What Does the Future Hold for Ending the HIV Epidemic Initiative (EHE)?
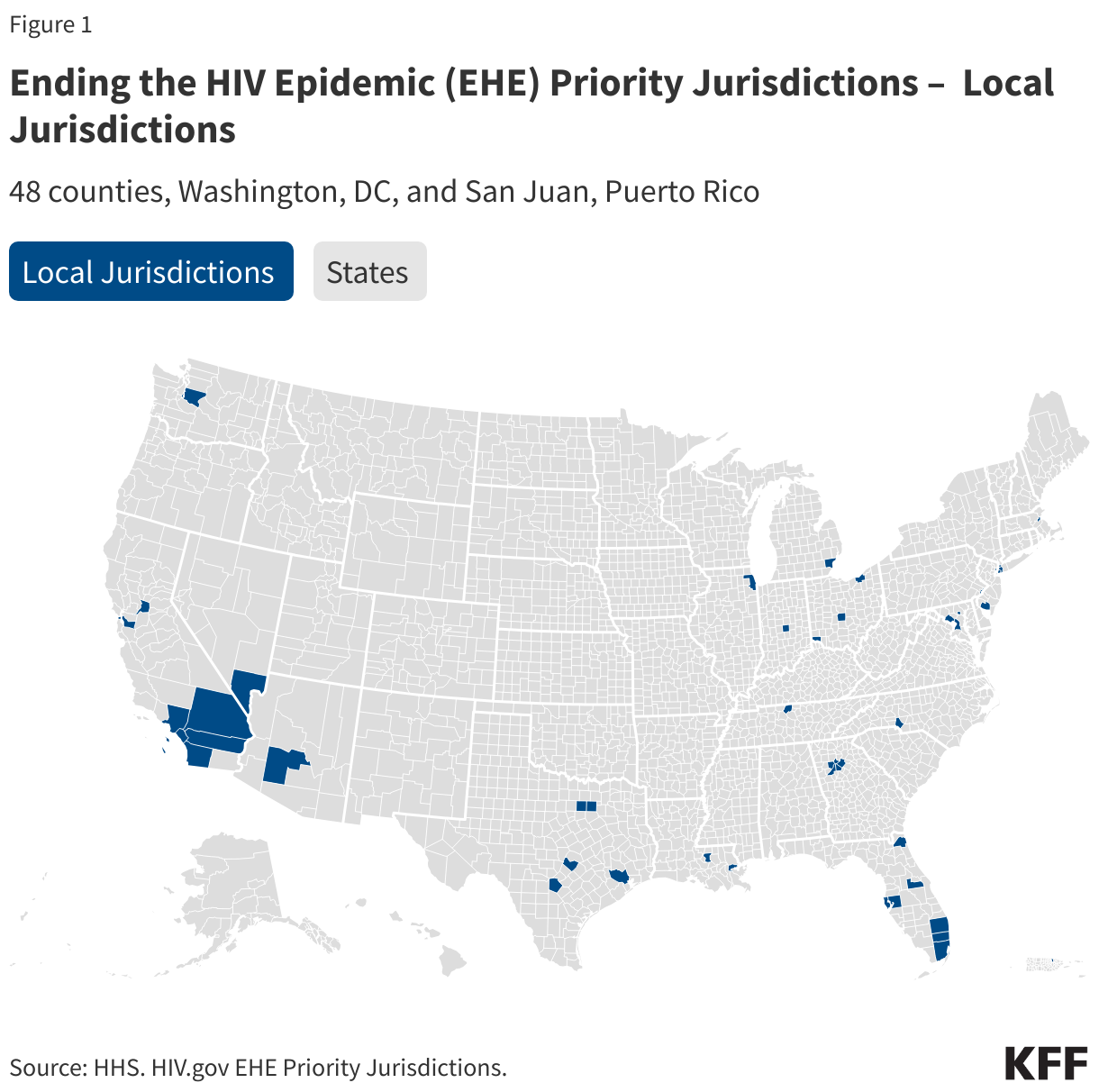
The Ending the HIV Epidemic Initiative (EHE) is a federal effort to address the HIV epidemic in the United States, by bringing new resources aimed at reducing the number of infections. EHE set the ambitious goals of reducing HIV incidence by 75% in five years and by 90% in ten years by focusing activities within four “pillars”: diagnose, treat, prevent and respond. The effort prioritizes 48 counties that had the highest number of HIV diagnoses between 2016 and 2017, San Juan, Puerto Rico, Washington D.C., and seven states with a substantial rural burden. It was created by the first Trump Administration, announced during the 2019 State of the Union, and continued by the Biden Administration. While there has been no formal announcement, a leaked document detailing budget and restructuring plans for the Department of Health and Human Services (HHS) suggests there will be significant changes to the federal HIV response, including eliminating the EHE. The leaked document is not official policy and not a final budget request. While Congress could still theoretically fund the initiative, it appears the Trump Administration is not currently planning to champion the effort.
This analysis examines what EHE has done to date and what its future might look like under the new administration.
What has the EHE done?
Funding
One of the primary changes the EHE made to the federal HIV landscape was to increase funding to core HIV programs, particularly the Centers for Disease Control and Prevention’s (CDC) HIV prevention branch and the Health Resources and Services Administration’s (HRSA) Ryan White HIV/AIDS Program. For many years, HIV funding at these core programs had been relatively flat and not keeping pace with inflation, increasing biomedical costs, and increases in HIV prevalence. The EHE infused new federal funding into these programs, as well as to HIV efforts at HRSA’s Health Centers program, the National Institutes of Health (NIH), and the Indian Health Service (IHS). In its first year, 2019, a small amount of funding was reprogrammed from other accounts to support the EHE and in FY 2020, Congress provided new funding which has continued over time. In FY 2024, the last budget year with known appropriated levels, EHE funding totaled $573.25 million, with the largest allocations going to CDC for prevention ($220 million) and Ryan White for care and treatment ($165 million). While these amounts represented the first major increases for these and other programs, they represent a fairly small increase in overall budgets. With these small increases, recipient agencies were able to conduct a range of activities to support the four pillars as discussed below. (See KFF’s EHE Funding Tracker for details on EHE funding.) Loss of EHE funding would return these programs to funding levels of a decade ago.

EHE Activities
EHE funding has supported the following activities across a range of HHS agencies:
- The Ryan White HIV/AIDS Program (within HRSA) is the nation’s HIV safety-net program providing care, treatment, and support services to about half of all people with HIV. EHE funding extends the reach of the program and especially focuses on engaging people who are newly diagnosed in HIV care and treatment and reengaging others who have fallen out-of-care. It also supports training activities. Specific outcomes from Ryan White EHE efforts inlcude:
- The number of clients newly engaged in care and served by EHE-funded Ryan White providers nearly doubled between 2020 (11,792) and 2022 (22,001), an increase of 87%.
- The estimated number of clients re-engaged in HIV care and served by EHE providers nearly tripled between 2020 (7,085) and 2022 (19,204), an increase of 171%.
- EHE funding also afforded grantees greater flexibility to cover certain services more comprehensively, such as psychiatry, intensive case management, housing, and trauma-informed care, among others.
- The health center program (also within HRSA) provides care to tens of millions of people, including for those with limited resources. Health centers have historically provided some HIV care and prevention services and EHE allowed them to extend their reach in this area. Specific outcomes from Health Center EHE efforts inlcude:
- The number of patients served with PrEP services in EHE funded health centers increased by 26% (compared to a 4% increase across health centers nationwide) between 2021 and 2023.
- The number of HIV tests conducted increased by 119% in EHE funded health centers (compared to a 62% increase across health centers nationwide) between 2020 and 2023 .
- In 2022, 55% of clients (ages 15-65) in EHE funded health centers had ever been tested for HIV compared to 37% of clients in health centers that did not received EHE funding.
- Between 2020 and 2023 the share of health center patients diagnosed with HIV for the first time increased by 52% among those served within EHE funded health centers, compared to 32% between nationwide.
- In 2022, 86% of patients in EHE funded health centers were seen within 30 days of first HIV diagnosis, compared to 76% in non-EHE funded health centers.
- The share of health center patients with an HIV diagnosis increased 6% between 2019 (196,218) and 2023 (207,970), likely reflecting increases in HIV testing and linkage to care. (Data from KFF analysis of the HHS/HRSA Uniform Data System (UDS) 2019-2023.)
- The Centers for Disease Control and Prevention is the backbone of U.S. HIV prevention efforts and supports EHE funded jurisdictions in developing local implementation plans to meet specific local needs, culture, and environments and providing resources to implement those plans. As such jurisdictions plans differ from one another and therefore success metrics for how CDC funding is used vary within each location but can include increasing PrEP uptake, reducing testing barriers, leveraging telehealth, for example. Specific outcomes between 2021 and 2023 include the use of CDC EHE funds to:
- Provide >600,000 free HIV self-test kits
- Provide >1 million HIV tests, newly diagnosing 4,600 people with HIV
- Link 84% of people newly diagnosed with HIV to care within 30 days
- Provide PrEP to 61,000 people
- The National Institutes of Health, home to most federal HIV research funding and efforts, plays a role in EHE as well, to inform HHS and partners on evidence-based practices and effectiveness, including through making awards to Centers for AIDS Research (CFARs) and AIDS Research Centers (ARC) with research ranging thematically across centers.
- Between FY19-FY23 NIH funded 248 projects with EHE funding with about half of projects focusing on HIV prevention and others focusing on diagnosis, treatment, and response.
- Research findings are disseminated through publications, meetings, presentations, trainings/workshops, town halls, and across government.
- The Indian Health Services (IHS) also receives EHE funding to address the HIV and other syndemics within Indian Country. IHS EHE funding supports three-year cooperative agreements (Ending the HIV Epidemic in Indian Country (or ETHIC)) to seven tribal/urban Indian organizations for work aimed at eliminating the syndemics of HIV, hepatitis C, and STIs. Among other activities, EHE funding has allowed awardees to:
- create the HIV/HCV/STI Branch within the Office of Clinical and Preventive Services at IHS Headquarters and hire clinical and administrative staff
- increase HIV/HCV/STI testing (IHS EHE-supported sites performed over 20,000 HIV test)
- increase linkage to care
- attend HIV syndemic-related training
What Does the Future Hold for EHE?
While the EHE brought new funding for HIV services across the country and that funding has driven a range of new activities aimed at addressing HIV, it now appears the new Trump administration will discontinue funding these efforts. Ending EHE aligns with several administration actions which have sought to limit HIV funding and reduce the size of the HHS workforce, with those working in HIV related fields especially impacted. Multiple branches within the CDC’s Division of HIV Prevention were also eliminated and grantees have reported delays in receiving funding. In addition, recent reports that the administration seeks to cut CDC HIV prevention funding and the retraction of HIV related NIH grants also raises questions about its commitment to addressing HIV more broadly. The administration is also seeking to conduct a reorganization within HHS, including with the creation of a new agency, the Administration for a Healthy America (AHA). Per the press release, there are plans for AHA to consolidate activities from the Office of the Assistant Secretary for Health (OASH), HRSA, and other agencies. AHA will consist of multiple divisions, including one on HIV/AIDS. The leaked document appears to move the Office of Infectious Disease Policy (OIDP) at HHS to AHA. OIDP led on the EHE effort, providing coordination, management, and tracking progress, was thought to have initially been eliminated after all staff were let go in the earlier wave of firings. The Ryan White Program would also move to AHA and the document proposes eliminating the program’s EHE line as well as support for dental services, AIDS Education and Training Centers, demonstration programs, and the Minority AIDS Initiative.
While the leaked document is not formal policy, loss of EHE funding, federal coordination, leadership, expertise, and support, could reverse or stall recent successes. EHE jurisdictions would lose added flexibility that came with EHE funding at a time when state health budgets are strained and threats of Medicaid costs shifting to states loom. Such changes have the potential to lead to increases in new HIV infections, as well as disruptions in HIV care, both of which will have individual and population level impacts, setting back the recent gains made by the EHE.