The Affordable Care Act and Insurance Coverage Changes by Sexual Orientation
Data Note
The Affordable Care Act (ACA) has provided millions of Americans with new access to insurance coverage, in some cases for the first time. While a significant body of research has explored how the law has affected different populations, limited information has been available on insurance coverage changes by sexual orientation, in part due to the dearth of available nationally representative data about lesbian, gay, bisexual, and transgender (LGBT) individuals and insurance status.1
This data note provides the most up to date nationally representative estimates of insurance coverage changes among self-identified lesbian, gay and bisexual adults (LGB) under the ACA. It compares survey responses of nonelderly adults using the Sample Adult component from the Centers for Disease Control and Prevention’s (CDC) National Health Interview Survey (NHIS), 2013 and 2016 cycles.2 We find that rates of uninsurance decreased significantly among LGB adults after the implementation of the ACA’s major coverage changes. There was also a significant increase in Medicaid coverage. We were unable to examine changes in private insurance coverage due to sample size limitations.
Background
Historically, lesbian, gay, and bisexual individuals have faced barriers in accessing healthcare.3 Challenges result from stigma and discrimination, inequality in the workplace, refusal of care, and denial of coverage related to sexual orientation or gender identity. Prior to the ACA, insurance companies could deny LGBT individuals insurance coverage, exclude certain services (e.g. those related to gender transition), or charge higher rates based on sexual orientation or gender identity. Issuers were also able to deny insurance coverage or charge higher rates to people with health conditions that disproportionally affect LGBT individuals such as HIV, mental illness, and substance use disorders.4
Under the ACA, insurers are no longer permitted to consider health status when setting rates or issuing coverage. Further, issuers are prohibited from discriminating on the basis of sexual orientation or gender identity in coverage subject to the Essential Health Benefits, including plans sold on the health insurance marketplaces. (The law and implementing regulations also include additional protections that prohibit discrimination based on sex, defined to include gender identity and sex stereotypes, in any health program receiving federal funds, including: Medicaid, Medicare, the marketplaces, and providers who receive federal funds. However, as part of an ongoing lawsuit, a federal court has issued an injunction halting enforcement of this provision’s protections around gender identity.5 )
In addition to non-discrimination protections, the ACA introduced two main coverage pathways. The first is the Medicaid expansion, which provides Medicaid coverage to eligible individuals below 138% of FPL, basing eligibility on income and residency status alone rather than categorical eligibility (e.g. requiring disability or pregnancy in addition to being low-income). As a result of a Supreme Court decision, Medicaid expansion is effectively a state option and to date, 33 states (including DC) have expanded their programs.6 Second, legal US residents are now able to purchase private coverage through insurance Marketplaces with subsidies available to most between 100% and 400% of the federal poverty level (FPL).
In order to assess changes in coverage among LGB individuals under the ACA, we analyzed data for non-elderly adults from the NHIS, a nationally representative survey conducted by CDC on health and health behaviors. We compared data from 2013, prior to the implementation of major ACA insurance expansions to 2016, after implementation. We were not able to examine coverage among transgender individuals as the NHIS instrument category does not include transgender as a stand-alone category.
Findings
Using the 2013 and 2016 NHIS cycles, we estimate that there were 4.8 million U.S. adults between the ages of 18-64 who identified as lesbian, gay or bisexual in 2013, and 5.5 million in 2016. Based on both cycles, we estimate that LGB individuals in this age group make up about 3% of the US population. This is similar to estimates found in other research.7 Uninsurance declined and Medicaid coverage increased significantly for this population after the implementation of the ACA, as follows. (We are unable provide private insurance due to sample size limitations.):
The Uninsured
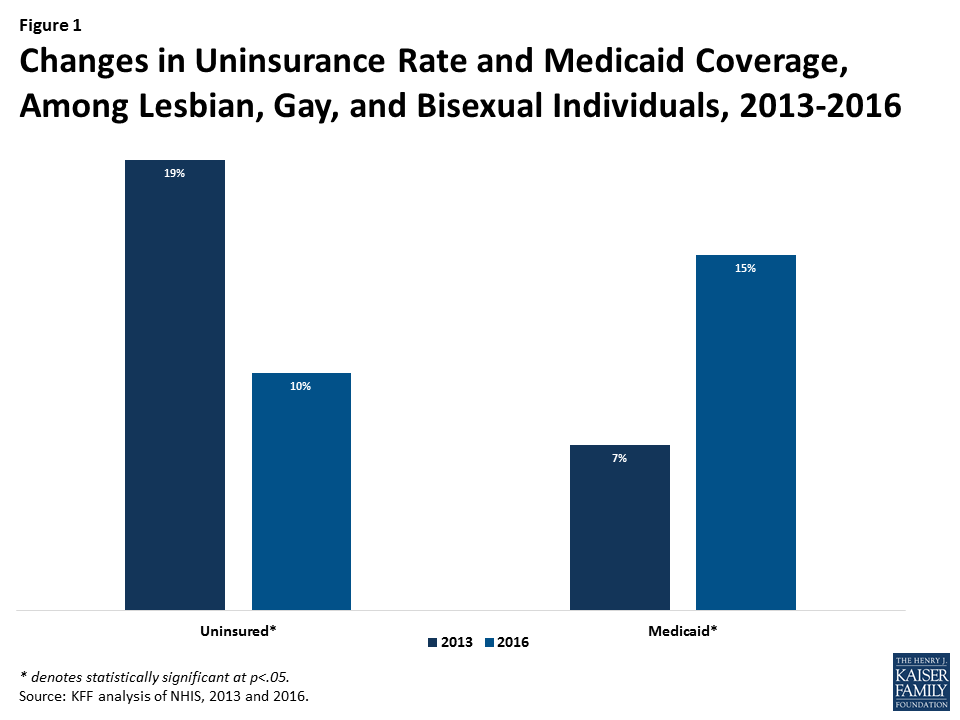
During the early years of ACA implementation, the rate of uninsurance among LGB individuals fell by almost half (from 19% in 2013 to 10% in 2016), representing an estimated 369,000 fewer uninsured LGB individuals in 2016 compared to 2013. The drop in the uninsurance rate experienced by LGB groups was similar to that seen among heterosexuals over this period.8
Medicaid
LGB individuals saw significant gains in Medicaid coverage between 2013 and 2016 (increasing from 7% to 15%), likely due to Medicaid expansion.9 This increase represents an estimated 511,000 more LGB individuals with Medicaid coverage in 2016 compared to 2013. Increases in Medicaid coverage over this period were not significantly different when comparing LGB individuals to heterosexual individuals.10
Discussion
The ACA has played a significant role in increasing insurance coverage and reducing the rate of uninsurance for people in the United States and many of these gains have translated to the LGB population. Under the ACA, LGB people experienced reductions in the uninsurance rate between 2013 and 2016. Gains in Medicaid coverage have driven this trend, though it is also likely that some uptick in private insurance coverage contributed to declines in the share uninsured as well. As the Administration, Congress, and states, continue to make changes to the health landscape, including to protections for LGBT individuals, it will be important to monitor these trends in future years.
Lindsey Dawson and Jennifer Kates are with the Kaiser Family Foundation. Anthony Damico is an independent consultant to the Kaiser Family Foundation.
Endnotes
- See Karpman M, Skopec L, and Long S. Urban Institute Health Policy Center. QuickTake: Uninsurance Rate Nearly Halved for Lesbian, Gay, and Bisexual Adults Since Mid-2013. 2015. Available at http://hrms.urban.org/quicktakes/Uninsurance-Rate-Nearly-Halved-for-Lesbian-Gay-and-Bisexual-Adults-since-Mid-2013.html and also Skopec L, and Long S. Data Watch: Lesbian, Gay, and Bisexual Adults Making Gains in Health Insurance and Access to Care. Health Affairs. 34(10):1769-1773, 2015. (survey driven analysis), Gonzales, G. and Henning-Smith, C. LGBT Health. The Affordable Care Act and Health Insurance Coverage for Lesbian, Gay, and Bisexual Adults: Analysis of the Behavioral Risk Factor Surveillance System. February 2017, 4(1): 62-67 (a point of time snapshot), Baker, K., Durso, L., and Cray. The Center for American Progress. A: Moving the Needle: The Impact of the Affordable Care Act on LGBT Communities. 2014. Available at https://cdn.americanprogress.org/wp-content/uploads/2014/11/LGBTandACA-report.pdf. (Limited to those below 400% FPL.), and Gates J. Gallup. In U.S., LGBT more likely than non-LGBT to be uninsured. 2014 Available from: http:// www.gallup.com/poll/175445/lgbtlikely-non-lgbt-uninsured.aspx ↩︎
- All estimates presented in this brief have a relative standard error (RSE) of less than 30%. For more detail regarding the NHIS questionnaire in 2013, see the relevant CDC publications at https://www.cdc.gov/nchs/data/series/sr_02/sr02_169.pdf and https://www.cdc.gov/nchs/data/nhsr/nhsr077.pdf. ↩︎
- Kates, J., et al. Kaiser Family Foundation. Health and Access to Care and Coverage for Lesbian, Gay, Bisexual, and Transgender Individuals in the U.S. 2016. Available at: https://modern.kff.org/disparities-policy/issue-brief/health-and-access-to-care-and-coverage-for-lesbian-gay-bisexual-and-transgender-individuals-in-the-u-s/ ↩︎
- Kates, J., et al. Kaiser Family Foundation. Health and Access to Care and Coverage for Lesbian, Gay, Bisexual, and Transgender Individuals in the U.S. 2016. Available at: https://modern.kff.org/disparities-policy/issue-brief/health-and-access-to-care-and-coverage-for-lesbian-gay-bisexual-and-transgender-individuals-in-the-u-s/ ↩︎
- At time of publication, HHS was reconsidering the final implementing rule that clarified these protections and had sent a draft proposed rule to the Department of Justice (a step forward in the rulemaking process). See: http://premiumtaxcredits.wikispaces.com/file/view/ Franciscan%20Alliance%20status%20report%208%204.pdf/616209859/Franciscan%20Alliance%20status%20report%208%204.pdf ↩︎
- Kaiser Family Foundation. State Health Facts. Status of State Action on the Medicaid Expansion Decision. Available at: https://modern.kff.org/health-reform/state-indicator/state-activity-around-expanding-medicaid-under-the-affordable-care-act/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D ↩︎
- See for example: G. Gates. Gallup News. In U.S., More Adults Identifying as LGBT. January 2017. Available at: http://news.gallup.com/poll/201731/lgbt-identification-rises.aspx; Ward, B., et al. CDC. National Health Statistics Reports. Sexual Orientation and Health Among U.S. Adults: National Health Interview Survey, 2013. No. 77. July 15, 2014. https://www.cdc.gov/nchs/data/nhsr/nhsr077.pdf ↩︎
- Kaiser Family Foundation Analysis of Centers for Disease Control and Prevention’s (CDC) National Health Interview Survey (NHIS), 2013 and 2016 cycles. (Data on heterosexual coverage not shown.) ↩︎
- Kaiser Family Foundation. State Health Facts. Status of State Action on the Medicaid Expansion Decision. (As of Jan. 16, 2018.) https://modern.kff.org/health-reform/state-indicator/state-activity-around-expanding-medicaid-under-the-affordable-care-act/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D ↩︎
- Kaiser Family Foundation Analysis of Centers for Disease Control and Prevention’s (CDC) National Health Interview Survey (NHIS), 2013 and 2016 cycles. (Data on heterosexual coverage not shown.) ↩︎