monitoring, oversight, and transparency.
Specific Republican policies, both during and after the Trump Administration, across key Medicaid topic areas include:
ACA Medicaid Expansion: The Trump Administration proposed and supported unsuccessful efforts to repeal and replace the ACA, including Medicaid expansion. More recent Republican proposals, the RSC FY 2025 budget and Project 2025, do not specify a complete repeal but seek to reduce the higher match rate for the Medicaid expansion group and eliminate expanded Marketplace subsidies.
Financing: The Trump Administration proposed and supported legislative proposals to limit federal Medicaid spending by restructuring Medicaid financing into a block grant or per capita cap. The RSC FY 2025 budget and Project 2025 also suggest a block grant or cap as well as changes in federal matching payments.
Eligibility, Benefits, and Cost-Sharing: The Trump Administration approved waivers that included work requirements as a condition of Medicaid eligibility, premiums, and other eligibility restrictions. The RSC FY 2025 budget and Project 2025 also propose restricting Medicaid eligibility, benefits, and continuity of coverage, including actions such as imposing work requirements, eliminating minimum eligibility thresholds, and providing state flexibility to redesign and eliminate certain benefits.
Prescription Drugs: The Trump Administration aimed to address high drug costs by allowing the importation of drugs from Canada and encouraging states to submit waivers to create closed formularies. Both the RSC FY 2025 budget and Project 2025 seek to repeal the IRA, citing its implications for drug innovation.
Long-Term Services and Supports: The Trump Administration reduced federal oversight over nursing facilities, but more recent Republican proposals give little indication of LTSS policy priorities.
Managed Care: The Trump Administration changed Medicaid managed care rules, including relaxing Medicaid managed care plan network adequacy rules and requirements for beneficiary protections. Project 2025 proposes to reform and increase oversight of Medicaid managed care but doesn’t provide specifics.
Details of Medicaid Policies and Proposals
Affordable Care Act (ACA) Medicaid Expansion
Context: The ACA expanded Medicaid coverage to nearly all adults up to 138% of the federal poverty level (FPL) ($20,783 for an individual in 2024), but it is effectively an optional policy for states following a ruling by the Supreme Court. As of summer 2024, 41 states including DC have expanded Medicaid while 10 states have not, leaving 1.5 million uninsured people in the “coverage gap” (adults who have incomes above their state’s eligibility for Medicaid but below poverty, making them ineligible for subsidies in the ACA Marketplaces). The ACA expansion group is financed with a 90% federal match rate or “FMAP”, so states pay 10% of the costs for the expansion group. Data from June 2023 show almost 24 million adults were enrolled in Medicaid through the ACA expansion eligibility pathway. Total spending for this population in fiscal year 2022 was over $155 billion, including $138 billion in federal spending and $17 billion in state spending. The ACA also created health insurance exchange markets, or Marketplaces, which offer subsidized coverage to those who are not eligible for Medicaid and who do not have access to other affordable coverage.
Biden-Harris: The Biden-Harris Administration enacted legislation to strengthen the ACA, including an additional fiscal incentive for states to adopt the ACA Medicaid expansion and temporary enhanced subsidies for Marketplace coverage. The Biden-Harris Administration has also taken action to increase funding for Marketplace outreach and navigators and has supported legislation to close the coverage gap (that never passed). Four new states have adopted Medicaid expansion since Biden and Vice President Harris took office, and the number of people with Marketplace coverage has grown significantly under the administration. The Biden-Harris Administration’s latest budget builds on these actions by proposing to make the enhanced Marketplace subsidies permanent and continuing to call for closing the coverage gap. As a part of a recent campaign speech focused on economic issues in North Carolina, Vice President Harris also highlighted health proposals including extending the enhanced Marketplace subsidies.
Trump and Republican Proposals: Former President Trump modeled proposals included in his 2019 and 2020 budgets on the Graham-Cassidy amendment, which called for repealing and replacing the ACA (the FY 2021 budget was more vague about health reform proposals). Other legislation introduced but not enacted during the Trump presidency — the American Health Care Act (AHCA) and the Better Care Reconciliation Act (BCRA) — also called for repealing and replacing the ACA. More recently released Republican proposals do not specify a complete repeal of the ACA, but the RSC FY 2025 budget proposes to eliminate the expanded ACA subsidies and reduce the FMAP for the Medicaid expansion group. Project 2025 also proposes “a fairer and more rational match rate” for the Medicaid expansion group.
Tradeoffs: The Biden-Harris Administration proposals would support expanded coverage but increase federal spending. Republican proposals would eliminate or severely limit access to affordable health insurance coverage for low-income adults but would reduce federal spending. Rolling back the ACA Medicaid expansion could also have implications for state fiscal conditions and providers. The federal government pays the vast majority of expansion costs, and the literatureshowsthat states expanding Medicaid under the ACA have realized budget savings, revenue gains, overall economic growth as well as observed positive effects on the finances of hospitals and other health care providers. Recent KFF polling finds that more than three in four (78%) enrollees and two-thirds of all adults in a non-expansion state say their state should expand Medicaid to cover more low-income uninsured people. Among the public overall, expanding Medicaid is largely split along partisan lines.
Context: Medicaid is an entitlement program, meaning individuals who meet eligibility requirements are guaranteed coverage and states are guaranteed federal matching funds without a cap for qualified services provided to eligible enrollees. The FMAP (federal match rate) for most Medicaid enrollees is determined by a formula in the law that provides a match of at least 50% and provides a higher federal match rate for states with lower per capita incomes. There are also higher match rates for certain services and populations like the ACA expansion group (90%). Medicaid also provides “disproportionate share hospital” (DSH) payments to hospitals that serve a large number of Medicaid and low-income uninsured patients to offset uncompensated care costs. Medicaid represents almost $1 out of every $5 spent on health care in the U.S. and provides significant financing for hospitals, community health centers, physicians, nursing homes, and community-based LTSS.
For state budgets, Medicaid is a spending item and at the same time the largest source of federal revenues. To help finance the state share of Medicaid, states can use funding from local governments or revenue collected from provider taxes and fees to help finance the state share of Medicaid within certain limits and rules.
Biden-Harris: The Biden-Harris Administration has built on the existing financing framework by expanding federal matching funds for priority areas, such as incentivizing states to expand Medicaid or Medicaid home and community-based services. The administration’s latest budget proposal (along with prior budgets) keeps the Medicaid financing system as is under federal law and also provides funding to improve program integrity and prevent fraud.
Trump and Republican Proposals: The Trump Administration and other Republican proposals examined aim to significantly limit federal Medicaid spending by restructuring Medicaid financing into a block grant or a per capita cap where states would receive a pre-set amount of funding for Medicaid in total or per enrollee. Typically, a base year of Medicaid spending would be established and then the aggregate or per enrollee caps would increase by a specified amount each year, typically tied to inflation or inflation plus some percentage. To generate federal savings, the total amount of federal spending would be less than what is expected under current law. Program costs in excess of the total or per enrollee caps would not be matched by the federal government, leaving states to cover these costs or reduce Medicaid spending. Proposals that cap federal Medicaid funding could also eliminate the entitlement to coverage or federal minimum requirements for eligibility and benefits. The Trump Administration FY 2020 budget proposed to convert federal Medicaid funding to a per capita allotment; this change along with other health care adjustments totaled $1 trillion in spending reductions relative to estimated spending under current law over 10 years. More recent Republican proposals, the RSC FY 2025 budget and Project 2025, call for capped Medicaid spending as well as a match rate of 50% for all eligibility groups and services (RSC FY 2025 budget) or a “blended” match rate (Project 2025).
Proposals that fundamentally change the financing structure and entitlement nature of the program would require legislative change and would have broad implications across all areas of Medicaid; however, even without legislative changes, presidential administrations have options to issue regulations or guidance as well as approve demonstration waivers which could result in incremental program changes. In lieu of major legislative changes to Medicaid financing, former President Trump also issued guidance and encouraged states to apply for Healthy Adult Opportunity waivers that offered states “extensive flexibility” to cover certain groups of enrollees in exchange for limits in federal financing and access to shared savings for spending below the set cap; however, no states were approved for such waivers. In addition to restructuring Medicaid financing, Republican proposals also include provisions to restrict the use of provider taxes, combat Medicaid improper payments, and improve program integrity.
Tradeoffs: Republican proposals would substantially reduce federal Medicaid spending and allow states additional flexibility to administer their programs. KFF analysis has found that Medicaid financing caps would also limit the ability of states to meet changing needs and demands (e.g. changing state demographics, emerging high-cost drugs, etc.), and could lock-in current state spending patterns that reflect historic Medicaid policy choices. States would likely have to make choices to cover fewer people, cut benefits, and/or lower payment rates for providers (though Medicaid is typically already the lowest payer), leaving more people uninsured and reliant on safety net providers or unable to access care. While states may gain additional flexibility to administer their programs, these new options are not likely to make up for significant cuts in federal spending. States would likely face challenges to maintaining coverage, with certain states (like those with higher health care costs or needs) more at risk. Proposed changes to the FMAP floor or the ACA match rate could reduce federal spending but have disparate effects on states. States with higher per capita incomes could be most affected by calls to lower the FMAP floor while states with lower per capita incomes could be most affected by proposals to have a uniform match rate of 50%. Across many Republican proposals, expansion states would fare worse than non-expansion states with proposals to reduce the expansion match.
Recent KFF polling found that nearly 9 in 10 (86%) Medicaid enrollees want Medicaid to largely continue as it is today, while one in ten (14%) support changing Medicaid to cap federal funding and give states greater flexibility in designing their programs. Somewhat fewer adults overall – though notably still a large majority – say the same (86% vs. 71%). KFF polling has also found that majorities of voters are worried about fraud, waste, and abuse in Medicaid, Medicare, and Social Security as well as in private health insurance plans. Both parties support reducing waste, fraud, and abuse and focusing on oversight of managed care plans and providers; however, there was more of a focus on reducing errors in eligibility determinations during the Trump presidency compared to a focus on oversight of providers and managed care plans during the Biden-Harris Administration.
Context: Medicaid provides financing for a variety of groups and for a wide range of services. To participate in Medicaid and receive federal matching funds, states must meet minimum federal requirements related to who is eligible and what services must be covered. States must provide certain mandatory benefits (e.g., hospital, physician, and nursing home services) to mandatory populations (e.g., children and low-income pregnant people) without waiting lists or enrollment caps. States may also receive federal matching funds to cover “optional” services (e.g., adult dental care and home and community-based services ) or “optional” groups (e.g., children and pregnant people with income above the limits established for mandatory populations). States do have the flexibility to charge premiums and cost-sharing for some enrollees, though federal law limits the extent to which states can impose these measures.
Section 1115 Medicaid demonstration waivers offer states an avenue to test new approaches in Medicaid that differ from what is required by federal statute. While there is great variation in how states have used waivers over time, waivers generally reflect priorities identified by states and the Centers for Medicare & Medicaid Services (CMS). States may obtain “comprehensive” Section 1115 waivers that make broad changes in Medicaid eligibility, benefits, provider payments, and other program rules; other waivers may be narrower and address specific populations or benefits.
Biden-Harris: The Biden-Harris Administration enacted the 2023 Consolidated Appropriations Act, which required states to implement 12-month continuous eligibility for children, made permanent the option for states to extend postpartum coverage to 12 months, and provided states with the option to cover certain justice-involved youth. Vice President Harris has called for reducing maternal mortality and morbidity, including encouraging states to adopt the postpartum Medicaid coverage extension. The Biden-Harris Administration also finalized a rule that aligns and streamlines enrollment and renewal requirements for most individuals in Medicaid; creates timeliness requirements for redeterminations of eligibility; eliminates access barriers for children enrolled in CHIP, such as waiting periods; and facilitates transitions between Medicaid, CHIP, and Marketplace coverage. During the unwinding of the Medicaid continuous enrollment provision, the administration issued guidance and identified a range of strategies and waiver flexibilities states could adopt to limit coverage losses among those who remained eligible.
For the 2025 budget year, the Biden-Harris Administration proposes to require 12 months of postpartum Medicaid coverage, expand state options to provide continuous eligibility for children for multiple years, and eliminate fees and premiums in separate CHIP programs. Further, the Biden-Harris Administration continues to encourage waivers to expand coverage, reduce health disparities, address the social determinants of health, and help individuals transition out of incarceration.
Trump and Republican Proposals: Consistent with the Trump Administration and older legislative proposals, recent Republican proposals would make a number of changes that limit Medicaid eligibility, benefits, and continuity of coverage as well as impose work requirements for enrollees. More specifically, both the RSC FY 2025 budget and Project 2025 propose work requirements, making changes to eligibility thresholds (like eliminating minimum income eligibility for children), establishing flexible accounts (like health savings accounts) to pay for health care, and providing state flexibility to redesign and eliminate certain benefits. Project 2025 also proposes targeted time limits or lifetime caps on benefits, requiring more frequent eligibility redeterminations, and increasing premiums and cost-sharing for some individuals. Capping federal funding, as all Republican proposals examined support, would also have implications for the entitlement (guarantee of coverage for eligible individuals that is part of current law) though none of the proposals clearly note what would become of the entitlement or minimum eligibility thresholds. Section 1115 waiver priorities promoted and approved under former President Trump included eligibility restrictions such as work and premium requirements and other conditions on coverage that did not require legislative changes to advance.
Tradeoffs: The Biden-Harris Administration proposals would expand access to coverage as well as keep more individuals connected to care over time but could increase spending. Continuous eligibility policies, which have been embraced by the Biden-Harris Administration, have been shown to lower rates of “churn,” or the temporary loss of Medicaid coverage in which enrollees disenroll and then re-enroll within a short period of time. When individuals churn on and off coverage, they experience gaps in coverage that can limit access to care and lead to delays in getting needed care. The Biden-Harris Administration proposals would also likely increase enrollment among eligible children by eliminating CHIP premiums and enrollment fees, which can pose barriers to coverage.
In contrast, Republican proposals support more frequent and robust eligibility redetermination processes to ensure that only eligible individuals remain enrolled in the program. However, with more frequent data checks, eligible individuals are at risk for losing coverage if they do not receive or understand notices or forms requesting additional information to verify eligibility or do not respond to requests within required timeframes. Some enrollees, such as working individuals whose monthly income fluctuates, would be at a higher risk of churning on and off Medicaid than others. In addition, most Republican proposals include work requirements. The data show that the majority of Medicaid enrollees are already working, and available implementation data suggests that Medicaid work and reporting requirements are confusing to enrollees and result in substantial coverage loss among eligible individuals who experience challenges with reporting requirements. Republican proposals also provide states additional flexibility by reducing requirements to cover certain benefits and allowing more premiums and cost-sharing. Overall, Republican proposals describe these changes as aligning Medicaid with private insurance, and they would likely reduce federal Medicaid spending. Because people on Medicaid have lower incomes and are sicker than the general population, these changes are also likely to pose barriers to enrollees’ ability to maintain coverage and access needed health care.
Context: All state Medicaid programs have opted to cover prescription drug benefits, and states have flexibility in how they administer the Medicaid pharmacy benefit within federal guidelines about pricing and rebates. Under the Medicaid Drug Rebate Program (MDRP), a manufacturer must enter into a rebate agreement with the Secretary of Health and Human Services, agreeing to rebate a specified portion of the Medicaid payment for the drug to the states and the federal government. In exchange, Medicaid programs cover nearly all of the manufacturer’s FDA-approved drugs, and the drugs are eligible for federal matching funds.
Biden-Harris: The Biden-Harris Administration enacted the Inflation Reduction Act (IRA) of 2022, a major piece of legislation with a number of prescription drug provisions aimed at reducing federal drug spending, including allowing the federal government to negotiate prices for some drugs in Medicare and requiring that drug manufacturers pay rebates for price increases above inflation in Medicare. The latest proposed budget outlines steps to build on the IRA, including expanding the Medicare drug negotiation program. The administration also approved Florida’s plan to import some prescription drugs from Canada, though implementation is contingent on further action by Florida. Within Medicaid, the Biden-Harris Administration has taken action to strengthen the MDRP by lifting the rebate cap, and their latest budget proposal includes provisions to expand the MDRP and allow the federal government to negotiate for supplemental rebates on behalf of state Medicaid programs, though these provisions have not passed. The Biden-Harris Administration also issued a proposed rule (yet to be finalized) aimed at increasing price transparency and established a voluntary model to increase access to cell and gene therapies for people with Medicaid.
Trump and Republican Proposals: The Trump Administration encouraged states to submit waivers allowing states to create closed formularies, enabling Medicaid programs to negotiate directly with manufacturers for drug coverage (under current law, the MDRP creates an open formulary). The Trump Administration also created a new pathway to allow states to import prescription drugs from Canada, finalized a rule allowing manufacturers to report multiple best prices under value-based purchasing agreements with the goal of increasing value-based arrangements in the MDRP, and proposed lifting the rebate cap (this was later lifted by Biden-Harris Administration legislation). Both the RSC FY 2025 budget and Project 2025 seek to repeal the IRA, citing its impact on innovation and patient access, and Project 2025 proposes to address drug shortages by eliminating manufacturer rebate payments for multi-source generic drugs. Further, broader Republican proposals to cut and cap federal Medicaid spending could have implications for prescription drug coverage, as it is an optional benefit.
Tradeoffs: Recent Republican proposals take aim at the IRA while the Biden-Harris Administration plans to continue strengthening the IRA. KFF polling has found most voters are supportive of the Biden-Harris Administration proposals that build on the IRA. While the IRA is expected to lower prescription drug costs for people with Medicare and reduce drug spending by the federal government, the provisions do interact with the MDRP and could increase overall Medicaid prescription drug spending. Both administrations have taken action on drug importation, but, while the idea of importing prescription drugs has bipartisan support among the general public, there are long-standing concerns in terms of ensuring drug safety. The approach is also opposed by the Pharmaceutical Research and Manufacturers of America (PhRMA) and the Canadian government and resulting savings estimates are unclear.
The Trump and Biden-Harris Administration records on the MDRP have diverged, with the Biden-Harris Administration working to strengthen the MDRP while the Trump Administration proposed allowing states to opt out of the program. While opting out of the MDRP could allow states to have more leverage when negotiating (because they could decide not to cover certain drugs completely), it is not clear that a closed formulary would result in savings, and closed formularies can restrict access to drugs for enrollees. Further, recent Republican proposals to address drug shortages and the late-era Trump Administration rule allowing multiple best price reporting could potentially weaken the MDRP and reduce the rebates states and the federal government receive from manufacturers. According to a Congressional Budget Office (CBO) study, rebates in the MDRP result in lower net drug prices in Medicaid compared with other federal programs.
Context: LTSS encompass the broad range of paid and unpaid medical and personal care services that assist with the activities of daily living such as eating and bathing and the instrumental activities of daily living such as preparing meals and managing medication. They are provided to people who need such services because of aging, chronic illness, or disability and may be provided in institutional settings such as nursing facilities or in people’s homes and the community. Services provided in non-institutional settings are known as home and community-based services (HCBS), and those settings may include a person’s home, adult day care centers, assisted living settings, and group homes. Medicaid is the primary payer for LTSS, providing services to an estimated 1.4 million enrollees in nursing facilities and 4.5 million enrollees in HCBS settings.
Federal Medicaid statutes require states to cover nursing facility care and home health, but coverage of other LTSS is optional. Most HCBS are provided through “waivers,” which allow states to offer a wide range of benefits and to choose—and limit—the number of people who receive such services. Unlike other Medicaid services, many states use waiting lists when the number of people seeking services exceeds the number of waiver slots available. An estimated 0.7 million people have been on HCBS waiting lists in most years between 2016 and 2023. Medicaid has historically spent more money on LTSS in institutional settings than on LTSS delivered in home and community-based settings, but over the past decade, Medicaid has spent more on HCBS than institutional care due to states’ community integration obligations under the Americans with Disabilities Act and the Supreme Court’s Olmstead decision. In Olmstead, the Supreme Court held that the unjustified institutionalization of people with disabilities is illegal discrimination and violates the Americans with Disabilities Act. A major challenge for Medicaid HCBS is finding enough workers, with employment levels in elderly care and nursing care facilities remaining below their pre-pandemic levels.
Biden-Harris: The Biden-Harris Administration increased federal financing for and oversight over Medicaid LTSS through increased funding, new legislative proposals, and rulemaking. The Administration enacted ARPA during the pandemic, which included a provision that temporarily increased the federal match rate for spending on Medicaid HCBS by 10 percentage points to expand access to HCBS and support direct care workers. The Biden-Harris Administration also issued legislative proposals calling for more permanent and extensive federal investments in Medicaid HCBS. The Biden-Harris Administration’s FY 2025 budget proposes further HCBS investment, requires the reporting of HCBS quality measures, and includes actions to further increase oversight of nursing facilities. The Administration also finalized several regulatory changes that would bolster Medicaid LTSS:
Several rules aimed at combatting discrimination on the basis of disability, which may provide people with disabilities greater autonomy and independence while they receive Medicaid LTSS;
Requirements for states to provide access to Medicaid HCBS, which includes ensuring payment rates are sufficient to support a workforce, reporting requirements related to waiting lists and other quality measures, and ensuring that 80% of Medicaid payments for certain HCBS are spent on compensation for direct care workers; and
Establishment of the first ever requirements for minimum staffing levels in nursing facilities with increased transparency around the percent of Medicaid payments for institutional LTSS that are spent on workforce compensation and private equity ownership of nursing facilities.
Trump and Republican Proposals: The Trump Administration budgets and other Republican proposals do not include specific changes to Medicaid LTSS, but past policies and current proposals hint that services for older adults may be favored over people with disabilities who are under age 65. The Trump Administration’s regulatory actions generally resulted in less federal oversight over LTSS. The Trump Administration took actions to reduce federal oversight of Medicaid LTSS, including issuing a proposed rule that would have reduced federal requirements for nursing facilities (but was never finalized), suspending routine inspections in nursing facilities during the early months of the COVID-19 pandemic, and delaying requirements for states to comply with federal rules surrounding HCBS (the “HCBS Settings rule).” When COVID-19 vaccines became available, the Trump Administration launched the Pharmacy Partnership for Long-Term Care Program to facilitate COVID-19 vaccinations in facilities where residents are ages 65 and older, though these initial federal vaccine programs did not cover settings that primarily serve people with disabilities under ages 65. Similarly, the 2024 Republican Party platform seeks to expand in-home care for older adults, but does not propose similar expansions for those with disabilities under age 65. It describes “shifting resources,” to support new policies to help seniors remain in their homes but does not specific what programs might be cut to free up such resources. Project 2025 includes language that would allow states “flexibility to redesign eligibility, financing, and service delivery of long-term care to serve the most vulnerable and truly needy and eliminate middle-income to upper-income Medicaid recipients,” which could include eliminating some of the optional Medicaid eligibility pathways that offer coverage to higher-income people who LTSS. Proposals that fundamentally change the financing structure of Medicaid such as cutting or capping federal spending would likely result in restrictions to LTSS.
Tradeoffs: The Biden-Harris Administration Medicaid LTSS policies could expand access to services and increase federal oversight of the quality of services provided but could increase spending on LTSS and reduce states’ flexibility in administering the Medicaid LTSS benefits. The Biden-Harris Administration has consistently called for legislative changes to provide additional funding for Medicaid LTSS (HCBS in particular).
In contrast, it is difficult to anticipate what specific proposals would emerge under a Trump Administration. The Trump Administration’s actions coupled with Republican proposals to eliminate the new nursing facility staffing standards and prohibit the requirement that 80% of Medicaid payments for certain HCBS are spent on compensation for direct care workers suggest that there would be less federal oversight of access to and quality of care, but more flexibility for states in providing Medicaid LTSS. Republican proposals support policies focusing on long-term care and helping seniors to remain in their homes but do not mention a role for Medicaid or home care for people under age 65, and nearly two thirds of people who use Medicaid HCBS are under age 65.
Context: States design and administer their own Medicaid programs within federal rules and determine how they will deliver and pay for care for Medicaid enrollees. Managed care is the dominant delivery system for Medicaid enrollees, with almost three-quarters of Medicaid beneficiaries enrolled in comprehensive managed care organizations (MCOs), accounting for about 52% of total Medicaid spending (or more than $415 billion) in FY 2022. State managed care contracts vary widely, in the populations required to enroll, the services covered (or “carved in”), and the quality and performance incentives and penalties employed. While there are federal and state requirements for managed care plans, plans have flexibility in certain areas, including in setting provider payment rates.
Managed care plans are at financial risk for the services covered under their contracts and receive a per member per month “capitation” payment for these services. To limit the amount that plans can spend on administration and keep as profit, CMS requires states to develop capitation rates for Medicaid to achieve a medical loss ratio (MLR) of at least 85%. The MLR reflects the proportion of total capitation payments received by an MCO spent on clinical services and quality improvement, where the remainder goes to administrative costs and profit. While there is no federal requirement for Medicaid plans to pay remittances to the state if they fail to meet the MLR standard, states have discretion to require remittances.
Biden-Harris: The Biden-Harris Administration released final Medicaid managed care regulations in 2024 aimed at improving access to care, quality, health outcomes, and health equity. The new rules establish national maximum wait time standards for certain appointments and a requirement for states to conduct independent secret shopper surveys to validate MCO compliance with wait time standards. The Biden-Harris Administration also finalized rules related to plan prior authorizations focused on streamlining process, reducing approval wait times, and improving transparency. The Biden-Harris Administration has taken action to improve Medicaid managed care monitoring, oversight, and transparency, releasing reporting templates and toolkits for states and publicly posting state managed care annual reports.
The Biden-Harris Administration enacted the 2024 Consolidated Appropriations Act, which included a financial incentive to encourage certain states to collect remittances from Medicaid MCOs that do not meet minimum MLR requirements. The Biden-Harris Administration’s FY 2024 and 2025 budgets went further proposing to require Medicaid managed care plans to meet an 85% minimum MLR and to require states to collect remittances if plans fail to meet the minimum MLR. The most recent budget also included provisions aimed at strengthening CMS’s Medicaid managed care financial oversight and compliance tools.
Trump and Republican Proposals: During his presidency, Trump took administrative action to change Medicaid managed care rules, including relaxing rules around network adequacy and beneficiary protections. Trump’s FY 2020 budget proposed changes to the Medicaid managed care waiver process (e.g., to lengthen the duration of certain managed care waivers) aimed at reducing administrative burden. Project 2025 notes the intent to reform and increase oversight of Medicaid managed care but doesn’t provide specifics. Proposals that fundamentally change the financing structure of Medicaid would likely also have implications for the delivery of care in Medicaid, impacting managed care plans.
Tradeoffs: Recent Democratic administrations have made sweeping changes to Medicaid managed care rules and regulations to advance program goals related to access to care, quality, fiscal and program integrity, beneficiary protections and support, and monitoring and oversight. However, establishing national standards and other state requirements can add state administrative burdens to come into compliance. The Biden-Harris Administration’s most recent budget proposed requiring Medicaid managed care plans to meet a minimum MLR of 85% (the statutory requirement for Medicare Advantage plans) and requiring states to collect remittances from plans if they fail to meet the required minimum (which would likely result in Medicaid savings)—to encourage plan investment in services and quality improvement and to prevent the retention of excessive profits.
The Trump Administration finalized changes to Medicaid managed care rules with chief goals that differed from Democratic administrations. The Trump Administration’s stated goals included reducing state and federal administrative burden, streamlining regulations, and promoting state flexibility and innovation in care delivery; however, tradeoffs could include fewer beneficiary protections, less oversight involving access to care, and variation in oversight across states.
With Vice President Harris promising to address medical debt as part of her economic plan, KFF Executive Vice President for Health Policy Larry Levitt explores why it is a symptom of the broader problem of affordable health care and reviews recent efforts to address it in this JAMA Health Forum post.
Note: Figure 1 was updated on April 30th, 2025, to reflect the recent passage of cell phone ban legislation in Arizona and New York.
Heading into the 2024-2025 school year, a growing number of states are implementing or considering state-wide bans on cellphones in schools. Many leaders in education and policymakers suggest cellphone bans will help mitigate youth mental health concerns and distractions during academic instruction. The resurgence of cellphone bans follows two advisories from the U.S. Surgeon General on the youth mental health crisis and the harmful impacts of social media use and recommendations from UNESCO to limit cellphone use in schools across the world. Unlike many recent political issues, school cellphone ban policies have largely received bipartisan support, and the Biden-Harris administration continues to promote online safety for youth. At the same time, research on the effectiveness of cellphone bans is limited, and although multiple states are adopting these bans, challenges remain with enforcement, accommodating exceptions, and equity.
How widespread are school cellphone bans?
Cellphone bans began decades ago amid concerns about drug deals among students via cellphones or pager devices, and have fluctuated since. In 2009, 91% of public schools prohibited cellphone use, which fell to 66% in 2015 before rising again to 76% in 2021. Cellphone bans are now being considered at the state level in light of growing student academic and mental health concerns that are associated with excessive use of smartphones.
Eleven states have passed state-wide policies that ban or restrict cellphone use in schools as of April 30th, 2025 (Figure 1). These policies vary from state to state.
Arizona’s Governor signed a bill in April of 2025 that instructs schools to limit student cell phone use during the school day, including non-instructional time, with exceptions for educational and medical purposes. The bill also directs schools to restrict internet and social media access for students.
Arkansas‘ Governor signed a law in February 2025 requiring each school district to create a cell phone use policy before the 2025-2026 school year that limits students’ phone use during the school day, following its pilot program in 2024. Policies must be submitted to and approved by Arkansas’ Division of Elementary and Secondary Education.
California’s Governor recently signed the Phone-Free School Act, which requires school districts and charter schools to develop and adopt a phone policy that either limits or entirely prohibits smartphone use during school by July of 2026. Exceptions will be made for medical necessity, emergencies, educational purposes, or with faculty permission.
Florida passed a phone ban for K-12 classrooms that prohibits cellphone use during class time and blocks access to social media for all devices on district Wi-Fi. Additionally, there is a digital literacy component beginning in sixth grade that requires education on the spread of misinformation on social media and digital footprints. The ban went into effect in July 2024.
Indiana’sban prohibits students from using any portable wireless device (including cellphones, gaming devices, laptops, and tablets) during instructional time, with exceptions from teachers and/or administrators, or during emergencies. Each school board in Indiana is then expected to draft and publicly post specific policies for their schools – i.e. whether students can access their devices during lunch or what consequences students may face for using prohibited devices. The ban went into effect in July 2024.
Louisiana passed a ban, which will take effect in the 2024-2025 academic year, that prohibits both the use and possession of cellphones throughout the school day. If cellphones are brought onto school property, they must be turned off and stored away. Exceptions can be made for students who require learning accommodations.
Minnesota’s bill instructs school districts and charter schools to adopt policies on student cell phone use and possession by March 2025, but it does not specify the nature or extent of these policies.
New York’s governor signed a bill in April of 2025 instructing school districts to create and implement plans to restrict all student cellphone use during the school day, including non-instructional time, by the 2025-2026 academic year.
Ohio’s ban, similarly to Indiana’s, requires every school district to create and implement official policies regarding cellphone use at school. The bill includes exceptions for those with health conditions that require monitoring or for learning accommodations. The bill will take effect in July 2025.
South Carolina’s ban was implemented via the Governor’s Budget Proviso 1.103, which requires public schools seeking State Aid to Classrooms to implement the model policy drafted by the State Board of Education beginning in January 2025. The Board’s model policy was approved in September of 2024, prohibiting students from accessing unauthorized electronic devices unless authorized for educational or health purposes. A special exception is made for students who volunteer for emergency response organizations, who must receive written permission.
Virginia’s Governor established Executive Order 33, which ordered state officials to solicit public opinion regarding cellphones in schools to allow them to create definitions of “cellphone-free education” and to publish both model implementation plans and draft policy guidance to inform public school systems’ phone policies. The governor also ordered the state to make $500,000 available to support the implementation of school cellphone policies.
Seventeen states have introduced state-wide legislation that bans or restricts cellphone use in schools and education departments in seven states have issued recommended policies or pilot programs that similarly aim to ban or restrict cellphone use in schools (Figure 1). States are taking a variety of measures to mitigate cellphone use during instruction time. In Connecticut and West Virginia, their respective education departments have issued guidance on restricting cellphone use in schools (Figure 1). Pilot programs via the education department in Delaware allocate funds for students to use lockable magnetic phone pouches during school hours. Similarly, while legislation is under consideration in Pennsylvania, the Governor amended the existing School Safety and Mental Health grant program, allowing for the purchase of lockable phone pouches. Georgia has restricted access to social media platforms during school, and New Jersey established a commission to study the effects of social media use at school. Utah introduced a bill that subsequently failed, but draft bills indicate that these states continue to work towards phone-free learning environments.
Implementation and enforcement of cellphone bans may be difficult to navigate. The enforcement of these cellphone bans often becomes an added responsibility for teachers. Exceptions to these bans are also challenging to navigate as many students may need their devices for medical reasons or parents have differing expectations for maintaining contact. Additionally, cellphone bans have brought to light equity concerns – for example, New York’s prior state-wide cellphone ban was lifted in 2015 in part because of stricter enforcement at schools serving students from low-income households compared to schools serving students from high-income households. At the same time, banning cellphones has been linked to positive outcomes, such as improved test scores, especially among students who typically do not perform as well academically.
What is the connection between cellphone use and mental health?
Youth often use cellphones to access social media and social media is linked to poor mental health. In 2023, a survey of adolescents found that 51% reported using social media for at least four hours per day. Adolescent social media use is associated with higher rates of anxiety and depression, exposure to harmful content – the effects of which adolescents are more susceptible to – and body dissatisfaction and eating disorders, especially among girls. Excessive social media use and social media addiction are associated with sleep issues, which may result in negativeneurologicaleffects. However, social media use among youth can also be beneficial as it allows for self-expression, finding communities with shared interests, and accessing important resources, including mental health resources.
Approximately nine in ten public schools report occurrences of cyberbullying – a form of bullying through technological devices, including cellphones – among students (Figure 2). Cyberbullying is associated with social and emotional distress, depression, and suicidalideation among youth and is more often experienced by female and sexual minority youth compared to their peers. In 2023, 16% of high school students reported electronic bullying, and this was heightened among LGBT+ adolescents (25%) and females (21%). Technological devices can also be used to create and spread digitally altered pornographic content without consent – a practice that primarily targets females and may negatively impact their mental health. Further, cellphoneownership among youth is linked to increased experiences of cyberbullying.
Excessive cellphone use can distract from in-person socialization and is associated with loneliness among adolescents. Establishing and building relationships with peers is beneficial to youth well-being and can have a protective effect on adolescents experiencing adversity. With the distraction of cellphones, peer relationship-building may be negatively impacted.
Approximately 40% of public schools report moderate to severe negative impacts on student learning and on teacher and staff morale when students use their electronic devices without permission (Figure 3). Many teachers report that students being distracted with their cellphones is a major problem in their classrooms and that enforcing cellphone restrictions is challenging. The presence of smart phones may reduce cognitive capacity, especially for those highly addicted to their phones, and notifications disrupt focus and attention. Further, there is a negative association between time spent on smartphones and academic performance.
What is known on the effectiveness of cellphone bans and other actions to address youth mental health?
While evidence on the outcomes of school cellphone bans is limited, widespread concerns regarding the harms of smartphone use on youth well-being continue to invoke action by policymakers and leaders in education. Emerging research on student outcomes is mixed, with some studies suggesting improvements in student mental health and academic performance and a reduction in bullying, and othersshowing little to no change. While evidence on school bans is inconsistent, rising concerns regarding the harms of social media and internet use among youth have led to policy and safety measures being introduced at the state and federal level. For instance, policymakers recently introduced bipartisan legislation – the Focus onLearning Act – that calls on the U.S. Department of Education to conduct studies on the impact of cellphone use on students’ academic and mental health outcomes, among other provisions. Additionally, as of December 2024, the U.S. Department of Education called on all states and districts to adopt measures to manage cellphone use in schools and published guidance which includes example policies, considerations to accommodate needs of different populations, and policy evaluation and modification guidelines. This guidance was published in response to the Biden-Harris Administration’s efforts to address youth mental health and online safety. Other multi-prong approaches are also being implemented, such as the Biden-Harris administration’s continued efforts to improve online safety for children. These include creating the Kids Online Health and Safety Task Force, which recently released Best Practices for Families and Guidance for Industry, and a Call to Action to mitigate image-based sexual abuse. Additionally, the Surgeon General recommended that social media platforms include a warning label that states that social media is linked to poor mental health among adolescents.


 Irving Washington
Irving Washington  Hagere Yilma
Hagere Yilma