5 Things to Know: A Look at the Proposed Medicaid Eligibility & Enrollment Rule
On August 31, the Centers for Medicare and Medicaid released a proposed rule designed to make it easier for eligible people to obtain and maintain coverage in Medicaid and the Children’s Health Insurance Program (CHIP). Together, Medicaid and CHIP provide coverage to 89 million low-income people. The Affordable Care Act (ACA) made significant changes to help simplify, streamline, and coordinate eligibility and enrollment across health programs, especially for children and adults, but complexities remain, and some eligible people are not enrolled or churn on and off the program. While there are broad eligibility and enrollment rules, states administer the Medicaid program and there is considerable variation in eligibility, enrollment, and renewal policies. The proposed rule would create more uniform processes across states and are in line with the Biden Administration’s focus on strengthening coverage and access. While Medicaid eligibility is complex and the proposed rule contains many provisions, this policy watch highlights some of the most notable changes.
1. The proposed rule enhances timeliness requirements for state eligibility determinations and creates new requirements for states when they receive returned mail.
Existing rules specify that states are required to determine eligibility for Medicaid within 90 days for those applying on the basis of disability and 45 days for other applicants, but timeframes are not provided for when applicants need to provide additional information at renewal and for changes in circumstances. The proposed rule creates uniform requirements to help ensure applicants have sufficient time to submit required documentation to states at application, renewal and when changes in circumstances are reported. The proposed rule also specifies that states must check available data sources, conduct outreach using different modalities, and try to obtain forwarding address information before moving to terminate enrollees from coverage due to returned mail.
Data show that 1 in 10 Medicaid enrollees may disenroll and then re-enroll in Medicaid within one year (churn). Data also suggest that states implementing periodic eligibility checks between renewals may have contributed to Medicaid enrollment declines prior to the pandemic. Eligible individuals are at risk for losing coverage if they do not receive or understand forms requesting information to verify eligibility or do not respond to states’ requests within required timeframes. While many states have policies in place to conduct follow-up on returned mail, some states may disenroll individuals if mail is returned.
2. The proposed rule simplifies enrollment and renewal policies for people who are age 65 or older or have disabilities, many of whom are also enrolled in Medicare.
The ACA simplified eligibility processes for children and adults under age 65 who are not eligible on account of a disability. Eligibility for those populations depends on applicants’ Modified Adjusted Gross Income (MAGI) on their tax returns. The ACA established renewal requirements, such as using pre-populated renewal forms and conducting renewals on an annual basis. (A required renewal process on an annual basis is not the same as 12-month continuous eligibility, where enrollment is guaranteed for a year even if there are changes in income that have to be reported.) The proposed rule would apply similar simplified processes for people who are eligible because of a disability or being age 65 or older (referred to as “non-MAGI” populations because eligibility is not determined using MAGI). A recent survey shows that all but one state (West Virginia) conduct annual renewals for non-MAGI populations, but 15 do not use pre-populated renewal forms.
The proposed rule would also make significant changes to the eligibility determination process for two specific groups of beneficiaries: those who are considered “medically needy” and those who are eligible for the Medicare Savings Programs (MSP), which provide coverage of Medicare premiums and in some cases, cost sharing, through the Medicaid program.
- In the 34 states that offer a Medically Needy or spend-down pathway, people who are considered “medically needy” must show that they meet Medicaid income eligibility requirements after deducting health care expenses. Individuals living in institutions are currently allowed to project their future spending for the purposes of determining eligibility. The proposed rule would extend the same flexibility to some enrollees living in home and community settings.
- People who are eligible for MSP are also eligible for Medicare’s Low-Income Subsidy (LIS) for prescription drug coverage and the proposed rule would leverage LIS eligibility and enrollment data to streamline the MSP enrollment process. Integrating those systems could increase enrollment as data show that over 1.1 million people were enrolled in LIS and eligible for—but not enrolled in—MSP. Changes include ensuring that applications for LIS also are treated as applications for MSP, encouraging states to use the definitions of income and wealth that are used for determining LIS eligibility (which tend to be higher than the MSP income and wealth limits), and auto-enrolling LIS applicants who are receiving Supplemental Security Income.
3. The proposed rule also prohibits some policies that may be enrollment barriers for children in CHIP.
The proposed rule would eliminate waiting periods (or periods of uninsurance), coverage lockouts for failure to pay premiums, and annual or lifetime caps on benefits for children enrolled in separate CHIP (S-CHIP) programs. These policies are not permitted in Medicaid or other insurance affordability programs. Prior to the start of the pandemic, 13 states required waiting periods in S-CHIP of one month to 90 days, but two states have since eliminated their waiting periods. Additionally, prior to the pandemic, 14 states imposed a lockout period, usually 90 days, for failure to pay premiums. The proposed rule would also streamline processes to facilitate transitions between Medicaid and CHIP by requiring Medicaid and S-CHIP to accept eligibility determinations made by the other program, to develop procedures for each program to accept electronic transfers of information, and to provide combined notices for transitions between Medicaid and S-CHIP.
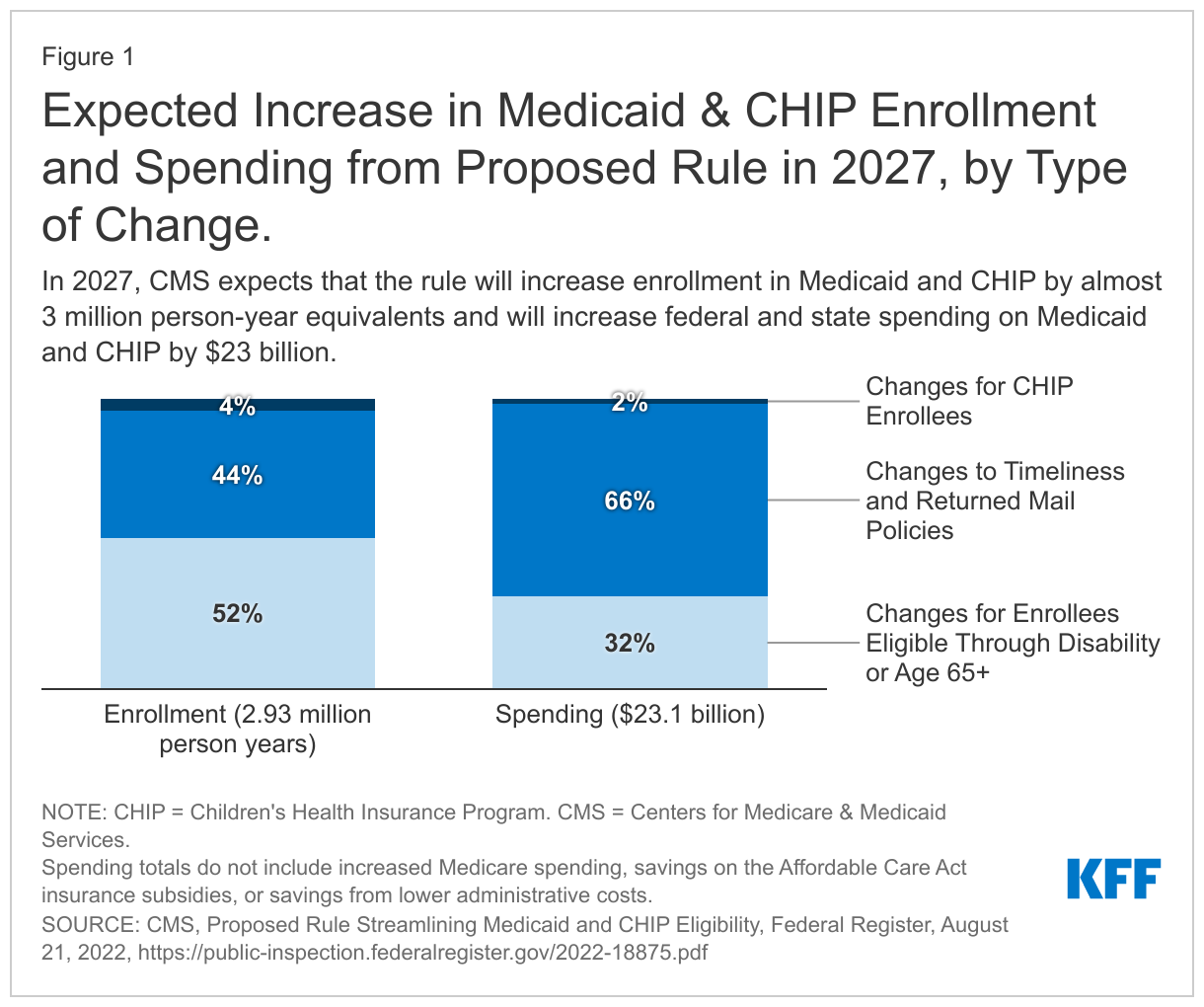
4. When fully implemented, the proposed rule is expected to increase coverage (and costs tied to new coverage) but reduce administrative costs and burden.
The Centers for Medicare & Medicaid Services (CMS) estimates that the rule would increase the number of person years of enrollment (a measure that calculates the number of new months of enrollment divided by 12) by nearly 3-million-person years after it is fully implemented in 2027 (Figure 1). The biggest source of new enrollment (1.5 million new person years) is due to changes made to eligibility processes for non-MAGI enrollees. Another 1.3 million new enrollment years come from changes relating to timeliness and returned mail policies that affect all Medicaid enrollees, and the final 0.1 million come from changes to the CHIP program.
The proposed rule estimates increased costs tied to Medicaid and CHIP enrollment gains of $23 billion in 2027 ($14.1 billion in federal funds and $9.1 in state funds), two-thirds of which results from changes affecting all Medicaid enrollees ($15.3 billion), Changes to non-MAGI rules account for $7.4 billion and the remaining $0.4 billion stems from changes to the CHIP program. In that year, CMS also estimates $2.6 billion in new Medicare spending, $4.0 billion in savings on subsidies provided through ACA marketplace coverage, and $1.2 billion in savings from lower administrative costs and improvements to program integrity. The estimated change in federal spending in 2027 would be $12.8 billion.
Estimates of increased coverage and costs are highly uncertain largely because it is hard to predict how states and people will respond to the new policies. It is also difficult to estimate how many people are eligible for, but not enrolled, in Medicaid and CHIP currently, particularly among people eligible for Medicaid on the basis of disability or being age 65 or older.
5. Looking ahead, CMS is seeking comments about how the proposed changes would intersect with the unwinding of the Public Health Emergency (PHE).
As CMS finalizes provisions in the rule sometime next year, implementation of the rule could coincide with the unwinding of the PHE. The Medicaid continuous enrollment requirement, which has been in place during the PHE, prevents states from disenrolling people from Medicaid; however, once the PHE ends, states will need to conduct redeterminations and renewals for all enrollees for the first time in over two years. CMS acknowledges that imposing these new requirements on states during the unwinding period following the end of the PHE could be challenging, even if the long-term effects are to make it easier for eligible individuals to enroll and retain coverage. In addition, recognizing states will need to make systems changes, and in some cases, legislative changes to comply with the requirements, CMS indicates it is considering an effective date 30 days following publication of the final rule while providing states with 12 months to come into full compliance. The agency seeks comment on the reasonableness of this timeframe.