Health Center Patient Trends, Enrollment Activities, and Service Capacity: Recent Experience in Medicaid Expansion and Non-Expansion States
Executive Summary
In thousands of medically underserved communities across the U.S., community health centers enroll low-income people in health coverage and provide care to millions of patients. Against the backdrop of significant health center expansion over several years and a full year of expanded health coverage under the Affordable Care Act (ACA), this brief examines change between 2013 and 2014 in the volume and health coverage profile of health center patients, and health center enrollment activities and service capacity, comparing states that implemented the ACA Medicaid expansion in 2014 and states that did not expand Medicaid in 2014. The study is based on 2014 data from the federal Uniform Data System and a 2014 national survey of health centers.
Several key findings emerged from the analysis:
- In 2014, health centers served 22.5 million patients – an increase of nearly 1.2 million patients over 2013. From 2013 to 2014, the number of health center patients covered by Medicaid rose by 1.85 million, or 22%.
- Between 2013 and 2014, the share of health center patients covered by Medicaid rose from 40% to 46%, the share with private insurance rose from 14% to 16%, and the share who were uninsured declined from 35% to 28%.
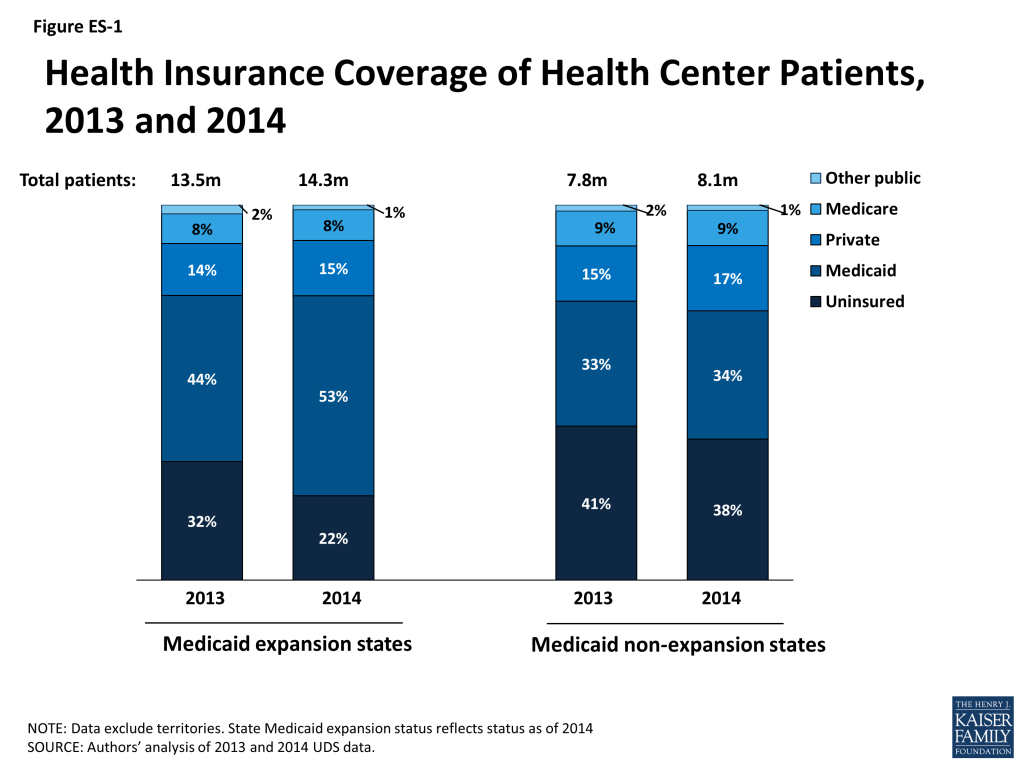
- Changes in health center patient coverage were sharply different between Medicaid expansion and non-expansion states (Figure ES-1). In expansion states, the share of patients with Medicaid rose by 20% and the share who were uninsured fell by 29%. In non-expansion states, the share with Medicaid rose by 3% and the share who were uninsured fell by 8%. Private coverage rates remained low in both groups of states because most health center patients have income below the poverty level and are thus ineligible for Marketplace subsidies.
- During the first ACA open enrollment period, the vast majority of all health centers provided Medicaid application assistance, but expansion states were more likely to assist with renewing Medicaid and selecting Medicaid plans, while non-expansion states were more likely to assist with Marketplace applications and Qualified Health Plan selection.
- Health centers in expansion states were significantly more likely than those in non-expansion states to report having expanded their capacity for dental and mental health services since the start of 2014. They were also more likely to report increased wait times for appointments, possibly reflecting greater increases in demand for services associated with larger gains in coverage among health center patients in these states.
Issue Brief
Introduction
Community health centers play a major role in providing health care for millions of people who reside in areas designated by the federal government as medically underserved, based on high rates of poverty and infant mortality and other measures of health care need.1 In 2014, 1,249 community health centers in the 50 states and DC served nearly 22.5 million people.2 Another 81“look-alike” health centers, which meet all health center requirements but receive no federal funding, served nearly 900,000 additional patients.3 Health center patients are much more likely to be poor or low-income than Americans overall, and they are much more likely to be uninsured.4 Six in ten health center patients are nonelderly adults – a population largely excluded from Medicaid before the ACA.
The ACA expanded Medicaid eligibility to nonelderly adults up to 138% of the federal poverty level (FPL) and provided income-related subsidies for the purchase of private insurance through new Marketplaces for people with income between 100% and 400% FPL. Both these new avenues of coverage, but particularly the Medicaid expansion, have the potential to lower the uninsured rate among health center patients, a largely low-income population. Following the Supreme Court ruling that effectively made the Medicaid expansion to adults optional for states, many, but not all, states implemented it. In states that did not expand Medicaid, adults with incomes between 100% and 138% FPL are eligible for Marketplace subsidies. But in these states, many adults below 100% FPL fall into a coverage gap because they are above the Medicaid income cut-off in their state but below the income eligibility threshold for Marketplace subsidies. In Medicaid expansion states, there is a continuum of coverage options for low-income adults, with Medicaid for those up to 138% FPL and Marketplace subsidies for those with higher income.
The ACA coverage expansions have important implications for health centers, which anchor health care in underserved communities, providing comprehensive primary care, case management, and enabling services such as medical transportation, and serving as an entry point for access to more specialized care. In addition, health centers have experience providing onsite outreach and enrollment assistance to uninsured patients who may be eligible for Medicaid or other coverage. During the first ACA open enrollment period, health centers provided enrollment assistance to more than 10 million people.5
To investigate and compare the historical and recent experience of health centers in Medicaid expansion and non-expansion states, the Kaiser Family Foundation and the Geiger Gibson RCHN Community Health Foundation Research Collaborative at George Washington University’s Milken Institute School of Public Health used federal data to assess changes in health center patient volume and insurance coverage in the two groups of states. Findings from a nationwide survey of health centers, fielded in Fall 2014, provide insight into additional differences between health center experiences in Medicaid expansion and non-expansion states, related to their enrollment assistance efforts and service capacity. This survey followed on a Fall 2013 survey to assess health centers’ outreach and enrollment activities on the eve of the first year of ACA coverage expansions.6
Data and Methods
We analyzed data from the federal Uniform Data System (UDS), into which all health centers report annually, to assess growth in the volume of health center patients between 2013 and 2014 and over the 2004-2014 decade; 2014 UDS data became available for analysis in late August 2015. We also used UDS data to examine 2013-2014 changes in the health coverage profile of health center patients overall and separately in Medicaid expansion and non-expansion states.7
We used data from the 2014 Follow-up Survey of Health Centers’ Outreach and Enrollment Activities to analyze health centers’ enrollment assistance activities during the first ACA open enrollment period (October 1, 2013 through March 31, 2014); major barriers to their current enrollment efforts; and increases in selected measures of service capacity since January 1, 2014. We emailed the survey between late September and November 2014 to all health centers listed in the 2013 UDS (2014 UDS data were not yet available). A total of 6798 health centers in all 50 states and DC responded, yielding an overall response rate of 57%; the response rate was 50% or higher in 44 states and DC, and the lowest rate in any state was 40%. The survey responses were almost evenly distributed between the Medicaid expansion states (including DC) (n=364) and the non-expansion states (n=315). To adjust for observed differences between respondents and non-respondents, we weighted the survey data by total health center patients, the proportion reported as racial/ethnic minorities, and total revenue per patient, using the 2014 UDS data.
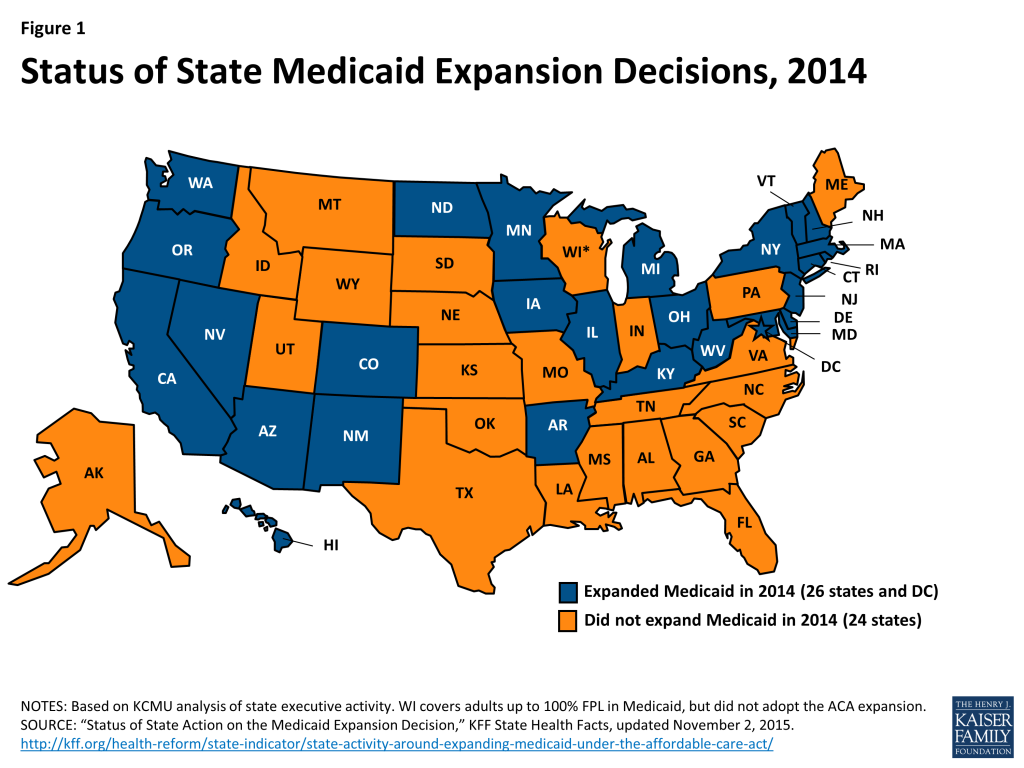
To investigate differences between the experiences of health centers in Medicaid expansion and non-expansion states, we sorted the UDS and survey data based on the Medicaid expansion status of the state in which the health center grantee was located. In most of our analyses, we counted states as Medicaid expansion states if they implemented the expansion at any time during 2014 (Figure 1). However, in our analysis of health center enrollment activities during the first ACA open enrollment period, we counted states as expansion states only if their Medicaid expansion was in effect on January 1, 2014. Therefore, two states that expanded Medicaid later in 2014 (Michigan and New Hampshire) were considered non-expansion states for this purpose.9
Findings
The number of people served by health centers and the number covered by Medicaid both grew substantially from 2013 to 2014.
- In 2014, health centers served 22.5 million patients, an increase of 1.2 million patients over 2013. Over the course of the decade 2004-2014, the number of health centers rose by more than one-third, from 887 to 1,249, and the volume of patients served by health centers nearly doubled (Figure 2).
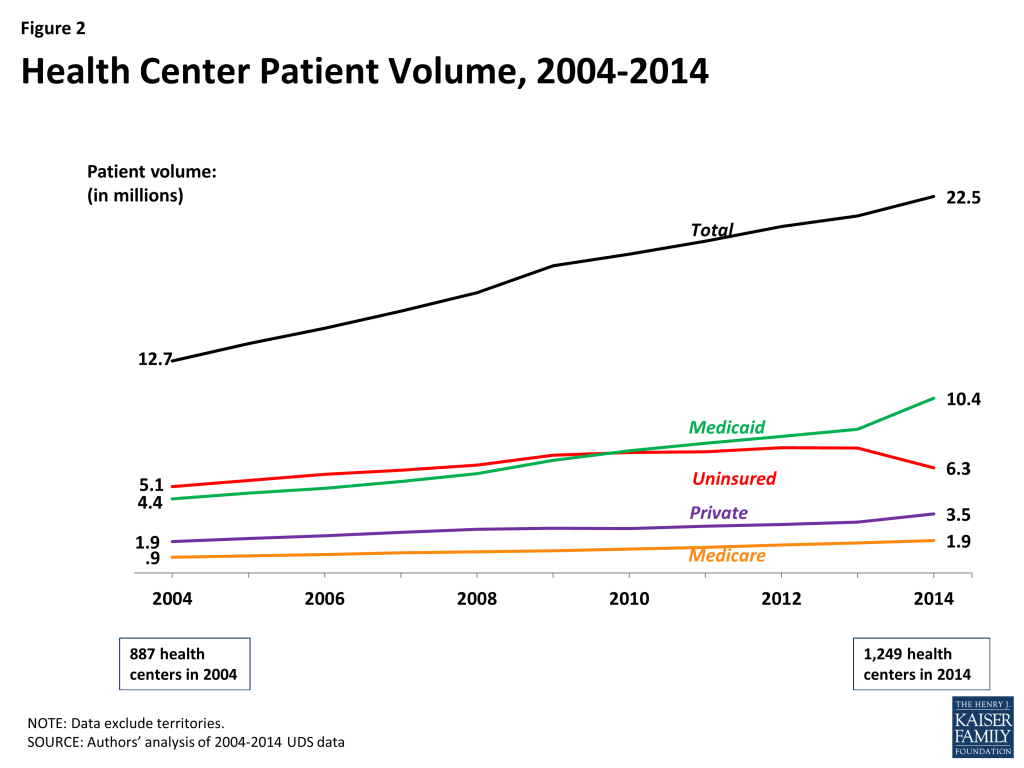
- Between 2013 and 2014, the number of health center patients with Medicaid coverage rose by 1.85 million, or 22%. Over the decade 2004-2014, the number of health center patients covered by Medicaid more than doubled, rising from 4.4 million to 10.4 million. The Medicaid increase during the decade is attributable to multiple factors, including the impact of demographic, programmatic, and economic changes (e.g., population growth, state Medicaid eligibility policies, and the 2007-2009 economic recession). It is also attributable to the ACA Medicaid expansion in states that chose to implement it.
health coverage among health center patients changed markedly between 2013 and 2014, the year the ACA Coverage expansions took effect.
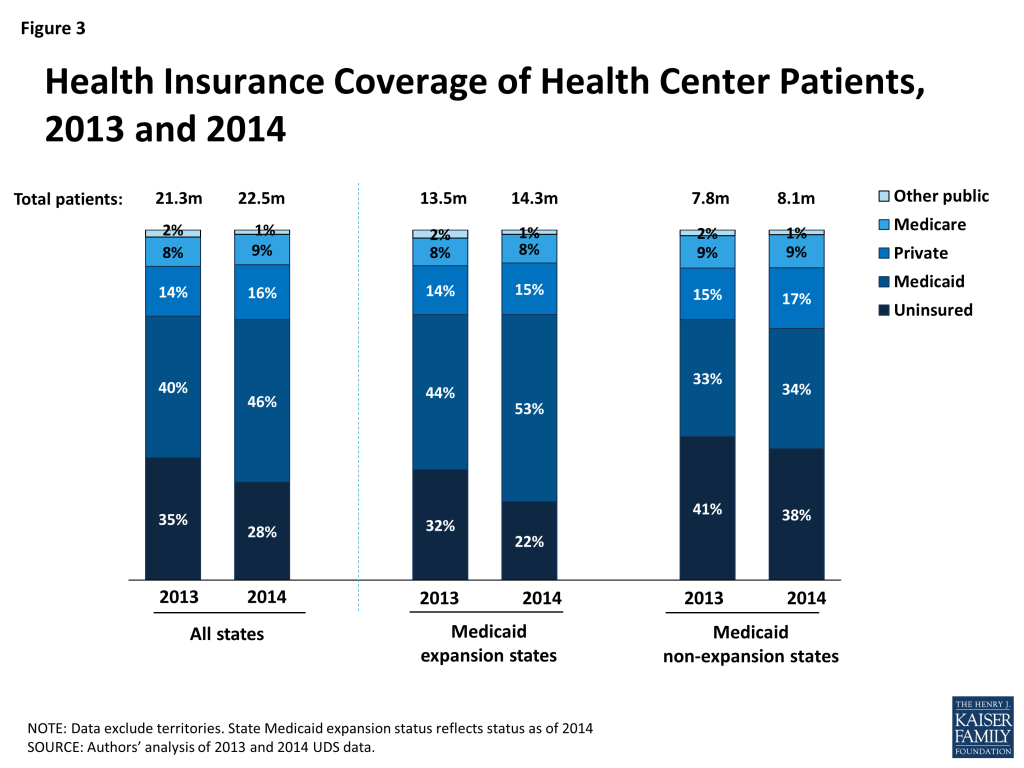
- The share of health center patients with Medicaid increased sharply. From 2013 to 2014, the first year the Medicaid expansion was in effect in the states that adopted it, the share of health center patients with Medicaid grew by 15%, from 40% to 46% (Figure 3). To put this one-year increase in perspective, the average annual increase share of health center patients with Medicaid during the 10-year period 2004-2014 was 3% (data not shown).
- The uninsured rate among health center patients declined sharply. The uninsured rate among health center patients declined by 20% between 2013 and 2014, dropping from 35% to 28%. Once more, for perspective, the average annual decline in the uninsured rate among health center patients over 2004-2014 was approximately 3.5%.
- The share of health center patients with private insurance increased, but remained small. The share of health center patients with private coverage rose from 14% to 16% between 2013 and 2014. The private coverage rate among health center patients remains low due to health center patients’ low income, lack of access to employer-sponsored insurance, and limited access to subsidies for Marketplace coverage.
health center patients’ coverage profile is different in medicaid expansion versus non-expansion states.
- Even before the ACA Medicaid expansion took effect in 2014, Medicaid coverage rates were higher and uninsured rates were lower in the expansion states than in the non-expansion states. In 2013, 44% of health center patients were covered by Medicaid in states that expanded Medicaid in 2014, compared to 33% of health center patients in the states that did not expand Medicaid. At least in part, this difference reflects higher pre-ACA Medicaid eligibility in the expansion states. In 2013, the median Medicaid income eligibility threshold for adults with dependent children was 106% FPL in states that expanded Medicaid in 2014, but just 48% FPL in states that did not expand Medicaid.10
- Between 2013 and 2014, the Medicaid coverage rate among health center patients increased much more in Medicaid expansion states than non-expansion states, and to a higher level. In the 2013-2014 timeframe, the share of health center patients covered by Medicaid rose by 20%, from 44% to 53%, in the expansion states. In the non-expansion states, the share with Medicaid rose by 3%, from 33% to 34% (Figure 4).
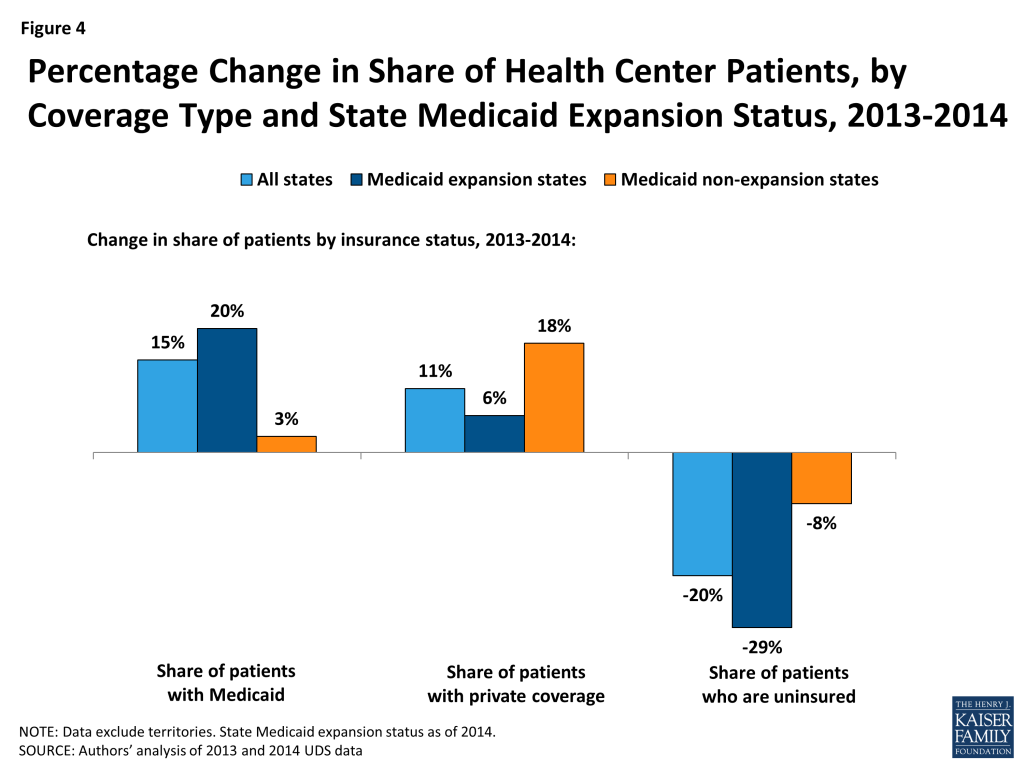
- The share of health center patients with private insurance grew more in Medicaid non-expansion than expansion states, but remained low even in non-expansion states. Between 2013 and 2014, private coverage among health center patients increased from 15% to 17% in the non-expansion states and from 14% to 15% in the Medicaid expansion states. While small, the increase indicates that some patients who obtain private insurance continue to rely on health centers for care. Still, the relatively small share of health center patients with private coverage even in non-expansion states indicates that Marketplace subsidies have limited potential as a coverage pathway for the health center patient population – a large majority of health center patients (71%) have incomes below 100% FPL, making them ineligible for Marketplace subsidies.11
- The uninsured rate among health center patients declined much more in the Medicaid expansion states, and the gap between expansion and non-expansion states widened. Between 2013 and 2014, the uninsured rate for health center patients in expansion states fell by 29%, from 32% to 22%; it fell by 8%, from 41% to 38%, in non-expansion states. In short, for health center patients, insurance coverage in non-expansion states fell even further behind coverage in expansion states. In expansion states, there is a continuum of coverage options for low-income adults, with Medicaid eligibility for those up to 138% FPL and Marketplace subsidies for those with income above that level. On the other hand, in non-expansion states, many uninsured adults below poverty remain in a coverage gap, largely excluded from Medicaid in their states but also ineligible for Marketplace subsidies.12
Health Centers in Medicaid Expansion and Non-expansion States Invest Differently in Enrollment Assistance.
- During the first ACA open enrollment period, health centers in Medicaid expansion states were more likely than those in non-expansion states to provide Medicaid enrollment assistance. All health centers received federal grants to provide outreach and enrollment assistance during the first ACA open enrollment period (October 1, 2013 – March 31, 2014). In the health center survey, more than 80% of health centers in both Medicaid expansion and non-expansion states reported providing assistance with Medicaid applications during this first open enrollment period. However, health centers in expansion states were significantly more likely than those in non-expansion states to assist patients with Medicaid renewal (78% vs. 66%) and Medicaid plan selection (69% vs. 49%) (Table 1).
- Health centers in non-expansion states were more likely than those in expansion states to provide Marketplace enrollment assistance. By a small but statistically significant increment, a larger share of health centers in non-expansion states provided assistance with applications for Marketplace subsidies in the first ACA open enrollment period, compared to health centers in Medicaid expansion states (94% vs. 89%). Health centers in non-expansion states were also significantly more likely to provide assistance with a Qualified Health Plan selection compared to health centers in expansion states (87% vs. 79%). Precluded from securing Medicaid for most of their poorest uninsured patients, health centers in non-expansion states may have been more inclined to invest in assistance to help those with income of at least 100% FPL obtain coverage through the Marketplace.
| Table 1: Enrollment Assistance Provided by Health Centers During the First ACA Open Enrollment Period | ||
| Medicaid expansion states | Medicaid non-expansion states | |
| Medicaid assistance | ||
| Assistance with Medicaid/CHIP applications | 86.9% | 81.7% |
| Assistance with Medicaid renewals | 78.4% | 66.5%* |
| Assistance with Medicaid plan selection | 69.2% | 48.8%* |
| Marketplace assistance | ||
| Assistance with Marketplace applications | 88.5% | 94.2%* |
| Assistance with Qualified Health Plan selection | 78.7% | 87.1%* |
| NOTE: For this analysis, Michigan and New Hampshire were counted as non-expansion states because their Medicaid expansion was not effective January 1, 2014. *Difference from Medicaid expansion states is significant at p<.05. | ||
Health centers in Medicaid Expansion and Non-expansion States Report Some Common and Some Different major Barriers to Current Enrollment Activities.
- Among health centers in non-expansion states, the state decision not to expand Medicaid was, by far, the most frequently reported major barrier to enrollment assistance. Nearly all (94%) health centers in non-expansion states ranked their state’s decision not to expand Medicaid as a major barrier to their enrollment assistance activities (Table 2).
- About half of health centers in both groups of states reported patient confusion about eligibility for coverage as a major barrier. The large share of all health centers citing this issue indicates that patients’ understanding of their coverage options was unrelated to state Medicaid expansion status and, rather, that confusion was widespread everywhere in the early post-ACA implementation period studied.
- Large shares of health centers in both Medicaid expansion and non-expansion states ranked problems related to documentation requirements and inadequate state information as major barriers to enrollment assistance. About 40% of health centers in Medicaid expansion states ranked incomplete or missing income, residency, or citizenship information as a major barrier, as did a significantly smaller but still large share (30%) of health centers in non-expansion states. Likewise, inaccurate or inconsistent answers from the state were considered a major barrier by 40% of health centers in expansion states and 30% of those in non-expansion states. One-quarter of health centers in expansion states and more than one-third in non-expansion states ranked inadequate consumer information provided by the state as a major barrier.
- Inadequate outreach by the state was also cited as a major barrier to enrollment assistance. One in three health centers in non-expansion states, and one in five in expansion states, ranked inadequate state outreach as a major barrier to their current enrollment activities. Roughly one in five health centers in both groups of states considered the lack of a state procedure manual and inadequate funding major barriers; more than one in 10 health centers in both groups cited the lack of culturally and/or linguistically appropriate materials.
| Table 2: Barriers to Current Health Center Enrollment Activities | ||
| Share of health centers reporting issue as a major barrier | Medicaid expansion states | Medicaid non-expansion states |
| State decision not to expand Medicaid | N/A | 93.9% |
| Patient confusion regarding eligibility for insurance programs | 50.8% | 48.7% |
| Incomplete or missing income, residency, or citizenship documentation from patients | 39.9% | 30.0%* |
| Inadequate funding | 20.4% | 17.7% |
| Inadequate outreach by the state | 19.4% | 34.8%* |
| Inaccurate or inconsistent answers from the state | 39.6% | 29.3%* |
| Lack of state procedure manual | 22.4% | 23.3% |
| Inadequate consumer information provided by the state | 25.7% | 36.1%* |
| Lack of culturally and/or linguistically appropriate documents and materials | 18.1% | 13.2% |
| State navigator requirements | 12.6% | 11.0% |
| Inadequate staff training for enrollment system | 9.2% | 4.9%* |
| Inadequate staff understanding of enrollment system | 5.4% | 4.9% |
| *Difference from Medicaid expansion states is significant at p<.05. | ||
Health Center Service Capacity is More Likely to have Expanded in Medicaid Expansion states.
- Health centers in Medicaid expansion states were significantly more likely than those in non-expansion states to report expanded service capacity since January 2014. Health centers in expansion states were more likely than those in non-expansion states to have increased dental service capacity (37% vs. 31%) and mental health service capacity since January 2014 (42% vs. 35%) (Figure 5). These results are consistent with a finding from previous work that higher Medicaid income eligibility for adults and greater health center capacity were correlated.13 It is reasonable to surmise that increased patient revenues generated by increased coverage among low-income populations help health centers to expand their service capacity.

- At the same time, wait times for health center appointments increased more in expansion states than in non-expansion states. Health centers in expansion states were more likely to report increased wait times to obtain an appointment compared to health centers in non-expansion states (35% vs. 20%). Increased wait times for appointments may reflect greater demand for health center services in Medicaid expansion states and increased strains on health center capacity at least in the short term.
Discussion
The findings from this study demonstrate that expanded health coverage under the ACA has lowered the uninsured rate among health center patients in all states. The largest gains in coverage among health center patients have occurred in Medicaid expansion states, a reflection of the deep poverty of the communities that health centers serve. In non-expansion states, the subgroup of health center patients with incomes equal to at least 100% FPL can qualify for Marketplace subsidies. The uptick in private coverage rates among health center patients in non-expansion states suggests that this coverage pathway – premium subsidies for Marketplace coverage – make a difference to health center patients as well as other low income people in non-expansion states.14 However, as important as the Marketplace subsidies are, most health center patients are too poor to qualify for them; furthermore, those who do qualify can face premiums and significant out-of-pocket burdens for deductibles, coinsurance, and copayments, depending on the plan they select. As coverage continues to expand under the ACA, health center grants will remain essential to keep care affordable for privately insured patients through income-related fee reductions, and to support the fundamental safety-role health centers play in serving the uninsured, who account for more than one in five health center patients even in states that have expanded Medicaid and almost 40% of health center patients in non-expansion states.
The finding that health centers in Medicaid expansion states were more likely to have expanded service capacity suggests that new patient revenues associated with the Medicaid expansion improved health centers’ financial position to invest. The health centers in non-expansion states lagged behind, but the grant funding provided to all health centers through the special ACA trust fund has provided crucial resources to help them build capacity to provide care, too.
Regardless of their state’s Medicaid expansion status, health centers play a crucial role in providing outreach and enrollment assistance to their patients and communities. Substantial gains in health coverage among health center patients provide new evidence of the impact of their efforts. Health centers are well-equipped to assist patients who are very poor, new to navigating a complex system of coverage, enrollment, and plan selection, and often without access to technology necessary to enroll online. Even so, despite streamlined enrollment systems under the ACA, patient confusion about eligibility and documentation requirements pose major challenges to health centers’ current enrollment activities. Health center grant funding will remain important to sustaining health centers’ ability to link their patients and communities to coverage.
Looking Ahead
As ACA implementation proceeds, a key ongoing role for health centers will be to identify and enroll uninsured health center patients who are eligible for coverage. Some patients remain ineligible for Medicaid or ACA coverage because of their immigration status. But health centers’ ability to connect patients with coverage is most powerfully influenced by state Medicaid expansion decisions, and at this writing, 20 states have not moved forward, leaving millions uninsured and straining health centers’ capacity to serve them. These non-expansion states are mostly in the South,15 where poverty is deepest, communities of color are more concentrated,16 and gaps in access to preventive care and treatment, leading to avoidable complications of disease and poor health outcomes17 are particularly great. It will be important to continue to assess the implications of Medicaid expansion for health center primary care capacity, including access to pediatric care, women’s health services, general adult medicine, and services for special needs populations, such as patients with physical and mental health disabilities. Understanding the broader impacts of Medicaid expansion on low-income communities, for example, on employment opportunities and local economies, would also help to inform state policy choices.
The high uninsured rate even among health center patients in Medicaid expansion states underscores the continuing importance of federal grant funding for health centers, as well as coverage expansion, to sustain and improve access to care in underserved communities. In addition, considering the significant role of health centers in serving Medicaid beneficiaries and other low-income populations, the extent to which they are integrated into emerging delivery systems that involve new provider alignments and performance-driven payment systems will have important implications for health care access and quality, the future of the health care safety-net, and efforts to improve population health.
Funding support for this paper was provided to The George Washington University by the RCHN Community Health Foundation.
Endnotes
- Health Resources and Services Administration. Negotiated Rulemaking Committee on the Designation of Medically Underserved Populations and Health Professional Shortage Areas: Final Report to the Secretary, Table 5. 2011. http://www.hrsa.gov/advisorycommittees/shortage/nrmcfinalreport.pdf ↩︎
- The total number of health centers in 2014 was 1,278 when health centers in the U.S. territories are included. Bureau of Primary Health Care, Health Resources and Services Administration. National 2014 Health Center Data, 2015. http://bphc.hrsa.gov/uds/datacenter.aspx?q=tall&year=2014&state= ↩︎
- Bureau of Primary Health Care, Health Resources and Services Administration. National 2014 Look-Alikes Data, 2015 http://bphc.hrsa.gov/uds/lookalikes.aspx?state=national ↩︎
- Shin P et al., A Profile of Community Health Center Patients: Implications for Policy, 2013, Kaiser Commission on Medicaid and the Uninsured, Kaiser Family Foundation and the RCHN Community Health Foundation. https://modern.kff.org/medicaid/issue-brief/a-profile-of-community-health-center-patients-implications-for-policy/ ↩︎
- Sharac J et al., How has the Affordable Care Act Benefitted Medically Underserved Communities? National Findings from the 2014 Community Health Centers Uniform Data System, 2015, Policy Research Brief No. 42, Geiger Gibson/RCHN Community Health Foundation Research Collaborative, George Washington University. http://www.rchnfoundation.org/?p=4998 ↩︎
- Shin P et al., Assessing the Potential Impact of State Policies on Community Health Centers’ Outreach and Enrollment Activities, 2014, Policy Research Brief No. 35, Geiger Gibson/RCHN Community Health Foundation Research Collaborative, George Washington University. http://www.rchnfoundation.org/?p=3814 ↩︎
- Data on health centers in the U.S. territories were excluded from this analysis. ↩︎
- The number of responses including health centers in U.S. territories was 693. ↩︎
- Kaiser Family Foundation. State Health Facts: Status of State Action on the Medicaid Expansion Decision, November 2015. https://modern.kff.org/health-reform/state-indicator/state-activity-around-expanding-medicaid-under-the-affordable-care-act/ ↩︎
- Kaiser Family Foundation. Medicaid Eligibility for Adults as of January 1, 2014, https://modern.kff.org/medicaid/fact-sheet/medicaid-eligibility-for-adults-as-of-january-1-2014/ ↩︎
- Bureau of Primary Health Care, Health Resources and Services Administration. National 2014 Health Center Data, 2015. http://bphc.hrsa.gov/uds/datacenter.aspx?q=tall&year=2014&state= ↩︎
- Garfield R et al., The Coverage Gap: Uninsured Poor Adults in States That Do Not Expand Medicaid: An Update. Kaiser Family Foundation, 2015. http://files.kff.org/attachment/issue-brief-the-coverage-gap-uninsured-poor-adults-in-states-that-do-not-expand-medicaid-an-update ↩︎
- Shin P et al., Medicaid and Community Health Centers: The Relationship between Coverage for Adults and Primary Care Capacity in Medically Underserved Communities. Kaiser Family Foundation, 2012. https://modern.kff.org/health-reform/issue-brief/medicaid-and-community-health-centers-the-relationship/ ↩︎
- This hypothesis is consistent with recent findings that individuals with income of 100-150% FPL made up nearly half of Marketplace purchasers in non-expansion states, but under one-quarter of those in Medicaid expansion states. U.S. Department of Health and Human Services. “Health Insurance Marketplaces 2015 Open Enrollment Period: March Enrollment Report.” ASPE Issue Brief (2015): 1-72. http://aspe.hhs.gov/pdf-report/health-insurance-marketplace-2015-open-enrollment-period-march-enrollment-report ↩︎
- Garfield et al., op. cit. ↩︎
- Artiga S et al., The impact of the coverage gap in states not expanding Medicaid by race and ethnicity, Kaiser Family Foundation, 2015. https://modern.kff.org/disparities-policy/issue-brief/the-impact-of-the-coverage-gap-in-states-not-expanding-medicaid-by-race-and-ethnicity/ ↩︎
- Schoen C et al., Health Care in the Two Americas: Findings from the Scorecard on State Health System Performance for Low-Income Populations, 2013, The Commonwealth Fund, 2013. http://www.commonwealthfund.org/publications/fund-reports/2013/sep/low-income-scorecard ↩︎