Potential Effects of the Proposed Medicaid Eligibility Rule for Newly Enrolled Medicare-Medicaid Enrollees
Editor’s Note: This brief was updated on April 3, 2023. We reduced the follow-up period in our analysis from 12 months to 11 months, which aligns with CMS’ approach for analyzing Medicare administrative data.
On August 31, 2022, the Centers for Medicare & Medicaid Services (CMS) released a proposed rule designed to make it easier for people to obtain and maintain coverage in Medicaid. Among the many changes in that rule are several major changes to the eligibility process for people with Medicare who are also eligible for help from Medicaid. CMS proposes to better integrate Medicaid applications with eligibility and enrollment data based on Medicare Part D Low-Income Subsidies (LIS) for prescription drugs. The proposed rule would also automatically enroll some people in Medicare Savings Programs where Medicaid pays their Medicare premiums and, in many cases, cost sharing, for people with limited financial resources.
In this issue brief, we estimate rates of Medicaid coverage loss among people who became Medicare-Medicaid enrollees (MMEs) during 2018 for the first time. They may have had Medicare or Medicaid in a prior year, but were newly dually-eligible for both programs. We compare outcomes for partial-benefit MMEs and full-benefit MMEs. For partial-benefit enrollees, Medicaid pays Medicare premiums and, in many cases, also pays Medicare’s deductibles and cost sharing on behalf of MMEs. Full-benefit MMEs also receive the full range of Medicaid benefits that are not covered by Medicare, such as long-term services and supports and non-emergency medical transportation. Among full-benefit MMEs, we defined loss of coverage as losing full Medicaid benefits. In 2018, there were 12.0 million MMEs in the 50 states and D.C., including 11 million in the 42 states included in this analysis. Of those 11 million, we included 1.3 million newly-enrolled MMEs in the analysis. See methods for further details on the study population and outcomes of interest.
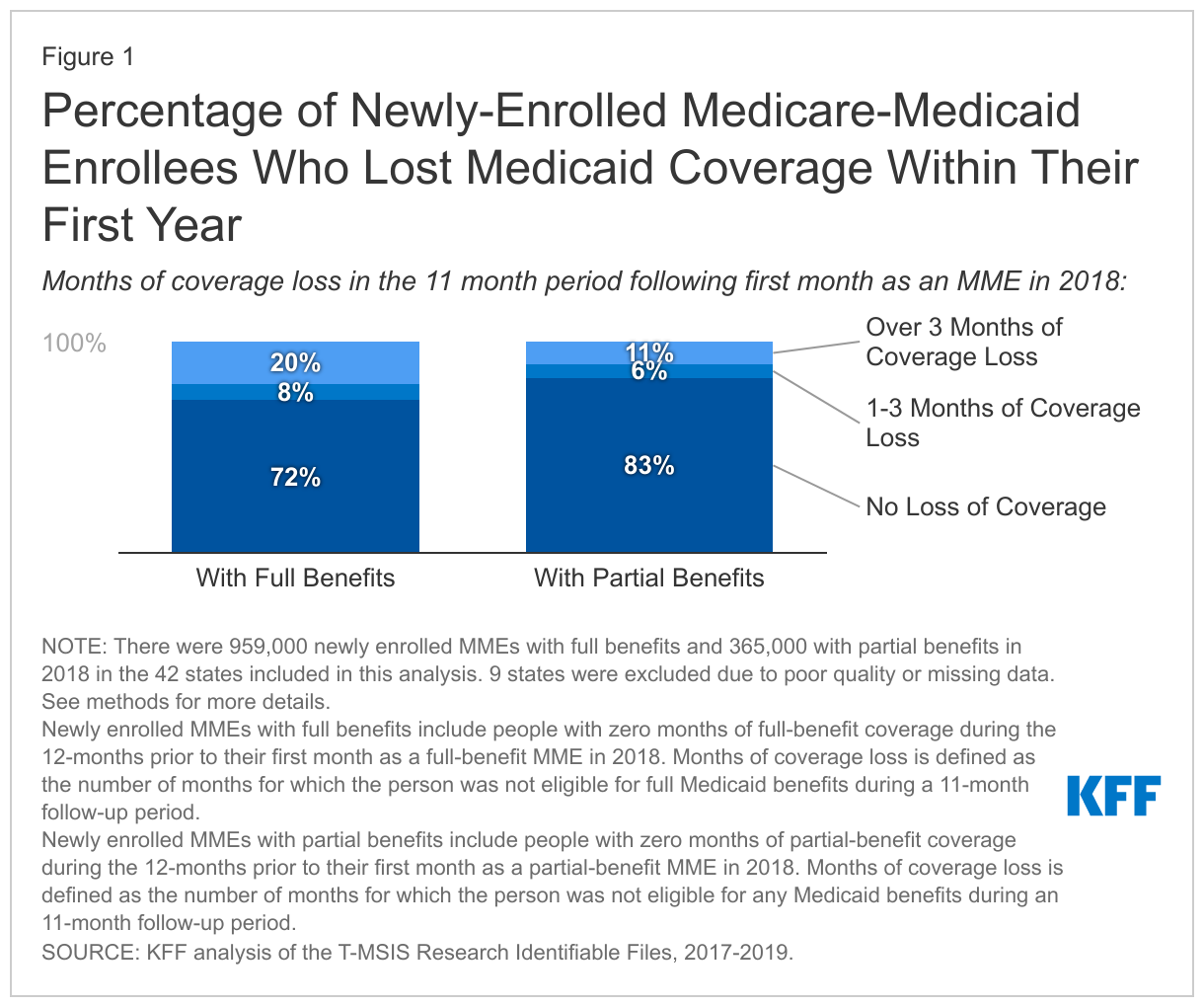
Our analysis finds that 28% of newly-enrolled full-benefit MMEs in 2018 lost coverage within their first year of enrollment and 20% lost coverage for more than 3 months. Among newly-enrolled partial benefit MMEs, 17% lost coverage for one or more months and 11% lost coverage for more than 3 months. Such substantive rates of Medicaid coverage loss among Medicare beneficiaries are notable because many Medicare beneficiaries live on fixed incomes and are unlikely to experience increases in income or assets that would trigger losing eligibility for Medicaid. Instead, the loss of Medicaid likely reflects administrative burdens associated with verifying applicants’ eligibility and renewing their enrollment. The proposed rule aims to reduce Medicaid coverage loss by reducing those burdens.
How Does the Proposed Rule Simplify Eligibility and Enrollment Processes for Medicare-Medicaid Enrollees?
The Medicaid proposed rule addresses several factors that contribute to high rates of Medicaid coverage loss among Medicare enrollees. The proposed rule would simplify the eligibility process for MMEs. Those changes are intended to increase enrollment among Medicare beneficiaries who have never enrolled in Medicaid and to reduce the number of Medicaid enrollees who lose coverage only a few months after enrolling on account of administrative barriers. Specifically, the rule would:
- Encourage states to use the LIS definitions of financial resources so that the financial resource documentation Medicare beneficiaries complete for LIS would also document eligibility for Medicaid,
- Require states with definitions of financial resources that differ from LIS to accept applicants’ self-reported value of resources unless the state already has information that is inconsistent with that value, and
- Require states to assist applicants with procuring appropriate documentation validating income and assets when it is required.
The rule also aims to reduce loss of Medicaid at the time of renewal. Those changes are intended to reduce the number of Medicaid enrollees who are still eligible but lose coverage during the renewal process on account of administrative barriers. Specifically, the rule would:
- Require states to renew Medicaid only once per year,
- Eliminate states’ option to require an in-person interview as part of the application process,
- Apply other simplified enrollment and renewal requirements that already exist for children and other adults in Medicaid, and
- Institute requirements for how states must respond when mail to an applicant or enrollee is returned.
CMS estimates that the changes affecting MMEs would result in an additional 1.5 million person-years of Medicaid enrollment, nearly $7 billion in additional Medicaid spending, and nearly $3 billion in additional Medicare spending in the year 2027. Medicaid spending would increase because Medicaid would be paying for additional months of Medicare premiums and in some cases, Medicare cost sharing and Medicaid benefits. Medicare spending is expected to increase because Medicaid coverage of cost sharing would lead MMEs to use more Medicare-covered services. Because the enrollment process would be simpler and there would be fewer renewals, the proposed rule would decrease Medicaid administrative spending. (CMS estimates that administrative spending would decrease by over $1 billion in 2027, but that includes administrative savings from provisions that would affect all Medicaid and CHIP enrollees in addition to the provisions affecting MMEs.)
What Do the Data Show?
In describing the proposed changes, CMS cited a study that showed nearly 30% of Medicare-Medicaid enrollees (MMEs) lost Medicaid for a least one month and over 20% lost coverage for more than 3 months in the year after their initial enrollment month. That study used Medicaid claims data from 2006 – 2010 and limited the analysis to full-benefit MMEs. The Medicare-Medicaid Coordination Office within CMS recently updated that analysis using Medicare administrative data from 2016 – 2018. Their new analysis found that rates of coverage loss were largely unchanged.
KFF finds that 28% of newly-enrolled full-benefit MMEs in 2018 lost at least one month of coverage within their first year of enrollment (Figure 1). The analysis also finds that 20% lost over three months of coverage. New partial-benefit MMEs in 2018 had lower loss of coverage than full-benefit MMEs, with 17% losing at least one month of coverage within their first year of enrollment and 11% losing over 3 months. Among those MMEs who lost coverage within the first year, the vast majority lost coverage for more than 3 months. People who lose Medicaid coverage for more than 3 months include some Medicare beneficiaries who lost Medicaid at the time of renewal in states that do more than one renewal period per year. There are also people losing Medicaid before the renewal period which may suggest that individuals were disenrolled due to post-enrollment eligibility verification. Post-enrollment eligibility verification may require submission of detailed financial records that enrollees have trouble locating and would be prohibited in most cases under the proposed rule.
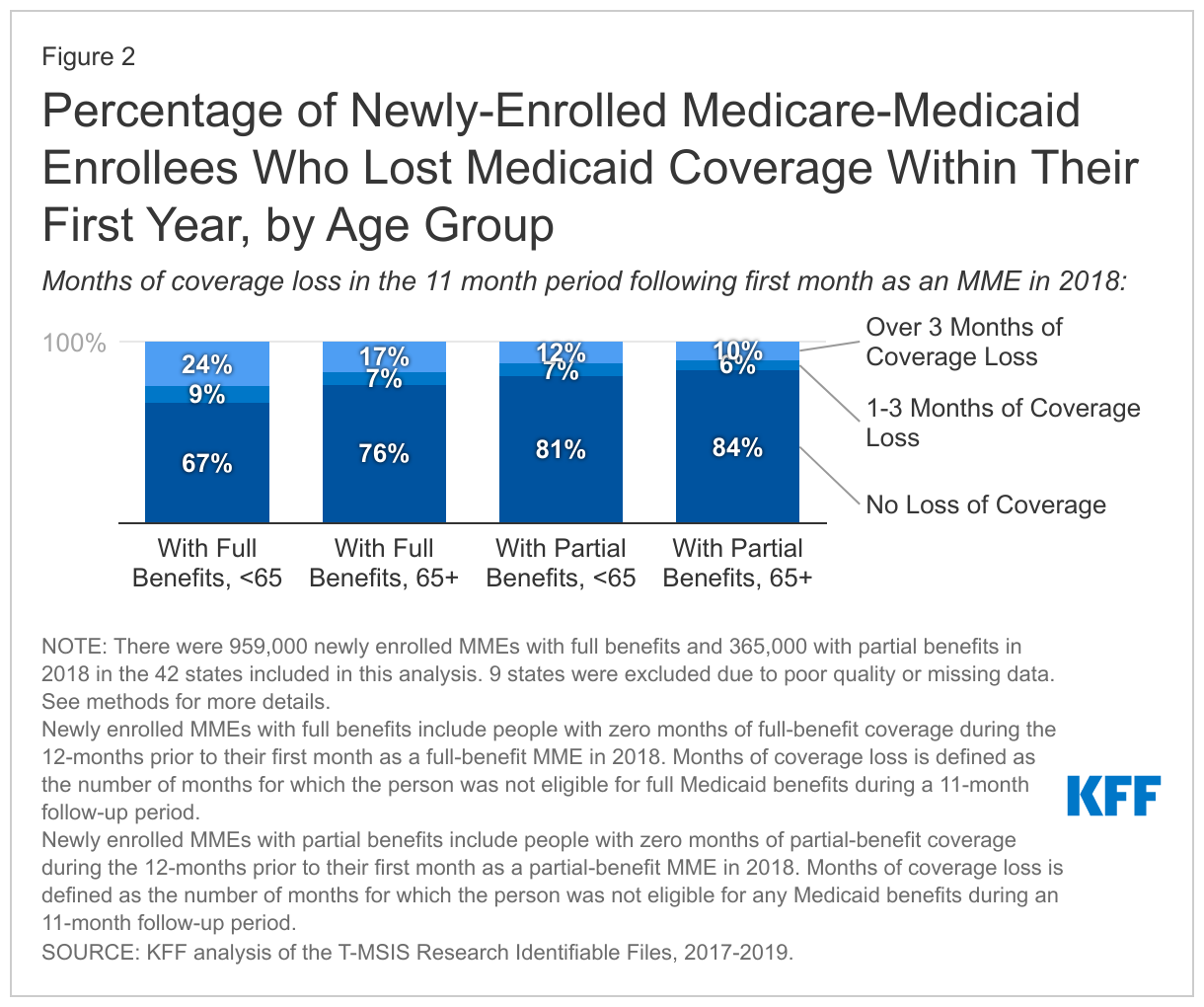
Coverage loss in the first year of enrollment was more common among newly-enrolled full-benefit MMEs under the age of 65 than among newly-enrolled full-benefit MME ages 65 and older: 33% lost coverage for one or more months in their first year of enrollment (Figure 2). In contrast, coverage loss was lower among full-benefit MMEs 65 and older: 24% lost coverage for one or more months. Coverage loss was lower among all partial-benefit MMEs of all ages - 19% of those under 65 and 16% of those ages 65 and older lost coverage for at least one month.
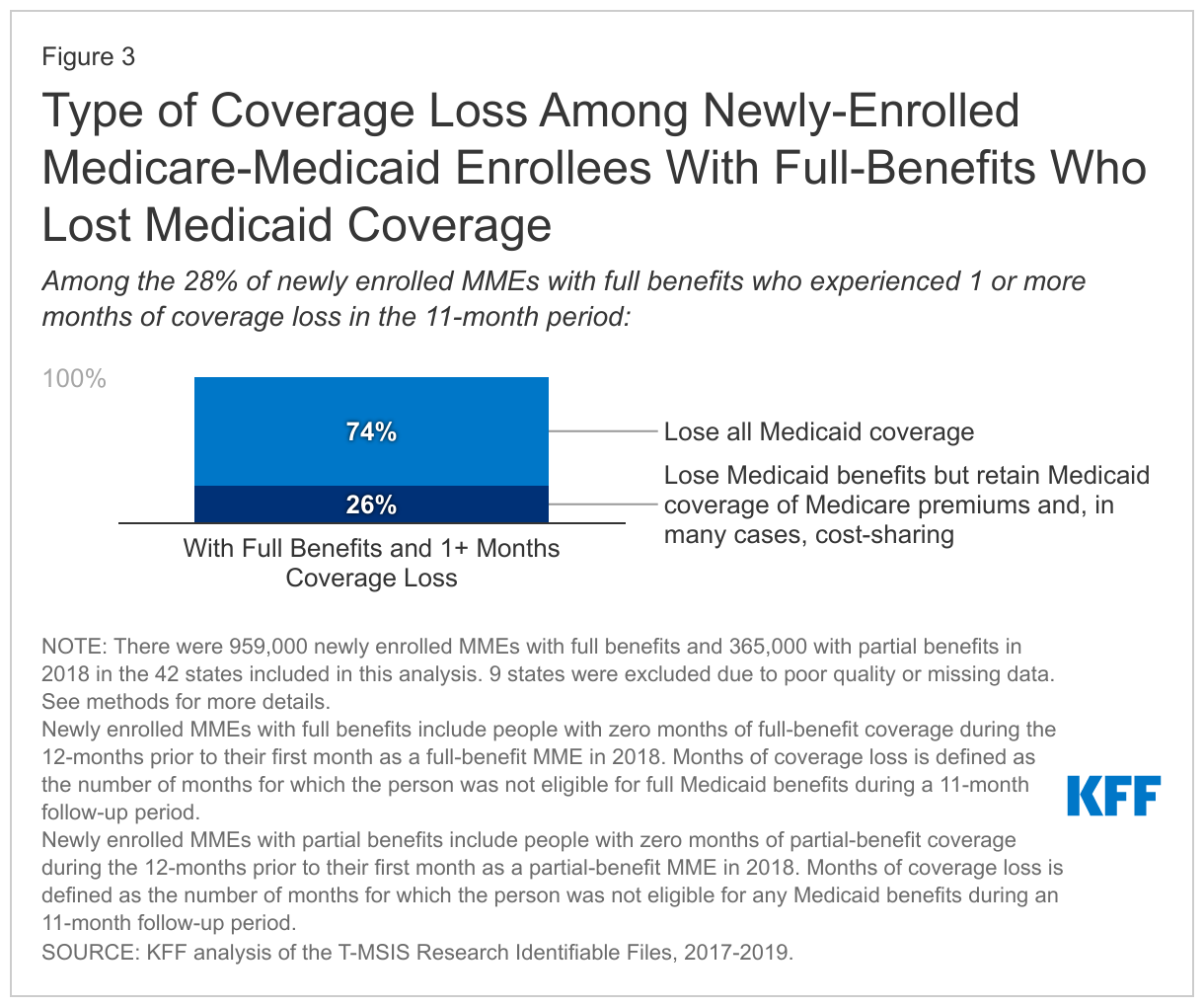
Among the 28% of newly enrolled full-benefit MMEs who lost Medicaid, 74% lost all Medicaid coverage for at least one month during their 11-month follow-up period, including coverage of Medicare premiums and cost-sharing, and other Medicaid benefits (Figure 3). Those Medicare beneficiaries would have had to start paying Medicare premiums and if applicable, cost-sharing. The remaining 26% lost eligibility for full Medicaid but retained Medicaid coverage of Medicare premiums and cost sharing (if applicable). All MMEs who lose coverage no longer have coverage of Medicaid benefits, which include long-term supports and services and nonemergency medical transportation among other services and may be particularly important for people who are elderly or with disabilities. In some states, Medicaid benefits include dental, vision, and hearing - services which are important to Medicare beneficiaries but not covered by Medicare.
Looking Ahead
Our analysis shows that just under one-third of MMEs lose Medicaid in their first year of enrollment, which is unexpected given most MMEs are living on fixed incomes and unlikely to experience changes in eligibility. These findings highlight the challenges people face when trying to access Medicaid and how the new proposed rule could help people more easily navigate the application and eligibility renewal processes. They also build on the findings of older research that CMS cited as a basis for the proposed changes. This analysis does not explore how many people losing coverage re-enroll in Medicaid, whether rates of Medicaid coverage loss differ for MMEs who are not new to the program, and how the proposed rule would impact Medicare beneficiaries who are eligible for Medicaid but not enrolled. Understanding those issues will be helpful to better understand the potential effects of the proposed rule.
Methods
Data: We used monthly enrollment and eligibility information from the 2017-2019 T-MSIS Research Identifiable Demographic-Eligibility Files and linked records across years using the Chronic Condition Warehouse beneficiary ID.
Identifying Newly Enrolled Full-Benefit and Partial Benefit MMEs: We identified MMEs using the monthly dual eligibility code but used the monthly restricted benefits code to determine which MMEs were eligible for full benefits (codes 1,A,D,4,5,7) or were only eligible for partial benefits (2,3,C,6,E,F). The dual eligibility code indicates full and partial benefit status for some types of MMEs, but for other types (such as Qualified Individuals) it does not. Using the restricted benefits code allowed us to identify some enrollees who would be categorized as partial-benefit using the dual eligibility code but are likely to have had full Medicaid benefits. We defined newly enrolled full-benefit MMEs as people who were full-benefit MMEs for at least one month in 2018 and were not full MMEs for the 12-month period prior. We defined newly enrolled partial-benefit MMEs as people who were partial-benefit MMEs for at least one month during 2018 and were not MMEs for the 12-month period prior.
Enrollee and State Exclusion Criteria: We excluded states whose rates of coverage loss for newly enrolled MMEs with full benefits were greater than 25 percentage points different than CMS’ recent findings. We eliminated six states based on these criteria (DE, KY, ME, MI, NE, and RI). We also excluded one state that reported no MME enrollment in 2017-2018 (AR) and two states that reported only partial MME enrollment in 2017-2018 (MS, ID).
Defining Coverage Loss: We estimated enrollment outcomes for 11 months after the original enrollment month, for a total of 12 months follow-up. In each month, we assigned MME’s benefit status as “full,” “partial,” or “none” and then summed the number of months by benefit status. For partial-benefit MMEs, greater than zero months of no benefits indicated coverage loss. For full-benefit MMEs, greater than zero months of no benefits or partial benefits indicated coverage loss. We also split coverage loss among full-benefit MMEs into coverage loss with no Medicaid and coverage loss with partial benefits, using the number of months of partial and no coverage variable.
Sensitivity Analyses: We found broadly similar results when we used the dual eligibility code instead of the monthly restricted benefits code to determine Medicaid eligibility and when we excluded MMEs who were eligible for Medicaid on a medically-needy basis (eligibility is determined monthly for those enrollees).
This work was supported in part by Arnold Ventures. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.