Difficult Tradeoffs: Key Findings on Workplace Benefits and Family Health Care Responsibilities from the 2020 KFF Women’s Health Survey
Issue Brief
Key Takeaways
- About two-thirds of women who work for pay say that their employer offers them paid sick leave (66%), paid vacation (68%) and a retirement plan (66%), and just over four in ten report that they are offered paid parental leave or paid family and medical leave.
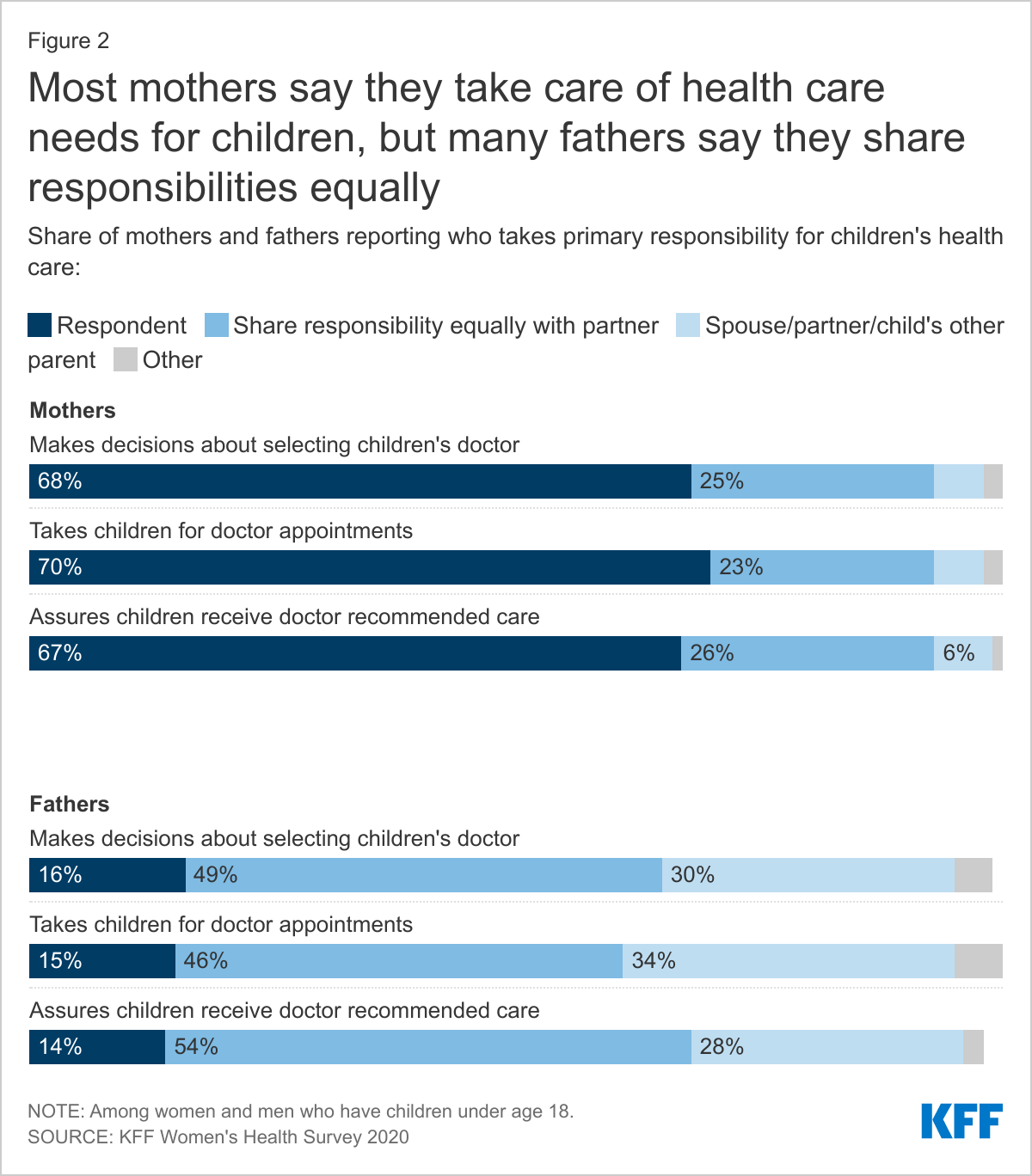
- Among women with school age children, more than six in ten report that they are the ones who usually take charge of health care responsibilities such as choosing their children’s provider (68%), taking them to appointments (70%), and following through with recommended care (67%). Fathers are more likely than mothers to say they share responsibility for these tasks equally with a partner.
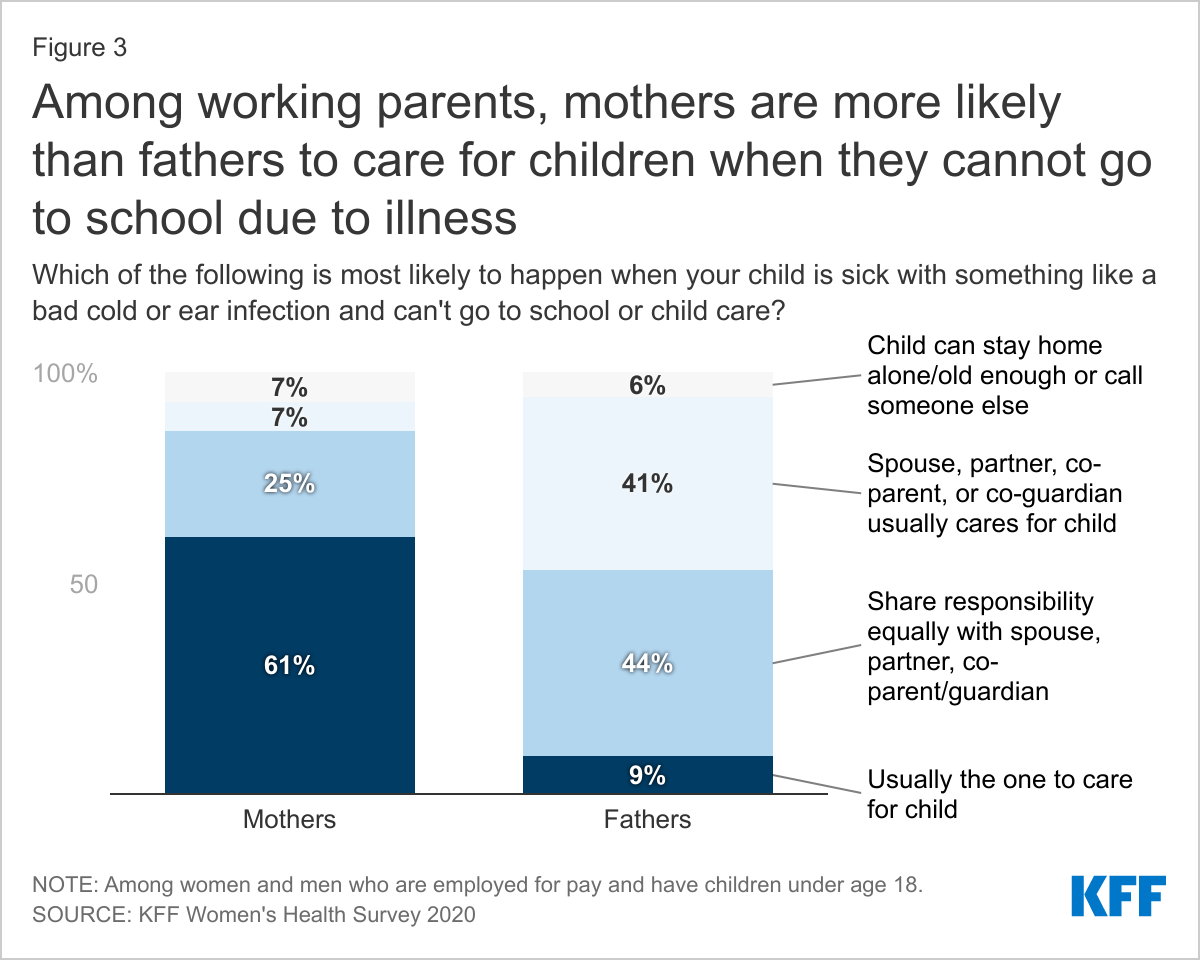
- Among employed parents, mothers are more likely than fathers to report they care for children when they are sick and cannot attend school. Nearly half (46%) of mothers say they are not paid when they take time off to care for children who cannot go to school.
- Mothers who are low-income or in part-time jobs are more likely than those with higher incomes and full-time jobs to report missing work when their children are sick and less likely to have paid sick leave benefits.
Introduction
The persistent challenges that working mothers face in balancing family and work responsibilities came into clear focus during the COVID pandemic. These challenges were intensified by a huge increase in caregiving needs, a shift to homeschooling, a dearth of childcare options, and widespread social isolation. Many women who were considered essential workers did not have the opportunity to work from home and many, particularly women of color, also bore the impact of a sharp rise in unemployment that was exacerbated by decades of structural racism. For many working women, economic security is intertwined with health issues, including workplace benefits such as insurance coverage, paid sick leave, and paid family leave. It is also related to women’s roles as mothers and primary managers of their children’s health care.
This brief provides new data from the KFF Women’s Health Survey, a nationally representative survey of 3,661 women and 1,144 men ages 18-64 (Methodology) conducted November 19, 2020 – December 17, 2020. Among several topics related to women’s health and well-being, we asked respondents about employment and family health care needs. In this brief, we highlight how workplace benefits and caring for children’s health care differ by gender and among different subpopulations of women.
Workplace Benefits
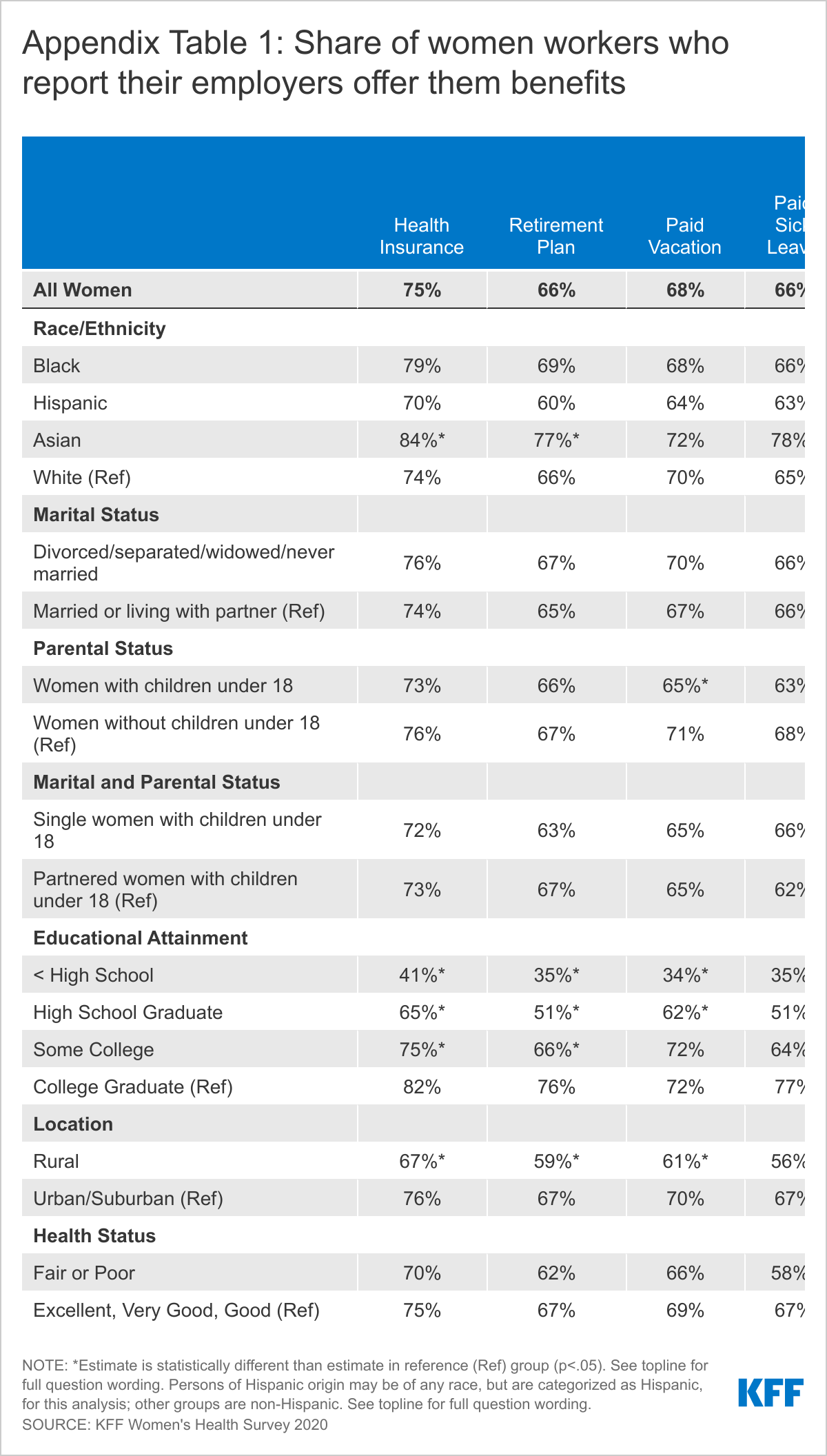
The majority of women who are employed for pay say their employer offers them health insurance, paid sick leave, paid vacation, and a retirement plan. Most, however, are not offered paid parental leave or family and medical leave. Three in four employed women (75%) say their employers offer health insurance (Table 1). About two-thirds report that their employer offers them paid sick leave (66%), paid vacation (68%) and a retirement plan (66%). However, most report that they are not offered paid parental leave or paid family and medical leave. Just over four in ten women workers say they are offered these benefits.
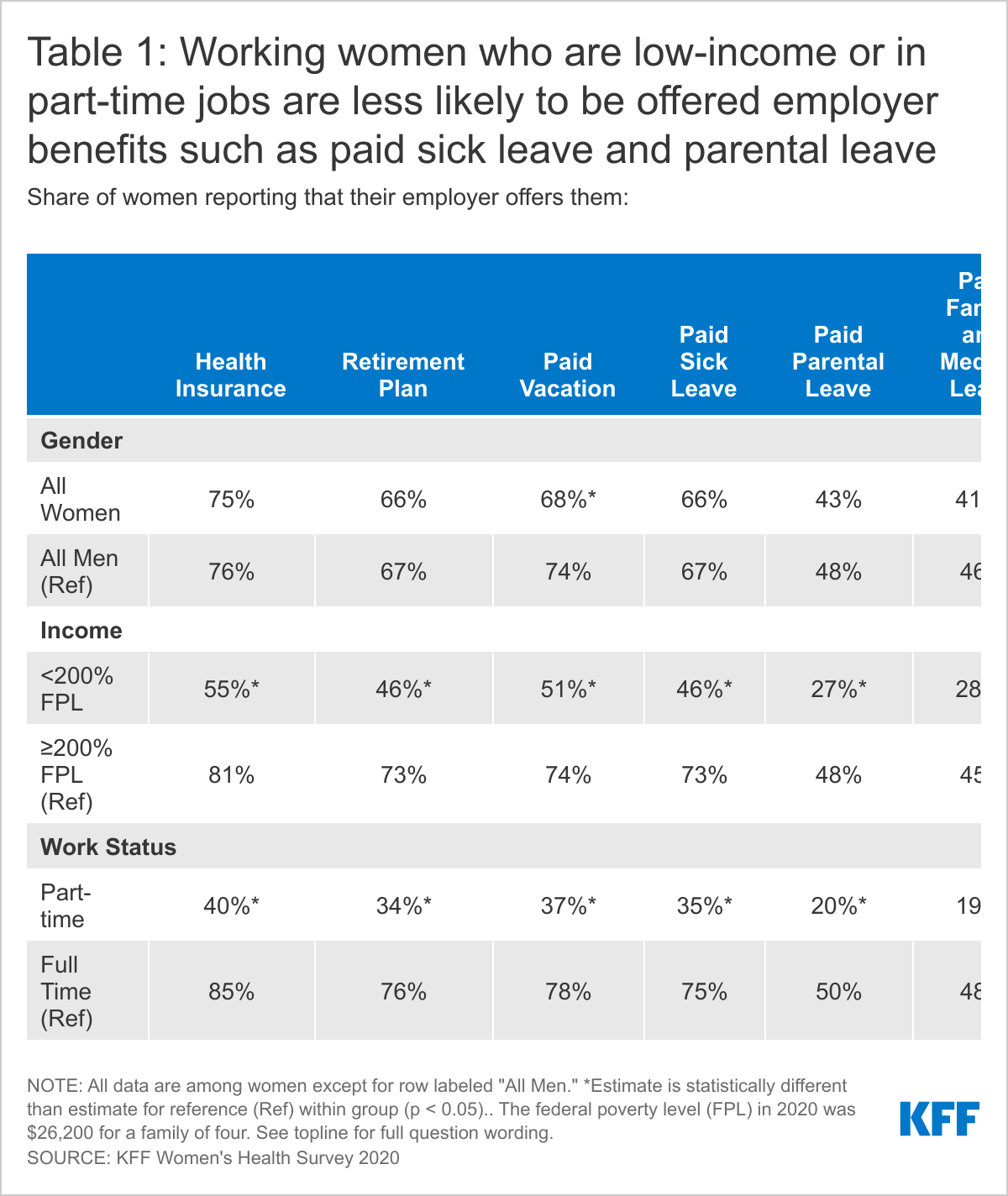
Men report receiving most of these same benefits in similar rates, except that a higher share of men report they are offered paid vacation (74%) and paid family and medical leave (46%). Across the board, low-income women and those with part-time employment are less likely to be offered any of these benefits compared to their higher income and full-time counterparts.
There are also consistent gaps in workplace benefits by educational attainment and geography with lower rates among women in rural areas compared to urban and suburban areas. Among women of color, Asian women report the highest offer rates of several benefits, including health insurance, paid vacation, paid sick leave, and paid parental leave (Appendix Table 1).
Awareness of Paid Parental Leave
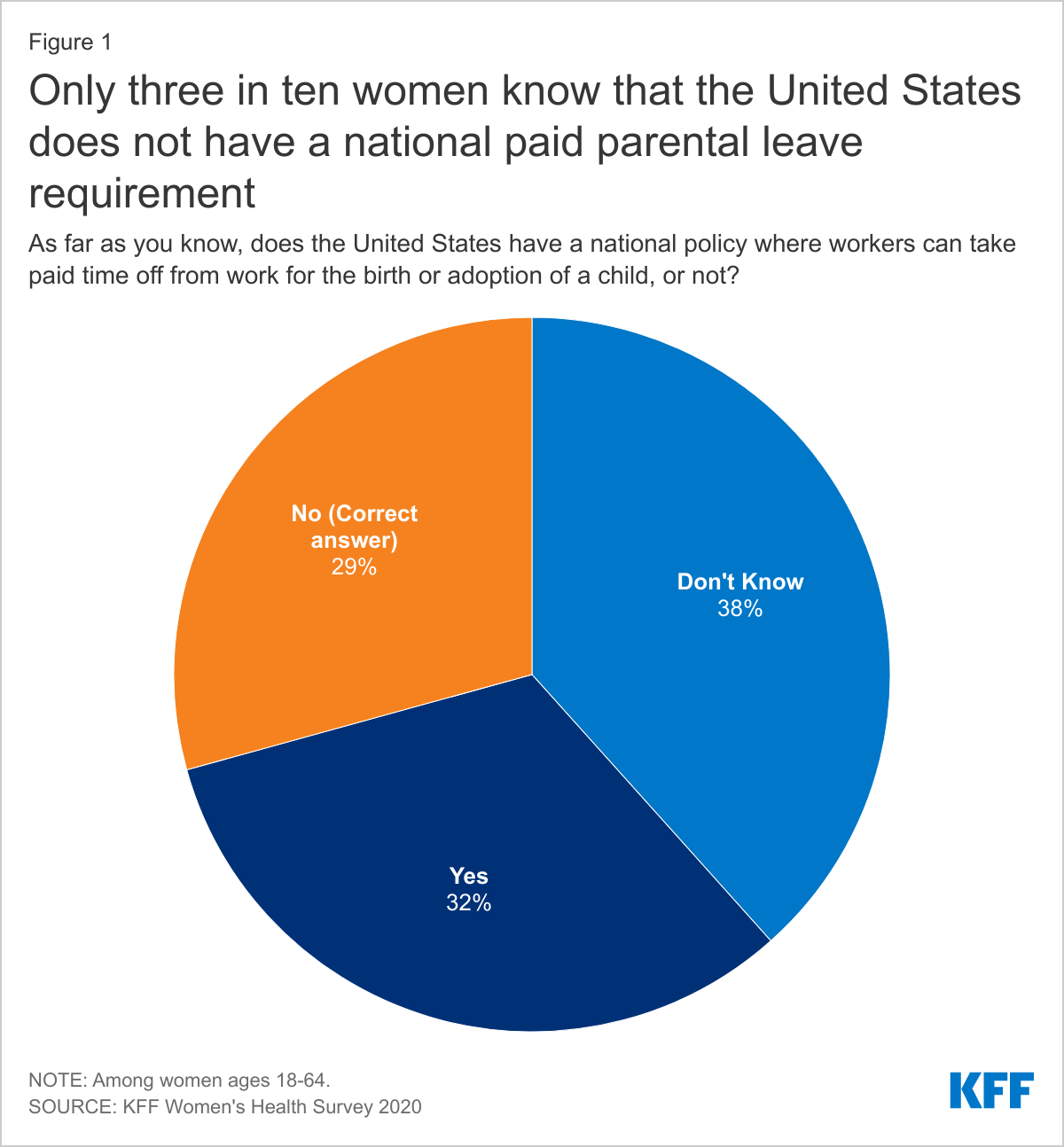
Unlike most high-income countries, there is no federal requirement for employers to offer paid leave to workers after the birth or adoption of a child in the US, although this benefit is required in a few states. The federal Family and Medical Leave Act (FMLA) requires some employers to provide unpaid leave as well as job protection to eligible employees who take time off for the arrival of a child or to care for ill family members, but does not require employers to pay for this time. Despite the fact that few employers offer parental leave to their workers, only three in ten women (29%) are aware that the US does not have a national requirement to provide paid parental leave to workers. About a third of women think (erroneously) that there is a national paid parental leave policy and almost four in ten say that they do not know if there is one (Figure 1). People may not know about the lack of a benefit unless they try to use it and realize they don’t have one.
Parental Roles for Children’s Health
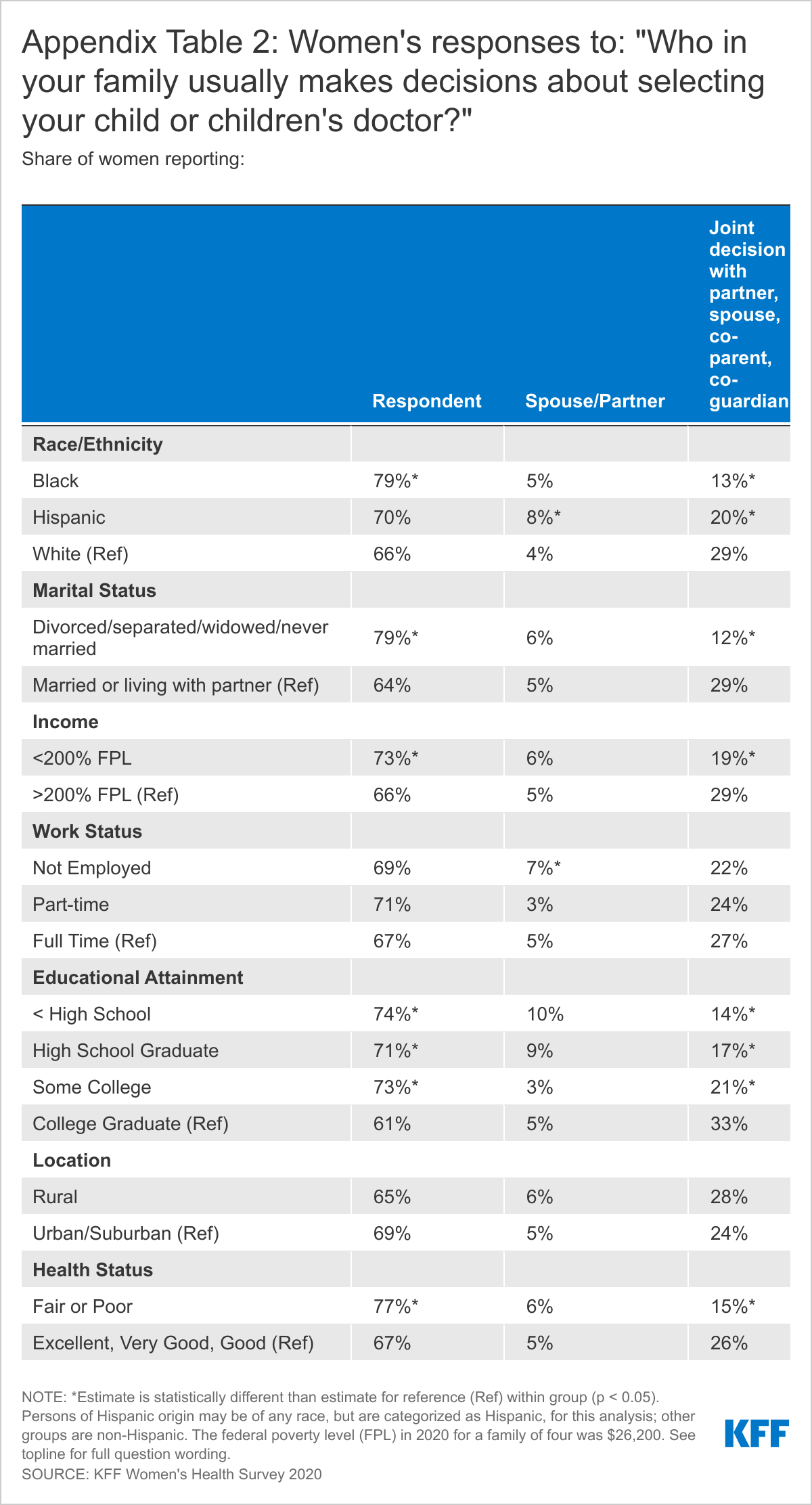
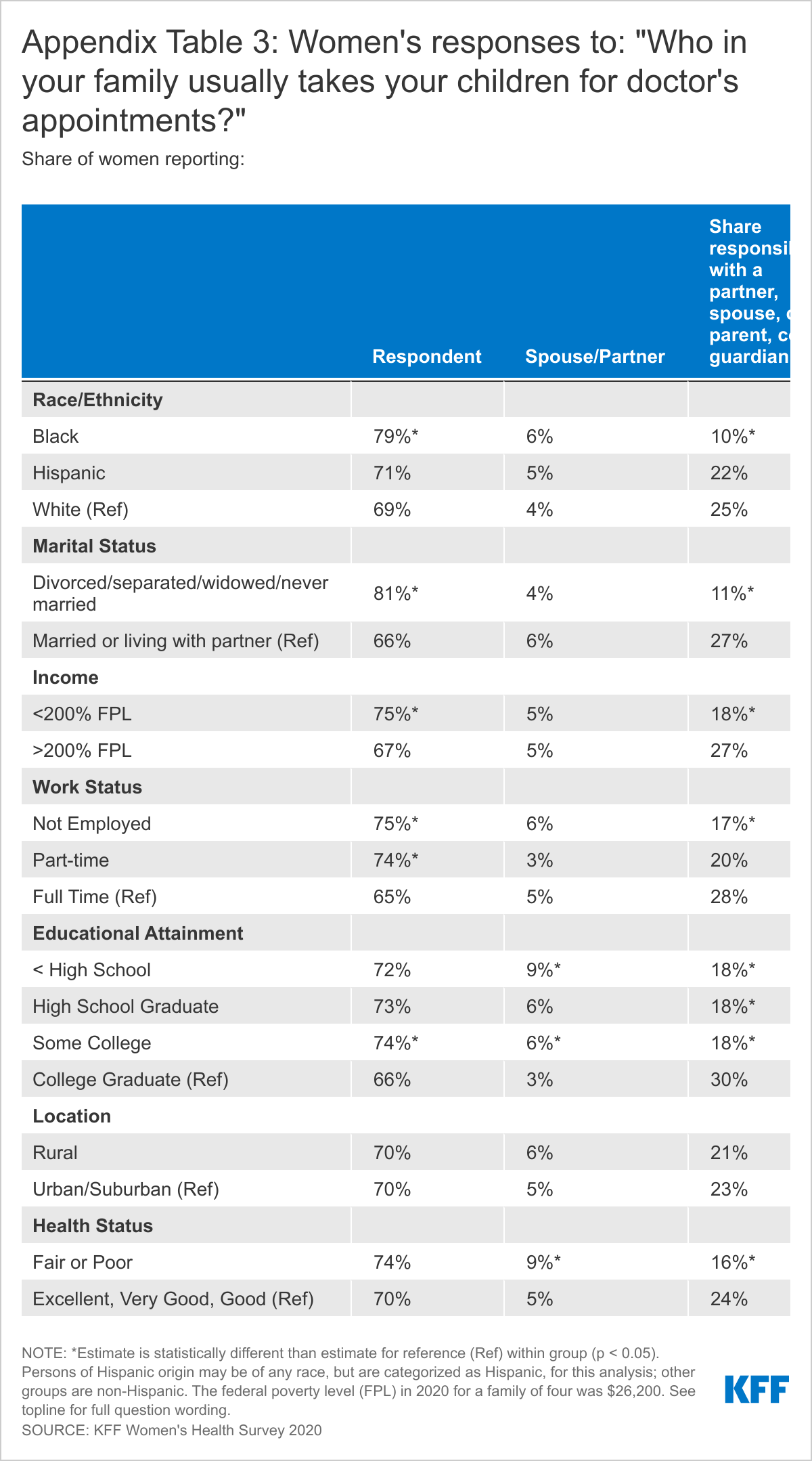
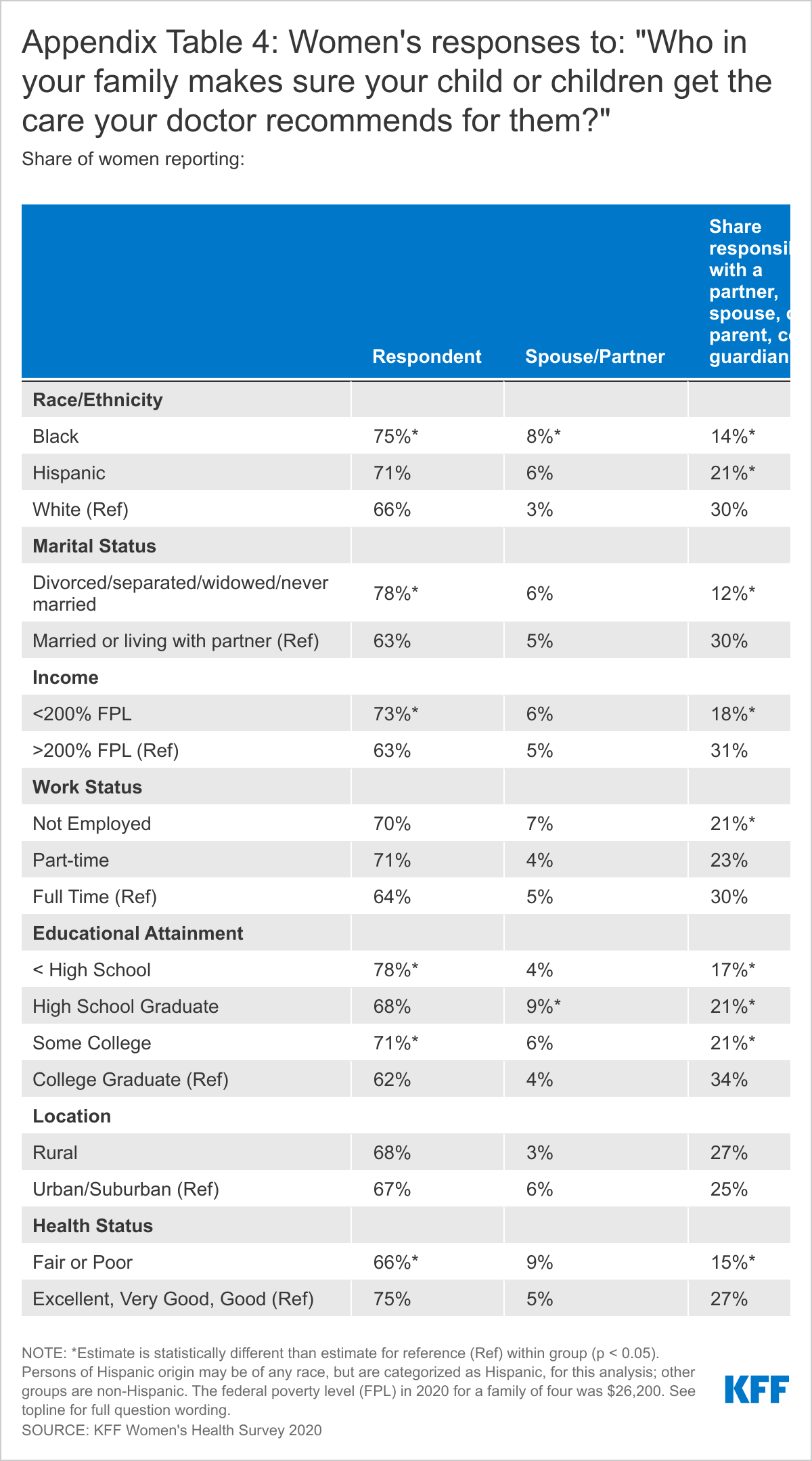
Mothers and fathers have very different perspectives about who takes the lead in managing family health. In most households, women say they are the managers of their families’ health care needs, with fathers playing a lesser role. Many fathers, however, say they share responsibility with a partner jointly. Among women with children under 18, more than six in ten report that they are the ones who usually take charge of health care responsibilities such as choosing their children’s provider (68%), taking them to appointments (70%), and following through with recommended care (67%), compared to less than a fifth of fathers who report they take care of these tasks (Figure 2). Mothers and fathers differ somewhat on their assessment of their involvement in children’s health care. While fathers are more likely to report that their partners take care of their children’s health needs than themselves, they are also more likely than mothers to report that it is a joint responsibility. About half of fathers say they share health care responsibilities equally with a partner or other parent, compared to about a quarter of mothers.
There are some variations in children’s health care responsibilities between groups of women by race/ethnicity, income, marital status, and education level (Appendix Tables 2, 3, 4). Black women are more likely to say that they attend to children’s health care needs and are less likely to share the work with a partner compared to White women. Single mothers and low-income mothers are also more likely than partnered and higher income mothers to say that they are typically responsible for managing their children’s health care.
Impact of Children’s Health Needs on Working Parents
Among working parents, mothers report they are more likely than fathers to care for children when they are sick and cannot attend school. Six in ten working mothers (61%) say they are usually the one to take care of children who are sick and cannot got to school, more than six times the share of working fathers (9%) who say this is the case (Figure 3). However, this is another topic where men are more likely to say that they share in the work equally. A quarter of mothers and 45% fathers say they share responsibility for this jointly.
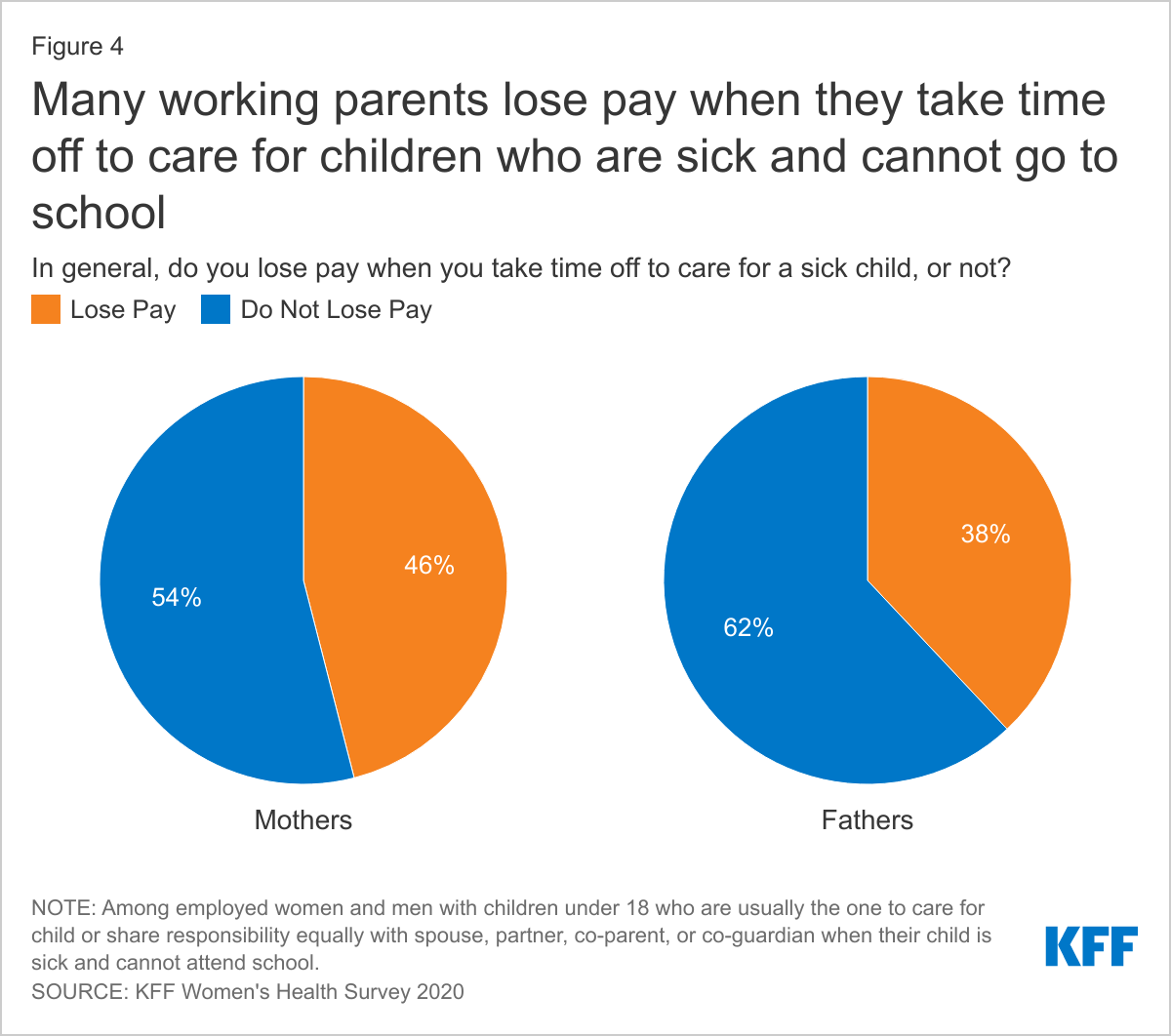
Caring for children’s health can have tangible economic consequences for parents, but especially for women. When mothers care for children because they are sick and cannot go to school, 46% are not paid for time off, as is the case for 38% of men (Figure 4). Considering that nearly one-fifth of children miss at least three school days a year due to illness or injury, missing work to care for sick kids is a common occurrence with negative economic implications for many employed parents. Furthermore, as schools re-open, there could be a rise in parents missing work to stay home with children due to COVID concerns.
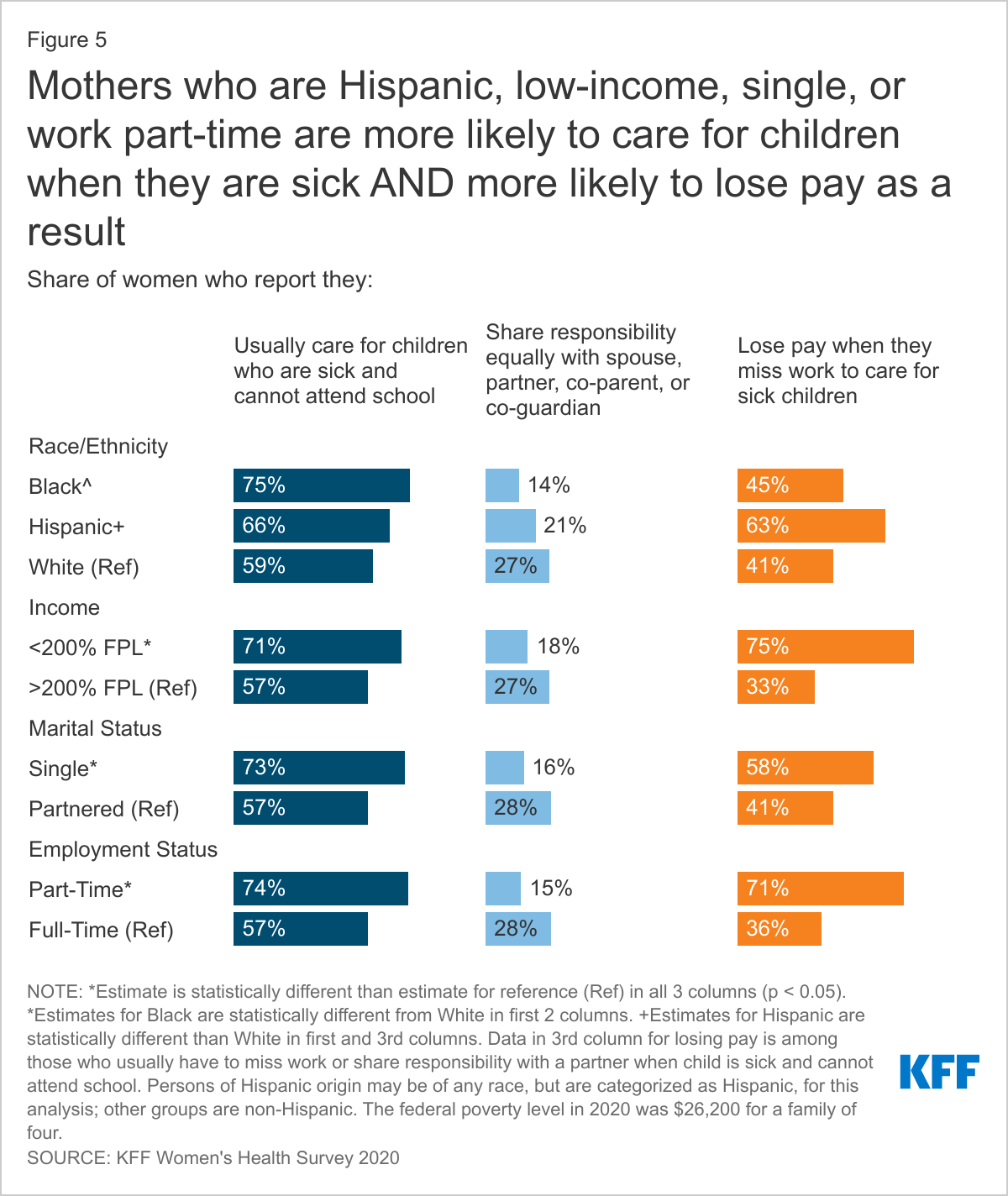
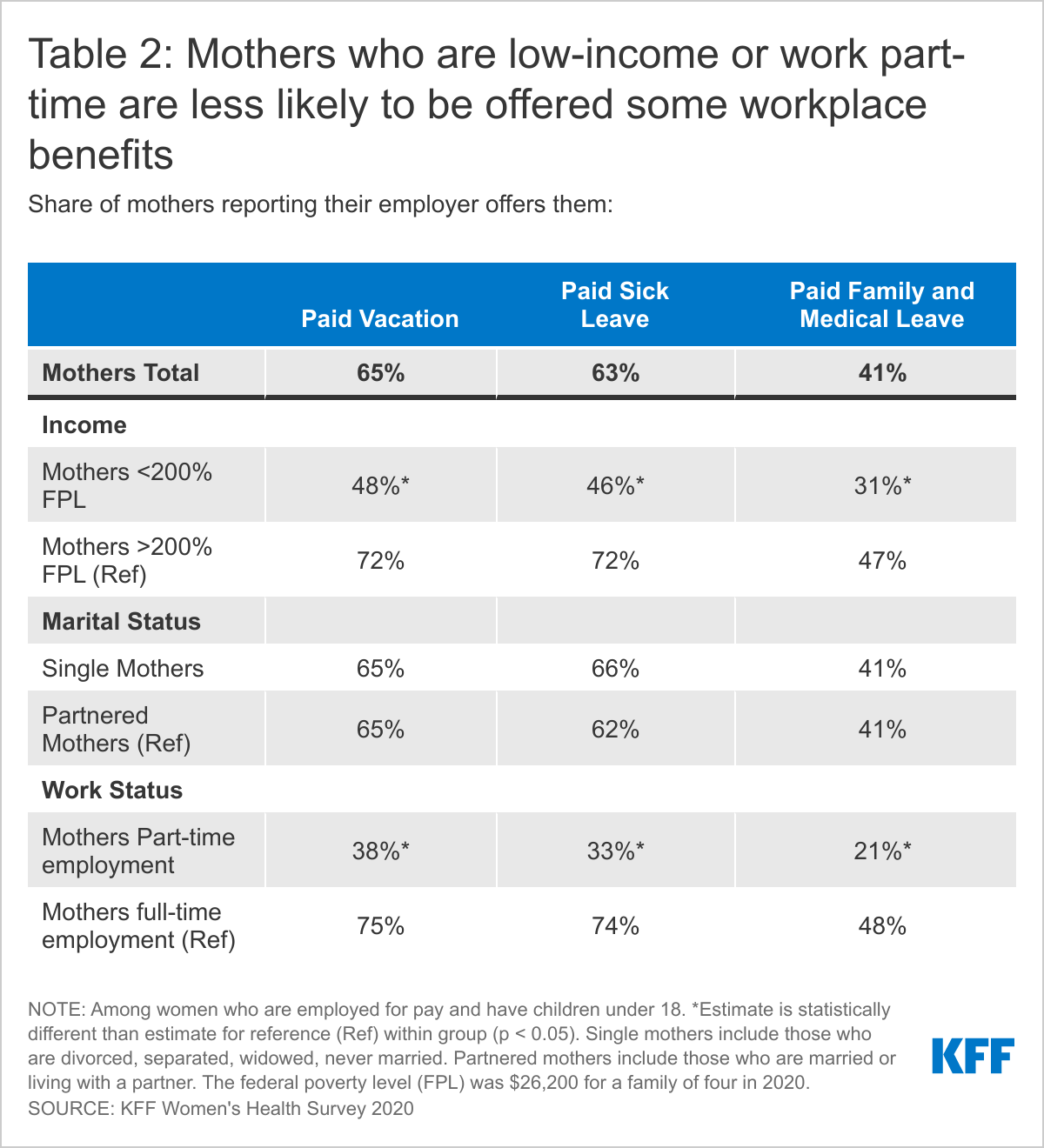
Mothers in part-time jobs, those who are low-income, and who are single parents are more likely to report they are the ones to care for children when they are sick compared to their full-time, higher income, and partnered counterparts. Low-income mothers who must miss work when their child is sick are also far more likely to lose pay (75%) compared to higher income mothers (33%) (Figure 5). Additionally, there is a large disparity in workplace benefits, with offer rates of paid sick leave and paid vacation significantly lower among mothers who are low-income or part-time employees (Table 2).
Conclusion
Women now comprise at least half of the nation’s workforce, yet median earnings for women are 81% of men’s earnings, a gap that has persisted for years and is even larger for women of color. Roughly seven in ten women with children under age 18 are in the labor force, but can face challenges without access to paid parental leave. The United States remains one of the few industrialized nations that does not require paid leave for major health events, such as the birth or adoption of a child, to care for an aging relative, or for routine sick leave that most workers will need at some point. For many women, even a month of leave after childbirth is unaffordable and unattainable without paid time off. Additionally, missing work when their children are sick, including with COVID-19, has an economic cost, as nearly half are not paid when they take a sick day.
Women continue to be the primary health care managers for their families, although some share the work for children’s health care with partners, and perceptions of responsibility for caregiving differ substantially between mothers and fathers. Mothers will play a significant role in the nation’s pandemic recovery, as they are likely to take the lead on getting kids vaccinated once vaccines are available for children. This survey finds that many working women, particularly those with lower incomes or in part-time jobs, do not have workplace protections such as paid sick days or paid family leave. This past year, this gap has been amplified by the lack of in person education for school aged children and childcare closures, along with an unparalleled national health crisis that has disproportionately affected low-income communities of color across the nation. While federal policymakers have addressed some of these gaps through the various federal COVID relief laws passed by Congress, these measures are restricted to certain industries and employer sizes, and time-limited. For some women, the system is largely working. But, for many others, including those who are in low-wage jobs or work part-time hours, the financial consequences of taking time off to care for their children can force them to make difficult tradeoffs between their financial wellbeing or their families’ health.
Methodology
The 2020 KFF Women’s Health Survey was designed and analyzed by researchers at the Kaiser Family Foundation (KFF) of a representative sample of 4,805 adults, ages 18-64 years old (3,661 women and 1,144 men). The survey was conducted online and telephone using AmeriSpeak®, the probability-based panel of NORC at the University of Chicago. U.S. households are recruited for participation using address-based sampling methodology and initial invitations for participation are sent by mail, telephone, and in-person interviews. Interviews were conducted in English and Spanish online (4,636) and via the telephone (169). Our previous Women's Health Surveys were conducted exclusively by telephone, so trend data are not included in our 2020 survey. Interviews for this survey were conducted between November 19 and December 17, 2020, among adults living in the United States. KFF paid for all costs associated with the survey.
The sample for this study was stratified by age, race/ethnicity, education, and gender as well as disproportionate stratification aimed at reaching uninsured women, women who identify as LGBT, Asian women, and women 18-49 years old. The sampling also took into consideration differential survey completion rates by demographic groups so that the set of panel members with a completed interview for a study is a representative sample of the target population. This survey includes people who self-identified as 'female' or 'male’ regardless of their sex at birth. While our goal was to be as inclusive as possible, we were not able to obtain a large enough sample to support a separate questionnaire that addresses the unique health concerns and experiences of non-binary or gender-fluid people to include them in this survey. We recognize that additional study is needed to better understand the health and access issues faced by non-binary people.
A series of data quality checks were run and cases determined to be poor-quality, as defined by surveys with a length of interview of less than 33% of the mean length of interview and with high levels of question refusal (>50%) were removed from the final data (n=96). Weighting involved multiple stages. First, the sample was weighted to match estimates for the national population from the 2020 Current Population Survey on age, gender, census division, race/ethnicity, and education. The second round of weights adjusted for the study’s sampling design. All statistical tests of significance account for the effect of weighting.
The margin of sampling error including the design effect for the full sample of women is plus or minus 2 percentage points. Numbers of respondents and margins of sampling error for key subgroups are shown in the table below. For results based on other subgroups, the margin of sampling error may be higher. Sample sizes and margins of sampling error for other subgroups are available by request. Note that sampling error is only one of many potential sources of error in this or any other public opinion poll.
| Group | N (unweighted) | M.O.S.E |
| Men Ages 18-64 | 1,144 | +/- 4 percentage points |
| Women Ages 18-64 | 3,661 | +/- 2 percentage points |
| Women Ages 18-49 | 2,695 | +/- 2 percentage points |
| White Women Ages 18-64 | 1,813 | +/- 3 percentage points |
| Black Women Ages 18-64 | 603 | +/- 5 percentage points |
| Hispanic Women Ages 18-64 | 801 | +/- 5 percentage points |
| Asian Women Ages 18-64 | 246 | +/- 8 percentage points |
| LGB Women Ages 18-64 | 392 | +/- 7 percentage points |
| Heterosexual Women Ages 18-64 | 3,239 | +/- 2 percentage points |
| Women < 200% FPL | 1,471 | +/- 3 percentage points |
| Women ≥200% FPL | 1,943 | +/- 3 percentage points |
Appendix