VOLUME 13
Myths About Raw Milk and Vaccines
This is Irving Washington and Hagere Yilma. We direct KFF’s Health Misinformation and Trust Initiative and on behalf of all of our colleagues across KFF who work on misinformation and trust we are pleased to bring you this edition of our bi-weekly Monitor.
KFF Authors:
 Irving Washington
Irving Washington  Hagere Yilma
Hagere Yilma Summary
This volume discusses politicized narratives linking vaccines to autism and misleading claims about the benefits of raw milk. It also examines the impact of perceived expertise and trust on misinformation beliefs and how AI in mental health care may unintentionally contribute to the spread of false information.
Recent Developments
False Claims Linking Vaccines to Autism May Further Hinder Vaccination Rates

The high number of pertussis (whooping cough) and measles cases reported in the U.S. this year compared to last year may reflect a shift in confidence in public health recommendations made by federal health officials. While vaccination remains the most effective way to prevent these diseases, a KFF analysis found a continued decline in routine immunization rates among U.S. kindergartners, with coverage for key vaccines such as MMR, DTaP, polio and varicella falling below pre-pandemic levels and, in the case of measles, below the threshold needed to prevent measles outbreaks. These trends, driven in part by vaccine misinformation and growing partisan divides over vaccine requirements, raise concerns about the potential for further declines under a Trump administration that has signaled skepticism towards vaccine effectiveness and safety.
On November 14, President-elect Donald Trump confirmed that he plans to nominate Robert F. Kennedy Jr., who has a history of sharing false or misleading claims about vaccine safety, to head the U.S. Department of Health and Human Services. During an interview on NBC’s Meet The Press, Trump suggested that Kennedy’s role would include investigating the debunked theory linking vaccines to autism, citing rising autism rates in the U.S., despite the scientific consensus that vaccines do not cause autism.
Kennedy’s claims about autism and vaccines often gain traction on social media, where other accounts amplify his message on their platform, particularly around the timing of high-profile events. For example, in the days before and after Trump announced his plan to nominate Kennedy, several X posts shared a video clip of Kennedy speaking at Hillsdale College in 2023, in which he falsely claimed that “there’s no front-end safety testing” for routine vaccines and suggested that vaccines cause autism, as well as ADHD, sleep disorders, language delays, Tourette’s syndrome, and narcolepsy. Four X accounts with large followings and a history of spreading false claims about vaccines shared the video between November 12 and November 15, receiving hundreds of thousands to millions of views. The most popular post of the four garnered approximately 6.7 million views, 148,000 likes, 52,000 reposts, and 1,500 comments as of December 5. Top comments on the post reinforced the debunked myth that vaccines cause autism, further spreading misinformation.
False claims that vaccines cause autism have existed for years and have been repeatedly debunked. The theory that vaccines cause autism was first popularized in 1998 by a small study that was later retracted, and the study’s author lost his medical license due to falsified information. Since then, decades of credible studies have consistently shown that vaccines are not associated with autism. Still, the myth persists, and concerns about mRNA COVID-19 vaccines have led to an increase in false claims about vaccine safety, including false claims linking vaccines to autism.
Polling Insights:
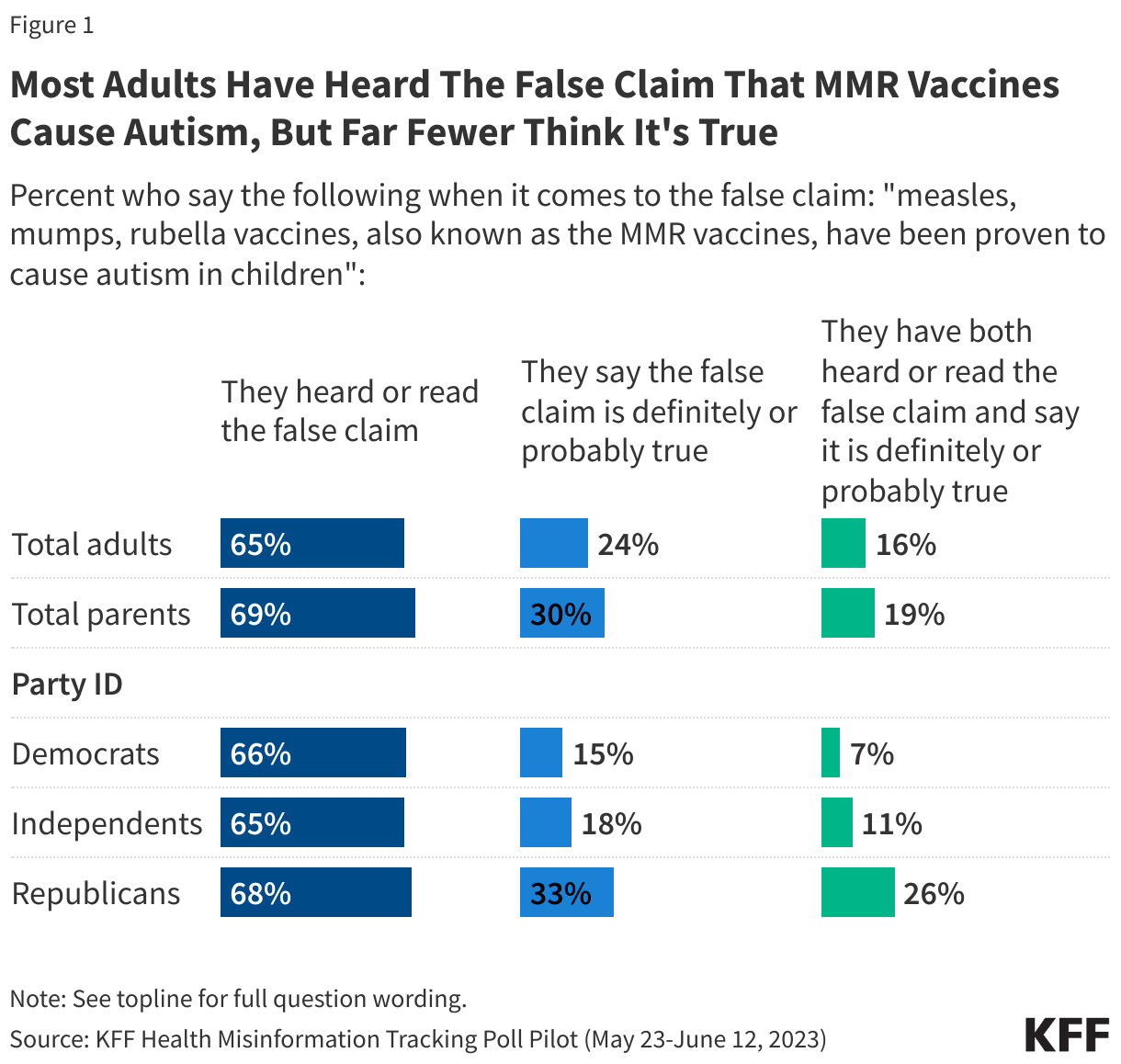
KFF polling has found that misinformation related to MMR vaccines causing autism in children was a widely-encountered piece of health misinformation, with 65% of adults, including a similar share of parents, saying they had read or heard the false claim that “MMR vaccines have been proven to cause autism in children” (Figure 1). Fewer adults overall, however, said they thought this claim was definitely or probably true (25% of adults and 30% of parents). Combining these two measures, about one in six adults (16%) and one in five parents (19%) said they both had heard that MMR vaccines cause autism and believe this is probably or definitely true.
While similar shares across partisan groups report having heard the false claim that MMR vaccines cause autism, a larger share of Republicans compared to Democrats and independents say this false claim is definitely or probably true.
Notably, most of the public express some degree of uncertainty about the false claim that MMR vaccines have been proven to cause autism, with 43% saying it is “probably false” and 20% saying it is “probably true.”
USDA Orders Bird Flu Testing for Milk Supply Amid Ongoing Raw Milk Misinformation

The U.S. Department of Agriculture (USDA) announced mandatory bird flu testing for the nation’s milk supply beginning December 16, after the H5N1 virus was first detected in U.S. dairy herds earlier this year. The FDA and CDC explain that pasteurization effectively neutralizes the virus, along with other germs such as E. coli and salmonella, but false claims about the health benefits of unpasteurized or raw milk may continue to motivate raw milk consumption. Social media platforms amplify the appeal of raw milk by promoting its perceived health and beauty benefits, while simultaneously claiming that federal regulatory bodies want to suppress consumption for potentially nefarious reasons.
Raw milk advocates often misrepresent the difference between pasteurized and unpasteurized milk to portray raw milk as more beneficial to health than pasteurized milk, claiming that the pasteurization process destroys healthy enzymes, probiotics, and vitamins. However, studies show that while pasteurization can reduce certain enzymes and vitamins, the levels in milk are generally too low to have a significant impact on health anyway. Advocates of raw milk also commonly cite a 2011 study to support claims that raw milk consumption reduces the risk of asthma in children. However, this study did not include a comparison group of people who consumed pasteurized milk, making it difficult to draw conclusions about the effect of pasteurization on asthma. Efforts to address these claims about raw milk should focus on clarifying these nuances rather than dismissing them as misinformation. Educating people about the science behind pasteurization and the actual nutritional content of milk can help counter misleading claims and provide a more informed perspective on raw milk.
Research Insights
Perceived Expertise Influences Trust in Nutrition Misinformation Among Youth

A study published in the nutrition journal Appetite examined how young people process nutrition-related misinformation on social media, focusing on how perceived source expertise influences trust in the information. Researchers exposed 480 adolescents aged 16 to 22 to either accurate or misleading nutrition claims from social media profiles created for influencers, celebrities, and health journalists. They found that while adolescents did not change their beliefs or behavioral intentions after exposure to misinformation, they were more likely to trust information when it came from someone they perceived as an expert —even when that person was not a real expert and lacked health or nutrition credentials. In addition, participants struggled to identify false claims, suggesting gaps in media literacy that make young people more susceptible to misinformation from those they perceive as experts.
Source: Lissens, M., Harff, D., & Schmuck, D. (2024). Responses to (Un) healthy Advice: Processing and Acceptance of Health Content Creators’ Nutrition Misinformation by Youth. Appetite, 107812.
The Impact of Trust on Belief in Fake News, Conspiracy Theories, and Vaccine Hesitancy

A study published in PLOS Global Health explored the relationship between people’s trust in information and their likelihood of believing fake news, conspiracy theories, and vaccine hesitancy. The researchers conducted two surveys in the United Kingdom to assess three trust-related traits, including credulity (trusting too easily), mistrust (excessive skepticism), and balanced trust. The study found that participants with high credulity were more likely to believe fake news and conspiracy theories, particularly those related to COVID-19. The study also linked childhood adversity to increased belief in fake news, conspiracy theories, and vaccine hesitancy. Mistrust and credulity were found to mediate this relationship, suggesting that disruptions in trust caused by childhood adversity may influence these beliefs and behaviors. These findings emphasize the importance of promoting balanced trust, encouraging critical thinking while avoiding excessive skepticism as a strategy for improving public health communication.
Source: Tanzer, M., Campbell, C., Saunders, R., Booker, T., Luyten, P., & Fonagy, P. (2024). The role of epistemic trust and epistemic disruption in vaccine hesitancy, conspiracy thinking and the capacity to identify fake news. PLOS Global Public Health, 4(12), e0003941.
AI & Emerging Technology
AI Used for Mental Health Care Poses Risks of Sharing False Information

The growing use of AI in mental health care raises concerns about its potential to contribute to misinformation. As AI technologies like chatbots become more integrated into mental health support, there is a risk that they could provide incorrect or harmful advice, as seen with a chatbot from the National Eating Disorders Association that exacerbated eating disorders. AI’s inherent tendency to be overly confident, even when wrong, could further fuel misinformation if not properly regulated. This year, Utah enacted one of the first laws focused on addressing these risks by developing regulations to improve data privacy, protect against harmful practices, and clarify the roles of licensed professionals in using AI tools. Other states, such as Colorado and California have also introduced policies related to AI and health in other domains, but a state-by-state approach could create a confusing and inconsistent regulatory landscape.
About The Health Information and Trust Initiative: the Health Information and Trust Initiative is a KFF program aimed at tracking health misinformation in the U.S., analyzing its impact on the American people, and mobilizing media to address the problem. Our goal is to be of service to everyone working on health misinformation, strengthen efforts to counter misinformation, and build trust.

The Monitor is a report from KFF’s Health Information and Trust initiative that focuses on recent developments in health information. It’s free and published twice a month.
Sign up to receive KFF Monitor
email updates
Support for the Health Information and Trust initiative is provided by the Robert Wood Johnson Foundation (RWJF). The views expressed do not necessarily reflect the views of RWJF and KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities. The Public Good Projects (PGP) provides media monitoring data KFF uses in producing the Monitor.