
Medicaid Balancing Incentive Program: A Survey of Participating States
Introduction
Developing and expanding home and community-based alternatives to institutional care is a priority for many state Medicaid programs, and significant progress has been made over the last twenty years to increase the percentage of long-term services and supports (LTSS) dollars that go toward providing HCBS (Figure 2). The Affordable Care Act (ACA) established the Medicaid Balancing Incentive Program (BIP) as one option available to states to further support LTSS rebalancing efforts.
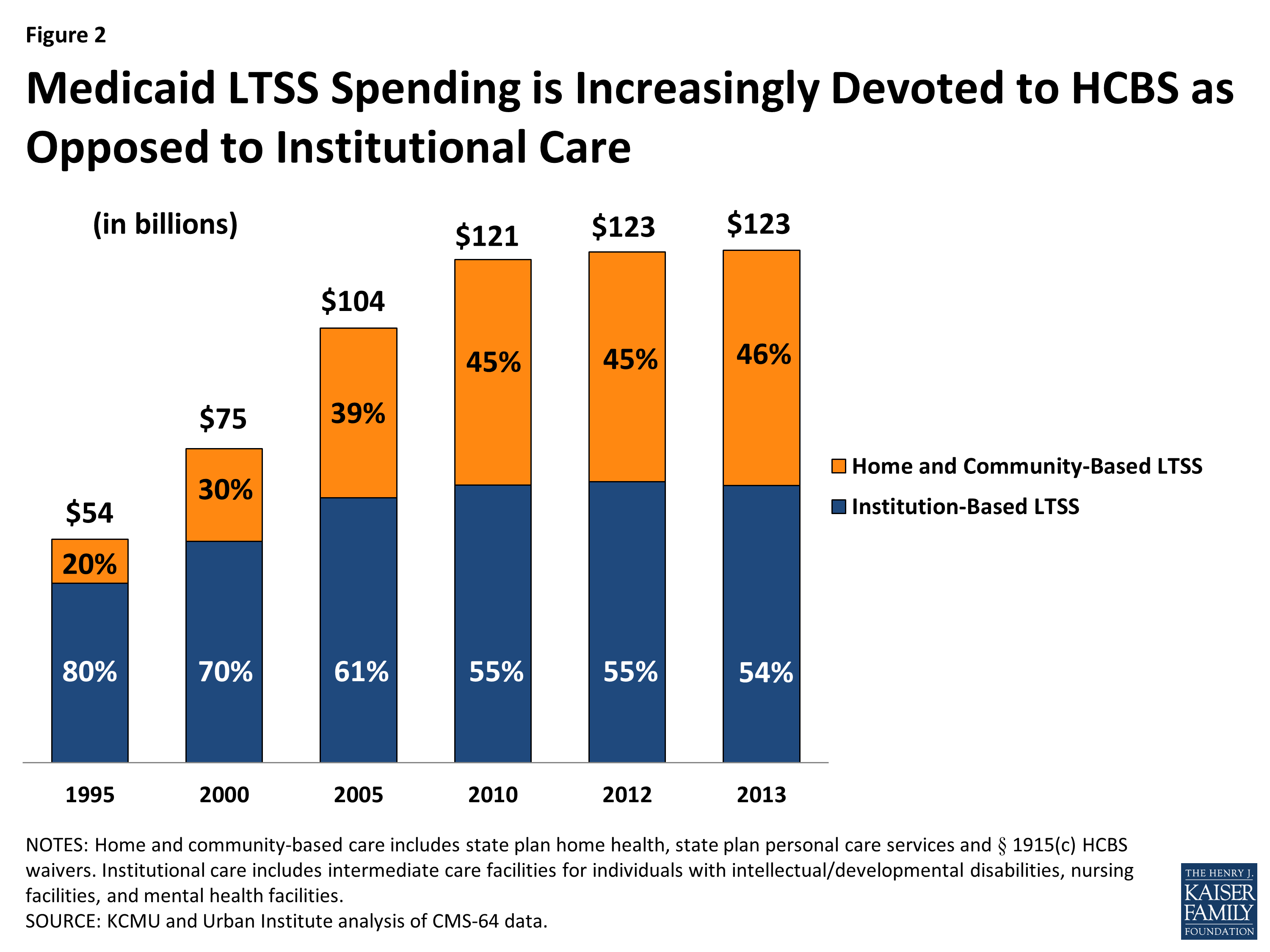
Figure 2: Medicaid LTSS Spending is Increasingly Devoted to HCBS as Opposed to Institutional Care
As of May 2015, eighteen states are participating in BIP (Figure 3). Twenty-one of 38 eligible states were approved for BIP; however, three states are no longer participating. BIP authorizes $3 billion in enhanced federal funding from October 2011 through September 2015 for the provision of new or expanded home and community-based services (HCBS) as an alternative to institutional care.
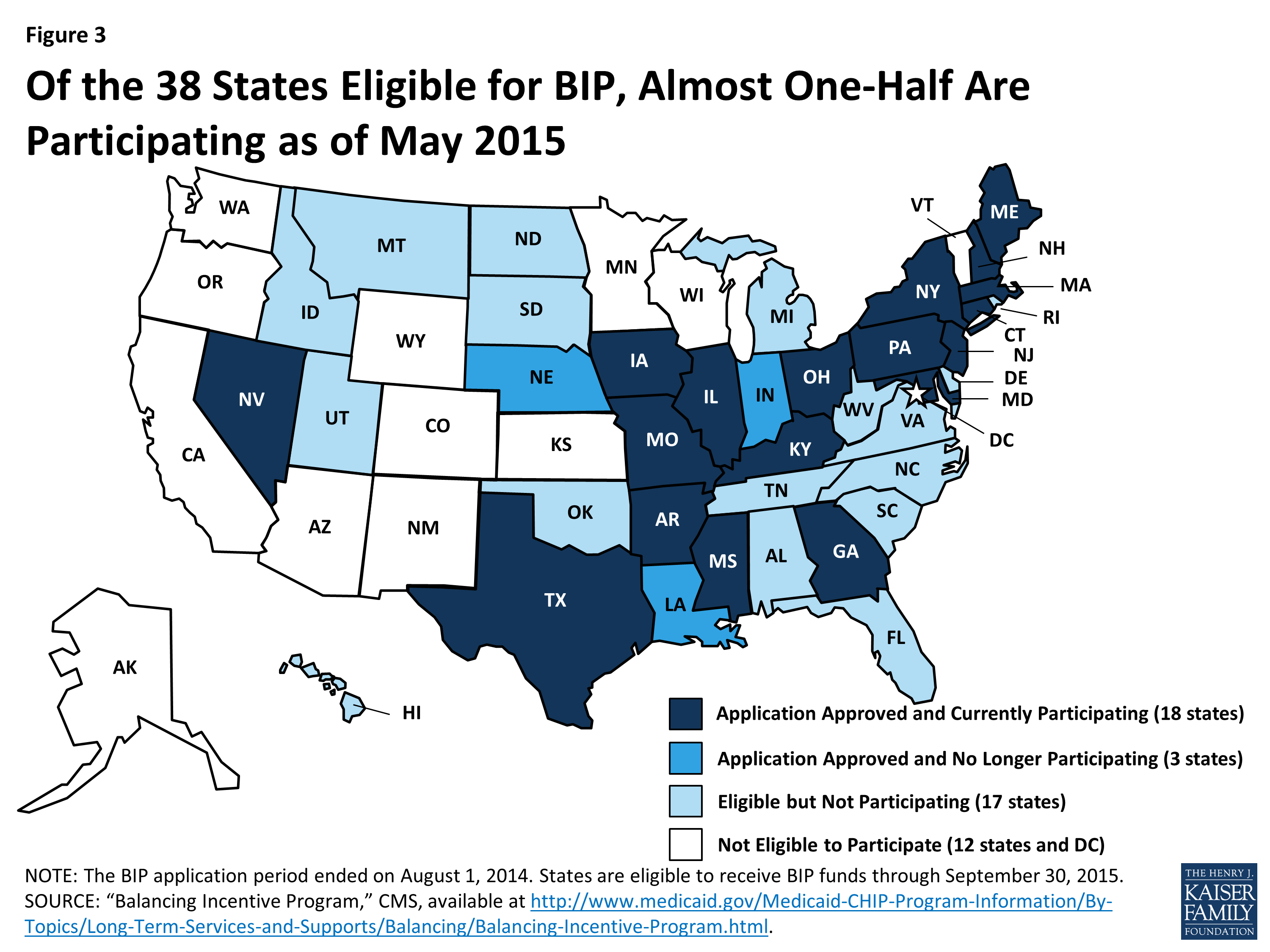
Figure 3: Of the 38 States Eligible for BIP, Almost One-Half Are Participating as of May 2015
Under BIP, states that devoted less than 50 percent of their total Medicaid LTSS spending to HCBS in Fiscal Year (FY) 2009 are eligible for an enhanced Federal Medical Assistance Percentage (FMAP) for all Medicaid HCBS provided from October 2011 through September 2015. States that spent less than 25 percent (1 state) must adopt a target of 25 percent of total LTSS spending on HCBS by September 2015, and can receive a five percent increase in their FMAP. States that spent between 25 to 50 percent of their Medicaid LTSS dollars on HCBS (the remainder of states) must adopt a target of 50 percent of total LTSS spending on HCBS and are eligible to receive a two percent increase (Figure 4). BIP states must use the enhanced federal funds to expand or enhance HCBS and may not adopt more restrictive eligibility standards than were in place on December 31, 2010.1
In addition to reaching the financial benchmarks, states participating in BIP must make the following three structural changes in their Medicaid LTSS delivery systems:
- A “no wrong door”/single entry point system (NWD/SEP) for all LTSS;
- Conflict-free case management (CFCM) services (to avoid conflicts among agencies that provide both individual assessments and service delivery); and
- A core standardized assessment (CSA) instrument to determine eligibility for HCBS.2
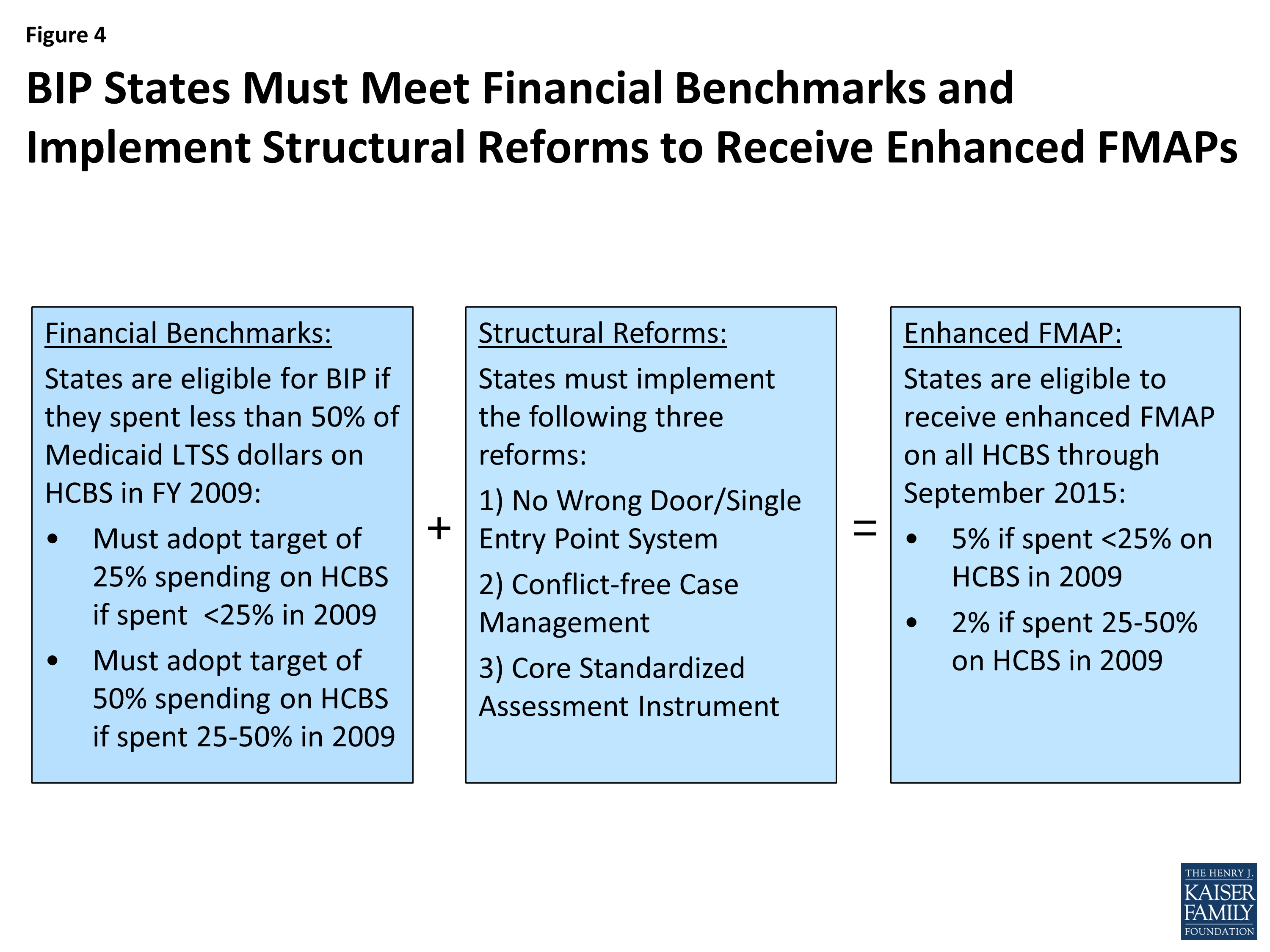
Figure 4: BIP States Must Meet Financial Benchmarks and Implement Structural Reforms to Receive Enhanced FMAPs
Methodology
During the summer of 2014, the Kaiser Family Foundation’s Commission on Medicaid and the Uninsured surveyed BIP states about basic program information, progress with implementing the BIP structural requirements, stakeholder engagement, evaluation activities, and the use of enhanced federal funds in support of other Medicaid LTSS rebalancing efforts. Each state approved to participate in BIP as of September 2014 (21 states) received the written survey instrument, and 17 states (81%) submitted a complete questionnaire. Of the 17 states that responded, 16 states are currently participating in BIP, and one state (LA) is no longer participating. Four states (AR, GA, IN, and NE) opted not to participate in the survey; Indiana indicated its intent to withdraw from BIP, and Nebraska was newly approved in September 2014, but has since withdrawn from BIP. Given that states were at various stages of implementation during the survey period (May through August 2014), not all of the survey questions were applicable to every state’s program. States ineligible to participate in BIP (12 states and DC) as well as states that were eligible but not participating (17 states) were not surveyed. The data summarized here were provided directly from BIP Project Directors and other state staff. The full survey instrument can be found in Appendix A of this report.
Key Findings
1. States report that BIP is helping them achieve their goal of rebalancing LTSS in favor of HCBS.
States’ motivations for pursuing BIP were to gain access to enhanced federal funding to support HCBS, improve their LTSS eligibility determination and service planning infrastructure, and expand access to Medicaid LTSS relative to institutional services.
BIP represents a significant funding opportunity for LTSS delivery reform and rebalancing LTSS expenditures. States cited the ability to access the enhanced federal match as a major motivation for pursuing BIP. States, such as Connecticut and Maryland, that are taking advantage of the Community First Choice (CFC) option, with its own enhanced funding, also have the ability to stack enhanced FMAPs and further LTSS rebalancing efforts.
Project Directors reported that BIP provided an opportunity to fund some needed infrastructure changes and quality improvement efforts, including the CSA and the NWD/SEP system. BIP has enabled states to streamline access to and information about community services and supports through implementation of the required structural changes. For example, states noted that by implementing a standardized assessment tool, individuals would not have to go through multiple assessment processes associated with different waivers to find the one that best meets their needs.
States provided examples of how BIP supported structural reforms in their LTSS systems, such as the following:
Illinois cited the policy expertise and access to technical assistance available through BIP as a major motivation for pursuing BIP and providing critical resources to adopt and implement structural changes in the state’s LTSS system.
Connecticut reported that BIP helped the state focus on building consensus across departments to develop a NWD/SEP system and common assessment tool.
States also reported that BIP helped them expand access to HCBS in lieu of institutional services. For example, Illinois stated that BIP helped facilitate the implementation of consent decrees resulting from three Olmstead class action lawsuits impacting Medicaid beneficiaries residing in institutional settings. The settlements resulted in additional funds devoted to transition assistance and other HCBS so that individuals can live in the most integrated community-based setting appropriate for their needs.
Medicaid LTSS spending on HCBS increased by more than one quarter in 14 BIP states between 2009 and 2014.
Eighteen states reported positive gains in the amount of Medicaid LTSS spending devoted to HCBS since 2009, with 14 states increasing HCBS spending by at least 25 percentage points between 2009 and the end of 2014 (Figure 5). Eight states reported already exceeding the target of 50 percent of LTSS spending on HCBS by the fourth quarter of 2014, while the remaining BIP states are making progress toward their spending goal (Table 1). The one state with a 25 percent spending target (MS) reported exceeding its target by the fourth quarter of 2014. Since 2009, the year on which eligibility for BIP was based, Mississippi (111%) and Ohio (86%) have
made the largest gains in the percentage of total LTSS dollars devoted to HCBS.
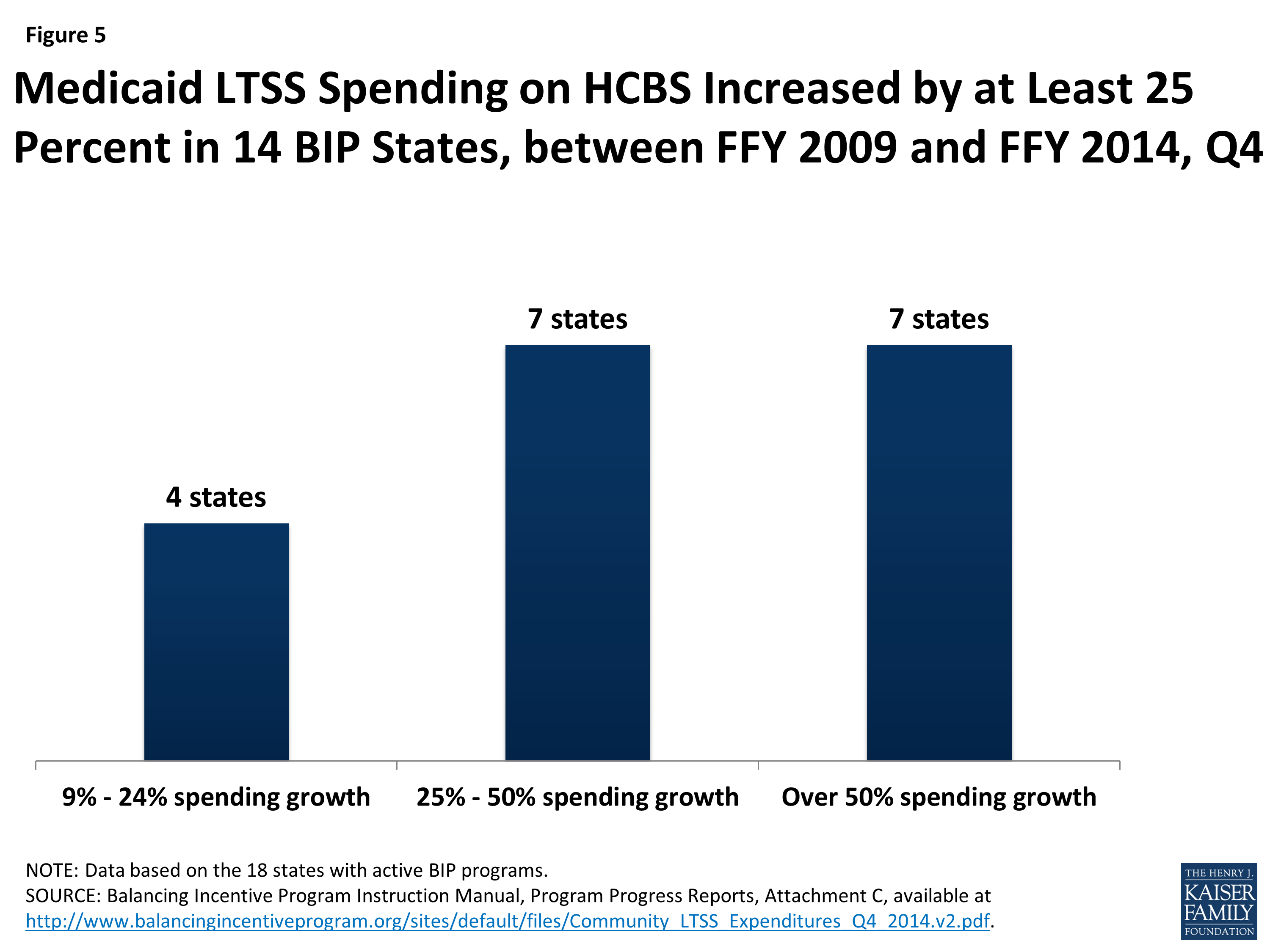
Figure 5: Medicaid LTSS Spending on HCBS Increased by at Least 25 Percent in 14 BIP States, between FFY 2009 and FFY 2014, Q4
| Table 1: Share of Total Medicaid LTSS Dollars Devoted to HCBS in BIP States | |||
| State | Share of Total Medicaid LTSS Dollars Devoted to HCBS |
Percentage Change from
FFY 2009 to FFY 2014, Q4
|
|
| FFY 2009 | FFY 2014, Q4 | ||
| Arkansas | 29.8% | 49.7% | 66.8% |
| Connecticut | 44.1% | 48.1%* | 9.1% |
| Georgia | 37.4% | 47.5% | 27.0% |
| Illinois | 27.8% | 44.3% | 59.4% |
| Iowa | 39.8% | 51.1% | 28.4% |
| Kentucky | 31.1% | 49.5% | 59.2% |
| Louisiana** | 36.4% | 44.8% | 23.1% |
| Maine | 49.1% | 56.8% | 15.7% |
| Maryland | 36.8% | 58.9% | 60.1% |
| Massachusetts | 44.8% | 65.1% | 45.3% |
| Mississippi | 14.4% | 30.4% | 111.1% |
| Missouri | 40.7% | 56.6% | 39.1% |
| Nevada | 41.6% | 48.8% | 17.3% |
| New Hampshire | 41.2% | 46.5%* | 12.9% |
| New Jersey | 26.0% | 46.1% | 77.3% |
| New York | 46.7% | 58.8% | 25.9% |
| Ohio | 32.5% | 60.5% | 86.2% |
| Pennsylvania | 33.0% | 45.1% | 36.7% |
| Texas | 46.9% | 58.8% | 25.4% |
|
NOTES: Table omits 2 states (IN and NE) that withdrew from BIP and did not participate in KCMU’s survey. *FFY 2014 Q4 data are not available, so FFY 2014 Q3 data are shown for CT and NH. **As of December 2014, Louisiana is no longer participating in BIP.
SOURCE: Balancing Incentive Program Instruction Manual, Program Progress Reports, Attachment C, available at http://www.balancingincentiveprogram.org/sites/default/files/Community_LTSS_Expenditures_Q4_2014.v2.pdf.
|
|||
BIP Project Directors were asked to report on strategies that are helping states reach their Medicaid HCBS spending goal (of 25% or 50% of total Medicaid LTSS dollars). The most frequently reported strategy was increasing the number of transitions from institutions to HCBS. Several states cited building upon their Money Follows the Person (MFP) demonstration achievements in rebalancing as helping them make progress toward the goal of increasing spending on HCBS. These achievements included improvements to IT systems and streamlining access to services for beneficiaries. States also reported that increasing the number of HCBS waiver slots and increasing outreach and education efforts around HCBS options were effective approaches to increase both total and relative HCBS spending. Other responses included: financial incentives for managed care organizations (MCOs) to provide increased community capacity, implementation of managed long-term services and supports (MLTSS) programs, institutional payment rate reductions, and implementing CFC.
All BIP states anticipate that the program’s required structural reforms will increase beneficiary access to HCBS.
Several states anticipate a significant increase in beneficiary access to HCBS, as a result of BIP’s structural requirements and as barriers to access are removed. Streamlined eligibility processes and access through NWD/SEP entities are expected to increase access to HCBS. Across the states, the development and expansion of the NWD/SEP system seeks to provide unbiased information to individuals seeking LTSS. The initial screening is used to prioritize those who are most at risk for institutionalization, and the CSA ensures that an objective tool is used across multiple programs to assess the functional needs of individuals applying for services. The CSA helps ensure that beneficiaries do not have to repeat their stories, and increased efficiency in the assessment and service plan development processes may reduce delays in service initiation.
State examples in this area included the following:
Iowa designed an integrated database that supports the information and referral functions of its toll-free number and website with a goal of expanding access to information about LTSS regardless of funding source or level of need. Transportation information will also be included in the database and is anticipated to increase beneficiary access to HCBS.
In Texas, individuals will be able to access Texas’ initial screening instrument via the web, telephone, or by visiting an Aging and Disability Resource Center (ADRC). The initial screening will cover all areas of LTSS and will provide individuals with a list of referrals to the agencies that can best meet their needs. Additionally, the agencies will receive the referral information and will contact the individual, if the person consents. Collectively, these process improvements have the potential to allow quicker, more efficient access to HCBS for individuals and families (including caregivers).
2. BIP is helping states make further progress in streamlining and standardizing the infrastructure that facilitates beneficiary access to HCBS.
Half of BIP states had a NWD/SEP system in place prior to BIP, and states are using BIP to further develop these systems to increase beneficiary access to HCBS.
A NWD/SEP system aims to provide individuals with information about HCBS, determine eligibility, and enroll individuals in services. NWD/SEP systems can take many different forms depending on how they are defined.3 In many states, the ADRC networks serve as the NWD/SEP system, providing outreach, access to information, and referrals for public and non-profit community-based providers. As a result of BIP, Project Directors reported making changes to new or existing NWD/SEP systems including implementing enhanced options counseling, coordinating and integrating data across multiple entry points, expanding local ADRC coverage areas, streamlining access to HCBS across different disability populations and care settings, and collaborating across government agencies and programs to implement a more unified information and referral system for LTSS. Project Directors noted that NWD/SEP system improvements could be achieved through meeting BIP infrastructure requirements that include designation of NWD/SEP systems, a website about HCBS options in the state, and a statewide 1-800 number that connects individuals to the NWD/SEP.
The following are selected state-specific examples of progress toward implementing a NWD/SEP system as a result of BIP:
Prior to BIP, Missouri’s state Medicaid and collaborating agencies interacted at the local level on a daily basis via phone and email. BIP funding has allowed the state to enhance the existing process so that any of the state agencies, HCBS providers, other stakeholders, and the public can utilize the toll-free number and website to access information about HCBS.
Connecticut is integrating its NWD/SEP eligibility system as a result of BIP. The new system will automate and coordinate functional assessments and financial eligibility determinations for LTSS. It will also include a predictive modeling feature that will assist both with pre-screening applications as well as linking the applicant with an appropriate case manager based on service needs. Through the creation of a personal account within the NWD/SEP system, beneficiaries will be able to request non-medical transportation services and view their personal health record, assessments, care plans, and Medicaid benefit statement.
Maine is expanding its NWD/SEP system to include mental health entities, an LTSS website, the state’s financial eligibility determination agency, Center for Independent Living, Medicaid eligibility office, and the 2-1-1 toll-free information line. Maine’s 2-1-1 will be strengthened and enhanced under BIP by becoming Maine’s comprehensive statewide directory for information and referrals regarding Maine’s LTSS. Assistance from Maine’s 2-1-1 could include triage and referral, assistance with pre-screening/application, and transfer to an assisting agency within Maine’s NWD/SEP system. Training for Maine’s 2-1-1 call center operators will be expanded to include information about Medicaid LTSS eligibility, the functional assessment process, and enhancement of the 2-1-1 resource database. State NWD/SEP system entities will also be trained on all available LTSS for adults and children with physical, intellectual, and behavioral health disabilities. Trainings for NWD/SEP entities will include information on the assessment process, eligibility, contracted agencies, and prescreening.
Nearly three-quarters of BIP states (12 of 17) had a CFCM system in place prior to BIP, for at least some of their HCBS programs, and states are using BIP to expand firewalls and CFCM across all medical and LTSS services.
As defined in CMS guidance, conflicts may arise when a social service organization serves as both the agency assessing the individual for services and the agency delivering the services.4 This can result in either over or under utilization of services or development of a care plan that does not promote independence and is not person-centered. While there is no template for CFCM for states to insert into the design of their existing LTSS systems, CMS did provide guidance on some key elements of a CFCM system, including a care plan that is free from bias and influence.5 Key elements in designing a CFCM system include: clinical or non-financial eligibility determination separate from direct service provision, use of case managers and evaluators of beneficiaries’ need for services not related to the consumer, ensuring robust oversight and monitoring, having clear pathways for grievances and appeals, and facilitating meaningful stakeholder engagement.6
While most states had some elements of CFCM in place prior to BIP, some states noted their behavioral health Medicaid programs were not conflict-free (for example, individual providers could both determine eligibility and offer services) and are working to mitigate this issue for these services. States with existing CFCM systems reported a number of strategies in place to mitigate potential conflicts including administrative firewalls, beneficiary choice, data driven assessments, robust quality management programs, grievance procedures and state oversight.
Some state-specific examples include:
Texas monitors CFCM through state approval of care plans, a beneficiary satisfaction survey, analysis of referrals, a beneficiary complaint system, and data-driven assessments.
Iowa held a series of stakeholder engagement sessions with a representative group of case managers to capture current model practices and garner support for recommended changes to state regulations to formalize CFCM procedures. In addition, the state Medicaid agency’s HCBS Quality Assurance Team and state Division of Mental Health and Disability Services will integrate questions to evaluate CFCM into routine surveys of all providers. The state’s program integrity unit is also conducting quarterly analyses to determine areas of potential concern and monitor potentially problematic utilization patterns, such as service systems that provide both case management as well as home and community-based waiver services.
As a result of BIP, states are working to develop core standardized assessment instruments; prior to BIP, almost all (15 of 17) states were using multiple population-specific functional needs assessment instruments.
The goal of BIP’s CSA requirement is to develop an instrument that determines eligibility for Medicaid HCBS, identifies an individual’s service and support needs, and informs their care plan.7 Per CMS guidance, the CSA instrument and assessment process should be uniform for a given population across the state. The CSA should capture a Core Dataset (CDS) that includes activities of daily living (ADLs), instrumental activities of daily living, medical conditions/diagnoses, cognitive functioning/memory needs, and behavioral needs. Prior to BIP, some states used the same tool to assess seniors and non-elderly adults with physical disabilities; however, most tools were population specific and varied by state. Implementing a standardized automated assessment instrument may help states reduce inefficiencies and administrative burdens associated with having multiple assessments and more equitably allocate services across populations. States can also use the assessment data collected to inform program planning, budgeting, quality monitoring, and reporting.
Some states are further along than others in meeting the CSA requirements. Maine’s existing assessment tools capture all the required CSA domains so the state is now focused on strengthening the coordination of the assessment and referral process. Connecticut developed a single assessment tool for all populations receiving Medicaid services; to start, the state built a cross walk from each of the nine existing tools to the common standard assessment. The state added additional questions specific to each population to the tool. The universal assessment tool will then be automated within the state’s new eligibility management system. In Maryland, BIP provided funding to implement a CSA, including the testing, training, and programming of the tool within a web-based tracking system, and an enhanced web-based eligibility tracking system, including a telephonic time-keeping system for personal assistance providers.
Nevada will be moving to a CSA and converting several manual LTSS processes to more automated IT functions. New York is automating population-specific instruments with the core data set into one system. Texas is adding questions to its assessments related to physical disabilities and mental illness. These questions allow all LTSS beneficiaries an opportunity to discuss mental health issues and limitations related to ADLs.
3. BIP supports LTSS rebalancing efforts by building on existing Medicaid HCBS options available to states.
BIP funds are creating opportunities for states to build on existing Medicaid LTSS funding streams, including Money Follows the Person, to increase beneficiary access to HCBS.
BIP is helping states address longstanding barriers to rebalancing, such as decentralized information and referral systems and lack of standardization across assessment tools. All states that participate in BIP also participate in the MFP demonstration. States reported building upon infrastructure changes and improvements made with MFP to implement BIP. BIP and MFP share a common goal of rebalancing through the use of enhanced funding, with MFP focused on institutional to community transitions and BIP focused on infrastructure reforms. Both programs are designed to work together and across populations in order to expand HCBS options. Relying on stakeholder input and lessons learned from MFP, states reported building broader infrastructure changes, such as a NWD/SEP system or making further improvements to their IT systems and internal processes for a more unified efficient LTSS system.
Most states are using BIP funding to expand HCBS by increasing the number of waiver slots available and provide more beneficiaries with access to HCBS.
Fifteen (of 17) states reported using BIP funding to expand HCBS waiver programs (Figure 6). Of those states, 14 used BIP funding to increase the number of waiver slots available and three states added services to existing waivers. Examples of new services include care management, health promotion and education programs, individual and family support services, substance abuse treatment services, and support broker services for individuals who self-direct their services. Six states (CT, IA, MD, MS, NY and TX) used BIP funding to implement new or expanded ACA LTSS initiatives including CFC, health homes, and the § 1915(i) HCBS state plan option.
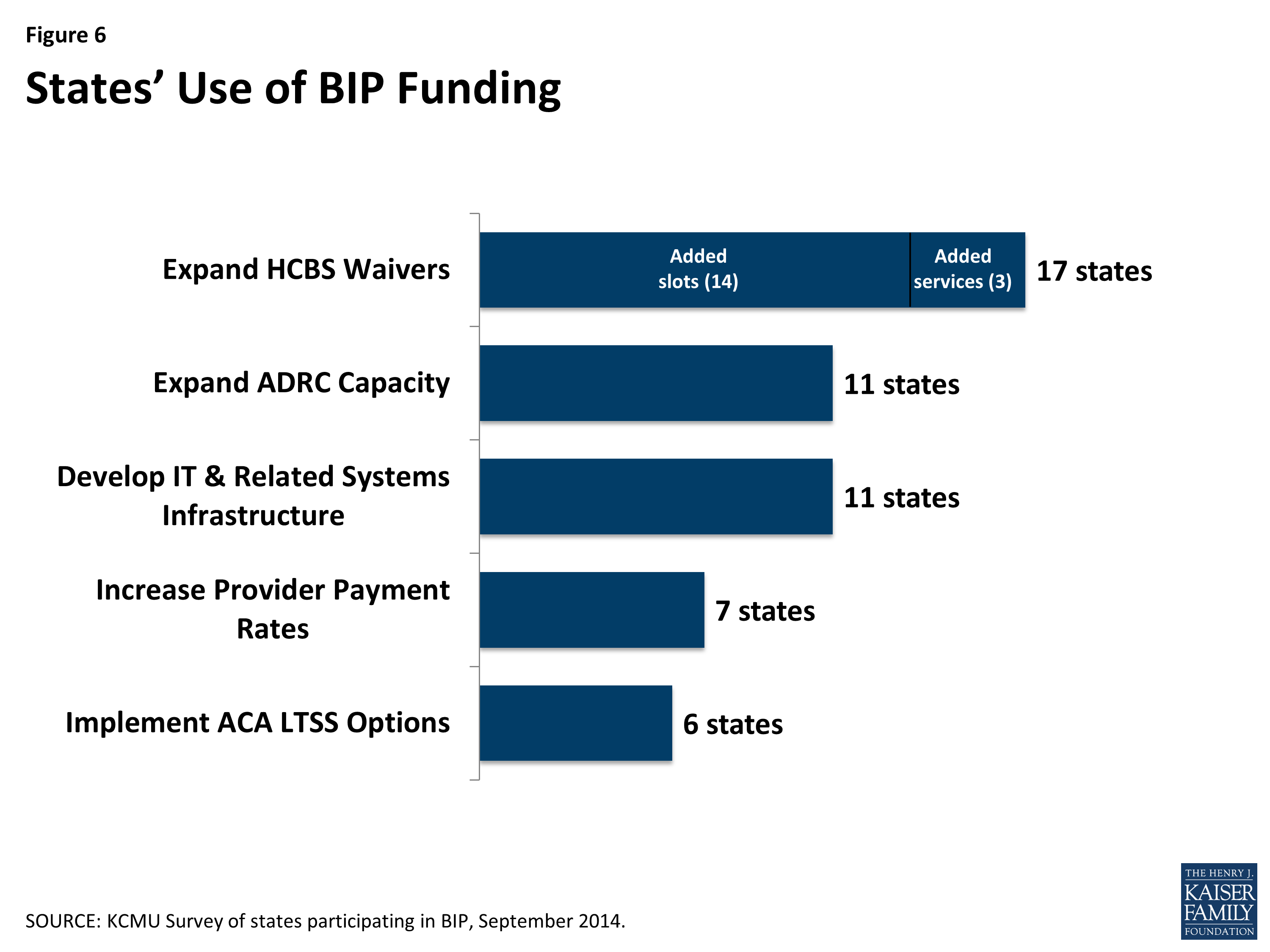
Figure 6: States’ Use of BIP Funding
Iowa participates in MFP and added the health home state plan option and the § 1915(i) HCBS state plan option for adults with serious emotional disturbance. By participating in BIP and expanding these HCBS options, Iowa is moving towards rebalancing LTSS spending.
All 17 BIP states that responded to the survey reported using BIP funds to target specific Medicaid populations including seniors, individuals with physical disabilities and individuals with I/DD. Fifteen states are using BIP funds to target individuals with mental illness, and 12 states are targeting individuals residing in institutions who are transitioning to the community.
States are using BIP funds to support other LTSS initiatives including the ADRC grant programs, training initiatives, and provider payment rate increases.
Most BIP states (13 of 17) reported building on existing ADRC networks to develop the infrastructure needed to develop a NWD/SEP system. Enhancing the state’s ADRC network by increasing their number and coverage areas, requiring all ADRCs to achieve fully functional status, and better integrating Medicaid functional and financial eligibility determination processes will facilitate access to HCBS. BIP Project Directors also reported using the enhanced funds to support the following LTSS initiatives: streamlining or automating beneficiary screenings/assessment (13 states), expanding ADRC capacity (11 states), developing IT and related systems infrastructure (11 states), offering training initiatives for beneficiaries, providers, or health plans (10 states), improving access to substance abuse/rehabilitative services (9 states), and increasing provider payment rates (7 states).
BIP also created opportunities for collaboration across state agencies and with various stakeholder groups. All BIP Project Directors reported partnering with other state agencies, and the majority of states listed partnering with ARDCs (16 states) and Area Agencies on Aging (14 states). Other partnerships included IT and/or technical assistance providers (13), information and referral providers or resource network members (12 states), community behavioral health providers (12 states), and disability service providers (12 states).
4. States report some common challenges encountered to date related to measuring quality, coordinating with capitated managed LTSS delivery systems, and implementing the required structural reforms.
States are collecting a variety of quality data through BIP, but there is little overlap in these measures across HCBS programs and states, which can lead to challenges in evaluating HCBS quality.
States’ varied responses to the quality/evaluation survey question illustrate the challenges associated with uniformly assessing HCBS quality. BIP states are required to collect three types of data: service data (claims/encounter data), quality data linked to population-specific outcomes (captures provider quality of care), and outcome measures (assesses beneficiary satisfaction). States must report to CMS the data and measures that will be collected and the methodology for collecting those measures.8 States most frequently cited ongoing review of HCBS waiver programs, NCQA/HEDIS measures, and the Medicaid Adult Health Quality Measures as their mechanisms in place to track quality. CMS has also awarded Testing Experience and Functional Assessment Tools (TEFT) planning grants to states to use health information technology to develop HCBS quality measures.9 Six BIP states (CT, GA, KY, LA10, MD, NH) have received TEFT funding as of November 2014 (see Text Box 1).
Quality initiatives related to outcomes data focused on the development of measures by population to assess beneficiary and family caregiver experience and satisfaction. Examples include the National Core Indicators and the Participant Experience Survey, as well as the MFP Quality of Life survey for those transitioning from institutions to the community. Other selected examples included Consumer Assessment of Healthcare Providers and Systems (CAHPS), critical incident reporting, and the Mental Health Statistics Improvement Programs Survey. Where possible, states reported choosing BIP reporting measures that overlapped with those used for other HCBS initiatives (for example, health homes and the financial alignment demonstrations for dual eligible beneficiaries) to increase overlap and to move toward standardized quality metrics.
| Text Box 1: Measuring Quality in HCBS Programs Via Testing Experience and Functional Tools (TEFT) Grants |
| The federal Testing Experience and Functional Tools (TEFT) planning and demonstration grants make available up to $45 million ($4 million per awardee) through November 2017 to states to support the collection, testing, and reporting of adult quality measures for use in Medicaid HCBS programs. Any state may apply to participate in one or more of the following TEFT components: (1) test and evaluate a modified set of Continuity Assessment Record and Evaluation (CARE) functional capacity measures; (2) test and evaluate new measures of beneficiary experience in Medicaid HCBS programs; (3) identify and align health information technology practices; and (4) identify and align electronic LTSS standards.Of the nine states with TEFT planning grants, six (CT, GA, KY, LA, MD, and NH) are participating in BIP. All six BIP-TEFT states plan to test the beneficiary experience survey, and four states (CT, GA, KY, LA) plan to test the CARE assessment. States may use TEFT functional assessment measures to meet the BIP core standardized assessment requirement.For more information, see Amended Announcement Invitation to Apply for FY2013, Patient Protection and Affordable Care Act Section 2701, Planning and Demonstration Grant for Testing Experience and Functional Tools in Community-Based Long Term Services and Supports (TEFT), Funding Opportunity Number: CMS-1H1-13-001, available at http://www.medicaid.gov/AffordableCareAct/Downloads/TEFT-FOA-9-10.pdf. |
States that are implementing BIP in a capitated managed LTSS delivery system encounter additional challenges and opportunities in implementing BIP’s structural reforms.
Implementing BIP in a managed care environment requires states to work closely with MCOs to ensure coordinated implementation of the structural requirements. A growing number of states are enrolling seniors and people with disabilities in Medicaid MLTSS programs and implementing initiatives aimed at better coordinating and integrating Medicare and Medicaid services for dual eligible beneficiaries, through capitated or managed fee-for-service arrangements.11 We asked states to describe their MCO coordination efforts to implement the BIP structural requirements. Six BIP states reported operating MLTSS programs, and one state reported interest in moving toward a MLTSS program.
In New Jersey, BIP’s structural requirements were included in the design of its MLTSS program. The state Medicaid agency trained MCOs on these elements before MLTSS was launched. Educational sessions included the elements of CSA, CFCM, and the ADRC as the NWD/SEP. MCOs will be monitored on their use of these requirements.
In Texas, MCOs will be using a common assessment for all LTSS beneficiaries and participating in the initial LTSS screening by receiving referrals electronically. Additionally, MCOs are working with the ADRCs – the basis for the state’s NWD/SEP system – to ensure that the services coordination function fulfills CFCM requirements.
At the same time that states are implementing CFCM systems and policies, several BIP states are also shifting the delivery of LTSS systems to MCOs and acknowledged delineating role separation in a managed care environment as a challenge. The implementation of MLTSS has furthered principles of CFCM through the separation of functional eligibility determination, service planning, and ongoing care coordination functions, but the role of the MCOs in CFCM warrants further monitoring to determine if these processes are conflict-free. In addition, separating functions may result in loss of individual and programmatic expertise, either in an organization or across a population.
States reported challenges related to implementing the BIP structural reforms and are addressing these challenges through additional training and supervision, enhanced IT infrastructure testing, and integration with data management systems.
Developing a functional assessment instrument for individuals with behavioral health needs that incorporates the BIP core data set requirements can be a challenge for states. Several states reported challenges identifying a suitable tool and developing assessment questions for people with behavioral health conditions. For example, Texas reported a challenge with developing assessment questions related to mental health that would be appropriate for “bachelor level” assessors to ask. This challenge is being addressed through training and supervision. Other challenges reported by states related to the timeline for implementation of the core data set requirements (given the additional training involved with a new assessment tool) and the length of time it takes to administer an initial screening.
Once a state’s functional assessment tools are determined to meet BIP’s CSA requirements, attention turns to the IT infrastructure necessary to implement these tools. We asked states to describe how data is accessed by state and local agencies and providers to get a better understanding of information sharing policies. States reported that protected health information is an inherent component of the HCBS waiver case management system and that appropriate protocols for data security have been and are being developed for online systems. In Maryland, beneficiary assessments are stored in a web-based tracking system where the state Medicaid agency, local health departments (assessors), utilization control agent, and support planners have access to client records and assessment data. Other survey responses about data sharing included negotiating details about provider-specific policies, establishing memoranda of understanding between local agencies specifying information sharing policies, and implementing manual processes where documents are transferred within divisions, using HIPAA officers for oversight. Five states reported they were still in the process of developing the necessary data security requirements that set out the information sharing parameters between the states and other local entities. One state noted that it was still in the process of procuring a uniform assessment tool and therefore, the wrap-around IT system had not yet been determined.
States were asked to report on significant challenges related to compliance with CFCM and responses included: the need for more training and skills building in person-centered planning, standardizing multiple care plan formats across waivers and Medicaid services, eliminating paperwork and process duplications and inefficiencies, navigating staff turnover, and achieving financial sustainability. Additional resources may be needed to either train new staff or sustain expertise in a person-centered planning process. It is important to make sure that in an effort to eliminate conflicts, states do not disrupt care coordination efforts and beneficiary access to services.
Another challenge reported by BIP states was the fact that BIP mitigation strategies alone are not enough to comply with the HCBS rule’s CFCM requirements.12 In addition to BIP’s CFCM requirements, the new federal HCBS regulations include requirements to mitigate conflicts of interest.13 States anticipated challenges with defining an approach to CFCM that addresses the specific requirements in both the BIP guidance and the CMS HCBS regulations, often within the context of a rapidly changing LTSS delivery system.
5. While BIP has helped states make progress in LTSS rebalancing, the time-limited nature of the program creates some challenges and leaves open questions about its future.
Most states (14 of 17) report being on pace to meet the structural requirements by BIP’s end date of September 30, 2015, but states also cite the short timeline remaining for the program as a challenge.
BIP Project Directors cited the short timeline for implementation as the most significant challenge related to BIP’s NWD/SEP system requirements. The seven states that were without a NWD/SEP system at the onset of BIP acknowledged challenging aspects of meeting this objective within a limited period of time, including the following: facilitating the necessary interagency collaborations given the multitude of systematic changes underway; aligning program requirements, processes, and vision across the state’s LTSS system, designing the IT infrastructure to house assessment information and share data across agencies; working in an environment of staff and resource shortages; and developing of a long-range sustainability plan that is mutually agreeable and attainable by all collaborating state agencies. States that were further ahead in meeting the BIP NWD/SEP system requirement also reported challenges related to the timeline for implementation and acknowledged that expanding the expertise necessary to assist certain populations, such as those with developmental disabilities or mental illness, takes time and resources.
Strategies that are helping to keep states on pace with the BIP requirements include working with CMS and other TA consultants and collaborating in work groups across various state program offices. Ohio brought together two stakeholder groups – an implementation group and an advisory group – to ensure all stakeholders as well as sister agencies were working together to implement a NWD/SEP system. Iowa highlighted that its NWD/SEP system improvement efforts include expanding the ADRC network and developing a regional base of mental health and disability services, where beneficiaries can choose services from more than one county. While most states reported being on pace to meet the three structural requirements, some expressed concern that the September 30, 2015 expiration of the program poses a challenge. For example, one state reported challenges related to developing and implementing cross-agency electronic systems within this timeframe.
At the time of the survey, only half the states reported having a sustainability plan in place to maintain the structural changes when BIP expires.
All states reported working on a sustainability plan that includes securing funding to support BIP infrastructure changes going forward, but only half had finalized such a plan at the time of the survey. Some of the funding sources identified were state general funds, federal administrative matching funding, and MFP funding (although the MFP demonstration is set to expire in 2016). Sustainability plans require states to make decisions about which state agency will oversee certain aspects of the BIP structural requirements after the program expires.
Follow-up interviews with BIP states that are no longer participating in the program revealed challenges reaching the spending target of 50 percent of total spending on HCBS by the September 2015 deadline. Project directors also cited the inability to sustain the required infrastructure changes (without the enhanced FMAP) as a major factor in states’ decisions to withdraw from BIP. Still, these states made progress towards rebalancing HCBS during the BIP incentive period, and project directors noted that rebalancing efforts are continuing, using the BIP rebalancing objectives, despite withdrawing from BIP.
Conclusion
States are making progress under BIP towards a more unified person-centered LTSS system. Under BIP, the availability of enhanced federal funding is increasing access to Medicaid HCBS. The structural reform requirements are enabling infrastructure improvements that help streamline information and referral services for people needing LTSS and reducing administrative inefficiencies in many states’ eligibility determination and service planning processes. BIP funds are creating opportunity for states to build upon existing Medicaid LTSS rebalancing efforts already underway, including MFP, and make enhancements to LTSS processes, systems, and infrastructure that may be in place long after BIP expires this fall. Congressional action would be needed to extend these two programs, BIP and MFP, and doing so would bolster state efforts to promote access to HCBS. Collectively, these system reform efforts are helping states reach a desired goal of serving Medicaid beneficiaries with LTSS needs in the most integrated setting. Without BIP funding, states will likely be challenged to continue funding the structural requirement implementation and improvement efforts while also monitoring how such efforts advance longstanding rebalancing initiatives and affect beneficiaries, particularly within the context of managed care delivery systems.
