Ongoing Impacts of the Pandemic on Medicaid Home & Community-Based Services (HCBS) Programs: Findings from a 50-State Survey
Issue Brief
Executive Summary
Widespread workforce shortages are the biggest challenges facing state Medicaid home and community-based (HCBS) programs and those shortages were greatly amplified by the COVID-19 pandemic, which reduced the number of potential workers and increased the demand for services. The American Rescue Plan Act (ARPA) and COVID-19 public health emergency (PHE) authorities gave states new—but temporary—flexibility and funding to address pandemic-related challenges, which all states used. Those initiatives enabled states to respond to the pandemic and invest in HCBS programs, helping millions of seniors and people with disabilities who rely on Medicaid HCBS to meet daily self-care and independent living needs in community-based settings.
This issue brief presents the latest findings on key state policy choices about Medicaid HCBS in 2022 based on the 20th KFF survey of state officials administering Medicaid HCBS programs in all 50 states and DC. The data were collected from April through September 2022. The survey was sent to each state official responsible for overseeing the administration of HCBS benefits (e.g., home health, personal care, and services for specific populations such as people with physical disabilities), but some states submitted responses for the state overall. All states responded to the 2022 survey, but response rates for certain questions varied. Key findings include:
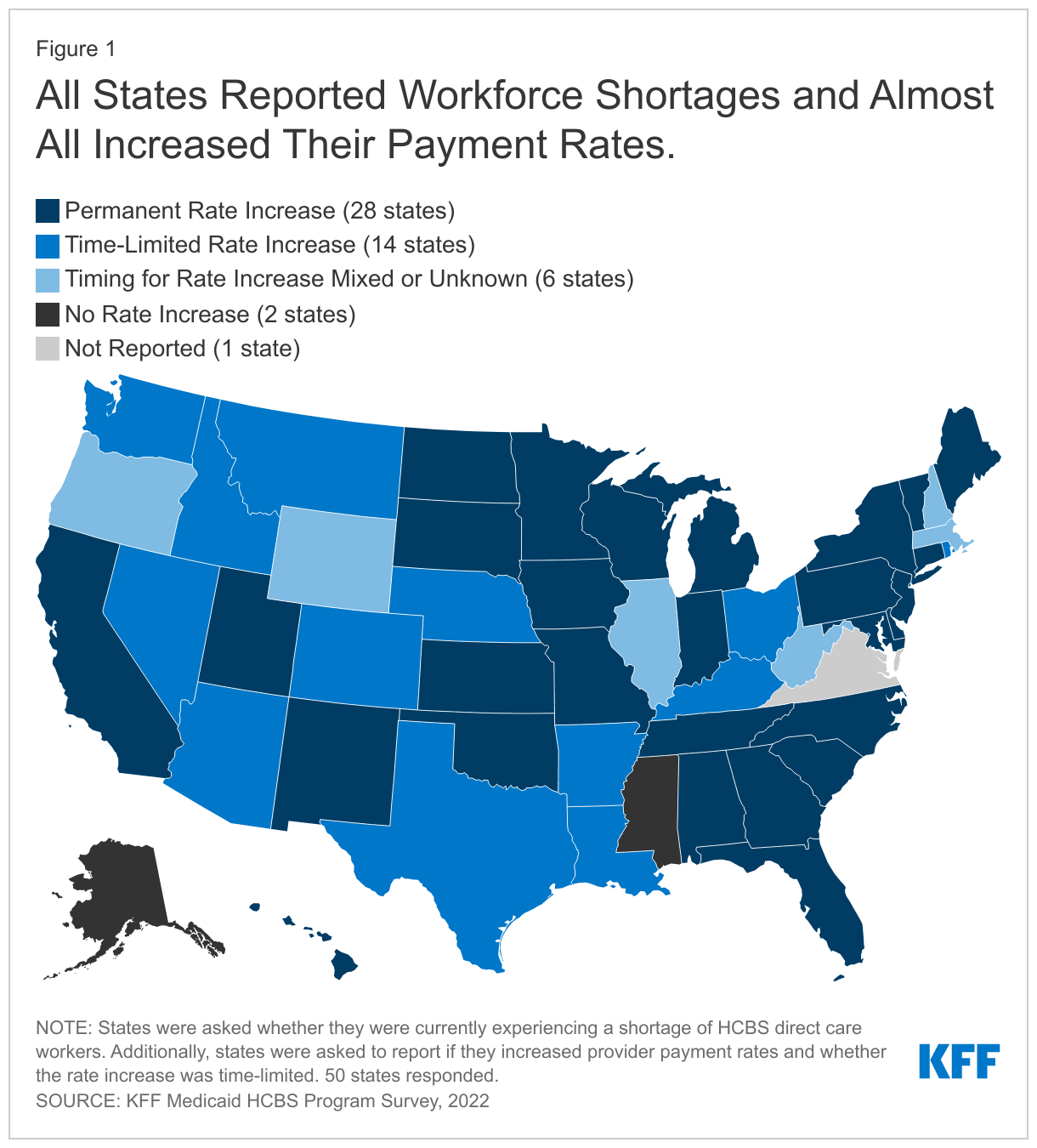
All responding states indicated they were experiencing shortages of direct care workers in 2022 (see Figure). States most frequently cited workforce shortages as the pandemic’s primary impact across all HCBS settings. As the pandemic persisted, HCBS workforce shortages contributed to provider closures. Most states (44) reported a permanent closure of at least one Medicaid HCBS provider during the pandemic, up from 30 states in 2021. This trend suggests that even as the broader economy returns to normal, HCBS providers continue to struggle.
Almost all states (48) responded to the workforce crisis by increasing HCBS provider payment rates. While some of these increases may have been supported through temporary ARPA funding or emergency PHE authorities, more than half of states plan to continue rate increases even after temporary funding and authorities expire. States also increased self-directed and family caregiving opportunities for HCBS beneficiaries throughout the pandemic. All states offer at least one HCBS program with the option for enrollees to self-direct their services. Forty-eight states allow legally responsible relatives (LRRs) to be paid caregivers, up from 36 states in 2020.
When asked about how they used the ARPA funding, over two-thirds of states (35) reported initiatives with high start-up costs that were generally time-limited to avoid higher ongoing costs after enhanced federal funding ended. Ten (of those 35) states reported pursuing both time-limited and ongoing HCBS initiatives using ARPA funds. Some of the most common initiatives included offering providers bonuses or incentive payments to stay on, developing or expanding worker training or certification programs, funding studies to assess provider rates or workforce development, expanding workforce registries, and upgrading IT systems.
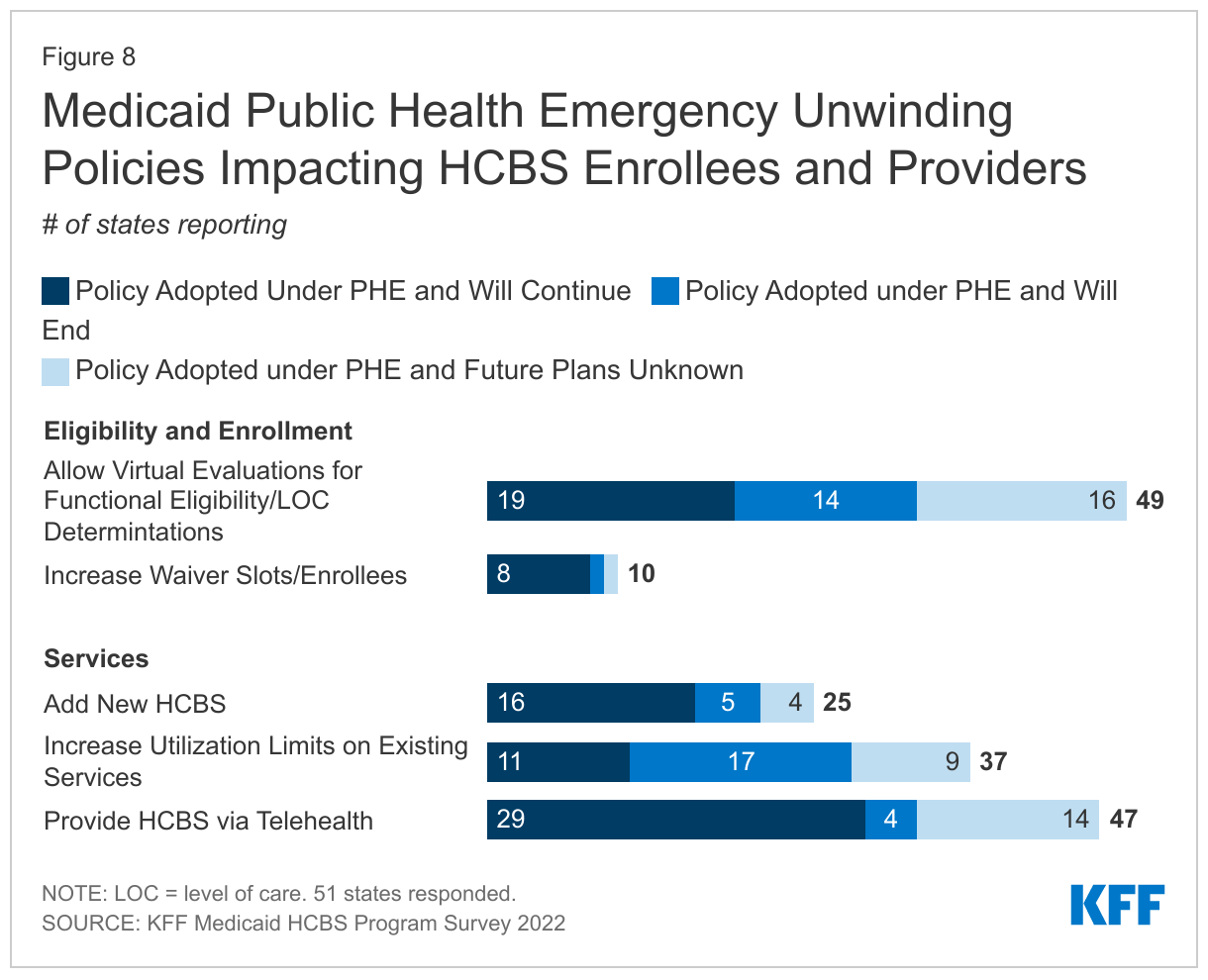
States adopted policies to streamline enrollment processes and expand access to Medicaid HCBS during the PHE, and states reported that some policies (e.g. telehealth) will continue after the PHE ends. All states (49 of 49 reporting) allowed virtual evaluations for eligibility determinations and almost all (47 of 49 reporting) provided telehealth service delivery. Many states also provided more services to HCBS users by increasing utilization limits or offering new waiver services. Telehealth service delivery will continue in most states but increases in utilization limits are more likely to expire at the end of the PHE. Fewer states opted to use the PHE authorities to expand waiver slots or eligibility.
The COVID-19 pandemic illuminated fundamental, long-term challenges for states in providing Medicaid HCBS, but also provided opportunities for change, particularly with new authorities and funding. While states have adopted a number of policies to bolster the HCBS workforce, it remains to be seen whether initiatives undertaken during the pandemic will yield more systemic changes longer-term. Policymakers of both parties have called for additional changes to HCBS including eliminating waiting lists for services (nearly 656,000 people were on a waiting list in 2021), increasing opportunities for family members to be paid caregivers, increasing wages for all HCBS providers, and enabling more people to live in their homes as they age. Although there is consensus on those broad policy goals, there is little consensus on how to pay for significant federal investments needed to achieve these goals, suggesting it may be some time before major reforms are enacted.
Introduction
The COVID-19 pandemic exacerbated existing challenges for state Medicaid home and community-based (HCBS) programs and the people they serve, most notably a heightened shortage of direct care workers coupled with increased demand for services. Together, the American Rescue Plan Act (ARPA) and the COVID-19 public health emergency (PHE) authorities gave states new but temporary federal funding and policy flexibility to address pandemic-related challenges. All states used these initiatives to make investments in their HCBS programs, helping millions of seniors and people with disabilities who rely on Medicaid HCBS to meet daily self-care and independent living needs in community-based settings. As states continue pandemic recovery efforts, consumer demand for HCBS remains high and longstanding challenges facing Medicaid HCBS including the aging population and provider workforce shortages will likely continue for the foreseeable future.
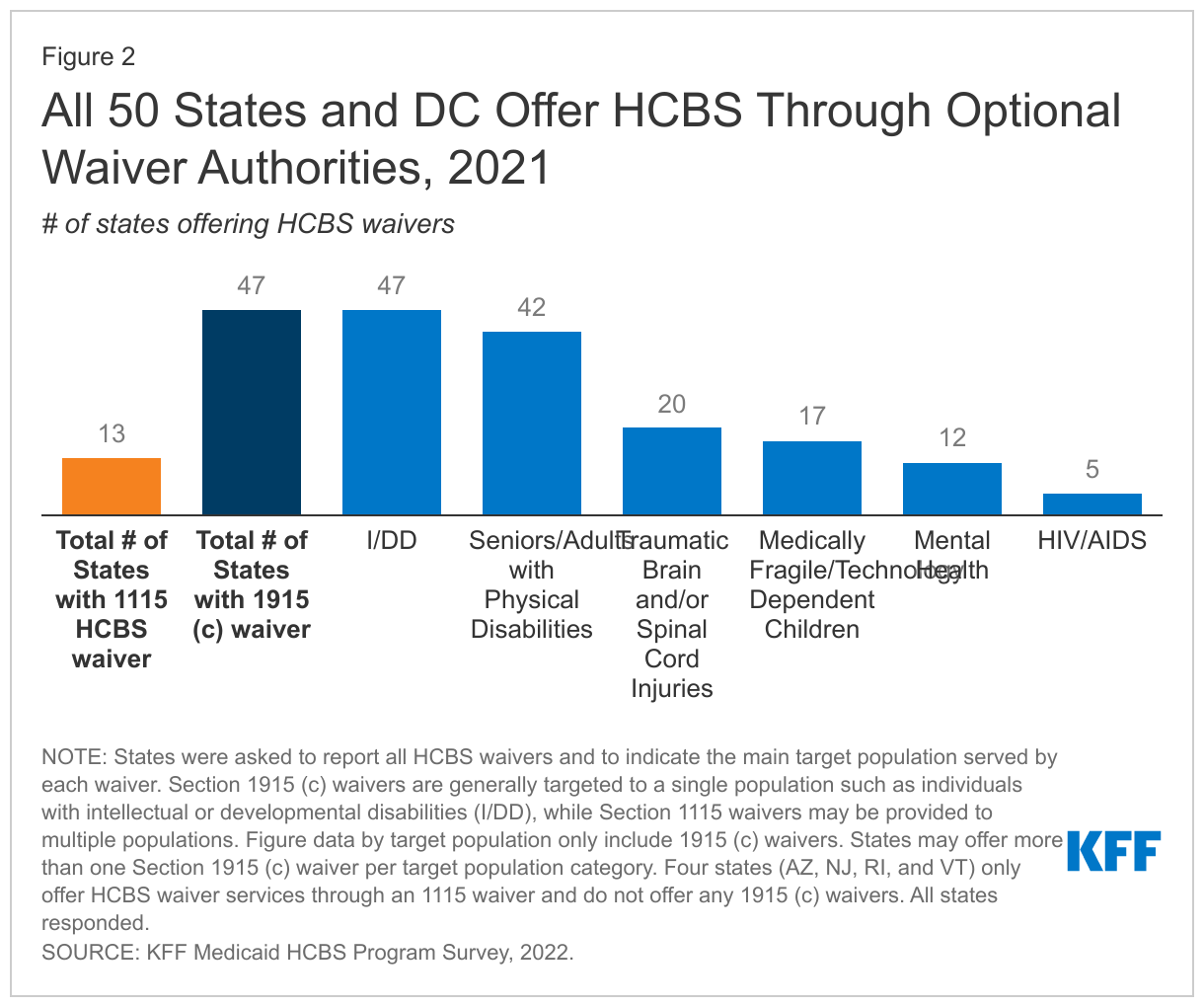
Medicaid paid for about two-thirds of all HCBS in 2020, and waivers are the primary authority that states use to offer HCBS benefit packages with all of the 50 states and D.C. providing at least some HCBS through either a 1915(c) or an 1115 waiver. Medicaid HCBS encompass a wide range of medical and nonmedical services that assist Medicaid beneficiaries with physical, mental, and other chronic conditions or disabilities. States are required to cover Medicaid long-term services and supports (LTSS) provided in nursing homes, while all HCBS other than home health care services are optional. HCBS may be provided through state plans but are more commonly provided through waivers. Unlike Medicaid state plan authorities, which require states to cover everyone who meets certain eligibility criteria, waivers allow states to provide services to specific populations, limit the number of people served, and expand financial eligibility. The Centers for Medicare & Medicaid Services (CMS) estimates that nearly 8 million Medicaid enrollees had at least one claim for a service that could potentially be HCBS during 2019.
This issue brief presents the latest findings from a survey of states on key state policy choices about Medicaid HCBS in 2022 and the HCBS waiver landscape as of 2021. We also asked states about policies they adopted in response to the COVID-19 pandemic through the ARPA and PHE authorities, and whether they planned to continue policies adopted through PHE authorities. The Appendix Tables contain detailed state-level data.
What is the Current Landscape of Medicaid HCBS?
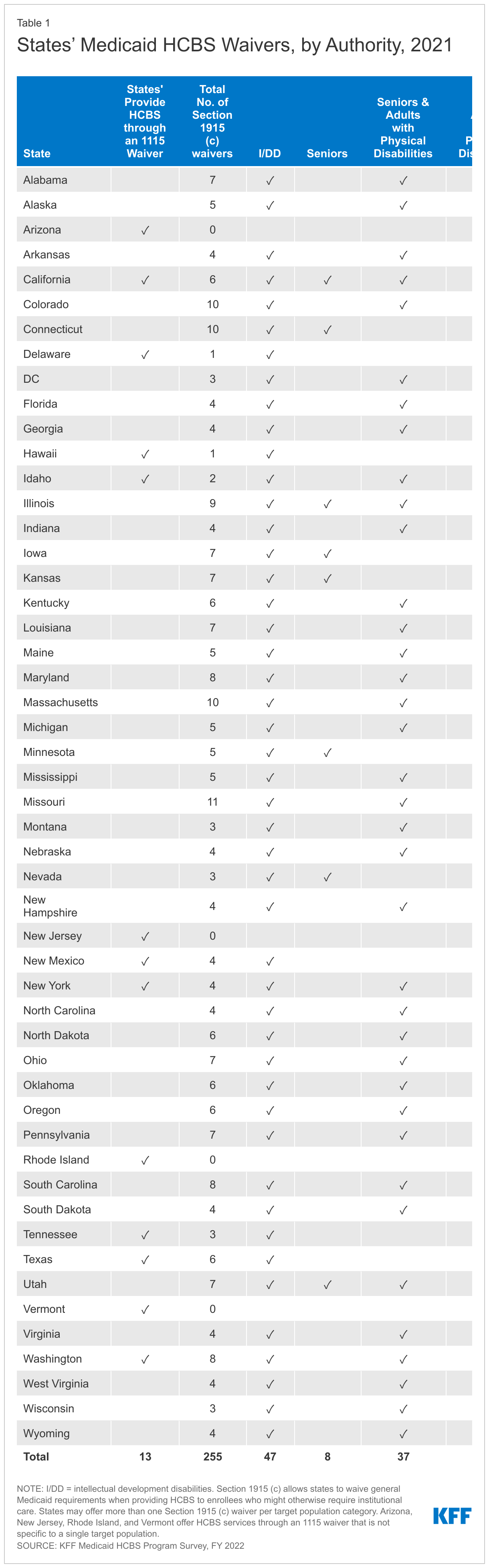
When asked about the waivers they had in 2021, states reported offering 255 waivers under 1915(c) authority, which is the largest source of HCBS spending. (The four states that do not provide HCBS through 1915(c) authority all offer HCBS services through an 1115 waiver.) Section 1915(c) waivers are generally targeted to a single population, such as people with physical disabilities or people with intellectual and development disabilities (I/DD). The number of Section 1915(c) waivers averages five per state. Almost all states serve people with I/DD, seniors, and nonelderly adults with physical disabilities through 1915(c) waivers (Figure 2, Appendix Table 1). Fewer states use HCBS waivers to serve people with traumatic brain and/or spinal cord injuries (TBI/SCI), children who are medically fragile or technology dependent, people with mental health disparities, and people with HIV/AIDS. States may use other authorities such as 1115 waivers to provide HCBS, but when HCBS are provided through 1115 waivers, they may be provided to multiple—or broader—target populations and may be part of larger Medicaid reforms. Thirteen states reported offering HCBS waivers authorized under Section 1115 in 2021.
Four states reported offering new waivers in 2021, the most recent year in which states were asked to report all of their HCBS waivers. Alabama and the District of Columbia reported new 1915(c) waivers serving populations with I/DD, while Missouri had a new 1915(c) waiver serving seniors and adults with physical disabilities. Idaho reported offering a new Section 1115 waiver serving individuals with mental illness. Additionally, Oregon submitted a new 1115 waiver request to provide in-home supports to individuals with higher income and assets and for those who do not meet nursing facility level of care criteria. Tennessee has pending waiver amendments to integrate the 1915 (c) waivers into its 1115 waiver.
New funding from the ARPA and authorities granted to states under the PHE helped states respond to the challenges posed by the pandemic. Under the PHE authority, the federal government granted states temporary authorities that were intended to maintain enrollment and service levels during extraordinary times. The current PHE is currently in effect until January 11, 2023, and the Biden administration has said it will give states a 60-day notice before ending the PHE. Since that notice was not issued in November 2022, it is expected the PHE will be extended again. At the end of the PHE, most waivers and broad flexibilities will expire, requiring states to either end the temporary practices or transition the practices to a permanent authority with CMS approval.
Enacted in March 2021, the ARPA increased the federal medical assistance percentage (FMAP) by 10 percentage points for states’ HCBS expenditures that were paid between April 1, 2021, and March 31, 2022. Receipt of the funds required states to demonstrate that the additional federal funding would not supplant any state funds for HCBS. To implement that requirement, participating states are required to submit spending plans that describe the amount of funds they received from the higher FMAP and on how they are spending those funds on HCBS. Activities funded with the additional ARPA money must be intended to enhance, expand, or strengthen HCBS such as providing retention bonuses or student loan forgiveness for HCBS workers, expanding coverage of HCBS, or funding infrastructure investments related to the delivery of HCBS. States have until March 31, 2025 to spend the extra federal funds that were provided for HCBS expenditures that were paid between April 1, 2021 and March 31, 2022. Funds spent after March 31, 2022, are reimbursed at the states’ normal FMAPs instead of at the higher FMAP.
How is the Pandemic Affecting the Workforce?
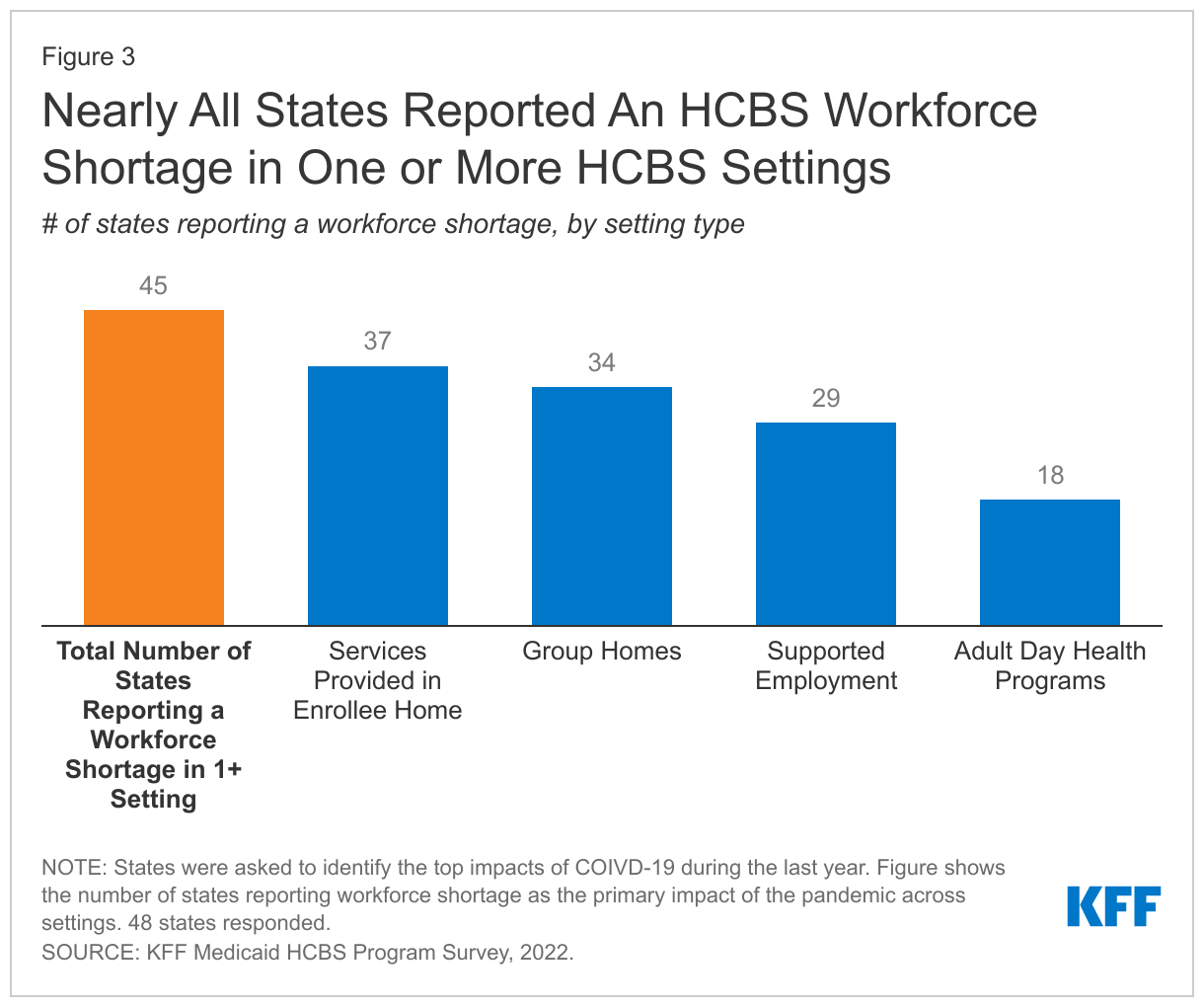
Workforce shortages have been exacerbated by the pandemic: All states that responded to this question indicated they were experiencing shortages of direct care workers in 2022. When asked about shortages for specific types of workers, states reported shortages of all types of HCBS providers including home health aides, personal care attendants, direct support professionals, and community-based mental health providers. States most frequently cited workforce shortages as the pandemic’s primary impact across all HCBS settings including in-home services, group homes, adult day health programs, and supported employment programs (Figure 3).
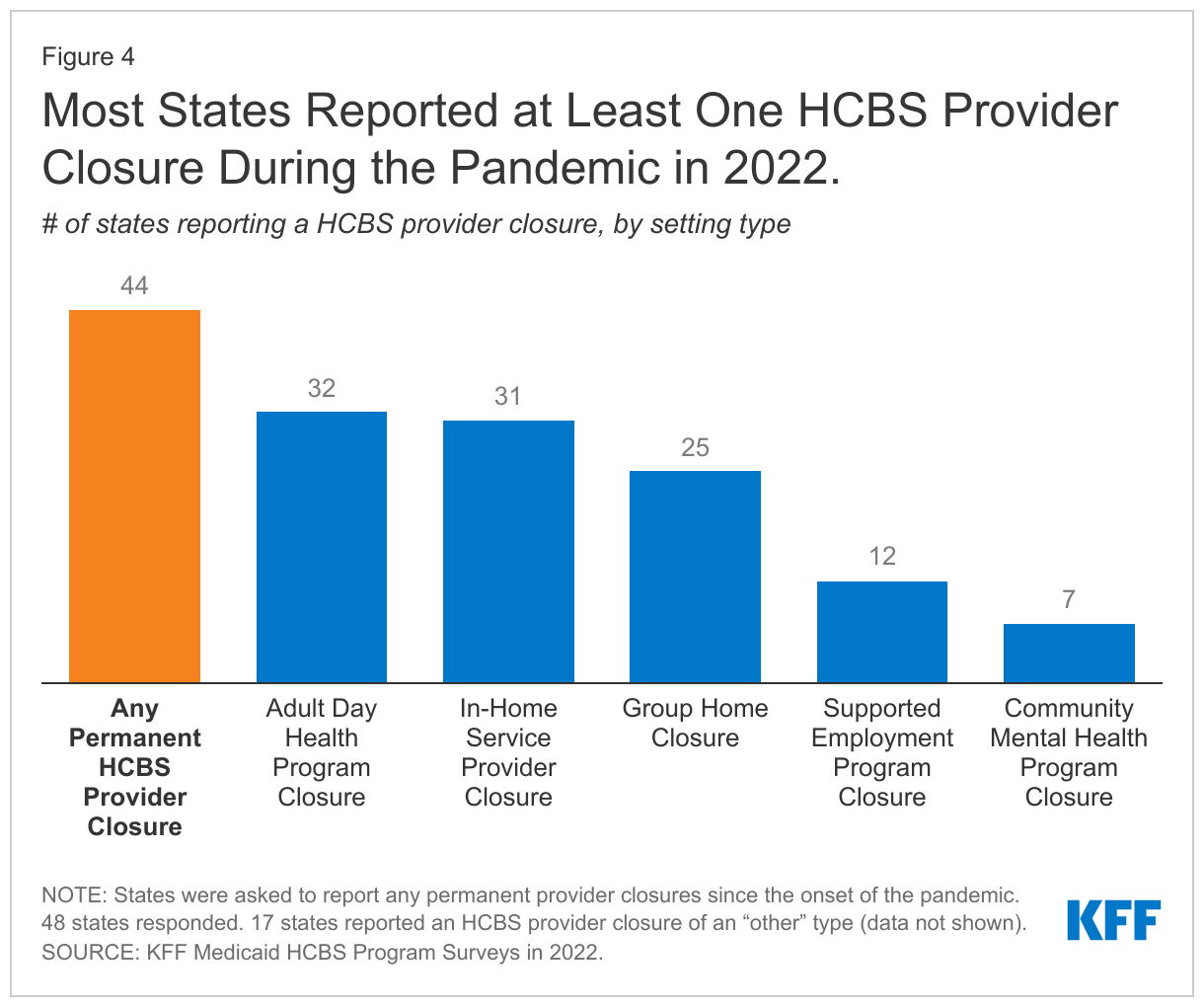
As the pandemic persisted, HCBS workforce shortages contributed to provider closures: 44 states reported a permanent closure of at least one Medicaid HCBS provider during the pandemic (Figure 4). States reported more closures in 2022 than the year prior (30), suggesting that even as the broader economy returns to normal, HCBS providers continue to struggle. Although states did not provide explanations for why so many HCBS providers closed in 2022, it could be attributed to ongoing workforce shortages potentially coupled with provider financial difficulties stemming from pandemic-related service disruptions. Other research shows that the pandemic’s effect on employment was particularly profound for LTSS workers. Recent analysis on the Peterson-KFF Health System Tracker shows that the number of workers dropped by 14% in nursing care facilities and by 9% in community elder care facilities between February 2020 and June 2022. Many states (31) reported permanent closures affecting services provided in enrollees’ homes, adult day programs (32), and group homes (25). Fewer states reported permanent closures of other types of HBCS providers such as community mental health providers and supported employment providers, who provide job search, placement, and coaching support.
How did States Respond to the Workforce Crisis?
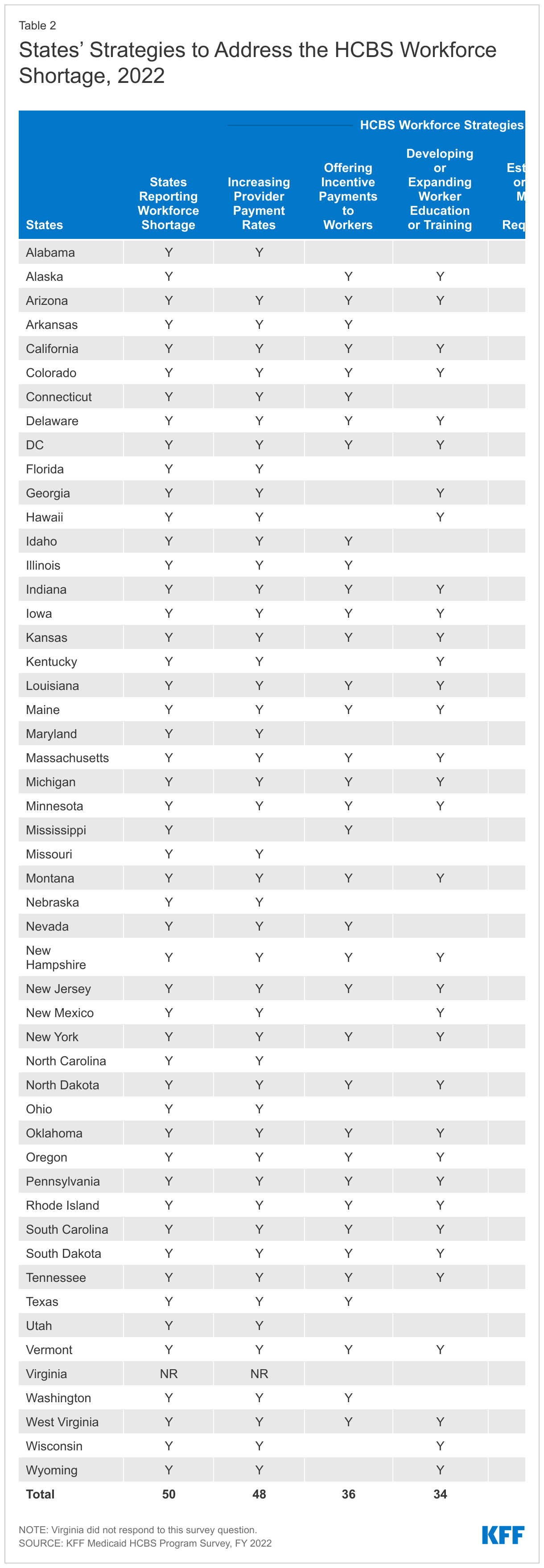
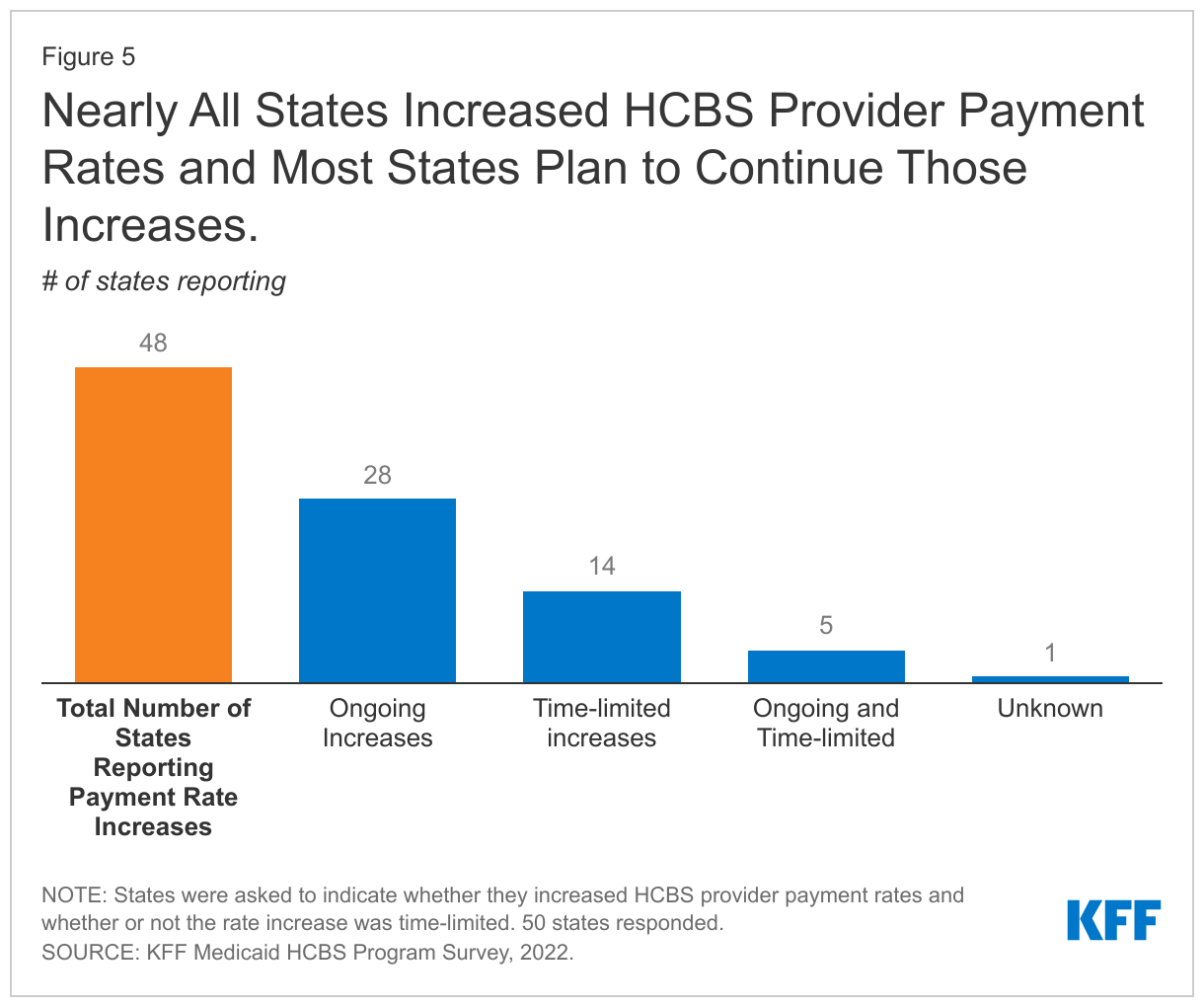
When asked about their overall responses to workforce shortages, most states reported that they increased HCBS provider payment rates and most plan to continue those rate increases even after pandemic authorities and funding end (Figure 5). Among the 48 states that increased rates, over half (28) plan ongoing increases to provider payment rates. For the remaining states,14 implemented time-limited increases, 5 implemented a combination of both time-limited and ongoing increases, and 1 state reported that they didn’t know whether the rate increases would be permanent.
Half (24) of the states that increased provider payment rates required the rate increase to be passed through to worker wages. These requirements typically are being implemented through provider attestation (18 states) or another method such as a statutorily specified split between the workers and the agency or through post-payment audits and cost reporting (10 states). Few states added such a requirement to Medicaid provider agreements (4) or health plan contracts (2). The other strategies states reported using to address the workforce shortage included offering incentive payments to recruit workers (36), developing or expanding worker education programs (34 states), and establishing or raising a minimum wage requirement for workers (20 states) (Appendix Table 2).
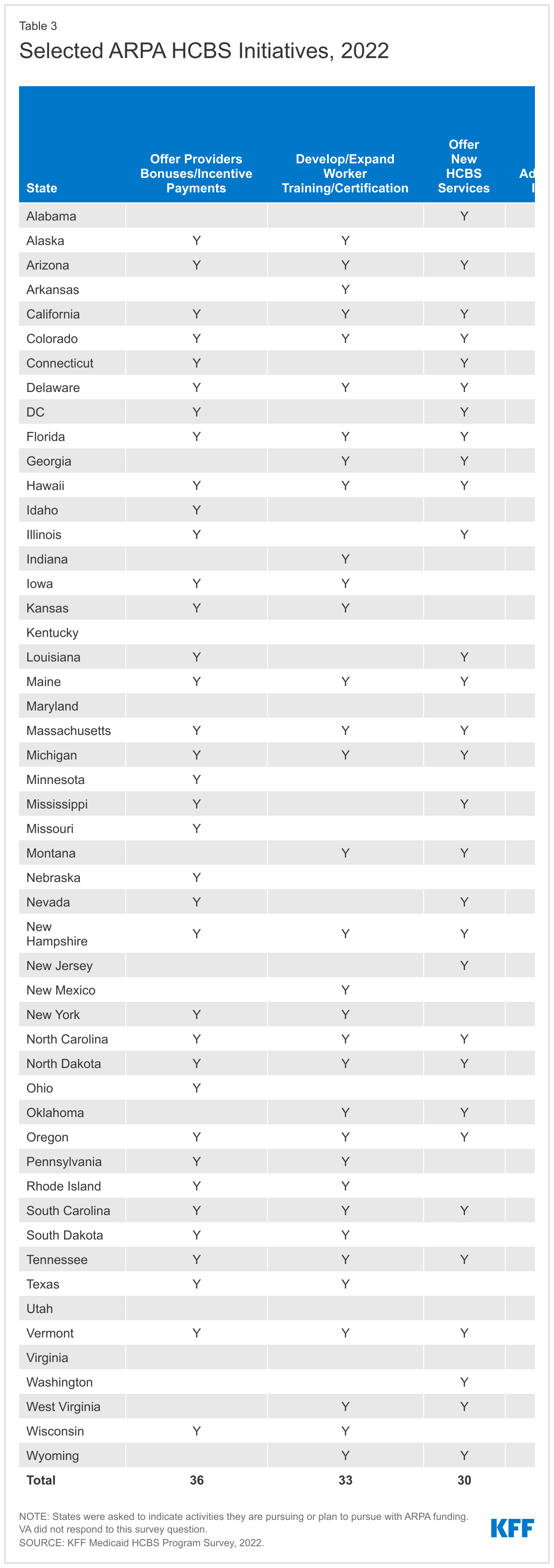
All states participated in the ARPA HCBS program and when asked how they used the funding, most states reported making upfront investments and confronting immediate recruitment and retention challenges in the workforce (Appendix Table 3). Most states (35) chose initiatives with high start-up costs that were generally time limited so that they would not face higher ongoing costs in the future after the period of enhanced federal funding ended. For example, states used ARPA funding to provide bonuses or incentive payments (36), develop or expand worker training or certification programs (33), expand family caregiver supports (23), fund studies to assess provider rates or workforce development (21), and develop or expand workforce registries (15). It is unknown to what extent those initiatives will continue after states have exhausted the additional federal funding they received from the ARPA.
“Self-direction has increased in all programs in which it is offered. When traditional site-based programs were closed/short-staffed due to the pandemic, this provided additional opportunities to learn about self-direction, and individuals and families were able to hire staff to continue to receive support.” – State official
States increased self-directed and family caregiving opportunities for HCBS beneficiaries throughout the pandemic as one way of addressing workforce challenges (Figure 6, Appendix Table 4). All states offer self-directed opportunities for Medicaid HCBS beneficiaries. Self-direction typically allows individuals to select and dismiss their direct care workers, determine worker schedules, set worker payments rates, and/or allocate their services budgets. Over half of states (30) reported an increase in the number of enrollees self-directing Medicaid HCBS since the onset of the pandemic, while just two states (OR, TX) reported a decline.
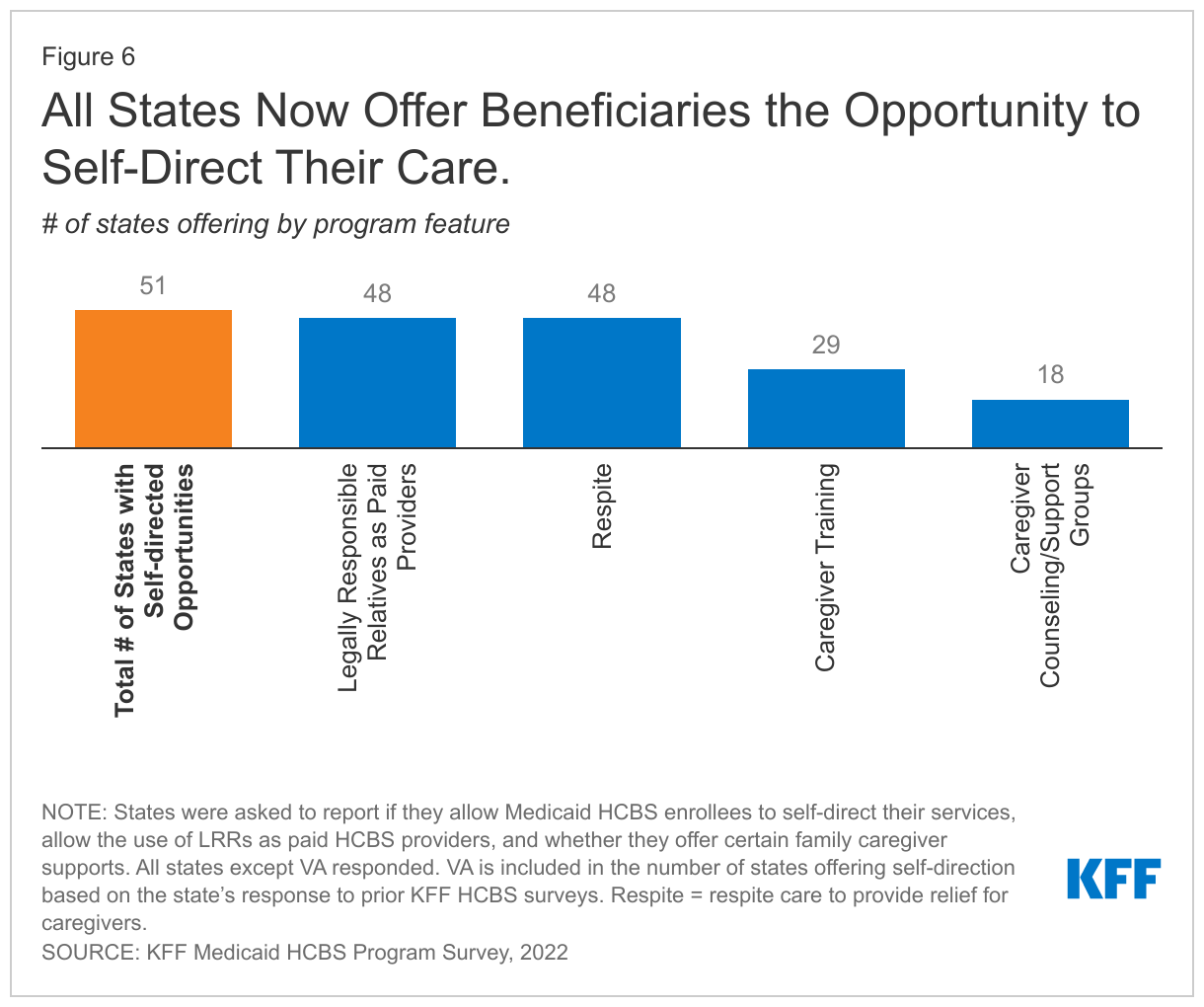
One of the biggest changes during the pandemic is that 48 states now allow legally responsible relatives (LRRs) to be paid caregivers (up from 36 in 2020). Legally responsible relatives may include a spouse, parent, or adult child. Covering more provider types, including LRRs, can help to increase access to services that meet daily need such as personal care and habilitation, especially when other providers are not available. About half of states (27 of 45 reporting) report an increase in the number of paid LRRs since the onset of the COVID-19 pandemic, while the remaining states saw no change (6) or reported unknown (12). Over three-quarters of states (39) reported that payment to LLRs was granted through the PHE/Medicaid emergency authority and half of those states (20) plan to make this flexibility permanent for at least one HCBS program/waiver.
A second major change is that all states now offer some types of supports for family caregivers, who may be either paid or unpaid. Most states (36) offer more than one type of support for family caregivers. Frequently reported family supports include respite care (48), caregiver training (29), and caregiver counseling/support groups (18). There were 14 states that reported other types of supports such as peer support services, family caregiver stipends, child day support, and supported family living.
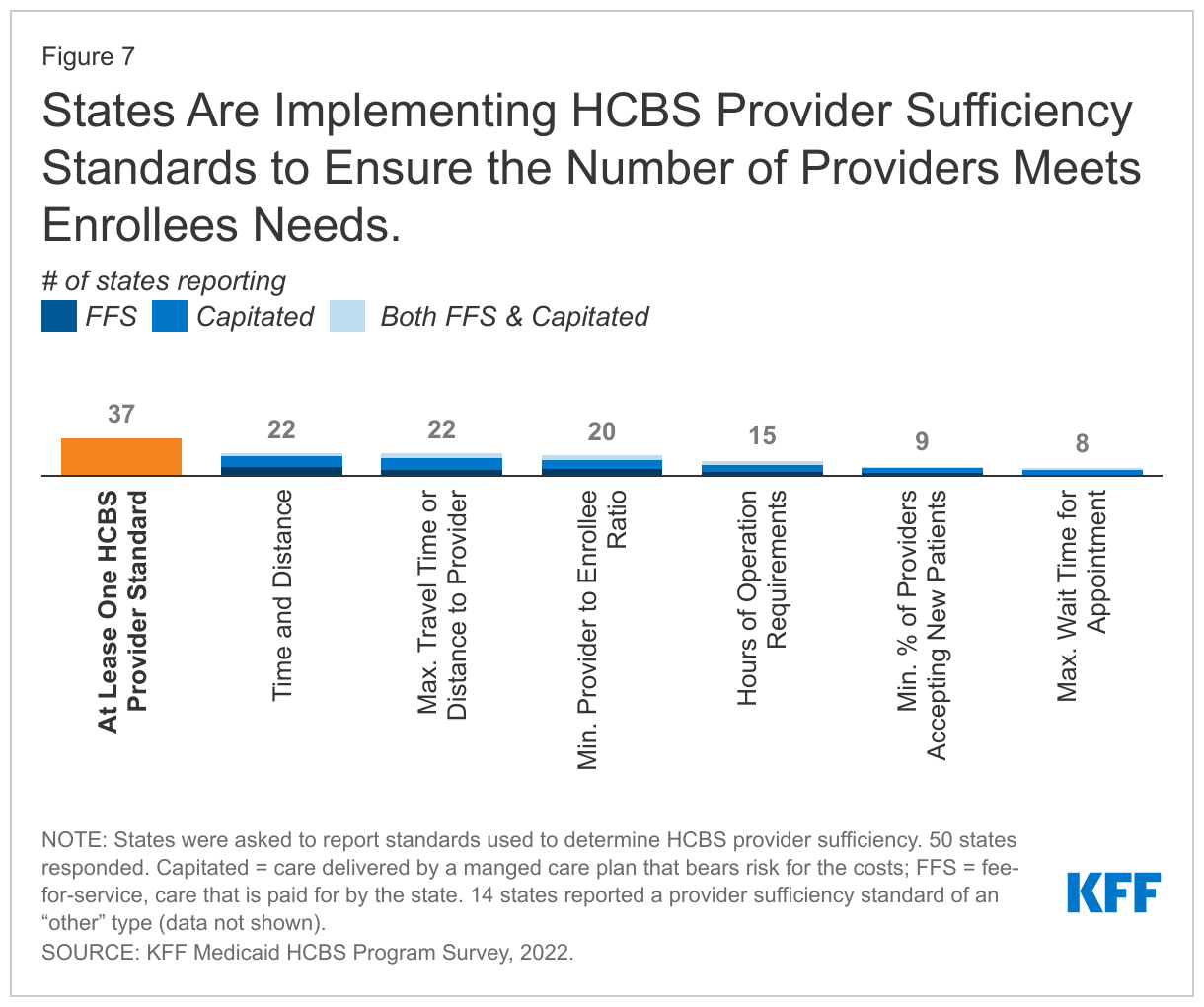
Most (37) states report using HCBS provider sufficiency standards to help measure the extent to which there are sufficient providers to meet enrollee needs (Figure 7). For services that the states pay for directly, there are no consequences for failing to meet the standards, but they provide a useful tool for assessing provider availability and the sufficiency of the provider network. Alternatively, states are required to use provider sufficiency standards in their contracts with private care plans when HCBS are delivered by those plans. CMS finalized changes to those managed care regulations in 2020. The 2020 rule removes the requirement that states use time and distance standards to ensure health plans’ provider network adequacy and instead allows states to choose any quantitative standard. Alternate standards could include minimum provider to enrollee ratios, maximum travel time or distance to providers, minimum percentage of contracting providers accepting new patients, maximum wait times for an appointment, or hours of operation requirements.
About half of states (27) required at least one network adequacy standard for HCBS providers in a fee-for-service (FFS) model, while 23 states required at least one standard in a capitated (risk-based) model. The most common standards include time and distance when an enrollee must travel to a provider (22 states), maximum travel time or distance to a provider (22 states), and minimum provider to enrollee ratio (20 states). Fewer states reported hours of operation requirements, minimum percentage of providers accepting new patients and maximum wait time for an appointment.
What Other HCBS Strategies Did States Use to Respond to the Pandemic?
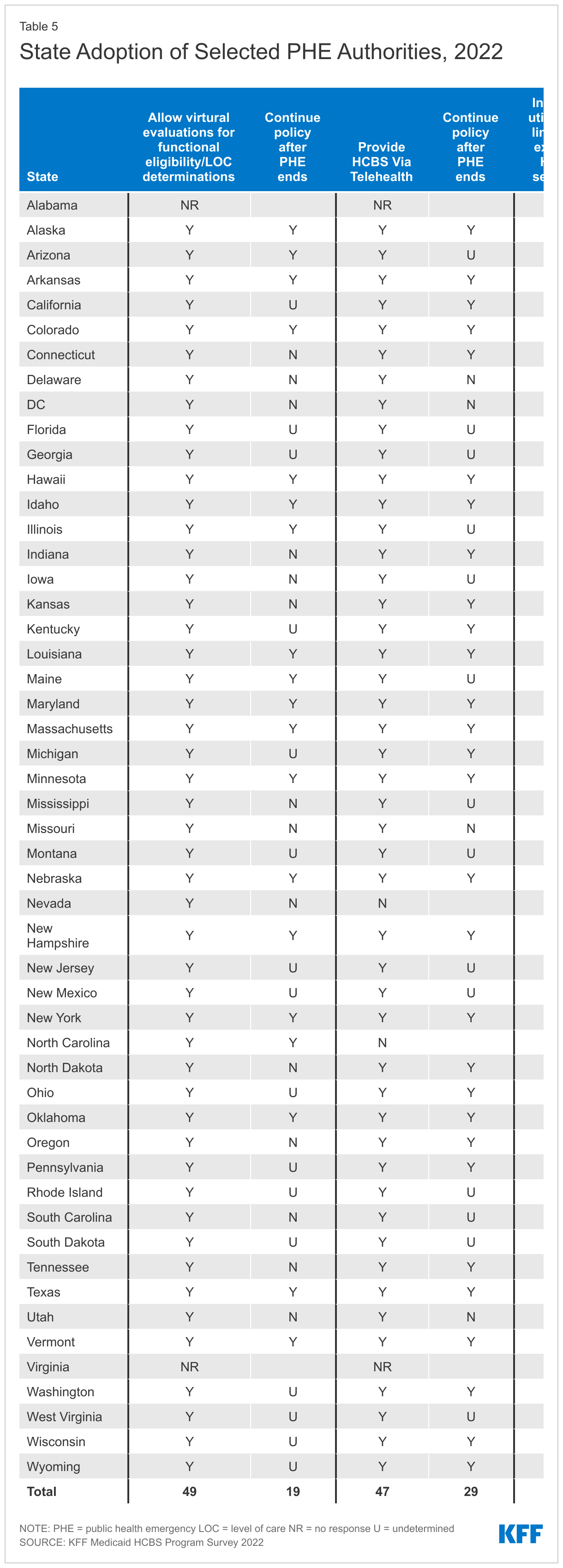
States have adopted numerous policies to streamline and expand access to Medicaid HCBS during the PHE, and some policies are expected to continue after the PHE ends (Figure 8, Appendix Table 5). One of the biggest changes to Medicaid HCBS policy during the pandemic was the use of virtual evaluations for determining enrollees’ eligibility for HCBS and their appropriate level of care. All states (49 of 49 reporting) adopted virtual evaluations. Of those, 10 states plan to continue this policy once the PHE ends and 9 noted the policy would only continue under certain circumstances or as needed. The remaining states were either uncertain about future plans (16) or plan to discontinue the policy (14) once the PHE ends.
Fewer states opted to use the PHE authorities to expand waiver slots or eligibility. Ten states reported increasing the number of waiver slots during the PHE, and eight states will continue after the PHE ends. Five states expanded eligibility either by expanding waiver financial eligibility limits (IL, NC, NV, OR) or functional eligibility criteria (MD).
“Limits for some HCBS were extended to better support individuals through the pandemic. Pre-pandemic limitations will be in place 6 months after the PHE ends.” – State official
Twenty-five states added new services to at least one HCBS waiver during the PHE, with home delivered meals the most frequently reported new service (9 states). Sixteen states will continue to offer these new waiver services after the PHE ends, five states were planning to end the services when the PHE ends, and the final four states were still undecided at the time of the survey. Most states provided more services to HCBS users by increasing utilization limits, but many of those changes will end when the PHE does. Thirty-seven states increased utilization limits on existing HCBS services, with less than one third (eleven) of states opting to continue the policy after the PHE ends. States reported increasing limits for home delivered meals, respite, day supports, personal care services, dental, and home modifications.Almost all states provided telehealth services to address challenges in delivering in-person HCBS during the pandemic. All but two (47 of 49 responding) states reported providing HCBS via telehealth in at least one waiver, and almost two-thirds (29) of states plan to allow at least some telehealth service delivery moving forward. States reported relying on telehealth for services such as: wellness checks, case management, supported employment, life skills training, behavioral and mental health counseling, companion, and adult day and habilitation services.
Some states used ARPA funds to make changes to their HCBS programs beyond confronting workforce challenges. Although most states reported workforce-related uses of the ARPA funding, over half of states reported offering new HCBS services and adopting or upgrading information technology systems (e.g., incident reporting, case management, and electronic visit verification) with the ARPA money (30 states each). Twelve states reported adopting or expanding HCBS quality measures (Appendix Table 3).
Looking Ahead
The COVID-19 pandemic illuminated fundamental, long-term challenges for states in providing Medicaid HCBS, but also provided opportunities for change, particularly with new authorities and funding. While states have adopted many new policies to bolster the HCBS workforce, it remains to be seen whether initiatives undertaken during the pandemic will yield more systemic changes longer-term.
In the recent months, CMS has also taken steps to improve the accessibility and quality of Medicaid HCBS. In July, the agency released the first-ever set of HCBS quality measures to promote consistent evaluation of quality across state HCBS programs and over time. The list of measures is extensive and encompasses a number of difference outcomes, but reporting is currently voluntary and it’s uncertain how widely the measures will be used. In August, CMS awarded planning grants to three states and two territories, joining the 36 states that participate in the Money Follows the Person program, which is a demonstration that allows states to receive additional federal funding for HCBS delivered to people who transition from institutional to community-based settings. That month, the agency also issued a proposed rule aimed at easing the application and enrollment process for Medicaid, which included several changes intended to increase Medicaid enrollment among seniors and individuals with disabilities.
States reported that a permanent FMAP increase for HCBS would enable them to prioritize more systemic improvements over the longer-term, such as increasing the number of waiver slots or adding permanent wage increases instead of temporary increases in the form of bonuses or incentive payments. Although it’s unlikely that the ARPA FMAP increase – which would require increased federal funding – will be made permanent in the near term, policymakers of both parties have called for systemic changes to HCBS including eliminating waiting lists, increasing opportunities for family members to be paid caregivers, increasing wages for all HCBS providers, and enabling more people to live in their homes as they age. It is unclear whether the consensus on those broad policy goals will translate into new federal laws or funding.
Appendix