Health Care in Puerto Rico and the U.S. Virgin Islands: A Six-Month Check-Up After the Storms (Report)
Key Findings
Puerto Rico and the U.S. Virgin Islands (USVI) suffered significant damage to their infrastructure and health care systems from Hurricanes Irma and Maria in September 2017. Drawing on interviews with residents and key stakeholders as well as public reports, this brief provides an overview of the status of the recovery efforts six months after the storms, with a focus on the health care systems. It finds:
- Recovery has progressed, but major challenges remain. Power is back in many areas but remains unstable in Puerto Rico, and remote areas of the island are still without power. There are some signs of economic recovery, but revenues are still down, particularly in USVI, where major hotels remain closed. Many homes are still damaged, and individuals face ongoing financial challenges. Schools in USVI continue to operate on part-day schedules, and many school-aged children have left both territories. Others, particularly young professionals and health care providers, continue to migrate away from the islands, leaving an older population with less family support.
- Physical and mental health needs have increased. Gaps in care and medication have led to worsened chronic conditions, such as diabetes and hypertension. The unstable power in Puerto Rico makes it challenging to manage chronic conditions due to difficulties refrigerating insulin and accessing oxygen, dialysis, and other machines. Many individuals are struggling emotionally amid sharp increases in depression, anxiety, panic attacks, and post-traumatic stress disorder.
- Health care systems have resumed operations, but there are limitations on access and gaps in services. Hospitals in Puerto Rico are operational, while hospitals and other facilities in USVI are still operating at limited capacity due to major structural damage. Clinics in both territories have resumed operations, but a number of Puerto Rico’s clinics lack stable power. Loss of providers has exacerbated pre-existing access challenges for specialty care and mental health services.
- Federal relief funding for Medicaid provides essential support but does not address underlying fiscal problems. The budget bill increased the federal caps on Medicaid funding and provided Medicaid funds at 100% federal match from January 2018 through September 2019. However, it does not address underlying fiscal problems or the disparity in federal Medicaid match rates and the cap on federal Medicaid funds faced by the territories.
- Individuals, hospitals, clinics, and territory officials are taking steps to prepare for future natural disasters but have limited time and resources to prepare before the next hurricane season. Amid recovery and preparation efforts, the territories are also engaged in major delivery system reform efforts.
Introduction
Hurricane Maria made landfall in Puerto Rico and the U.S. Virgin Islands (USVI) on September 20th, two weeks after Hurricane Irma hit on September 6, 2017. The storms caused significant physical damage to the infrastructure and health care systems, leaving severe economic and health consequences in their wakes. This brief provides an overview of the status of the recovery in Puerto Rico and USVI six months after the storms, with a focus on the health care systems and health needs of residents. It is based on public reports and over 30 in-person and phone interviews with residents, local and federal government officials, and providers conducted between February and April 2018. The brief builds on earlier work that examined how residents in Puerto Rico were faring two months after the storm and key issues for recovery in Puerto Rico and USVI identified during a Fall 2017 roundtable with key stakeholders.
Amid continuing recovery efforts following hurricanes #Irma and #Maria, health care systems in #PuertoRico and the #USVI have resumed operations, but there are still limitations on access and gaps in services.
Pre-Storm Challenges and Early Recovery Status
Hurricanes Irma and Maria caused devastating damage to both Puerto Rico and USVI, and exacerbated pre-existing fiscal and health challenges. The storms damaged and destroyed key transportation, communication, and electricity infrastructure, creating major economic and health care problems. These problems exacerbated existing difficulties, many of which stemmed from disparities in the federal government’s treatment of territories compared to states.1
Prior to the storms, Puerto Rico and USVI had fiscal challenges, including high rates of debt, poverty, and unemployment, and they faced a range of health disparities. In Puerto Rico, the population had higher rates of fair/poor health, heart attack/heart disease, diabetes, depression, disability, low-birthweight infants, and infant mortality than both USVI and the United States overall. The share of uninsured in USVI (30%) was much higher than in Puerto Rico (7%) and the rest of the United States (12%). In addition, Puerto Rico and USVI suffered from poor health infrastructure and a shrinking health care workforce.
Unlike states, federal Medicaid funds are capped for Puerto Rico and USVI, and they have a fixed federal Medicaid match rate that is lower than the rate they would receive if they were states. The 50 states and D.C. receive federal Medicaid funding on an open-ended basis, with a federal match rate that varies across states based on state per capita income. In contrast, annual federal Medicaid funding for the territories is subject to a statutory cap, with a fixed federal match rate of 55%. This match rate is lower than the rate the territories would receive if the rate was based on per capita income like the states. Prior to the storms, Puerto Rico also was anticipating facing a large funding gap as additional funds provided under the Affordable Care Act (ACA) were running out.
Two months after the storms, residents in Puerto Rico reported continued difficulties meeting basic needs, and daily life remained challenging. Many were without power, and some continued to have problems accessing water and gas. Many individuals were still displaced from their homes or had family and friends living with them, and many schools were still closed or operating on shortened schedules. Moreover, individuals were facing increased financial pressures, as work options were limited with many businesses remaining closed. Residents pointed to increased physical health needs and difficulties managing chronic conditions without power and with limited access to fresh food. They also described profound effects on their mental and emotional health, with many feeling stressed and anxious and having trouble sleeping at night.
In a Fall 2017 roundtable discussion, key stakeholders pointed to short- and long-term options to address health care needs in Puerto Rico and USVI, and emphasized the need to address pre-existing fiscal debt problems as well as economic damages from the storms. They identified building a strong health care system with adequate financing as a key component of economic development and recovery. In particular, they noted the importance of both short-term federal funding relief for Medicaid and legislation to address the longer-term issues of the cap on federal funds and lower federal match rate for the territories.
Status of Recovery Six Months After the Storms
There has been continued progress with recovery, but many challenges remain.
Although progress has continued with power restoration, power remains unstable in Puerto Rico, and remote areas have not had their power restored. FEMA reported that less than 10% of Puerto Rico was still without power as of March 16, 2018,2 and Puerto Rico’s government reports that approximately 95% of Puerto Rico Electric Power Authority (PREPA) customers had power generation as of April 5, 2018.3 It is unclear when the entire island will have power restored. In USVI, all electricity customers had their power restored by March 9, 2018,4 and power is generally stable. Many interviewees went months without power, with some only recently regaining it at the time of the interviews. Although some had access to generators, they noted that they could only run the generators on an intermittent basis and faced costs to maintain and fuel them. Interviewees in Puerto Rico noted that, although more areas have power restored, it is unstable and remote areas remain without power. They said that the power instability contributes to uncertainty, stress, and complication in their daily lives. For example, some said that they limit purchases of fresh food since it may be lost if they have a power outage. Unreliable cellular and internet access also contributes to ongoing communication challenges in both territories.

There are some early signs of economic recovery, but revenues and tourism are still down, particularly in USVI, where major hotels have not reopened. Interviewees in both territories noted that, although some businesses have reopened, others have closed or are operating on a limited scale. Interviewees also noted that the presence of relief workers on the islands has helped fuel revenues for hotels and restaurants, but their departures leave a growing gap in business. Overall, tourism remains down, particularly in USVI, where the major hotels are still closed. In Puerto Rico, total lodgings registered with the Puerto Rico Tourism Company in January 2018 were down over 54% from January 2017, with the decline even greater in non-metropolitan areas.5 As of February 27, 2018, 85% of hotels were operating.6 In USVI, approximately 40% of traditional hotel accommodations across the territory were open as of March 1, 2018, but many of those open were filled with relief workers.7 All ports were open, and cruise ship ports of call to St. Thomas had returned to their pre-hurricane levels.

Views on response and recovery efforts vary across entities engaged in providing assistance.
Many residents felt that the federal response through FEMA has been slow and inadequate. Interviewees noted that FEMA assistance is limited and not available to everyone. Several residents said they had applied for FEMA assistance to repair their homes but were denied or were still waiting for a response. Others noted that they had received $500 in aid from FEMA but would not be receiving any additional assistance. As of mid-April 2018, FEMA had approved 449,000 of the 1.1 million registrations for assistance for the Individual Assistance Program, providing a total of $1.2 billion in funds.8 In March 2018, FEMA announced plans to accept signed self-declarations of homeownership for cases in which all other forms of verification are destroyed or nonexistent, to help address gaps in assistance stemming from challenges showing proof of ownership and other documentation.9 FEMA has also extended the deadline to register for FEMA assistance to June 18, 2018.10 Individuals had mixed views on local government response efforts. Some were frustrated with local governments’ efforts and felt that they were not doing enough to assist individuals and/or were complicating or slowing recovery efforts. Others felt that the local response has been strong and played a helpful role in recovery within the community.
Hospitals, clinics, and local health officials had generally positive views of their experiences working with federal partners and the military. Territory officials and some providers reported positive experiences with FEMA, noting that they were working closely with the agency to finalize damage assessments and rebuild facilities. Officials in USVI noted that, through their coordination with FEMA, they will be able to build back health facilities at a higher level to provide greater resiliency for future storms. Providers and officials also described positive working relationships with their partners at the U.S. Department of Health and Human Services (HHS), including staff from the Centers for Medicare and Medicaid Services (CMS). In addition, the Office of the Assistant Secretary for Preparedness and Response (ASPR) and the Health Resources and Services Administration (HRSA) within HHS have been active in the recovery and working closely with FEMA, territory officials, and providers. ASPR leads the nation’s medical and public health preparedness, response to, and recovery from disasters and public health emergencies,11 while HRSA works to improve access to health care for vulnerable and underserved communities and individuals.12 ASPR representatives report continuing to work with territory officials to close the gap between their prioritized health care needs and resources to meet them. As part of its support for community health centers, HRSA described its top priorities as training personnel, building up communications, and expanding capacity for mental health services. In addition to the HHS agencies, several interviewees described positive experiences working with the military, particularly immediately after the storms to bring supplies and services to remote regions.
Interviewees noted that clinics played a key role in response efforts, particularly in the immediate aftermath of the storms, but received little government support. They noted that clinic staff were instrumental in connecting with individuals after the storms to assess their needs and bring them necessary supplies, medications, and services. Clinics described how staff traveled out to the surrounding community on a daily basis to assess needs and coordinate responses. Clinic representatives generally felt that they had very limited government support in the aftermath of the storms, noting that they did not receive any assistance obtaining fuel for generators, which was a major challenge. In addition, one clinic representative noted that, although they had been involved in emergency planning activities, the government did not coordinate with the clinic on response efforts.
Many interviewees felt that private organizations, volunteers, and local communities have played an instrumental role in recovery. They noted that private organizations and volunteers, often coming from the mainland, brought supplies and services into communities, including health care services. Moreover, residents pointed to the strength and resiliency within their communities, noting that neighbors worked together to provide support as well as supplies and resources. Many interviewees also emphasized that local individuals leading recovery efforts have been working tirelessly for months amid their own losses and difficulties, and they noted the importance of providing support for these individuals.

Individuals’ Daily Lives and Health Needs
Many individuals continue to face major challenges in their daily lives as a result of the storms.
Many residents still have major damage to their homes, with some still living in alternative living arrangements with other family. Across both territories, many homes still have blue tarp roofs awaiting long-term repairs. All of the interviewed residents who experienced damage to their homes were still in the process of repairing their homes. Some were living in their damaged homes, while others had made other living arrangements, typically living with other family members. Some interviewees said that these living arrangements had led to increased stress and strains on family relationships. According to FEMA, as of March 16, 2018, more than 3,500 Puerto Ricans were still living in hotels on the island and across 37 states with temporary housing vouchers.13 FEMA has extended this temporary sheltering program twice; the most recent extension ends on May 14, 2018.14

Residents continue to face financial instability, reflecting more limited work options and ongoing costs associated with recovery. Interviewees noted that many individuals have lost or changed jobs or experienced reductions in work hours following the storms, which has increased financial strains on families and forced some to deplete their savings. Further, they pointed to increased costs associated with recovery, including generator fuel, replacement of damaged and lost items, and repairs. Some said that increased financial pressures have forced them to change or postpone plans for the future, such as delaying education and career plans.
Children’s daily lives and education remain disrupted. In USVI, with many schools still damaged, they are sharing space and operating on four-hour schedules. Interviewees noted that this arrangement is difficult for children and parents, particularly for parents to accommodate work schedules to the reduced school hours. Many families with school-aged children have left USVI due to the limited school schedule. Interviewees noted that it is unclear how long schools will continue to operate on the part-day schedule, and that additional families may leave if it extends into the next school year. Teachers in Puerto Rico also noted that students have left the island, and that many may not return. On April 5, 2018, Puerto Rico’s Department of Education announced the closure of 283 of its approximately 1,110 schools for the 2018-2019 school year, due to a reduction of 38,762 students since May 2017.15 The movement of school-aged children off the islands is leading to separation of families in some cases. For example, children may be sent to live with a relative on the mainland while the parents remain on the islands. In addition, interviewees noted that children who have stayed on the islands are experiencing problems performing in school, with some still displaced from their homes and/or without power, and some dealing with ongoing fear and emotional stress from the storms.

Residents, particularly young professionals and health care providers, are continuing to migrate away from the islands. Interviewees noted that outmigration had been an issue prior to the hurricanes and that the storms exacerbated this problem, particularly among young professionals and health care providers. They noted that, as these populations leave, the remaining population is older and has less family available to help care for them. Although data on Puerto Rico and USVI population loss since the storms are limited, one analysis found that the net number of domestic air passengers departing Puerto Rico between August and November 2017 was roughly 160,000 people above trend.16 In its new fiscal plan, the Puerto Rican government projects a 10.9% cumulative decline in population over the six years following the hurricanes.17 Another study projects that between 114,000 and 213,000 Puerto Rico residents will leave the island annually in the aftermath of Hurricane Maria. The study estimates that Puerto Rico may lose up to 470,335 residents, or 14% of the population, from 2017-2019 alone.18 Projections indicate that Florida will receive the majority of this outflow, with approximately 41,000 to 82,000 people expected there in the first year after Hurricane Maria.19
Physical and mental health needs have increased.
Providers, health officials, and residents pointed to increases in physical health problems after the storms. While territory officials and providers noted that they were successful in preventing and containing major outbreaks of disease following the storms, interviewees described increases in other health care needs. They said that some individuals experienced worsened chronic conditions, such as diabetes and hypertension, due to gaps in care and medications following the storms. They also noted that limited access to fresh food and increased reliance on highly processed provisions have made it more difficult for many individuals to manage their chronic conditions. Some residents and providers described new or worsened health problems, such as ulcers and weight gain, due to increased stress. Some also pointed to increases in orthopedic problems, such as back, shoulder, and knee pain, associated with moving heavy objects as part of recovery-related activities as well as a lack of elevators during power outages for people living in high-rise buildings.

Housing and transportation challenges and the continued instability of power have made it more difficult for individuals to access care and manage their conditions. For example, the power instability has made it difficult to keep insulin refrigerated and has limited access to oxygen, dialysis, and other machines. Providers also noted that, as an increasing number of individuals leave the island, many elderly residents have lost caregiving support, leaving them with gaps in care. Red Cross personnel have been monitoring and supporting residents of public housing in USVI and have found that many individuals are still disoriented from the storms. Elderly residents have faced particular issues, such as intrusive thoughts and nightmares, trouble sleeping and eating, and isolation due to the lack of a support system. One interviewee also pointed to particular challenges facing people with serious mental illness who are not in appropriate housing situations and lack sufficient support.
Mental health needs have sharply increased, and many individuals are still struggling emotionally six months after the storms. Individual residents described ongoing emotional effects, including stress and anxiety, problems sleeping and eating, and crying and depression. Providers, including community health centers that conduct routine screenings for mental health needs, also reported sharp increases in depression, anxiety, panic attacks, and post-traumatic stress disorder (PTSD) among the communities they serve. Some interviewees pointed to ongoing emotional struggles among children, noting that some become very fearful and cry every time it rains. Preliminary data also point to growing mental health needs. From November 2017 through January 2018, a crisis hotline run by Puerto Rico’s Department of Health received 3,050 calls from people who said they had attempted suicide, a 246% increase compared to the same time last year.20 In the same three-month period, the hotline received 9,645 calls from people who said that they had thought about attempting suicide — an 83% jump from the same time last year.21 Despite the growing need, interviewees indicated that many residents are not receiving mental health care, reflecting long-term stigma associated with receiving mental health services and a limited supply of mental health providers.
Analysis points to a potentially higher death rate stemming from the storms than the official counts. The official death toll from Hurricane Maria in Puerto Rico stands at 6422 , and five deaths were attributed to Hurricanes Irma and Maria in USVI.23 However, a New York Times report in December 2017 estimated hurricane-related deaths in Puerto Rico as high as 1,052 based on analysis of mortality data compared to previous years.24 The additional deaths were most often attributable to sepsis, pneumonia, and breathing disorders, which could have been caused indirectly by the hurricanes due to effects such as delayed medical treatment, power outages for medical equipment, and poor conditions in homes and health care facilities. The Governor of Puerto Rico signed an executive order in January 2018 to establish a working group tasked with revising the number of deaths related to Hurricane Maria.25 Additional external work is underway to study Hurricane Maria-related excess mortality in Puerto Rico as well.26

Recovery of the Health Care System
Parts of the health care system have resumed operations, but gaps in services remain.
Prior to the hurricanes, residents in both territories relied on a system of hospitals and clinics as well as private providers for care. There were approximately 70 hospitals providing care in Puerto Rico,27 along with 20 federally funded health centers that provided primary and preventive care services at 93 urban and rural sites.28 In USVI, there were two hospitals, Schneider Regional Medical Center on St. Thomas and the Governor Juan F. Luis Hospital and Medical Center on St. Croix, as well as two Federally Qualified Health Centers (FQHCs), including the St. Thomas East End Medical Center Corporation on St. Thomas and the Frederiksted Health Center (FHC) on St. Croix. In addition, the Schneider Regional Medical System operated the Myrah Keating Smith Community Health Center on St. John. The USVI Department of Health operated three health facilities across the three major islands.29 Both territories also had a network of private providers, although they were facing provider shortages and difficulties attracting and retaining providers.

Hospitals and clinics in Puerto Rico have resumed operations, but a number of clinics still do not have stable power. In Puerto Rico, hospitals were prioritized as critical facilities, and local officials provided support to resume operations as quickly as possible after the hurricanes. Six months after the storms, all of the hospitals are operational. Many of the clinics in Puerto Rico suffered damages and lost power.30 While they have resumed operations, as of mid-March 2018, approximately 1 in 10 (11%) of the permanent health center sites have limited or no grid power. Three of these health centers have intermittent grid power and rely on generators as a backup source of power, while five remain without grid power and rely solely on generators. An additional health center converted to solar power in lieu of continuing to rely on a generator, and five health centers are operating from mobile vans. Clinic directors noted that they tried to resume operations as quickly as possible after the storms but received little support and faced challenges due to limited generator capacity and difficulty obtaining fuel for generators. Interviewees emphasized that the mountainous regions and offshore islands of Puerto Rico continue to have major access problems six months after the storms. Many residents in remote regions, particularly elderly individuals, remain unable to travel to sites of care. Through volunteer, military, and other efforts, some individuals are continuing to go into these communities to deliver care, but as relief efforts phase out, these access difficulties may increase. On the offshore islands, availability of services remains severely limited, requiring dialysis patients to travel to the main island for care.

In USVI, services remain limited due to major structural damage to the hospitals and other facilities, requiring some patients to continue to be transferred off-island for care. In USVI, both hospitals as well as some urgent care centers and health department facilities suffered damage from the storms that limited their operations. Schneider Regional Medical Center on St. Thomas suffered major structural damage, leaving it with limited capacity to provide inpatient care, emergency services, and dialysis care six months after the storms. The storms also destroyed its cancer treatment center, leaving it unable to provide radiation treatment. Since the storms, the hospital has lost over 170 employees, including many nursing staff, and it is relying on travel and temporary nurses to help fill in the gaps created by these losses. As of mid-April 2018, the hospital was waiting on a final determination from FEMA as to whether it will repair and rebuild the existing facility or construct a new facility. The storms also caused significant damage to the Myrah Keating Smith Community Health Center on St. John, leaving it inoperable. It has since been merged into a Department of Health clinic on the island. Directors from both FQHCs reported limited physical damage, enabling them to resume operations quickly after the storms. However, FHC reported that it has lost nurses, dental staff, and ancillary workers, stretching remaining staff members to meet patient needs while continuing to deal with periodic power outages. Overall, the ongoing service limitations across the USVI require continued off-island transfers for individuals with high needs and limit the ability of evacuated individuals to return home. Prior to and in the immediate aftermath of the storms, the Department of Health coordinated the evacuation of almost 800 people, including many dialysis patients. Officials noted that modular units and dialysis trailers are being brought to USVI to expand service capacity, which will hopefully reduce off-island transfers and allow more evacuees to return home.
Many private providers remain closed or have left the territories, which has exacerbated pre-existing access challenges, particularly for specialty and mental health care. Interviewees noted that, prior to the storms, the territories had difficulty attracting and retaining a sufficient supply of specialty providers due to low payment rates. Moreover, mental health services in both territories were limited. The storms exacerbated these issues, as many private providers remain closed and an increasing number of providers have left the island, while health needs, particularly mental health needs, have increased. Recruiting and retaining providers and allied health professionals currently is a top priority for health facilities and local health officials in both territories.
Hospitals and clinics are facing increased financial strain as the territories’ uninsured populations grow due to increases in unemployment. Respondents noted that, as people lose jobs, many are losing health insurance. While some may qualify for Medicaid coverage, a number are becoming uninsured. Hospital and clinic staff noted that this shift in coverage is increasing financial strain on their operations due to losses of commercial pay patients.
Federal relief funding for Medicaid provides essential support, but major fiscal challenges remain.
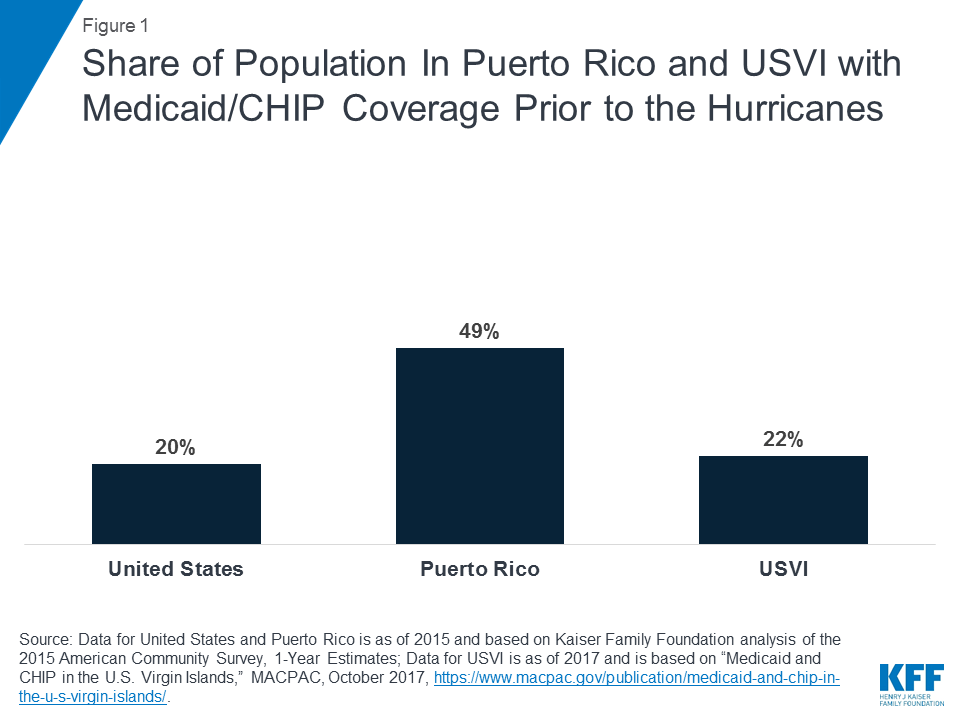
Both territories have taken steps to facilitate access to Medicaid. Medicaid and the Children’s Health Insurance Program played important roles covering residents in both territories before the storms, covering nearly half of the population in Puerto Rico (49%) and over one in five individuals (22%) in USVI (Figure 1). Puerto Rico delayed Medicaid renewals for 12 months and USVI delayed renewals for six months to help individuals maintain stable coverage amid the recovery efforts. Local officials and providers also noted that they are engaging in outreach and education efforts to help reach and enroll individuals who may be newly eligible for Medicaid as they are losing jobs and income. In USVI, hospitals’ use of presumptive eligibility determinations is helping to facilitate access to coverage, and they are planning to expand use of presumptive eligibility to the clinics. Puerto Rico officials said that, overall, they are expecting a small increase in enrollment of about 1%, which would reflect both an increase in the number of individuals qualifying for the program and disenrollment of individuals leaving the island.
The February 2018 federal budget bill provided instrumental federal support for the territories’ Medicaid programs, but it did not address underlying disparities faced by the territories. Unlike the states, which receive federal Medicaid matching funds based on a formula tied to per capita income on an open-ended basis, the territories receive a fixed federal match rate (55%) that is lower than what they would receive based on the per capita income formula and are also subject to a cap on federal funds. The budget bill increased the federal caps for Puerto Rico ($4.8 billion) and USVI (approximately $142.5 million) and provided Medicaid funds at 100% federal match from January 2018 through September 2019.31 Local officials and providers noted that these funds provide much needed immediate assistance and fiscal relief, but they expressed significant concerns about what will happen when the funding ends since no long-term changes were made to the federal match rate or cap on federal funds. They noted that, when the federal funding ends, they will face major fiscal challenges, particularly since the territories’ economies will not have fully recovered by that time. They stressed the importance of a longer-term solution to address the disparities in their federal match rate and cap on federal funds as well as other differences in how the territories are treated, including their exclusion from receipt of Disproportionate Share Hospital payments and variations in Medicare payments.
Amid recovery efforts, the territories are also engaged in delivery system reform efforts.
To achieve savings required by its Fiscal Oversight Board, Puerto Rico is implementing major delivery system reform on a rapid timeline. Under the fiscal plan that the Puerto Rican government proposed to comply with the Federal Control Board, the territory targets an $841 million reduction in health care spending by FY2023.32 The fiscal plan also proposes a new health care model designed to achieve administrative and financial efficiency. Currently, one of four MCOs, along with an additional plan serving a special population, serves each of eight geographic regions on the island.33 Beginning on October 1, 2018, the new model will require MCOs to compete in a single territory-wide region to provide services to the approximately 1.3 million enrollees across the island.34 Other changes will include increased preference for generic drugs, a capped per-member-per-month payment amount, and benefit redesign. Some stakeholders question whether reducing health care spending while trying to rebuild infrastructure and capacity is prudent, especially since costs are currently lower than costs on the mainland. Given the focus on recovery efforts and other system demands, there are also concerns about whether local governments can implement these reforms on the currently required timeline.
USVI is also engaged in broad delivery system reform efforts aimed at reducing fragmentation of care and expanding access to services. Before the hurricanes, providers and officials in USVI had been collaborating on improvements to the delivery system. Following the storms, they expanded their efforts by arranging six USVI-led working groups focused on different aspects of the health care system in terms of storm recovery and mitigation for future natural disasters. These working groups include topics such as environmental health, patient-centered models of care, and data-informed community health. Health care officials in the territory are already pursuing a number of steps to achieve a more integrated system, such as building up case management and navigator services, increasing outreach to the uninsured or underinsured through provider referrals, and expanding access to telemedicine. They are also collaborating on hurricane recovery by working together on issues such as mental health, reinforcing electronic health data systems, and a continued focus on achieving a robust health care workforce.
Preparing for the Next Hurricane Season
Individuals and organizations are seeking to improve their preparations and resilience for future hurricanes and other disasters, but they have limited time to do so before the coming hurricane season. Individuals noted specific steps that they will likely take to prepare for future hurricanes, including taking out more cash, obtaining medication supplies for longer periods of time, establishing communication plans with friends and families, and identifying safer places to shelter. One major challenge facing individuals, however, is that many houses remain damaged and are unlikely to be repaired before the next hurricane season begins. Hospitals and clinics are also reviewing their disaster response plans. They noted that their top priorities include facilitating access to power and communications by expanding generator capacity, exploring solar power options, identifying ways to ensure refrigeration for medications amid power outages, and obtaining satellite phones. Other actions they noted are improving the pre-staging of supplies, identifying patients with health needs to ensure that they have adequate medications and supplies, collecting and documenting information to assist with disaster response (e.g., location coordinates and generator fuel capacity), and planning for rapid support of staff. Some providers noted that they are reviewing their budgeting for emergency response and exploring options, such as obtaining mobile units, to expand their capacity to provide services in the community in the aftermath of a disaster. It was noted that clinics played a key role in the immediate response, as they were able to reach people quickly, and that it will be important to recognize and enhance their response capacity in the future. Interviewees noted that, while some steps can be taken quickly to improve recovery and response efforts, others will take time that extends beyond the coming hurricane season.

Conclusion
In September 2017, Hurricanes Irma and Maria created historic damage to Puerto Rico and USVI, exacerbating preexisting economic and health issues. Six months after the storms, continued progress has occurred with recovery, but much work remains. Individuals’ lives remain disrupted, with many homes still damaged and individuals continuing to face financial pressures and insecurity. While power has been largely restored in USVI, the territory’s hospitals continue to deal with significant infrastructural damage, limiting service capacity. In Puerto Rico, power remains unstable, and remote areas continue to face major access challenges. In both territories, increased outmigration of providers has increased pre-existing access limitations for both specialty and mental health care. At the same time, mental and physical health needs have increased, particularly for depression, anxiety, and chronic conditions such as diabetes and hypertension. Children, elderly individuals, and people with disabilities have been particularly affected and face ongoing challenges, including loss of support as family members leave the islands. The temporary federal funding relief for Medicaid passed by Congress will provide essential support for the territories’ health care system, but the relief funding does not address underlying fiscal problems or the disparity in federal Medicaid match rates and the cap on federal Medicaid funds faced by the territories. Individuals and organizations are taking steps to prepare for future natural disasters but have limited time and resources to prepare for the coming hurricane season, which is just weeks away.
Endnotes
- The Territory Clause of the U.S. Constitution and subsequent case law authorize Congress to treat territories differently than states under federal laws and programs as long as there is a “rational basis” for the differential treatment. Federal law provides that residents of the territories are generally not required to pay federal income tax, and the territories have special rules regarding Medicaid, Medicare and Supplemental Security Income (SSI). Congressional Task Force on Economic Growth in Puerto Rico, Report to the House and Senate (Washington, DC: Dec. 20, 2016), https://www.finance.senate.gov/imo/media/doc/Bipartisan%20Congressional% 20Task%20Force%20on%20Economic%20Growth%20in%20Puerto%20Rico%20Releases%20Final%20Report.pdf. ↩︎
- U.S. Federal Emergency Management Agency, “Six Months After Maria: Progress Made, Work Continues” (Washington, DC: Federal Emergency Management Agency, Mar. 16, 2018), https://www.fema.gov/news-release/2018/03/16/six-months-after-maria-progress-made-work-continues, accessed Apr. 18, 2018. ↩︎
- Government of Puerto Rico, “StatusPR” (Puerto Rico, 2018), http://status.pr/?lng=en, accessed Apr. 18, 2018. ↩︎
- U.S. Federal Emergency Management Agency, “Power Restored to All Eligible Electric Customers in U.S. Virgin Islands” (Washington, DC: Federal Emergency Management Agency, Mar. 9, 2018), https://www.fema.gov/news-release/2018/03/09/power-restored-all-eligible-electric-customers-us-virgin-islands, accessed Apr. 18, 2018. ↩︎
- Lucia Molina, Registrations and Occupancy Report in Lodgings Endorsed by the PRTC (San Juan, Puerto Rico: Government of Puerto Rico, Puerto Rico Tourism Company, Mar. 12, 2018), https://www.prtourism.com/dnn/Portals/0/PDF_Statistics/JanREG_OCUP18.pdf?ver=2018-03-12-165327-520; Lucia Molina, Registrations and Occupancy Report in Lodgings Endorsed by the PRTC (San Juan, Puerto Rico: Government of Puerto Rico, Puerto Rico Tourism Company, Aug. 29, 2017), https://www.prtourism.com/dnn/Portals/0/PDF_Statistics/Jan17Registration_Occupancy.pdf?ver=2018-02-09-121921-447. ↩︎
- Government of Puerto Rico, “StatusPR” (Puerto Rico, 2018), http://status.pr/?lng=en, accessed Apr. 18, 2018. ↩︎
- U.S. Virgin Islands Department of Tourism, “U.S. Virgin Islands Update: March 1, 2018” (U.S. Virgin Islands: Department of Tourism, Mar. 1, 2018), https://drive.google.com/file/d/19j-_x2ogDQmismkELD9LVsjSsFT_WeGx/view, accessed Apr. 18, 2018; see also Beverly Nicholson-Doty, “United States Virgin Islands” (U.S. Virgin Islands: Commissioner of Tourism, Feb. 6, 2018), http://myemail.constantcontact.com/U-S–VIRGIN-ISLANDS-TRAVEL-UPDATE-FROM-COMMISSIONER-OF-TOURISM-BEVERLY-NICHOLSON-DOTY—FEBRUARY-6–2018.html?soid=1101882102592&aid=qGRDSUuX-VQ, accessed Apr. 18, 2018. ↩︎
- FEMA Spokesperson, Apr. 16, 2018; see also U.S. Federal Emergency Management Agency, “Puerto Rico Hurricane Maria (DR-4339)” (Washington, DC: Federal Emergency Management Agency, last updated Dec. 7, 2017), https://www.fema.gov/disaster/4339, accessed Apr. 18, 2018. ↩︎
- U.S. Federal Emergency Management Agency, “FEMA Provides Alternatives for Verifying Proof of Ownership in Puerto Rico” (Washington, DC: Federal Emergency Management Agency, Mar. 10, 2018), https://www.fema.gov/news-release/2018/03/10/fema-provides-alternatives-verifying-proof-ownership-puerto-rico, accessed Apr. 18, 2018. ↩︎
- U.S. Federal Emergency Management Agency, “Hurricane Survivors Have Until June 18 to Register with FEMA” (Washington, DC: Federal Emergency Management Agency, Mar. 15, 2018), https://www.fema.gov/news-release/2018/03/15/hurricane-survivors-have-until-june-18-register-fema-0, accessed Apr. 18, 2018. ↩︎
- U.S. Department of Health & Human Services, “Public Health Emergency: HHS Office of the Assistant Secretary for Preparedness and Response” (Washington, DC: Assistant Secretary for Preparedness and Response (ASPR), Apr. 5, 2018), https://www.phe.gov/about/aspr/Pages/default.aspx, accessed Apr. 18, 2018. ↩︎
- U.S. Department of Health and Human Services, “About HRSA” (Washington, DC: Health Resources & Services Administration, November 2017), https://www.hrsa.gov/about/index.html, accessed Apr. 18, 2018. ↩︎
- U.S. Federal Emergency Management Agency, “Six Months After Maria: Progress Made, Work Continues” (Washington, DC: Federal Emergency Management Agency, Mar. 16, 2018), https://www.fema.gov/news-release/2018/03/16/six-months-after-maria-progress-made-work-continues, accessed Apr. 18, 2018. ↩︎
- FEMA spokesperson, Apr. 16, 2018. ↩︎
- Government of Puerto Rico, Department of Education, “Departamento de Educación Anuncia las 828 Escuelas Operacionales Para el Curso Escolar 2018-19” (San Juan, Puerto Rico: Government of Puerto Rico, Department of Education, Apr. 5, 2018), https://twitter.com/EDUCACIONPR/status/981998908732792833, accessed Apr. 18, 2018. ↩︎
- Jason Bram, Puerto Rico and the U.S. Virgin Islands After Hurricanes Irma and Maria, Economic Press Briefing (New York, NY: Federal Reserve Bank of New York, Feb. 22, 2018), https://www.newyorkfed.org/medialibrary/media/press/PressBriefing-PuertoRico-USVI-February222018.pdf. ↩︎
- Government of Puerto Rico. “New Fiscal Plan for Puerto Rico” (San Juan, Puerto Rico: Apr. 5, 2018), http://www.aafaf.pr.gov/assets/newfiscalplanforpuerto-rico-2018-04-05.pdf, accessed Apr. 18, 2018. ↩︎
- Edwin Meléndez and Jennifer Hinojosa, Research Brief: Estimates of Post-Hurricane Maria Exodus from Puerto Rico (New York, NY: Center for Puerto Rican Studies, CUNY Hunter College, October 2017), https://centropr.hunter.cuny.edu/sites/default/files/RB2017-01-POST-MARIA%20EXODUS_V3.pdf. ↩︎
- Edwin Meléndez and Jennifer Hinojosa. Research Brief: Estimates of Post-Hurricane Maria Exodus from Puerto Rico (New York, NY: Center for Puerto Rican Studies, CUNY Hunter College, October 2017), https://centropr.hunter.cuny.edu/sites/default/files/RB2017-01-POST-MARIA%20EXODUS_V3.pdf. ↩︎
- Comisión Para la Prevención del Suicidio. Estadísticas Preliminares de Casos de Suicidio, Puerto Rico, Febrero 2018 (Rio Piedras, Puerto Rico: Puerto Rico Department of Health, February 2018), http://www.salud.gov.pr/Estadisticas-Registros-y-Publicaciones/Estadisticas%20Suicidio/Febrero%202018.pdf. ↩︎
- Comisión Para la Prevención del Suicidio. Estadísticas Preliminares de Casos de Suicidio, Puerto Rico, Febrero 2018 (Rio Piedras, Puerto Rico: Puerto Rico Department of Health, February 2018), http://www.salud.gov.pr/Estadisticas-Registros-y-Publicaciones/Estadisticas%20Suicidio/Febrero%202018.pdf. ↩︎
- Frances Robles, et al, New York Times. “Official Toll in Puerto Rico: 64. Actual Deaths May be 1,052.” (New York, NY: The New York Times, Dec. 9, 2017), https://www.nytimes.com/interactive/2017/12/08/us/puerto-rico-hurricane-maria-death-toll.html. ↩︎
- United States Virgin Islands Department of Justice, Press Release: AG Walker: Five hurricane-related deaths recorded in the Territory (USVI: Department of Justice, Office of the Attorney General, Oct. 2, 2017), http://usvidoj.codemeta.com/documents/AG%20Walker%20said%20five%20hurricane-related%20deaths%20recorded%20in%20the%20Territory.pdf. ↩︎
- Frances Robles, et al, New York Times. “Official Toll in Puerto Rico: 64. Actual Deaths May be 1,052.” (New York, NY: The New York Times, Dec. 9, 2017), https://www.nytimes.com/interactive/2017/12/08/us/puerto-rico-hurricane-maria-death-toll.html. ↩︎
- Office of the Governor of Puerto Rico. “Governor Rosselló establishes working group to revise the number of deaths related to Hurricane Maria” (San Juan, Puerto Rico: La Fortaleza, Oficina del Gobernador, Jan. 4, 2018), http://www.fortaleza.pr.gov/content/governor-rossell-establishes-working-group-revise-number-deaths-related-hurricane-maria, accessed Apr. 18, 2018. ↩︎
- George Washington University Division of External Relations. “SPH Research Project to Study Hurricane Mortality in Puerto Rico” (Washington, DC: George Washington University, Feb. 22, 2018), https://gwtoday.gwu.edu/sph-research-project-study-hurricane-mortality-puerto-rico, accessed Apr. 18, 2018. ↩︎
- Government of Puerto Rico, Department of Health. “Directorio de Hospitales Publicos y Privados” (Rio Piedras, Puerto Rico: Department of Health), http://www.salud.gov.pr/Servicios-al-Ciudadano/Pages/Directorio-de-Hospitales-Publicos-y-Privados.aspx, accessed Apr. 18, 2018. ↩︎
- Kaiser Family Foundation, “Health Centers in Puerto Rico: Operational Status after Hurricane Maria” (Washington, DC: Kaiser Family Foundation, Mar. 16, 2018), https://modern.kff.org/medicaid/fact-sheet/health-centers-in-puerto-rico-operational-status-after-hurricane-maria/, accessed Apr. 18, 2018. ↩︎
- Government of USVI, Department of Health. “Department Overview” (USVI: Department of Health), http://doh.vi.gov/about/overview.html, accessed Apr. 18, 2018. ↩︎
- Kaiser Family Foundation, “Health Centers in Puerto Rico: Operational Status after Hurricane Maria” (Washington, DC: Kaiser Family Foundation, Mar. 16, 2018), https://modern.kff.org/medicaid/fact-sheet/health-centers-in-puerto-rico-operational-status-after-hurricane-maria/, accessed Apr. 18, 2018. ↩︎
- 115th Congress of the United States of America. H.R. 1892. “Bipartisan Budget Act of 2018” (Washington, DC: U.S. Congress, Jan. 3, 2018), https://www.congress.gov/115/bills/hr1892/BILLS-115hr1892enr.pdf. ↩︎
- Government of Puerto Rico. “New Fiscal Plan for Puerto Rico” (San Juan, Puerto Rico: Apr. 5, 2018), http://www.aafaf.pr.gov/assets/newfiscalplanforpuerto-rico-2018-04-05.pdf, accessed Apr. 18, 2018. ↩︎
- Medicaid and CHIP Payment and Access Commission, Medicaid and CHIP in Puerto Rico (Washington, DC: Medicaid and CHIP Payment and Access Commission, February 2018), https://www.macpac.gov/wp-content/uploads/2016/09/Medicaid-and-CHIP-in-Puerto-Rico.pdf. ↩︎
- Government of Puerto Rico. “New Fiscal Plan for Puerto Rico” (San Juan, Puerto Rico: Apr. 5, 2018), http://www.aafaf.pr.gov/assets/newfiscalplanforpuerto-rico-2018-04-05.pdf, accessed Apr. 18, 2018. ↩︎