Key Facts About Medicare Part D Enrollment, Premiums, and Cost Sharing in 2021
The Medicare Part D program provides an outpatient prescription drug benefit to older adults and people with long-term disabilities in Medicare who enroll in private plans, including stand-alone prescription drug plans (PDPs) to supplement traditional Medicare and Medicare Advantage prescription drug plans (MA-PDs) that include drug coverage and other Medicare-covered benefits. This analysis provides the latest data about Medicare Part D enrollment, premiums, and cost sharing in 2021 and trends over time, based on data from the Centers for Medicare & Medicaid services (CMS) Part D Enrollment, Benefit, Landscape, and Low Income Subsidy files.
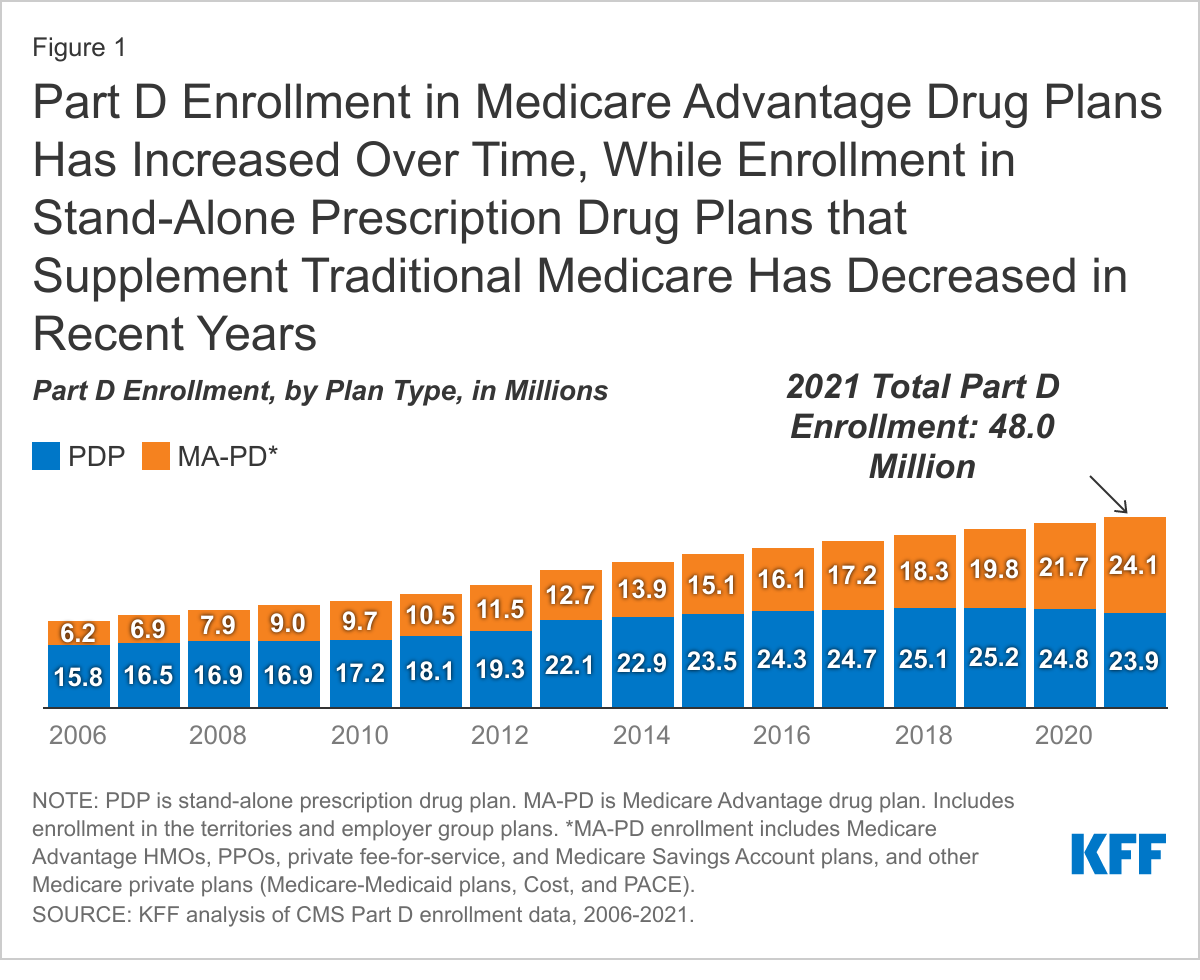
Part D enrollment in Medicare Advantage drug plans has increased over time, while enrollment in stand-alone prescription drug plans has decreased in recent years
A total of 48 million people with Medicare are currently enrolled in plans that provide the Medicare Part D drug benefit, representing more than three-quarters (77%) of all Medicare beneficiaries. This total includes plans open to everyone with Medicare, including stand-alone PDPs and MA-PDs, and plans for specific populations, including retirees of a former employer or union and Medicare Advantage Special Needs Plans (SNPs). Over time, Part D enrollment in MA-PDs has increased, reflecting enrollment growth in Medicare Advantage plans overall, while enrollment in PDPs has decreased each year since 2019.
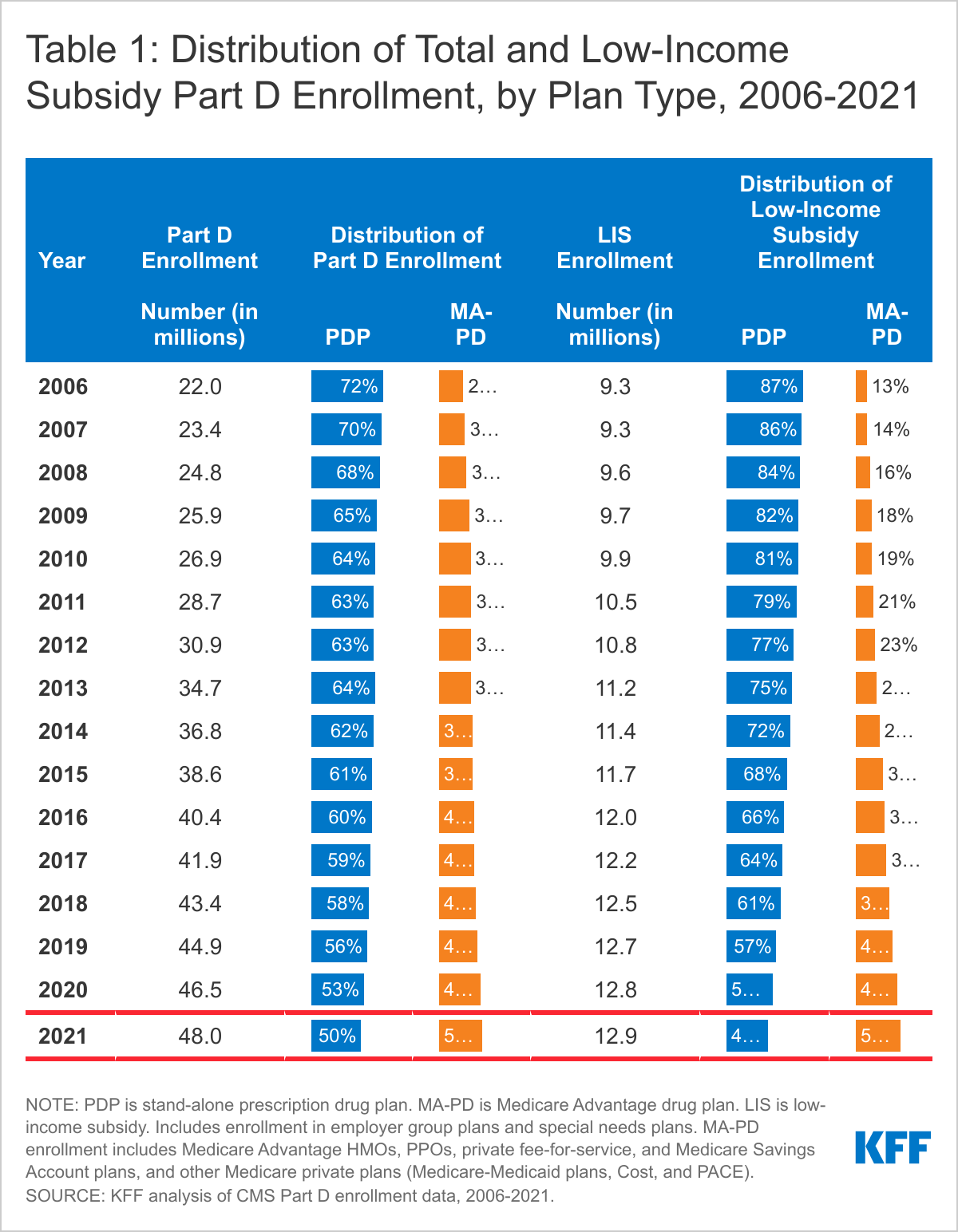
In 2021, half of all Part D enrollees are enrolled in stand-alone PDPs (50%), and the other half are in MA-PDs (50%), but a slightly larger number of enrollees are in MA-PDs (24.1 million) than in PDPs (23.9 million) (Figure 1, Table 1). (MA-PD enrollment includes Medicare Advantage HMOs, PPOs, private fee-for-service, and Medicare Savings Account plans, and other Medicare private plans, including Medicare-Medicaid plans, Cost plans, and PACE plans). Between 2020 and 2021, the number of MA-PD enrollees increased by 11%, while enrollment in PDPs decreased by 4%.
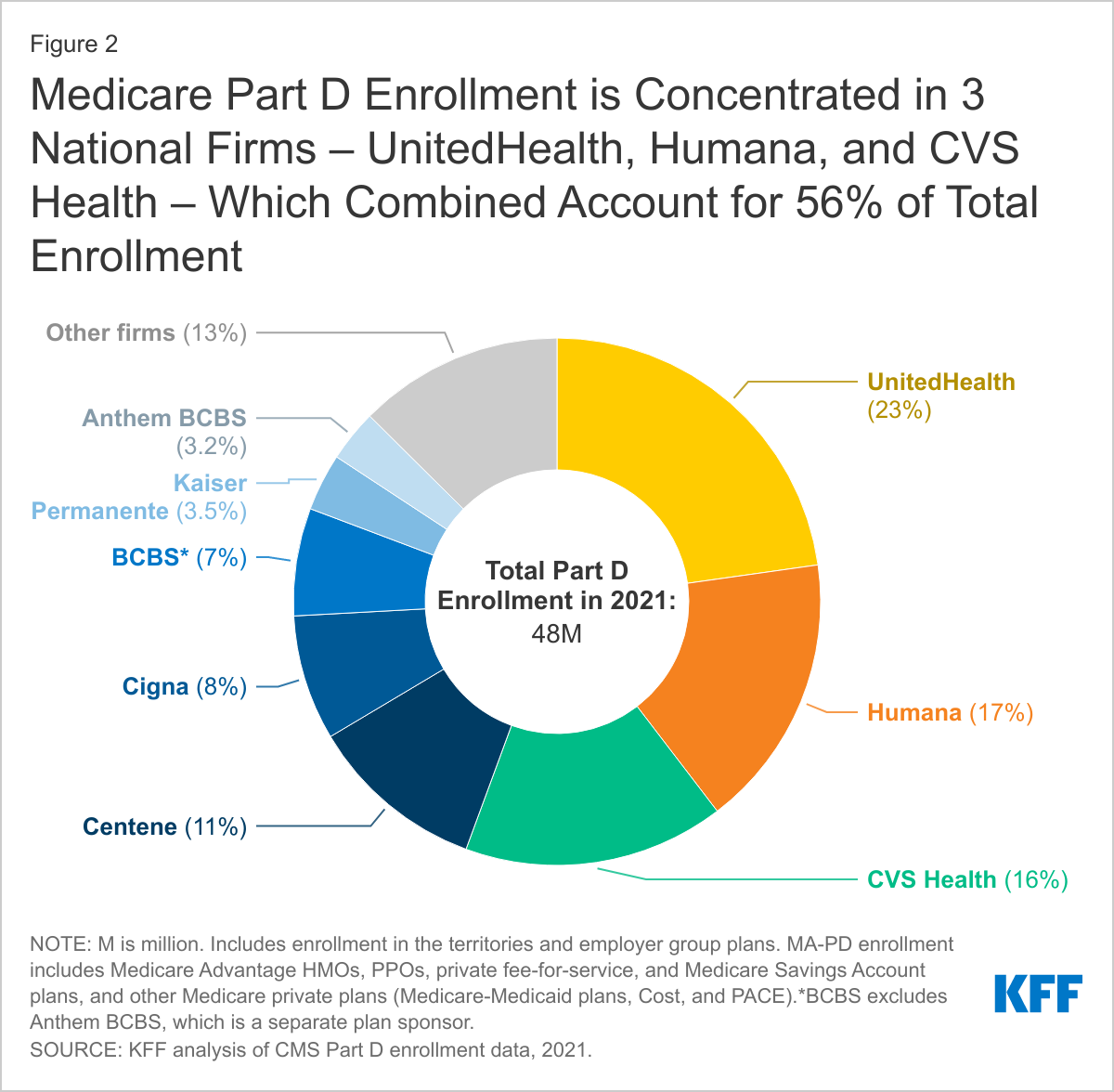
Part D enrollment is concentrated in 3 national firms – UnitedHealth, Humana, and CVS – which have a combined 56% of total enrollment
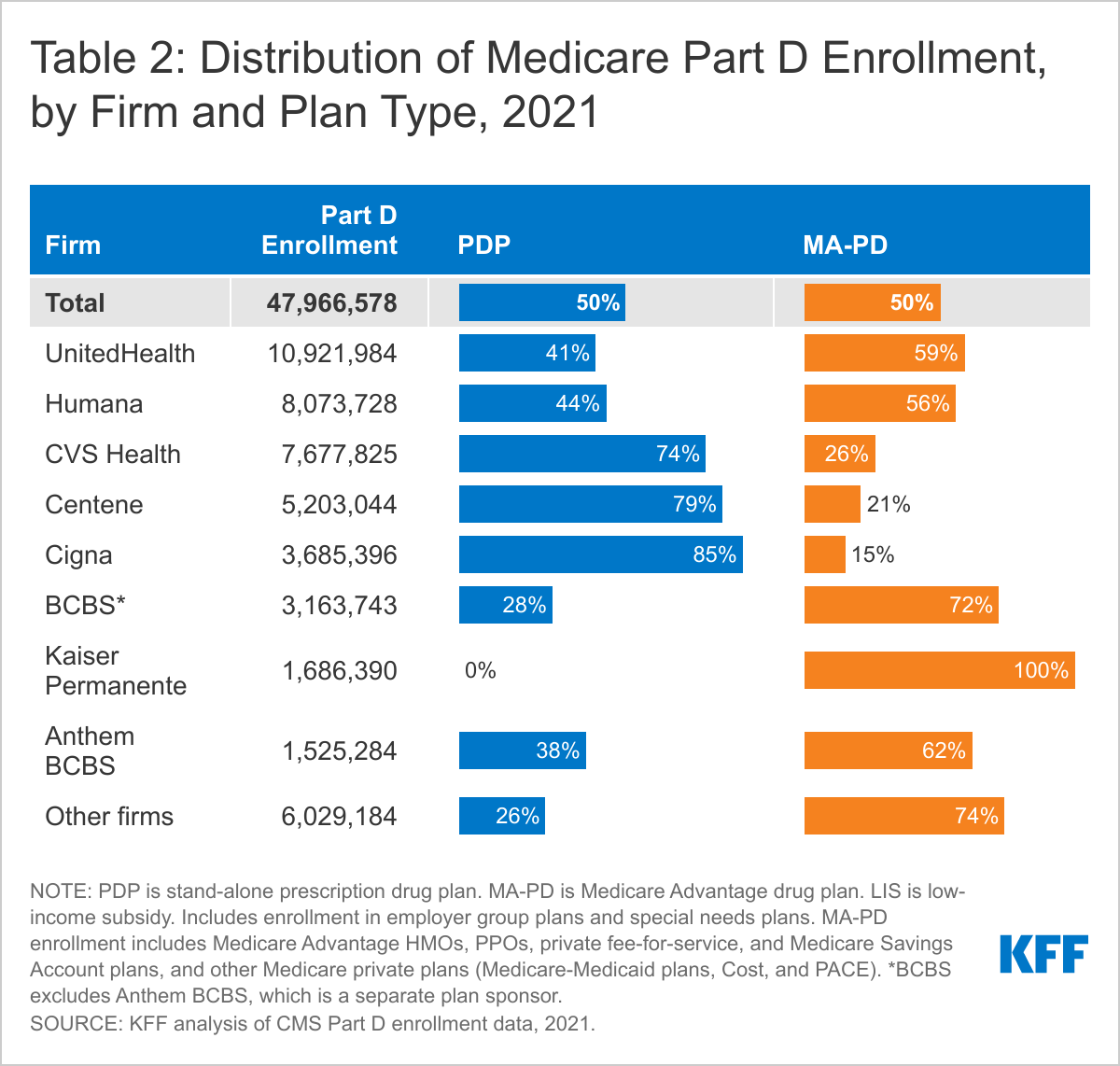
The top three firms – UnitedHealth, Humana, and CVS Health – cover close to 6 in 10 of all beneficiaries enrolled in Part D in 2021 (56%), while the top five firms – including Centene and Cigna – account for three-quarters (74%) of Part D enrollment (Figure 2). With the exception of Kaiser Permanente, which exclusively offers MA plans, the top Part D plan sponsors offer both stand-alone PDPs and MA-PDs. For most firms, Part D enrollment is more concentrated in one market than the other; for example, CVS Health, Centene, and Cigna have greater enrollment in PDPs than MA-PDs (Table 2).
An increasing share of beneficiaries receiving low-income subsidies are enrolled in Medicare Advantage drug plans, with just over half now enrolled in MA-PDs
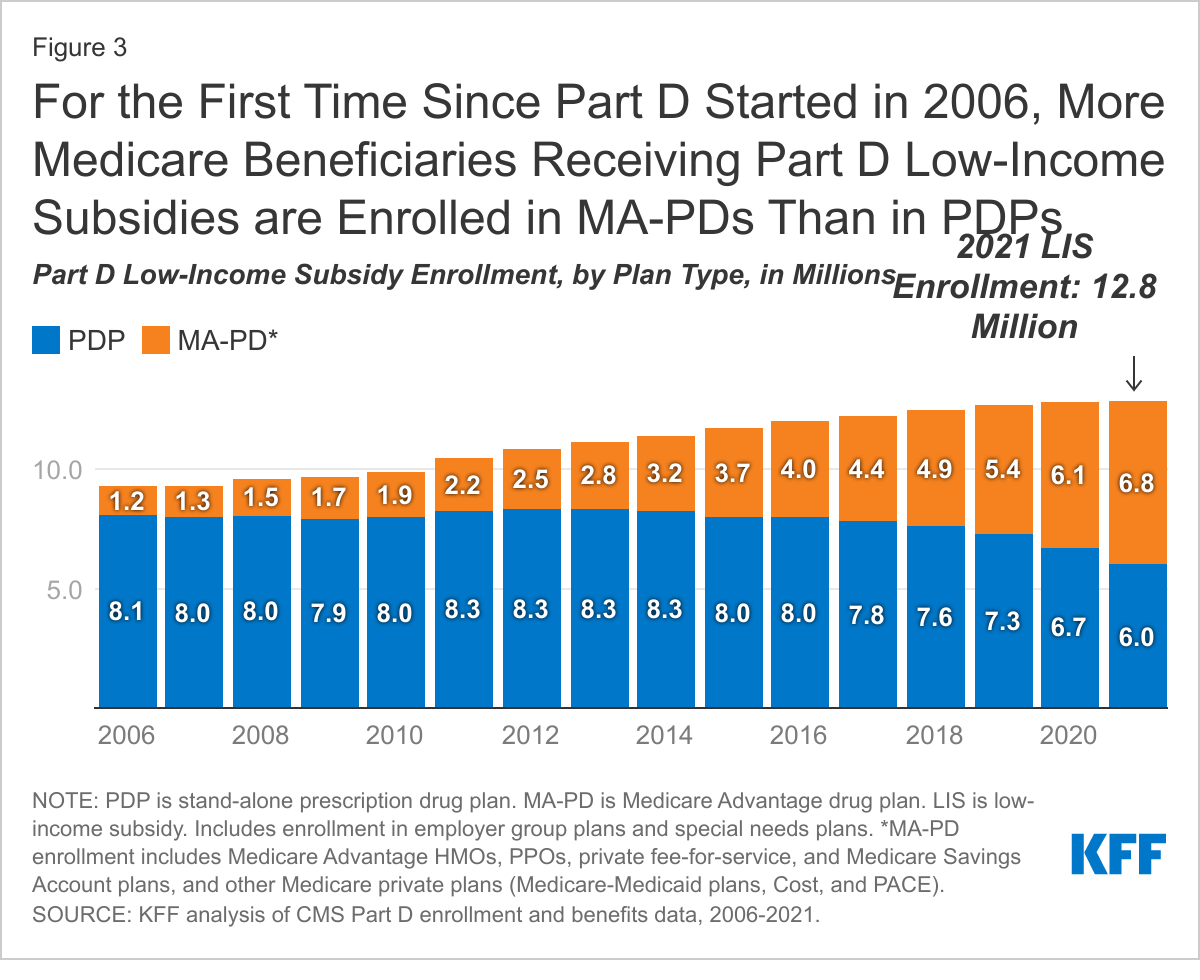
In 2021, nearly 13 million Part D enrollees, or just over 1 in 4, receive premium and cost-sharing assistance through the Part D Low-Income Subsidy (LIS) program. These additional financial subsidies, also called “Extra Help,” pay Part D premiums for eligible beneficiaries, as long as they enroll in stand-alone PDPs designated as premium-free “benchmark” plans, and reduce cost sharing. For the first time since Part D started in 2006, more LIS enrollees are in MA-PDs (6.8 million) than in PDPs (6.0 million) (Figure 3). Reflecting overall trends in Part D enrollment, the share of LIS enrollees in stand-alone PDPs has declined over time, from 87% in 2006 to 47% in 2021, while the share in MA-PDs has increased, from 13% in 2006 to 53% in 2021 (Table 1).
As part of increased enrollment in MA-PDs, more than one quarter of all LIS enrollees (26%) are now enrolled in Medicare Advantage Special Needs Plans (SNPs), up from only 4% in 2006. SNPs limit enrollment to beneficiaries with certain characteristics, including those with certain chronic conditions (C-SNPs), those who require an institutional level of care (I-SNPs), and those who are dually enrolled in Medicare and Medicaid (D-SNPs), which account for the majority of SNP enrollees.
Monthly Part D premiums have decreased somewhat in recent years; the 2021 weighted average premium for drug coverage is 3 times larger for PDPs than for MA-PDs
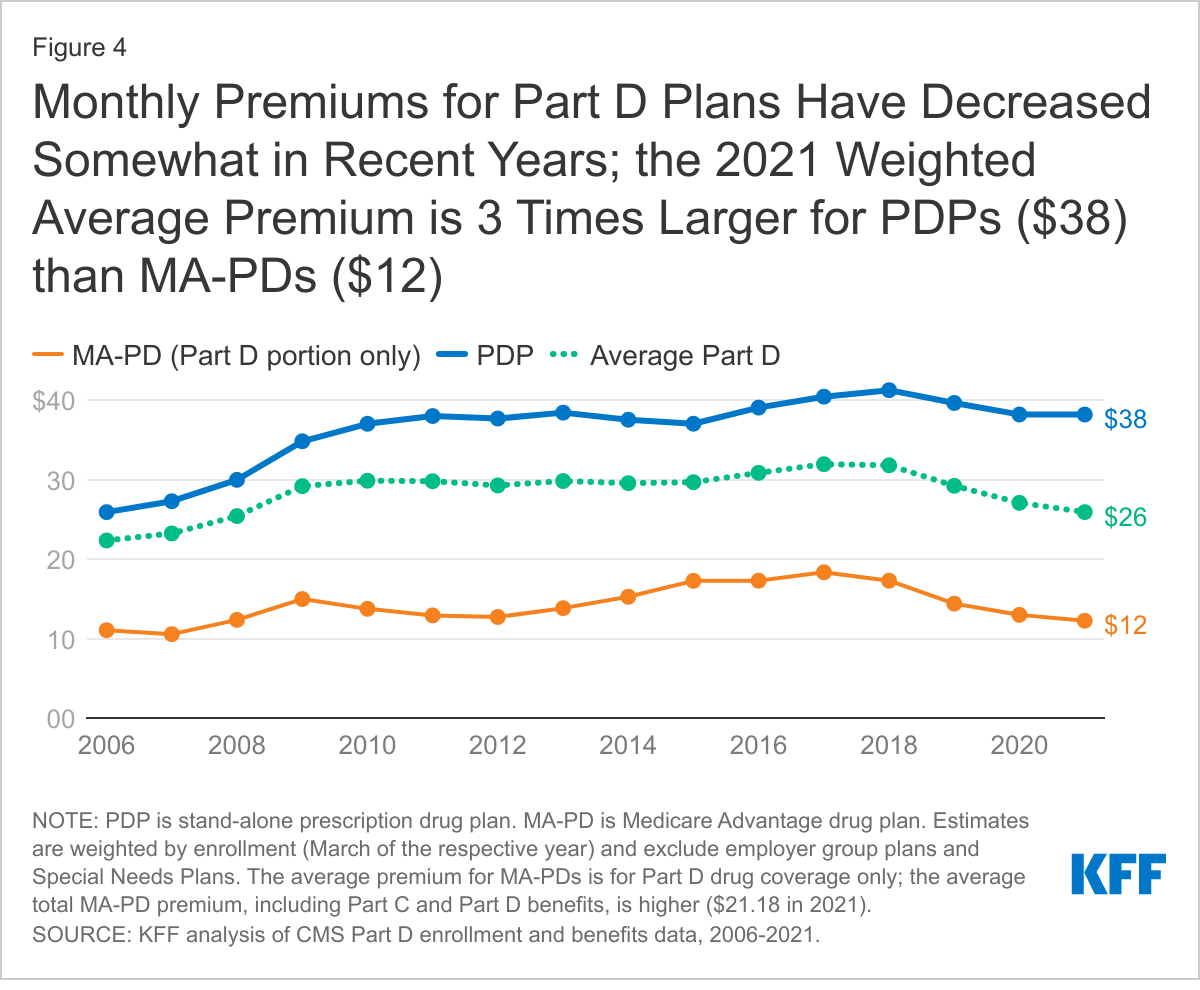
In 2021, the weighted average monthly premium for PDPs is $38, a 7% reduction (-$3) from a high of $41 in 2018 (Figure 4). The average monthly PDP premium amount has decreased somewhat in recent years, and has remained within a few dollars of the 2021 average since 2010. For MA-PDs, the monthly premium for the Part D portion of covered benefits averages $12 in 2021 (and $21 for Part C and Part D benefits combined). The average premium for drug coverage in MA-PDs is lower than the average premium for PDPs due in part to the ability of MA-PD sponsors to use rebate dollars (which may include bonuses) from Medicare payments for benefits covered under Parts A and B to lower their Part D premiums. The combined weighted average Part D premium across both types of plans is $26 in 2021, a reduction of roughly 20% (-$6) from 2018, driven largely by a decrease in the Part D portion of the monthly MA-PD premium.
The moderation of growth in the average Part D premium in recent years is likely related to changes in the Part D benefit that have reduced plan liability, in particular, an increase in the manufacturer coverage gap price discount on brand-name drugs from 50% to 70% in 2019, which has led to a reduction in plan liability for brand-name drugs during the coverage gap phase. Lower plan liability helps constrain total costs, enabling plans to lower their bids and, therefore, premiums. The average premium reduction among MA-PDs specifically is related to both an increase in the availability of zero premium plans and the reduction in plan liability for brand-name drug costs during the coverage gap phase.
Most Part D enrollees in 2021 (51% of PDP enrollees and 87% of MA-PD enrollees) are in plans offering enhanced benefits, which can include a lower (or no) deductible, reduced cost sharing, or a higher initial coverage limit than under the standard benefit design. The weighted average premium in 2021 for enhanced benefit PDPs is $44, which is roughly 40% higher than the monthly premium for PDPs offering the basic benefit ($32).
The average Part D deductible has increased for PDPs, while decreasing for MA-PDs; the 2021 weighted average annual drug deductible is 3.5 times larger in PDPs than in MA-PDs
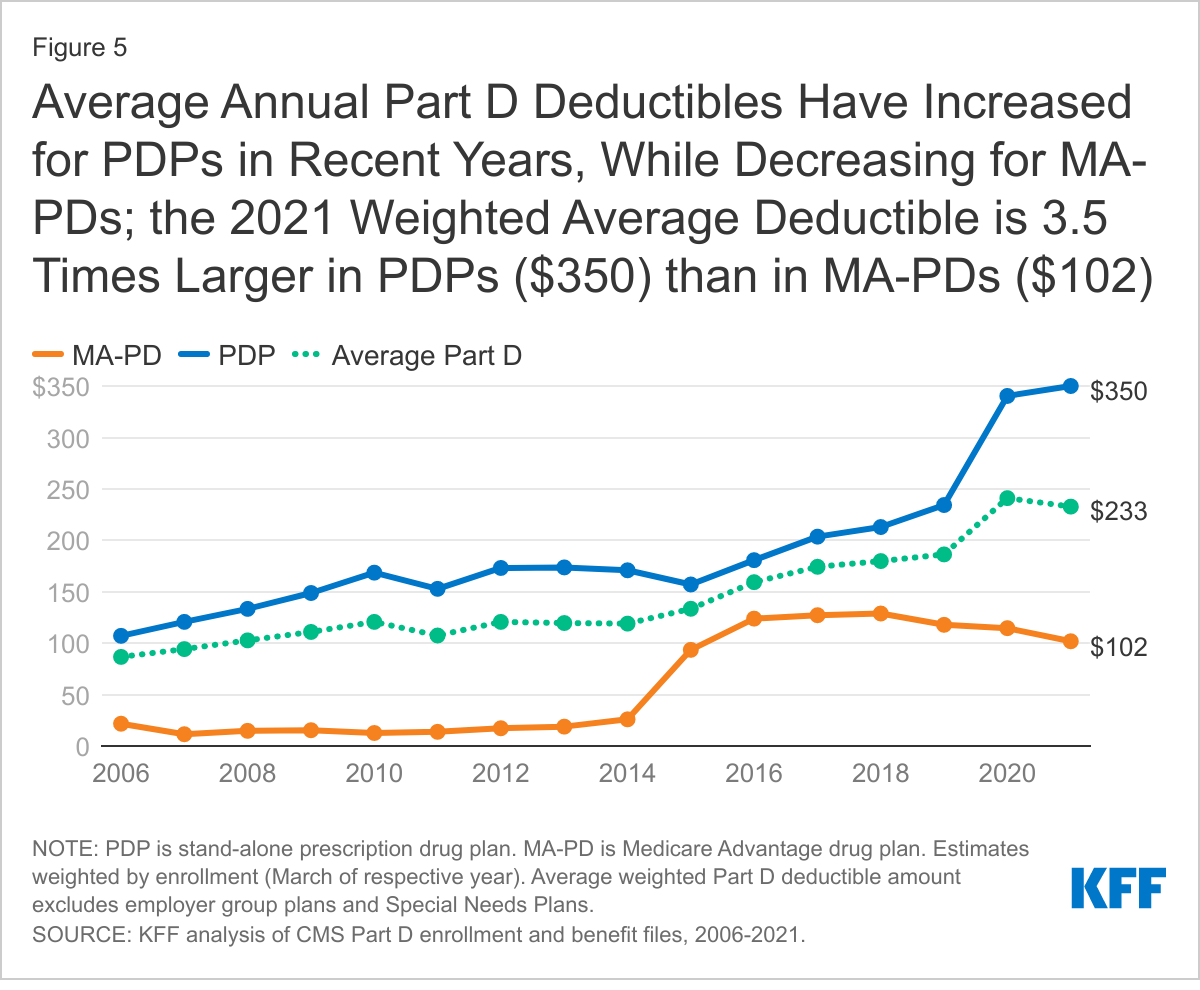
In 2021, a large majority of PDP enrollees (86%) are in plans that charge a deductible, with nearly two-thirds (64%) in PDPs that charge the standard amount of $445 in 2021. Conversely, less than 1 in 5 MA-PD enrollees (18%) are in plans that charge the standard Part D deductible, and nearly half (47%) are in plans that charge no drug deductible. These enrollment patterns explain the wide divergence between PDPs and MA-PDs in the enrollment-weighted average Part D deductible amount. For PDPs, the average Part D deductible in 2021 is $350, 3.5 times larger than the average drug deductible in MA-PDs ($102) (Figure 5).
The increase in the weighted average Part D deductible for PDPs was particularly steep between 2019 and 2020, when two national PDPs modified their plan design from charging no deductible to charging a partial or full deductible in all or nearly all regions. Charging a full or partial deductible provides plans with an additional lever to reduce their liability, particularly for those enrollees who have relatively low total drug costs, and keep premium growth in check. Conversely, MA-PDs have more leverage to reduce Part D premiums because of rebate dollars from Medicare, and with the majority of MA-PDs offering enhanced benefits, they are more likely to have lower or no deductibles than PDPs.
Most Part D enrollees pay less than $10 for generic drugs, but many pay $40-$100 (or coinsurance of 40%-50%) for brand-name drugs; a larger share of MA-PD enrollees than PDP enrollees pay the maximum 33% coinsurance for specialty tier drugs
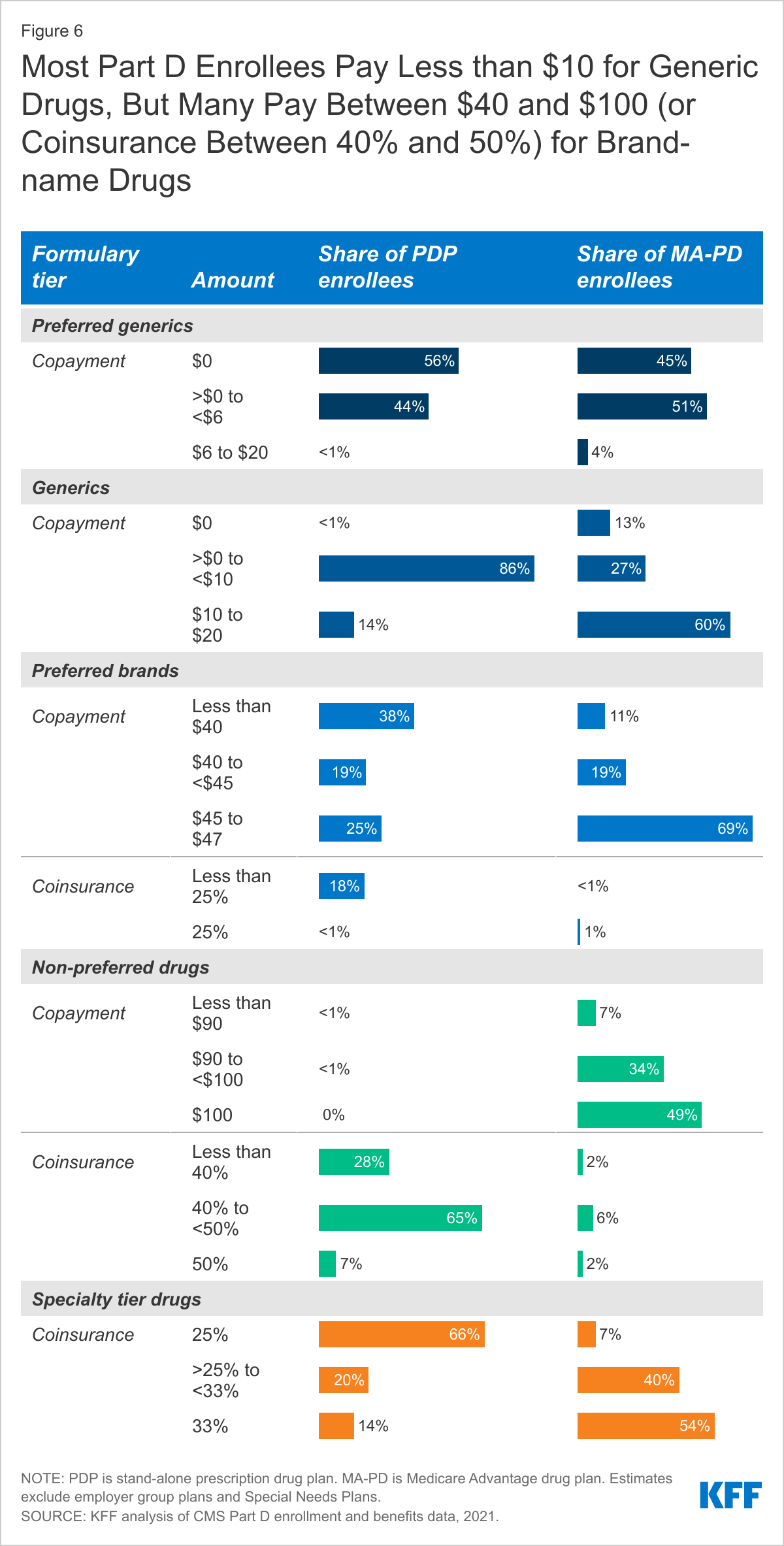
Most Part D enrollees face relatively low cost sharing for preferred generic drugs, but higher amounts for generics not on the preferred tier. One-half of Part D enrollees (both PDP and MA-PD enrollees) pay $0 for preferred generics in 2021, but many pay $10 or more per prescription for generics that are not on the preferred tier (Figure 6). For preferred generics, 56% of PDP enrollees and 45% of MA-PD enrollees have a $0 copayment, while 44% of PDP enrollees and 51% of MA-PD enrollees face prescription copayments greater than $0 but less than $6. For generic drugs that are not on the preferred generic tier, most PDP enrollees (86%) pay less than $10, while more than half of MA-PD enrollees (60%) pay between $10 and $20. (We did not compare which specific drugs are covered on each tier in PDPs and MA-PDs, which would also influence enrollees’ out-of-pocket costs.)
For non-preferred drugs, most MA-PD enrollees face copayments while most PDP enrollees face coinsurance; for preferred brands, copayments are more common than coinsurance for enrollees in both types of plans. For preferred brands, 57% of PDP enrollees pay monthly copayments less than $45, while 69% of MA-PD enrollees pay $45 to $47. For drugs on the non-preferred tier (which can be all brands or a mix of brands and generics), virtually all PDP enrollees pay coinsurance between 25% and 50% in 2021, while most MA-PD enrollees (83%) pay copayments between $90 and $100. The maximum cost-sharing amount permitted by CMS is $47 or 25% for preferred brands and $100 or 50% for non-preferred drugs in 2021.
A larger share of MA-PD enrollees than PDP enrollees face the maximum 33% coinsurance rate for specialty tier drugs. For specialty tier drugs, defined by CMS as those that cost at least $670 per month, a much larger share of MA-PD enrollees than PDP enrollees are in a plan that charges the maximum 33% coinsurance (54% vs. 14%), while a much larger share of PDP enrollees than MA-PD enrollees are in a plan that charges the minimum 25% coinsurance (66% vs. 7%). Only those plans that waive some or all of the standard deductible are permitted to set the specialty tier coinsurance rate above 25%. Most PDP enrollees are in plans that charge the standard $445 deductible in 2021, while most MA-PD enrollees are in plans that charge either no or a lower deductible.
Juliette Cubanski is with KFF. Anthony Damico is an independent consultant.