The Trump Administration’s Foreign Aid Freeze and Global Health: The Biggest Gaps Left on the Donor Landscape
With the Trump administration instituting a foreign aid freeze, including a stop-work order, cancelling the vast majority of foreign aid grants and contracts, and moving to dismantle USAID, U.S. global health programs have been effectively shuttered. Even the limited waivers that have been granted for some services have not resulted in any significant funds flowing or services offered, according to multiple lawsuits and other reports.
This situation presents considerable risks to the health of millions of people in low- and middle-income countries, given the role the U.S. has played in this area. Indeed, the U.S. government has been the largest donor to global health for decades, carving out health one of its main sectors of international development, across multiple administrations and Congresses, through the provision of significant financial assistance, technical expertise, and personnel. However, this has also meant that the U.S. has disproportionately shouldered the burden for health programs, making health especially vulnerable to U.S. policy fluctuations and changes, and especially to the recent, abrupt halt in funding.
A recent analysis from the Center for Global Development identified countries most vulnerable to these cuts. This analysis examines the relative role of the U.S., compared to other donors (governments as well as multilateral institutions), in global health. We used disbursement data from the Organisation of Economic Development (OECD) Creditor Reporting System (CRS), averaged over a three-year period (2021-2023), to smooth out spending fluctuations (all totals and percent share present the per year average over the period). We focused on bilateral donor spending (e.g., the funding a donor gives directly to or on behalf of specific countries) vs. multilateral spending (e.g., the funding a donor gives to a multilateral institution that is then pooled with other donor contributions and provided to countries) because such funding is attributed to the multilateral institution as the donor in the CRS database. In addition, at this time, no U.S. government funding to the main multilateral funders of global health services has been halted. We looked at overall health spending as well as spending for HIV, tuberculosis (TB), and malaria. We removed COVID-19 funding given that it was emergency in nature and not enduring. Due to lack of available data, this analysis does not include domestic funding from recipient countries that are also used for health and in some case may be significant, although in general, GDP growth in low and middle income countries continues to lag due to the effects of COVID-19 and many face significant debt burdens that limit their ability to increase resources for health.
As this analysis shows, given that the U.S. has been the largest donor to global health, the gap left, should cuts and disruption continue, would be quite significant. This is especially true in the case of HIV for which the U.S. provides almost two-thirds of bilateral assistance. In addition, there are several countries that could be disproportionately affected by U.S. cuts, given that they are both very low-income and rely heavily on the U.S. for health assistance. Whether other donors, or countries themselves, would be able to make up such losses is unknown but seems unlikely given broader global economic trends.
Findings
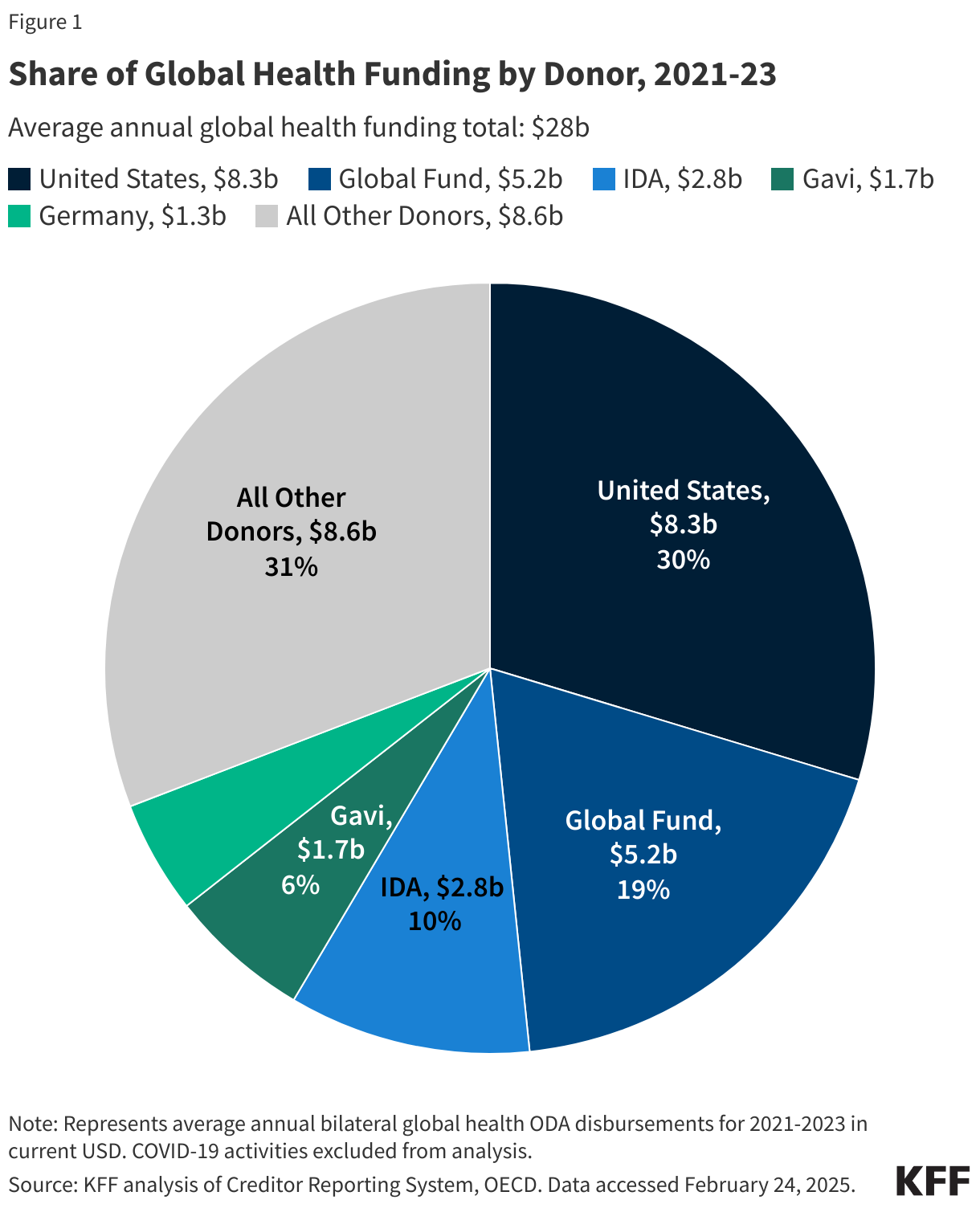
The U.S. government was the single largest donor to health in low- and middle-income countries over the 2021-2023 period. The U.S. provided 30% of all health assistance, or $8.3 billion per year in bilateral support. The next largest donor was the Global Fund to Fight AIDS, Tuberculosis and Malaria (Global Fund), providing 19% or $5.2 billion each year over the period. The third largest donor was the World Bank’s International Development Association (IDA) (10% or $2.8 billion per year), followed by Gavi, the Global Alliance for Vaccines and Immunization (Gavi) at 6% ($1.7 billion per year) Germany (5% or $1.3 billion per year). All other donors each represented less than 5%. See Figure 1. It is important to note that government donors also fund multilateral entities focused on health and other areas, so these data underestimate the relative contributions of governments to health. The U.S., for example, is the Global Fund’s largest donor, providing approximately a third of its funding while the UK is Gavi’s largest donor providing about a quarter of its funding. Still, at this point, the Trump administration has not issued stop-work orders for the main multilateral entities that support health.
For HIV, the U.S. provided almost two-thirds of all donor support (63% or $5.2 billion per year) over the 2021-2023, making this area of health especially vulnerable to U.S. cuts. The next largest donor was the Global Fund (32% or $2.6 billion). The EU and UNAIDS provided 1%; while all other donors each provided less than 1%. Because the U.S. is the largest donor to the Global Fund, any reductions in its support would have an even greater and disproportionate impact on the HIV response. See Figure 2.
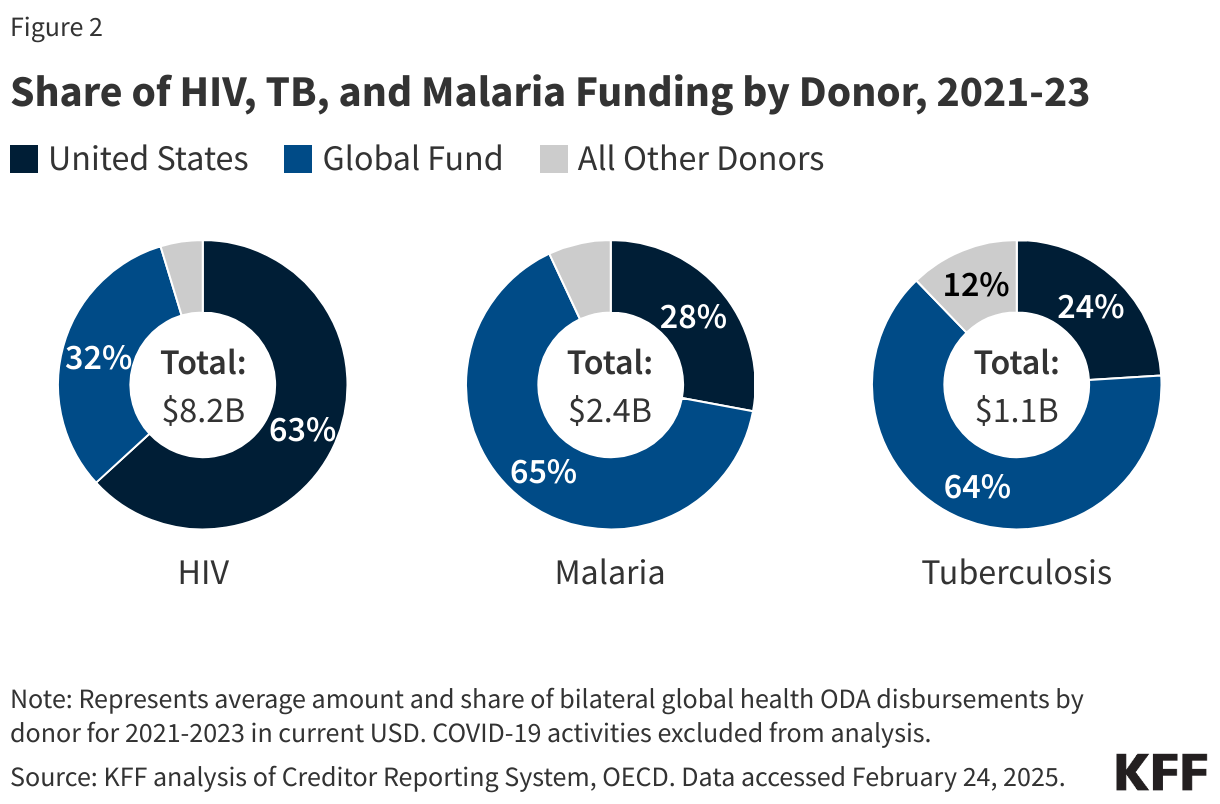
For malaria, the Global Fund was the single largest donor (65% or $1.6 billion) over the period. The U.S. was second largest at 28% or $673 million. The EU and IDA each provided 2% and all other donors were at 1% or less. As with HIV, reductions to Global Fund support by the U.S. would affect the global malaria response. See Figure 2.
Similarly, the Global Fund was the largest donor to TB efforts, providing 64% or $707 million per year over the period. The U.S. was the next largest, at 24% or $266 million, followed by the EU (4%) and Australia (2%). All other donors provided 1% or less. See Figure 2.
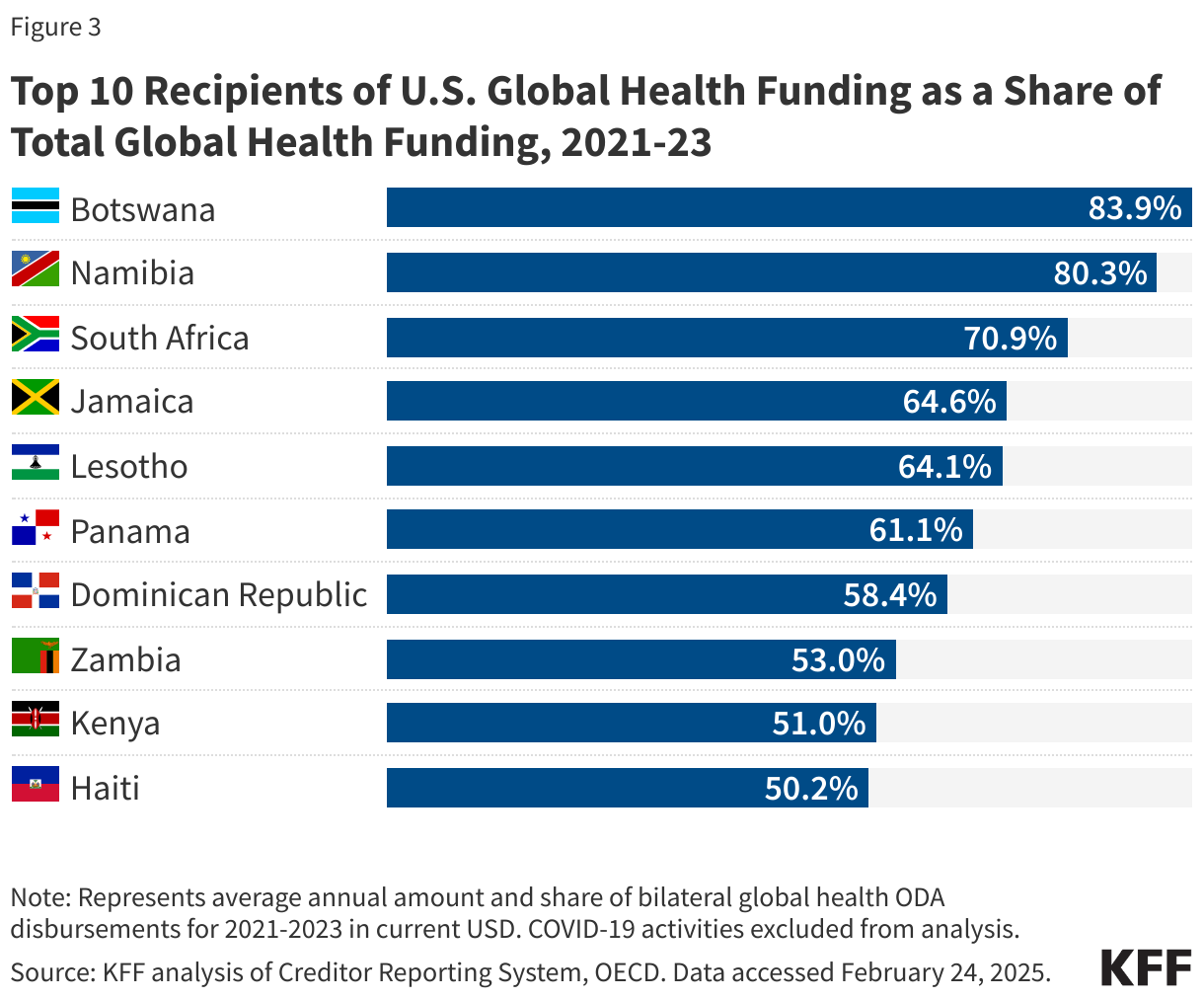
Some countries would be disproportionately affected by U.S. cuts in health aid, compared to others. Whereas the U.S. provided 30% of direct health assistance per year during the 2021-2023 period, it provided 50% or more of health assistance in 11 countries, including several low or lower-middle-income countries (Eswatini, Haiti, Kenya, Lesotho, and Zambia), one of which is currently conflict-affected (Haiti). Others are upper-middle-income (Botswana, Dominican Republic, Namibia, Jamaica, and South Africa) or high-income (Panama) and could likely more easily absorb U.S. cuts. See Figure 3.
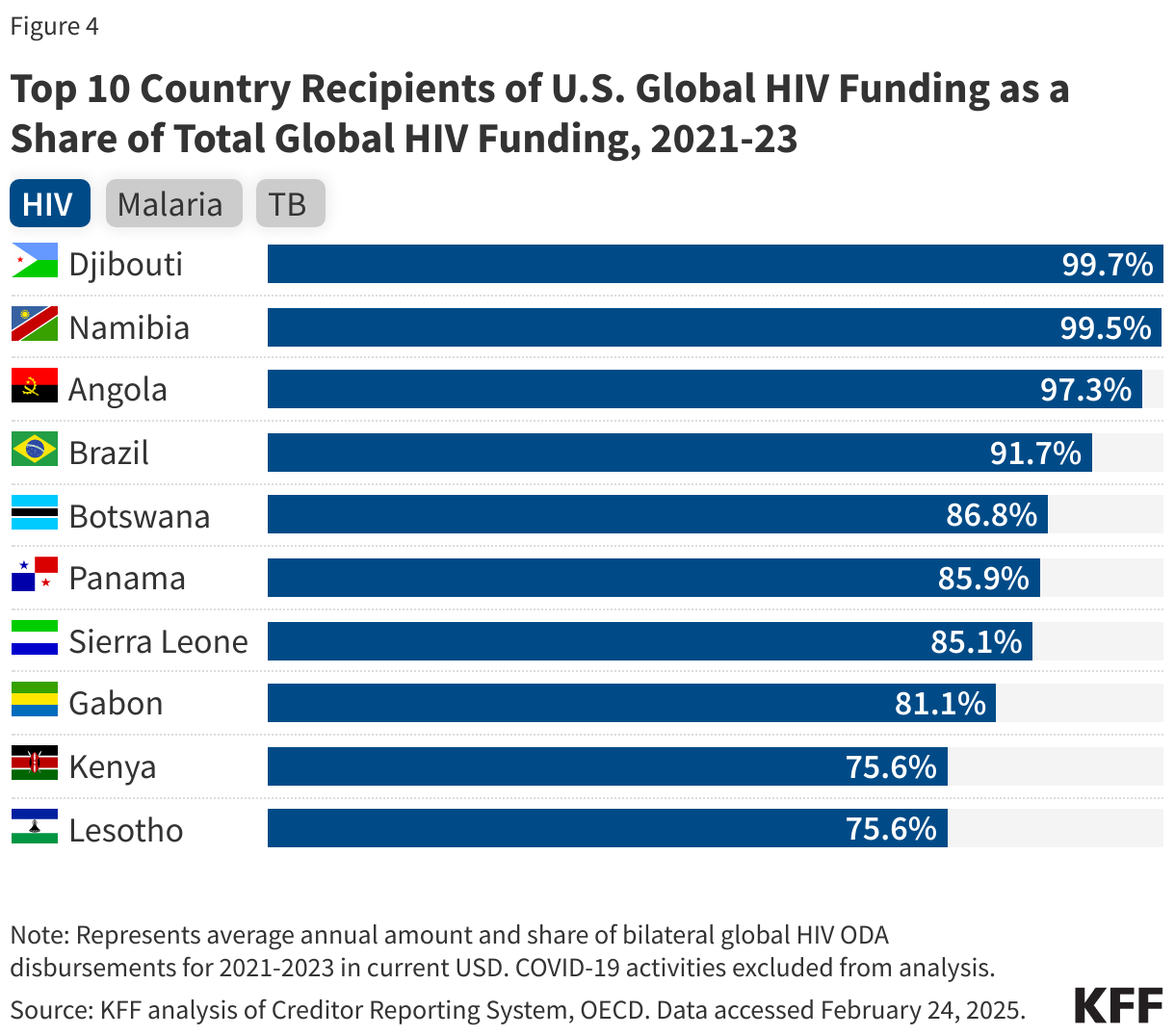
Country reliance on U.S. support is even more concentrated for HIV. Eight countries receive 80% or more of their donor support for HIV from the U.S., compared to 63% across all recipients. For malaria, seven countries receive 50% or more of their funding from the U.S., and for TB the U.S. accounts for more than 50% of funding in nine countries. See Figure 4.