Health and Health Care in the U.S.-Mexico Border Region
Introduction
The four states (Arizona, California, New Mexico, and Texas) along the U.S.-Mexico border are home to over 78 million people of whom 8 million live in 44 counties that form the border area and border activity is at an all-time high.1 ,2 ,3 This year, there have been over two million encounters at the U.S.-Mexico border, which is 24% higher than the number of encounters last year. Although migrants and asylum seekers generally have short stays in border communities, this increased activity is leading to growing demands on border processing capacity and border communities that already face health and socioeconomic challenges and to some state governors busing migrants to other states.4 ,5 ,6 . Understanding of who lives in the region and their experiences, including their health and access to health care, may help inform efforts to address their needs.
Overall, people living in the four border states generally are more likely to be Hispanic and noncitizen immigrants compared to those in other parts of the country. They also are generally more likely to be poor, and uninsured.7 This analysis further examines differences between and within border states in sociodemographic characteristics, health coverage and access to care, as well as health outcomes of people living there. It is based on KFF’s analysis of county-level data from the American Community Survey (ACS) five-year data tables, the Health Resources and Services Administration’s Area Health Resource Files (AHRF), the Centers for Disease Control and Prevention’s (CDC) WONDER database, and the Behavioral Risk Factors Surveillance System (BRFSS). Aside from 2020 mortality data from CDC, the most recent reliable available county-level data from these sources are from 2019. All differences described between border and non-border counties and between states in the text are statistically significant at the p<0.05 level. The data included in this brief are from the two years preceding the influx at the U.S.-Mexico border to provide context for the situation in the border region before the recent increase in immigration activity.
The findings show that, across many of the measures examined, Texas fared worse compared to the other border states. Moreover, within Texas, individuals in border counties faced increased challenges compared to those in non-border counties, with particularly low levels of educational attainment and income, higher shares of households with limited English proficiency (LEP) and no computer access, higher uninsured rates, and more limited access to providers. In the other border states, there are smaller differences in these measures between people living in border vs. non-border counties. In contrast to the other border states, Texas has not implemented the Affordable Care Act (ACA) Medicaid expansion to adults, contributing to lower rates of Medicaid coverage and higher uninsured rates compared with the other states, especially in border counties.
While immigration remains a contentious political issue, these findings highlight the potential benefits of providing resources and support to the border region to meet the needs of the growing number of migrants and asylum seekers in the area. Better preparedness, more job opportunities, and a greater allocation of resources to help migrants assimilate in the community may be helpful not only in improving socioeconomic and health outcomes and reducing disparities in border areas, but in improving the economy overall, particularly in these border communities.8 Policies that increase opportunities for newly arriving migrants to work, such as reducing the wait time for applying for work authorization, could also reduce overcrowding at migrant shelters.9 Although such policies could increase competition for jobs, research has found that immigrants and U.S.-born citizens in the low-skilled workforce usually fill different types of jobs as opposed to competing for the same types of jobs.10 A separate study found that immigrants in the U.S create more jobs than they take, thereby improving the economic outcomes for U.S.-born workers.11
Funding to support organizations providing direct assistance to newly arriving migrants and asylum seekers, funding to support community health workers and Federally Qualified Health Centers in border areas, and funding to address social needs such as poverty and LEP may help improve outcomes in the border region.12 Moreover, implementation of the Medicaid expansion in Texas could help to increase overall coverage rates and provide increased financial resources to support health providers and the health care system.
What happens when migrants arrive at the U.S.-Mexico border?
Immigration activity at the border is at an all-time high, with over two million encounters in 2022, a number that is 24% higher than the year before. Historically, the U.S.-Mexico border was primarily used as an entry point by migrants from Mexico, Guatemala, Honduras, and El Salvador; however, migrants from other countries, including Venezuelans, Cubans, and Nicaraguans, accounted for 43% of border encounters in 2022, a 39 percentage point increase since 2017.13 Some migrants from European countries like Ukraine have also used the Southwestern border between the U.S. and Mexico to seek entry into the country following political turmoil.14
U.S. Customs and Border Protection (CBP) screens and processes migrants and asylum seekers when they arrive at the border. Based on this screening, individuals may be returned to Mexico under Title 42 or other policies, detained, placed under expedited removal to return to their home country, or, if seeking asylum, released into the U.S. with a notice to appear in court or report for further processing.15 ,16
A range of nonprofit organizations help support migrants and asylum-seekers in the border region. Individuals released from custody may seek to reunite with family and friends already living in the U.S., with many traveling on to other areas of the country outside of the border region. However, they typically have very limited or no resources available and often rely on nonprofit organizations for assistance, particularly when they first arrive in the country. While refugees are authorized to work immediately upon arrival to the U.S.,17 asylum seekers must wait at least 150 days after filing their asylum application to apply for employment authorization and are not eligible to receive employment authorization until at least 180 days post-asylum filing, limiting their opportunities to work.18 The U.S. Congress recently appropriated $150 million in funding through the Federal Emergency Management Agency to reimburse faith-based, nonprofit, and government organizations providing humanitarian assistance, such as food and housing, to migrants.
Who lives in the U.S.-Mexico border region?
Overall, there are 78 million people living in the four states (Arizona, California, New Mexico and Texas) along the U.S.-Mexico border. Within these four states, there are 44 counties that sit along the border that are home to over 8 million people. Most (32) of these counties are in Texas, while 6 are in New Mexico, 4 are in Arizona, and 2 are in California. These states also include 316 non-border counties, with Texas again accounting for the largest number of these counties (222).
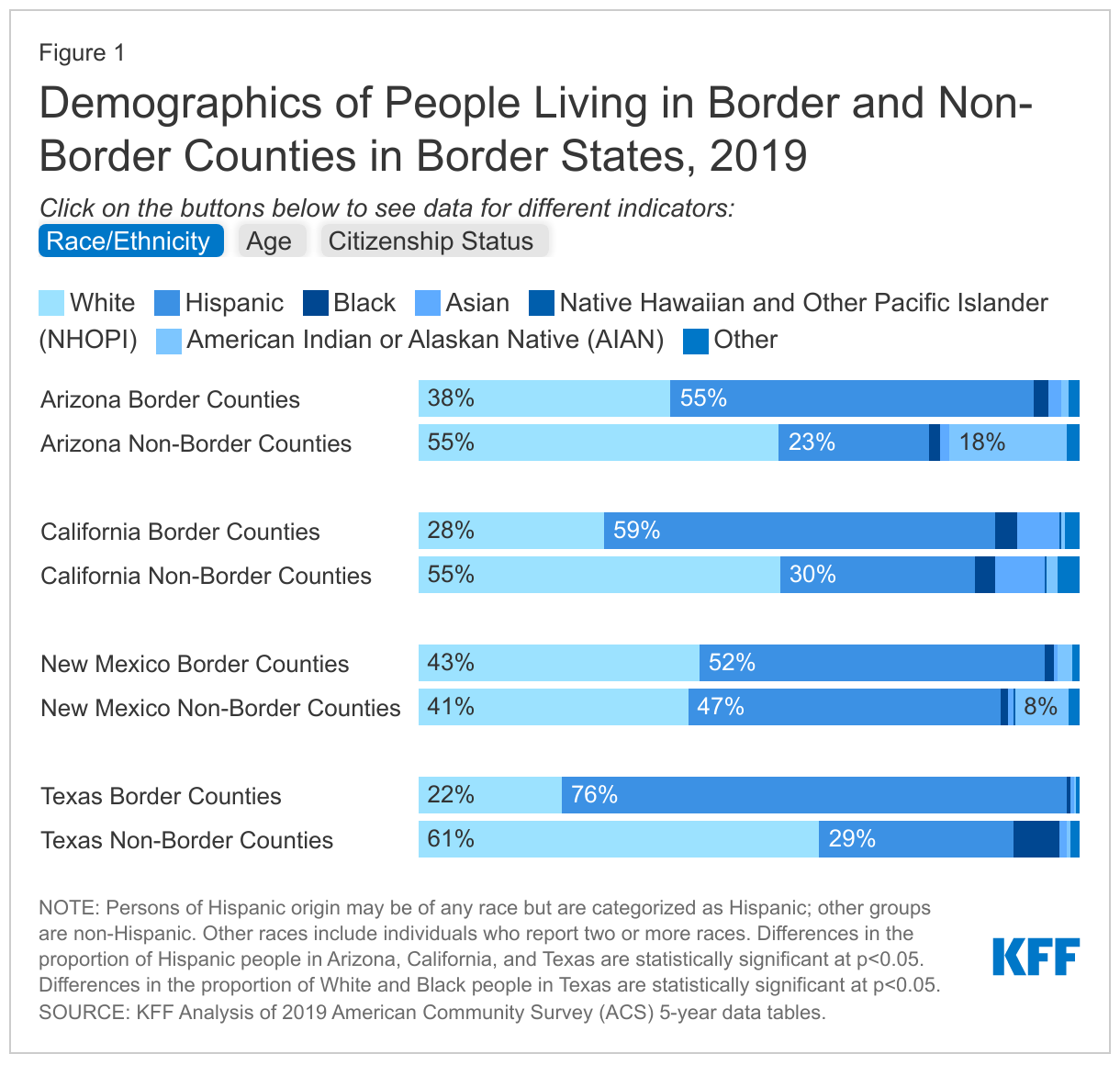
In Arizona, California, and Texas, border county residents are more likely to be Hispanic as compared with those in non-border counties (Figure 1). In Arizona, California, and New Mexico, over half of residents in border counties are Hispanic, while this share rises to over three-quarters (76%) in Texas. In contrast, Hispanic people make up less than a quarter of residents in non-border counties in Arizona (23%) and less than a third of non-border county residents in Texas (29%) and California (30%), while they account for closer to half of people in non-border counties in New Mexico (47%). The age distribution of people living in border and non-border counties is largely similar across all four states.
In Arizona and Texas, border counties include higher shares of noncitizens compared with non-border counties, but the vast majority of residents in both types of counties in all four states are U.S.-born citizens. In Arizona and Texas, roughly one in ten people in border counties is a noncitizen, which is higher than non-border counties. The share is slightly higher in California border counties (13%) and lower in New Mexico border counties (6%) with no statistically significant difference between border and non-border counties in these states. Across all four states, the large majority (over 80%) of residents in both border and non-border counties are U.S. citizens, with most being U.S.-born citizens.
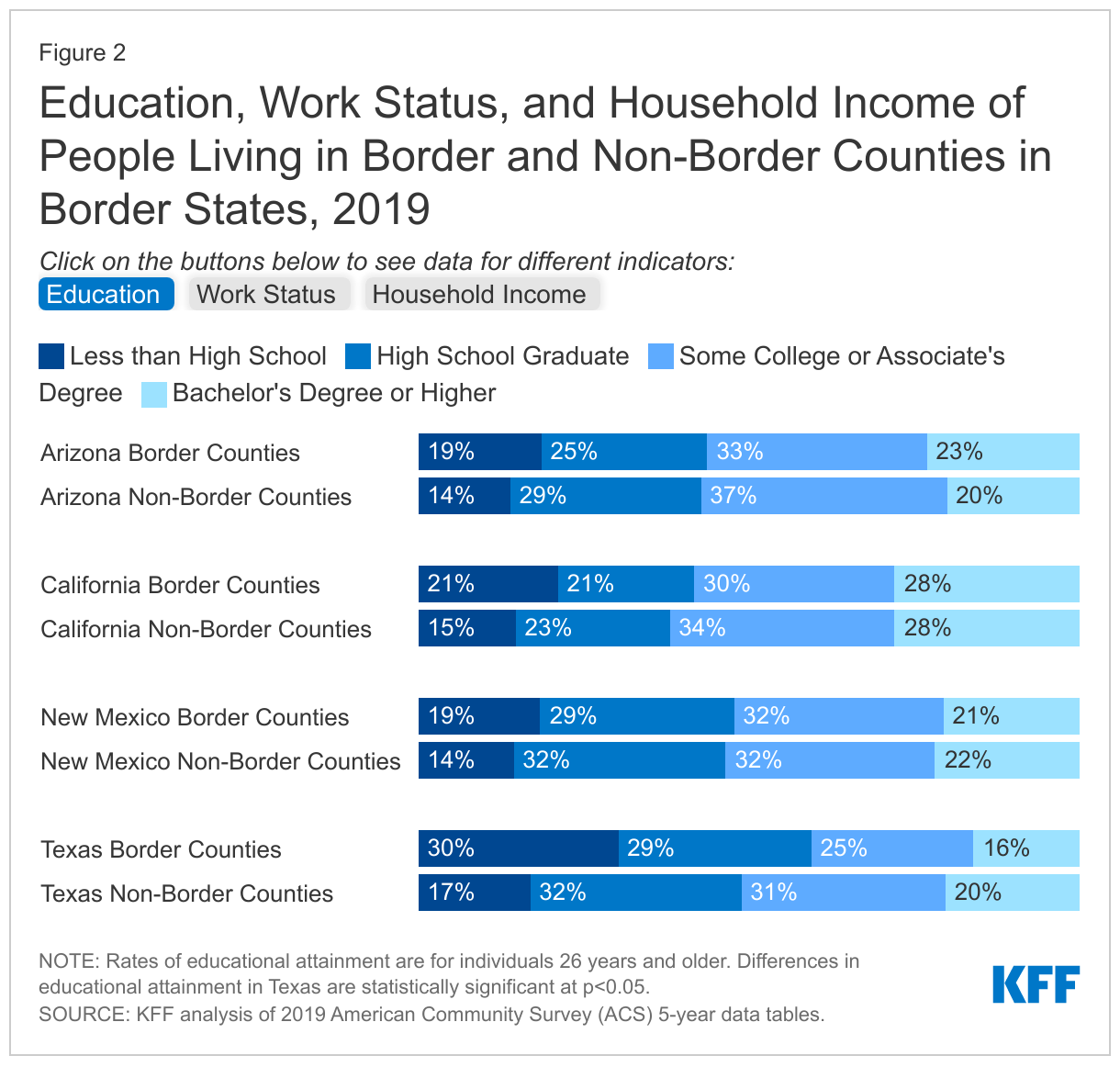
In Texas, border county residents have lower levels of educational attainment, full-time employment, and household incomes than their counterparts in non-border counties. (Figure 2). In Texas, the proportion of border county residents with less than a high school education is nearly twice as high as non-border county residents (30% vs. 17%). In contrast, the share of residents with less than a high school education is similar across border and non-border counties in the other three states. Regarding employment, the share of individuals living in border counties who are full-time workers is similar to the share in non-border counties in Arizona (48% vs. 45%), California (45% vs. 47%), and New Mexico (43% vs. 48%). However, the share of people in border counties who are full-time workers is lower than the share in non-border counties in Texas (49% vs. 55%), which has the highest share of full-time workers in non-border counties across the four states. Consistent with these findings, households in border counties in Texas are more likely than households in non-border counties to have incomes less than $25,000 (25% vs. 16%) and less likely to have incomes at or above $100,000 (18% vs. 28%). In contrast, the income distribution in Arizona, California, and New Mexico is similar between border and non-border counties. In California, over a third of residents in both border and non-border counties has household income of at least $100,000, which is higher compared to the other three states.
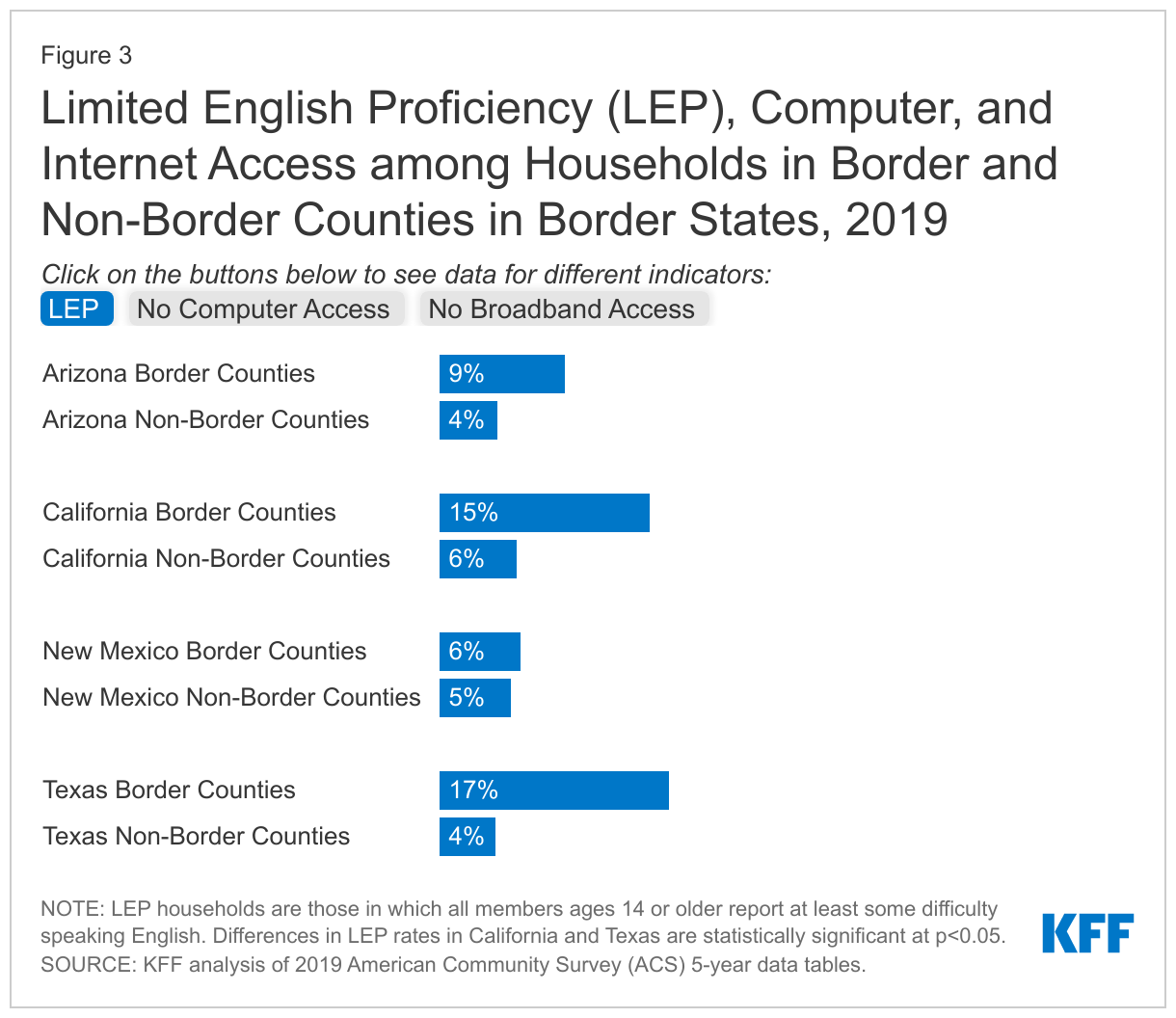
In California and Texas, households in border counties are more likely than those in non-border counties to face language barriers (Figure 3). Texas and California have the highest shares of households with limited English proficiency (LEP) in border counties (17% and 15%, respectively), which are over four and three times higher than the shares in their non-border counties (4% and 6%, respectively). In Arizona and New Mexico there are no statistically significant differences between border and non-border counties in the share of households with LEP. Access to computers and broadband access is generally similar between border and non-border counties in Arizona, California, and New Mexico. However, in Texas, nearly a quarter (23%) of households in border counties lack computer access compared to 14% of those in non-border counties. Texas also has the highest shares of households reporting no broadband access in both border and non-border counties across the four states, with lower broadband access in non-border than border counties (22% without broadband access vs. 18% without broadband access).
What is the status of health and health care in the border region?
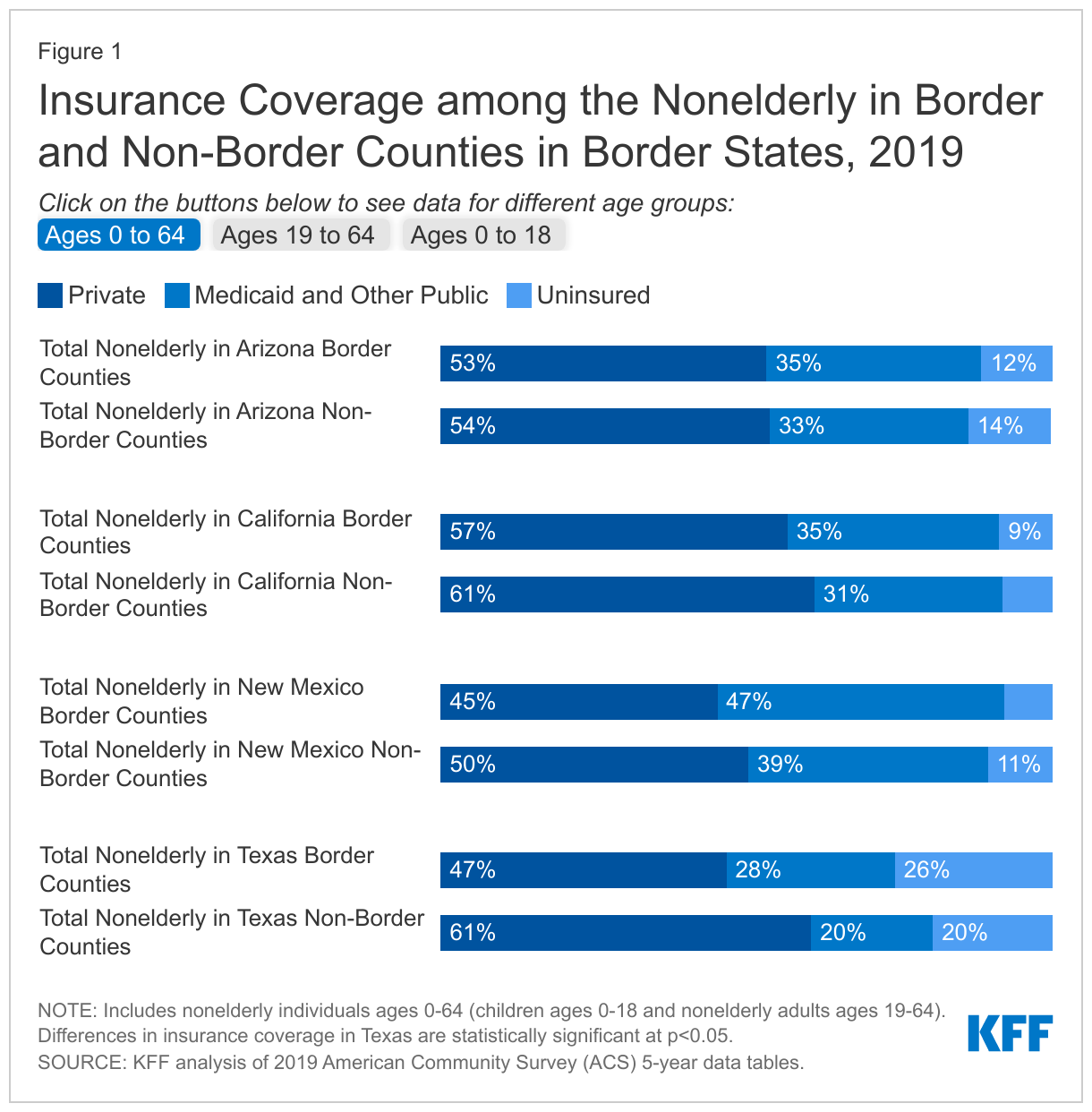
Uninsured rates among nonelderly residents in both border and non-border counties in Texas are at least twice as high as the other three border states, and nonelderly residents in its border counties are more likely to be uninsured than those in its non-border counties (26% vs. 20%) (Figure 4). In Texas, private coverage rates are lower in border counties than non-border counties. While the Medicaid coverage rate is higher in border counties than non-border counties, it does not fully offset the difference in private coverage leading to the higher uninsured rate for its residents in border counties. In the other three border states, there are no significant differences in insurance coverage patterns between border and non-border counties. The higher uninsured rates in Texas are mostly driven by higher uninsured rates for nonelderly adults, which are particularly high in border counties, where one in three adults lacked coverage. Children in Texas also have higher uninsured rates compared to the other border states, but there is little difference in uninsured rates for children in border vs. non-border counties.
In contrast to the other border states, Texas has not implemented the ACA Medicaid expansion to lower-income adults, contributing to its lower rates of Medicaid coverage and higher uninsured rates compared to the other states. Overall, over 770,000 poor adults are in the Medicaid coverage gap in Texas, accounting for over a third of all adults in the gap nationwide.19 As noted, in Texas, border county residents have lower levels of full-time employment and household incomes than their counterparts in non-border counties, which may contribute to the lower rates of private coverage in the border counties. While Medicaid coverage helps offset some of this difference, border counties also include higher shares of noncitizens compared with non-border counties, who may face eligibility restrictions for Medicaid. Specifically, those who are undocumented are not eligible to enroll in Medicaid or CHIP or to purchase coverage through the Marketplaces.
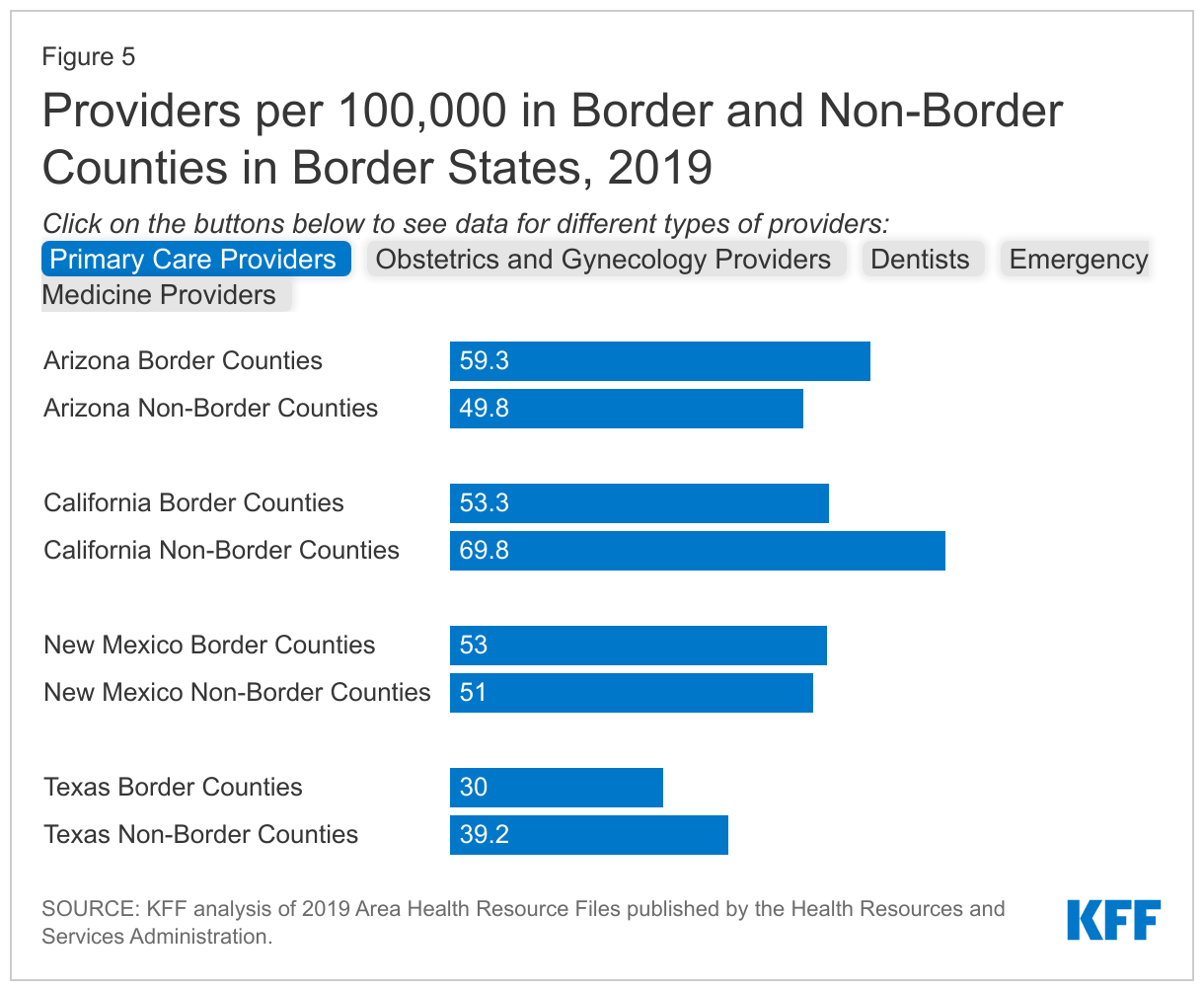
In California and Texas, border counties have a more limited supply of certain health care providers than non-border counties. Moreover, Texas has more limited availability of all four types of providers examined in both border and non-border counties compared with the other three states. In Arizona and New Mexico, the supply of providers between border and non-border counties varies based on provider type (Figure 5). For example, Arizona has fewer dentists per 100,000 people in border counties vs. non-border counties (45.3 vs. 55.1) but has more primary care providers per 100,000 in border counties vs. non-border counties (59.3 vs. 49.3).
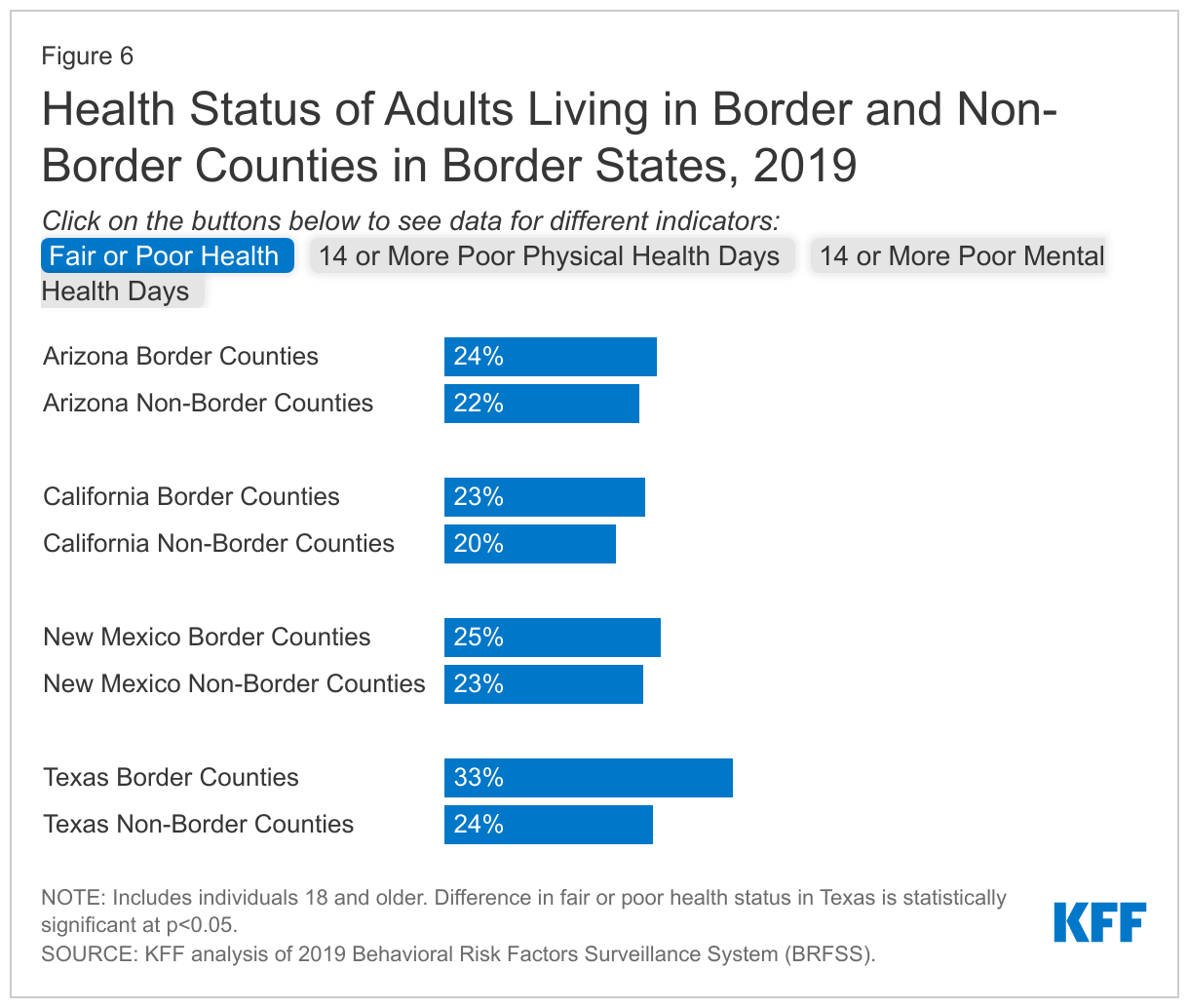
Adults in Texas border counties are more likely to report poor physical health compared to non-border counties. In Texas border counties, one-third of adults report being in fair or poor health as compared to roughly one-quarter in border and non-border counties in the other border states (Figure 6).There is limited variation in the share reporting 14 or more poor physical or mental health days in a month across border and non-border counties in the four states, however, more adults reported 14 or more poor mental health days in Texas as compared to the other three states.
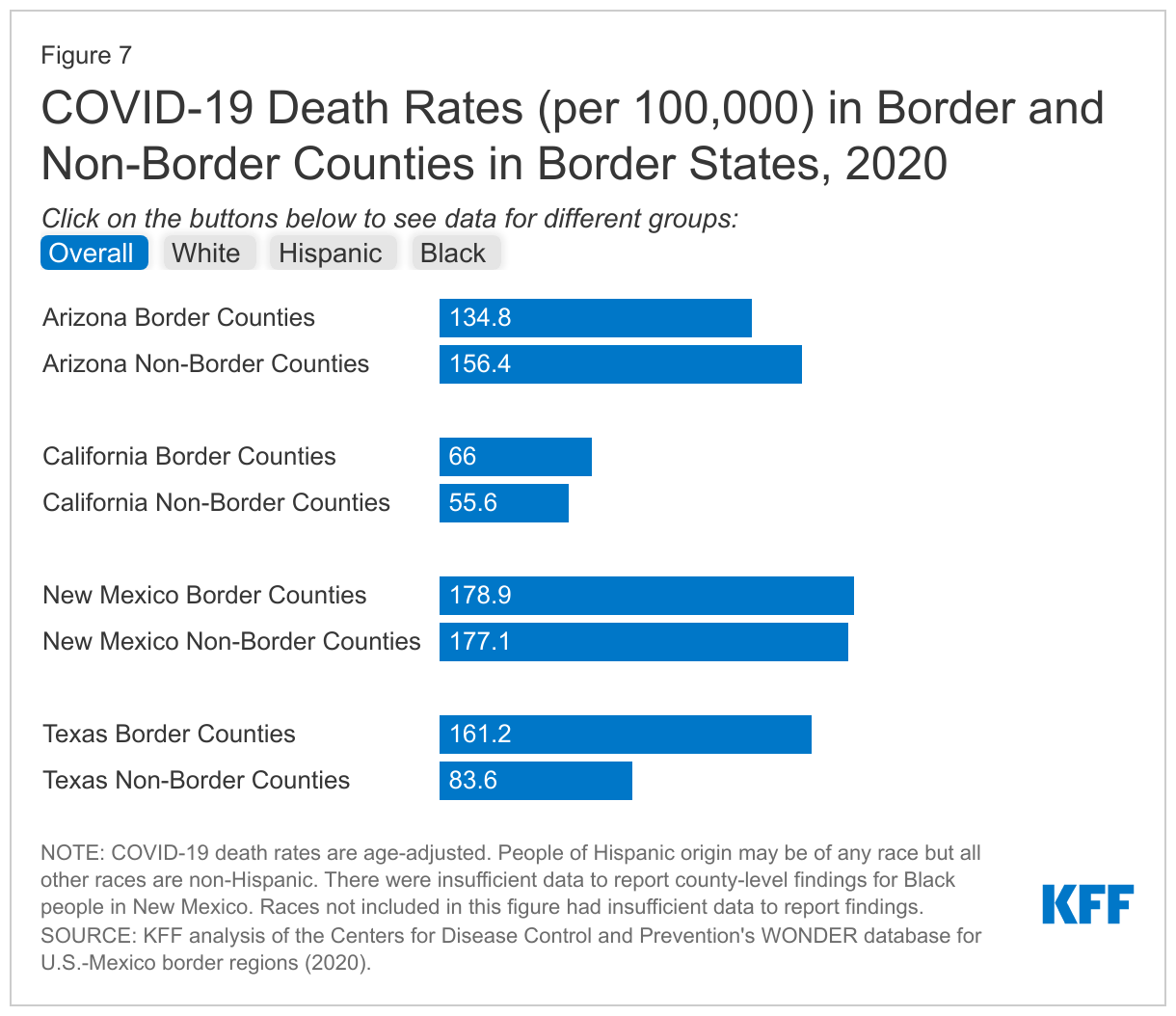
California, New Mexico, and Texas had higher rates of COVID-19 deaths in border counties vs. non-border counties overall, with the largest difference in Texas, where the border county death rate was nearly twice as high as the rate for non-border counties (161.2 vs. 83.6 per 100,000) (Figure 7). These differences are primarily driven by a higher COVID-19 death rate among Hispanic people in border counties vs. non-border counties. Across the four states, Texas had the highest death rate among Hispanic people. Moreover, within Texas, the death rate among Hispanic people was over 1.5 times higher in border counties than in non-border counties (290.9 vs. 167.1 per 100,000). The death rate for White people in Texas border counties was also higher than their counterparts in non-border counties (89.5 vs. 67.2).
Implications
With the recent surge in immigration activity at the border, it is helpful to better understand who lives in the region and their experiences, including their health and access to health care. Overall, people in the four states along the U.S.-Mexico border are more likely to be Hispanic, noncitizen immigrants, poor, and uninsured than people in other areas of the country. This analysis reveals further distinctions between and within these four states. It shows that, across many of the measures examined, Texas fared worse compared to the other border states. Moreover, within Texas, individuals in border counties fare worse across many examined measures compared to those in non-border counties, with particularly low levels of educational attainment and income, higher shares of households with LEP and no computer access, higher uninsured rates, and limited access to providers. In the other border states, there are smaller differences between people living in border vs. non-border counties.
In contrast to the other border states, Texas has not implemented the ACA Medicaid expansion to adults, contributing to lower rates of Medicaid coverage and higher uninsured rates. These differences are particularly pronounced in its border counties, where over a quarter of nonelderly residents, including one in three nonelderly adults, lacked health coverage. These high uninsured rates coupled with more limited availability of providers, particularly in border counties, likely contribute to challenges accessing health care and strains on safety-net providers, which are likely exacerbated by increased social and economic challenges in these areas.
Overall, these findings highlight the potential benefits of providing resources and support to the border region to meet the needs of the growing number of migrants and asylum seekers in the area. Better preparedness, more job opportunities, and a greater allocation of resources to help migrants assimilate in the community may be helpful not only in improving socioeconomic and health outcomes and reducing disparities in border areas, but in improving the economy overall, particularly in these border communities. Policies that increase opportunities for newly arriving migrants to work, such as reducing the wait time for applying for work authorization, could also reduce overcrowding at migrant shelters. Funding to support organizations providing direct assistance to newly arriving migrants and asylum seekers, funding to support community health workers and Federally Qualified Health Centers in border areas, and funding to address social needs such as poverty and LEP may help improve outcomes in the border region. Moreover, implementation of the Medicaid expansion in Texas could help to increase overall coverage rates and provide increased financial resources to support health providers and the health care system. Immigration remains a contentious political issue, and there are other competing demands for public dollars, but this analysis shows particularly acute health and social needs along the U.S.-Mexico border.
- U.S. Census Bureau, “Quick Facts”, https://www.census.gov/quickfacts, accessed November 14, 2022. ↩︎
- U.S. Census Bureau, “County Population Totals: 2020-2021”, https://www.census.gov/data/tables/time-series/demo/popest/2020s-counties-total.html, accessed November 14, 2022. ↩︎
- U.S. Customs and Border Protection (2022), “Southwest Land Border Encounters”, https://www.cbp.gov/newsroom/stats/southwest-land-border-encounters, accessed October 20, 2022. ↩︎
- Pew Charitable Trusts (2022), “Minus the Politics, Migrants Often Use Buses, Planes to Reach Shelter”, https://www.pewtrusts.org/en/research-and-analysis/blogs/stateline/2022/10/04/minus-the-politics-migrants-often-use-buses-planes-to-reach-shelter, accessed October 26, 2022. ↩︎
- National Public Radio (2022), “A dramatic shift at the border as migrants converge on a remote corner of South Texas” https://www.npr.org/2022/09/23/1124561261/a-dramatic-shift-at-the-border-as-migrants-converge-on-a-remote-corner-of-south-, accessed September 23, 2022. ↩︎
- Migration Policy Institute (2022), “Busing and Flights of Migrants by GOP Governors Mark a New Twist in State Intervention on Immigration”, https://www.migrationpolicy.org/article/migrant-asylum-seeker-busing, accessed October 26, 2022. ↩︎
- Kaiser Family Foundation (KFF), “State Health Facts”, https://modern.kff.org/statedata/, accessed October 28, 2022. ↩︎
- The Brookings Institution (2022), “Who are the 1 million missing workers that could solve America’s labor shortages?”, https://www.brookings.edu/blog/up-front/2022/07/14/who-are-the-1-million-missing-workers-that-could-solve-americas-labor-shortages/, accessed October 26, 2022. ↩︎
- Press Herald (2022), “Rep. Pingree submits bill to shorten asylum seekers’ wait time for work authorization”, https://www.pressherald.com/2022/02/11/pingree-introduces-bill-to-shorten-waiting-period-for-asylum-seeker-work-authorization/, accessed October 26, 2022. ↩︎
- Urban Institute (2015), “Immigrants and native workers compete for different low-skilled jobs”, https://www.urban.org/urban-wire/immigrant-and-native-workers-compete-different-low-skilled-jobs, accessed November 14, 2022. ↩︎
- Azoulay, Pierre, Benjamin F. Jones, J. Daniel Kim, and Javier Miranda. 2022. "Immigration and Entrepreneurship in the United States." American Economic Review: Insights, 4 (1): 71-88. ↩︎
- Rural Health Information Hub (2019), “Rural Border Health”, https://www.ruralhealthinfo.org/topics/border-health, accessed October 21, 2022. ↩︎
- Migration Policy Institute (2022), “Record-Breaking Migrant Encounters at the U.S.-Mexico Border Overlook the Bigger Story”, https://www.migrationpolicy.org/news/2022-record-migrant-encounters-us-mexico-border, accessed October 26, 2022. ↩︎
- National Public Radio (2022), “Thousands of Ukrainian refugees arrive at U.S.-Mexico Border”, https://www.npr.org/2022/04/08/1091769484/hundreds-of-ukrainian-refugees-at-the-u-s-mexico-border-hoping-for-asylum, accessed September 23, 2022. ↩︎
- Kaiser Family Foundation (KFF) (2022), “Title 42 and its Impact on Migrant Families”, https://modern.kff.org/racial-equity-and-health-policy/issue-brief/title-42-and-its-impact-on-migrant-families/, accessed October 26, 2022. ↩︎
- U.S. Citizenship and Immigration Services (2022), “Asylum”, https://www.uscis.gov/humanitarian/refugees-and-asylum/asylum, accessed October 21, 2022. ↩︎
- U.S. Citizenship and Immigration Services (2022), “Refugees”, https://www.uscis.gov/humanitarian/refugees-and-asylum/refugees, accessed October 26, 2022. ↩︎
- U.S. Citizenship and Immigration Services (2022), “USCIS Stopped Applying June 2020 Rules Pursuant to Court Order in Asylumworks v. Mayorkas”, https://www.uscis.gov/laws-and-policy/other-resources/class-action-settlement-notices-and-agreements/uscis-stopped-applying-june-2020-rules-pursuant-to-court-order-in-asylumworks-v-mayorkas#:~:text=You%20may%20apply%20for%20employment,you%20file%20your%20asylum%20application., accessed October 21, 2022. ↩︎
- Kaiser Family Foundation (KFF) (2021), “The Coverage Gap: Uninsured Poor Adults in States that Do Not Expand Medicaid”, https://modern.kff.org/medicaid/issue-brief/the-coverage-gap-uninsured-poor-adults-in-states-that-do-not-expand-medicaid/, accessed October 26, 2022. ↩︎