Historical Trends in U.S. Funding for Global Health
Key Findings
- The U.S. is the largest donor to global health in the world, and funding for global health has grown over time. To provide context for the release of the first, full budget request from the Biden administration, this brief provides an overview of trends in U.S. global health funding. It examines both regular as well as supplemental, or emergency, appropriations over time, changes in funding for major program areas, and trends in the distribution between bilateral and multilateral support.
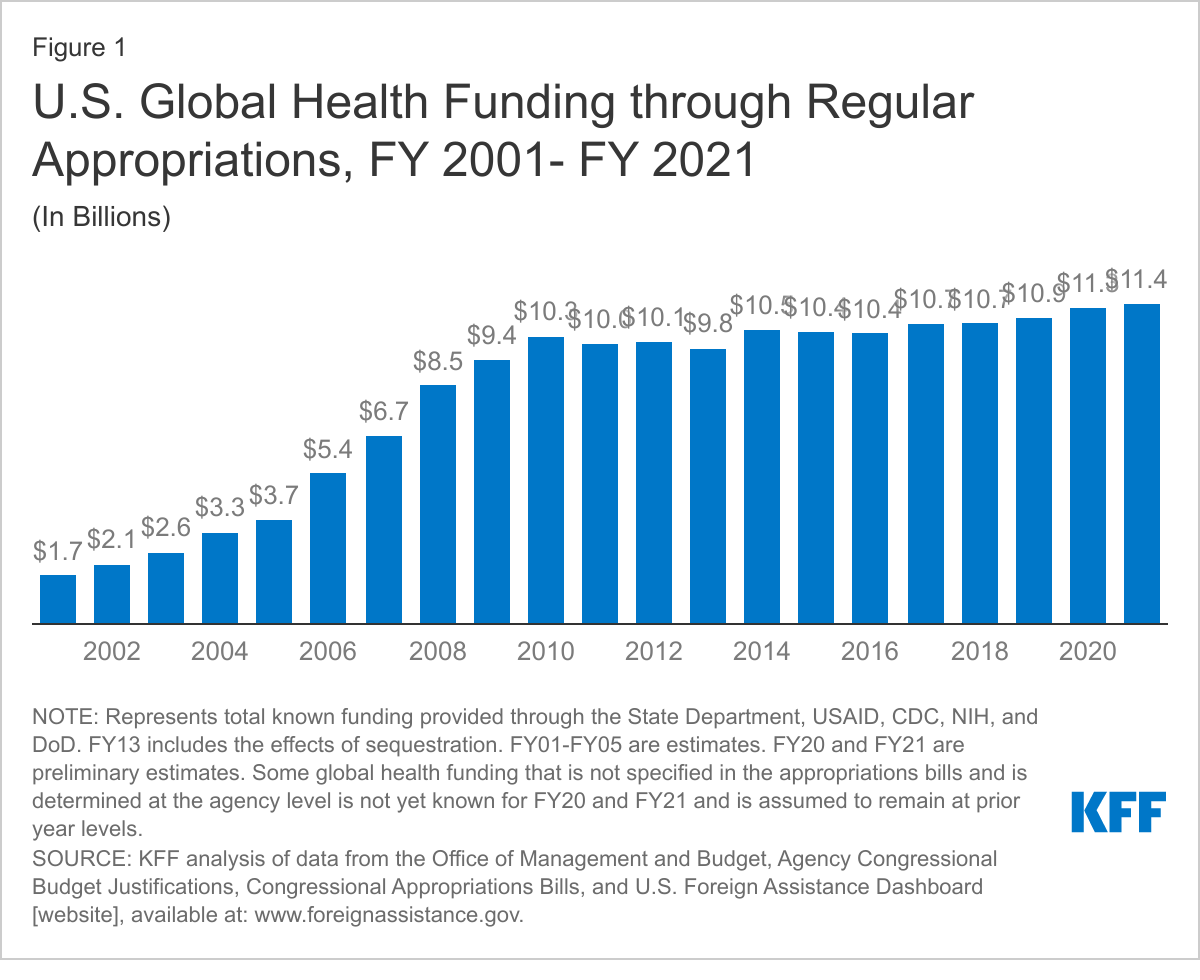
- U.S. funding for global health, through regular appropriations, has grown significantly over the past two decades, rising from $1.7 billion in FY 2001 to $11.4 billion in FY 2021, with the steepest increase occurring in the earlier decade. Most of the increase ($8.3 billion or 85%) was provided between FY 2001–FY 2011, a decade which marked the creation of PEPFAR, the Global Fund to Fight AIDS, Tuberculosis and Malaria, and the President’s Malaria Initiative.
- Since FY 2011, funding increases have been more modest. Between FY 2011 and 2021, funding rose by $1.4 billion, most of which has come in recent years. There were also fluctuations over the period, including some declines.
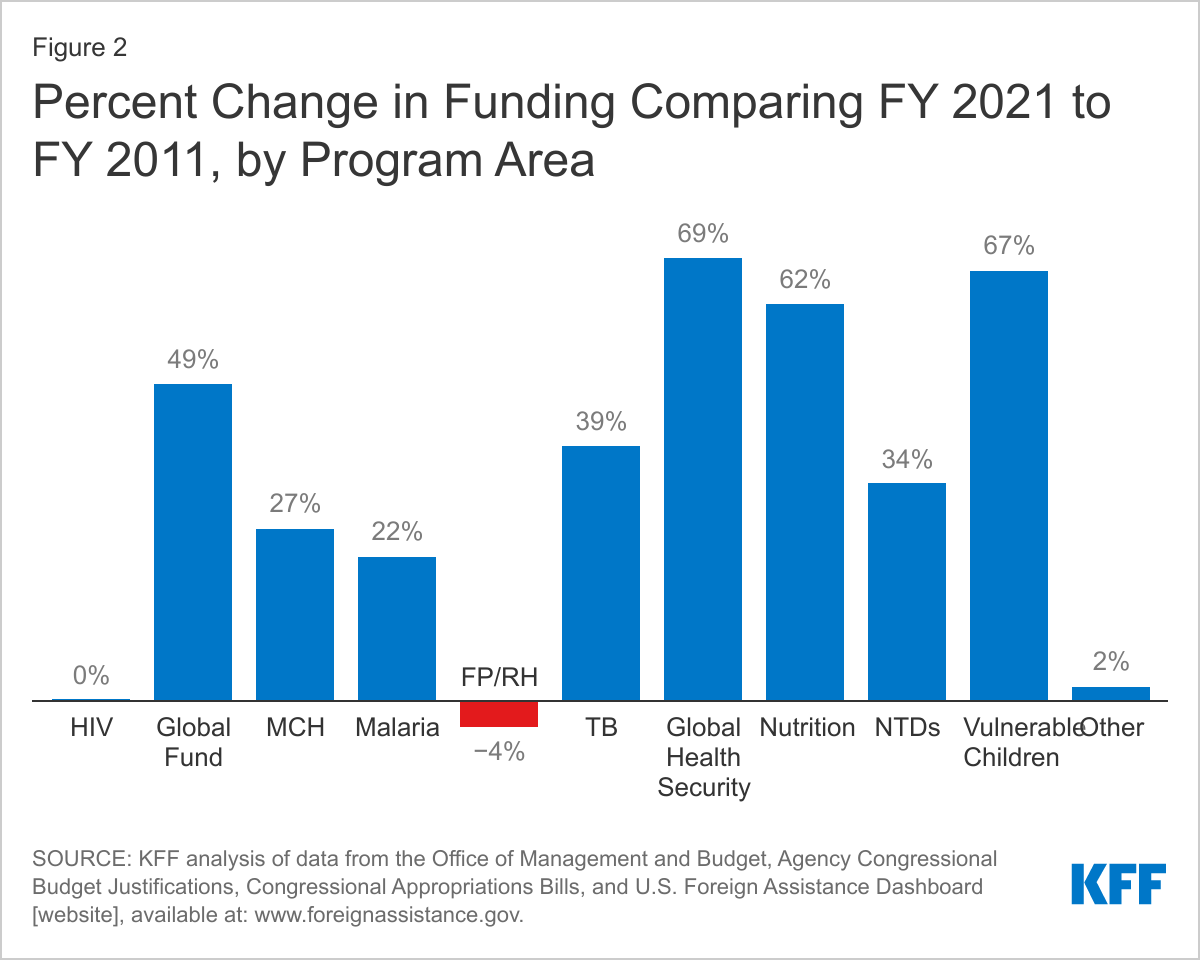
- Funding for most global health program areas has increased since FY 2011, particularly the Global Fund and global health security; funding was flat for PEPFAR and declined for family planning and reproductive health. All other program areas – tuberculosis, malaria, maternal and child health, nutrition, vulnerable children, and neglected tropical diseases – increased over the period.
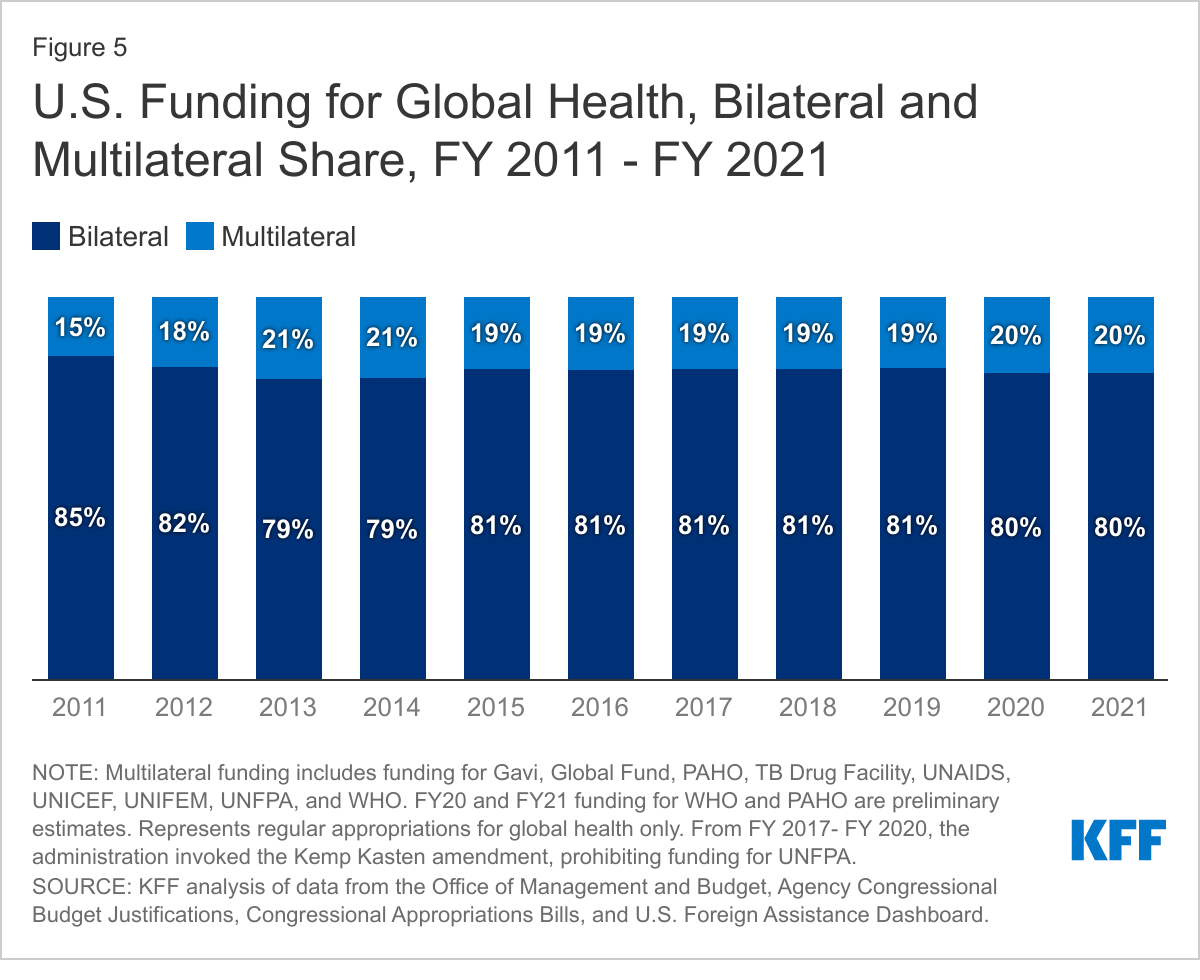
- Most global health funding has been provided bilaterally (ranging from 79-85% between FY 2011 and 2021), but the amount and share of funding for multilateral organizations has increased at a faster rate. Bilateral funding increased by 8% over the period while multilateral funding increased by 48%. Funding for multilateral organizations now makes up a fifth (20%) of the global health budget, up from 15% in FY 2011.
- Emergency funding, provided to respond to specific disease threats, has become a more prominent part of the global health budget in recent years. Since FY 2011, the U.S. has provided $11.8 billion in emergency funding for global health (9% of overall global health funding over the period). Most of this funding (90%) has been provided for COVID-19. Emergency funding has also been provided to respond to Ebola and Zika outbreaks.
Issue Brief
Introduction
On April 9, 2021, the Biden administration released an initial, discretionary FY 2022 budget request to Congress, kicking off the annual budget process (see Appendix). While a full budget request is expected at the end of May, the initial proposal includes $10 billion for global health activities (see Box 1), with a heavy focus on and significant increase for ($800 million above FY 2021 levels) global health security. Although Congress ultimately determines funding levels each year, the president’s budget request serves as an important indication of the administration’s priorities. The President’s first budget request is especially significant as it will provide an important signal for the administration’s broader approach to and priorities for U.S. global health engagement. Indeed, COVID-19 has elevated global health security in particular to the top of U.S. domestic and international agendas, and the President has already taken steps to bolster U.S. global health engagement, including rejoining the World Health Organization (WHO) and joining COVAX, the global mechanism to secure and deliver COVID-19 vaccines. To provide context for the release of the administration’s first, full budget request for FY 2022, this brief provides an overview of historical trends in U.S. global health funding, including changes in program-specific funding over time, the distribution between bilateral and multilateral support, and in the increasing use of emergency supplemental funding in response to outbreaks, which has become a more prominent part of the U.S. global health budget.
Box 1: Overview of U.S. Global Health Funding
Major program areas that receive U.S. global health funding: PEPFAR (HIV), Tuberculosis (TB), Malaria, Global Fund to Fight AIDS, Tuberculosis, and Malaria (Global Fund), Neglected Tropical Diseases (NTDs), Maternal and Child Health (MCH) (including polio), Nutrition, Family Planning and Reproductive Health (FP/RH), Vulnerable Children program, Global Health Security, Other Public Health Threats.
Departments and agencies that provide U.S. global health funding:The majority of U.S. government funding for global health is captured under the Global Health Programs (GHP) account at the U.S. Agency for International Development (USAID) and the Department of State (State). Additional funding for global health is provided through the Economic Support Fund (ESF), Development Assistance (DA), and Assistance for Europe, Eurasia and Central Asia (AEECA) accounts at USAID, the International Organizations and Programs (IO&P) and the Contributions to International Organizations (CIO) accounts at State, and through the Centers for Disease Control (CDC), National Institutes of Health (NIH), and Department of Defense (DoD). Congress specifies funding levels for global health areas (e.g. HIV, TB, MCH, GHS, etc.) under the GHP, CIO and IO&P accounts at USAID and State as well as for global health programs at CDC. Congress does not specify global health funding amounts under the ESF, AEECA, and DA accounts or at NIH and DoD and instead provides this authority to the administration; as a result, global health funding under these accounts and at NIH and DoD has fluctuated over the period.
Trends in Overall Funding for Global Health Through Regular Appropriations
Global health represents the largest share of U.S. international development aid,1 and funding for global health through regular appropriations has grown significantly since FY 2001. Between FY 2001, when funding was $1.7 billion, and FY 2021, funding for global health increased by almost $10 billion, most of which ($8.3 billion or 85%) was provided between FY 2001–FY 2011, marking the creation of PEPFAR, the Global Fund to Fight AIDS, Tuberculosis and Malaria, and the President’s Malaria Initiative. Funding increases slowed in the years after the global financial crisis that began in 2008, and even declined slightly in the early part of the next decade. While it somewhat recovered, increases over the past decade have been more modest, rising by $1.4 billion between FY 2011 and FY 2021, driven primarily by increases to the Global Fund and global health security.2 In FY 2021 U.S. funding for global health through regular appropriations totaled $11.4 billion, its highest level to date.3 Additional funding has also been provided through emergency, supplemental funding (see below).
Program Area Trends
While funding for most global health program areas increased over the last decade, funding for PEPFAR (bilateral HIV) remained flat and funding for family planning and reproductive health (FP/RH) declined; overall funding, as well as funding for all program areas, fluctuated over the period. The biggest increases were for the Global Fund (which represented the largest dollar amount increase) and global health security (which represented the largest percentage increase) (see Figure 2).
Key program area trends over the past decade include the following:
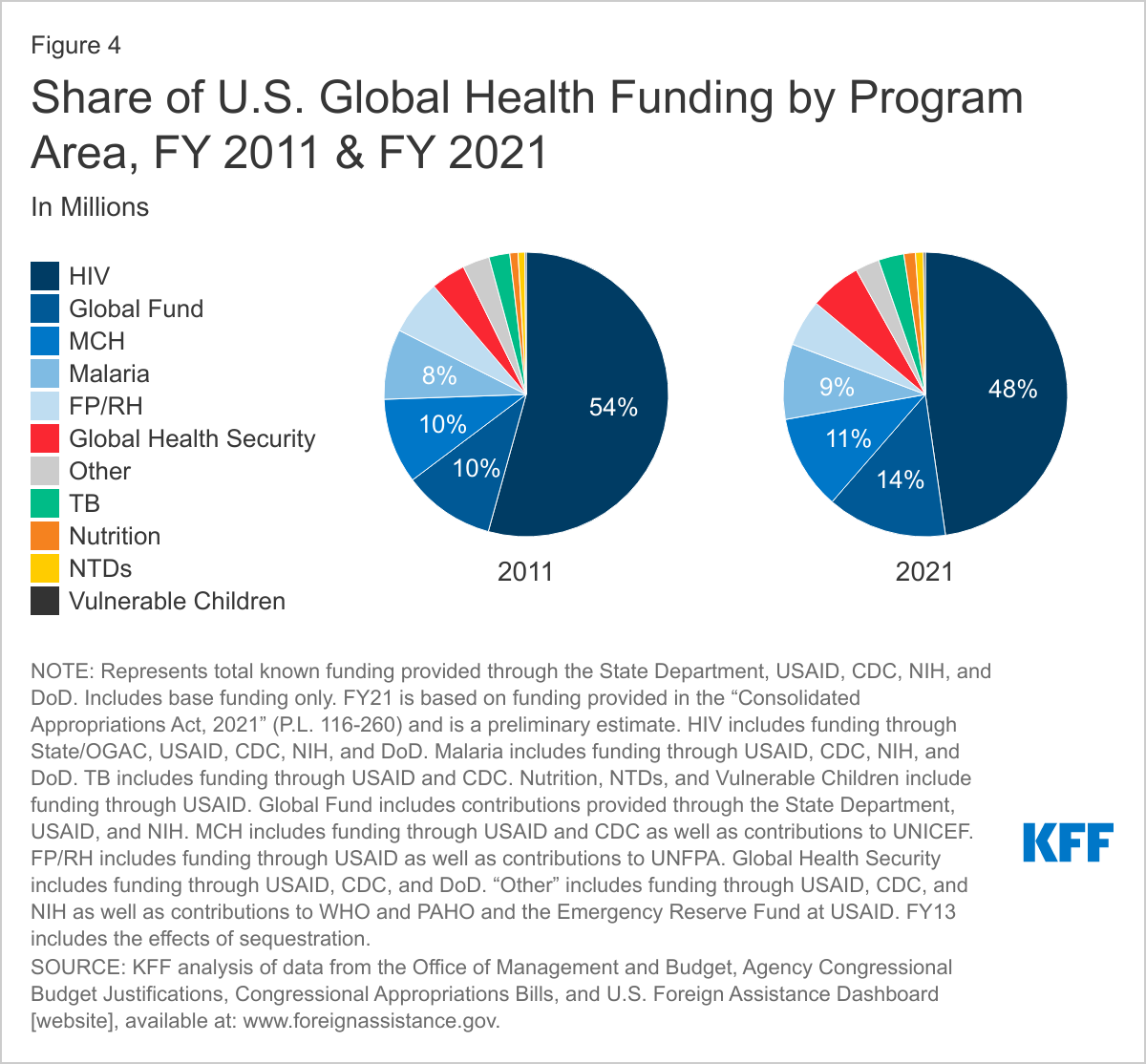
- PEPFAR (Bilateral HIV). PEPFAR funding has ranged between $4.7 billion and $5.5 billion since FY 2011, though current levels are about the same as funding a decade ago (see Figure 3). There was a significant dip in funding after FY 2012 (of more than $400 million), and funding did not rebound until FY 2019, where it has remained since. While funding for bilateral HIV programs has historically accounted for the largest share of the U.S. global health budget, its share has declined over time, dropping from 54% in FY 2011 to 48% in FY 2021 (see Figure 4). Bilateral HIV funding is provided through the GHP account at USAID and State, the ESF account at USAID, and through CDC, NIH, and DoD. Additional funding for PEPFAR was recently provided through emergency COVID-19 funding (see below).
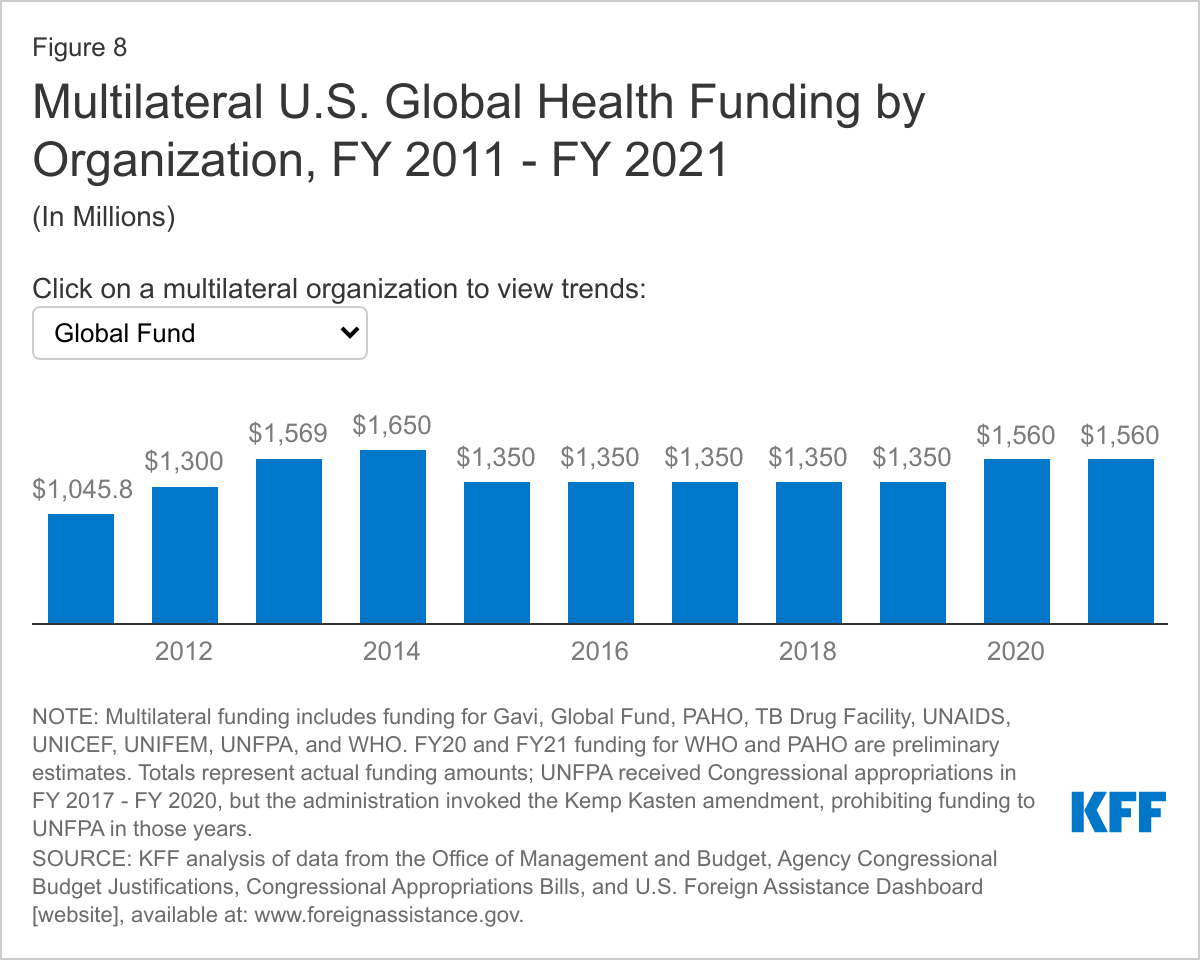
- The Global Fund. The U.S. has been the largest donor to the Global Fund since its inception. U.S. contributions to the Global Fund in FY 2021 ($1,560 million) were $514 million (49%) above the FY 2011 level ($1,046 million), the largest increase of any global health program, although funding fluctuated over the period (see Figure 2 and 3). The Global Fund has represented the second largest share of the U.S. global health budget, and that share has increased somewhat, from 10% to 14% over the period (see Figure 4). U.S. funding for the Global Fund is provided through the GHP account at State. In the past, some funding has also been channeled through NIH as well. Additional funding for the Global Fund was recently provided through emergency COVID-19 funding (see below).
- Maternal and Child Health (MCH). MCH funding, which includes funding for polio, Gavi, the Vaccine Alliance (Gavi), and the United Nations Children’s Fund (UNICEF), in FY 2021 was $261 million (27%) above FY 2011 level ($974 million), although there was fluctuation over the period (see Figures 2 and 3). Increases in funding are largely due to increases in funding for polio efforts and for Gavi. When polio and Gavi amounts are removed, other MCH funding in FY 2021 ($703 million) was $47 million (-6%) below the FY 2011 level ($751 million). MCH funding has accounted for the third largest share of the U.S. global health budget over the decade and is provided through the GHP, ESF, AEECA, and DA accounts at USAID, as well as through the State Department and CDC (see Figure 4). Additional funding for Gavi was recently provided through emergency COVID-19 funding (see below).
- Malaria. Global malaria funding, most of which is provided through the President’s Malaria Initiative, in FY 2021 was $179 million (22%) above the FY 2011 level ($800 million), with the largest increase occurring between FY 2016 and FY 2017 (see Figures 2 and 3) Funding for global malaria efforts has represented the fourth largest share of the U.S. global health budget and is provided through the GHP account at USAID, as well as through CDC, NIH, and DoD (see Figure 4).
- Family Planning and Reproductive Health (FP/RH). Funding for international FP/RH in FY 2021 ($608 million) was $25 million (-4%) below the FY 2011 level ($633 million), representing the only global health program area that decreased over the period (see Figure 2). FP/RH funding, which has represented the fifth largest share of the global health budget, fluctuated slightly during the earlier part of the decade and has remained flat at $608 million in recent years (see Figures 3 and 4). Funding is provided through the GHP, ESF, and AEECA accounts at USAID, as well as through contributions to UNFPA provided through the State Department. From FY 2017- FY 2020, the Trump administration invoked the Kemp-Kasten amendment, withholding funding for UNFPA and reallocating it to USAID’s family planning, maternal, and reproductive health activities (see the KFF Kemp-Kasten explainer).
- Global Health Security. Global health security funding in FY 2021 ($670 million) was $273 million (69%) above the FY 2011 level ($397 million), representing the largest percentage increase compared to all other program areas (see Figure 2). Despite these overall increases, there was some fluctuation over the decade (see Figure 3). Global health security has represented the sixth largest share of the U.S. global health budget, and that share has increased somewhat (from 4% in FY 2011 to 6% in FY 2021). Funding is provided through the GHP and ESF accounts at USAID, as well as through CDC and DoD. Much of the growth in global health security funding occurred in recent years in response to specific disease outbreaks, leading to more attention to pandemic preparedness and global health security (see later section on emergency supplemental funding for more details on funding for Ebola, Zika, and COVID-19).
- Tuberculosis (TB). Global TB funding in FY 2021 ($332 million) was $94 million (39%) above the FY 2011 level ($238 million) (see Figure 2). Most of this growth has occurred in recent years (see Figure 3). Funding is provided through the GHP and ESF accounts at USAID, as well as through CDC.
- Nutrition. Global nutrition funding in FY 2021 ($150 million) was $57 million (62%) above the FY 2011 level ($93 million), with much of the increase occurring in the earlier part of the decade and flattening in recent years (see Figures 2 and 3). Funding is provided through the GHP, ESF, and DA accounts at USAID.
- Neglected Tropical Diseases (NTDs). Global NTD funding in FY 2021 ($103 million) was $26 million (34%) above the FY 2011 level ($77 million), with much of the increase occurring earlier in the decade and flattening in recent years (see Figures 2 and 3). Funding is provided through the GHP account at USAID.
- Vulnerable Children. Funding for the vulnerable children program, the smallest global health program, in FY 2021 ($25 million) was $10 million (67%) above the FY 2011 level ($15 million), with funding growing steadily throughout the period (see Figures 2 and 3). Funding is provided through the GHP account at USAID.
- Other. Funding for global health is also provided to the World Health Organization (WHO) and Pan American Health Organization (PAHO) (see more details for these organizations in the multilateral funding section below), as well as the Fogarty International Center (FIC) at NIH and an “Emergency Reserve Fund” at USAID, which was created in FY 2017.4 Together, this funding increased slightly when comparing FY 2021 to FY 2011 levels (see Figures 2 and 3).

Trends in Bilateral vs Multilateral Funding
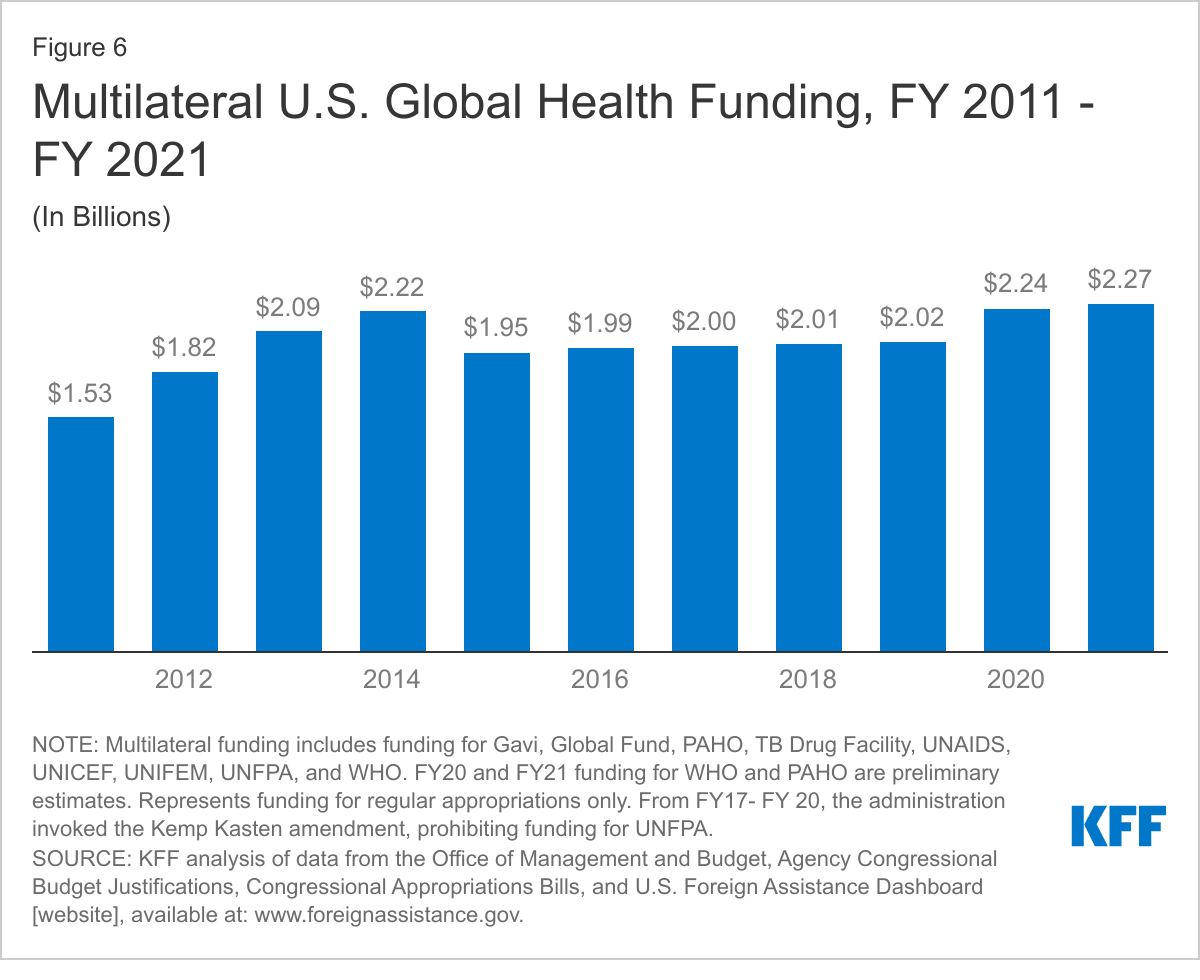
U.S. global health funding is provided through two types of channels: bilateral (i.e. country-to-country) and multilateral (i.e. multi-country, pooled support directed through an international organization; see Box 2). While the vast majority of U.S. funding for global health is provided bilaterally (ranging from 79-85% of the global health budget from FY 2011 to FY 2021), both the amount and share of funding for multilateral organizations has increased at a faster rate. Bilateral funding increased by 8% over the period while multilateral funding increased by 48%. The multilateral share, which increased over the decade (and experienced fluctuations throughout the period), now represents about a fifth (20%) of U.S. global health funding in FY 2021, up from 15% in FY 2011 (see Figure 5 and 6).5
Box 2: Multilateral health organizations supported by the U.S., including FY 2021 funding amounts though regular appropriations
- Gavi, the Vaccine Alliance (Gavi): $290 million
- Global Fund to Fight AIDS, Tuberculosis and Malaria (Global Fund): $1,560 million
- Joint United Nations Programme on HIV/AIDS (UNAIDS): $45 million
- Pan-American Health Organization (PAHO): $65.8 million*
- TB Global Drug Facility (at Stop TB Partnership): $15 million
- United Nations Children’s Fund (UNICEF): $139 million
- United Nations Family Planning Agency (UNFPA): $32.5 million
- World Health Organization (WHO): $122.7 million*
* Funding amounts for PAHO and WHO are not yet known and for comparison purposes, are assumed to remain at the FY 2020 level.
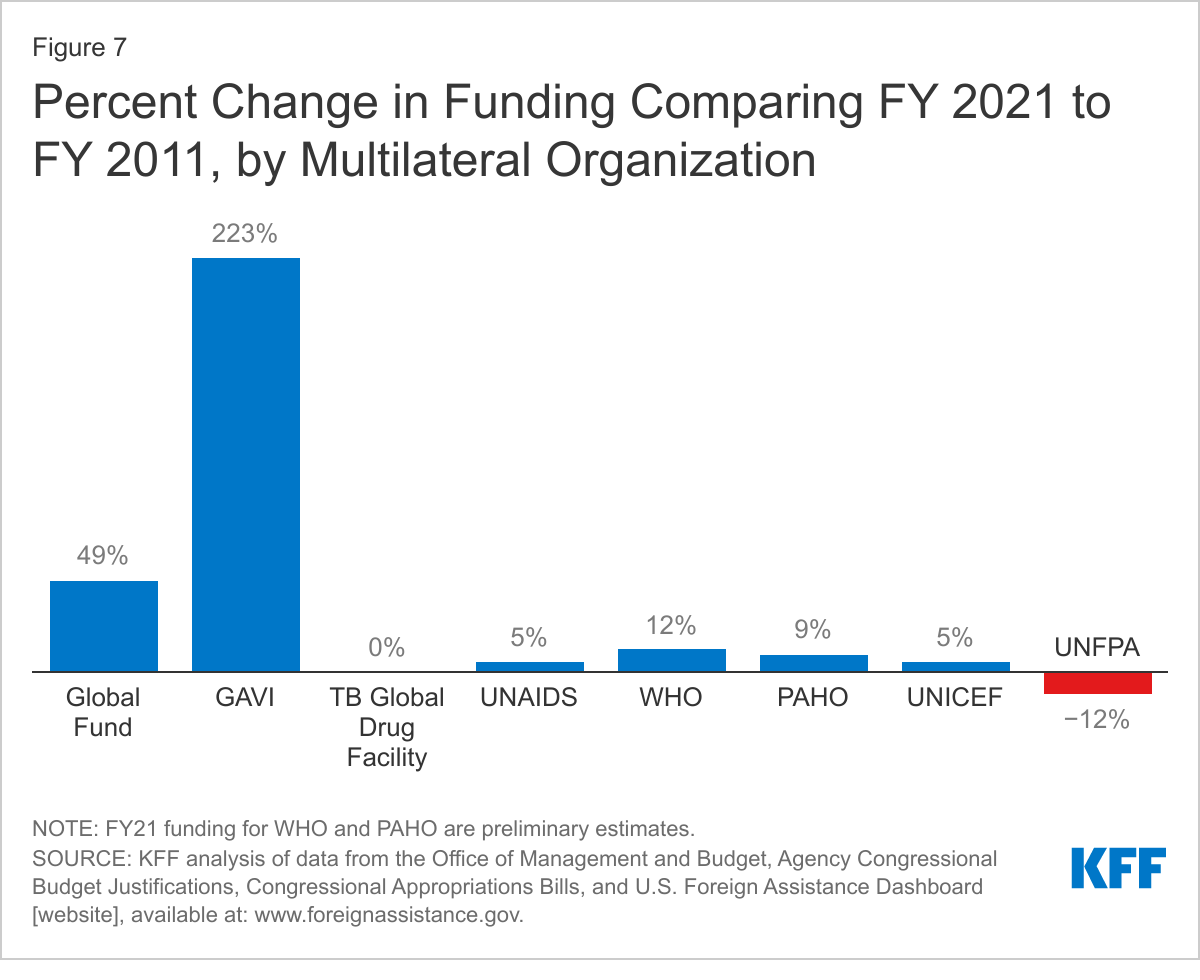
Funding for most multilateral organizations increased in FY 2021 compared to FY 2011 levels, with the exception of the TB Global Drug Facility, which remained flat, and UNFPA, which decreased overall and did not receive funding in some years due to the Kemp Kasten amendment (see Figure 7). 6 While Gavi increased by the greatest percentage amount (223%) compared to other multilateral organizations, the Global Fund increased by the largest dollar amount ($514 million compared to Gavi’s $200 million increase). The Global Fund has represented 67-75% of multilateral funding for global health each year over the past decade. Funding for the Global Fund, while rising overall, fluctuated over the past decade, in contrast to all other multilateral organizations, which either increased or remained essentially flat over the period, except for UNFPA (see Figure 8).
Trends in U.S. Emergency Supplemental Funding
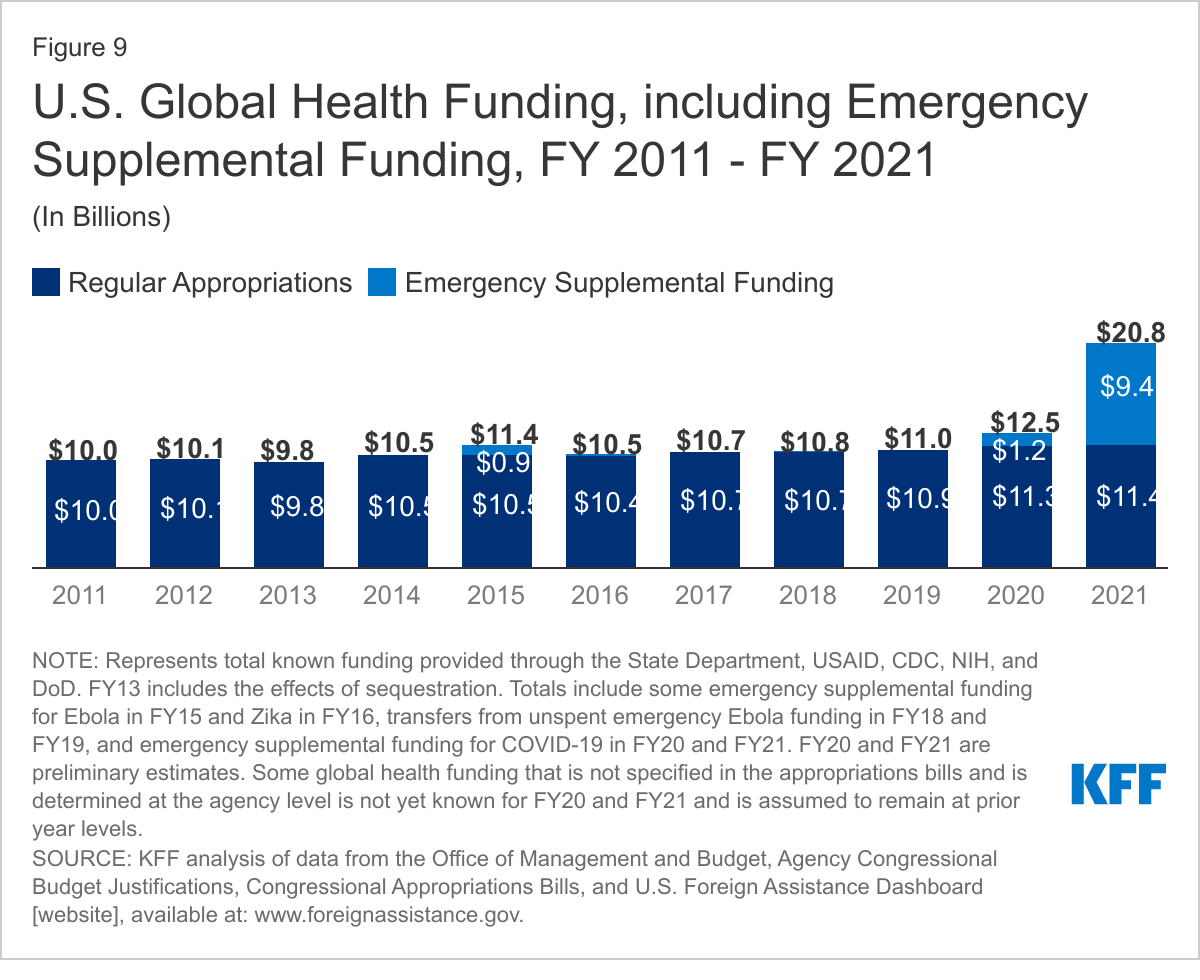
In addition to global health funding provided through regular appropriations, emergency funding, appropriated in response to outbreaks, has become a more prominent part of the budget. Since FY 2011, the U.S. has provided $11.8 billion in emergency supplemental funding (representing 9% of overall global health funding over the period) to address outbreaks, almost all of which (90%) has been provided in response to COVID-19 (see Figure 9). Global health funding through emergency appropriations over the past decade includes:
- $909 million in FY 2015 to address Ebola.7
- $145.5 million in FY 2016 to address Zika.8
- $10.6 billion to address COVID-19 ($1.2 billion in FY 2020 and $9.4 billion in FY 2021).9 Of this, $4 billion was provided to COVAX, $250 million to PEPFAR, and $3.5 billion to the Global Fund.
Looking Ahead
The U.S. government is the largest donor to global health in the world.10 As this analysis demonstrates, U.S. funding for global health has grown significantly over time, marking the start of major new programs. However, the vast majority of that growth occurred from FY 2001 to 2010, with the creation of PEPFAR. In the last decade, funding for most program areas within the global health budget has increased, but only quite modestly. In addition, the U.S. has provided a significant amount of emergency supplemental funding on top of regular appropriations for global health to respond to disease outbreaks in recent years. While the Biden administration has already taken steps to bolster U.S. global health engagement, largely in response to the COVID-19 pandemic, the forthcoming release of his first, full budget request for FY 2022 will provide an important window into the administration’s further priorities for global health.
Appendix
U.S. Annual Budget Process11
The U.S. annual budget process starts when the President submits a detailed budget request to Congress for the upcoming fiscal year, which begins on October 1 and ends on September 30. Signaling the administration’s priorities, the request, which is developed through an interactive process between federal agencies and the President’s Office of Management and Budget (OMB), includes recommendations to Congress on funding levels for federal programs. The request is usually submitted by the first Monday in February, but sometimes the submission is delayed, particularly when a new administration takes office, as is the case today. In addition, when a new administration takes office, sometimes the President submits an initial, abbreviated budget, as was done this year (this was also done at the beginning of both the Obama and Trump administrations), and a fuller more detailed budget later. Once the President submits the detailed budget request to Congress, the House and Senate develop a budget plan, or a “budget resolution,” through their budget committees. After both the House and Senate pass these budget resolutions, a process that generally takes place in March or April, the bills go to the floor, where a conference between the House and Senate resolves any differences within the budget resolution and an agreement between the two houses is made. The budget resolution serves as a blueprint for the actual appropriations process, where House and Senate Appropriations committees set spending totals for federal agencies and programs. Once each appropriations committee sets these amounts and allocations, the bills are considered by the House and Senate, where a conference agreement, which resolves any differences between the two bills, is made. Once a conference bill is passed by both the House and Senate, it goes to the President and is signed into law.
Endnotes
- KFF analysis of OECD DAC CRS database, May 2021. ↩︎
- In FY 2013, sequestration occurred, resulting in cross the board cuts in funding to all global health program areas. ↩︎
- Represents U.S. regular appropriations only. ↩︎
- The Emergency Reserve Fund at USAID was created in the FY 2017 Omnibus bill to respond to contagious infectious disease outbreaks and would be made available if there is an “emerging health threat that poses severe threats to human health.” The only year the Emergency Reserve Fund received funding through regular appropriations was in FY 2017. ↩︎
- U.S. multilateral funding includes support to the Pan-American Health Organization (PAHO), Joint United Nations Programme on HIV/AIDS (UNAIDS), United Nations Children’s Fund (UNICEF), United Nations Family Planning Agency (UNFPA), World Health Organization (WHO), Gavi, the Vaccine Alliance, the Global Fund to Fight AIDS, Tuberculosis and Malaria, and the TB Global Drug Facility. ↩︎
- While Congress provided funding for UNFPA each year between FY 2011 and FY 2021, President Trump invoked the Kemp-Kasten amendment to withhold funding from the organization (see KFF explainer on UNFPA funding & Kemp-Kasten amendment). President Biden has directed the U.S. Secretary of State to take the necessary steps to resume funding to UNFPA. ↩︎
- KFF. The U.S. Response to Ebola: Status of the FY2015 Emergency Ebola Appropriation; December 2015. ↩︎
- KFF. The Status of Funding for Zika: The President’s Request, Congressional Proposals, & Final Funding; October 2016. ↩︎
- KFF. Global Funding Across U.S. COVID-19 Supplemental Funding Bills; March 2021. ↩︎
- KFF. Donor Funding For Health in Low-& Middle-Income Countries, 2002-2013. November 2015. https://modern.kff.org/global-health-policy/report/donor-funding-for-health-in-low-middle-income-countries-2002-2013/. ↩︎
- U.S. government, “Budget of the U.S. Government” webpage, October 2019. Accessed: https://www.usa.gov/budget. Congressional Research Service, “Introduction to the Federal Budget Process”, February 26, 2020. Center on Budget and Policy Priorities, “Policy Basics: Introduction to the Federal Budget Process” webpage, April 2020. Accessed: https://www.cbpp.org/research/introduction-to-the-federal-budget-process ↩︎