A Look at Waiting Lists for Medicaid Home- and Community-Based Services from 2016 to 2023
Home- and community-based services (HCBS) waivers allow states to offer a wide range of benefits and to choose—and limit—the number of people who receive services. The only HCBS that states are required to cover is home health, but states may choose to cover personal care and other services such as private duty nursing through the Medicaid state plan. Those benefits are generally available to all Medicaid enrollees who need them. States may use HCBS waivers to offer expanded personal care benefits or to provide additional services such as adult day care, supported employment, and non-medical transportation. Because waivers may only be offered to specific populations, states often provide specialized benefits through waivers that are specific to the population covered, such as providing supported employment only to people under age 65. KFF estimates that over 4 million Medicaid enrollees use HCBS, and that the numbers of people using HCBS through the state plan are similar to the numbers using HCBS through waivers.
States’ ability to cap the number of people enrolled in HCBS waivers can result in waiting lists when the number of people seeking services exceeds the number of waiver slots available. Waiting lists reflect the populations a state chooses to serve, the services it decides to provide, the resources it commits, and the availability of workers to provide services. In addition, states’ waiting list management approaches differ with regard to prioritization and eligibility screening processes, making comparisons across states difficult. States are only able to use waiting lists for optional services so the number of people on waiting lists can increase when states offer a new waiver or make new services available within existing waivers; in these cases, the number of people receiving services increases, but so does the number of people on a waiting list. In many cases, people may need additional services, but the state doesn’t offer them to anyone or only offers them to people with certain types of disabilities. Waiting lists would not capture the unmet needs of those people. Finally, although people may wait a long time to receive waiver services—36 months on average—most people are eligible for other types of HCBS while they wait.
Even though HCBS waiting lists are an imperfect measure of unmet need, there are no alternative measures available. Many HCBS programs were enacted or expanded in response to the Olmstead decision, a court ruling that found the unjustified institutionalization of people with disabilities is illegal discrimination. As the 25th anniversary of Olmstead nears, waiting lists are sometimes described as contributing to the risk of unnecessary institutionalization for people with disabilities, and policy makers across political parties have proposals to address them. A recent proposed rule would require states to report the number of people are on waiting lists but is not clear how that requirement would be defined.
This data note provides new information about waiting lists from KFF’s most recent survey of state Medicaid HCBS programs, including a discussion of why waiting lists are an incomplete measure of unmet need and why they are not necessarily comparable across states or over time. In the 2023 survey, KFF asked states to report the number of people who were on “interest” lists for HCBS, as well as waiting lists, a difference from prior years (see Box 1). Key takeaways include:
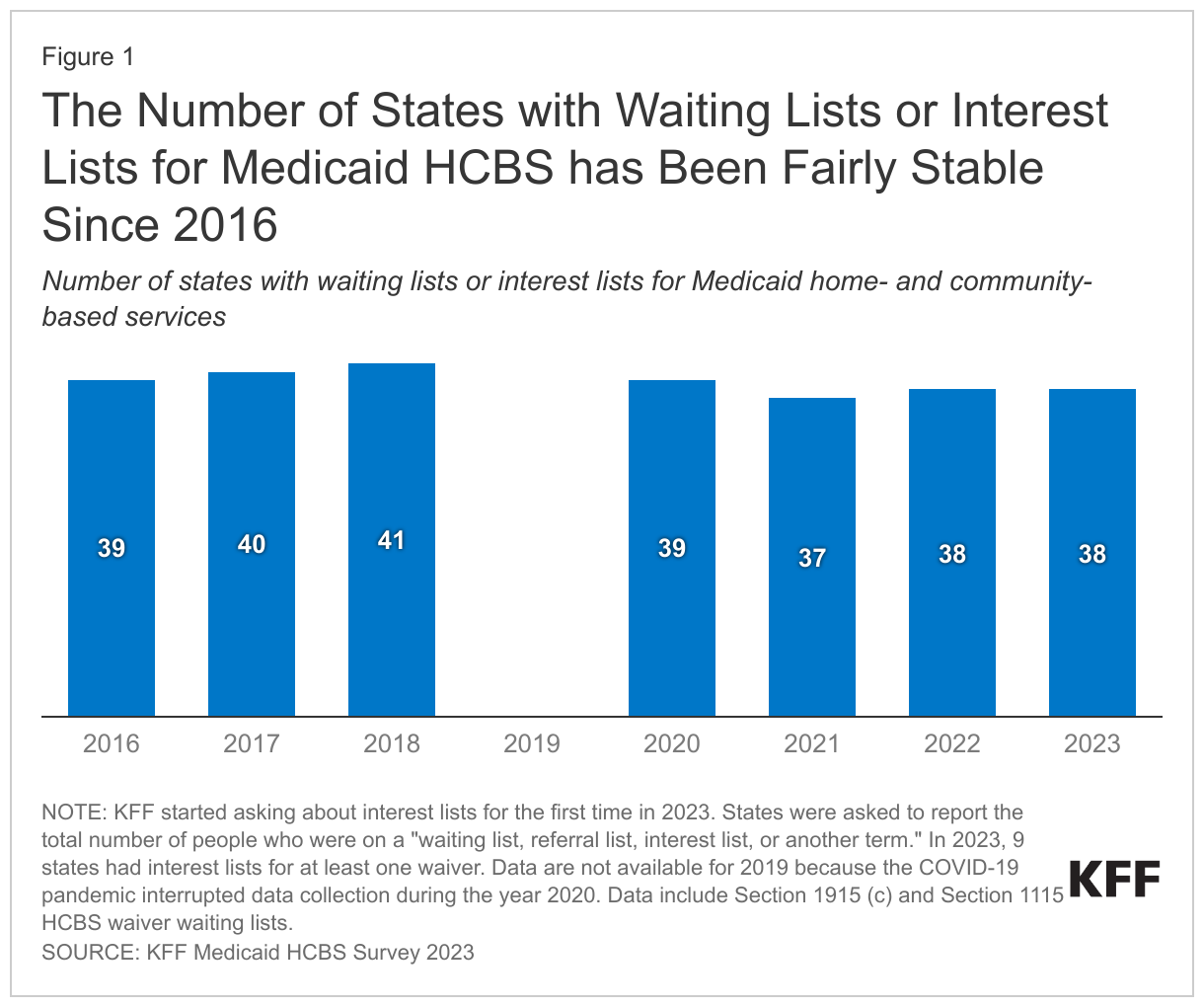
- The number of states that maintain waiting lists or interest lists for people who would like to receive HCBS has fluctuated little between 2016 and 2023.
- In most years since 2016, there have been close to 0.7 million people on waiting lists or interest lists, with a total of over 692,000 in 2023.
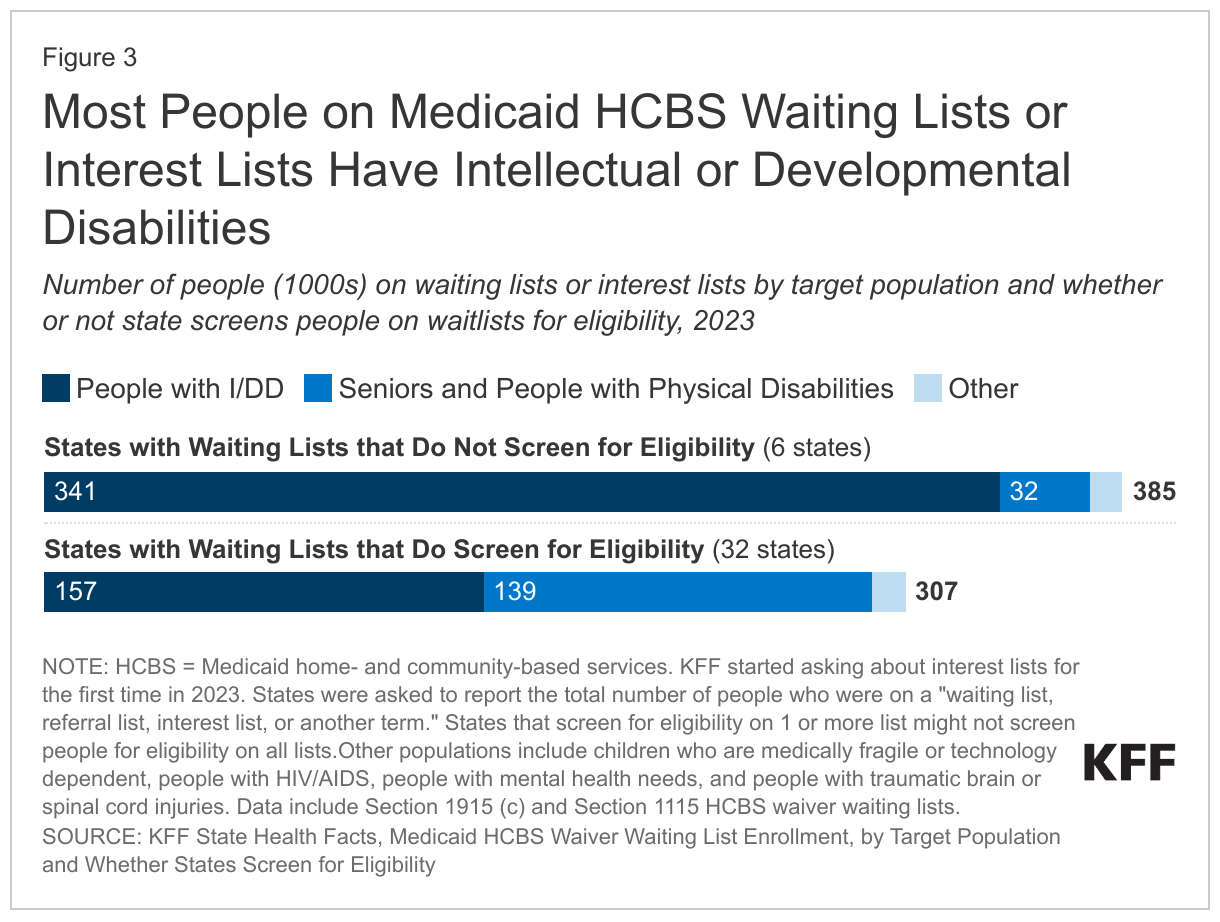
- Most people on waiting lists or interest lists have intellectual or developmental disabilities and most live in states that do not screen any people for eligibility prior to adding them to waiting lists.
- Most people on waiting lists or interest lists are eligible for personal care provided through states’ regular Medicaid programs or for services provided through specialized state plan HCBS benefits.
KFF also recently updated the waiting list indicators on State Health Facts to help people better understand who is on waiting lists and what those waiting lists mean.
How did the number of states with waiting lists change between 2016 and 2023?
Between 2016 and 2023 the number of states with waiting lists has fluctuated between 35 and 41 and is currently at 38 states (Figure 1). While some Affordable Care Act (ACA) opponents have cited waiver waiting lists to argue that expanding Medicaid diverts funds from seniors and people with disabilities, research shows that ACA Medicaid expansion has led to gains in coverage for people with disabilities and chronic illnesses. Waiting lists for HCBS predate the ACA Medicaid expansion, which became effective in most states in 2014, and both expansion and non-expansion states have waiting lists. Waiver enrollment caps have existed since HCBS waiver authority was added to federal Medicaid law in the early 1980s.
Box 1: Changes to KFF’s 2023 Survey on Waiting Lists and Interest Lists
In 2023, KFF asked states to report the total number of people who were on a “waiting list, referral list, interest list, or another term” for HCBS whereas older surveys only asked about waiting lists or referral lists. The change reflects states’ increasing use of terms other than “waiting list” to keep track of people who had expressed interest in HCBS but are not receiving services. KFF broadened the survey to increase the comparability of data across states and across years if states transition to use of different terms.
Prior to 2023, some states used terms other than waiting lists to describe their lists and reported data in the KFF survey, but periodically a state would change its terminology and approach, resulting in what appeared a large fluctuation in the number of people on “waiting lists.” For example, in 2018, Louisiana had nearly 30,000 people on a waiting list for their intellectual or developmental disability waiver. The state implemented a new system to screen people for urgent HCBS needs. Those that met the criteria for urgent needs were placed immediately in services and people with less pressing needs were placed on a “registry” that replaced the older waiting list. By 2020, the waiting list was eliminated. KFF’s assessment is that the broader survey question will capture data that are as consistent with the older years’ data as possible and provide for more meaningful comparisons between states.
When asked specifically, the 2023 survey showed how widespread the use of interest lists was: In 2023, there were more people on interest lists (361,000) than on waiting lists (331,000). The use of the term “interest lists” has important ramifications for a proposed rule on Medicaid access. Under that rule, states would be required to report the number of people on waiting lists, but it’s unclear whether the requirement would apply to lists that are described as interest lists or registries.
A smaller change to KFF’s survey in 2023 was to ask the states to report the number of people on the waiting list at the time the survey was completed. Historically, KFF asked states to report the number of people on waiting lists in the prior year. In the spring of 2023, KFF asked states to report the number of people on waiting lists in 2022, but also the number of people currently on the list. Future years’ surveys will only ask about current waiting list numbers.
Despite the changes to KFF’s survey question, there were few changes in the number of states that reported any waiting lists between the 2022 survey (which requested data from 2021) and the 2023 survey. There were more changes in waiting lists for specific types of waivers, however, with three states eliminating waiting lists for specific waivers, including Connecticut for people with intellectual or developmental disabilities, and North Carolina and West Virginia for people with traumatic brain or spinal cord injuries. Connecticut reported a new list for people with mental health conditions and South Carolina reported several new “processing lists,” that track people’s movement from intake to enrollment for people who are 65 and older or with physical disabilities, for medically-fragile or technology-dependent children, for people with mental health conditions, and for people with HIV or AIDs.
How did the number of people on waiting lists change between 2016 and 2021?
In most years between 2016 and 2023, nearly 0.7 million people have been on waiting lists or interest lists for HCBS (Figure 2). One factor that contributes to changes over time—especially the notable decline between 2018 and 2020—is that not all states screen for Medicaid eligibility prior to adding people to waiting lists and changes in this policy may result in changes in waiting list volumes. For example, between 2018 and 2020, the total number of people on waiting lists decreased by 155,000 or 19%. However, nearly half of that change came from Ohio’s implementation of a waiting list assessment of waiver eligibility, which reduced the size of the state’s waiting list by nearly 70,000 people. In 2023, most states (32) with waiting lists screened individuals for waiver eligibility among at least one waiver, but even among those states, 5 did not screen for all waivers. There were 6 states that do not screen for eligibility among any waivers and those 6 states (Alaska, Illinois, Iowa, Oklahoma, Oregon, and Texas) account for over half of all people on waiting lists. Changes in total waiting lists over time may reflect changes in states’ policies towards eligibility screening (Figure 2).
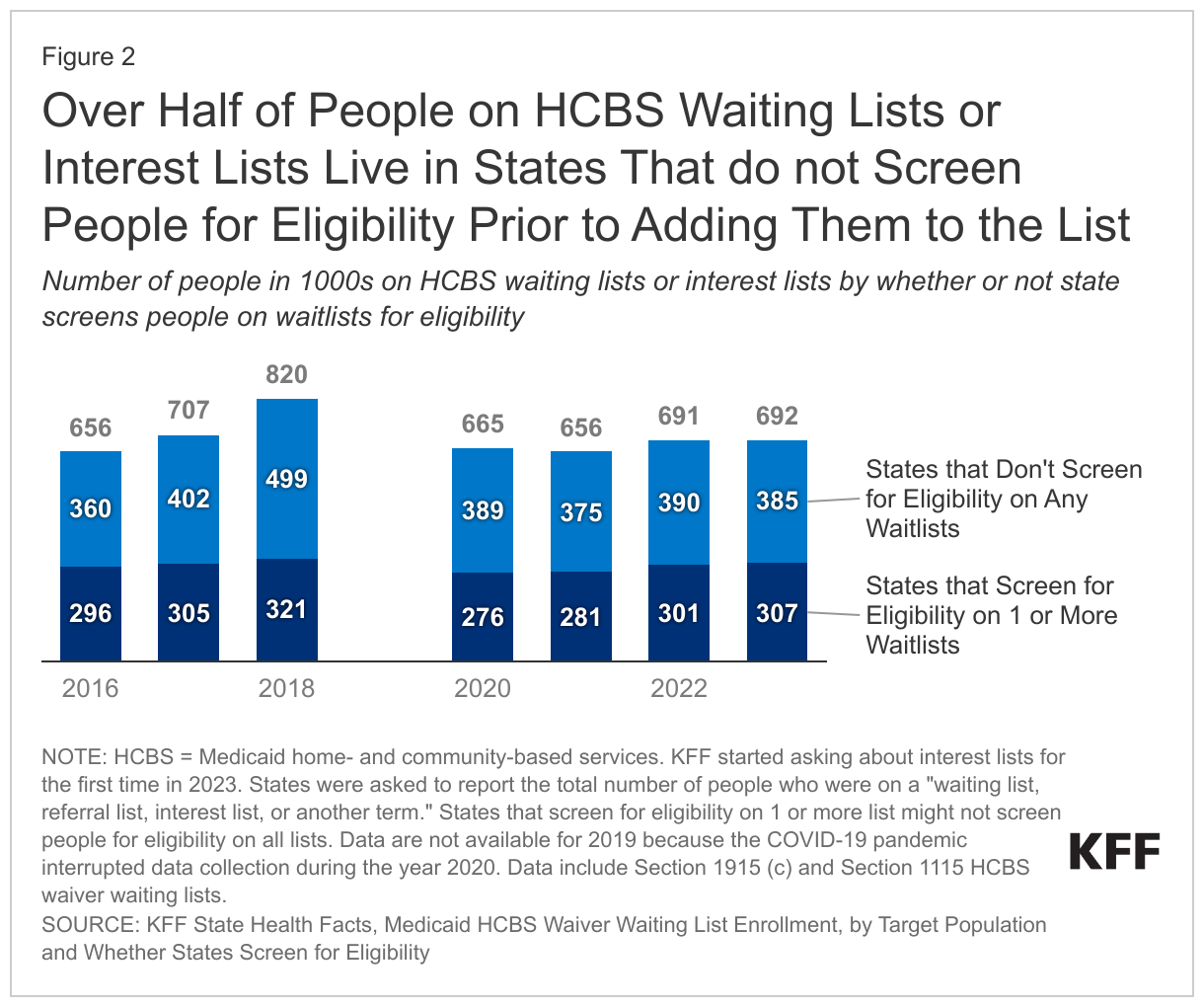
In all years since 2016, over half of people on HCBS waiting lists or interest lists lived in states that did not screen people on waiting lists for eligibility. One reason waiting lists provide an incomplete picture of need is that not all people on waiting lists will be eligible for services. Stakeholder interviews about HCBS waiting lists found that when waiver services are provided on a first-come, first-served basis, people enrolled in waiting lists are in anticipation of future need. That study found that in some states, families would add their children to waiting lists for people with intellectual or developmental disabilities (I/DD) at a young age, assuming that by the time they reached the top of the waiting list, their children would have developed the immediate need for services. Many of those waivers offer comprehensive HCBS packages that include supported employment, supportive housing, or round-the-clock services. Among the six states that do not screen people for eligibility on any lists, five have only waiting lists and the sixth uses interest lists (Illinois does not establish eligibility until selection but does do a preliminary evaluation of eligibility prior to placing someone on the list).
Between 2021 and 2023, total enrollment in waiting lists and interest lists increased by 6%. Overall, there was an increase in the number of people on waiting or interest lists in 18 states and a decrease in 16 states. Some states had significant decreases in their waiting lists such as New Mexico which used additional federal funding from the American Rescue Plan Act to decrease their waiting list for people with I/DD from 3,500 in 2022 to fewer than 300 in 2023. Virginia’s waiting list also decreased significantly from 23,000 in 2021 to under 15,000 in 2022 and 2023.
Increases in waiting lists may reflect improved data about people seeking services. For example, Texas revised its questionnaire to gather more data about people who are interested in HCBS and the number of people on waiting lists/interest lists statewide rose from 312,000 in 2021 to 343,000 in 2023. New York is currently building a portal to track the services received and the number of people waiting for services. The portal will help target provider capacity but may also show an increase in the number of people “waiting” for services that is attributable to improved data collection rather than an increase in unmet needs (New York reported that they had an interest or referral list but that the number of people on it was unknown).
Who is on waiting lists for HCBS?
Most people on waiting lists have intellectual or developmental disabilities (I/DD), particularly in states that do not screen for waiver eligibility before placing someone on a waiting list. People with I/DD comprise 88% of waiting lists in states that do not screen for waiver eligibility, compared with 51% in states that do determine waiver eligibility before placing someone on a waiting list (Figure 3). People with I/DD comprise almost three-quarters (72%) of the total waiver waiting list population. Seniors and adults with physical disabilities account for one-quarter (25%), while the remaining share (3%) includes children who are medically fragile or technology dependent, people with traumatic brain or spinal cord injuries, people with mental illness, and people with HIV/AIDS. People who are on HCBS waiting lists are generally not representative of the Medicaid population or the population that uses HCBS. Most people on waiting lists have I/DD, but KFF analysis shows that people with I/DD comprise fewer than half of the people served through 1915(c) waivers (the largest source of Medicaid HCBS spending).
How long do people on HCBS waiting lists wait to access services and do they have access to HCBS while waiting?
In 2023, people on the waiting or interest lists waited an average of 36 months to receive HCBS waiver services (27 of 38 states responding), down from 45 months in 2021. People with I/DD waited the longest for services, 50 months on average. The average waiting period for other waiver populations ranged from 5 months for waivers targeting seniors to 37 months for waivers that serve people with autism. People with I/DD residing in states that do not screen for eligibility wait longer for services than people with I/DD residing in states that do screen for waiver eligibility (61 months versus 45 months, on average).
Most people on waiting or interest lists are eligible to receive other types of HCBS while they wait. Among the nearly 700,000 people on lists for waiver services in 2023, living arrangements are unknown for more than 600,000. Among the people whose living arrangements are known, 97% (77,000) lived in the community and 3% (2,000) lived in institutional settings. While waiting for waiver services, people living in the community are likely to be eligible for other HCBS through Medicaid state plans. Of the over 4 million people who use HCBS, KFF estimates that roughly half use services provided through the Medicaid state plan, such as personal care to help with bathing or preparing meals, therapies to help people regain or acquire independent living skills, and assistive technology. States may not use waiting lists to restrict the number of people eligible to use such services and over 80% of people on HCBS waiting lists are eligible for personal care or other state plan services. They would not, however, have access to more specialized services such as supported employment or adult day care. People on waiting lists who receive state plan services may also have fewer hours of personal care than they would in a waiver program, or they may not have assistance with some of the activities they need help with such as bathing, dressing, preparing meals, or managing medication.
What to watch?
How might shortages of HCBS workers create problems for states seeking to reduce the number of people on waiting lists? The COVID-19 pandemic exacerbated existing workforce shortages across all HCBS settings and KFF’s most recent survey of state HCBS programs highlighted states efforts to try and address those shortages. Waiting lists may reflect both shortages of workers and insufficient state funds. Although states reported increasing provider payment rates and other efforts to bolster the workforce, challenges remain and some of states’ policies for addressing those challenges have ended with the conclusion of pandemic-era programs. It remains to be seen how policy changes enacted during the pandemic will affect the provision of HCBS in future years and whether the investments in HCBS through the American Rescue Plan Act will result in capacity increases even after the federal funding ends.
How might recently proposed rules affect the number of people on waiting lists or interest lists? One proposed rule on Medicaid access would require states to report on the number of people “who are waiting to enroll in the waiver program,” but it’s unclear whether that requirement would also apply to interest lists, which may include people who are interested in services but not “waiting to enroll.” The rule would make other changes, also intended to increase Medicaid enrollees’ access to HCBS. Increased access to HCBS would increase Medicaid spending, but there is no new federal funding beyond the standard federal matching payments provided to states for Medicaid costs. Funding challenges for states may be particularly relevant given other potential requirements for more staffing in nursing homes, which would tend to increase states’ spending on institutional long-term services and supports. Another proposed rule would codify the Olmstead court decision that requires services to be provided in the most integrated setting appropriate and has spurred many expansions of HCBS waivers.