Introduction
Native Hawaiian or Pacific Islander (NHPI) people experience substantial and enduring disparities in health and health care. These, in part, reflect specific challenges in accessing health care such as geographic isolation, economic challenges, and limited availability of culturally appropriate care. Furthermore, NHPI communities are often excluded from data and analysis due to their smaller population sizes. This limits the visibility and understanding of their health outcomes and experiences accessing health care, impeding efforts to address their health care needs and eliminate disparities.
Given the importance of increasing the understanding of experiences among these groups as part of advancing equity, this brief provides an overview of NHPI experiences across key measures of health, health access, and social and economic factors that influence health. It is based on KFF analysis of data from multiple datasets including the 2018-2022 American Community Survey, the 2022 Behavioral Risk Factor Surveillance System, and the Centers for Disease Control and Prevention (CDC) WONDER online database. This report also incorporates analysis from Key Data on Health and Health Care by Race and Ethnicity, which examines how people of color fare compared to White people across 64 measures of health, health care, and social determinants of health. Racial and ethnic groupings for each measure vary depending on the data source. Data reported by ethnic identity are limited to people who identify as NHPI alone. Data reported for the continental U.S. refers to the 48 contiguous states, District of Columbia (DC), and Alaska. Data for many health outcome measures are not available by ethnic subgroup. Data are limited to NHPI people residing within the 50 states and DC1 .
Key takeaways include:
NHPI people represent people from diverse backgrounds. The majority of NHPI people identify with more than one race and ethnicity. NHPI people have ethnic origins tracing back to several islands in the Pacific Ocean that have varying relationships with the U.S. Among NHPI people residing in the 50 states and DC, most live in Hawaii and California.
NHPI people fare worse than White people across the majority of examined measures of health, health care, and social determinants of health. Reflective of lower rates of private coverage, NHPI (9%) people under age 65 are somewhat more likely to be uninsured than White people (7%). Roughly a quarter of NHPI adults (24%) under age 65 report not having a personal provider compared to 17% of White adults. Additionally, similar shares of NHPI adults (20%) report fair or poor health status as White adults (16%). NHPI people have higher birth risks and worse birth outcomes compared to White people. This may in part reflect limited access to prenatal care, as NHPI women (22%) are over four times more likely to receive late or no prenatal care than White women (5%). NHPI people also have higher rates of pregnancy-related mortality (62.8 per 100,000) and infant mortality (8.5 per 100,000) compared to their White counterparts (14.1 per 100,000 and 4.5 per 100,000, respectively). Although the majority of NHPI people under age 65 are in working families, they have higher rates of poverty than White people (15% vs. 10%). Roughly half of NHPI people (54%) own a home compared to about three quarters of their White counterparts (76%). NHPI people have similar or better health outcomes compared to White people across a few health measures. NHPI people (both at 20%) have a similar likelihood of reporting fair or poor health and 14+ mentally unhealthy days compared to White people (16% and 15%, respectively). NHPI adults (6%) are less likely to have a heart attack or heart disease than White people (8%) yet have similar rates of heart disease-related mortality (173.2 per 100,000 vs. 173.1 per 100,000, respectively).
Among NHPI people, there is significant variation in key factors that influence health, including health coverage, income, and homeownership, with Marshallese people faring the worst across all examined measures. Among NHPI people under age 65, uninsured rates range from less than one in ten of Chamorro (8%), Samoan (9%), and Native Hawaiian (9%) people to nearly one in four (24%) Marshallese people. Homeownership rates also vary from roughly two-thirds of Fijian people (65%) to 14% of Marshallese people.
Data gaps prevent the ability to fully identify and understand health disparities for NHPI people. Data are insufficient or not disaggregated for NHPI people for many health and health care measures. Among available data, NHPI people fare worse than White people for the majority of measures. For some measures there is no significant difference, but this sometimes may reflect the smaller sample size for NHPI people in many datasets, which limits the power to detect statistically significant differences.
These data highlight the importance of continued efforts to address disparities in health and health care for NHPI people in ways that account for the diversity of the population and their experiences. Continued efforts to increase the availability of disaggregated data for NHPI people overall and by ethnicity, such as oversampling to generate adequate sample sizes to produce reliable estimates and changes to the collection and reporting of data on race and ethnicity, will also be important for improving the ability to identify and understand the disparities they face and assessing the impact of interventions to address them.
Overview of NHPI People in the U.S.
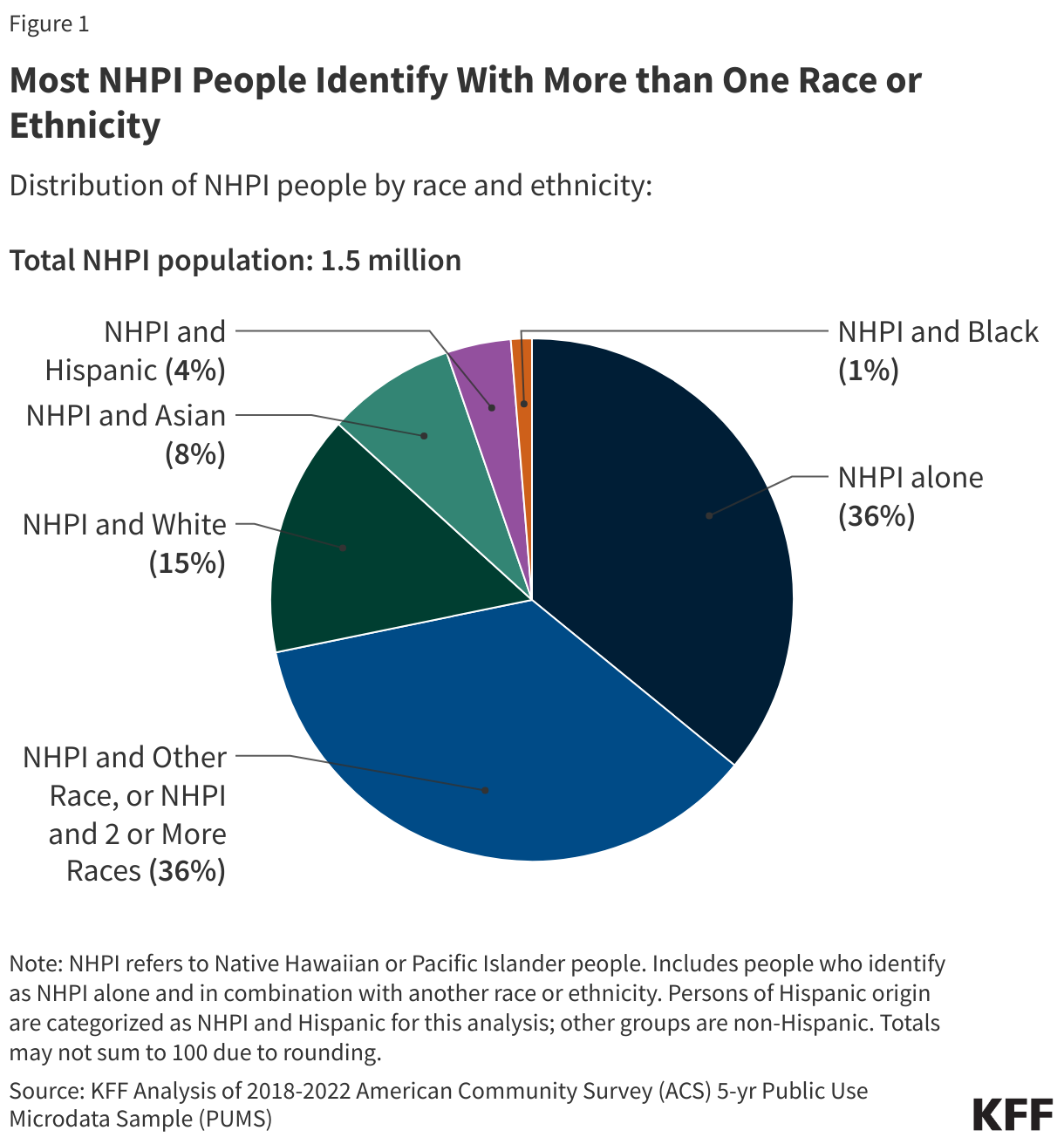
The NHPI population has grown and become more diverse over time. As of 2022, there were roughly 1.5 million people in the U.S. who identify as NHPI alone or in combination with another racial or ethnic group. The majority of NHPI people identify as NHPI and at least one other race, while just about one in three NHPI people identify as NHPI alone (36%) (Figure 1).
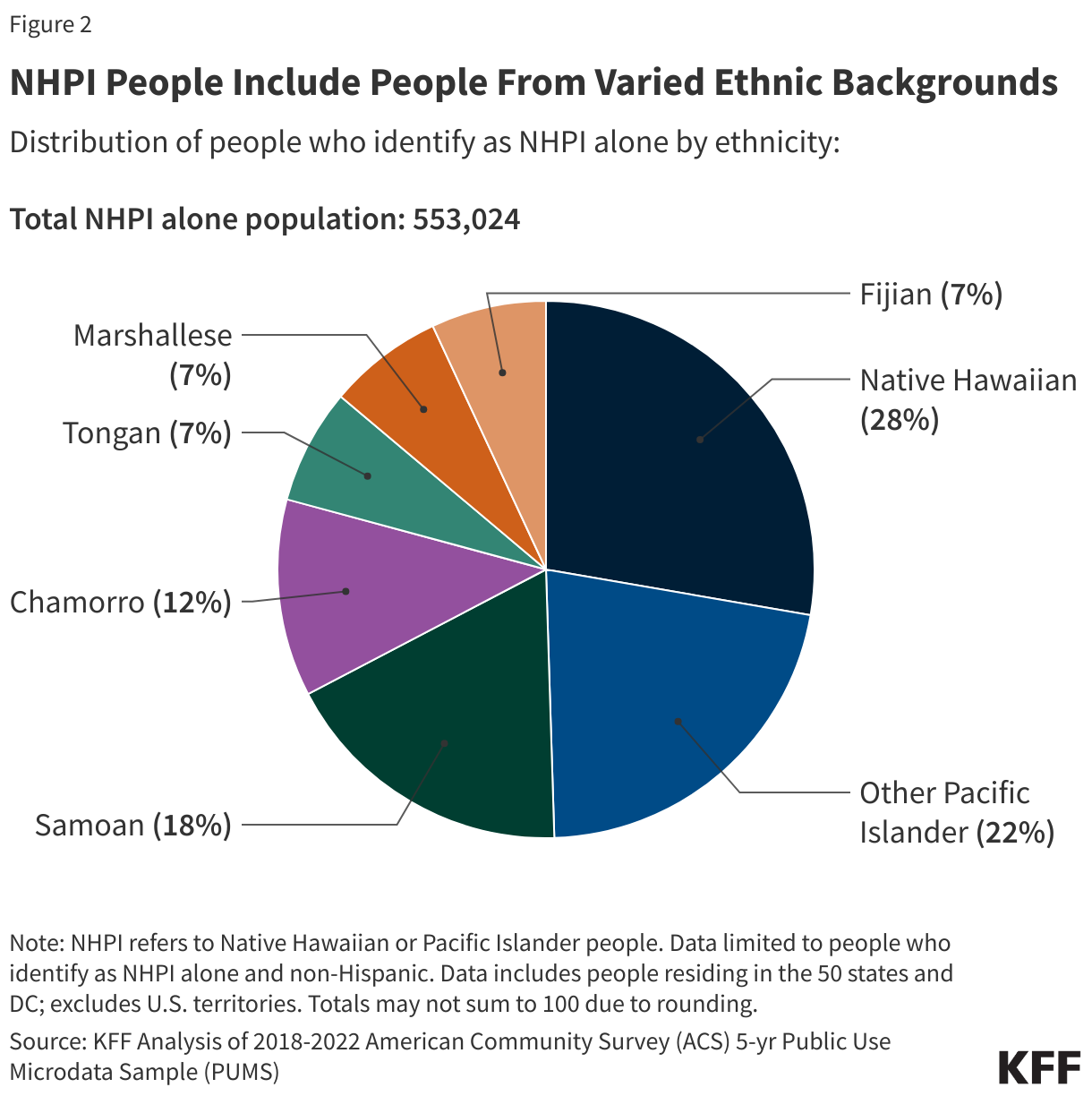
NHPI people trace their family origins to several islands in the Pacific Ocean with varying relationships with the U.S. Among people who identify as NHPI alone, 28% are Native Hawaiian. About one in five (18%) are Samoan, about one in eight are Chamorro (12%), and less than one in ten identify as Fijian (7%), Tongan (7%), or Marshallese (7%) (Figure 2). The remaining 22% identify as one of the remaining other Pacific Islander groups, including Palauan, Tahitian, Chuukese, Pohnpeian, Yapese, and other groups.
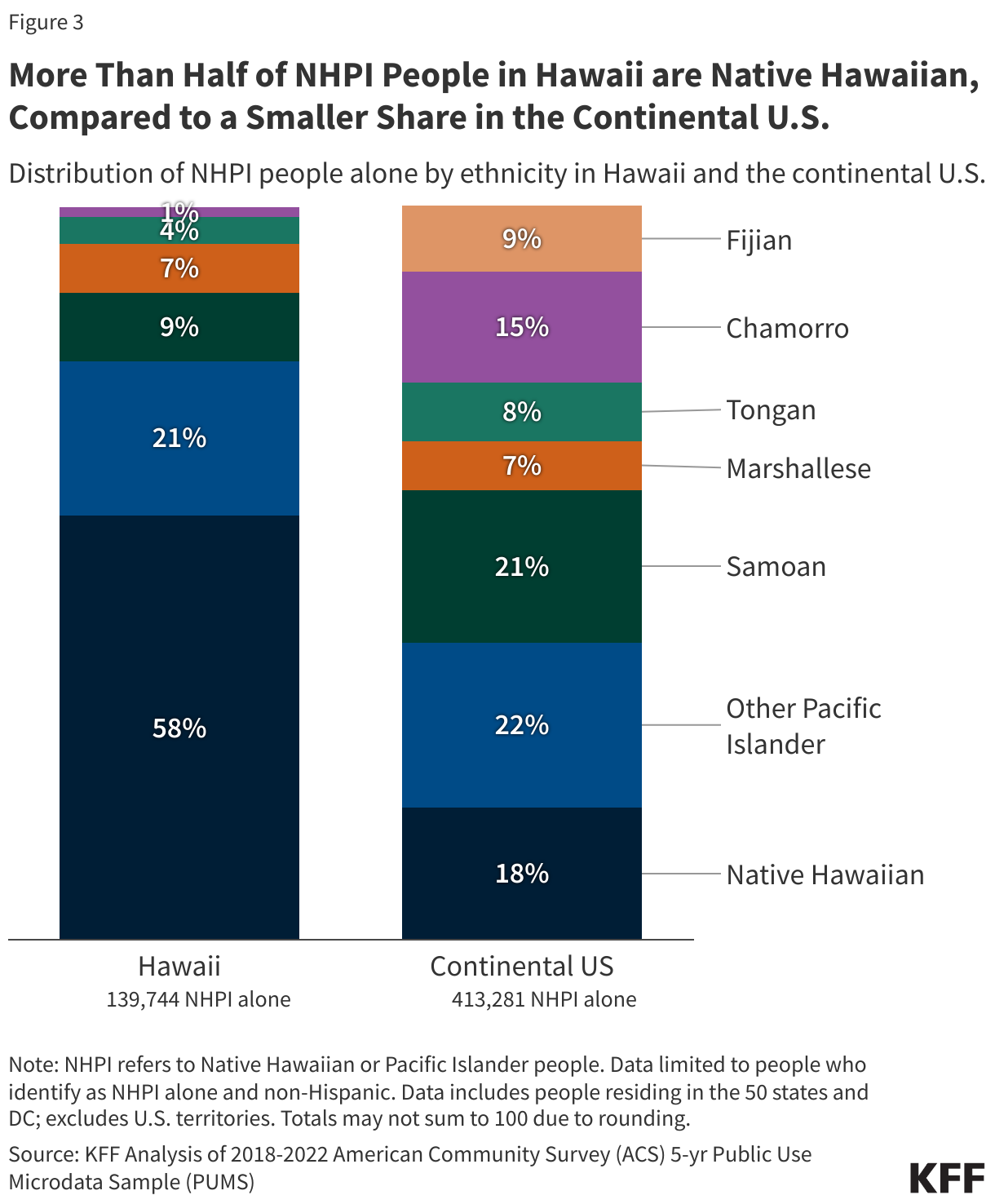
There is significant variation in the ethnic identity among NHPI people living in Hawaii compared to the continental U.S. Not surprisingly, among those who identify as NHPI alone, the majority of those residing in Hawaii are Native Hawaiian (58%), while ethnic identity is more mixed among those living in the continental U.S. (Figure 3).
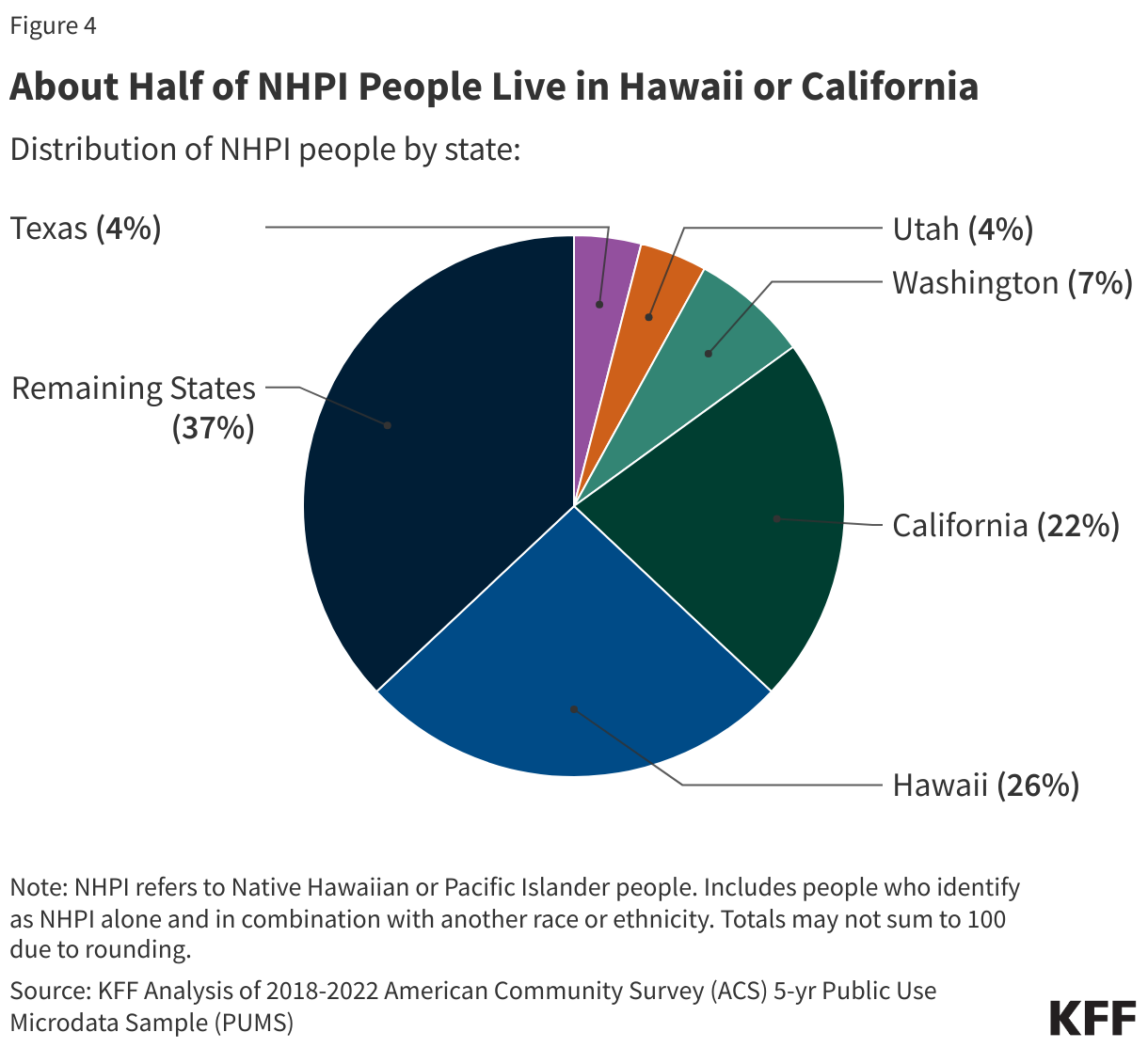
Among NHPI people (alone or in combination with another race or ethnicity) living within the 50 states and DC, nearly half reside in Hawaii (26%) and California (22%) alone (Figure 4). Washington state (7%) accounts for the next largest share of NHPI people in the U.S., followed by Utah (4%) and Texas (4%). Many NHPI people also reside in their homelands and across the U.S. territories of Guam, Samoa, the Commonwealth of the Northern Mariana Islands, and the Freely Associated States (FAS) that include the Federated States of Micronesia, the Republic of the Marshall Islands, and the Republic of Palau. However, data for NHPI people living in the territories and FAS are limited and not reflected in this analysis.
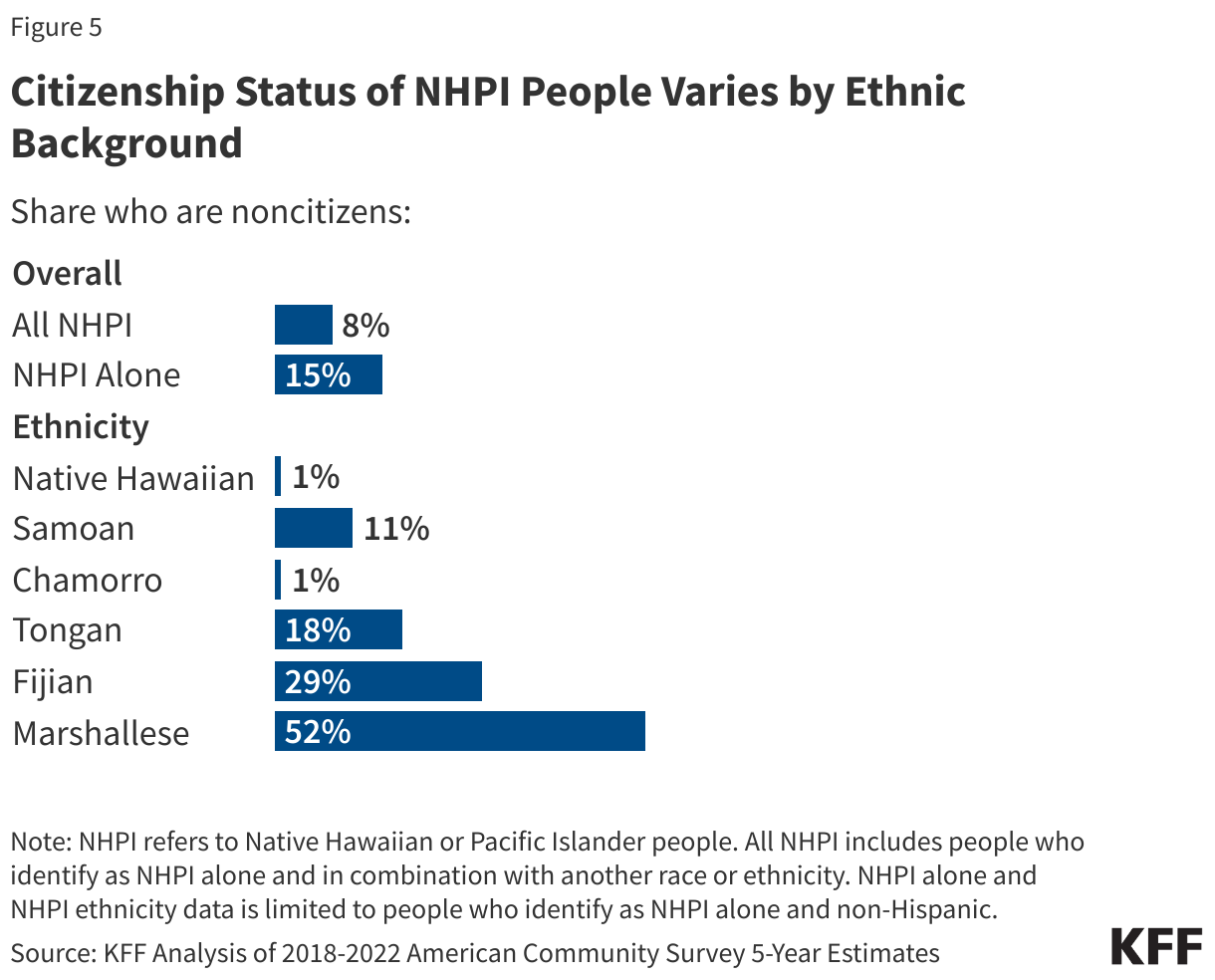
Most NHPI people (92%) living in the U.S. are. citizens, however, citizenship status varies among NHPI ethnic groups, reflecting differences in birth citizenship rights across locations to which they trace their origins. Specifically, people born in Hawaii and the U.S. territories of Guam (Chamorro people), and Northern Mariana Islands are U.S. citizens by birth. People born in the U.S. territory of American Samoa are not granted citizenship but are considered U.S. nationals. People born in the FAS, which are part of the Compact of Free Association with the U.S., are not conferred U.S. citizenship at birth, but are guaranteed the right to live, work, and access health care in the U.S. Other Pacific Islands are independent nations and therefore people born in these countries are not provided U.S. citizenship at birth. Reflecting these differences, among NHPI people living in the U.S., Native Hawaiian and Chamorro people have small shares of noncitizens (both at 1%). A larger share of Samoan (11%), Tongan (18%), and Fijian (29%) people are noncitizens, while more than half (52%) of Marshallese people are noncitizens (Figure 5).
(Back to top)
Health Coverage, Access, and Use
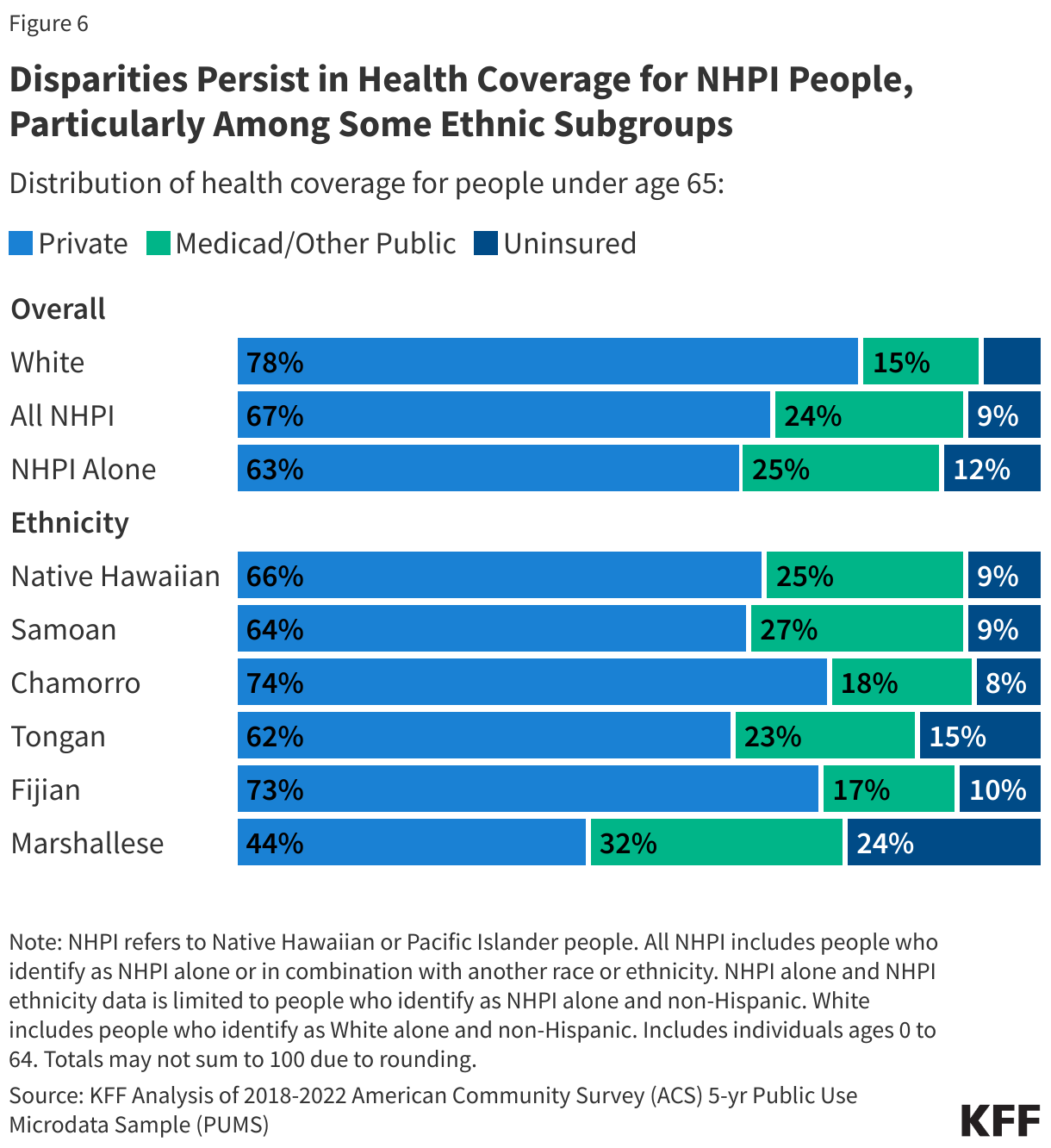
Overall, uninsured rates among NHPI people under age 65 are somewhat higher than uninsured rates among their White counterparts (9% vs. 7%) (Figure 6). This reflects lower rates of private coverage (67%) compared to White people (78%). Public coverage helps fill but does not fully offset this gap. Among people under age 65 who identify as NHPI alone, uninsured rates vary by ethnicity, ranging from about one in ten Chamorro (8%), Samoan (9%), Native Hawaiian (9%), and Fijian people (10%) to about one in seven (15%) Tongan people and about one quarter (24%) of Marshallese people.
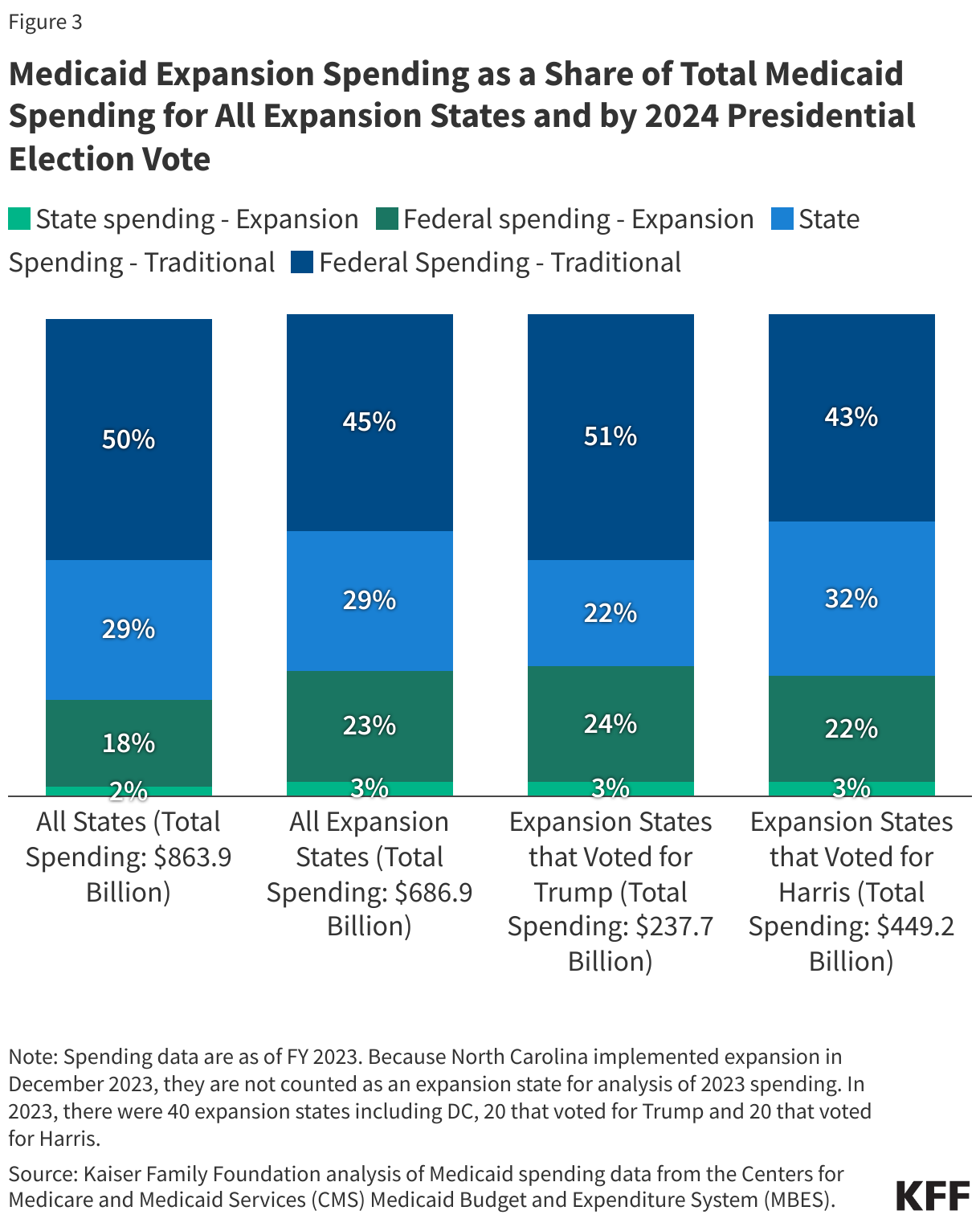
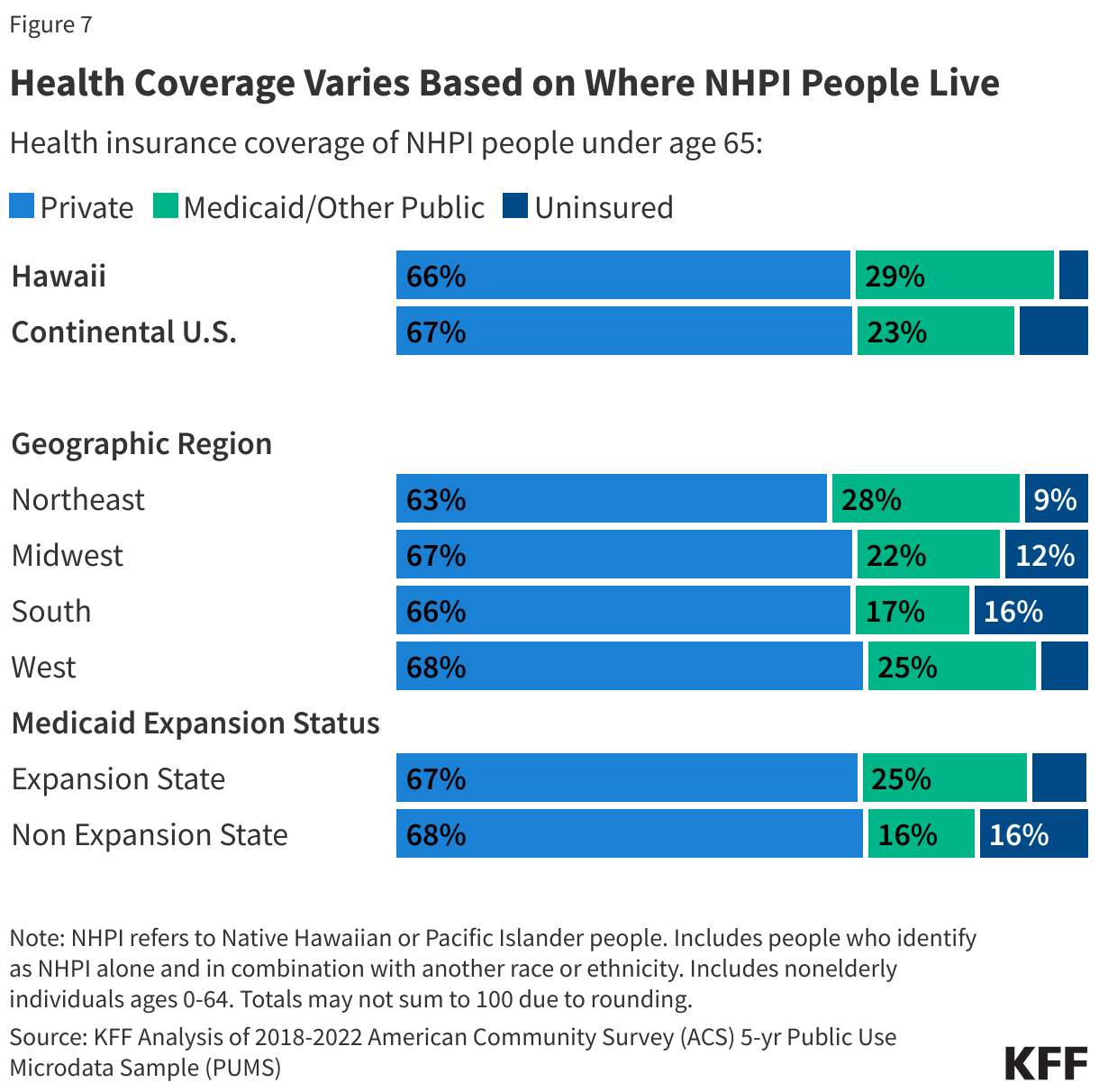
Health coverage patterns also vary based on where NHPI people live. The uninsured rate for NHPI people living in Hawaii is about half that of those living in the continental U.S. (4% vs. 10%). This pattern is largely driven by more expansive Medicaid coverage, reflecting the state’s adoption of the Affordable Care Act (ACA) Medicaid expansion for low-income adults and other eligibility expansions. Hawaii also has a longstanding mandate for employers to offer health insurance to eligible employees which facilitates access to private coverage. Uninsured rates also vary across geographic regions, ranging from 7% in the Western U.S. to 16% in the Southern U.S. These geographic patterns in part reflect differences in Medicaid expansion status among states. Many of the remaining states that have not yet adopted the ACA expansion to low-income adults are in the South. NHPI people under age 65 living in non-expansion states are twice as likely to be uninsured as those in expansion states (16% vs. 8%) (Figure 7).
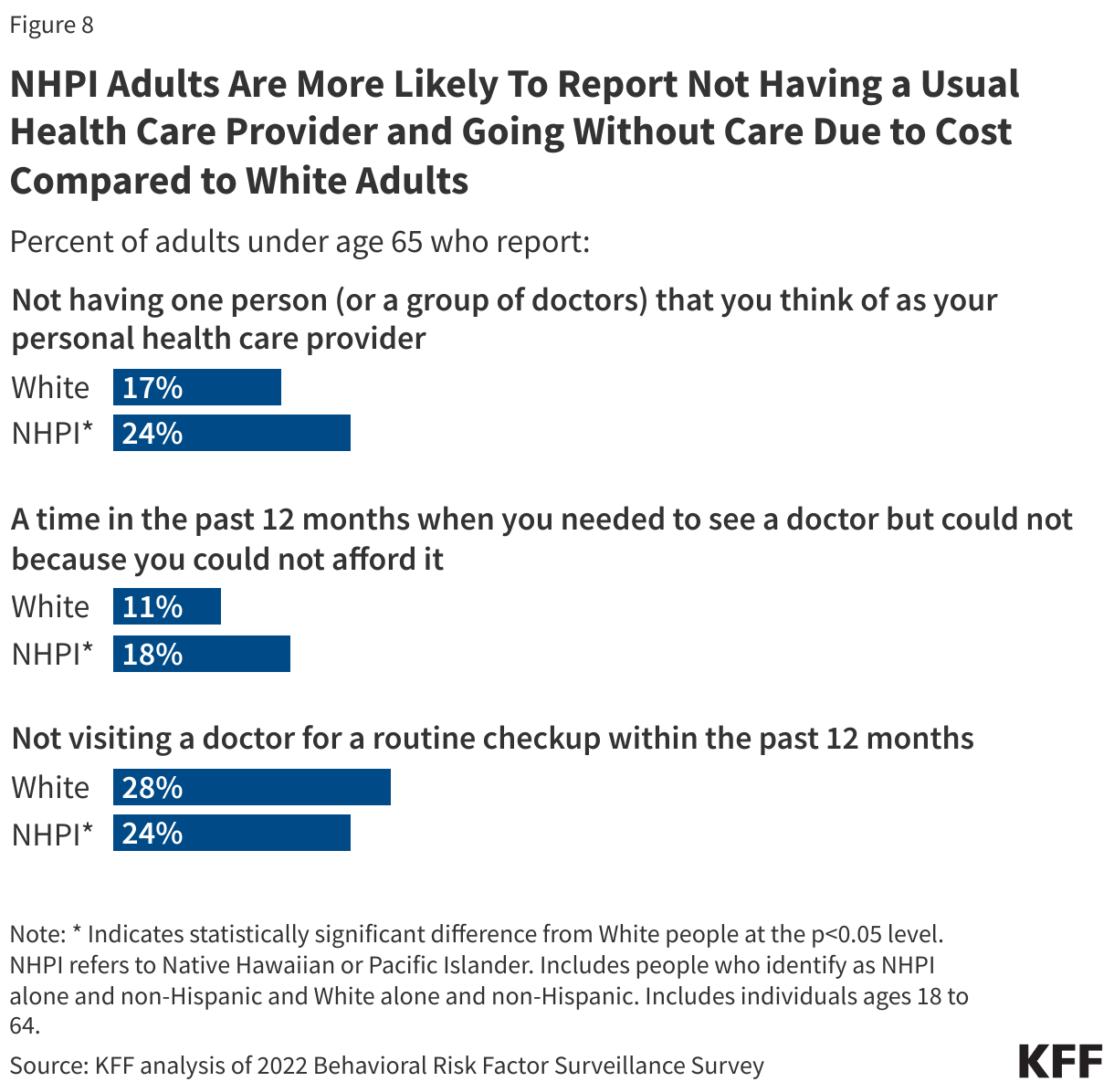
NHPI adults are more likely to report not having a usual doctor or provider or going without care due to cost than White adults but are less likely to say they went without an annual check-up. About a quarter of NHPI adults (24%) under age 65 report not having a personal provider compared to 17% of White adults (Figure 8). NHPI adults (18%) also are more likely to report not seeing a provider due to cost compared to 11% of White adults. However, NHPI adults are less likely to say they went without a routine checkup in the past 12 months than White adults (24% vs. 28%).
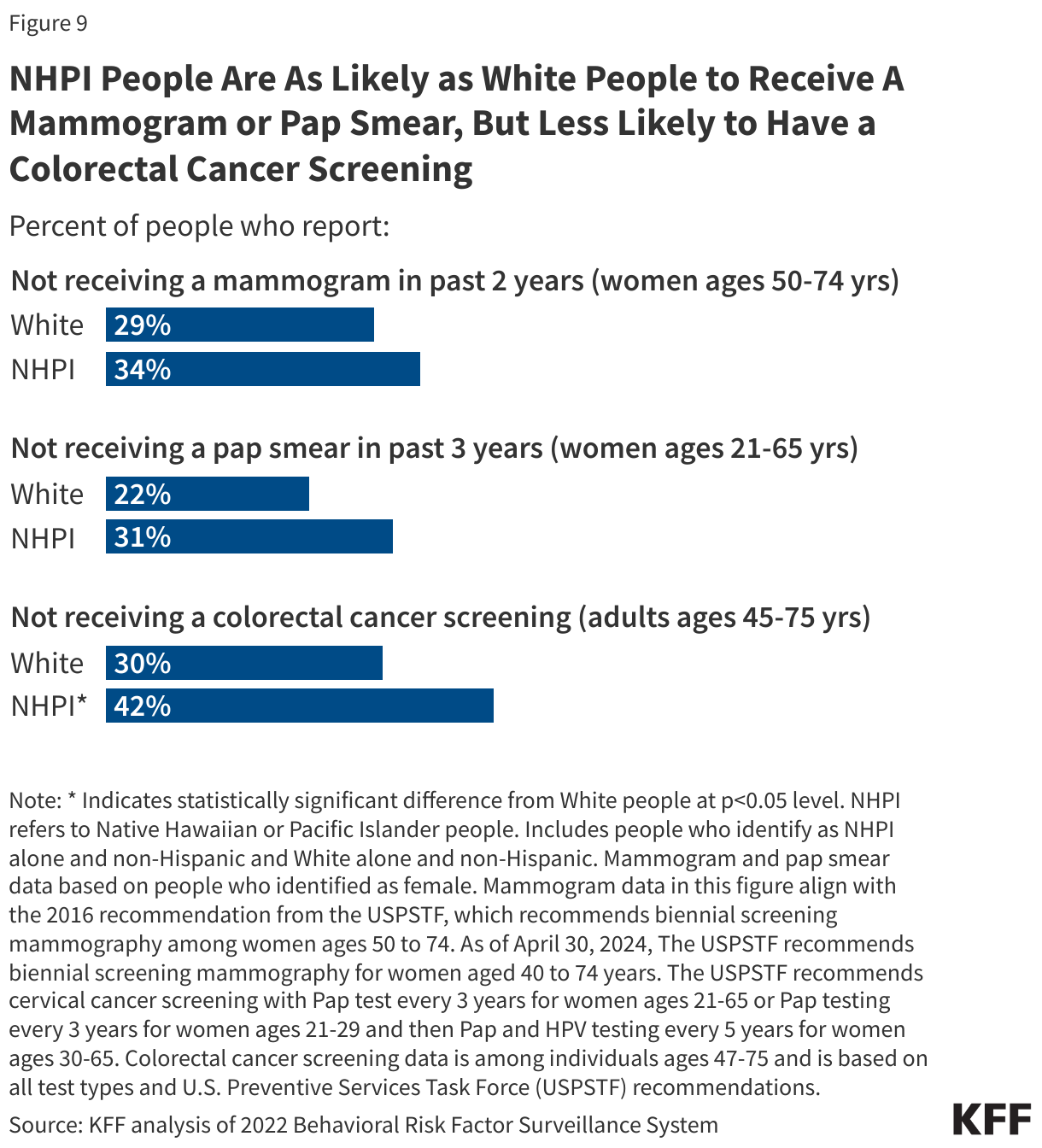
NHPI people are more likely to report going without colorectal cancer screening compared to White people but are as likely to receive a mammogram or pap smear. Among those recommended for colorectal cancer screening, about four in ten (42%) NHPI people did not receive a colorectal cancer screening compared to about three in ten (30%) White people (Figure 9). As of 2022, among women ages 50-74 (the age group recommended for screening for breast cancer prior to updates in 2024, which lowered the starting age to 40), the share of NHPI women (34%) who did not receive a mammogram in the past two years was not significantly different from the share of White women (29%). Similarly, the difference in the share of NHPI women (31%) ages 21 to 65 years (the age group recommended for screening for cervical cancer) who did not receive a pap smear was not significantly different from their White counterparts (22%).
(Back to top)
Health Outcomes of NHPI People
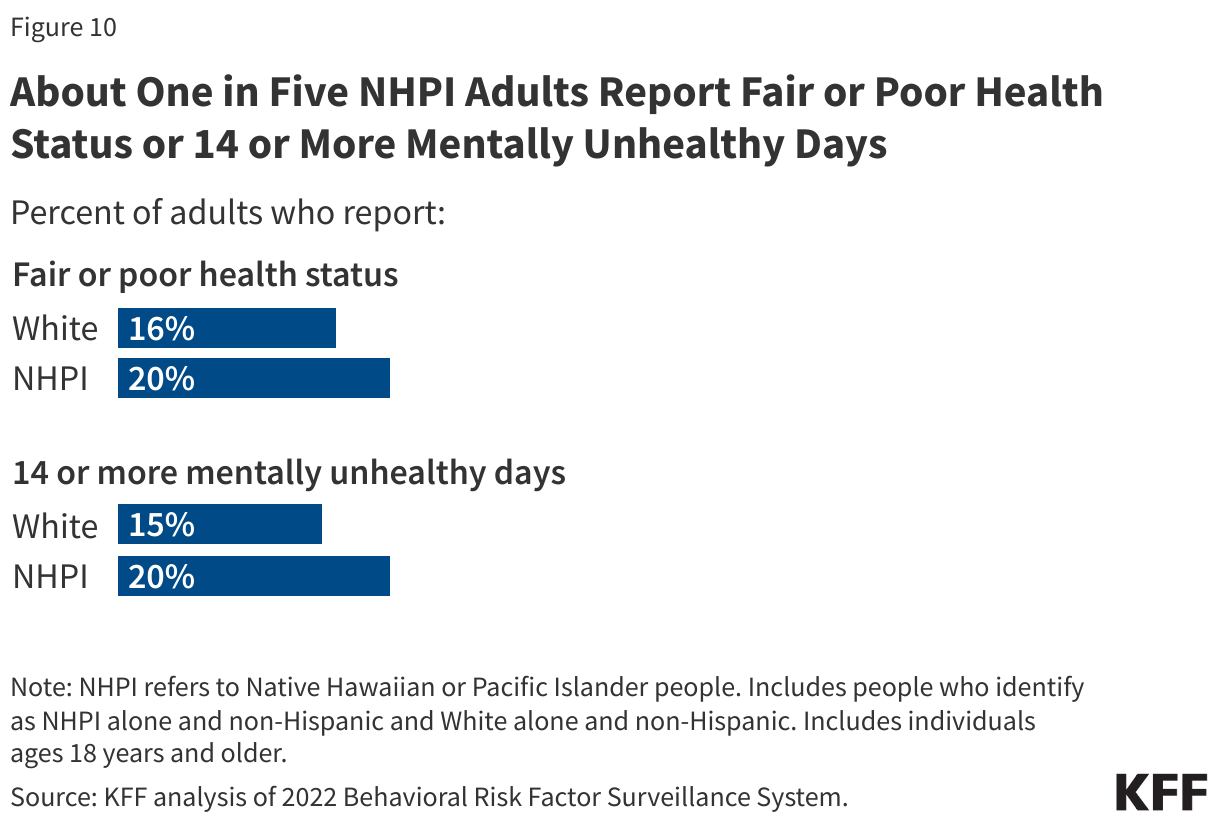
One in five NHPI adults report fair or poor health status (20%) and having 14+ mentally unhealthy days (20%), which are similar to the rates for White people (Figure 10).
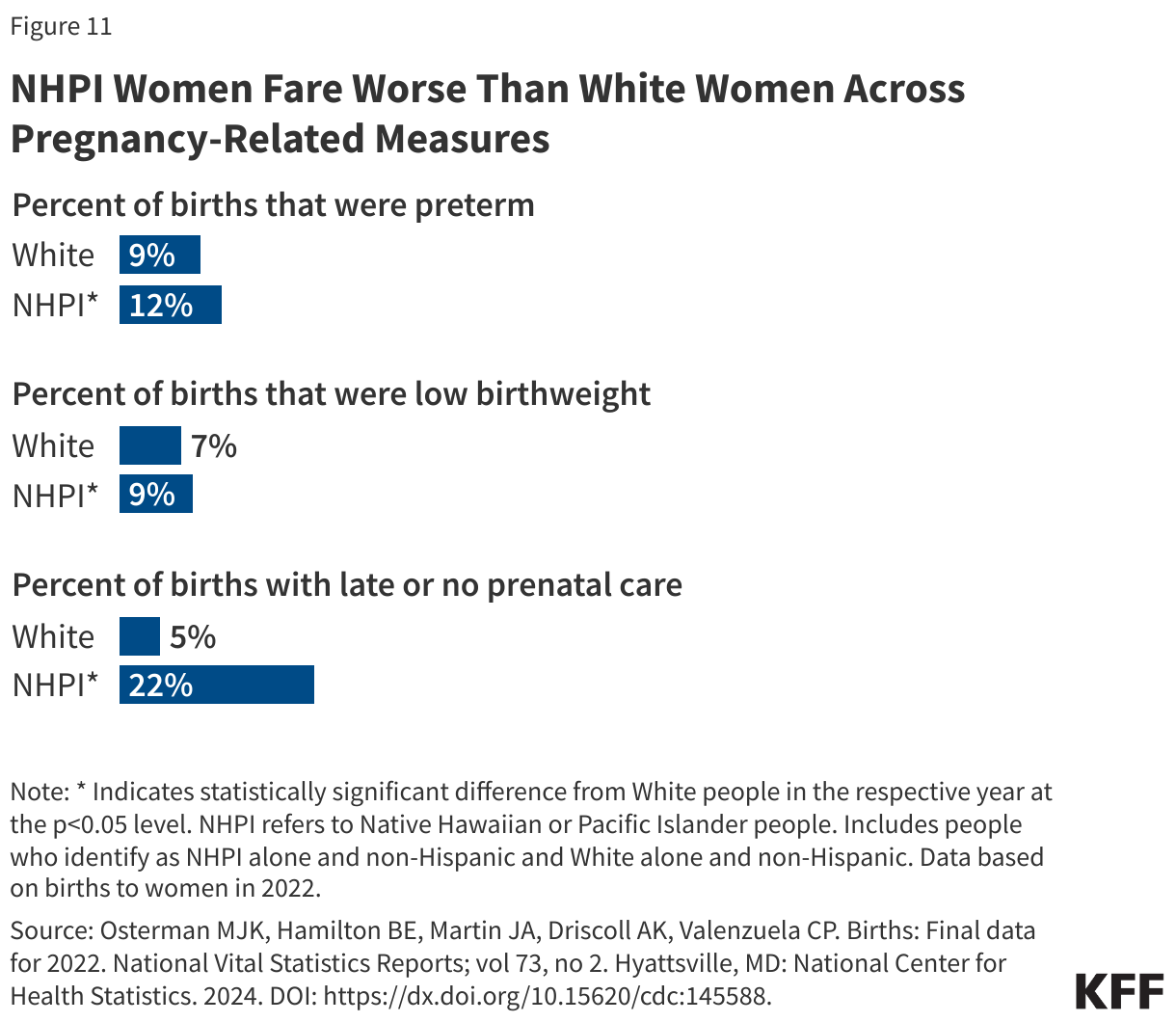
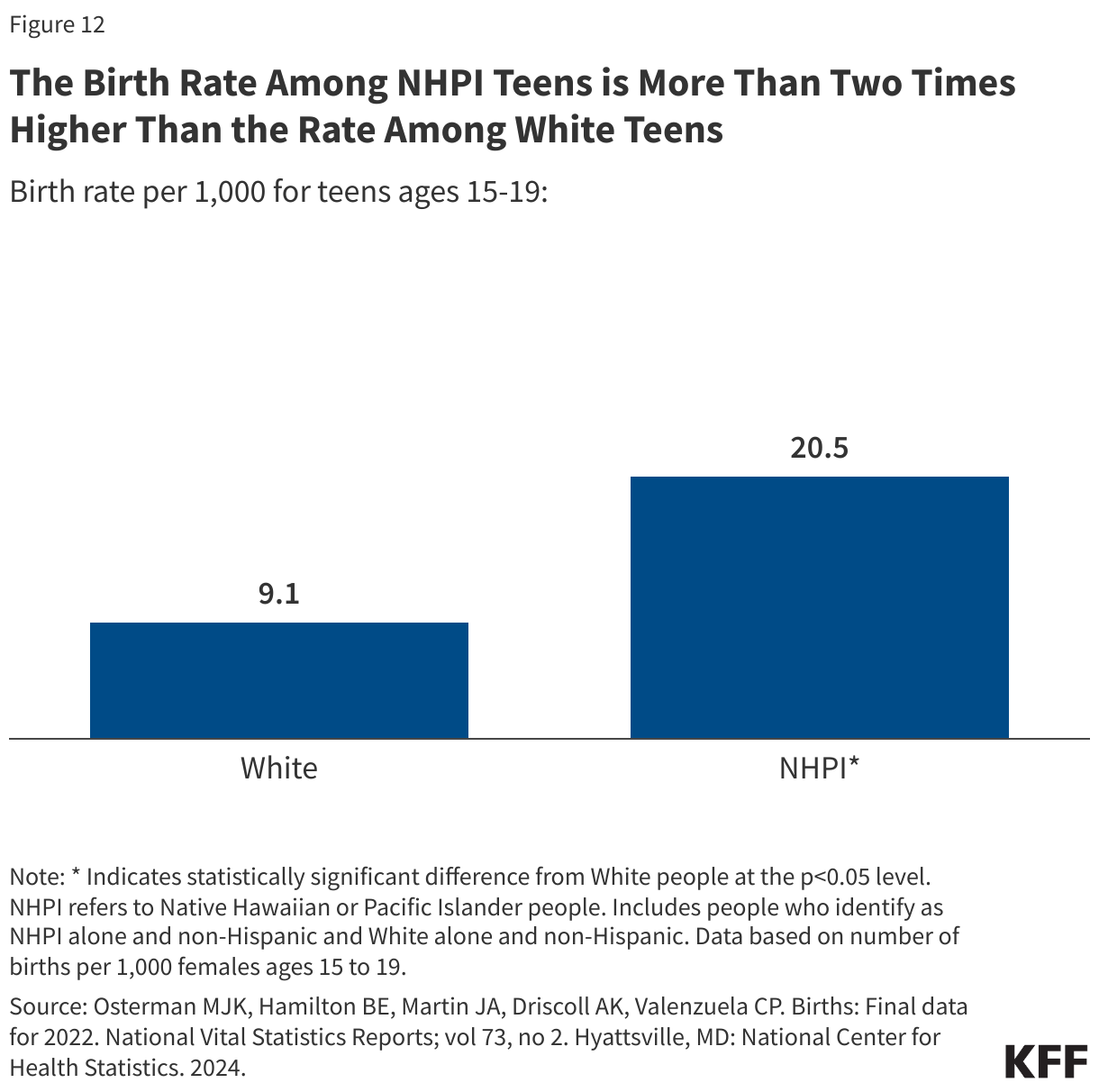
NHPI women fare worse than their White counterparts across multiple measures of birth risks and outcomes. NHPI women have higher shares of preterm births (12% vs. 9%) and low birthweight births compared to White women (9% vs. 7%) (Figure 11). Notably, NHPI women (22%) are four times more likely than White women (5%) to begin receiving prenatal care in the third trimester or to receive no prenatal care at all. Additionally, NHPI teen birth rates (20.5 per 1,000) are more than two times higher than the rate among White teens (9.1 per 1,000) (Figure 12).
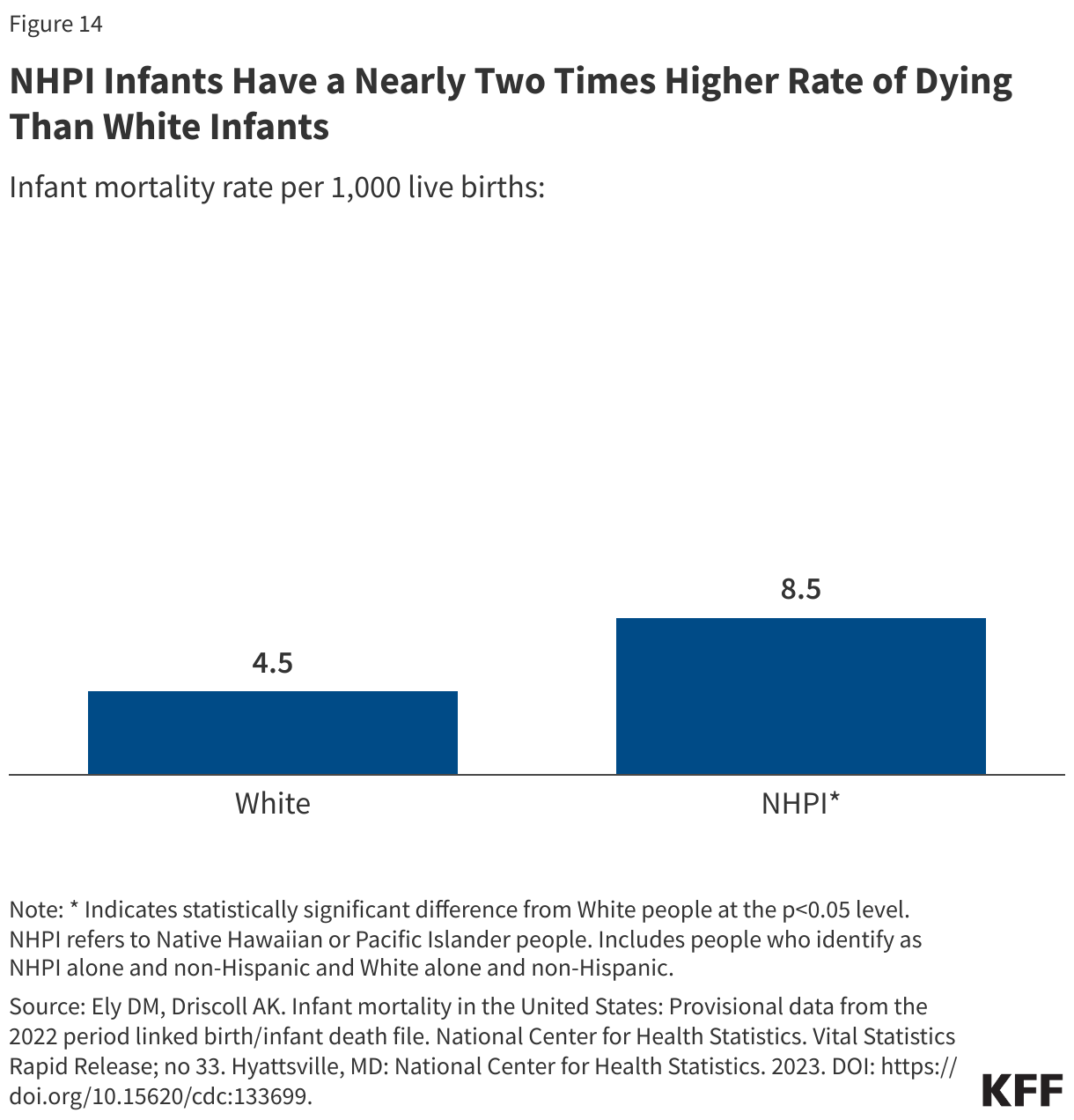
NHPI people have higher rates of pregnancy-related and infant mortality than White people. NHPI people have nearly five times higher pregnancy-related death rate than White people (62.8 vs. 14.1 per 100,000) (Figure 13). NHPI infants are nearly twice as likely to die as White infants (8.5 vs. 4.5 per 1,000) (Figure 14).
Chronic Disease
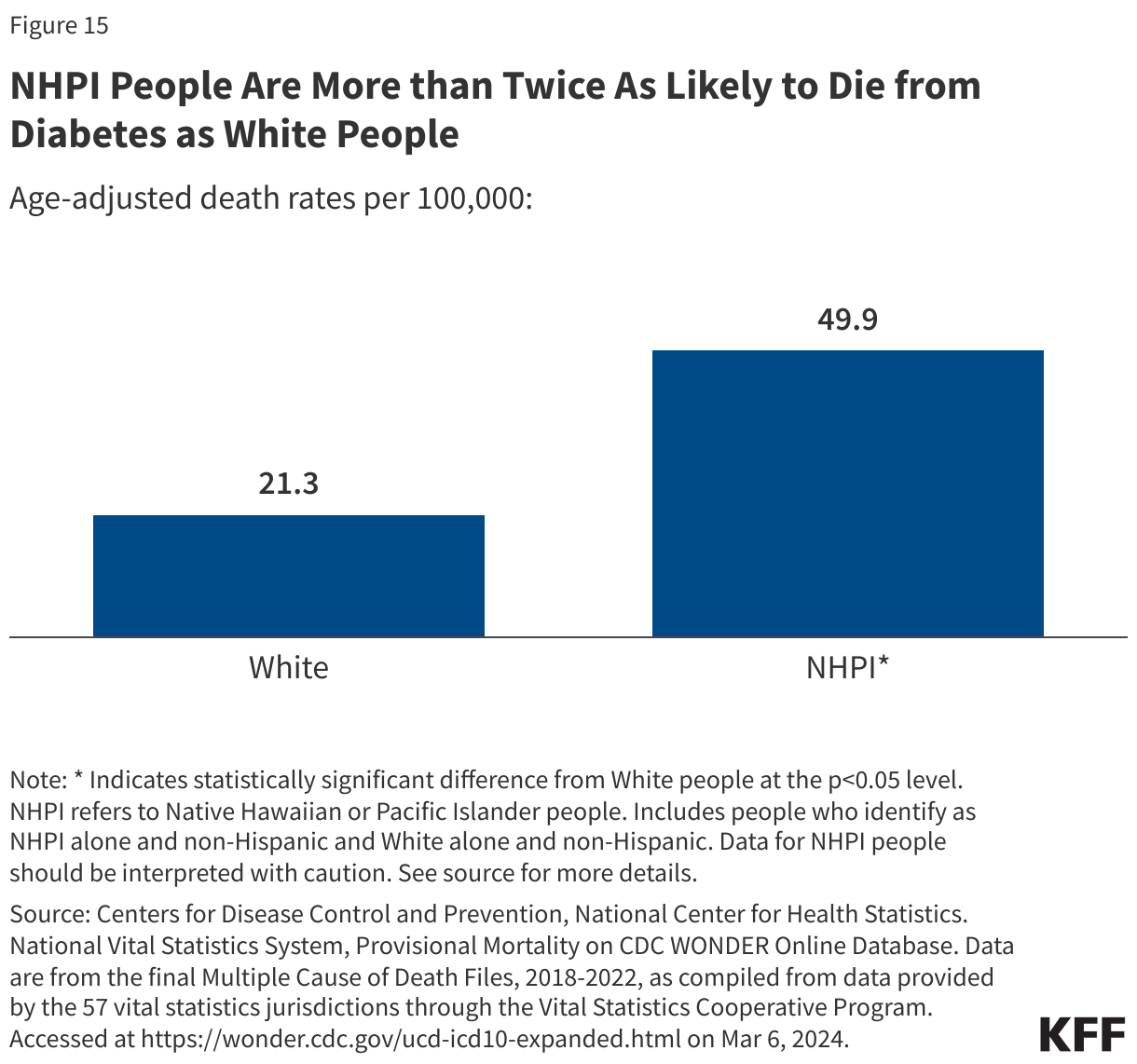
NHPI adults are more than two times as likely to die from diabetes than White adults (Figure 15). Diabetes rates for NHPI people (15%) do not statistically differ from the rate for White adults (11%), but the diabetes death rate for NHPI people is more than twice as high as the rate for White adults (49.9 vs. 21.3 per 100,000). The diabetes mortality rate for NHPI people is based on a small number of observations and should be interpreted with caution.
NHPI adults are less likely to have a heart attack or heart disease than White adults but are at similar risk of dying due to heart disease. While rates of heart attack or heart disease are lower for NHPI adults (6%) compared to White adults (8%), the rate of heart disease-related mortality is similar (173.2 per 100,000 vs. 173.1 per 100,000, respectively).
Cancer
During 2015-2019, the latest period for which disaggregated data for NHPI people were available, there were over 18,000 new cancer cases among NHPI people. Breast cancer is the most diagnosed cancer type among women across NHPI ethnic groups, as is the case for most other racial and ethnic groups, ranging from 25% among Samoan women to 44% among Fijian women. For Native Hawaiian, Samoan, Tongan, and Fijian men, the most commonly diagnosed cancer type is prostate cancer, while the most commonly diagnosed cancer for Chamorro men is lung cancer. While updated data as of 2021 is available for other racial and ethnic groups, disaggregated data on rates of cancer incidence are unavailable for NHPI people.
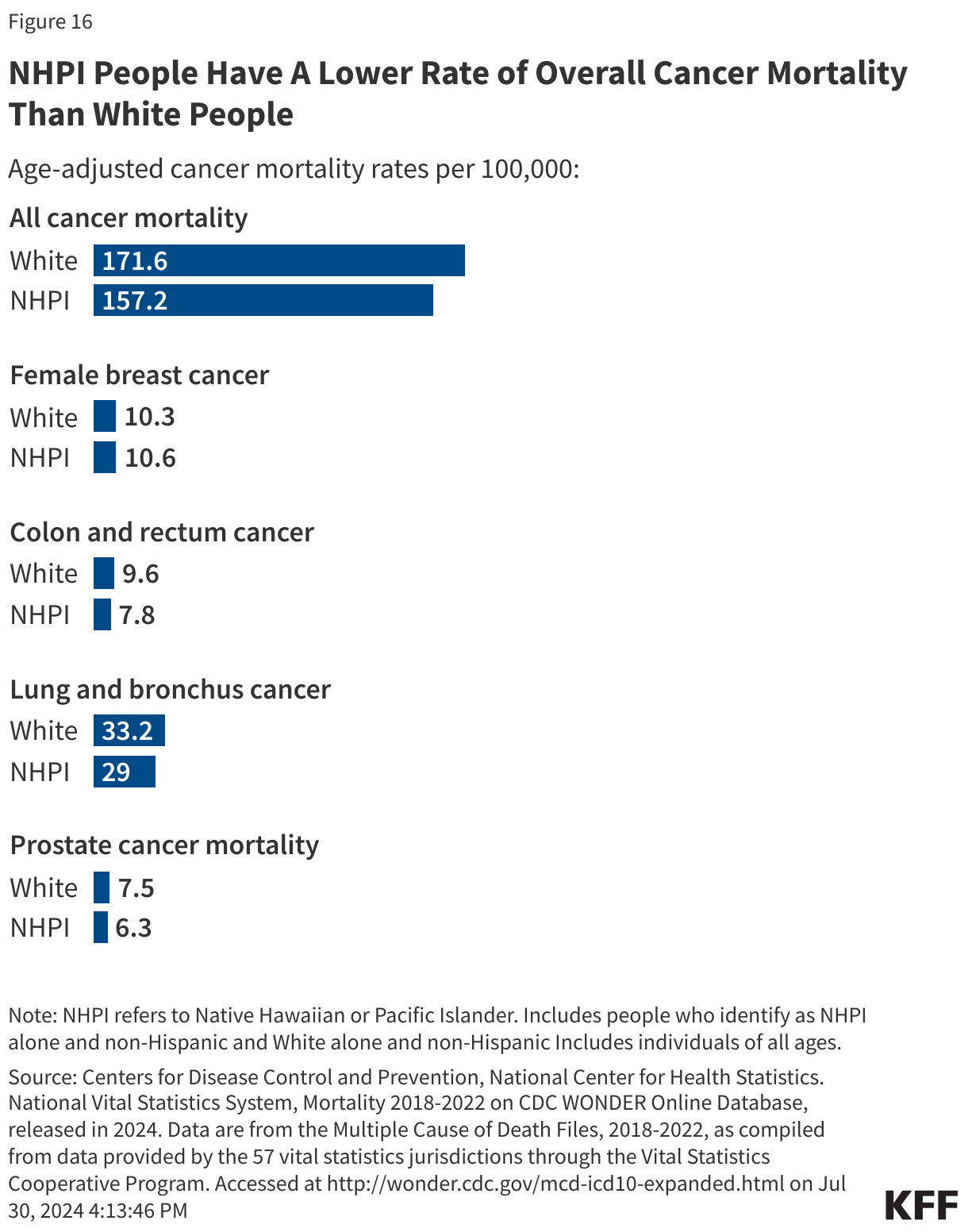
Overall, NHPI people have lower rates of cancer mortality than White people across most types of cancer. NHPI people have lower rates of all cancer-related deaths than White people (157.2 per 100,000 versus 171.6 per 100,000) (Figure 16). NHPI people have similar rates of female breast cancer mortality than White people (10.6 vs. 10.3 per 100,000). They have lower mortality rates of colon and rectum cancer (7.8 vs. 9.6 per 100,000), lung and bronchus cancer (29 vs. 33.2 per 100,000), and prostate cancer (6.3 vs. 7.5 per 100,000).
Mental Health
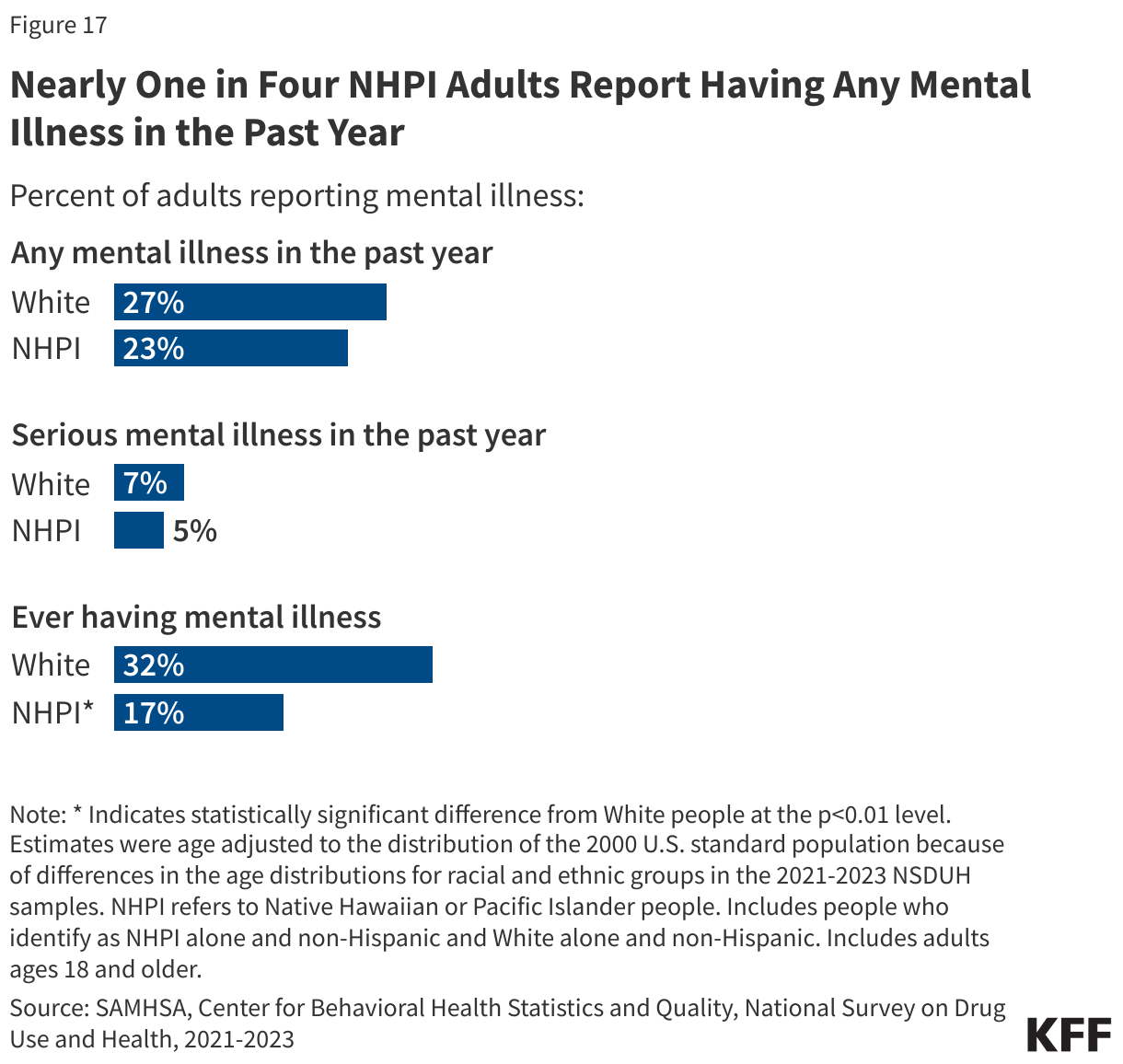
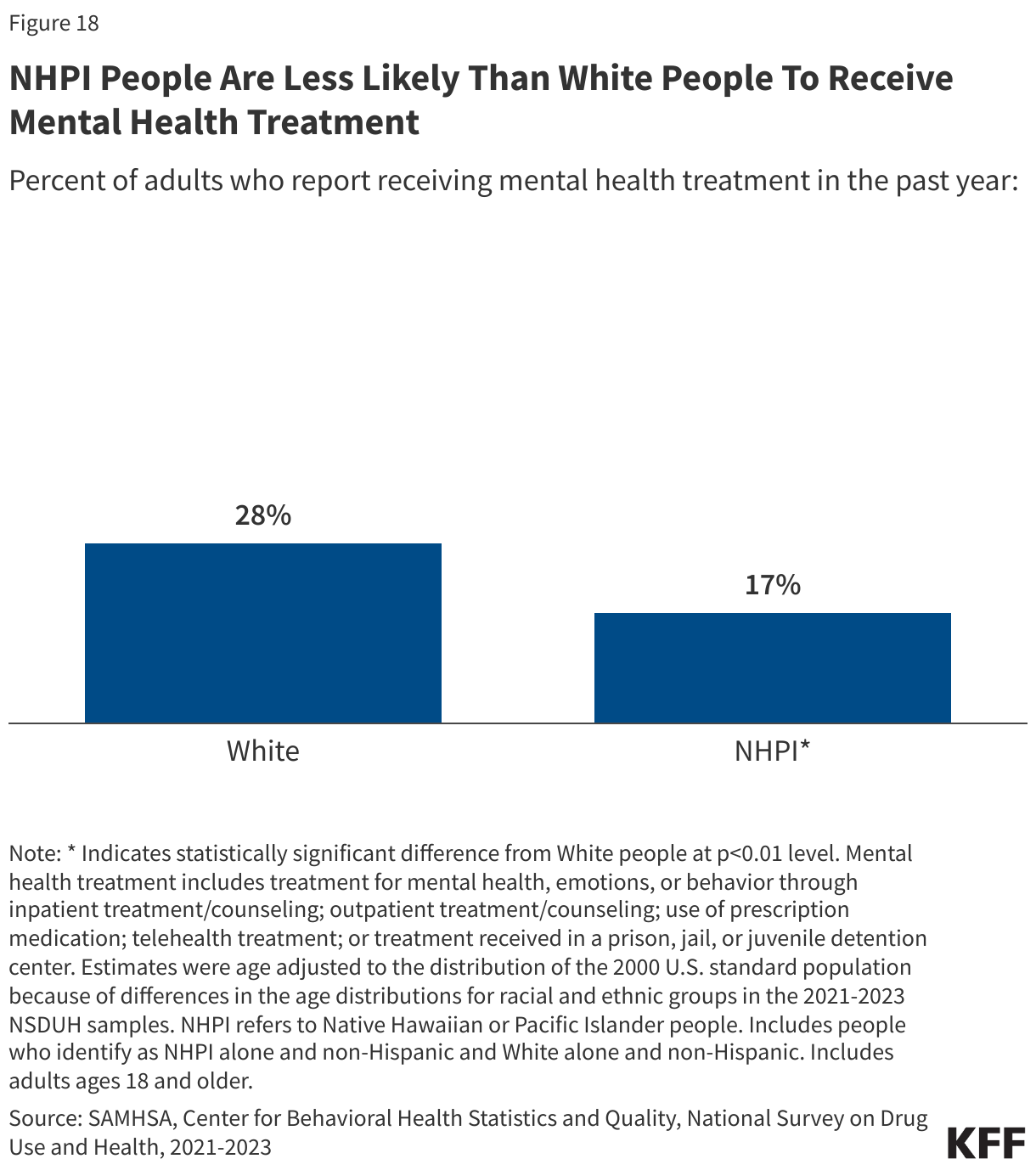
Reported rates of mental illness among NHPI people are similar to White people, but research suggests mental illness could be underdiagnosed among NHPI people. About one quarter of NHPI adults (23%) report experiencing any mental illness in the past year, similar to their White counterparts (27%). The share of NHPI adults reporting serious mental illness is also similar to White adults (5% vs 7%) (Figure 17). NHPI people (17%) are nearly half as likely to report ever having mental illness compared to White people (32%). However, research suggests that a lack of culturally sensitive screening tools that detect mental illness, coupled with structural barriers could contribute to underdiagnosis of mental illness among people of color.
NHPI people are less likely to receive treatment compared with White people. 16% of NHPI people report receiving treatment in the past year compared to over one in four White people (26%) (Figure 18).
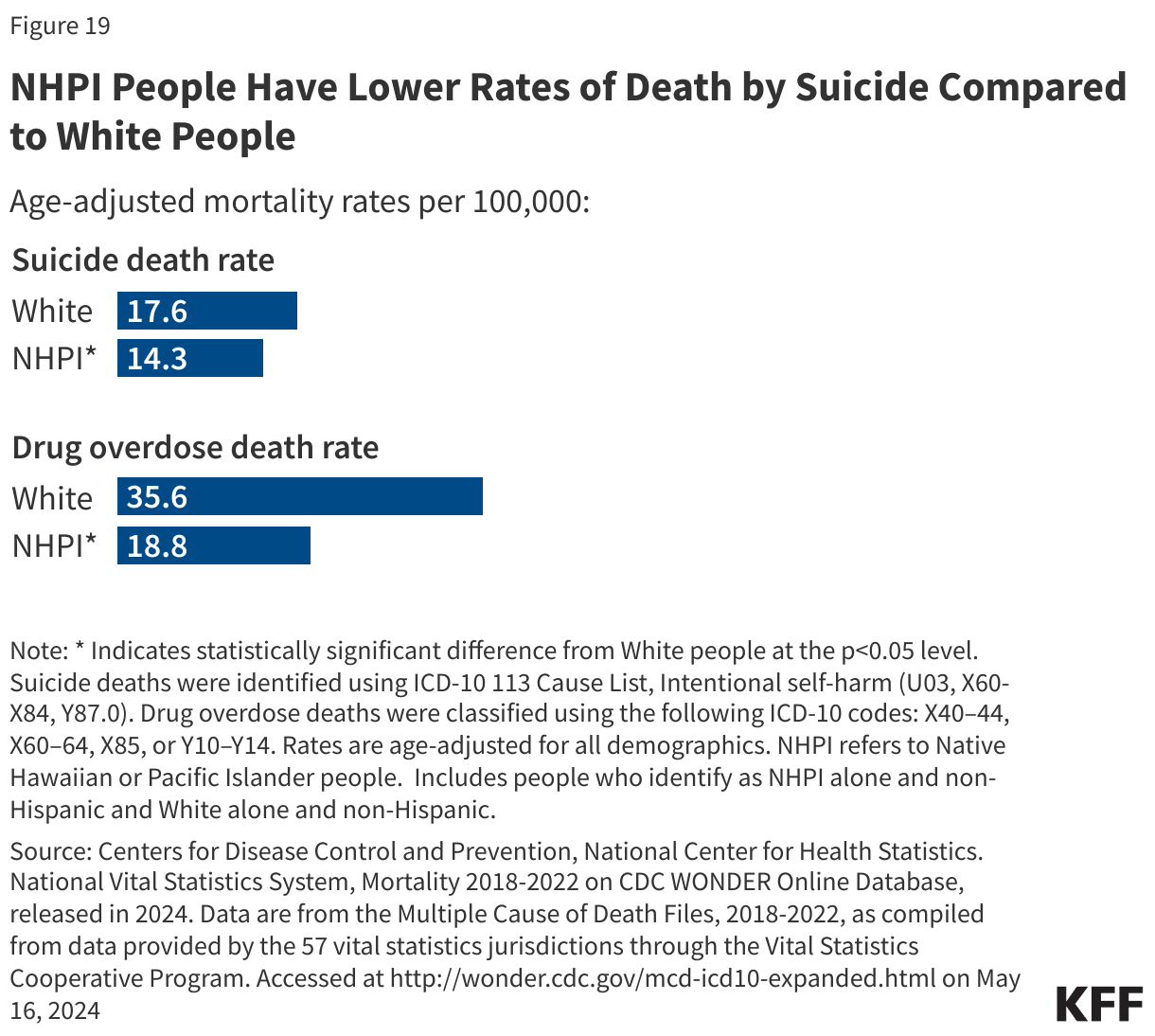
NHPI adults have lower rates of deaths by suicide and drug overdose than White people (Figure 19). As of 2022, the suicide death rate for NHPI adults (14.3 per 100,000) is lower than the rate for White adults (17.6 per 100,000). Between 2011 and 2021, Asian or Pacific Islander people experienced a faster increase in suicide death rates than White people. The data was not disaggregated and therefore the changes observed cannot specifically be attributed to Asian or NHPI racial groups, alone. Suicide data are not available for NHPI adolescents. NHPI adults have roughly half the rate of drug overdose deaths than their White counterparts (18.8 vs. 35.6 per 100,000). Between 2022 and 2023, the number of opioid overdose deaths among Asian or Pacific Islander people declined by 2%, a smaller decline than that of White people (-14%). Opioid overdose death data are combined for Asian and Pacific Islander people.
(Back to top)
Social And Economic Factors that Influence Health
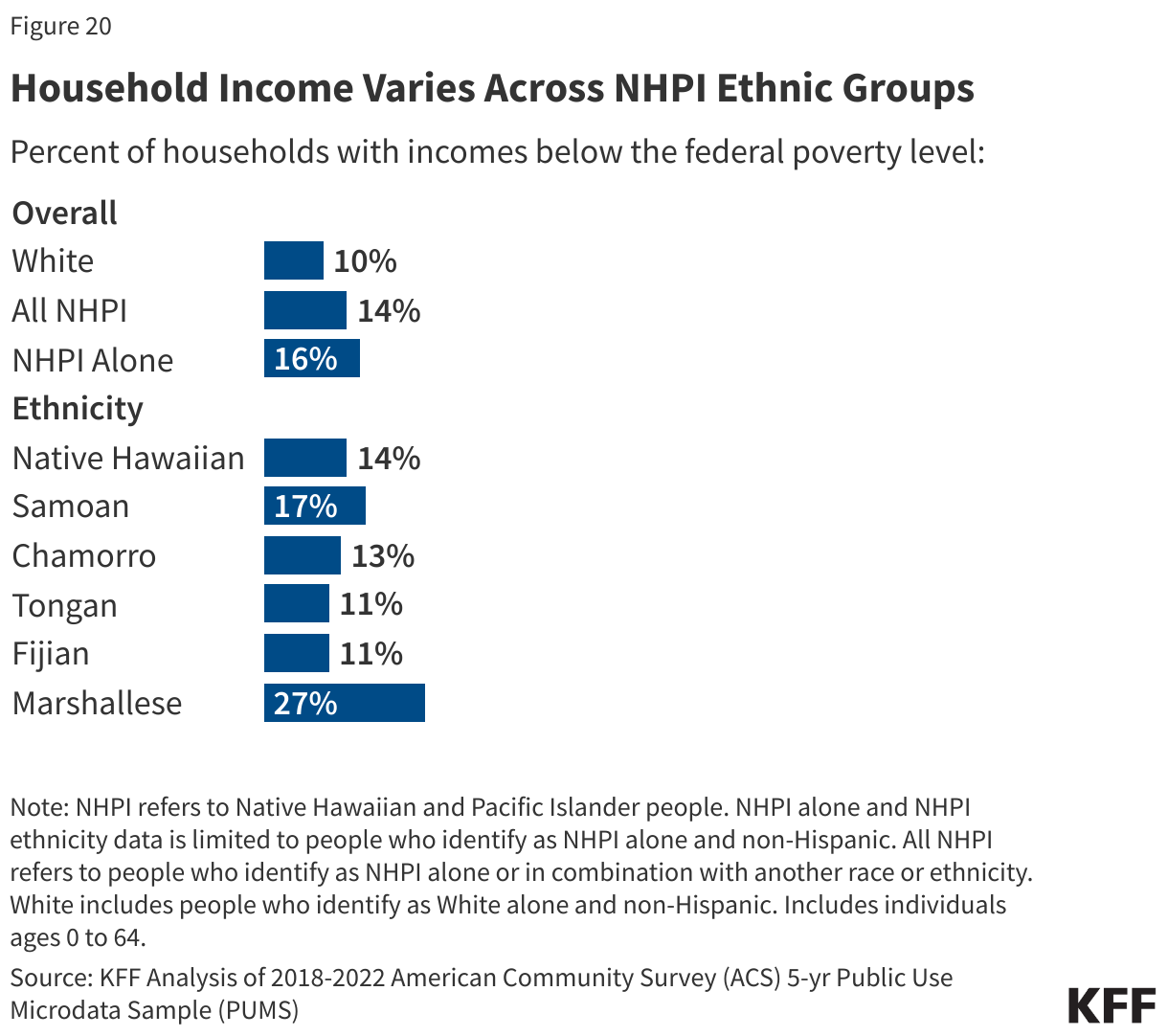
Across ethnic groups, most NHPI people are in working families, but there is significant variation in family income among NHPI people. Most NHPI people under age 65 are in a family with at least one worker (77%). Although the majority are in working families, NHPI people under age 65 are more likely to have income below the poverty level than their White counterparts (15% vs. 10%), with the share ranging from 11% among Tongan and Fijian people to 27% among Marshallese people (Figure 20).
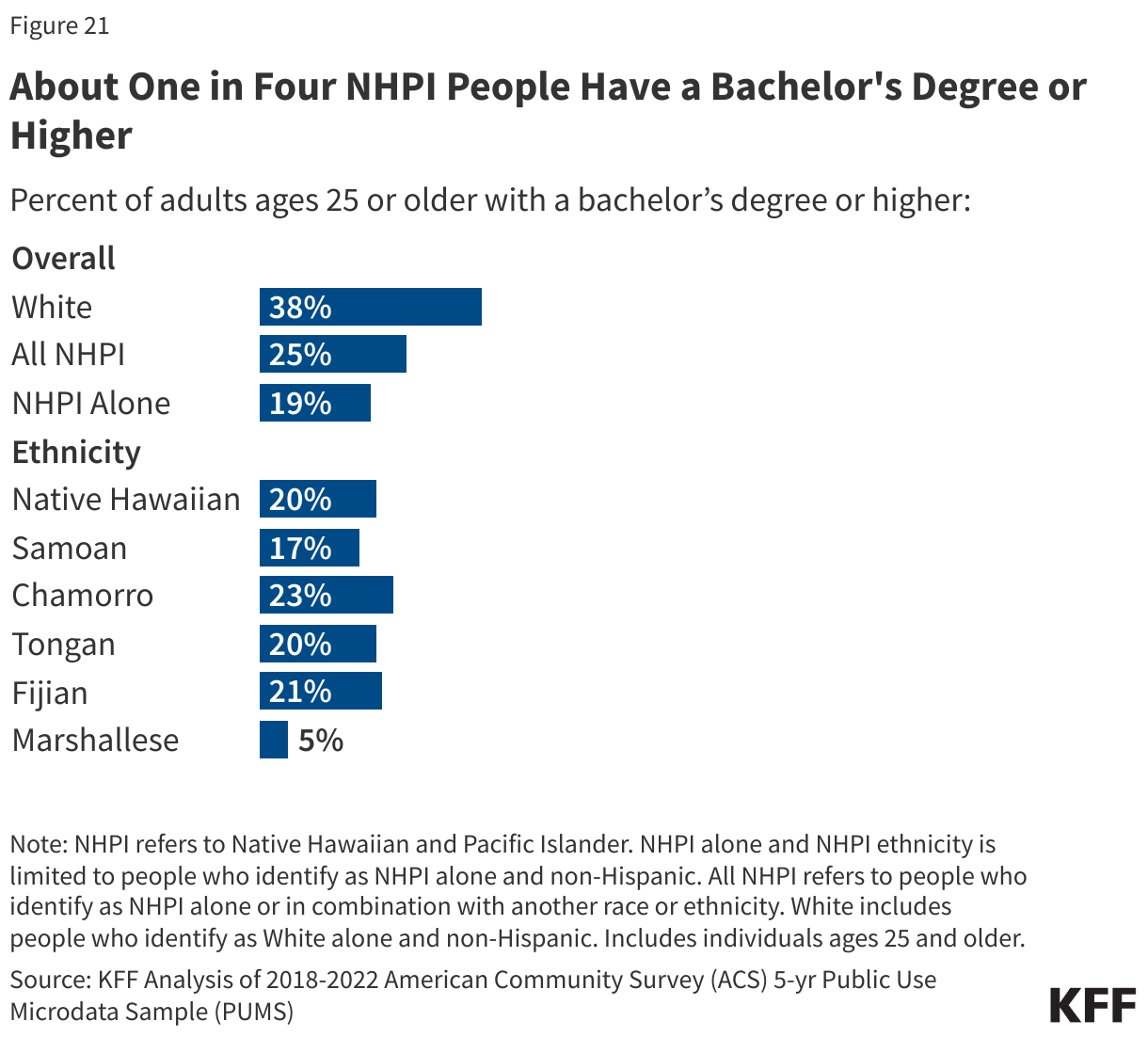
NHPI people have lower educational attainment compared to White people, but there is significant variation among NHPI people. Among adults ages 25 and older, one in five adults who are NHPI alone (19%) and one quarter of all NHPI adults (25%) report having a bachelor’s degree or higher compared to nearly four in ten White adults (38%) (Figure 21). Among NHPI people, the share with a bachelor’s degree ranges from 5% of Marshallese people to nearly one quarter (23%) of Chamorro people.
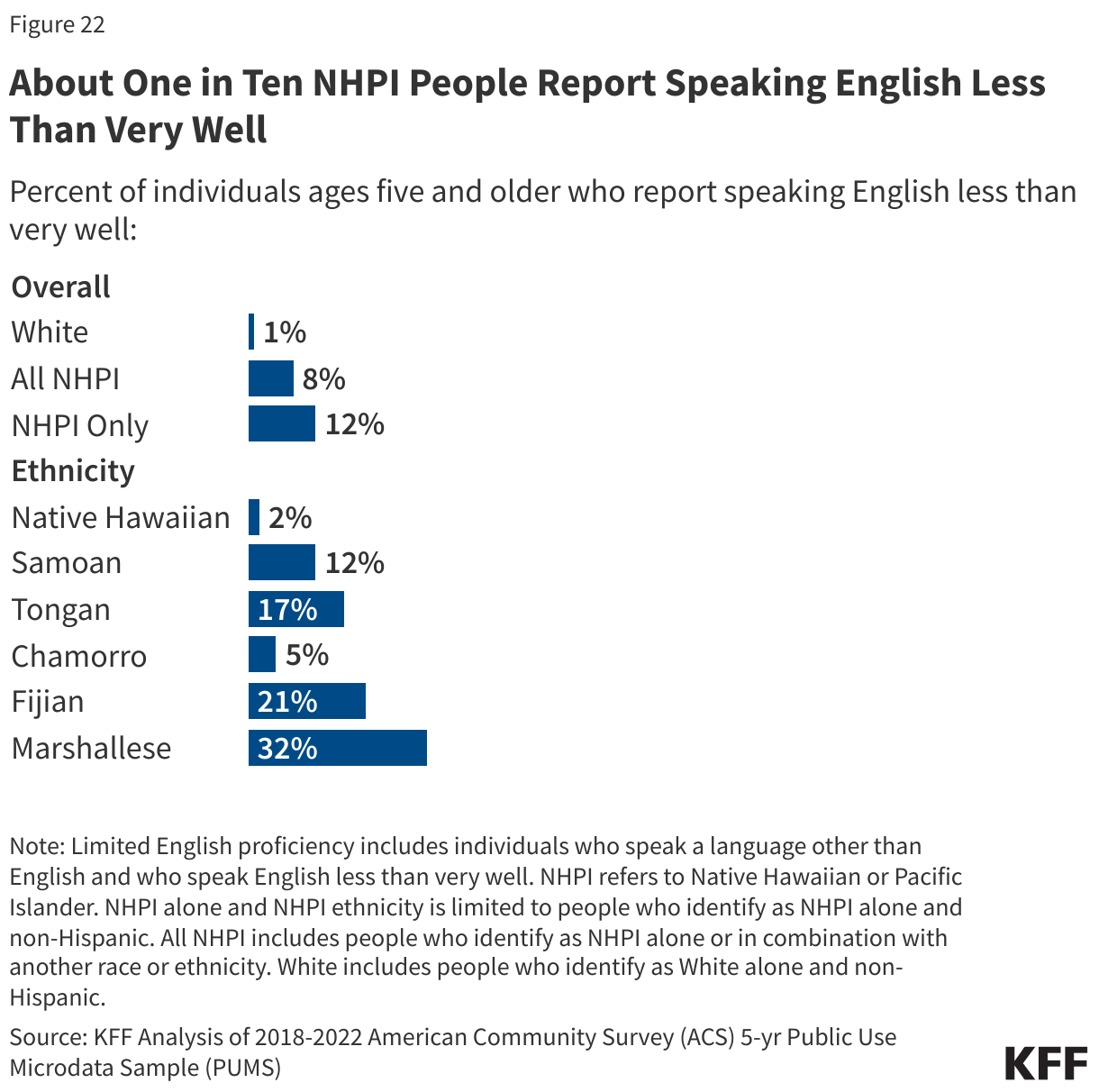
About one in ten (8%) NHPI people report speaking English less than very well compared to one percent of White people (Figure 22). Among NHPI people, limited English proficiency varies by ethnicity, ranging from about 2% of Native Hawaiian people to 5% of Chamorro people and one third of Marshallese people (32%). 17% of Tongan people and about one in five Fijian people (21%) report speaking English less than very well.
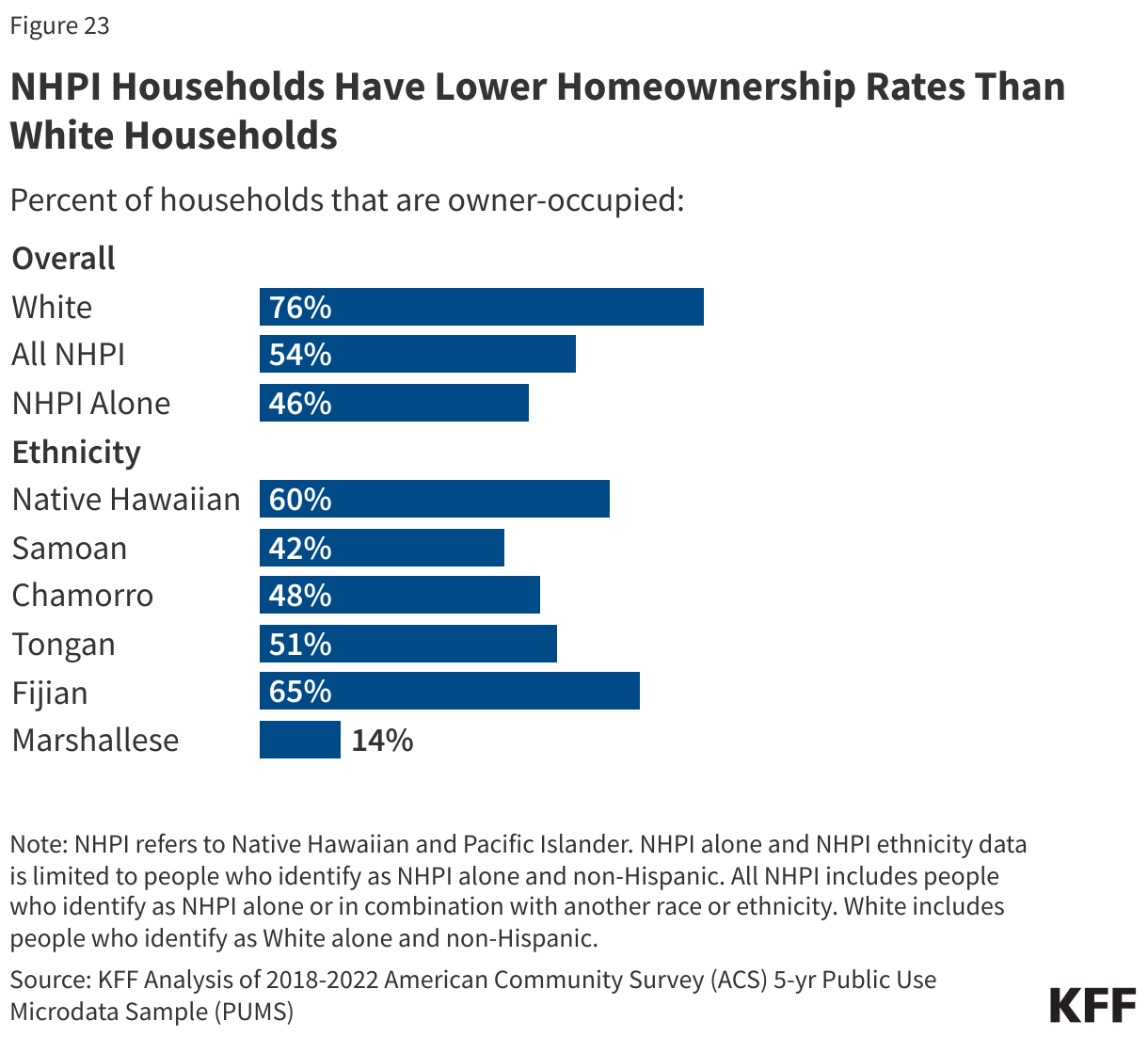
Overall, NHPI households (54%) have lower rates of homeownership compared to White households (76%) (Figure 23). Homeownership rates vary among NHPI people, ranging from about one in seven Marshallese households (14%) to about roughly half of Tongan households (51%), six in ten Native Hawaiian households (60%), and about two thirds of Fijian households (65%). Despite U.S. promises to return ancestral lands to Native Hawaiian people under the Hawaiian Homes Commission Act of 1920, home ownership rates among NHPI people in Hawaii remain at 56%. Some of the barriers to homeownership faced by Native Hawaiians include the high cost of living and the failures and long waitlists under the Hawaiian Homes Commission Act. The Maui wildfires have further increased housing demand and may exacerbate barriers to homeownership.
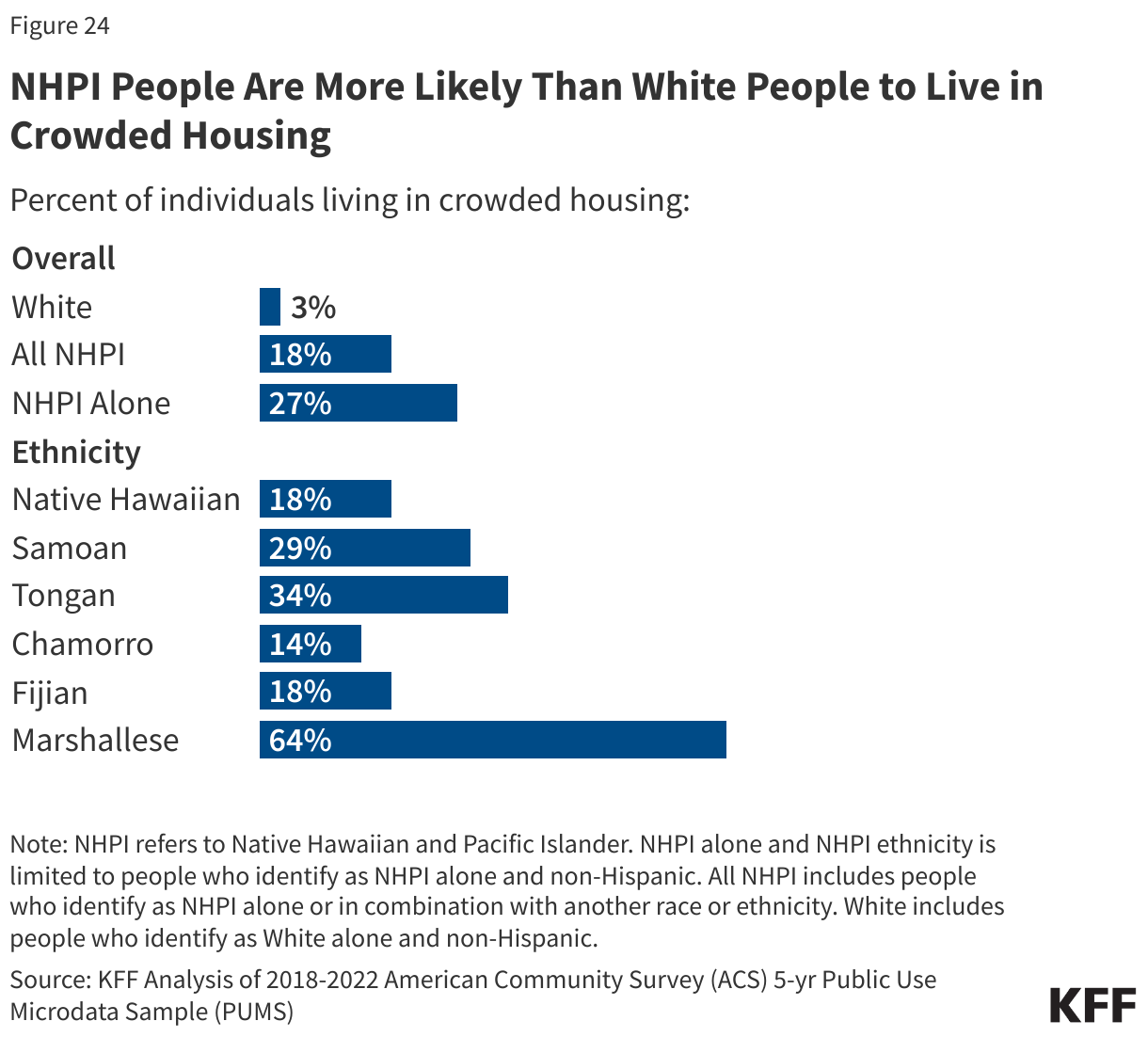
NHPI people are more likely to live in “crowded” housing compared to White people, and this share is higher among NHPI people living in Hawaii compared to those living in the continental U.S. (Figure 24). Nearly one in five (18%) people who identify as NHPI alone or in combination with another race or ethnicity and about a quarter of people who identify as NHPI alone (27%) report living in crowded housing compared to 3% of White people. “Crowded housing” is defined as housing with more than one occupant per room (not counting bathrooms, porches, balconies, hallways, or unfinished basements, etc.). Among NHPI people, the share of people living in crowded housing ranges from 14% for Chamorro people to 64% for Marshallese people. About three in ten (29%) NHPI people living in Hawaii report living in crowded housing compared 7% of White people living in Hawaii and to 15% of NHPI people in the continental U.S. NHPI people have the highest share of people living in multigenerational housing —households containing three or more generations— compared to other racial and ethnic groups, which may contribute to the higher share reporting crowded housing. Family is considered a core value in NHPI culture and is defined very broadly to include extended family. Consequently, living in multigenerational households is more common among NHPI people and is considered a strength within the community. Additionally, Hawaii consistently ranks as the most expensive state to live in, which can also lead to crowded housing conditions.
(Back to top)