How Present-Day Health Disparities for Black People Are Linked to Past Policies and Events
Today’s health and health care disparities are rooted in a long history of U.S. policies and events and reflect the ongoing impacts of racism at multiple levels, including in systems, structures, policies, and interpersonal interactions. Understanding this past and how it shapes present-day disparities can help inform and guide efforts to address them. It also is important to recognize the resilience of marginalized people in the face of these challenges and disparities and to consider how to build on their strengths by prioritizing community engagement and leadership to mitigate disparities and improve overall health and well-being. This brief examines how past policies and events are linked to present-day disparities among Black people in health care and health outcomes. It is based on KFF’s interactive timeline of How History Has Shaped Racial and Ethnic Health Disparities and KFF’s 2023 Racism, Discrimination, and Health Survey.
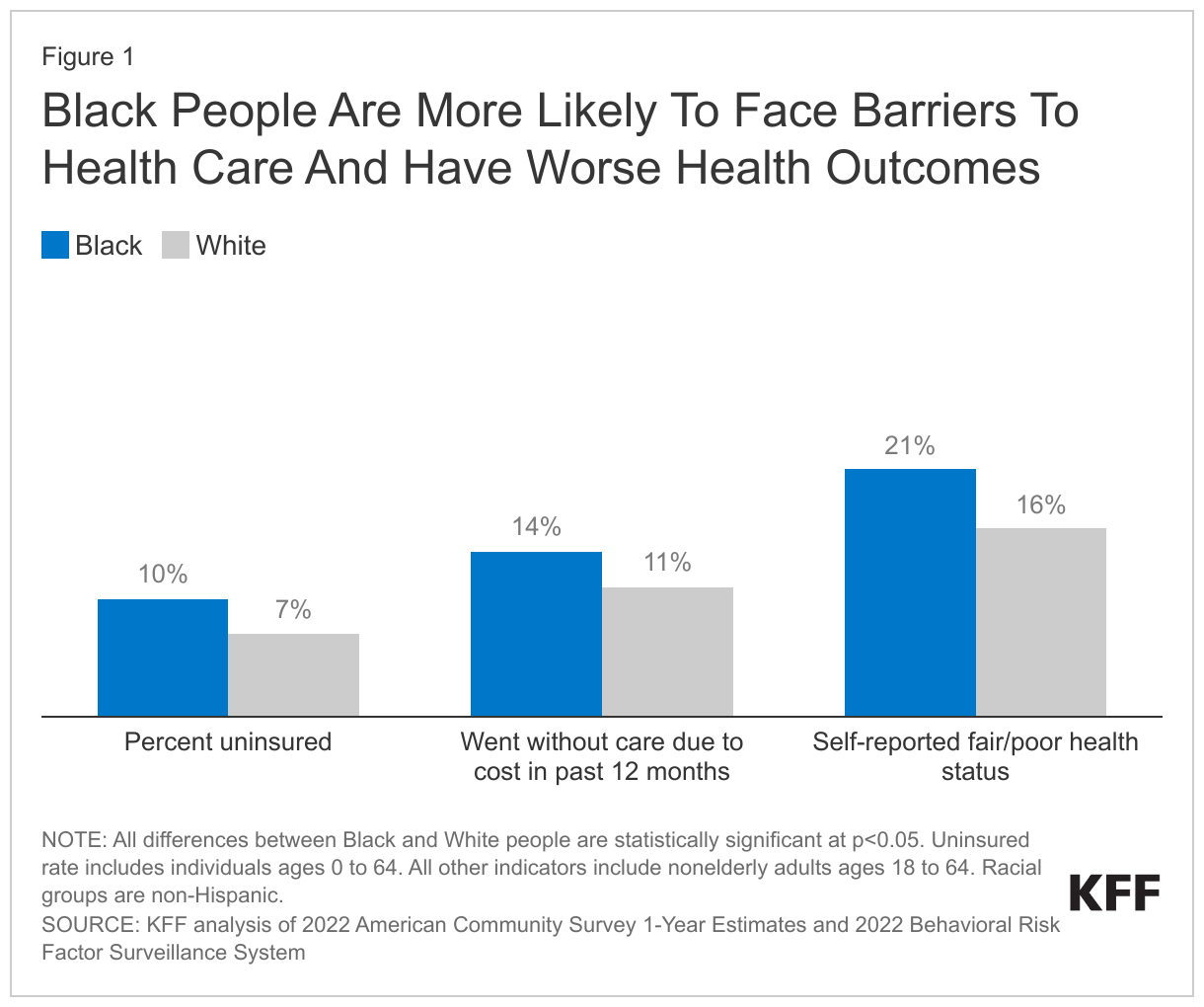
Today, Black people face persistent disparities in health care and health outcomes. These include higher uninsured rates, being more likely to go without care due to cost, and worse reported health status (Figure 1). Their life expectancy is nearly five years shorter compared to White people (72.8 years vs. 77.5 years). Black infants have a more than two times higher infant mortality rate than White infants (10.6 per 1,000 v. 4.4 per 1,000 as of 2021), and Black people are nearly three times more likely than White people to die due to pregnancy-related reasons (39.9 vs. 14.1 per 100,000 live births between 2017-2019).
Health and health care disparities faced by Black people today are rooted in and reflect historic racist and discriminatory practices and beliefs. Race is a social construct and there are no biologic differences by race. However, many historic policies and events were rooted in since disproven beliefs about biologic differences by race and white supremacy. These inaccurate beliefs contributed to false ideas, such as Black people feeling less pain than White people, and to historic abuses and mistreatment of Black people by the medical system. For example, in the 1800s doctors experimented on enslaved Black women to develop new surgical techniques, low-income women of color were subjected to forced sterilization during the early 1900s, and the federal government left poor Black men untreated for syphilis to study the disease progression under the infamous 40-year U.S. Public Health Service Untreated Syphilis Study at Tuskegee that began in 1932.
Although science has since disproven these theories, these beliefs continue to permeate the U.S. health care system today. As recently as 2016, a study found continued widespread beliefs among White medical students, residents, and laypeople in biologic differences between Black and White people, including believing that Black people have thicker skin than White people or that their blood coagulates more quickly. Race also continues to play a role in medical education and clinical decision making through provider attitudes and biases, disease stereotyping and nomenclature, and as part of clinical algorithms, tools, and treatment guidelines.
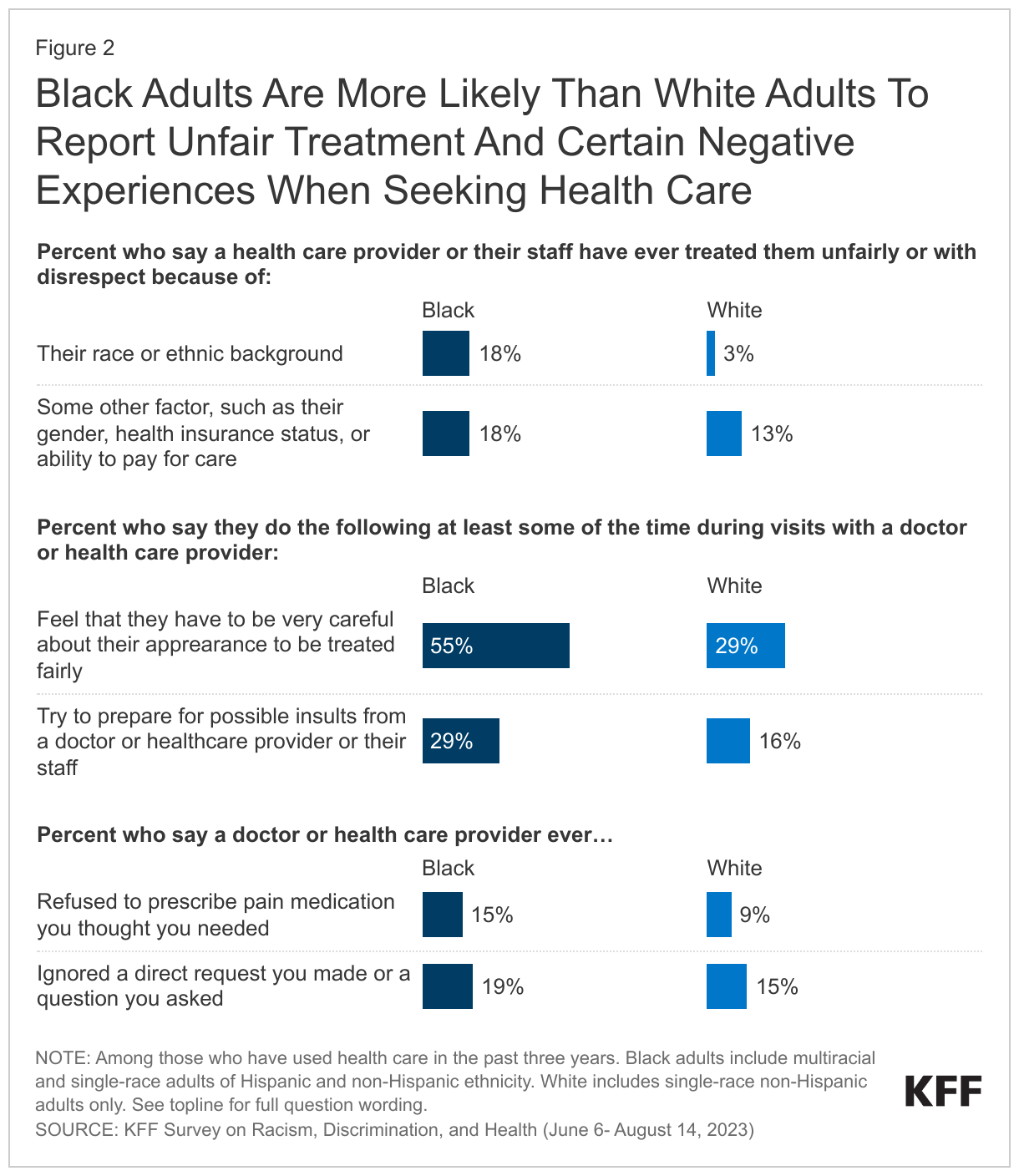
This history also continues to be reflected in people’s experiences seeking health care. A 2023 KFF survey found that Black adults are more likely than their White peers to say they were treated unfairly or with disrespect by a health care provider due to their race and ethnicity and to report certain negative experiences, including being refused pain medication they thought they needed or having a request or question ignored (Figure 2). Over half of Black adults say they feel they must be very careful about their appearance to be treated fairly during health care visits, and roughly three in ten say they prepare for possible insults from providers or staff during health care visits. Reflecting these experiences, Black adults are more likely than White adults to view racism as a major problem in health care and less likely to say they trust providers to do what is right for them and their community, although the majority still trust doctors and health care providers to do what is right at least most of the time.
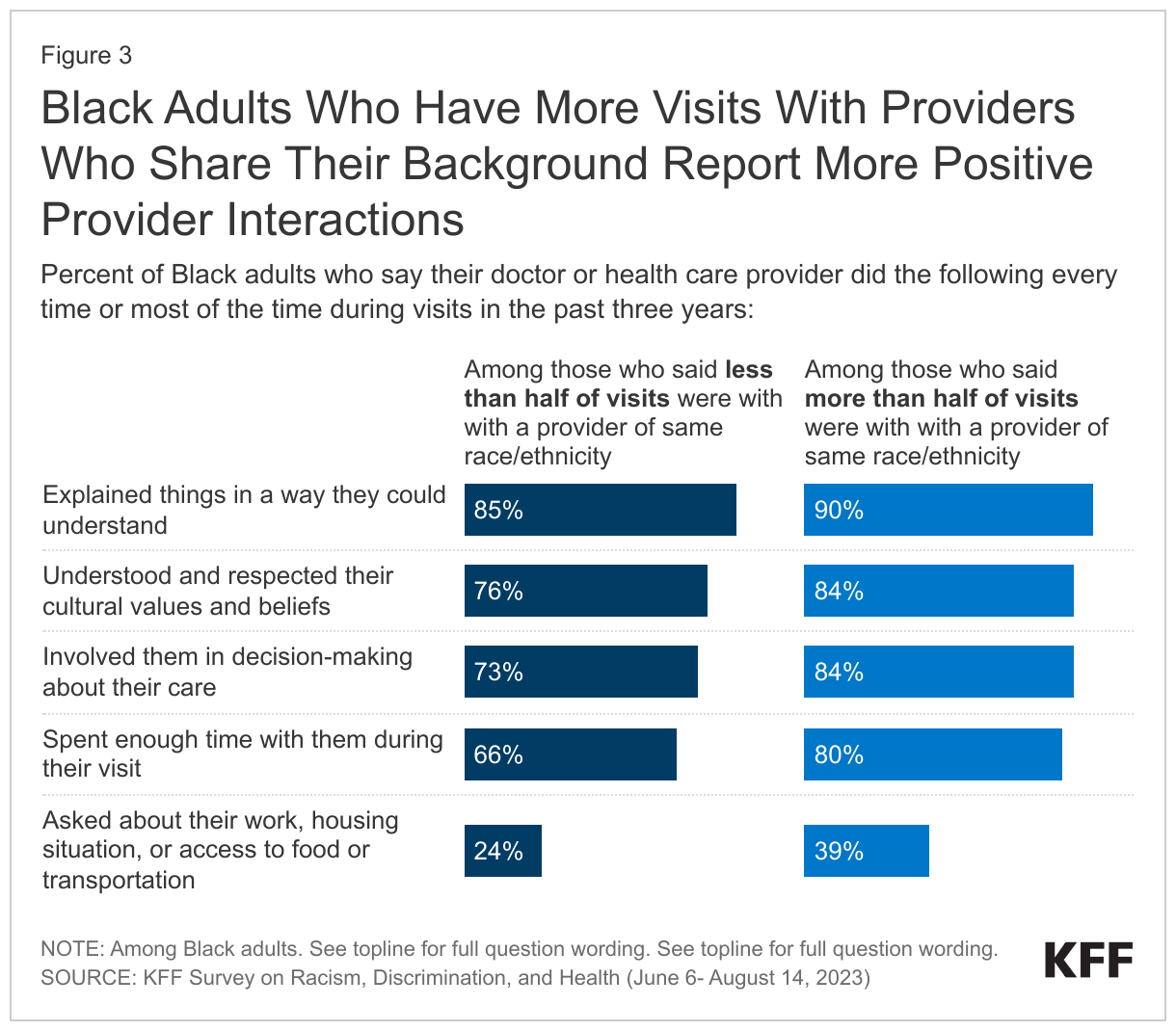
Research suggests that having a more diverse health workforce may help to address some of these challenges. KFF 2023 survey data show that Black adults who have more visits with providers who share their racial or ethnic background report more positive provider interactions (Figure 3). They also are more likely to trust doctors and other health care providers to do what is right for them and their community all or most of the time. Other research suggests that patient and provider racial concordance may contribute to improved health care use and health outcomes including lower emergency department use, reductions in racial disparities in mortality for Black infants, and increased visits for preventative care and treatment. However, Black adults are less likely than White adults to have most of their visits with a provider who has a shared background due to underrepresentation in the health care workforce.
The lack of diversity in the health care workforce today is rooted in historic actions. Prior to desegregation of public education, colleges and universities were established to educate Black students, and, by the late 19th century, there were seven medical colleges focused on training Black doctors. In 1910, the Flexner report, a study funded by the American Medical Association and the Carnegie Foundation to assess the state of medical education in the U.S. and Canada, was issued. The report recommended closing most of the historically Black medical schools, resulting in just two surviving—Meharry Medical College and Howard University. The number of Black physicians declined in the wake of these closures, and despite actions in more recent years to increase diversity of medical students, Black physicians remain underrepresented relative to their share of the population. The 2023 Supreme Court ruling against the use of affirmative action policies in higher education could exacerbate this issue, with experts concerned that the ruling will erode progress in diversifying the health care workforce.
Beyond these experiences within the health care system, Black people face an array of underlying structural inequities in social and economic factors that are major drivers of health. One of the most significant factors is ongoing residential segregation. A large share of the Black population lives in urban areas that have less access to resources that support health and that pose more exposure to health risks. Today’s residential segregation reflects past policies—in particular, redlining. Under legislation passed in the 1930s, residential neighborhoods were graded based on their mortgage risk, with higher risk neighborhoods marked in red—the origin of the phrase “redlining.” One of the factors that determined this grading was the racial make-up of the community, with Black neighborhoods more likely to be redlined. This made it difficult for people living in and near Black neighborhoods to access mortgage loans, and at the same time Black families were blocked from buying homes in newly developing suburbs. While the Fair Housing Act passed in the 1960s eventually prohibited housing discrimination, by then many Black families were priced out of suburban neighborhoods due to rising housing prices.
Today’s housing patterns continue to reflect these past discriminatory policies and leave Black people facing increased health risks. As a result of ongoing residential segregation and disinvestment into areas where Black people are more likely to live, they are more likely to live in areas that have more limited educational and employment opportunities, more limited access to healthy food options, less access to green space, and more limited transportation options, which in turn make it more difficult to access health coverage and care and pursue healthy activities. Moreover, many of these areas pose increased environmental and climate-related health risks, including increased exposure to extreme heat, lead, pollution, and toxic or hazardous materials.
Looking ahead, Black people could disproportionately benefit from new medical advancements given higher rates of many health conditions, but they face increased barriers to accessing them. One contributing factor to this disparity is underrepresentation in clinical trials. This underrepresentation reflects structural access barriers such as more limited access to trials sites, less access to transportation or technology, and limited eligibility for trials, if being uninsured or having an underlying condition excludes individuals from participation. They may also have less knowledge of trials because physicians are less likely to discuss them with patients of color and/or have concerns or reluctance about participating in them due to the medical system’s historic abuse, and mistreatment of Black people. Black people also face disparities in accessing new drugs and therapies when they come to market. New drugs often have high out of pocket costs, which may create more financial barriers for Black people due to underlying inequities in coverage and income. Biases in clinical decision-making processes and limitations in access to providers may also inhibit access.
As clinical algorithms and artificial intelligence are increasingly used to guide clinical care and treatment decisions in health care, it will be important to assess how they may impact disparities. Algorithms can lead to biases in treatment. For example, some have historically incorporated race as a factor in ways that contribute to disparities in treatment. One of the most well-known examples of this practice is the use of different measures to test kidney function for Black patients; a practice which is beginning to be phased out at many institutions. Algorithms may also result in biased treatment if they are built on underlying data that are biased or that are not representative of a diverse population. However, there is the opportunity for carefully designed algorithms to reduce bias in treatment and care.
