Opioid Deaths Fell in Mid-2023, But Progress Is Uneven and Future Trends are Uncertain
Since the opioid epidemic was declared a public health emergency in 2017, it has claimed 454,464 lives, with opioid-related deaths rising by 67% between 2017 and 2023. Initially driven by prescription opioids and heroin, the epidemic has shifted in recent years, with illicit synthetic fentanyl—a substance 100 times more potent than morphine—now dominating most markets. Even a small amount of fentanyl can be lethal, and in 2023, 7 in 10 counterfeit opioid pills contained a deadly dose.
Although provisional CDC data show a decline in opioid deaths in 2023, the death toll remains much higher than just a few years ago, keeping this issue in the spotlight. Both former President Trump and Vice President Harris have records related to addressing the opioid epidemic, but they also have proposed different approaches to ongoing and future efforts to address the issue. Trump’s 2024 campaign emphasizes a stricter law enforcement strategy aimed at reducing trafficking, primarily through reinstating and tightening border policies and tougher punishment, including the death penalty for “traffickers and drug smugglers.” In contrast, the Biden-Harris administration’s multi-pronged strategy includes reducing supply, expanding harm reduction, and improving access to treatment, with Harris placing a stronger emphasis on increasing fentanyl seizures through enhanced detection technology at the border and ports. Along with the 1 in 3 adults who report in a KFF survey that they or a family member have been addicted to opioids (29%) or illegal drugs (27%), both President Biden and Vice-Presidential hopeful J.D. Vance have close family members who have experienced addiction.
This analysis examines opioid overdose deaths from the last two decades (2003-2023), with a particular focus on the decline in deaths observed in the last six months of 2023. Opioid overdose deaths include fatalities from intentional acts (suicide or homicide), unintentional acts (poisoning or drug assault), or cases of unknown intent. Regardless of other substances involved, any death with opioid involvement is classified as an opioid overdose death. According to provisional 2023 CDC WONDER data, fewer than 1% of deaths remain undetermined. Key takeaways from this analysis include the following:
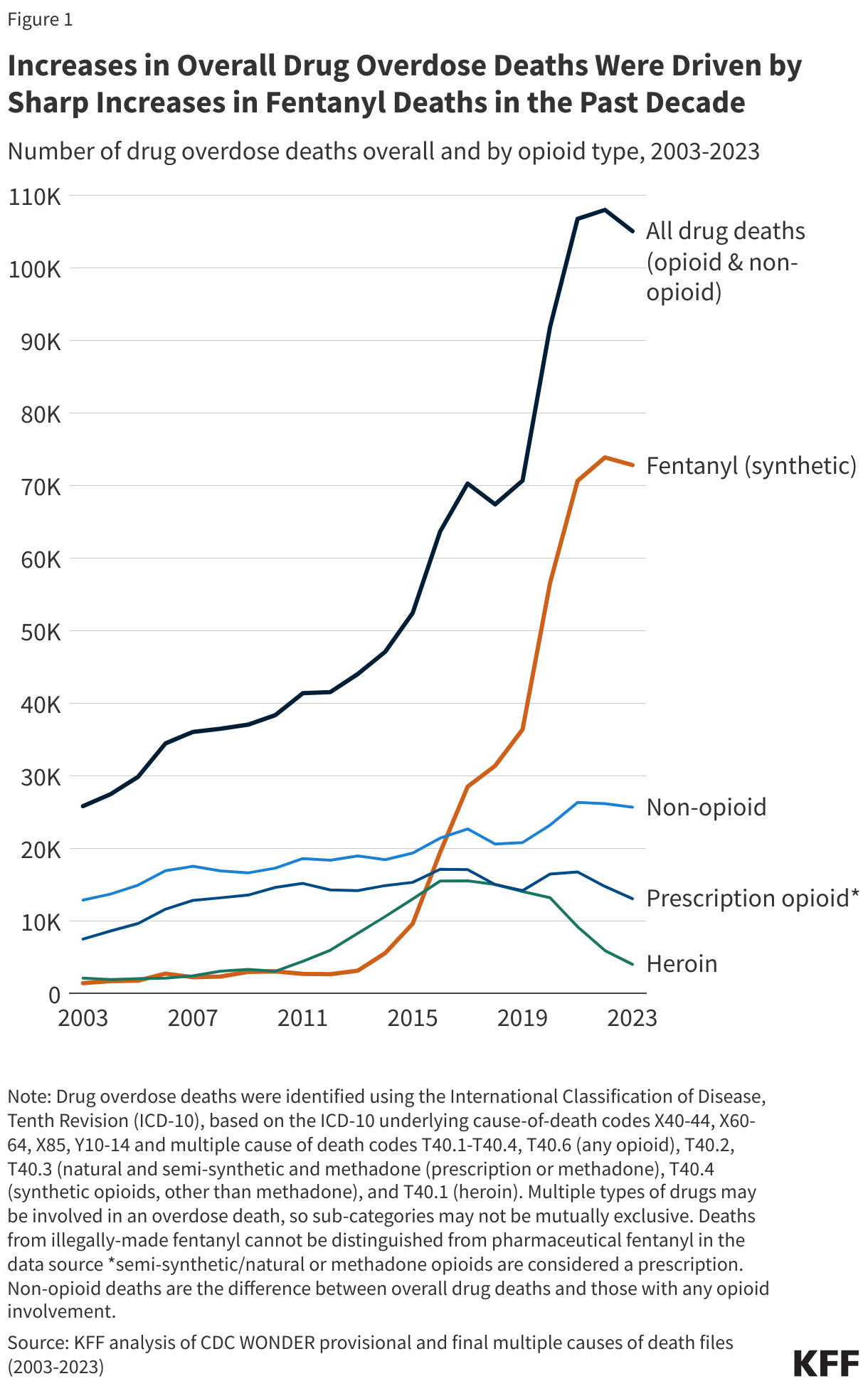
- Fentanyl-involved opioid deaths drove rises in overall overdose deaths, by over 23-fold from 2013 to 2023, while prescription opioid deaths stayed steady and heroin deaths declined.
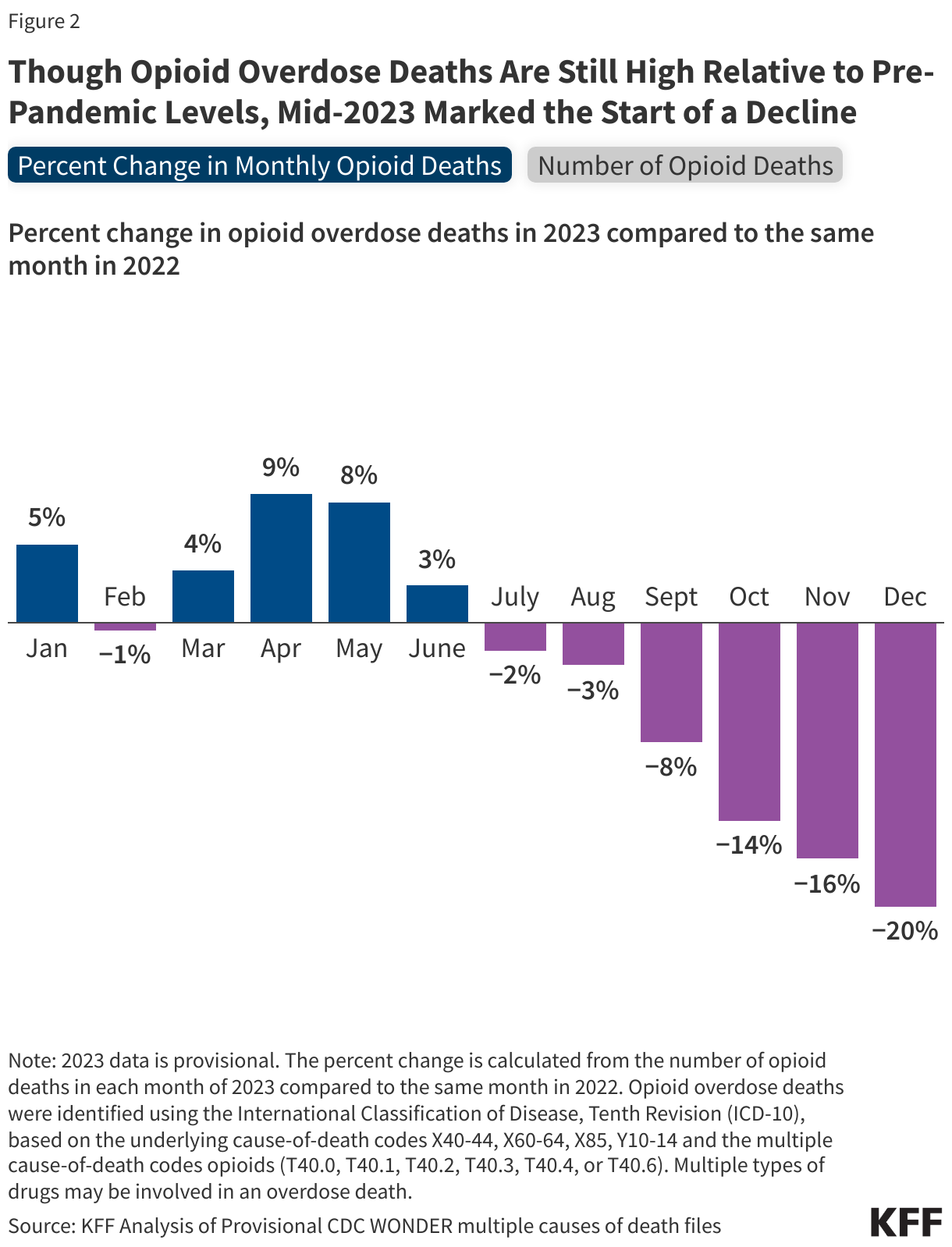
- In the second half of 2023, opioid overdose deaths started to decline, and by December 2023, they were 20% fewer than there were in December 2022. While it is unclear how much any specific policy may have contributed to the decline, a number of policies were implemented, including those focused on reducing supply of fentanyl, increasing treatment, and improving access to harm reduction supplies—such as opioid overdose reversal medication.
- Opioid death rates varied widely by race, ethnicity, age, and sex. In the second half of 2023, White people saw the largest decline (-14%) while declines in other racial and ethnic groups were much smaller. Opioid deaths increased for people 65+, while falling in all other age groups.
- In 2023, opioid death rates were the highest in WV, DC, and DE (71.4, 49.9, and 47.5/100,000, respectively), while states with the lowest opioid death rates included NE, SD, and IA (4.3, 5.7, and 8.4/100,000, respectively). In three-quarters of states, opioid deaths declined in the last six months of 2023 compared to the same period in 2022.
What are the trends in opioid deaths?
The sharp rise in drug deaths in recent years was driven by fentanyl deaths. Fentanyl-involved opioid deaths surged more than 23-fold over the last decade, while prescription opioid deaths remained steady and heroin deaths declined. Fentanyl deaths more than doubled during the pandemic, increasing from 36,359 in 2019 to 73,838 in 2022 (Figure 1). Illicit synthetic fentanyl (referred to as fentanyl for simplicity) is inexpensive to produce and often mixed into other drug supplies, such as methamphetamine and cocaine. In addition to increases in fentanyl supply, other factors, such as pandemic-related stressors, disruptions in treatment, and other life challenges, as well as insufficient treatment infrastructure and a shortage of skilled providers, may have contributed to rises in opioid deaths.
In the second half of 2023, opioid overdose deaths began to decline and continued to fall through the end of the year. In July 2023, deaths were 2% lower than in July 2022, and by December, they were 20% lower compared to December 2022. Looking at 2023 alone, opioid deaths dropped from 6,928 in July to 5,841 in December, a decrease of over 1,000 deaths (Figure 2). Early provisional and partial data for the first quarter of 2024 point to a continuation of this downward trend through early 2024.
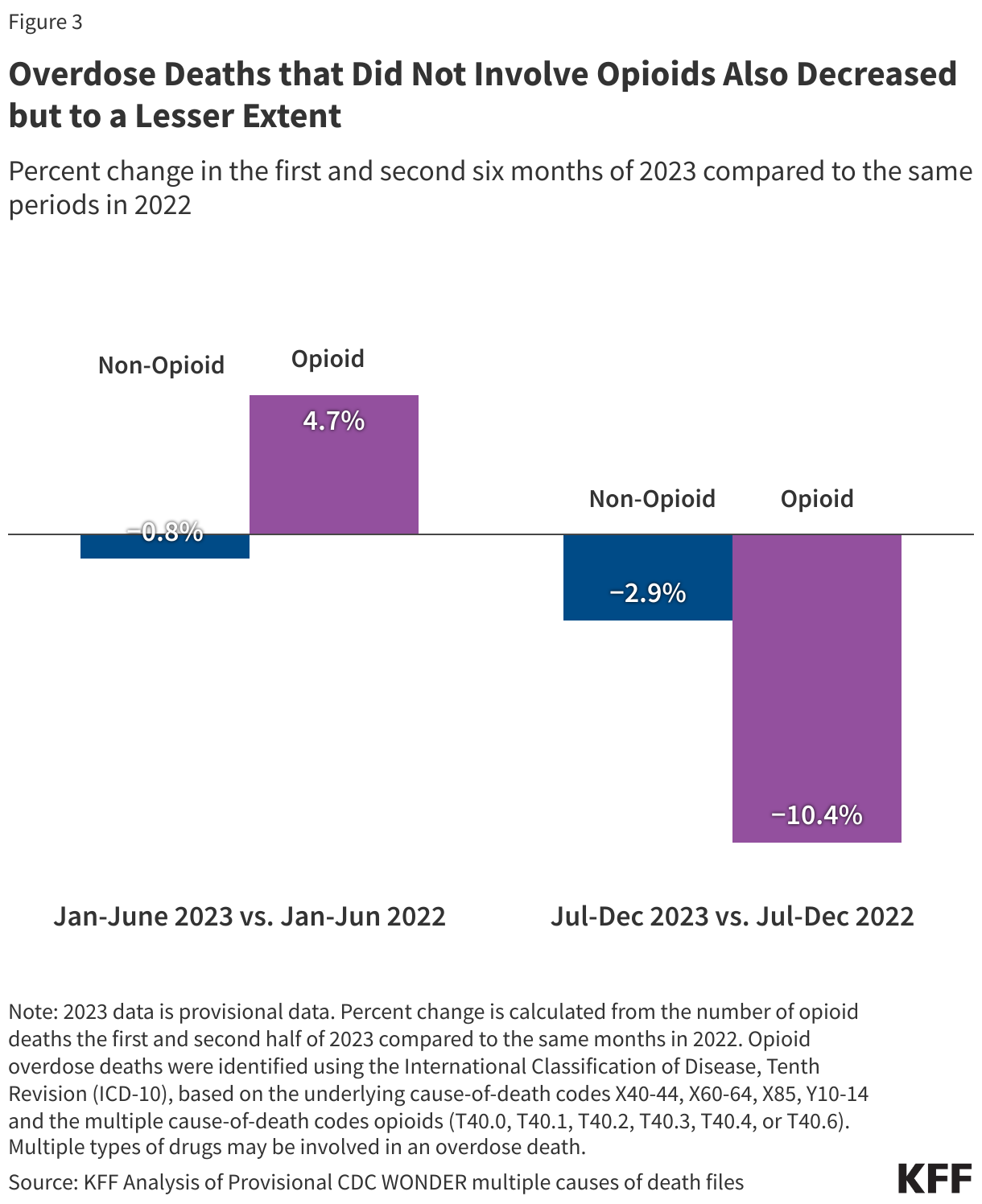
Non-opioid overdose deaths also fell in the last half of 2023 compared to the previous year, though the decline was smaller (-3% vs. -10% for opioid deaths) (Figure 3). Non-opioid deaths refer to drug overdose deaths that did not involve opioids, such as those involving only non-opioid drugs, like cocaine or methamphetamine. Non-opioid deaths account for a much smaller share, about one-third, of overall drug overdose deaths.
While it is too early to determine if the decline in opioid overdose deaths will continue, several federal policies aimed at reducing deaths may have played a role. The Biden-Harris administration’s strategy for the opioid epidemic focuses three key areas: expanding harm reduction and public awareness, improving access to treatment and supports, and reducing the supply and spread of illicit drugs, particularly fentanyl. FDA’s approval of the first over the counter opioid overdose medication likely increased public access to the medication. Federal opioid response grants and settlement funds supported low-barrier distribution of naloxone and other harm reduction tools, like fentanyl test strips, while campaigns like the DEA’s “One Pill Can Kill,” raised public awareness of fentanyl risks. Federal policies extended or permanently relaxed in-person requirements for methadone and buprenorphine treatment. Federal investments in the broader mental health services, such as 988 and mobile crisis, may have also contributed, perhaps through connections to care. Efforts to reduce fentanyl supply are also ongoing, with increased seizures at U.S. borders and ports of entry.
How do opioid death rates vary across demographics groups?
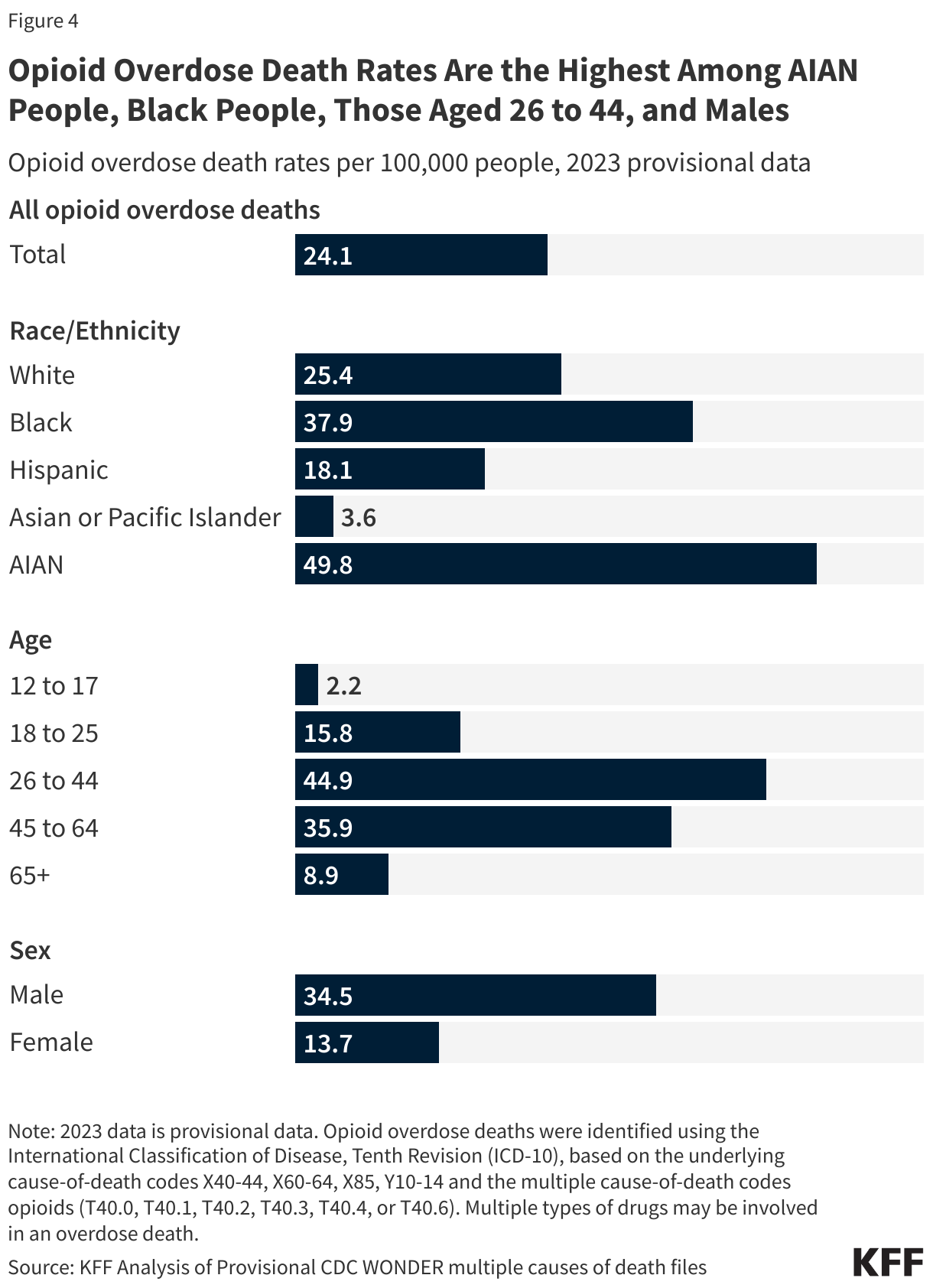
In 2023, opioid death rates were highest among American Indian/Alaska Native (AIAN) and Black people, individuals aged 26 to 44, and males (Figure 4). AIAN and Black people had the highest death rates across race and ethnicity, at 49.8 and 37.9 per 100,000, respectively. Earlier in the opioid epidemic, overdose rates were highest among White people, but this trend shifted with opioid death rates for Black people surging over 700%, compared to a 140% rise for White people in the past decade. The high rates of opioid deaths among American Indian and Alaska Native (AIAN) people mirrors broader worsening trends in behavioral health, including the highest and fastest-growing suicide and overall drug overdose rates. Among age groups, those aged 26 to 44 had the highest death rates, followed by those aged 45 to 64. Although people aged 12-17 and 65+ have lower overall rates, these groups have seen substantial increases in recent years. In 2023, opioid death rates among males were more than double those of females, with males also experiencing the largest increase over the past decade, rising 238%.
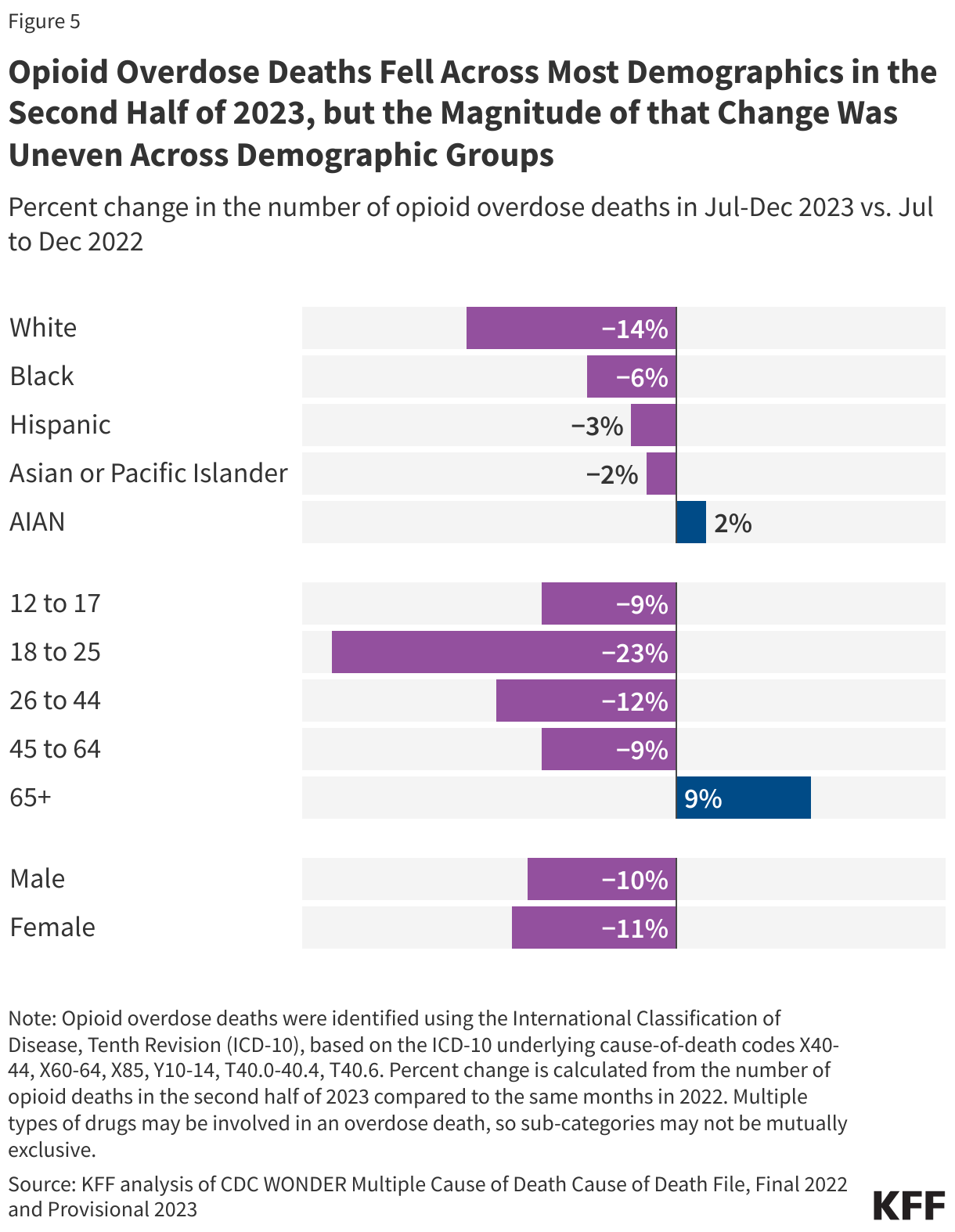
Opioid overdose deaths decreased across most racial and ethnic groups from the last 6 months of 2023 compared to the same period in 2022, but drops were greater among White people (-14%) compared to other racial and ethnic groups (-2 to -6%, Figure 5). The larger decline in these deaths among White people may reflect racial disparities in access to OUD treatment. Prior KFF analyses found that White people were more likely to have access to medications used to treat OUD compared to Black and Hispanic people. The uptake of medication treatment services is also low among AIAN people.
While opioid overdose deaths decreased for all non-elderly age groups in the last six months of 2023, they increased for elderly adults (65+). Young adults saw the largest decline (-23%) in opioid deaths from the second half of 2023 compared to the second half of 2022. The rise in overdose deaths among elderly adults (9%) during the same period may be linked to challenges in detecting and treating substance use disorder (SUD) in this group, as symptoms can be mistaken for age-related decline. When a SUD is identified, stigma, decreased social support, transportation, and physical comorbidities can complicate access to treatment services—along with few SUD treatment programs that are designed for geriatric adults. Older adults have higher rates of opioid prescriptions, but co-prescribing of overdose reversal medication is low.
How do opioid death rates vary across states and how have they changed?
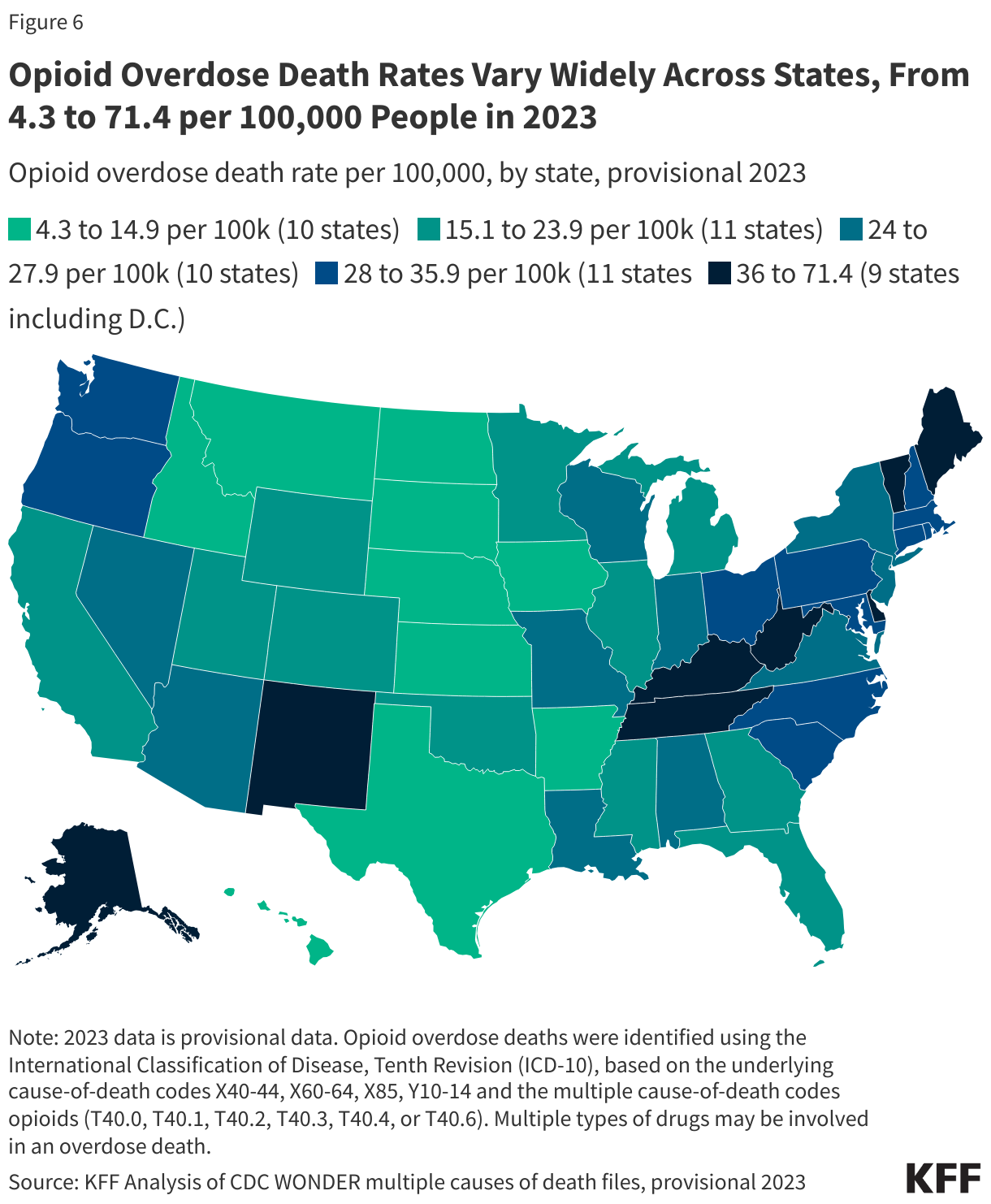
Opioid overdose death rates varied widely across states in 2023, from 4.3 per 100,000 in Nebraska to 71.4 per 100,000 in West Virginia (Figure 6). Nebraska, South Dakota, and Iowa had the lowest rates, with 4.3, 5.7, and 8.4 deaths per 100,000 people, respectively. West Virginia had the highest rate at 71.4 per 100,000—over 40% higher than the next highest rate in D.C., which was 49.9 per 100,000. The national opioid death rate was 24.1 per 100,000, with 33 states having rates within 10 deaths per 100,000 of the national death rate (Figure 5).
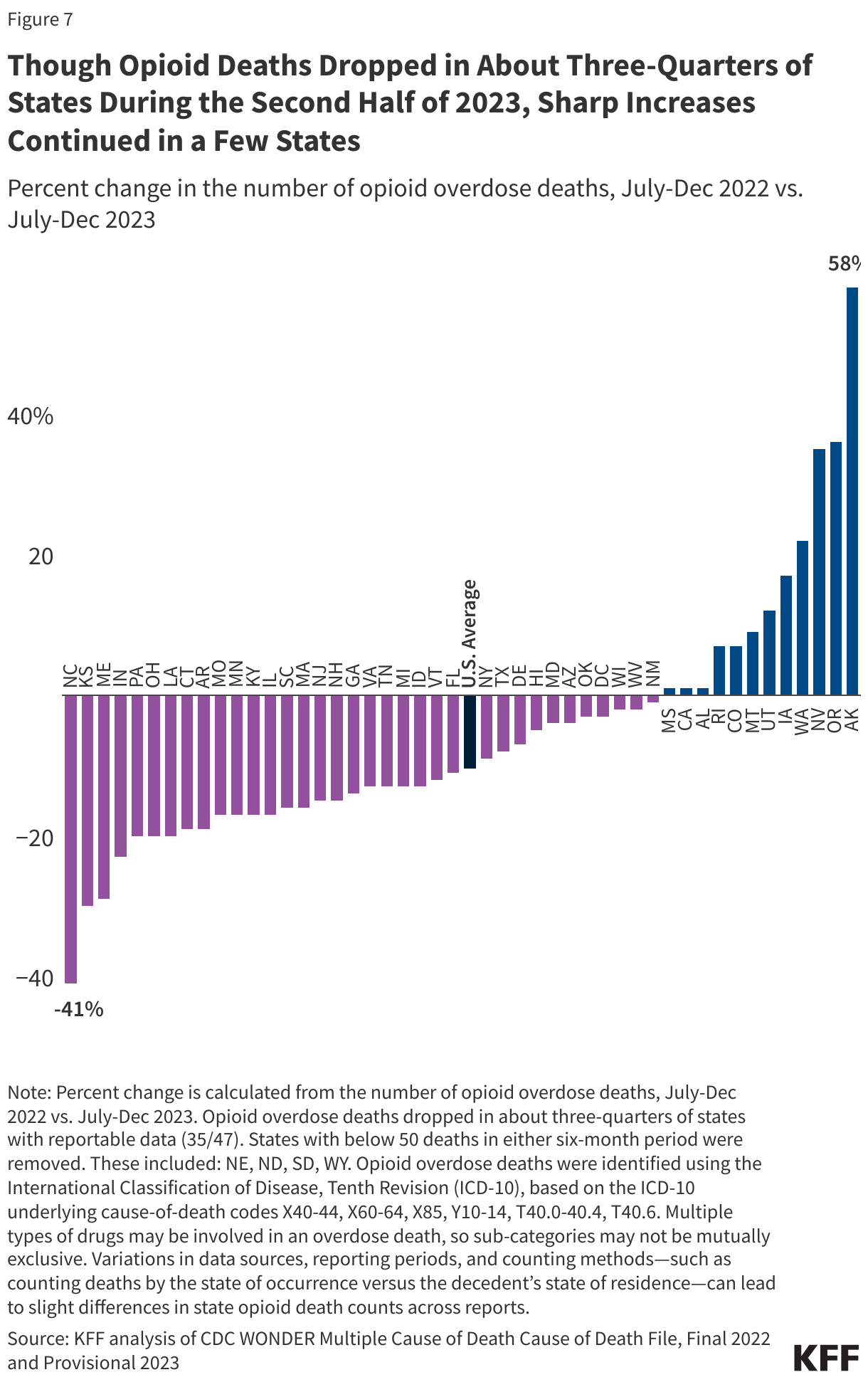
The last 6 months of 2023 brought drops in opioid deaths nationally and in about three quarters of states, compared to the same months in 2022 (Figure 7). Over this period, opioid overdose deaths decreased the most in North Carolina (-41%), remained relatively steady in New Mexico and Mississippi (-1%, +1%, respectively), and increased the most in Alaska (+58%).
States can develop their own approaches to addressing the opioid epidemic or build on federal initiatives, but state actions vary. State decisions about allocation of state opioid response grants and settlement funds for low barrier access to naloxone and other harm reduction tools, as well as efforts to ease access to treatment vary by state and may impact outcomes. Some states, like Virginia, have invested in campaigns to expand awareness about fentanyl in drug supplies, building on federal messaging campaigns like the DEA’s “One Pill Can Kill.” State decisions on Medicaid coverage and limits for certain populations and substance use services, along with whether to adopt federal opportunities that expand treatment and health coverage to high-risk groups, such as incarcerated individuals nearing release, may also influence outcomes.