Coverage of Breast Cancer Screening and Prevention Services
Among women in the United States, breast cancer is the most diagnosed cancer and the second leading cause of cancer death. In 2021, an estimated 4 million women in the U.S. were living with breast cancer. The Affordable Care Act (ACA) and many state laws have provisions that assure that most women with private insurance, Medicaid, and Medicare have coverage for breast cancer screening services. This typically includes mammography but can also include genetic testing and preventive medications for high-risk women over the age of 35. This factsheet discusses breast cancer screening and prevention services and reviews the scope of private and public insurance coverage, as well as access to those services, for women in the U.S.
Breast Cancer in the United States
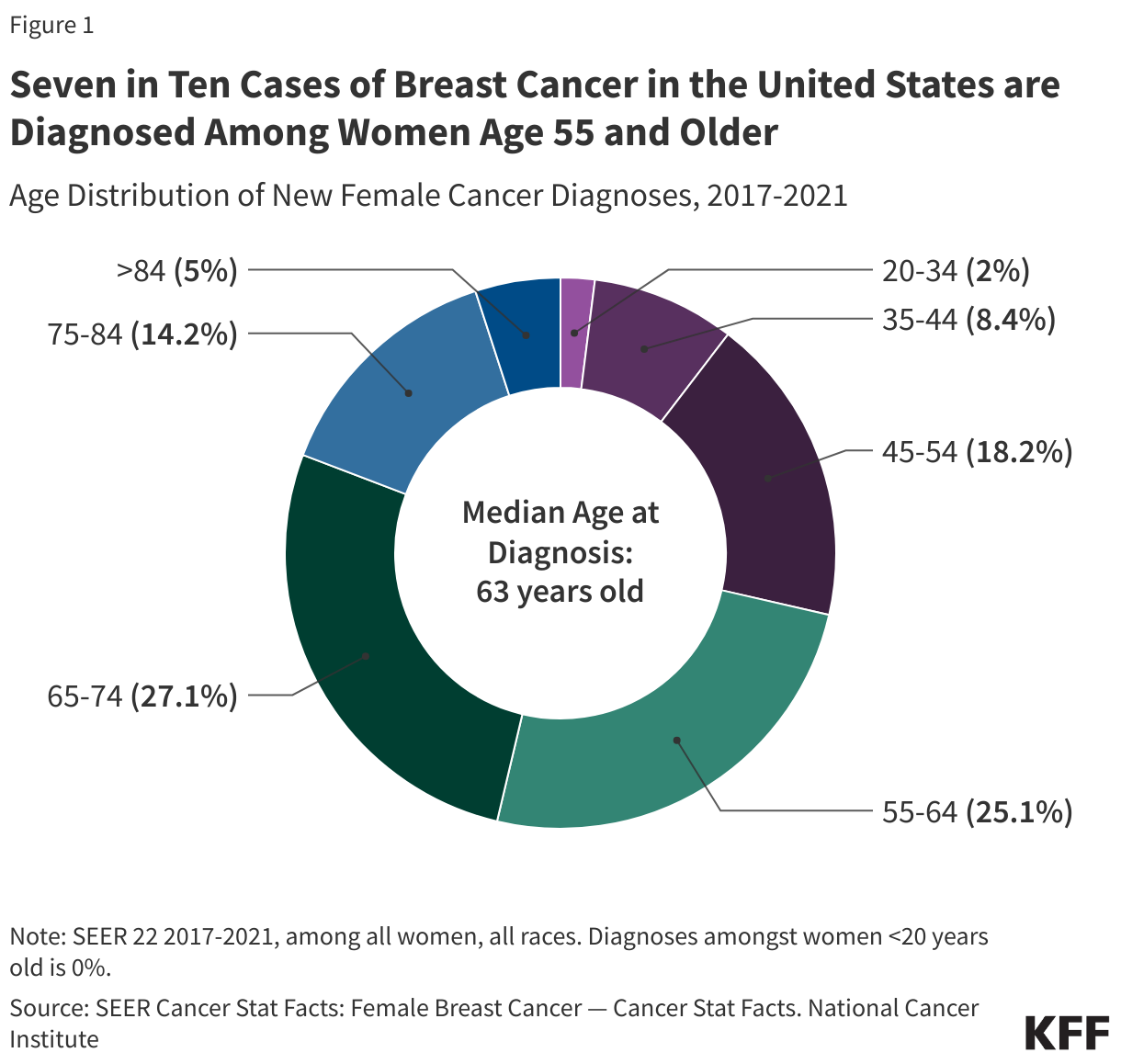
Breast cancer makes up about 16% of all new cancer diagnoses in the U.S., and approximately 1 in 8 women will be diagnosed with breast cancer during their lifetime. In 2025, there will be an estimated 316,950 new cases of female breast cancer and 42,170 deaths attributable to breast cancer in the U.S. Breast cancer is most often diagnosed among middle-aged and older women, with 71% of new cases diagnosed among women 55 and older (Figure 1).
Most breast cancers are diagnosed at an early stage. Sixty-six percent of breast cancers diagnosed are localized, meaning they are found only in the organ in which they started; 25% are regional, meaning the cancer has spread to surrounding organs; and 6% have metastasized, meaning the cancer has spread to other regions of the body. Risk factors for breast cancer include, but are not limited to, a personal or family history of breast cancer, genetic predispositions, breast density, obesity, drinking alcohol, early menstruation, and delayed menopause.
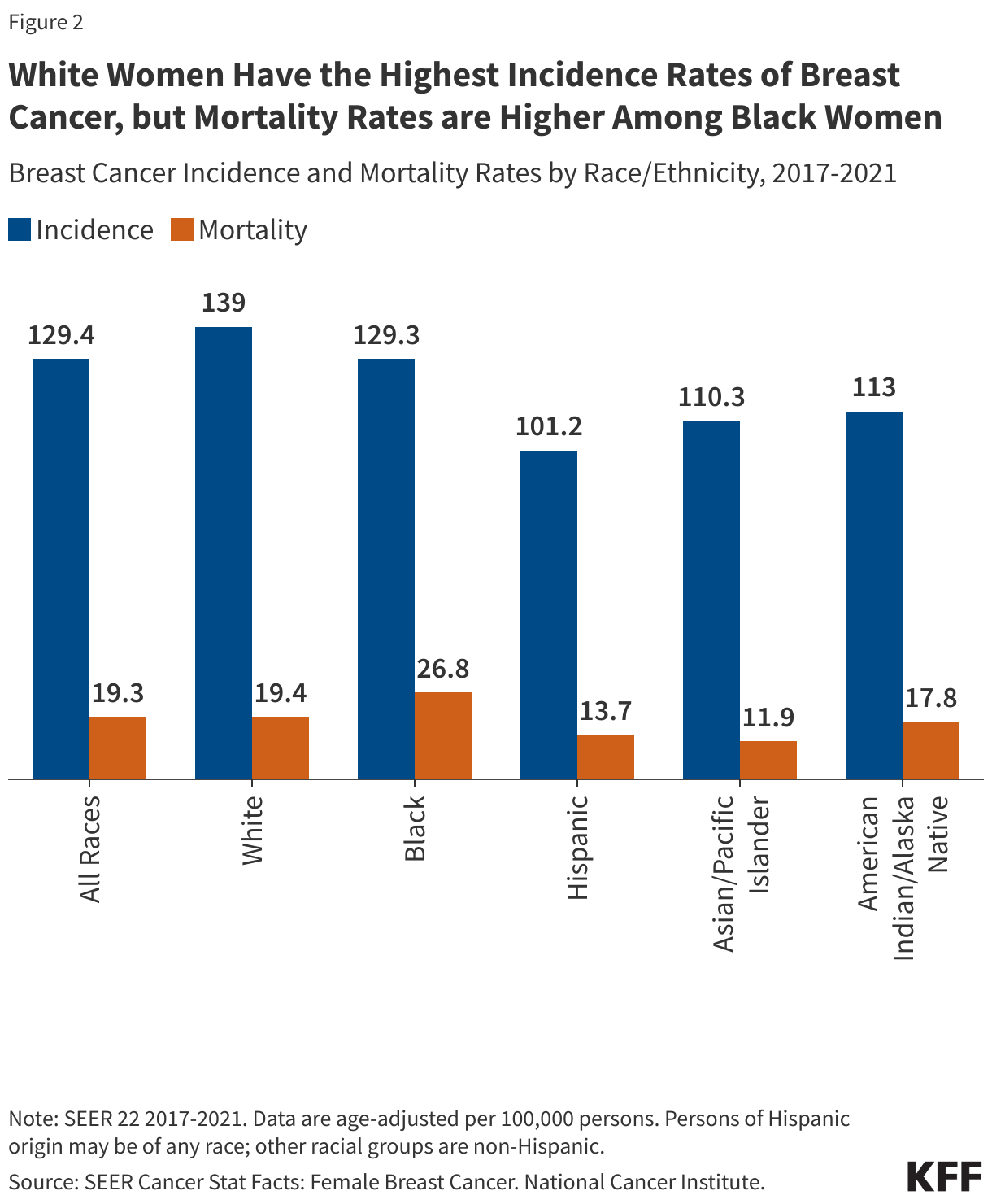
In the U.S., while white women have the highest incidence of breast cancer, black women have higher breast cancer mortality rates (Figure 2). These disparities are likely attributable to a combination of factors, such as differences in stage at diagnoses, as well as disparities in access to screening, follow-up care, and treatment.
Although very rare (less than 1%), men can develop breast cancer. In 2025, there will be approximately 2,800 cases of male breast cancer diagnosed and 510 deaths.
Breast Cancer Preventive Services
While several health organizations issue guidelines for breast cancer screening and prevention, private insurance coverage of clinical preventive services under the ACA is governed by recommendations from the United States Preventive Services Task Force (USPSTF) and the Health Resources and Services Administration (HRSA). The Women’s Preventive Services Initiative (WPSI) is the group that works with HRSA by providing clinical recommendations for preventive services specific to women and makes coverage recommendations to HRSA for breast cancer screening. Under these guidelines, private group and individual insurance plans and state Medicaid expansion programs must cover the following breast cancer screening and prevention services at no cost to the consumer: 1) screening mammography at least every 2 years and as frequently as once a year for women ages 40 to 74 with average-risk for breast cancer; 2) genetic counseling and testing for mutation of the BRCA1 and BRCA2 genes in some women with a personal or family history of breast, ovarian, fallopian tube, or peritoneal cancer; 3) preventive medication for some women with elevated risk of breast cancer and at low risk for adverse medication effects (Table 1). Some medical professionals recommend other services for women at higher risk for breast cancer, but these services are not currently subject to the ACA’s preventive services coverage requirement. The ACA’s preventive services requirement is currently the subject of ongoing litigation in the case Kennedy v. Braidwood Management. Depending on the eventual outcome of that case, there could be changes to preventive services requirements in the future.

Mammography Utilization
Screening mammography is a low-dose x-ray that provides images of the internal structures of the breast and is the most common screening test for breast cancer.
Current HRSA guidelines—which define no-cost coverage standards for private insurance—and WPSI recommend biennial screening mammography to start no earlier than age 40 and no later than age 50 for average-risk women and continue through at least age 74, while the USPSTF breast cancer screening guidelines recommend biennial screening mammography for women aged 50 to 74, and states that starting mammography screening before age 50 should be an individual decision based on preference and patient values. The USPSTF also concludes that there is insufficient evidence to assess the benefits and harms of screening mammography for women 75 years and older.
In 2022, 77% of women ages 50-74 reported having had a mammogram in the past two years (Figure 3). Screening rates are higher among women with insurance (74%) compared to those without insurance (37%).

Mammography use varies by state (Figure 4). Among women ages 50-74, Rhode Island reported the highest rate of mammography use (85.5%) whereas Wyoming reported the lowest rate (64%).

Breast Density
Breast density refers to the amount of fibrous and glandular tissue (or, fibroglandular tissue) in the breast compared to the amount of fatty tissue. Dense breasts have more fibroglandular tissue, while less dense breasts have more fatty tissue. Although breast density is a risk factor for developing breast cancer, breast density changes naturally throughout one’s lifetime, and dense breasts are very common—nearly half of women over 40 years old who have had a mammogram have dense breasts. As of September 2024, the U.S. Food and Drug Administration (FDA) requires mammography facilities to report the presence of breast density detected by imaging to both patients and providers.
Mammograms are the most used imaging method for breast cancer screening, but dense breasts can be difficult to interpret with this technique. Fibroglandular tissue and masses in the breast appear similarly in mammogram images, meaning cancerous masses may go undetected in someone with dense breasts. Consequently, additional imaging such as ultrasound, MRI, or digital breast tomosynthesis (DBT) may be required to complete a breast cancer screening. However, follow up imaging for women with dense breasts is not currently required to be covered by insurance as preventive services.
Genetic Testing and Screening for BRCA 1/ BRCA 2 Mutations
Mutations to the tumor suppressor genes BRCA1 and BRCA2, increase the risk of female breast and ovarian cancers, as well as fallopian tube, peritoneum, pancreatic, and skin cancers. While almost 13% of women in the general population will develop breast cancer at some point in their lives, over 60% of women who have inherited a mutation in either BRCA1 or BRCA2 will develop breast cancer in their lifetime. Factors associated with an increased likelihood of having a harmful BRCA1 or BRCA2 mutation include: personal or family history of breast cancer diagnoses before age 50, cancer in both breasts, both breast and ovarian cancers in the same individual, reoccurring cases of breast cancer, family history of BRCA mutations, cases of male breast cancer, and being of Ashkenazi Jewish descent.
Currently, the USPSTF recommends that primary care providers use a familial risk assessment tool to screen women who have a personal or family history of breast, ovarian, tubal, or peritoneal cancers or have an ancestry associated with BRCA 1/2 gene mutations. It is also recommended that women with positive screenings receive genetic counseling and, if necessary, BRCA genetic testing. This screening is required to be covered by insurance plans without cost sharing as a preventive service due to the USPSTF recommendation.
Preventive Medication
The use of medications to help reduce the risk or delay the onset of cancer is called chemoprevention. Raloxifene and aromatase inhibitors are two medications used to reduce primary breast cancer risk in postmenopausal women, while tamoxifen reduces risk in premenopausal women and women who do not have a uterus. The USPSTF recommends that clinicians should discuss and offer to prescribe these risk-reducing medications to some women 35 and older who are at an increased risk for breast cancer and at low-risk for adverse medication effects. This is covered without cost-sharing for those with private insurance or under Medicaid expansion. While Medicare covers chemoprevention, patients may be subject to cost-sharing for these drugs. It is recommended that women who are not at an increased risk for breast cancer should not take these medications prophylactically.
Programs for Breast Cancer Services
Most women with public and private insurance have coverage for breast cancer screening services, but the scope of coverage can differ based on the type of insurance plan, how they qualify for Medicaid, and in the case of Medicare, where they live. While there are programs to assist uninsured and underserved women, these programs only reach a fraction of eligible women.
- Private Individual and Group Insurance Plans—The ACA requires most private group and individual insurance plans (including most employer plans) to cover recommended preventive services with an “A” or “B” rating from the USPSTF, as well as preventive services recommended by HRSA, without consumer cost-sharing. In addition to covering the full cost of mammograms starting at age 40, plans must cover genetic screening and preventive medication for high-risk women. Currently, there is ongoing litigation over the scope of the preventive services requirement in the case, Braidwood Management Inc. v. Becerra, which could affect coverage policy of preventive health services in the future.
- Medicaid— Under the ACA, women who qualify for Medicaid through their state’s Medicaid expansion are entitled to the same screening and preventive services as women who are covered by private insurance. Traditional Medicaid programs consider breast cancer screening and preventive services to be “optional” and the scope of coverage is determined by the state. A 2021 state survey of Medicaid programs, however, found that most states cover breast cancer screening and prevention services under both expansion and traditional eligibility pathways.
- Medicare—Medicare Part B covers annual screening mammograms at no-cost for women 40 and over. Coverage for BRCA genetic testing is not required nationally, but may be covered in some regions based on local coverage determinations. Women enrolled in a Medicare Part D drug plan who are at high-risk for breast cancer may have coverage for chemoprevention drugs, but there is no requirement for Part D plans to cover these drugs without cost sharing.
- TRICARE—TRICARE, the public program for military personnel and dependents, covers screening mammography for women 40 and older, BRCA genetic counseling, and chemoprevention, but is not required to offer coverage without cost-sharing. Out-of-pocket costs for consumers vary by an individual’s specific level of TRICARE coverage and active-duty status.
- The National Breast and Cervical Cancer Early Detection Program (NBCCEDP)—The NBCCEDP is a CDC program that helps low-income, uninsured, and underinsured women access breast and cervical cancer screening, diagnostic, and treatment services. Uninsured and underinsured women are eligible for the program if they are at or below 250% Federal Poverty Level (FPL) and are between the ages of 40 to 64 for breast cancer screenings. In 2023, 273,989 women received NBCCEDP-funded breast cancer services, including mammograms, screening MRIs, clinical breast exams, and diagnostic services.
- The Breast and Cervical Cancer Prevention and Treatment Act (BCCPTA)—Passed in 2000, the BCCPTA gives states the option to extend Medicaid coverage to uninsured women under 65 who are diagnosed with breast or cervical cancer through NBCCEDP-funded screening programs. Although all states and D.C. provide full Medicaid benefits to women who receive breast cancer treatment through the NBCCEDP, eligibility requirements may vary by state. In 2001, the Native American Breast and Cervical Cancer Treatment Technical Amendment Act was passed to extend eligibility to American Indian and Alaska Native women who qualify for health services through a tribal organization or the Indian Health Service.