Medicaid Policy Approaches to Facilitating Access to Vaccines for Low-Income Children
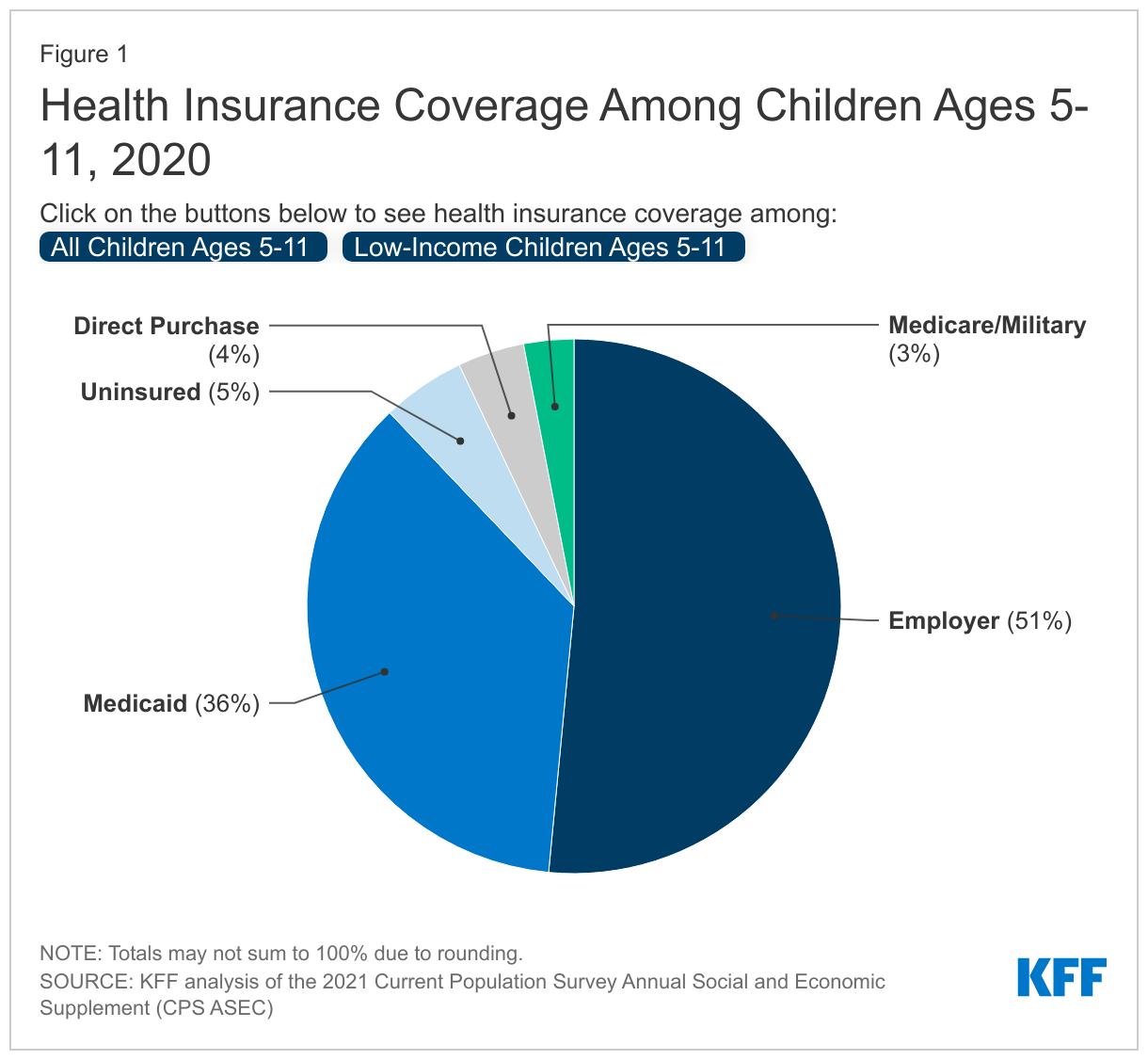
Following the recent US Food & Drug Administration’s (FDA) authorization and the Centers for Disease Control and Prevention’s (CDC) recommendation, children ages 5-11 are now eligible to receive Pfizer-BioNTech’s COVID-19 vaccine. There may be unique challenges to vaccinating young children, particularly those from low-income families who may face additional barriers to access. Among all children ages 5-11, over one-third (36%) are covered by Medicaid, and 70% of children ages 5-11 with incomes below 200% of the Federal Poverty Level (FPL) are covered by Medicaid (Figure 1). State Medicaid programs and Medicaid managed care plans are looking at a range of policy options to facilitate access to vaccines for young, low-income children.
Low-income children may face barriers to vaccine access. KFF polling recently found that parents of children ages 5-11 with household incomes under $50,000 are more likely than those with higher incomes to say they are very or somewhat concerned about issues related to the coronavirus vaccine. In particular, low-income parents reported more concerns about accessing the vaccine, such as taking time off work or traveling to a place to receive a vaccine. Research prior to the pandemic similarly shows lower overall immunization rates for low-income children, likely stemming from difficulties with access such as a lack of information and outreach or transportation.
Low rates of vaccination among low-income children could have implications for ongoing disparities in prevalence of COVID-19 among communities of color. KFF analysis of the 2021 Current Population Survey Annual Social and Economic Supplement (CPS ASEC) finds over two-thirds of children ages 5-11 covered by Medicaid are children of color, including approximately 37% who are Hispanic and 21% who are Black. Black and Hispanic people have been less likely than their White counterparts to have received a vaccine over the course of the vaccine rollout; though the disparity is narrowing over time, disparities in children’s take-up of the vaccine could reverse that trend.
States report adopting a range of Medicaid strategies aimed at increasing vaccine uptake, several of which could extend to low-income children covered by the program. The Centers for Medicare & Medicaid Services (CMS) has highlighted several Medicaid flexibilities and funding opportunities states can use to promote vaccine access. For example, states can request Medicaid administrative federal matching funds for state funded monetary incentives for enrollees to encourage vaccine uptake. In KFF’s annual budget survey, several states reported Medicaid managed care organization (MCO) activities and incentives to promote vaccine take-up among Medicaid enrollees, including financial incentives for MCOs that meet vaccination targets. States also report using member incentives, such as gift cards, and provider incentives. Given that MCOs provide services to over the vast majority of child Medicaid enrollees, these activities may reach many children and families covered by the program. Other state activities focus on using providers to address vaccine hesitancy, which may be especially needed for parents with young children; Medicaid options in this area include vaccine administrative payment rates and financial incentives for achieving or increasing vaccination rates.
Strategies to target outreach can help improve vaccine uptake among low-income children. CMS notes Medicaid administrative federal matching funds can be used for beneficiary and provider community outreach such as disseminating information or materials and providing trainings. Several states in KFF’s annual budget survey reported using data collection and tracking to better target outreach and reduce disparities in COVID-19 vaccination rates. Strategies to employ trusted and diverse messengers of vaccine information can help with education and outreach to parental/caregivers (which is important because their consent for vaccines is required in all states, though DC and Philadelphia allow 11-year-olds to self-consent for the COVID-19 vaccine). For example, MCOs in Michigan report using community health workers to provide education and outreach to address vaccine hesitancy. Further, KFF analysis from June 2021 found community health centers were vaccinating larger shares of people of color compared to overall vaccination efforts, reflecting their established trusted relationships with communities of color.
While the cost of a COVID-19 vaccine is covered for all individuals, other policies can help to address additional barriers to accessing vaccines for low-income children. While the federal government recently implemented a paid leave policy for federal workers taking their children to vaccine appointments, other employers have not, and lower income workers may have more difficulty taking time off to get their children vaccinated. Additionally, arranging transportation to and from a vaccine appointment may be difficult for some, especially if a vaccine provider is not close by. In KFF’s annual budget survey states reported including assistance with vaccination scheduling and transportation coordination to increase access, as well as partnering with community-based organizations to provide vaccines where people can easily access them. Strategies that help parents more easily make and travel to vaccine appointments can help increase vaccine uptake among low-income children and reduce disparities in COVID-19 vaccination rates.