2014 Employer Health Benefits Survey
Abstract
This annual survey of employers provides a detailed look at trends in employer-sponsored health coverage, including premiums, employee contributions, cost-sharing provisions, and employer opinions. The 2014 survey included almost three thousand interviews with non-federal public and private firms.
Annual premiums for employer-sponsored family health coverage reached $16,834 this year, up 3 percent from last year, with workers on average paying $4,823 towards the cost of their coverage, according to the Kaiser Family Foundation/Health Research & Educational Trust (HRET) 2014 Employer Health Benefits Survey. Survey results are released here in a variety of ways, including a full report with downloadable tables, summary of findings, and an article published in the journal Health Affairs.
News Release
- A news release announcing the publication of the 2014 Employer Health Benefits Survey is available here.
Summary of Findings
- The Summary of Findings provides an overview of the 2014 survey results and is available under the Summary of Findings tab or as a pdf file in the “Download” box to the right.
Full Report
- The complete Employer Health Benefits Survey Report includes over 200 exhibits and is available under the Report tab or as a pdf file in the “Download” box to the right. The “Report” tab contains 14 separate sections. Users can also download each section separately from the “Download” box or download the complete set of section exhibits from the bottom of the respective section page.
Health Affairs
- The peer-reviewed journal Health Affairs has published an article with key findings from the 2014 survey: Health Benefits in 2014: Stability In Premiums And Coverage For Employer-Sponsored Plans.
Web Briefing
- On Wednesday, September 10, 2014, the Kaiser Family Foundation and the Health Research & Educational Trust (HRET) held a reporters-only web briefing to release the 2014 Employer Health Benefits Survey.
Interactive Graphic
- This graphing tool allows users to look at changes in premiums and worker contributions for covered workers at different types of firms, over time: Premiums and Worker Contributions Among Workers Covered by Employer-Sponsored Coverage, 1999-2014.
Key Exhibits – Chartpack
- Over twenty overview slides from the 2014 Employer Health Benefits Survey are available as a slideshow or as pdf.
Additional Resources
- Standard errors for selected estimates are available in the Technical Supplement here.
- Employer Health Benefits Surveys from 1998-2013 are available here. Please note that historic survey reports have not been revised with methodological changes.
- Researchers may request for a public use dataset by going to Contact Us and choosing “TOPIC: Health Costs.”
Researchers at the Kaiser Family Foundation, NORC at the University of Chicago, and Health Research & Educational Trust designed and analyzed the survey.
Summary Of Findings
Employer-sponsored insurance covers about 149 million nonelderly people.1 To provide current information about employer-sponsored health benefits, the Kaiser Family Foundation (Kaiser) and the Health Research & Educational Trust (HRET) conduct an annual survey of private and nonfederal public employers with three or more workers. This is the sixteenth Kaiser/HRET survey and reflects employer-sponsored health benefits in 2014.
The key findings from the survey, conducted from January through May 2014, include a modest increase in the average premiums for family coverage (3%). Single coverage premiums are 2% higher than in 2013, but the difference is not statistically significant. Covered workers generally face similar premium contributions and cost-sharing requirements in 2014 as they did in 2013. The percentage of firms (55%) which offer health benefits to at least some of their employees and the percentage of workers covered at those firms (62%) are statistically unchanged from 2013. The percentage of covered workers enrolled in grandfathered health plans – those plans exempt from many provisions of the Affordable Care Act (ACA) – declined to 26% of covered workers from 36% in 2013. Perhaps in response to new provisions of the ACA, the average length of the waiting period decreased for those with a waiting period and the percentage with an out-of-pocket limit increased. Although employers continue to offer coverage to spouses, dependents and domestic partners, some employers are instituting incentives to influence workers’ enrollment decisions, including nine percent of employers who attach restrictions for spouses’ eligibility if they are offered coverage at another source, or nine percent of firms who provide additional compensation if employees do not enroll in health benefits.
HEALTH INSURANCE PREMIUMS AND WORKER CONTRIBUTIONS
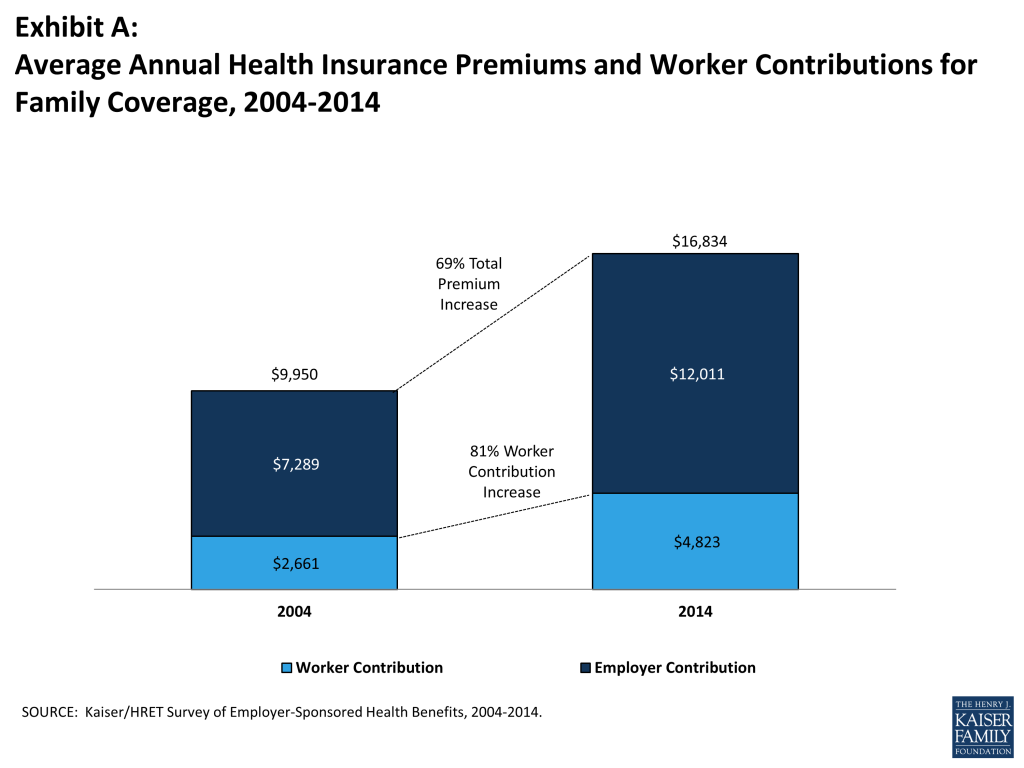
In 2014, the average annual premiums for employer-sponsored health insurance are $6,025 for single coverage and $16,834 for family coverage. The average family premium rose 3% over the 2013 average premium. Single coverage premiums rose 2% in 2014 but are not statistically different than the 2013 premium amounts. During the same period, workers’ wages increased 2.3% and inflation increased 2%.2 Over the last ten years, the average premium for family coverage has increased 69% (Exhibit A). Premiums have increased less quickly over the last five years (2009 to 2014), than the preceding five year period (2004 to 2009) (26% vs. 34%).
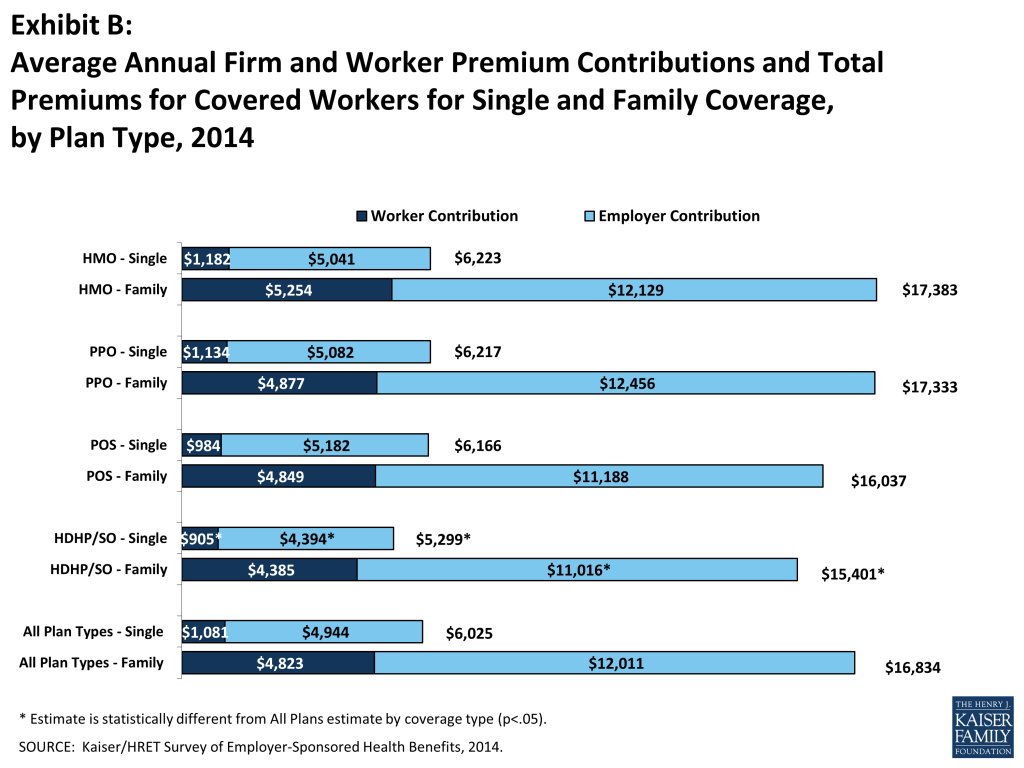
Average premiums for high-deductible health plans with a savings option (HDHP/SOs) are lower than the overall average for all plan types for both single and family coverage (Exhibit B), at $5,299 and $15,401, respectively. There are important differences in premiums by firm size: the average premium for family coverage is lower for covered workers in small firms (3-199 workers) than for workers in larger firms ($15,849 vs. $17,265).
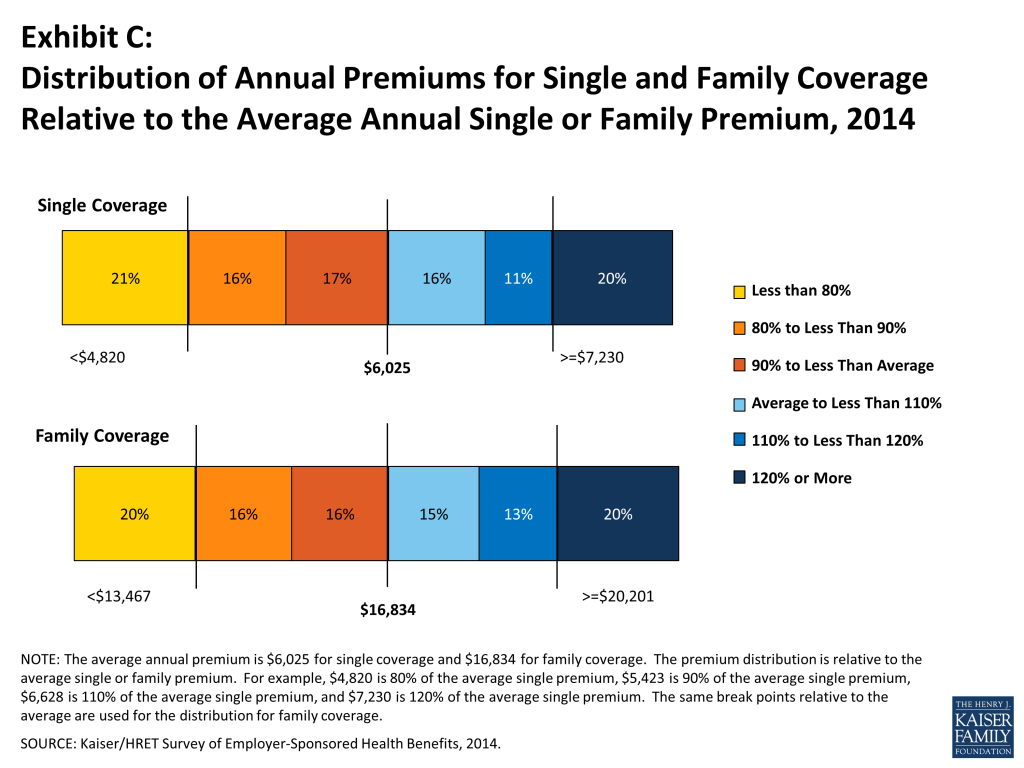
Premiums vary significantly around the averages for single and family coverage, resulting from differences in benefits, cost sharing, covered populations, and geographical location. Twenty percent of covered workers are in plans with an annual total premium for family coverage of at least $20,201 (120% of the average family premium), and 20% of covered workers are in plans where the family premium is less than $13,467 (80% of the average family premium). The distribution is similar around the average single premium (Exhibit C).
Most often, employers require that workers make a contribution towards the cost of the premium. Covered workers contribute on average 18% of the premium for single coverage and 29% of the premium for family coverage, the same percentages as 2013. Workers in small firms (3 – 199 workers) contribute a lower average percentage for single coverage compared to workers in larger firms (16% vs. 19%), but they contribute a higher average percentage for family coverage (35% vs. 27%). Workers in firms with a higher percentage of lower-wage workers (at least 35% of workers earn $23,000 or less) contribute higher percentages of the premium for single coverage (27% vs. 18%) and for family coverage (44% vs. 28%) than workers in firms with a smaller share of lower-wage workers.
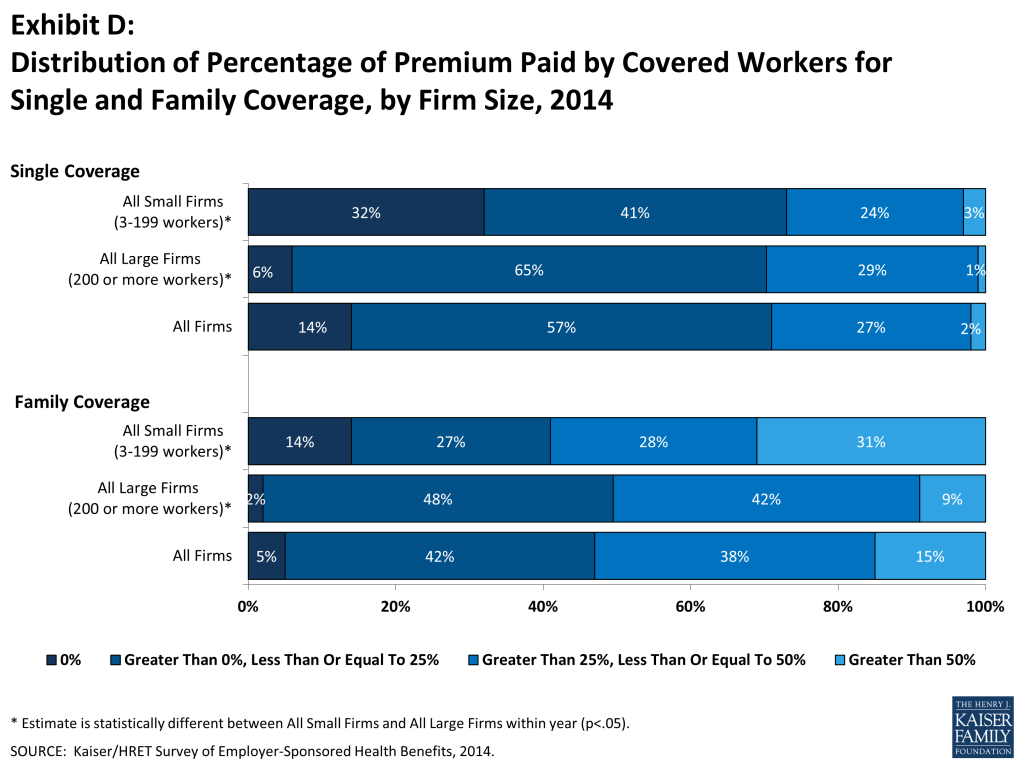
As with total premiums, the share of the premium contributed by workers varies considerably among firms. For single coverage, 57% of covered workers are in plans that require them to make a contribution of less than or equal to a quarter of the total premium, 2% are in plans that require a contribution of more than half of the premium, and 14% are in plans that require no contribution at all. For family coverage, 42% of covered workers are in plans that require them to make a contribution of less than or equal to a quarter of the total premium and 15% are in plans that require more than half of the premium, while only 5% are in plans that require no contribution at all for family coverage (Exhibit D).
Looking at the dollar amounts that workers contribute, the average annual premium contributions in 2014 are $1,081 for single coverage and $4,823 for family coverage. Covered workers’ average dollar contribution to family coverage has increased 81% since 2004 and 37% since 2009 (Exhibit A). Workers in small firms (3 – 199 workers) have lower average contributions for single coverage than workers in larger firms ($902 vs. $1,160), but higher average contributions for family coverage ($5,508 vs. $4,523). Workers in firms with a higher percentage of lower-wage workers (at least 35% of workers earn $23,000 or less) have higher average contributions for family coverage ($6,472 vs. $4,693) than workers in firms with lower percentages of lower-wage workers.
PLAN ENROLLMENT
PPO plans remain the most common plan type, enrolling 58% of covered workers in 2014. Twenty percent of covered workers are enrolled in a high-deductible plan with a savings options (HDHP/SO), 13% in an HMO, 8% in a POS plan, and less than 1% in a conventional (also known as an indemnity plan) (Exhibit E). Enrollment in HDHP/SOs increased significantly between 2009 and 2011, from 8% to 17% of covered workers, but has plateaued since then (Exhibit E). In 2014, twenty-seven percent of firms offering health benefits offer a high-deductible health plan with a health reimbursement arrangement (HDHP/HRA) or a health savings account (HSA) qualified HDHP.
Enrollment distribution varies by firm size; for example, PPOs are relatively more popular for covered workers at large firms (200 or more workers) than smaller firms (63% vs. 46%) and POS plans are relatively more popular among smaller firms than large firms (17% vs. 4%).

EMPLOYEE COST SHARING
Most covered workers face additional out-of-pocket costs when they use health care services. Eighty percent of covered workers have a general annual deductible for single coverage that must be met before most services are reimbursed by the plan. Even workers without a general annual deductible often face other types of cost sharing when they use services, such as copayments or coinsurance for office visits and hospitalizations.
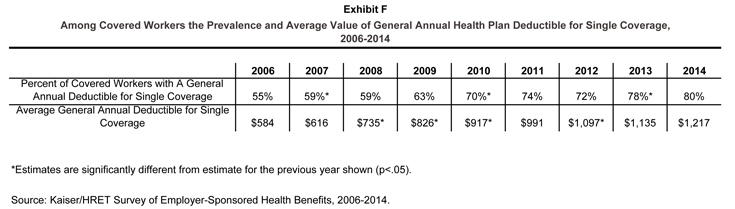
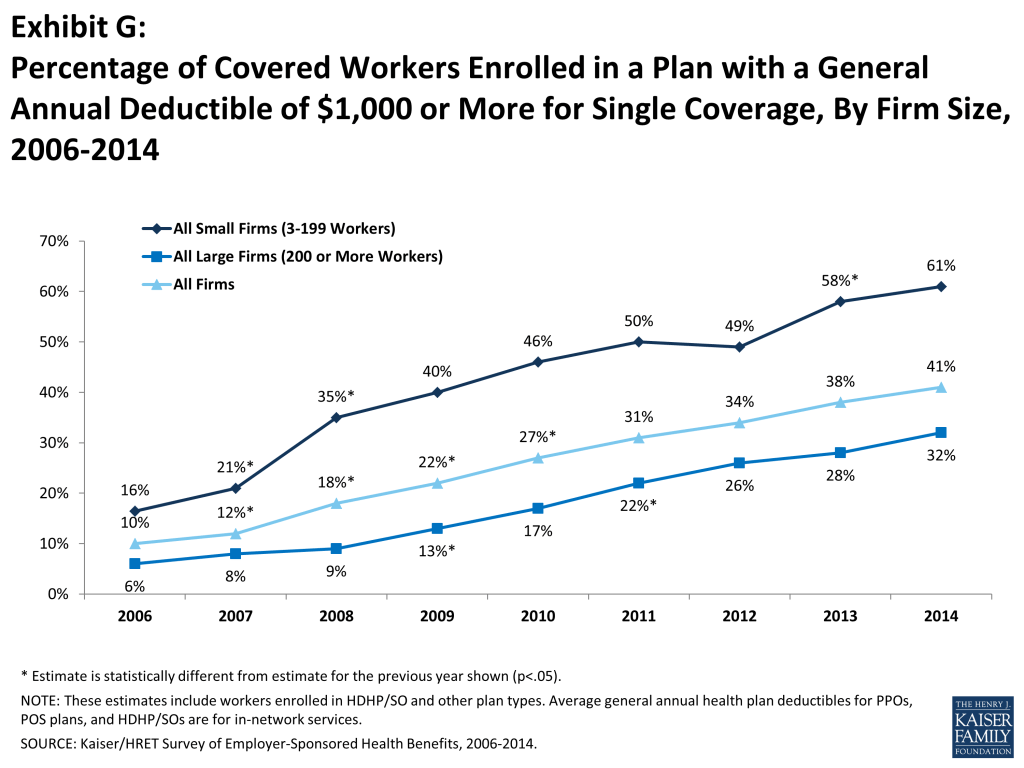
Among covered workers with a general annual deductible, the average deductible amount for single coverage is $1,217. The average annual deductible is unchanged from last year ($1,135), but has increased from $826 dollars in 2009. Deductibles differ by firm size: for workers in plans with a deductible, the average deductible for single coverage is $1,797 in small firms (3-199 workers), compared to $971 for workers in larger firms (Exhibit F). Covered workers in small firms are significantly more likely to have high general annual deductibles compared to those in larger firms. Sixty-one percent of covered workers in small firms are in a plan with a deductible of at least $1,000 for single coverage compared to 32% in larger firms; a similar pattern is seen for those in plans with a deductible of at least $2,000 (34% for small firms vs. 11% for larger firms) (Exhibit G).
The large majority of workers also have to pay a portion of the cost of physician office visits. Almost three-in-four covered workers pay a copayment (a fixed dollar amount) for office visits with a primary care physician (73%) or a specialist physician (72%), in addition to any general annual deductible their plan may have. Smaller shares of workers pay coinsurance (a percentage of the covered amount) for primary care office visits (18%) or specialty care visits (21%). For in-network office visits, covered workers with a copayment pay an average of $24 for primary care and $36 for specialty care. For covered workers with coinsurance, the average coinsurance for office visits is 18% for primary and 19% for specialty care. While the survey collects information only on in-network cost sharing, it is generally understood that out-of-network cost sharing is higher.
The cost sharing that a person pays when they fill a prescription usually varies with the type of drug – for example whether it is a generic, brand-name, or specialty drug – and whether the drug is considered preferred or not on the plan’s formulary. These factors result in each drug being assigned to a tier that represents a different level, or type, of cost sharing. Eighty percent of covered workers are in plans with three-or-more tiers of cost sharing. Copayments are the most common form of cost sharing for tiers one through three and coinsurance is the most common form of cost sharing for drugs on the fourth or higher tier of formularies. Among workers with three-or-more tier plans, the average copayments in these plans are $11 for first-tier drugs, $31 for second-tier drugs, $53 for third-tier drugs, and $83 for fourth-tier drugs. Apart from first-tier drugs, the average copayment amounts are similar to those reported last year. HDHP/SOs have a somewhat different cost-sharing pattern for prescription drugs than other plan types: just 62% of covered workers are enrolled in a plan with three-or-more tiers of cost sharing, while 15% are in plans that pay the full cost of prescriptions once the plan deductible is met, and 17% are in a plan with the same cost sharing for all prescription drugs.
Most workers also face additional cost sharing for a hospital admission or an outpatient surgery episode. After any general annual deductible is met, 62% of covered workers have a coinsurance and 15% have a copayment for hospital admissions. Lower percentages have per day (per diem) payments (5%), a separate hospital deductible (3%), or both copayments and coinsurance (10%). The average coinsurance rate for hospital admissions is 19%, the average copayment is $280 per hospital admission, the average per diem charge is $297, and the average separate annual hospital deductible is $490. The cost-sharing provisions for outpatient surgery are similar to those for hospital admissions, as most covered workers have either coinsurance (64%) or copayments (16%). For covered workers with cost sharing for each outpatient surgery episode, the average coinsurance is 19% and the average copayment is $157.
Most plans limit the amount of cost sharing workers must pay each year, generally referred to as an out-of-pocket maximum. The ACA, requires that non-grandfathered health plans, with a plan year starting in 2014 have an out-of-pocket maximum of $6,350 or less for single coverage and $12,700 for family coverage or less. In 2014, 94% percent of covered workers have an out-of-pocket maximum for single coverage, significantly more than 88% in 2013. While most workers have out-of-pocket limits, the actual dollar limits differ considerably. For example, among covered workers in plans that have an out-of-pocket maximum for single coverage, 54% are in plans with an annual out-of-pocket maximum of $3,000 or more, and 10% are in plans with an out-of-pocket maximum of less than $1,500.
AVAILABILITY OF EMPLOYER-SPONSORED COVERAGE
Fifty-five percent of firms offer health benefits to their workers, statistically unchanged from 57% last year and 61% in 2012 (Exhibit H). The likelihood of offering health benefits differs significantly by size of firm, with only 44% of employers with 3 to 9 workers offering coverage, but virtually all employers with 1,000 or more workers offering coverage to at least some of their employees. Ninety percent of workers are in a firm that offers health benefits to at least some of its employees, similar to 2013 (90%). Offer rates also differ by other firm characteristics; 53% of firms with relatively fewer younger workers (less than 35% of the workers are age 26 or younger) offer health benefits compared to 30% of firms with a higher share of younger workers.
Even in firms that offer health benefits, not all workers are covered. Some workers are not eligible to enroll as a result of waiting periods or minimum work-hour rules. Other workers do not enroll in coverage offered to them because of the cost of coverage or because they are covered through a spouse. Among firms that offer coverage, an average of 77% of workers are eligible for the health benefits offered by their employer. Of those eligible, 80% take up their employer’s coverage, resulting in 62% of workers in offering firms having coverage through their employer. Among both firms that offer and do not offer health benefits, 55% of workers are covered by health plans offered by their employer, similar to 2013 (56%).
RETIREE COVERAGE
Twenty-five percent of large firms (200 or more workers) that offer health benefits in 2014 also offer retiree health benefits, similar to the percentage (28%) in 2013 but down from 35% in 2004. Among large firms (200 or more workers) that offer retiree health benefits, 92% offer health benefits to early retirees (workers retiring before age 65), 72% offer health benefits to Medicare-age retirees, and 3% offer a plan that covers only prescription drugs. There may continue to be evolution in the way that employers structure and deliver retiree benefits. Among large firms offering health benefits, 25% of firms are considering changing the way they offer retiree coverage because of the new public health insurance exchanges established by the ACA. In addition to the public exchanges, there is considerable interest in exchange options offered by private firms. Four percent of large employers currently offer their retiree benefits through a private exchange.
WELLNESS, HEALTH RISK ASSESSMENTS AND BIOMETRIC SCREENINGS
Employers continue to offer programs in large numbers that help employees identify issues with their health and engage in healthier behavior. These include offering their employees the opportunity to complete a health risk assessment, and offering a variety of wellness programs that promote healthier lifestyles, including better diet and more exercise. Some employers collect biometric information from employees (e.g., cholesterol levels and body mass index) to use as part of their wellness and health promotion programs.
Almost one-third of employers (33%) offering health benefits provide employees with an opportunity to complete a health risk assessment. A health risk assessment includes questions about medical history, health status, and lifestyle, and is designed to identify the health risks of the person being assessed. Large firms (200 or more workers) are more likely than smaller firms to ask employees to complete a health risk assessment (51% vs. 32%). Among these firms, 51% of large firms (200 or more workers) report that they provide a financial incentive to employees that complete the assessment. Thirty-six percent of firms with a financial incentive for completing a health risk assessment reported that the maximum value of the incentive is $500 or more.
Fifty-one percent of large firms (200 or more workers) and 26% of smaller firms offering health benefits report offering biometric screening to employees. A biometric screening is a health examination that measures an employee’s risk factors, such as body weight, cholesterol, blood pressure, stress, and nutrition. Of these firms, one percent of large firms require employees to complete a biometric screening to enroll in the health plan; and 8% of large firms report that employees may be financially rewarded or penalized based on meeting biometric outcomes.
Virtually all large employers (200 or more workers) and most smaller employers offer at least one wellness program. Seventy-four percent of employers offering health benefits offer at least one of the following wellness programs in 2014: 1) weight loss programs, 2) gym membership discounts or on-site exercise facilities, 3) biometric screening, 4) smoking cessation programs, 5) personal health coaching, 6) classes in nutrition or healthy living, 7) web-based resources for healthy living, 8) flu shots or vaccinations, 9) Employee Assistance Programs (EAP), or a 10) wellness newsletter. Large firms (200 or more workers) are more likely to offer one of these programs than smaller firms (98% vs. 73%). Of firms offering health benefits and a wellness program, 36% of large firms (200 or more workers) and 18% of smaller firms offer employees a financial incentive to participate in a wellness program, such as smaller premium contributions, smaller deductibles, higher HSA/HRA contributions or gift cards, travel, merchandise or cash. Among firms with an incentive to participate in wellness programs, only 12% of small firms and 33% of large firms believe that incentives are “very effective” at encouraging employees to participate. In lieu of or in addition to incentives for participating in wellness programs, 12% of large firms have an incentive for completing wellness programs.
PROVIDER NETWORKS
High Performance or Tiered Networks. Nineteen percent of employers offering health benefits have high performance or tiered networks in their largest health plan. These programs identify providers that are more efficient or have higher quality care, and may provide financial or other incentives for enrollees to use the selected providers. Employers may use different criteria to determine which providers are in which tiers. Fifty-nine percent of firms whose largest plan includes a high performance or tiered provider network stated that the network tiers were determined both by providers’ “quality and cost/efficiency”, followed by 33% who selected “cost-efficiency”.
Narrow Networks. Some employers are limiting their provider networks to reduce the cost. Six percent of employers with 50 or more employees reported that their plan eliminated hospitals to reduce cost and eight percent offer a plan considered a narrow network plan. Only six percent of employers with 50 or more workers offering health benefits stated that “narrow networks” are a very effective strategy to contain cost, less than other strategies such as “wellness program” (28%) and “consumer drive health plans” (22%).
Retail Health Clinics. Fifty-seven percent of employers offering health benefits cover services provided by retail health clinics. These may be health clinics located in grocery stores or pharmacies to treat minor illnesses or provide preventive services, such as vaccines or flu shots. Among firms covering services in these settings, eight percent provide a financial incentive to receive services in a retail clinic instead of a physician’s office.
EMPLOYEE AND DEPENDENT ELIGIBILITY
Waiting Period. The ACA limits waiting periods to no more than 90 days for non-grandfathered plans with plan years beginning after January 1, 2014. The average length of waiting periods for covered workers who face a waiting period decreased from 2.3 months in 2013 to 2.1 months in 2014. Twenty-three percent of large firms and 10% of small firms with a waiting period indicated that they decreased the length of their waiting period during the last year. As more firms renew their plans in 2014 and lose grandfathering status more firms will be subject to this provision.
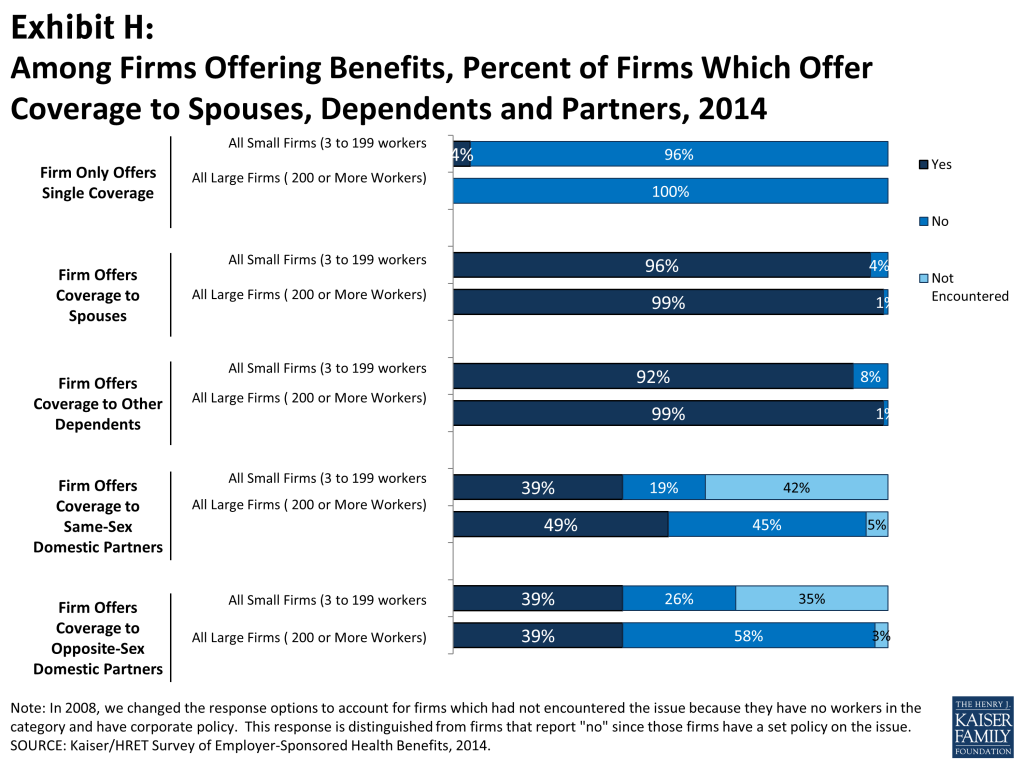
Dependent Coverage. The overwhelming majority of firms which offer coverage to at least some employees offer coverage to dependents (96%) (Exhibit H). Thirty-nine percent of firms offer coverage to same-sex domestic partners, the same percentage that offers coverage to opposite-sex domestic partners. Both percentages are similar to 2012, the last time the survey included this question. Some employers are requiring additional cost sharing (5%) or restricting eligibility for spouses (9%) to enroll if they have an offer of coverage from another source. Eighteen percent of large firms provide compensation or benefits to employees who do not enroll in coverage.
OTHER TOPICS
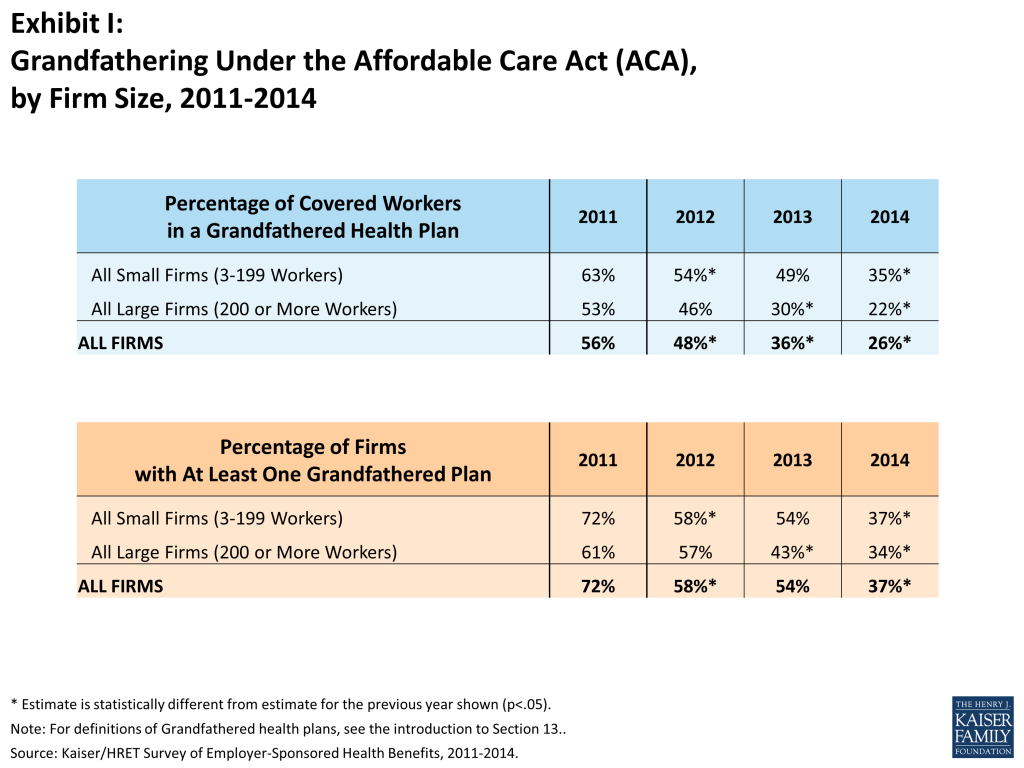
Grandfathered Health Plans. The ACA exempts “grandfathered” health plans from a number of its provisions, such as the requirements to cover preventive benefits without cost sharing or the new rules for small employers’ premiums ratings and benefits. An employer-sponsored health plan can be grandfathered if it covered a worker when the ACA became law (March 23, 2010) and if the plan has not made significant changes that reduce benefits or increase employee costs.3 Thirty-seven percent of firms offering health benefits offer at least one grandfathered health plan in 2014, less than 54% in 2013. Looking at enrollment, 26% of covered workers are enrolled in a grandfathered health plan in 2014, down from 36% in 2013 (Exhibit I).
Self-Funding. Fifteen percent of covered workers at small firms (3-199 workers) and 81% of covered workers at larger firms are enrolled in plans which are either partially or completely self-funded. The percent of covered workers enrolled in self-funded plans has increased for large firms since 2004, but has remained stable for both large and small firms over the last couple of years.
Private Exchanges for Large Employers. While relatively few covered workers at large employers currently receive benefits through a private or corporate health insurance exchange (3%), many firms are looking at this option. Private exchanges allow employees to choose from several health benefits options offered on the exchange. A private exchange is created by a consulting company or insurer, rather than a governmental entity. Thirteen percent of large firms are considering offering benefits through a private exchange and 23% are considering using a defined contribution method. This interest may signal a significant change in the way that employers approach health benefits and the way employees get coverage.
CONCLUSION
The 2014 survey found considerable stability among employer-sponsored plans. Similar percentages of employers offered benefits to at least some employees and a similar percentage of workers at those firms were covered by benefits compared to last year. Family premiums increased at a modest rate and single premiums are not statistically different than those reported last year. On average, covered workers contribute the same percentage of the premium for single and family coverage as they did last year.
The relatively quiet period in 2014 may give way to bigger changes in 2015 as the employer shared-responsibility provision in the ACA takes effect for large employers. This provision requires firms with more than 100 full time equivalent employees (FTEs) in 2015 and more than 50 FTEs in 2016 to provide coverage to their full-time workers or possibly pay a penalty if workers seek subsidized coverage in health care exchanges. While most large employers provide coverage to workers, not all do, and not all cover all of their full-time workers. In addition, the coverage offered by these larger employers must meet a certain value and must be offered at an affordable amount to workers. We expect some employers to revise eligibility and contributions for benefits in response to the new provisions.
The continued implementation of major reforms in the non-group market also may affect employer strategies going forward. For smaller firms not subject to the employer-responsibility requirement, the ability of their employees to receive subsidized nongroup coverage in health insurance exchanges may be an attractive alternative which would relieve the employer of the burden of sponsoring coverage. Small firms that have struggled to offer good coverage options may decide to stop offering now that other alternatives are available. In addition, a quarter of large firms offering retiree coverage to active workers indicated they were considering changes to the way they offered retiree coverage because of the implementation of the public exchanges. We may see shifts in the coverage options offered by some employers in response to these new options and new tax incentives.
Employer-sponsored coverage also will continue to evolve for reasons that are not related to the ACA. Employers and insurers continue to develop more integrated approaches to assessing individuals’ personal health risks and offering programs to address them. Wellness programs present enrollees with opportunities and challenges, including the possibility of much higher out-of-pocket costs if their health profile is a potentially costly one. Narrow networks and provider networks and new tools like reference pricing can lower premiums but also require enrollees to have a more active role in ensuring that they have access to the providers they want to use. And the development of private marketplaces for larger employers, if it continues, may signal a new direction where individual employers are less engaged in plan design and management and where more decisions and economic responsibility is shifted to employees.
Finally, the continuing improvement in the economy is likely to put new cost pressure on employers and insurers. Costs grew at low levels while the economy struggled, but are likely to rebound if the growth in the economy is sustained. The potential of higher premiums may push employers and insurers to accelerate some of the changes we already are seeing.
METHODOLOGY
The Kaiser Family Foundation/Health Research & Educational Trust 2014 Annual Employer Health Benefits Survey (Kaiser/HRET) reports findings from a telephone survey of 2,052 randomly selected public and private employers with three or more workers. Researchers at the Health Research & Educational Trust, NORC at the University of Chicago, and the Kaiser Family Foundation designed and analyzed the survey. National Research, LLC conducted the fieldwork between January and May 2014. In 2014 the overall response rate is 46%, which includes firms that offer and do not offer health benefits. Among firms that offer health benefits, the survey’s response rate is also 46%.
We ask all firms with which we made phone contact, even if the firm declined to participate in the survey: “Does your company offer a health insurance program as a benefit to any of your employees?” A total of 3,139 firms responded to this question (including the 2,052 who responded to the full survey and 1,087 who responded to this one question). Their responses are included in our estimates of the percentage of firms offering health coverage. The response rate for this question is 70%.
Since firms are selected randomly, it is possible to extrapolate from the sample to national, regional, industry, and firm size estimates using statistical weights. In calculating weights, we first determine the basic weight, then apply a nonresponse adjustment, and finally apply a post-stratification adjustment. We use the U.S. Census Bureau’s Statistics of U.S. Businesses as the basis for the stratification and the post-stratification adjustment for firms in the private sector, and we use the Census of Governments as the basis for post-stratification for firms in the public sector. Some numbers in the exhibits in the report do not sum up to totals due to rounding effects, and, in a few cases, numbers from distribution exhibits referenced in the text may not add due to rounding effects. Unless otherwise noted, differences referred to in the text and exhibits use the 0.05 confidence level as the threshold for significance. In 2014 we adjusted the premiums for a small number of firms which gave a composite family/single amount.
For more information on the survey methodology, please visit the Survey Design and Methods Section at http://ehbs.kff.org/.
The Kaiser Family Foundation, a leader in health policy analysis, health journalism and communication, is dedicated to filling the need for trusted, independent information on the major health issues facing our nation and its people. The Foundation is a non-profit private operating foundation, based in Menlo Park, California.
The Health Research & Educational Trust is a private, not-for-profit organization involved in research, education, and demonstration programs addressing health management and policy issues. Founded in 1944, HRET, an affiliate of the American Hospital Association, collaborates with health care, government, academic, business, and community organizations across the United States to conduct research and disseminate findings that help shape the future of health care.
Section One: Cost Of Health Insurance
The average annual premiums in 2014 are $6,025 for single coverage and $16,834 for family coverage. The average family premium increased 3% in the last year; the average single premium, however, is similar to the value reported in 2013 ($5,884). Family premiums have increased 69% since 2004 and have more than doubled since 2002. However, the average family premium has grown less quickly over the last five years than it did between 2004 and 2009 or between 1999 and 2004. Average family premiums for workers in small firms (3-199 workers) ($15,849) are significantly lower than average family premiums for workers in larger firms (200 or more workers) ($17,265).
Premium Costs for Single and Family Coverage
- The average premium for single coverage in 2014 is $502 per month, or $6,025 per year 1. The average premium for family coverage is $1,403 per month or $16,834 per year 1.
- The average annual premiums for covered workers in HDHP/SOs are lower for single ($5,299) and family coverage ($15,401) than the overall average premiums for covered workers. Average annual premiums for all other plan types, including PPOs, HMOs, and POS plans, are similar to the overall average premiums for covered workers 1.
- The average annual premium for family coverage for covered workers in small firms (3-199 workers) ($15,849) is lower than the average premium for covered workers in large firms (200 or more workers) ($17,265) 2. The average annual single premium for covered workers in small firms (3-199 workers) also is significantly lower than for workers in larger firms ($5,788 vs. $6,130).
- Average single and family premiums for covered workers are higher in the Northeast ($6,369 and $17,772) and lower in the South ($5,720 and $16,170) than the average premiums for covered workers in all other regions 3.
- Average single and family premiums for covered workers in the Wholesale ($5,189 and $15,599) and Retail ($5,355 and $14,979) industries are lower than the average premiums for covered workers in all other industries 4.
- Covered workers in firms where 35% or more of the workers are age 26 or younger have lower average single and family premiums ($5,292 and $15,182) than covered workers in firms where a lower percentage of workers are age 26 or younger ($6,079 and $16,955). Covered workers in firms where 35% or more of the workers are age 50 or older have higher average single and family premiums ($6,313 and $17,425) than covered workers in firms where a lower percentage of workers are age 50 or older ($5,759 and $16,286) 5 and 6.
- Covered workers in firms with a large percentage of lower-wage workers (at least 35% of workers earn $23,000 per year or less) have lower average single and family premiums ($5,175 and $14,177) than covered workers in firms with a smaller percentage of lower-wage workers ($6,093 and $17,044). Covered worker in firms with a large percentage of higher-wage workers (at least 35% of workers earn $57,000 per year or more) have higher average single and family premiums ($6,244 and $17,582) than covered workers in firms with a smaller percentage of higher-wage workers ($5,819 and $16,124) 5 and 6.
- There is considerable variation in premiums for both single and family coverage.
- Twenty percent of covered workers are employed by firms that have a single premium at least 20% higher than the average single premium, while 21% of covered workers are in firms that have a single premium less than 80% of the average single premium 7 and 8.
- For family coverage, 20% of covered workers are employed in a firm that has a family premium at least 20% higher than the average family premium, and another 20% of covered workers are in firms that have a family premium less than 80% of the average family premium 7 and 8.
Premium Changes Over Time
- The average premiums for covered workers in2014 are $6,025 annually, or $502 per month, for single coverage and $16,834 annually, or $1,403 per month, for family coverage. The 2014 average single premium is similar to the 2013 average premium (the 2 percent increase is not significant). However, the 2014 average family premium is 3 percent higher than the 2013 average premium 11.
- The $16,834 average annual family premium in 2014 is 26% higher than the average family premium in 2009 and 69% higher than the average family premium in 2004 11. The 26% premium growth seen in the last five years (2009 to 2014) is significantly lower than the 34% premium growth seen in the previous five year period, from 2004 to 2009 16.
- Premiums for both small and large firms have seen a similar increase since 2009 (25% for small and 26% for large). For small firms (3 to 199 workers), the average family premium rose from $12,696 in 2009 to $15,849 in 2014. For large firms (200 or more workers), the average family premium rose from $13,704 in 2009 to $17,265 in 2014 13.
- Since 2004, premiums for small firms (3 to 199 workers) have increased 63% ($15,849 in 2014 vs. $9,737 in 2004). The premiums for large firms have increased 72% ($17,265 in 2014 vs. $10,046 in 2004) 13.
- Average family premiums for firms with fewer low-wage workers (less than 35% of workers earn $23,000 per year or less) grew in the last year ($17,044 vs. $16,450), while premiums for family coverage for firms with many low-wage workers were similar to 2013 ($14,177 vs. $15,225) 15. Overall, premiums for family coverage have grown faster for firms with fewer low-wage workers than firms with many low-wage workers over the last year (4% vs. -7%), as well as the last five years (27% vs. 9%). A similar pattern is observed for single coverage, where average premiums have grown faster for firms with fewer lower-wage workers than firms with many lower wage workers over the last five years (26% vs. 12%).
- For large firms (200 or more workers), the average family premium for covered workers in firms that are fully insured has grown at a similar rate to premiums for workers in fully or partially self-funded firms from 2009 to 2014 (26% in both fully insured and self-funded firms) and from 2004 to 2014 (71% in fully insured firms vs. 73% in self-funded firms) 17.
Section Two: Health Benefits Offer Rates
While nearly all large firms (200 or more workers) offer health benefits to at least some employees, small firms (3-199 workers) are significantly less likely to do so. The percentage of all firms offering health benefits in 2014 (55%) is not statistically different from 2013 and 2012 (57% and 61%, respectively). Over a third of firms offering health benefits cover (39%) same-sex domestic partners; the same percentage which covers opposite-sex domestic partners. Nine percent of firms which offer family coverage restrict eligibility to a spouse when he/she has another offer of coverage. Among large employers offering health benefits 88% offer or contribute to separate dental benefits and 63% do so for separate vision benefits. Firms not offering health benefits continue to cite “cost” as the most important reason they do not offer health benefits (32%).
- Offer rates vary across different types of firms.
- Smaller firms are less likely to offer health insurance: 44% of firms with 3 to 9 workers offer coverage, compared to 64% of firms with 10 to 24 workers, 83% of firms with 25 to 49 workers, and 91% of firms with 50 to 199 employees 3.
- Offer rates throughout different firm size categories in 2014 remained similar to those reported in 2013 2.
- Firms with fewer lower-wage workers (less than 35% of workers earn $23,000 or less annually) are significantly more likely to offer health insurance than firms with many lower-wage workers (55% vs. 33%) 4. The offer rate for firms with many lower-wage workers is not significantly different from the 23% reported in 2013.
- We observe a similar pattern among firms with many higher-wage workers (35% or more of workers earn $57,000 or more annually) being more likely to offer coverage to employees (69% versus 47%) 4.
- The age of the workforce correlates with the probability of a firm offering health benefits. Firms where 35% or more of its workers are age 26 or younger are less likely to offer health benefits than firms where less than 35% of workers are age 26 or younger (30% and 53%, respectively) 4. The percentage of firms with many younger workers that offer health benefits is similar to the 23% reported in 2013.
- In 2014, 55% of firms offer health benefits not statistically different from the 57% reported in 2013 1.4
- Ninety-eight percent of large firms (200 or more workers) offer health benefits to at least some of their workers 3. In contrast, only 54% of small firms (3-199 workers) offer health benefits in 2014. The percentage of both small and large firms offering health benefits to at least some of their workers is similar to last year 2.
- Between 1999 and 2014, the offer rate for large firms (200 or more workers) has consistently remained at or above 97%.
- Since most firms in the country are small, variation in the overall offer rate is driven primarily by changes in the percentages of the smallest firms (3-9 workers) offering health benefits. For more information on the distribution of firms in the country, see the Survey Design and Methods Section and Exhibit M1.
- As the “employer shared responsibility” provision takes effect in 2015, some employers may adjust their workforce’s employment status to mitigate the provision’s impact. Starting in 2015, employers with more than 100 full time equivalents5 who do not offer their full-time employees coverage will pay a penalty if one of their employees receives a premium subsidy on a health insurance exchange. Employers will be charged a penalty of $2,000 for each employee beyond their first 30 employees if they do not offer coverage. For example, a firm with 65 employees would be charged $70,000 annually for not offering coverage (35 employees multiplied by $2,000 per employee). Employers that offer coverage may still be assessed a penalty if the coverage is either too expensive or does not meet minimum standards. Coverage offered by an employer must pay for 60% of a population’s covered medical expenses. In addition, the worker contribution to the premium cannot exceed 9.5% of the household’s income.
- Ninety-four percent of firms with 100 or more employees offered health benefits to at least some of their employees in 2014. Ninety percent of firms with between 50 and 99 workers offered benefits to at least some workers. Since the survey does not ask employers how many full-time equivalents they have, these firm size categories are determined by the number of workers at a firm and may include both full-time and part-time employees.
Part-Time and Temporary Workers
- Among firms offering health benefits, relatively few offer benefits to their part-time and temporary workers.
- In 2014, 24% of all firms that offer health benefits offer them to part-time workers, similar to the 25% reported in 2013 5. Firms with 200 or more workers are more likely to offer health benefits to part-time employees than firms with 3 to 199 workers (46% vs. 24%) 7.
- A small percentage (5% in 2014) of firms offering health benefits have offered them to temporary workers 6. The percentage of firms offering temporary workers benefits are similar for small firms (3-199 workers) and larger firms (5% vs. 9%) 8. The percentage of firms offering health benefits to temporary workers has remained stable over time.
Dental and Vision Benefits
- Fifty-three percent of firms offering health benefits offer or contribute to a dental insurance benefit for their employees that is separate from any dental coverage the health plans might include. This is not statistically different from the 54% reported in 2012, which is the last time the survey asked about dental benefits 10. Large firms (200 or more workers) are far more likely than smaller firms to offer or contribute to a separate dental health benefit (88% vs. 52%) 9.
- Thirty-five percent of firms offer or contribute to a vision benefit for their employees that is separate from any vision coverage the health plan might include, which is not statistically different than the 27% we reported in 2012 but higher than 17% in 2010 10.
- Large firms (200 or more workers) are more likely than smaller firms to offer or contribute to a separate vision care benefit, at 63% versus 34% 9.
Spouses, Dependents and Domestic Partner Benefits
The vast majority of firms offering health benefits offer benefits to spouses and dependents, such as children.
- In 2014, 96% of small firms (3 to 199 workers) and 99% of larger firms offering health benefits offer coverage to spouses. Similarly, in 2014, 92% of small firms and 99% of large firms offering health benefits cover other dependents, such as children. Four percent of small firms offering health benefits do not offer coverage to any dependents 11.
- This year we asked employers whether same-sex and opposite-sex domestic partners were allowed to enrolled in a firm’s coverage. While definitions may vary, employers often define domestic partners as an unmarried couple who have lived together for a specified period of time. Firms may define domestic partners separate from any legal requirements a state may have. Employers may have a different policy in different parts of the country.
- In 2014, 39% of firms offering health benefits offered coverage to unmarried opposite-sex partners, similar to the 37% who did so in 2012, the last time this question was asked). In 2014, 39% of firms offering benefits covered same-sex domestic partners, unchanged from the 31% in 2012 13.
- The rates at which firms have offered domestic partner benefits have increased over a longer period of time. For example, in 2014, 39% of firms offered benefits to same-sex domestic partners, a significant increase from the 22% that did so in 2008. The percentage of offering firms which covered opposite-sex domestic partner benefits has also increased from 24% in 2008 to 39% in 2014.
- When we ask employers if they offer health benefits to opposite or same-sex domestic partners, many firms report that they have not encountered the issue of whether benefits would be offered to domestic partners. At many small firms (3-199 Workers), the firm may not have formal HR policies on domestic partners simply because none of the firm’s employees have asked to cover a domestic partner. Regarding health benefits for opposite-sex domestic partners, 34% of firms report in 2014 that they have not encountered this need or that the question was not applicable. The vast majority of firms in the United States are small business; 61% of firms have between 3 and 9 employees and 98% have between 3 and 199 employees. Therefore statistics about the percentage of firms that offer domestic partner benefits is largely controlled by small businesses. More small firms (35%) compared to large firms (3%) indicate that they have not encountered this need or that the question was not applicable 12. Regarding health benefits for same-sex domestic partners, 41% of firms report that they have not encountered the need or that the question was not applicable. More small firms (3–199 workers) (42%) than larger firms (5%) report that they have not encountered the issue of offering benefits to same-sex domestic partners 12.
- Firms in the Northeast are more likely (60%) and firms in the South are less likely (25%) to offer health benefits to unmarried same-sex domestic partners than firms in other regions 12. Firms in the Northeast are more likely (50%) to offer health benefits to unmarried opposite-sex domestic partners than firms in other regions 12.
- Firms in the state and local government industry are less likely to offer either same sex or opposite sex domestic partner benefits than firms in other industries 12.
- Firms may adjust their eligibility for some dependents based on whether the dependent has another offer of coverage.
- Among firms offering coverage to spouses, spouses are not eligible to enroll for coverage if they are offered health insurance from another source at nine percent of firms 14.
- Five percent of firms offering coverage to spouses require a greater contribution for coverage if a spouse is offered health insurance from another source. Large employers (200 or more workers) are more likely than small employer to have this requirement (9% vs. 5%) 14.
Firms Not Offering Health Benefits
- The survey asks firms that do not offer health benefits if they have offered insurance or shopped for insurance in the recent past, and about their most important reasons for not offering coverage. Because such a small percentage of large firms report not offering health benefits, we present responses for smaller firms (3 to 199 workers) that do not offer health benefits.
- The cost of health insurance remains the primary reason cited by firms for not offering health benefits. Among small firms (3-199 workers) not offering health benefits, 32% cite high cost as “the most important reason” for not doing so, followed by “employees are generally covered under another plan” (24%) 15. This year we asked employers whether the launch of the health insurance exchanges for individuals was the primary reason for not offering benefits; nine percent of employers cited “employees have other options, including exchanges” and one percent said “employees will get a better deal on the health insurance exchanges” 15. More small firms indicated they did not offer because of “cost” and “employees are generally covered under another plan” than “employees have other options, including exchanges”.
- Many non-offering, small firms have either offered health benefits in the past five years, or shopped for alternative coverage options recently.
- Eighteen percent of non-offering, small firms (3-199 workers) have offered health benefits in the past five years, while 24% have shopped for coverage in the past year 16. The 24% of non-offering small firms which have shopped for coverage in the past year is similar to the 18% who did so last year.
- Among non-offering, small firms (3-199 workers), 7% report that they provide funds to their employees to purchase health insurance through the individual, or non-group, market, such as on an individual health insurance marketplace 17. The percentage of firms offering funds to purchase non-group coverage is similar to last year (10%).
- Three-quarters of small firms (3-199 employees) not offering health benefits believed that their employees would prefer a two dollar per hour increase in wages rather than health insurance 18. The percentage of small employers who believe that their employees would prefer a wage increase is the same as 2011 the last time the survey asked this question (75%).
- Small firms (3-199 workers) not offering health insurance gave a variety of estimates regarding the amount they believe the firm could afford to pay for health insurance for an employee with single coverage. Thirty-nine percent reported that they could pay less than $100 per month; 6% reported that they could pay $400 or more per month 19.
- Small firms (3-199 workers) not offering health benefits were asked to estimate what percentage of their employees had coverage from another source. Fifty percent of small employers estimated that three quarters or more of their employees were covered 20. On average, non-offering firms with between 3-9 employees believed that 75% of their employees had another source of coverage, 58% at firms with 10 to 24 employees, and 44% at firms with 25 to 199 employees.
SHOP Exchanges
Small Business Health Options Program (SHOP) are federal or state sponsored exchanges in which employers may offer and contribute to health insurance provided to their employees. In many states SHOP exchanges were not fully implemented and many employers experience technical difficulties when trying to enroll. Small employers may qualify for the small business health care tax credit when purchase coverage through the SHOP exchanges. In 2014, firms with 50 or fewer full-time equivalents are eligible to participate in a SHOP exchange.
- Because our survey gathers information about the total number of full-time and part-time employees in a firm, we cannot calculate the number of full-time equivalent employees and therefore could not limit survey responses only to firms within the size range eligible for the SHOP marketplaces. To ensure that we included employers that may have a number of part-time or temporary employees but could still qualify, we directed questions to employers with 3 to 75 total employees. This approach allowed us to capture some employers with more than 50 employees who would nonetheless be eligible, but it also means that that some employers who are unlikely to be eligible were asked these questions.
- Thirteen percent of firms with 3 to 75 employees who do not offer health benefits said they looked at purchasing coverage on a SHOP exchange. Similarly, twelve percent of firms with 3 to 75 employees that do offer health benefits looked at coverage on the SHOP exchanges 21.
- Among non-offering firms with 3 to 75 employees that chose not to purchase coverage on a SHOP exchange, 40% reported they did not do so because they were not interested and 28% said it was too expensive 22.
Section Three: Employee Coverage, Eligibility, And Participation
Employers are the principal source of health insurance in the United States, providing health benefits for about 149 million non-elderly people in America.6 Most workers are offered health coverage at work, and the majority of workers who are offered coverage take it. Workers may not be covered by their own employer for several reasons: their employer may not offer coverage, they may be ineligible for benefits offered by their firm, they may elect to receive coverage through their spouse’s employer, or they may refuse coverage from their firm. In 2015, new coverage requirements will be implemented that may affect employers’ decisions about offering health care coverage going forward.
- Among firms offering health benefits, 62% percent of workers are covered by health benefits through their own employer 2.
- When considering both firms that offer health benefits and those that don’t, 55% of workers are covered under their employer’s plan 1. This coverage rate has slowly decreased over time, down from 59% in 2009 and 61% in 2004.
Eligibility
- Not all employees are eligible for the health benefits offered by their firm, and not all eligible employees “take up” (i.e., elect to participate in) the offer of coverage. The share of workers covered in a firm is a product of both the percentage of workers who are eligible for the firm’s health insurance and the percentage who choose to take up the benefit.
- Seventy-seven percent of workers in firms offering health benefits are eligible for the coverage offered by their employer 2.
- Eligibility varies considerably by wage level. Employees in firms with a lower proportion of lower-wage workers (less than 35% of workers earn $23,000 or less annually) are more likely to be eligible for health benefits than employees in firms with a higher proportion of lower-wage workers (79% vs. 63%). We observe a similar pattern among firms with many higher-wage workers (35% or more of workers earn $57,000 or more annually) (83% vs. 73%) 3.
- Eligibility also varies by the age of the workforce. Those in firms with fewer younger workers (less than 35% of workers are age 26 or younger) are more likely to be eligible for health benefits than those in firms with many younger workers, at 79% versus 59% 3.
Take-up Rate
- Employees who are offered health benefits generally elect to take up the coverage. In 2014, 80% of eligible workers take up coverage when it was offered to them, the same rate as last year 2.7
- The likelihood of a worker accepting a firm’s offer of coverage also varies with the workforces’ wage level. Eligible employees in firms with a lower proportion of lower-wage workers are more likely to take up coverage (81%) than eligible employees in firms with a higher proportion of lower-wage workers (35% or more of workers earn $23,000 or less annually) (67%) 4. Similar patterns are seen in firms with a larger proportion of higher-wage workers, with workers in these firms being more likely to take up coverage than those in firms with a smaller share of higher wage workers (83% vs. 77%).
- Ninety-one percent of workers at public employers who offer health benefits take up coverage. Workers at private-for-profit employers are significantly less likely to do so – only 77% of these workers take up coverage 4.
Coverage
- There is significant variation by industry in the coverage rate among workers in firms offering health benefits. For example, only 37% of workers in retail firms offering health benefits are covered by the health benefits offered by their firm, compared to 74% of workers in finance, and 80% of workers in the transportation/communications/utilities industry category 2.
- Among workers in firms offering health benefits, those in firms with relatively few part-time workers (less than 35% of workers are part-time) are much more likely to be covered by their own firm than workers in firms with a greater percentage of part-time workers (69% vs. 35%) 5.
- Among workers in firms offering health benefits, those in firms with fewer lower-wage workers (less than 35% of workers earn $23,000 or less annually) are more likely to be covered by their own firm than workers in firms with many lower-wage workers (64% vs. 42%) 5. A comparable pattern exists in firms with a larger proportion of higher wage workers (35% or more earn $57,000 or more annually) offering health benefits (69% vs. 56%).
- Among workers in firms offering health benefits, those in firms with fewer younger workers (less than 35% of workers are age 26 or younger) are more likely to be covered by their own firm than those in firms with many younger workers (64% vs. 45%) 5.
- Ninety-eight percent of firms offering health benefits reported that they did not change eligibility criteria by either increasing or decreasing the share of workers eligible for health benefits in the last year 7.
Waiting Periods
- Waiting periods are a specified length of time after beginning employment before employees are eligible to enroll in health benefits. The ACA requires that waiting periods cannot exceed 90 days for non-grandfathered plans for plan years that begin on or after January 1, 2014. This survey is conducted from January to May annually, at which time many firms report information on their current plans. In some cases those plan years may have started in the previous calendar year (in this case, 2013). Some employers may have renewed their plan year in 2013 in order to delay implementing provisions of the ACA slated to take effect on January 1 2014. Also, many covered workers are enrolled in grandfathered health which are exempt from certain provisions of the ACA including the requirement to have a waiting period of less than 90 days (for more information see Section 13). If an employee is eligible to enroll on the 1st of the month, after two months this survey “rounds-up” and say the firm’s waiting period is three months. For these reasons some employers still have waiting periods exceed the 90 day maximum.
- Seventy-five percent of covered workers face a waiting period before coverage is available. Covered workers in small firms (3-199 workers) are more likely than those in large firms to have a waiting period, at 83% versus 72% 8. Workers in the West are more likely to face a wait for coverage than all other regions (82%).
- The average waiting period among covered workers who face a waiting period is 2.1 months 8. While 27% of covered workers face a waiting period of 3 months or more, only 4% face a waiting period of 4 months or more. Workers in small firms (3-199 workers) generally have longer waiting periods than workers in larger firms 9.
- In 2014, 11% of firms offering health benefits reported that they reduced the duration of the waiting period, significantly higher than the 2% that increased it 10.
- Ninety-one percent of covered workers at firms with many lower-wage workers (firms where 35% or more of the workforce makes $23,000 or less) face a waiting period before coverage is available compared to 76% at firms with few lower-wage workers.
- The percentage of covered workers who face a waiting period is similar to last year. The average length of the waiting period for covered workers who face a waiting period decreased, however, from 2.3 months to 2.1 months 11.
Section Four: Types Of Plans Offered
Most firms that offer health benefits offer only one type of health plan (85%) (See Text Box). Large firms (200 or more workers) are more likely to offer more than one type of health plan than smaller firms. Employers are most likely to offer their workers a PPO or HDHP/SO plan and are least likely to offer a conventional plan (sometimes known as indemnity insurance).
- Eighty-five percent of firms offering health benefits in 2014 offer only one type of health plan. Large firms (200 or more workers) are more likely to offer more than one plan type than small firms (3-199 workers): 44% vs. 14% 1.
- In addition to looking at the percentage of firms which offer multiple plan types, the percent of covered workers at firms which offer multiple plan types can be analyzed. Half (50%) of covered workers are employed in a firm that offers more than one health plan type. Sixty-three percent of covered workers in large firms (200 or more workers) are employed by a firm that offers more than one plan type, compared to 22% in small firms (3-199 workers) 2.
- Three quarters (77%) of covered workers in firms offering health benefits work in a firm that offers one or more PPO plans; 45% work in firms that offer one or more HDHP/SOs; 31% work in firms that offer one or more HMO plans; 13% work in firms that offer one or more POS plans; and 3% work in firms that offer one or more conventional plans 4.8
- Among firms offering only one type of health plan, large firms (200 or more workers) are more likely to offer PPO plans than small firms (3-199 workers) (71% versus 49%), while small firms are more likely to offer HMO (8%) and POS (20%) plans than larger firms (2% and 5%, respectively) 5.
- Eleven percent of covered workers are covered at firm which only offers an HDHP/SO.
The survey collects information on a firm’s plan with the largest enrollment in each of the plan types. While we know the number of plan types a firm has, we do not know the total number of plans a firm offers. In addition, firms may offer different types of plans to different workers. For example, some workers might be offered one type of plan at one location, while workers at another location are offered a different type of plan.
HMO is health maintenance organization.
PPO is preferred provider organization.
POS is point-of-service plan.
HDHP/SO is high-deductible health plan with a savings option such as an HRA or HSA.
Section Five: Market Shares Of Health Plans
Enrollment remains highest in PPO plans, covering more than half of covered workers, followed by HDHP/SOs, HMO plans, POS plans, and conventional plans. Enrollment distribution varies by firm size, for example, PPOs are relatively more popular for covered workers at large firms (200 or more workers) than smaller firms (63% vs. 46%) and POS plans are relatively more popular among smaller firms than large firms (17% vs. 4%). Enrollment in HDHP/SO plans (20%) remains statistically unchanged from 2012 (19%).
- Fifty-eight percent of covered workers are enrolled in PPOs, followed by HDHP/SOs (20%), HMOs (13%), POS plans (8%), and conventional plans (<1%) 1.
- After years of significant annual increases in the percentage of covered workers enrolled in HDHP/SO plans (8% in 2009, 13% in 2010, and 17% in 2011), enrollment has remained steady over the past three years (19% in 2012, and 20% in 2013 and 2014) 1. The percentage of covered workers enrolled in HDHP/SO plans at both large firms (200 or more workers) and smaller firms is similar to last year.
- Enrollment in HDHP/SOs is similar for firms with many lower wage workers (at least 35% of workers earn $23,000 per year or less) and those with fewer lower wage workers as well as between large firms (200 or more workers) and smaller firms.
- Enrollment in HMO plans is similar to 2013 but declined significantly from two years ago (16% in 2012) and five years ago (20% in 2009).
- Plan enrollment patterns vary by firm size. Workers in large firms (200 or more workers) are more likely than workers in smaller firms to enroll in PPOs (63% vs. 46%). Workers in small firms are more likely than workers in large firms to enroll in POS plans (17% vs. 4%) 2.
- Plan enrollment patterns also differ across regions.
- HMO enrollment is significantly higher in the West (25%) and significantly lower in the South (9%) and Midwest (8%) 3.
- Workers in the South (66%) are more likely to be enrolled in PPO plans than workers in other regions; workers in the West (51%) are less likely to be enrolled in a PPO 3.
- Enrollment in HDHP/SOs is higher among workers in the Midwest (27%) than in other regions 3.
- Plan enrollment patterns differ by industry as well.
- Covered workers in the state/local government industry (11%) are significantly less likely to be enrolled in an HDHP/SO plan than covered workers in other industries 3.
Section Six: Worker And Employer Contributions For Premiums
Premium contributions by covered workers average 18% for single coverage and 29% for family coverage.9 The average monthly worker contributions are $90 for single coverage ($1,081 annually) and $402 for family coverage ($4,823 annually). On average covered workers contribute a similar amount for family coverage in 2014 as they did in 2013 but more for single coverage ($90 vs. $83). There continues to be important differences by firm size; covered workers in small firms (3-199 workers) contribute a lower percentage of the premium for single coverage (16 percent versus 19 percent) but a much higher percentage of the premium for family coverage than covered workers in larger firms (35 percent versus 27 percent).
- In 2014, covered workers on average contribute 18% of the premium for single coverage and 29% of the premium for family coverage the same contribution percentages reported in 2013 1. These contributions have remained stable since 2010 for both single and family coverage.
- On average, workers with single coverage contribute $90 per month ($1,081 annually), and workers with family coverage contribute $402 per month ($4,823 annually), towards their health insurance premiums, similar to the amounts reported in 2013 for family coverage, but significantly higher for single coverage 2, 3, and 4.
- Worker contributions in HDHP/SOs are lower than the overall average worker contributions for single coverage ($905 vs. $1,081) 5. While employers contribute less for family coverage in HDHP/SO plans, the worker contribution is similar to the overall average.
- Worker contributions in other plan types are not statistically different from the overall average for either single or family coverage 5.
- In addition to differences between plan types, there are differences in worker contributions by type of firm. As in previous years, workers in small firms (3-199 workers) contribute a lower amount annually for single coverage than workers in large firms (200 or more workers), $902 vs. $1,160. In contrast, workers in small firms with family coverage contribute significantly more annually than workers with family coverage in large firms ($5,508 vs. $4,523) 8. One reason small firms may contribute a higher percentage for single coverage and a lower percentage for family coverage, compared to large firms, is to incentivize enrollment. Many insurers impose participation requirements on firms purchasing small-group coverage.
Variation in Worker Contributions to the Premium
- There is a great deal of variation in worker contributions to premiums.
- Thirty-one percent of covered workers contribute $1,513 or more annually (140% or more of the average worker contribution) for single coverage, while 20% of covered workers have an annual worker contribution of less than $649 (less than 60% of the average worker contribution) 15.
- For family coverage, 22% of covered workers contribute $6,752 or more annually (140% or more of the average worker contribution), while 24% of covered workers have an annual worker contribution of less than $2,894 (less than 60% of the average worker contribution) 15.
- The majority of covered workers are employed by a firm that contributes at least half of the premium for single and family coverage.
- Fourteen percent of covered workers with single coverage and 5% of covered workers with family coverage work for a firm that pays 100% of the premium 16.
- Covered workers in small firms (3-199 workers) are more likely to work for a firm that pays 100% of the premium for single coverage than workers in large firms (200 or more workers). Thirty-two percent of covered workers in small firms have an employer that pays the full premium for single coverage, compared to 6% of covered workers in large firms 17. For family coverage, 14% of covered workers in small firms have an employer that pays the full premium, compared to 2% of covered workers in large firms 17 and 18.
- Three percent of covered workers in small firms (3-199 workers) contribute more than 50% of the premium for single coverage, compared to one percent of covered workers in large firms (200 or more workers) 17. For family coverage, 31% of covered workers in small firms work in a firm where they must contribute more than 50% of the premium, compared to 9% of covered workers in large firms 17 and 18.
Difference by Firm Characteristics
- The percentage of the premium paid by covered workers varies by several firm characteristics.
- For family coverage, covered workers in firms with many lower-wage workers (35% or more earn $23,000 or less annually) contribute a greater percentage of the premium than those in firms with fewer lower-wage workers (44% vs. 28%) 21.
- Looking at dollar amounts, covered workers in firms with many lower-wage workers (35% or more earn $23,000 or less annually) on average contribute $6,472 for family coverage versus $4,693 for covered workers in firms with fewer lower-wage workers 13. Forty-two percent of covered workers at firms with many lower wage workers pay more than 50% of the premium for family coverage in contrast to 13% at firms with fewer lower wage workers 19.
- Covered workers with family coverage in firms that have at least some union workers contribute a significantly lower percentage of the premium than those in firms without any unionized workers (21% vs. 34%) 21.
- For workers with family coverage in large firms (200 or more workers), the average percentage contribution for workers in firms that are partially or completely self-funded is lower than the average percentage contributions for workers in firms that are fully insured (26% vs. 31%)10 21.
- Covered workers in private, for profit firms contribute a significantly higher percentage of the premium for single coverage (21%) than do workers in private not-for-profit firms (16%) and public organizations such as state or local governments (13%) 20.
Other Topics
- Among firms offering health benefits with fewer than 20 employees, 45% contribute different dollar amounts toward premiums for different employees 26. Employer may contribute different amounts to different employees based for a variety of reasons, including workers’ age, smoking status, seniority, job title or location.
- Among firms offering health benefits, one percent of small firms (3 to 199 workers) and 10% of larger firms have a policy where lower wage workers contribute a lower percentage of the premium than higher wage workers 27.
Changes over Time
- The amount which workers contribute to single coverage premiums has increased 94% since 2004 and 39% since 2009. Covered workers’ contributions to family coverage have increased 81% since 2004 and 37% since 2009. Over the last five years the average worker contribution for single and family coverage has risen at a similar rate.
- Over the last ten years the average worker contribution for family coverage has risen faster for large firms (200 or more workers) than smaller firms (63% vs. 93%). The average worker contribution for family coverage has risen at a similar rate for firms with many low income workers (35% or more earn $23,000 or less annually) and those with fewer low income workers over the past ten years.
Section Seven: Employee Cost Sharing
In addition to any required premium contributions, most covered workers face cost sharing for the medical services they use. Cost sharing for medical services can take a variety of forms, including deductibles (an amount that must be paid before most services are covered by the plan), copayments (fixed dollar amounts), and/or coinsurance (a percentage of the charge for services). The type and level of cost sharing often vary by the type of plan in which the worker is enrolled. Cost sharing may also vary by the type of service, such as office visits, hospitalizations, or prescription drugs.
The cost-sharing amounts reported here are for covered workers using services provided in-network by participating providers. Plan enrollees receiving services from providers that do not participate in plan networks often face higher cost sharing and may be responsible for charges that exceed plan allowable amounts. The framework of this survey does not allow us to capture all of the complex cost-sharing requirements in modern plans, particularly for ancillary services (such as durable medical equipment or physical therapy) or cost-sharing arrangements that vary across different settings (such as tiered networks). Therefore, we do not collect information on all plan provisions and limits that affect enrollee out-of-pocket liability.
General Annual Deductibles
- A general annual deductible is an amount that must be paid by the enrollee before most services are covered by their health plan. Non-grandfathered health plans are required to have some services such as preventative care available to enrollees without cost-sharing. Some plans require enrollees to meet a service specific deductible such as on prescription drugs or hospital admissions in lieu of or in addition to a general deductible.
- Eighty percent of covered workers are enrolled in a plan with a general annual deductible for single coverage; this is similar to 78% in 2013 2. Since 2009, the percentage of covered workers with a general annual deductible has increased from 63% to 80%.
- The percentage of covered workers enrolled in a plan with a general annual deductible is similar for small (3-199 workers) and larger firms (82% and 80%) 2.
- The likelihood of having a deductible varies by plan type. Workers in HMOs are less likely to have a general annual deductible for single coverage compared to workers in other plan types. Sixty-three percent of workers in HMOs do not have a general annual deductible, compared to 30% of workers in POS plans and 15% of workers in PPOs 1.
- Workers without a general annual plan deductible often have other forms of cost sharing for medical services. For workers without a general annual deductible for single coverage, 85% in HMOs, 78% in PPOs, and 77% in POS plans are in plans that require cost sharing for hospital admissions. The percentages are similar for family coverage 4.
- The dollars amounts of general annual deductibles vary greatly by plan type and firm size.
- The average annual deductible for covered workers across all plan types is $1,217. However, average deductibles vary considerably by plan type. The average annual deductibles among those covered workers with a deductible for single coverage are $1,032 for HMOs, $843 for PPOs, $1,215 for POS plans, and $2,215 for HDHP/SOs 5.
- The average general annual deductible for covered workers enrolled in single coverage has increased over time from $826 five years ago 7.
- Deductible amounts for HMOs and HDHP/SOs are higher compared to 2013 ($1,032 vs. $729 for HMOs and $2,215 vs. $2,003 for HDHP/SOs) 7. Covered workers enrolled at small firms (3-199 workers) have a similar deductible for HMO plans as they did in 2013. Covered workers at large firms enrolled in an HMO plan on average have a deductible of $726,11 significantly more than the amount reported in 2013.
- Deductibles are generally higher for covered workers in small firms (3-199 workers) than for covered workers in large firms (200 or more workers) across plan types 5. For covered workers in PPOs, deductibles in small firms are more than twice as large as deductibles in large firms ($1,420 vs. $657). On average, covered workers at small firms face higher general annual deductibles than covered workers at large firms ($1,797 vs. $971) 5.
- There is considerable variation in the dollar values of general annual deductibles for workers at different firms. For example 33% of covered workers enrolled in a PPO plan with a general annual deductible for single coverage have a deductible of less than $500 and 10% have a deductible of $2,000 or more 11.
- For family coverage, the majority of workers with general annual deductibles have an aggregate deductible, meaning all family members’ out-of-pocket expenses count toward meeting the deductible amount. Among those with a general annual deductible for family coverage, the percentage of covered workers with an average aggregate general annual deductible is 65% for workers in HMOs, 53% for workers in PPOs, 86% for workers in POS plans and 85% for workers in HDHP/SOs 13.
- The average amounts for workers with an aggregate deductible for family coverage are $2,328 for HMOs, $1,947 for PPOs, $2,470 for POS plans, and $4,522 for HDHP/SOs 14.
- The average aggregate deductible amount for family coverage for HDHP/SOs is higher compared to 2013 ($4,522 vs. $4,079). Deductible amounts are similar to last year for all other plan types 15.
- The other type of family deductible, a separate per-person deductible, requires each family member to meet a separate per-person deductible amount before the plan covers expenses for that member. Most plans with separate per-person family deductibles consider the deductible met for all family members if a prescribed number of family members each reach their separate deductible amounts. Plans may also require each family member to meet a separate per-person deductible until the family’s combined spending reaches a specified dollar amount.
- For covered workers in health plans that have separate per-person general annual deductible amounts for family coverage, the average plan deductibles are $870 for HMOs, $821 for PPOs, $1,153 for POS plans, and $2,126 for HDHP/SOs 14.
- Most covered workers in plans with a separate per-person general annual deductible for family coverage have a limit to the number of family members required to meet the separate deductible amounts 18.12 Among those workers in plans with a limit on the number of family members, the most frequent number of family members required to meet the separate deductible amounts is two for HMO and HDHP/SO plans, and three for POS plans 19.
- Forty-one percent of covered workers are in plans with a deductible of $1,000 or more for single coverage, similar to the percentage (38%) in 2013 9.
- Over the last five years, the percentage of covered workers with a deductible of $1,000 or more for single coverage has nearly doubled, increasing from 22% to 41% 9. Workers in small firms (3-199 workers) are more likely to have a general annual deductible of $1,000 or more for single coverage than workers in large firms (200 or more workers) (61% vs. 32%) 8.
- Eighteen percent of covered workers are enrolled in a plan with a deductible of $2,000 or more. Thirty-four percent of covered workers at small firms (3-199 workers) have a general annual deductible of $2,000 or more, in contrast to just 11% in large firms 8. The percentage of covered workers at large firms who face a deductible of $2,000 or more is significantly higher than last year 10.
- The majority of covered workers with a deductible are in plans where the deductible does not have to be met before certain services, such as physician office visits or prescription drugs, are covered.
- Large majorities of covered workers (76% in HMOs, 78% in PPOs, and 68% in POS plans) with general plan deductibles are enrolled in plans where the deductible does not have to be met before physician office visits for primary care are covered 21.
- Similarly, among workers with a general annual deductible, large shares of covered workers in HMOs (95%), PPOs (93%), and POS plans (89%) are enrolled in plans where the general annual deductible does not have to be met before prescription drugs are covered 21.
Hospital and Outpatient Surgery Cost Sharing
- In order to better capture the prevalence of combinations of cost sharing for inpatient hospital stays and outpatient surgery, the survey was changed to ask a series of yes or no questions beginning in 2009. The new format allowed respondents to indicate more than one type of cost sharing for these services, if applicable. Previously, the questions asked respondents to select just one response from a list of types of cost sharing, such as separate deductibles, copayments, coinsurance, and per diem payments (for hospitalization only). Due to the change in question format, the distribution of workers with types of cost sharing does not equal 100% as workers may face a combination of types of cost sharing. In addition, the average copayment and coinsurance rates for hospital admissions include workers who may have a combination of these types of cost sharing.
- Whether or not a worker has a general annual deductible, most workers face additional types of cost sharing when admitted to a hospital or having outpatient surgery (such as a copayment, coinsurance, or a per diem charge).
- For hospital admissions, 62% of covered workers have coinsurance and 15% have copayments. Lower percentages of workers have per day (per diem) payments (5%), a separate hospital deductible (3%), or both copayments and coinsurance (10%), while 15% have no additional cost sharing for hospital admissions after any general annual deductible has been met 22. For covered workers in HMO plans, copayments are more common (38%) and coinsurance (28%) is less common than in other plan types.
- The percentage of covered workers in a plan which requires coinsurance for hospital admission has increased from 55% in 2011 to 62% in 2014.
- The average coinsurance rate is 19%; the average copayment is $280 per hospital admission; the average per diem charge is $297; and the average separate annual hospital deductible is $490 24.
- The cost-sharing provisions for outpatient surgery are similar to those for hospital admissions, as most workers have coinsurance or copayments. Sixty-four percent of covered workers have coinsurance and 16% have copayments for an outpatient surgery episode. In addition, 1% have a separate annual deductible for outpatient surgery, and 7% have both copayments and coinsurance, while 18% have no additional cost sharing after any general annual deductible has been met 23.
- For covered workers with cost sharing for outpatient surgery, the average coinsurance is 19% and the average copayment is $157 24.
Cost Sharing for Physician Office Visits
- The majority of covered workers are enrolled in health plans that require cost sharing for an in-network physician office visit, in addition to any general annual deductible.13
- The most common form of physician office visit cost sharing for in-network services is copayments. Seventy-three percent of covered workers have a copayment for a primary care physician office visit and 18% have coinsurance. For office visits with a specialty physician, 72% of covered workers have copayments and 21% have coinsurance. Workers in HMOs, PPOs, and POS plans are much more likely to have copayments than workers in HDHP/SOs for both primary care and specialty care physician office visits. The majority of workers in HDHP/SOs have coinsurance (56%) or no cost sharing after the general annual plan deductible is met (24%) for primary care physician office visits 25.
- Among covered workers with a copayment for in-network physician office visits, the average copayment is $24 for primary care and $36 for specialty physicians 26, similar to $23 and $35 reported in 2013.
- Among workers with coinsurance for in-network physician office visits, the average coinsurance rates are 18% for a visit with a primary care physician and 19% for a visit with a specialist 26.
Out-Of-Pocket Maximum Amounts
- Most covered workers are in a plan that partially or totally limits the cost sharing that a plan enrollee must pay in a year. These limits are generally referred to as out-of-pocket maximum amounts. The ACA requires that non-grandfathered health plans with a plan year starting in 2014 have an out-of-pocket maximum of $6,350 or less for single coverage and $12,700 for family coverage. Firms that either renewed their plan prior to January 1st (known as “early renewals”) or plans which are grandfathered are not required to comply with this provision. As plans lose their grandfathered status, more firms will be subject to this provision. Many plans have complex out-of-pocket structures, increasing the difficulty of accurately collecting information on this element of plan design.
- In 2014, 94% percent of covered workers have an out-of-pocket maximum for single coverage, significantly more than 88% in 2013 37. Six percent of covered workers are in a plan that does not limit the amount of cost sharing enrollees have to pay for either single or family coverage 31.
- Covered workers without an out-of-pocket maximum, however, may not have large cost-sharing responsibilities. For example, 57% of covered workers in PPOs with no out-of-pocket maximum for single coverage have no general annual deductible compared to 86% of covered workers in PPOs who have an out-of-pocket limit. Among covered workers enrolled in a PPO plan without an out-of-pocket limit, less than one percent have a coinsurance for hospital admission and three percent for outpatient surgery.
- For covered workers with out-of-pocket maximums, there is wide variation in spending limits.
- Twenty-one percent of covered workers with an out-of-pocket maximum for single coverage have an out-of-pocket maximum of less than $2,000, while 9% have an out-of-pocket maximum of $6,000 or more 32.
- Covered workers with an out-of-pocket maximum in small firms (3 to 199 workers) are more likely than such workers in larger firms to be covered by a plan with an out-of-pocket maximum of $3,000 or more (61% vs. 51%).
- The percentage of covered workers who either do not have an out-of-pocket limit or have an out of pocket limit of more than $6,350 dollars for single coverage decreased from 14% in 2013 to 7% in 2014 37.
- Like deductibles, some plans have an aggregate out-of-pocket maximum amount for family coverage that applies to cost sharing for all family members, while others have a per-person out-of-pocket maximum that limits the amount of cost sharing that the family must pay on behalf of each family member. Sixty-eight percent of covered workers in a plan with an out-of-pocket maximum are in a plan with an aggregate limit 33.
- For covered workers with an aggregate out-of-pocket maximum for family coverage, 21% have an out-of-pocket maximum of less than $4,000 and 21% have an out-of-pocket maximum of $10,000 or more 34. Among workers with separate per-person out-of-pocket limits for family coverage, 72% have out-of-pocket maximums of less than $4,000 35.
- The ACA requires that most in-network deductibles, copays, and coinsurances are counted towards the out-of-pocket limit for non-grandfathered plans for plan years starting after January 1st, 2014. As discussed above some covered workers remain in plans that are not subject to this provision.
Section Eight: High-deductible Health Plans With Savings Option
To cover out-of-pocket expenses not covered by the plan, some employers offer high deductible plans which are paired with an account which allows enrollees to use tax-preferred savings to pay plan cost sharing and other out-of-pocket medical expenses. The two most common are health reimbursement arrangements (HRAs) and health savings accounts (HSAs). HRAs and HSAs are financial accounts that workers or their family members can use to pay for health care services. These savings arrangements are often (or, in the case of HSAs, always) paired with health plans with high deductibles. The survey treats high-deductible plans paired with a savings option as a distinct plan type – High-Deductible Health Plan with Savings Option (HDHP/SO) – even if the plan would otherwise be considered a PPO, HMO, POS plan, or conventional health plan. Specifically for the survey, HDHP/SOs are defined as (1) health plans with a deductible of at least $1,000 for single coverage and $2,000 for family coverage14 offered with an HRA (referred to as HDHP/HRAs); or (2) high-deductible health plans that meet the federal legal requirements to permit an enrollee to establish and contribute to an HSA (referred to as HSA-qualified HDHPs).15
Percentage of Firms Offering HDHP/HRAs and HSA-Qualified HDHPs, and Enrollment
- Twenty-seven percent of firms offering health benefits offer an HDHP/HRA or an HSA-qualified HDHP. Among firms offering health benefits, 4% offer an HDHP/HRA and 24% offer an HSA-qualified HDHP 1. The percentage of firms offering a HDHP/SO is similar to last year but has increased over time.
- Firms with 5,000 or more workers are significantly more likely to offer an HDHP/SO than smaller firms. Forty-five percent of firms with 1,000 or more workers offer an HDHP/SO, compared to 27% of firms with 3 to 199 workers, and 38% of firms with 200-999 workers 2. Not all covered workers enrolled at a firm which offers an HDHP/SO may be eligible to enroll in the plan; for example the HDHP/SO plan may only be offered in one location (see Section 4 for more information).
Health Reimbursement Arrangements (HRAs) are medical care reimbursement plans established by employers that can be used by employees to pay for health care. HRAs are funded solely by employers. Employers may commit to make a specified amount of money available in the HRA for premiums and medical expenses incurred by employees or their dependents. HRAs are accounting devices, and employers are not required to expend funds until an employee incurs expenses that would be covered by the HRA. Unspent funds in the HRA usually can be carried over to the next year (sometimes with a limit). Employees cannot take their HRA balances with them if they leave their job, although an employer can choose to make the remaining balance available to former employees to pay for health care.
HRAs often are offered along with a high-deductible health plan (HDHP). In such cases, the employee pays for health care first from his or her HRA and then out-of-pocket until the health plan deductible is met. Sometimes certain preventive services or other services such as prescription drugs are paid for by the plan before the employee meets the deductible.
Health Savings Accounts (HSAs) are savings accounts created by individuals to pay for health care. An individual may establish an HSA if he or she is covered by a “qualified health plan” –a plan with a high deductible (i.e., a deductible of at least $1,250 for single coverage and $2,500 for family coverage in 2014) that also meets other requirements.[1] Employers can encourage their employees to create HSAs by offering an HDHP that meets the federal requirements. Employers in some cases also may assist their employees by identifying HSA options, facilitating applications, or negotiating favorable fees from HSA vendors.
Both employers and employees can contribute to an HSA, up to the statutory cap of $3,300 for single coverage and $6,550 for family coverage in 2014. Employee contributions to the HSA are made on a pre-income tax basis, and some employers arrange for their employees to fund their HSAs through payroll deductions. Employers are not required to contribute to HSAs established by their employees but, if they elect to do so, their contributions are not taxable to the employee. Interest and other earnings on amounts in an HSA are not taxable. Withdrawals from the HSA by the account owner to pay for qualified health care expenses are not taxed. The savings account is owned by the individual who creates the account, so employees retain their HSA balances if they leave their job.
1 See U.S. Department of the Treasury, Health Savings Accounts, available at http://www.irs.gov/pub/irs-drop/rp-13-25.pdf
- In addition to looking at the percentage of firms which offer an HDHP/SO the survey can analyze the percentage of workers who are enrolled in this plan type. Twenty percent of covered workers are enrolled in an HDHP/SO in 2014, the same as last year 5. Enrollment in HDHP/SOs had increased significantly for several years (17% of covered workers in 2011 from 13% in 2010 and 8% in 2009) but has plateaued since 2012.
- Seven percent of covered workers are enrolled in HDHP/HRAs in 2014, and 14% percent of covered workers are enrolled in HSA-qualified HDHPs (Exhibit 8.6). Enrollment in both HSA-qualified HDHPs and HDHP/HRAs is similar to last year 5.
Plan Deductibles
- As expected, workers enrolled in HDHP/SOs have higher deductibles than workers enrolled in HMOs, PPOs, or POS plans.
- The average general annual deductible for single coverage is $2,265 for HDHP/HRAs and $2,205 for HSA-qualified HDHPs 7. These averages are similar to the amounts reported in recent years. There is wide variation around these averages 9. Twenty-three percent of covered workers are enrolled in a HDHP/SO with a deductible of $3,000 or more.
- Since 2006, the survey has collected information on two types of family deductibles. The survey asks employers whether the family deductible amount is (1) an aggregate amount (i.e., the out-of-pocket expenses of all family members are counted until the deductible is satisfied), or (2) a per-person amount that applies to each family member (typically with a limit on the number of family members that would be required to meet the deductible amount) (for more information see Section 7).
- The average aggregate deductibles for workers with family coverage are $4,909 for HDHP/HRAs and $4,391 for HSA-qualified HDHPs 7. There is wide variation around these average amounts for family coverage 11. A quarter of covered workers enrolled in HDHP/SO plans have an aggregate family deductible of $6,000 dollars or more.
Out-of-Pocket Maximum Amounts
- HSA-qualified HDHPs are legally required to have a maximum annual out-of-pocket liability of no more than $6,350 for single coverage and $12,700 for family coverage in 2014. After January 1, 2014 non-grandfathered HDHP/HRA plans will be required to comply with the same requirements.
- The average annual out-of-pocket maximum for single coverage is $3,825 for HDHP/HRAs16 and $3,953 for HSA-qualified HDHPs 7.
- As with deductibles, the survey asks employers whether the family out-of-pocket maximum liability is (1) an aggregate amount that applies to spending by any covered person in the family, or (2) a separate per person amount that applies to spending by each family member or a limited number of family members. The survey also asks whether spending by enrollees on various services counts towards meeting the plan out-of-pocket maximum.
- Among covered workers with family coverage whose out-of-pocket maximum is an aggregate amount that applies to spending by any covered person in the family, the average annual out-of-pocket maximums are $7,592 for HDHP/HRAs and $7,791 for HSA-qualified HDHPs 7. The out of pocket limits are similar between HDHP/HRAs and HSA-qualified HDHPs for single and family coverage.
Premiums
- In 2014, the average annual premiums for HDHP/HRAs are $6,040 for single coverage and $17,279 for family coverage 8.
- The average annual premium for workers in HSA-qualified HDHPs is $4,949 for single coverage and $14,514 for family coverage. These amounts are significantly lower than the average single and family premium for workers in plans that are not HDHP/SOs 8.
- The average single and family coverage premium for an HSA-qualified HDHP is less than the amounts for covered workers enrolled in HDHP/HRAs.
Worker Contributions to Premiums
- The average annual worker contributions to premiums for workers enrolled in HDHP/HRAs are $1,165 for single coverage and $4,933 for family coverage 8.
- The average annual worker contributions to premiums for workers in HSA-qualified HDHPs are $780 for single coverage and $4,126 for family coverage 8. The average contribution for single coverage for workers in HSA-qualified HDHPs is significantly less than the average premium contribution made by covered workers in plans that are not HDHP/SOs 8.
Employer Contributions to Premiums and Savings Options
- Employers contribute to HDHP/SOs in two ways: through their contributions toward the premium for the health plan and through their contributions (if any, in the case of HSAs) to the savings account option (i.e., the HRAs or HSAs themselves).
- Looking at only the annual employer contributions to premiums, covered workers in HDHP/HRAs on average receive employer contributions of $4,875 for single coverage and $12,346 for family coverage 8.
- The average annual employer contributions to premiums for workers in HSA-qualified HDHPs are $4,169 for single coverage and $10,388 for family coverage. These amounts are lower than the average contributions for single or family coverage for workers in plans that are not HDHP/SOs 8.
- When looking at employer contributions to the savings option, workers enrolled in HDHP/HRAs receive, on average, an annual employer contribution to their HRA of $1,390 for single coverage and $2,781 for family coverage 8.
- HRAs are generally structured in such a way that employers may not actually spend the whole amount that they make available to their employees’ HRAs.17 Amounts committed to an employee’s HRA that are not used by the employee generally roll over and can be used in future years, but any balance may revert back to the employer if the employee leaves his or her job. Thus, the employer contribution amounts to HRAs that we capture in the survey may exceed the amount that employers will actually spend.
- Workers enrolled in HSA-qualified HDHPs on average receive an annual employer contribution to their HSA of $769 for single coverage and $1,347 for family coverage 8.
- In some cases, employers that sponsor HSA-qualified HDHP/SOs do not make contributions to HSAs established by their employees. Thirty-three percent of employers offering single coverage and twenty-seven percent offering family coverage through HSA-qualified HDHPs do not make contributions towards the HSAs that their workers establish 8. Twenty-four percent of workers with single coverage and twenty-three percent of workers with family coverage in an HSA-qualified HDHP do not receive an account contribution from their employer 14 and 15. Many employers are beginning to incorporate more complex structures to fund savings accounts, including providing a higher contribution if workers complete wellness or other health promotion activities.
- The percentage of covered workers enrolled in a plan where the employer makes no HSA contribution for single coverage is similar to 31% last year and five years ago.
- The average HSA contributions reported above include the portion of covered workers whose employer contribution to the HSA is zero. When those firms that do not contribute to the HSA are excluded from the calculation, the average employer contribution for covered workers is $1,006 for single coverage and $1,744 for family coverage 8.
- Employer contributions to savings account options (i.e., the HRAs and HSAs themselves) for their employees can be added to their health plan premium contributions to calculate total employer contributions toward HDHP/SOs.
- For HDHP/HRAs, the average annual total employer contribution for covered workers is $6,265 for single coverage and $15,127 for family coverage. The average total employer contribution amounts for single and family coverage in HDHP/HRAs are higher than the average amount that employers contribute towards single and family coverage in health plans that are not HDHP/SOs 8.
- For HSA-qualified HDHPs, the average annual total employer contribution for covered workers is $4,937 for single coverage and $11,762 for workers with family coverage. The total amounts contributed for workers in HSA-qualified HDHPs for single and family coverage are similar to the amounts contributed for workers not in HDHP/SOs 8.
Variation in Employer Contributions to Savings Options
- There is considerable variation in the amount that employers contribute to savings accounts.
- Forty-four percent of covered workers are enrolled in a plan with an HRA annual contribution of less than $834 and 23% are enrolled in a plan with a contribution of $1,946 or more for single coverage 16
- Thirty-four percent of covered workers are enrolled in a plan with an HSA annual contribution of less than $462 and 24% are enrolled in a plan with a contribution of $1,077 or more for single coverage 17.
- Twenty-four percent of covered workers in an HSA-qualified HDHP work for an employer who does not make a contribution towards their employees HSA account 14. The percent of covered workers enrolled in an HSA-qualified HDHP without an employer contribution has remained consistent across time.
Cost Sharing for Office Visits, Outpatient Surgery and Hospital Surgery
- The cost-sharing pattern for primary care office visits differs for workers enrolled in HDHP/HRA and HSA Qualified HDHPs. Forty-six percent of covered workers enrolled in HDHP/HRAs have a copayment for primary care physician office visits compared to 7% enrolled in an HSA-qualified HDHP (Exhibit 8.18). Covered workers in HDHP/HRAs are less likely to have a coinsurance (38%) for a primary care physician office visits than those in a HSA Qualified HDHPs (64%) 18.
Section Nine: Prescription Drug Benefits
Almost all covered workers have coverage for prescription drugs. More than three in four covered workers are in plans with three or more cost-sharing tiers for prescription drugs. For these workers copayments, rather than coinsurance, continue to be the more common form of cost sharing.
- As in prior years, nearly all (more than 99%) covered workers in employer-sponsored plans have a prescription drug benefit.
- An overwhelming majority of covered workers (90%) have a tiered cost-sharing formula for prescription drugs in 2014 1. Cost-sharing tiers generally refer to a health plan placing a drug on a formulary or preferred drug list, which classifies drugs as generic, preferred, or non-preferred. Over the last few years, an increasing number of plans have created a fourth or even higher tier of drug cost sharing, which may be used for lifestyle drugs or expensive biologics. Employers often place various drugs in generic, preferred, or non-preferred tiers to encourage enrollees to select cheaper alternatives or to pass on to enrollees the higher costs of more expensive drugs. Sometimes employers will place high initial cost sharing for higher tier drugs but then include a coinsurance maximum to limit an enrollees total liability.
- Eighty percent of covered workers are enrolled in plans with three, four, or more tiers of cost sharing for prescription drugs, similar to 82% of covered workers in 2013 1.
- HDHP/SOs have different cost-sharing patterns for prescription drugs than other plan types. Only 43% of covered workers in HDHP/SOs are in a plan with three tiers of cost sharing for prescription drugs; 15% are in plans that pay 100% of prescription costs once the plan deductible is met 2.
Three or More Tiers
- Twenty percent of covered workers are in a plan that has four or more tiers of cost sharing for prescription drugs 1.
- Among workers covered by plans with three or more tiers of cost sharing for prescription drugs, copayments are far more common than coinsurance in the first three tiers 3. For covered workers in plans with three or more cost-sharing tiers, 39% face a copayment for fourth-tier drugs and 49% face coinsurance 3.
- For covered workers in plans with three, four, or more tiers of cost sharing for prescription drugs, the average drug copayments for second-tier drugs ($31), third-tier drugs ($53), and fourth-tier drugs ($83) are comparable to the amounts reported in 2013 ($29, $52, and $80, respectively) 4. However, for first-tier drugs, copayments increased slightly from $10 in 2013 to $11 in 2014.
- For covered workers in plans with three, four, or more tiers of cost sharing for prescription drugs who face coinsurance rather than copayments, coinsurance levels average 19% for first-tier drugs, 24% for second-tier drugs, 37% for third-tier drugs, and 29% for fourth-tier drugs. These estimates are similar to last year (16%, 25%, 38%, and 32%, respectively) 4.
Single and Two Tiers
- Ten percent of covered workers are in a plan that has two tiers for prescription drug cost sharing 1. Similar to workers in plans with more cost-sharing tiers, copayments are more common than coinsurance for workers in plans with two tiers 5. The average copayment for the first tier is $11, and the average copayment for the second tier is $30. The average coinsurance rate for the second tier is 27% 6.
- Five percent of covered workers are covered by plans in which cost sharing is the same regardless of the type of drug chosen .
- For those workers with the same cost sharing regardless of the type of drug, the average copayment is $15 and the average coinsurance is 22% 8.
- Coinsurance rates for prescription drugs often have maximum or minimum dollar amounts associated with the coinsurance rate; for example for generic or first tier drugs, 21% of workers with a coinsurance rate have only a maximum dollar amount attached to the coinsurance rate, 10% have only a minimum dollar amount, 27% have both, and 42% have neither 9.
Generic drugs: Drugs product that are no longer covered by patent protection and thus may be produced and/or distributed by multiple drug companies.
Preferred drugs: Drugs included on a formulary or preferred drug list; for example, a brand-name drug without a generic substitute.
Non-preferred drugs: Drugs not included on a formulary or preferred drug list; for example, a brand-name drug with a generic substitute.
Fourth-tier drugs: New types of cost-sharing arrangements that typically build additional layers of higher copayments or coinsurance for specifically identified types of drugs, such as lifestyle drugs or biologics.
Brand-name drugs: Generally, a drug product that is covered by a patent and is thus manufactured and sold exclusively by one firm. Cross-licensing occasionally occurs, allowing an additional firm to market the drug. After the patent expires, multiple firms can produce the drug product, but the brand name or trademark remains with the original manufacturer’s product.
Section Ten: Plan Funding
Federal law (the Employee Retirement Income Security Act of 1974, or ERISA) exempts self-funded plans from most state insurance laws, including reserve requirements, mandated benefits, premium taxes, and consumer protection regulations. Three in five covered workers are in a self-funded health plan. Self-funding is common among larger firms because they can spread the risk of costly claims over a large number of employees and dependents. Many self-funded plans use insurance, often called stoploss coverage, to limit the plan sponsor’s liability for very large claims or an unexpected level of expenses. More than three in five covered workers in fully or partially self-funded plans are in plans with stop-loss protection.
Self-Funded Plan: An insurance arrangement in which the employer assumes direct financial responsibility for the costs of enrollees’ medical claims. Employers sponsoring self-funded plans typically contract with a third-party administrator or insurer to provide administrative services for the self-funded plan. In some cases, the employer may buy stop-loss coverage from an insurer to protect the employer against very large claims.
Fully Insured Plan: An insurance arrangement in which the employer contracts with a health plan that assumes financial responsibility for the costs of enrollees’ medical claims.
- Sixty-one percent of covered workers are in a plan that is completely or partially self-funded, the same percentage reported in 2013 1. The percentage of covered workers who are in a self-funded plan has increased over time from 49% in 2000 and 54% in 2004, but has remained steady in the last five years (57% in 2009).
- The percentage of covered workers in self-funded plans in small (3-199 workers) and larger firms (15% and 81%) is unchanged from 2009 (15% and 77%, respectively) 2.
- The percentage of covered workers differs by plan type: 71% of covered workers in PPOs, 60% in HDHP/SOs, 32% in HMOs, and 22% in POS plans are in a self-funded plan 3. Plan enrollment varies by firm size.
- As expected, covered workers in large firms (200 or more workers) are significantly more likely to be in a self-funded plan than covered workers in small firms (3-199 workers) (81% vs. 15%) 4. The percentage of covered workers in self-funded plans increases as the number of employees in a firm increases. Eighty-three percent of covered workers in firms with 1,000 to 4,999 workers and 91% of covered workers in firms with 5,000 or more workers are in self-funded plans in 2014 4.
- The percentage of covered workers at small firms who are enrolled in a self-funded plan is similar to last year and has remained stable over the last couple of years 2.
- Sixty-five percent of workers in self-funded health plans are in plans that have stoploss insurance 10. Stoploss coverage limits the amount that a plan sponsor has to pay in claims. Stoploss coverage may limit the amount of claims that must be paid for each employee or may limit the total amount the plan sponsor must pay for all claims over the plan year.
- The percent of workers in self-funded health plans that are in plans with stoploss insurance is unchanged from 2011, when the survey first asked about stoploss insurance (65% in 2014 vs. 58%).
- Ninety-two percent of covered workers in self-funded plans that have stoploss protection are in plans where the stoploss insurance limits the amount that the plan must spend on each employee 11. This includes stoploss insurance plans that limit a firm’s per employee spending as well as plans that limit both a firm’s overall spending and per employee spending.
- Firms with per enrollee stoploss coverage were asked for the dollar amount where the stoploss coverage would start to pay for most or all of the claim (called an attachment point). The average attachment point in firms with 3-199 workers is about $134,000. For larger firms (200 or more workers) with a per-person limit, the average attachment point is about $328,000 11.
Section Eleven: Retiree Health Benefits
Retiree health benefits are an important consideration for older workers making decisions about their retirement. Health benefits for retirees provide an important supplement to Medicare for retirees age 65 or older. Over time, the percentage of firms offering retiree coverage has decreased.
- Twenty-five percent of large firms (200 or more workers) that offer health benefits to their employees offer retiree coverage in 2014, similar to 28% in 2013. There has been a downward trend in the percentage of firms offering retirees coverage, from 34% in 2006 and 66% in 1988 1.
- The offering of retiree health benefits varies considerably by firm characteristics.
- Very large firms (5,000 or more workers) are more likely to offer retiree health benefits than firms with 200-999 workers – 49% vs. 23% 2.
- Among large firms (200 or more workers) that offer health benefits, state and local governments (83%) are more likely than large firms in other industries to offer retiree health benefits. In contrast, large firms in the wholesale industry are less likely (5%) to offer retiree health benefits when compared to large firms in other industries 2.
- Large firms with fewer lower-wage workers (less than 35% of workers earn $23,000 or less annually) are more likely to offer retiree health benefits than large firms with many lower-wage workers (28% vs. 6%). A comparable pattern exists in firms with a larger proportion of higher-wage workers (35% or more earn $57,000 or more annually) versus firms with a small proportion of higher-wage workers (37% vs. 18%) 3.
- Large firms with at least some union workers are more likely to offer retiree health benefits than large firms without any union workers – 45% vs. 19% 3.
- Large, public employers such as state or local governments are more likely to offer retiree benefits than large private for-profit firms or private not-for-profit employers. (67% vs. 16% and 22%, respectively) 3.
- Among all large firms (200 or more workers) offering retiree health benefits, most firms offer them to early retirees under the age of 65 (92%). A lower percentage (72%) of large firms offering retiree health benefits offer them to Medicare-age retirees 4. These percentages are similar to 2013 and have remained stable over time.
- Among all large firms (200 or more workers) offering health benefits to active workers and offering retiree coverage, 65% offer health benefits to both early and Medicare-age retirees.
- Among all large firms (200 or more workers) offering retiree health benefits, 3% offer coverage which covers only prescription drugs 6.
Private Exchanges and Public Exchanges
- A private exchange is created by a consulting company or insurer, not by either a federal or state government. Private exchanges allow employees or retirees to choose from several health benefit options offered on the exchange. Four percent of large employers offering retiree health benefits do so through a private exchange 7. For more information on the use of private exchanges for active employees, please see section 14.
- Starting in 2014, households with an income between 100% and 400% of the federal poverty line and without an offer of employer coverage may be eligible for subsidized health insurance on federal and state exchanges. Some current retirees may be eligible for premium tax credits for coverage provided through these marketplaces.
- Twenty-five percent of large firms (200 or more workers) offering retiree health coverage say they are considering changes in the way they offer retiree health benefits because of the new marketplaces 8.
Section Twelve: Wellness Programs And Health Risk Assessments
A large majority of firms offering health benefits offer some type of wellness program, with large firms (200 or more workers) being more likely than smaller firms (3-199 workers) to do so. Thirty-six percent of large firms and 18% of small firms offering at least one wellness benefit offer financial incentives to employees who participate in wellness programs. Thirty-three percent of firms offer employees the opportunity to complete health risk assessments, with some of these firms tying financial penalties or rewards to employees who do so. Some employers have increased the complexity of their incentive programs, and are providing rewards and/or penalties to workers who complete a range of activities including health risk assessments, biometric screening and wellness programs. The interactions among these programs are difficult to capture in a survey. Only firms offering health benefits were asked about their wellness and health promotion programs
Wellness Benefits
For a variety of reasons, including efforts to improve health and lower costs, many employers and health plans offer wellness programs. Wellness programs may range from classes in nutrition or healthy living to a wellness newsletter.
- Seventy-four percent of firms offering health benefits offer at least one of the following wellness programs:
- Weight loss programs
- Biometric screenings
- Gym membership discounts or on-site exercise facilities
- Smoking cessation program
- Lifestyle or behavioral coaching
- Classes in nutrition or healthy living
- Web-based resources for healthy living
- Flu shot or vaccinations
- Employee assistance program (EAP)
- Wellness newsletter
- Large firms (200 or more workers) offering health benefits are more likely to offer each of the listed wellness programs than smaller firms. In addition, large firms (200 or more workers) offering health benefits are more likely to offer at least one of the listed wellness programs than smaller firms (98% vs. 73%) 3.
- The percent of large firms (200 or more workers) and small firms offering wellness programs is similar to last year.
- About half of firms offering health benefits offer flu shots or vaccinations (53%), a wellness newsletter (34%) or web-based resources for healthy living (39%). The offer rate for each type of wellness benefit included in the survey is presented in 1, 2 and 3.
- Among firms offering health benefits and at least one wellness program, 74% report that most of the wellness benefits they offer are provided by the health plan 4.18 Small firms (3 to 199 workers) are more likely than larger firms to report that most wellness programs are provided by the health plan (75% vs. 55%) 4. Some employers may have wellness programs offered by both the firm and their plan.
Incentives for Wellness benefits
- In order to encourage participation in wellness programs, firms may offer financial incentives to employees who participate.19
- Nineteen percent of firms offering wellness benefits offer at least one of the following financial incentives for participating in a wellness program:
- Lower premiums
- Reduced cost sharing
- Higher health reimbursement arrangement or HSA contributions
- Gift cards, travel, merchandise, or cash
- Large firms (200 or more workers) are more likely to offer these incentives for participating than smaller firms (36% vs. 18%) 5.
- A small percentage of firms offering health benefits and at least one of the listed wellness programs offers gift cards, travel, merchandise, or cash (14%), lower worker premium contributions (8%) or cost sharing (such as lower deductibles) (1%) as an incentive to encourage employees to participate. Among firms that offer a high-deductible health plan paired with a HRA or HSA, 2% offer workers who participate in wellness programs receive higher HSA or HRA contributions 5.
- In addition to offering employees incentives to participate in wellness program, some employers offer incentives to employees who complete programs or activities. The Affordable Care Act allows employers to increase the size of their financial incentives for completing wellness programs. Under new rules, firms can increase an employee’s premium contribution up to 30% of the cost of the plan for not completing wellness programs provided that the wellness program is reasonably designed and there are alternatives for employees who cannot meet the standard.
- Twelve percent of large firms offer a financial incentive to employees who complete a wellness program 7. Of these firms, 32% of employers reported that the maximum incentive an employee can be awarded for completing a wellness program is $500 or more.
- Firms with one of the listed incentives above for participating in wellness programs (lower premiums, reduced cost-sharing, higher HRA/HSA contributions or gift cards, travel, merchandise, or cash) were asked how effective they believed incentives were for encouraging participation. Only 14% of firms offering health benefits and at least one of the listed wellness programs think that financial incentives are “very effective” in encouraging employees to participate. Large firms (200 or more workers) offering incentives for participating in wellness programs are more likely than smaller ones to believe incentives are “very effective” (33% versus 12%) 6.
Health Risk Assessments
Some firms give their employees the opportunity to complete a health risk assessment to identify potential health issues. Health risk assessments generally include questions about medical history, health status, and lifestyle.
- Overall, 33% of firms offering health benefits offer their employees the opportunity to complete a health risk assessment. Large firms (200 or more workers) are more likely than smaller firms to offer employees this option (51% vs. 32%) 8.
- Some firms offer financial incentives to encourage employees to complete health risk assessments.
- Fifty-one percent of large firms (200 or more workers) offering health risk assessments give financial incentives to employees who complete a health risk assessment, and 36% of these offer a financial incentive that may be worth more than or equal to $500 10.
- Three percent of large firms (200 or more workers) that offer health risk assessments require employees to complete a health risk assessment in order to enroll in a health plan 9.
- Seven percent of large firms (200 or more workers) that provide employees the opportunity to complete a health risk assessment penalize employees with identified health risks factors who do not complete a wellness program (9%) 9.
- Among firms offering health benefits, the percentage of large firms (200 or more workers) who offer their employees the opportunity to complete a health risk assessment is similar to last year 14.
Biometric Screening
Biometric screening is a health examination that measures an employee’s risk factors, such as cholesterol, blood pressure, stress, and nutrition. Biometric outcomes may include meeting a target body mass index (BMI) or cholesterol level.
- Twenty-six percent of small firms (3 to 199 workers) and 51% of larger firms offering health benefits offer biometric screenings as a wellness benefit 1.
- Firms which offer their employees biometric screenings may include additional incentives for those employees who complete screenings. Among large firms (200 or more workers) offering biometric screenings, one percent require employees to complete biometric screenings in order to enroll in a health plan 12.
- Among large firms (200 or more workers) offering biometric screenings, eight percent reward or penalize employees for meeting biometric outcomes. Of these firms 42% offer a maximum financial incentive of $500 or more 13.
Section Thirteen: Grandfathered Health Plans
The Affordable Care Act (ACA) is bringing about a number of changes for the American health care system, including for employer-sponsored health insurance. In 2014 many new provisions took effect for group coverage including limits on waiting periods, out-of-pocket maximums, and many reforms for the small employer market. Other key provisions of the ACA, such as the non-discrimination requirements and the employer shared responsibility provision, were delayed until 2015. In some cases small employers were given new coverage options through SHOP exchanges, although the implementation was limited. SHOP marketplaces were available for shopping for coverage, but firms could not complete the transaction online and had to buy directly from the issuer or through a broker. (For more information, see Sections 2, 7, and 11, and the health reform implementation timeline at http://www.kff.org/interactive/implementation-timeline/.) The ACA exempts certain health plans that were in effect when the law was passed, referred to as grandfathered plans, from some of the new standards in the law; these include requirements to cover preventive benefits without cost sharing, have an external appeals process, or comply with the new benefit and rating provisions in the small group market.
Grandfathering
For the employer-sponsored market, health plans that were in place when the ACA was enacted (March 2010) can be grandfathered health plans. Interim final rules released by the Department of Health and Human Services on June 17, 2010, and amended on November 17, 2010, stipulate that firms cannot significantly change cost sharing, benefits, employer contributions, or access to coverage in grandfathered plans.20 New employees can enroll in a grandfathered plan as long as the firm has maintained consecutive enrollment in the plan.
Grandfathered plans are exempted from many of the ACA’s new requirements, but still must comply with other provisions as they become effective, including: (1) provide a uniform explanation of coverage, (2) report medical loss ratios and provide premium rebates if medical loss ratios are not met, (3) prohibit lifetime and annual limits on essential health benefits, (4) extend dependent coverage to age 26, (5) prohibit health plan rescissions, (6) prohibit waiting periods greater than 90 days, and (7) prohibit coverage exclusions for pre-existing health conditions.21 Firms must decide whether to grandfather their insurance plans, which limits the changes they can make to their plans, or whether to comply with the full set of new health reform requirements.
- There is a decline in the percentage of offering firms that have at least one health plan that is a grandfathered plan. Thirty-seven percent of offering firms have at least one grandfathered plan in 2014, down from 54% in 2013, 58% in 2012, and 72% in 2011.
- Worker enrollment in grandfathered plans also has decreased, with 26% of covered workers enrolled in a grandfathered health plan in 2014, down from 36% in 2013, 48% in 2012 and 56% in 2011 3.
- A similar decrease is seen by firm size. In 2014, 35% of covered workers in small firms (3-199 workers) enrolled in a grandfathered health plan, down from 49% in 2013, 54% in 2012, and 63% in 2011. For larger firms, 22% of covered workers enrolled in a grandfathered health plan, down from 30% in 2013, 46% in 2012, and 53% in 2011 3.
Section Fourteen: Employer Opinions And Health Plan Practices
Employers play a significant role in health insurance coverage – so their opinions and experiences are important factors in health policy discussions. Employers continue to innovate on how they offer, structure, and deliver their benefits. A considerable number of employers have developed strategies to reduce cost or improve quality through changes to their plan’s provider networks.
Employer Opinions on Cost Containment
Firms offering health benefits were asked to rate how effective several different strategies would be in reducing the growth of health insurance costs.
- Twenty-eight percent of firms offering health benefits stated that “wellness programs” would be very effective at containing health insurance costs, more than the percentage of firms indicating “tighter managed care restrictions”, “higher employee cost sharing”, “disease management programs”, “tiered provider networks” and “narrow networks”. The percentage of firms offering health benefits who thought that wellness programs would be very effective at containing health insurance costs was similar to the percentage who thought that consumer driven health plans would be very effective (28% and 22%, respectively) 1.
- Just six percent of firms offering health benefits stated that narrow networks would be very effective at containing health insurance costs 1. More firms offering health benefits indicated that narrow networks would be not at all effective at containing costs than any other strategy.
- Ten percent of firms offering health benefits thought that “tighter managed care restrictions” and 11% stated that “tiered provider networks” would be very effective at containing health care costs. Fewer employers offering health benefits thought these strategies would be very effective than either “Consumer-Driven Health Plans” or “Wellness Programs” 1.
Shopping for Health Coverage
More than one-half (58%) of firms offering health benefits reported shopping for a new health plan or a new insurance carrier in the past year, suggesting that the market is quite dynamic
3. The largest firms, those with a 1,000 to 4,999 employees or firms were with more than 5,000 workers, were less likely to shop for a new plan or carrier.
- Among firms that offer health benefits and shopped for a new plan or carrier, 27% changed insurance carriers. There were no significant differences between small firms (3 to 199 workers) and larger firms 4.
Tiered Networks
A tiered or high performance network is one that groups providers in the network together based on quality, cost, and/or the efficiency of the care they deliver. These networks encourage patients to visit preferred doctors by either restricting networks to efficient providers, or by having different copayments or coinsurance for providers in different tiers in the network.
- Nineteen percent of firms that offer health benefits include a high performance or tiered provider network in the health plan with the largest enrollment 5. This is similar to the 23% reported in 2013 and the 20% reported in 2011.
- Employers may use different criteria to determine which providers are included in which tiers. Fifty-nine percent of offering firms whose largest plan includes a high performance or tiered provider network stated that the network tiers were determined both by providers’ “quality and cost/efficiency”. Large firms (200 or more workers) were most likely to indicated that the tiers are determined by both “quality and cost/efficiency” than any other response option, including “cost/efficiency” alone (15%) 6.
Narrow Network Plans
Firms with 50 or more employees offering health benefits were asked about the prevalence of narrow or skinny networks. Narrow networks are plans which limit the number of providers who can participate to reduce costs. Typically narrow network plans include fewer providers than a typical PPO or HMO network.
- Eight percent of offering firms with 200 or more workers indicated that they offered a plan they considered to be a narrow network plan 8.
- Six percent of offering firms with 200 or more employees said that the carrier (or firm) eliminated a hospital or health system from a provider network in order to reduce costs 8.
Reference Pricing
Reference pricing is a system in which plans pay a set amount for a service and the enrollee is responsible for paying the difference between the service and the cost the provider charges. Reference pricing is intended to encourage enrollees to shop among providers for lower cost and/or higher value care. The survey asked employers with 50 or more employees if their plan with the largest enrollment used reference pricing for ANY service.
- The largest health plan at 13% of offering firms with 50 or more employees includes reference pricing for at least a service 7.
Retail Clinics
Retail clinics treat minor illnesses and provide preventive care at locations such as retail stores, pharmacies, and supermarkets. Among firms offering health benefits, over half (57%) cover care received at retail clinics in their plan with the largest enrollment. Among these firms covering care at retail clinics, 8% offer financial incentives to receive care at a retail clinic location rather than at a physician’s office
9.
- Large firms (200 or more workers) are more likely than small firms to both cover care received at a retail clinic and offer financial incentives to seek care at retail locations 9.
- The percentage of firms offering health benefits whose largest plan covers care at a retail clinic and who offer financial incentives for doing so is statistically unchanged from 2013.
Private Exchanges and Defined Contributions
Recently there has been considerable interest in private exchanges. An exchange is a marketplace for health insurance. Private exchanges allow employees to choose from several health benefit options offered on the exchange. A private exchange is created by a consulting company, rather than a governmental entity. There is considerable variation in the types of exchanges currently offered; some exchanges allow workers to choose between multiple plans offered by the same carrier, while in other cases multiple carriers participate. The exchange operator may establish strict standards for the plans offered or allow the insurers more flexibility in determining their plan offerings.
Private exchanges may or may not include a defined contribution for premiums. A defined contribution is a set dollar amount offered to the employee by the employer. Employees may then select one of several plans, paying the difference between the defined contribution and the cost of their chosen health insurance plan. This permits an employer to offer a larger variety of health plans to employees and to structure contributions or other rules to encourage employees to choose more efficient plans.
- Three percent of covered workers at large firms (200 or more workers) are enrolled at a firm which is currently offering health benefits through a private exchange 12.
- Thirteen percent of large firms (200 or more workers) offering health benefits are considering offering benefits through a private exchange. Among offering firms with at least 5,000 workers, 20% are considering offering benefits through the exchange 11.
- The percentage of large firms (200 or more workers) offering health benefits that are considering offering benefits through a private exchange is unchanged from last year. The percentage of firms with at least 5,000 workers considering a private exchange is down from 29% last year.
- Currently 12% of covered workers are employed at a firm that is considering moving to a private exchange.
- Twenty-three percent of large firms (200 or more workers) offering health benefits are considering using a defined contribution approach 11.
Methodology
The Kaiser Family Foundation and the Health Research & Educational Trust (Kaiser/HRET) conduct this annual survey of employer-sponsored health benefits. HRET, a nonprofit research organization, is an affiliate of the American Hospital Association. The Kaiser Family Foundation designs, analyzes, and conducts this survey in partnership with HRET, and also funds the study. KFF contracts with researchers at NORC at the University of Chicago (NORC) to work with Foundation and HRET researchers in conducting the study. Kaiser/HRET retained National Research, LLC (NR), a Washington, D.C.-based survey research firm, to conduct telephone interviews with human resource and benefits managers using the Kaiser/HRET survey instrument. From January to May 2014, NR completed full interviews with 2,052 firms.
Survey Topics
As in past years, Kaiser/HRET asked each participating firm as many as 400 questions about its largest health maintenance organization (HMO), preferred provider organization (PPO), point-of-service (POS) plan, and high-deductible health plan with a savings option (HDHP/SO).22 We treat EPOs and HMOs as one plan type and report the information under the banner of “HMO”; if an employer sponsors both an HMO and an EPO, they are asked about the attributes of the plan with the larger enrollment. Similarly, starting in 2013, plan information for conventional (or indemnity) plans was collected within the PPO battery. Less than one percent of firms which completed the PPO section had more enrollment in a conventional plan than a PPO plan.
As in past years, the survey includes questions on the cost of health insurance, health benefit offer rates, coverage, eligibility, enrollment patterns, premiums,23 employee cost sharing, prescription drug benefits, retiree health benefits, wellness benefits, and employer opinions.
Response Rate
After determining the required sample from U.S. Census Bureau data, Kaiser/HRET drew its sample from a Survey Sampling Incorporated list (based on an original Dun and Bradstreet list) of the nation’s private employers and from the Census Bureau’s Census of Governments list of public employers with three or more workers. To increase precision, Kaiser/HRET stratified the sample by ten industry categories and six size categories. Kaiser/HRET attempted to repeat interviews with prior years’ survey respondents (with at least ten employees) who participated in either the 2012 or the 2013 survey, or both. Firms with 3-9 employees are not include in the panel to minimize the impact of panel effects on the offer rate statistic. As a result, 1,587 of the 2,052 firms that completed the full survey also participated in either the 2012 or 2013 surveys, or both.24 The overall response rate is 46%.25
The vast majority of questions are asked only of firms that offer health benefits. A total of 1,827 of the 2,052 responding firms indicated that they offered health benefits. The response rate for firms that offer health benefits is also 46%.
We asked one question of all firms in the study with which we made phone contact , but where the firm declined to participate. The question was, “Does your company offer a health insurance program as a benefit to any of your employees?” A total of 3,139 firms responded to this question (including 2,052 who responded to the full survey and 1,087 who responded to this one question). These responses are included in our estimates of the percentage of firms offering health benefits.26 The response rate for this question is 70%. In 2012 the calculation of the response rates was adjusted to be slightly more conservative than previous years.
Firm Size Categories and Key Definitions
Throughout the report, exhibits categorize data by size of firm, region, and industry. Firm size definitions are as follows: small firms: 3 to 199 workers; and large firms: 200 or more workers. Exhibit M.1 shows selected characteristics of the survey sample. A firm’s primary industry classification is determined from SSI’s designation on the sampling frame. A firm’s ownership category and other firm characteristics used in exhibits such as 3.2 and 6.19 are based on respondents’ answers. While there is considerable overlap in firms in the “State/Local Government” industry category and those in the “public” ownership category they are not identical. For example, public school districts are included in the service industry even though they are publically owned
Exhibit M.2 displays the distribution of the nation’s firms, workers, and covered workers (employees receiving coverage from their employer). Among the over three million firms nationally, approximately 61.2% are firms employing 3 to 9 workers; such firms employ 8.2% of workers, and 3.4% of workers covered by health insurance. In contrast, less than one percent of firms employ 1,000 or more workers; these firms employ 48.2% of workers and 54.6% of covered workers. Therefore, the smallest firms dominate any statistics weighted by the number of employers. For this reason, most statistics about firms are broken out by size categories. In contrast, firms with 1,000 or more workers are the most important employer group in calculating statistics regarding covered workers, since they employ the largest percentage of the nation’s workforce.
Throughout this report, we use the term “in-network” to refer to services received from a preferred provider. Family coverage is defined as health coverage for a family of four.
Each year, the survey asks firms for the percentage of their employees who earn less than a specified amount in order to identify the portion of a firm’s workforce that has relatively low wages. This year, the income threshold is $23,000 per year for low-wage workers and $57,000 for high-wage workers. These thresholds are based on the 25th and 75th percentile of workers’ earnings as reported by the Bureau of Labor Statistics using data from the Occupational Employment Statistics (OES) (2011).27 The cutoffs were inflation adjusted and rounded to the nearest thousand. Prior to 2013 wage cutoffs were calculated using the now eliminated National Compensation Survey.
Rounding and Imputation
Some exhibits in the report do not sum to totals due to rounding effects. In a few cases, numbers from distribution exhibits may not add to the numbers referenced in the text due to rounding. Although overall totals and totals for size and industry are statistically valid, some breakdowns may not be available due to limited sample sizes or a high relative standard error. Where the unweighted sample size is fewer than 30 observations, exhibits include the notation “NSD” (Not Sufficient Data).
To control for item nonresponse bias, Kaiser/HRET imputes values that are missing for most variables in the survey. On average, 3% of observations are imputed. All variables are imputed following a hotdeck approach. In 2014, there were 15 variables where the imputation rate exceeded 20%. For these cases, the unimputed variable is compared with the imputed variable. Also, most of these cases were for individual plan level statistics – when aggregate variables were constructed for all of the plans the imputation rate is much lower. There are a few variables that Kaiser/HRET has decided not to impute; these are typically variables where “don’t know” is considered a valid response option (for example, firms’ opinions about effectiveness of various strategies to control health insurance costs or whether the firm is considering private exchanges.). In addition, there are several variables in which missing data is calculated based on respondents’ answers to other questions (for example, when missing employer contributions to premiums are calculated from the respondent’s premium and the ratio of contributions to premiums).
In 2012 the method to calculate missing premiums and contributions was revised; if a firm provides a premium for single coverage or family coverage, or a worker contribution for single coverage or family coverage, that information was used in the imputation. For example, if a firm provided a worker contribution for family coverage but no premium information, a ratio between the family premium and family contribution was imputed and then the family premium was calculated. In addition, in cases where premiums or contributions for both family and single coverage were missing, the hotdeck procedure was revised to draw all four responses from a single firm. The change in the imputation method did not make a significant impact on the premium or contribution estimates.
Starting in 2014, we elected to estimate separate single and family coverage premiums for firms that provided premium amounts as the average cost for all covered workers, instead of differentiating between single and family coverage. This method will more accurately account for the portion that each type of coverage contributes to the total cost for the 1 percent of covered workers who are enrolled at firms affected by this adjustment.
Sample Design
We determined the sample requirements based on the universe of firms obtained from the U.S. Census. Prior to the 2010 survey, the sample requirements were based on the total counts provided by Survey Sampling Incorporated (SSI) (which obtains data from Dun and Bradstreet). Over the years, we found the Dun and Bradstreet frequency counts to be volatile due to duplicate listings of firms, or firms that are no longer in business. These inaccuracies vary by firm size and industry. In 2003, we began using the more consistent and accurate counts provided by the Census Bureau’s Statistics of U.S. Businesses and the Census of Governments as the basis for post-stratification, although the sample was still drawn from a Dun and Bradstreet list. In order to further address this concern at the time of sampling, starting in 2009 we use Census data as the basis for the sample.
Starting in 2010, we also defined Education as a separate sampling category, rather than as a subgroup of the Service category. In the past, Education firms were a disproportionately large share of Service firms. Education is controlled for during post-stratification, and adjusting the sampling frame to also control for Education allows for a more accurate representation of both the Education and Service industries.
In past years, both private and government firms were sampled from the Dun and Bradstreet database. Beginning in 2009, Government firms were sampled from the 2007 Census of Governments. This change was made to eliminate the overlap of state agencies that were frequently sampled from the Dun and Bradstreet database. The sample of private firms is screened for firms that are related to state/local governments, and if these firms are identified in the Census of Governments, they are reclassified as government firms and a private firm is randomly drawn to replace the reclassified firm. The federal government is not included in the sample frame.
Finally, the data used to determine the 2014 Employer Health Benefits sample frame include the U.S. Census’ 2010 Statistics of U.S. Businesses and the 2007 Census of Governments. At the time of the sample design (December 2013), these data represented the most current information on the number of public and private firms nationwide with three or more workers. As in the past, the post-stratification is based on the most up-to-date Census data available (the 2011 update to the Census of U.S. Businesses was purchased during the survey field period). This year we used the 2012 Census of Governments to post-stratify.
In 2012, the method for calculating the size of the sample was adjusted. Rather than using a combined response rate for panel and non-panel firms, separate response rates were used to calculate the number of firms to be selected in each strata. In addition, the Mining stratum was collapsed into the Agriculture and Construction industry grouping. In sum, changes to the sampling method required more firms to be included and may have reduced the response rate in order to provide more balanced power within each strata.
Weighting and Statistical Significance
Because Kaiser/HRET selects firms randomly, it is possible through the use of statistical weights to extrapolate the results to national (as well as firm size, regional, and industry) averages. These weights allow Kaiser/HRET to present findings based on the number of workers covered by health plans, the number of total workers, and the number of firms. In general, findings in dollar amounts (such as premiums, worker contributions, and cost sharing) are weighted by covered workers. Other estimates, such as the offer rate, are weighted by firms. Specific weights were created to analyze the HDHP/SO plans that are offered with an HRA or that are HSA-qualified. These weights represent the proportion of employees enrolled in each of these arrangements.
Calculation of the weights follows a common approach. First, the basic weight is determined, followed by a nonresponse adjustment. As part of this nonresponse adjustment, Kaiser/HRET conducted a small follow-up survey of those firms with 3 to 49 workers that refused to participate in the full survey. Just as in years passed, Kaiser/HRET conducted a McNemar test to verify that the results of the follow-up survey are comparable to the results from the original survey. Next, we trimmed the weights in order to reduce the influence of weight outliers. First, we identified common groups of observations. Within each group, we identified the median and the interquartile range of the weights and calculated the trimming cut point as the median plus six times the interquartile range (M + [6 * IQR]). Weight values larger than this cut point are trimmed to the cut point. In all instances, very few weight values were trimmed. Finally, we calibrated the weights to U.S. Census Bureau’s 2011 Statistics of U.S. Businesses for firms in the private sector, and the 2012 Census of Governments as the basis for calibration / post-stratification for public sector firms. Historic employer weighted statistics were updated in 2011.
Between 2006 and 2012 only limited information was collected on conventional plans. Starting in 2013, information on conventional plans was collected under the PPO section and therefore the covered worker weight was representative of all plan types.
The survey contains a few questions on employee cost sharing that are asked only of firms that indicate in a previous question that they have a certain cost-sharing provision. For example, the copayment amount for prescription drugs is asked only of those that report they have copayments for prescription drugs. Because the composite variables (using data from across all plan types) are reflective of only those plans with the provision, separate weights for the relevant variables were created in order to account for the fact that not all covered workers have such provisions.
To account for design effects, the statistical computing package R and the library package “survey” were used to calculate standard errors.28 ,29 All statistical tests are performed at the .05 confidence level, unless otherwise noted. For figures with multiple years, statistical tests are conducted for each year against the previous year shown, unless otherwise noted. No statistical tests are conducted for years prior to 1999. In 2012 the method to test the difference between distributions across years was changed to use a Wald test which accounts for the complex survey design. In general this method was more conservative than the approach used in prior years. Exhibits such as 7.9, 7.10, 7.16 etc. are affected by the change.
Statistical tests for a given subgroup (firms with 25-49 workers, for instance) are tested against all other firm sizes not included in that subgroup (all firm sizes NOT including firms with 25-49 workers, in this example). Tests are done similarly for region and industry; for example, Northeast is compared to all firms NOT in the Northeast (an aggregate of firms in the Midwest, South, and West). However, statistical tests for estimates compared across plan types (for example, average premiums in PPOs) are tested against the “All Plans” estimate. In some cases, we also test plan-specific estimates against similar estimates for other plan types (for example, single and family premiums for HDHP/SOs against single and family premiums for HMO, PPO, and POS plans); these are noted specifically in the text. The two types of statistical tests performed are the t-test and the Wald test.
The small number of observations for some variables resulted in large variability around the point estimates. These observations sometimes carry large weights, primarily for small firms. The reader should be cautioned that these influential weights may result in large movements in point estimates from year to year; however, often these movements are not statistically significant.
Additional Notes on the 2014 Survey
Several provisions of the ACA took effect on January 1, 2014 which impacted non-grandfathered plans as well as plans renewing in calendar year 2014, such as the requirement to have an out of pocket limit and a waiting period of not more than three months. As a result, firms with non-grandfathered plans that reported that they did not have out-of-pocket limits, or waiting periods exceeding three months, were contacted during our data-confirmation calls. We did not have information on the month in which a firm’s plan or plans was renewed. Many of these firms indicated that they had a plan year starting prior to January 2014, so these ACA provision were not yet in effect for these plans.
Firms with 200 or more workers were asked: “Does your firm offer health benefits for current employees through a private or corporate exchange? A private exchange is one created by a consulting firm or an insurance company, not by either a federal or state government. Private exchanges allow employees to choose from several health benefit options offered on the exchange.” Employers were still asked for plan information about their HMO, PPO, POS and HDHP/SO plan regardless of whether they purchased health benefits through a private exchange or not.
Historical Data
Data in this report focus primarily on findings from surveys jointly authored by the Kaiser Family Foundation and the Health Research & Educational Trust, which have been conducted since 1999. Prior to 1999, the survey was conducted by the Health Insurance Association of America (HIAA) and KPMG using a similar survey instrument, but data are not available for all the intervening years. Following the survey’s introduction in 1987, the HIAA conducted the survey through 1990, but some data are not available for analysis. KPMG conducted the survey from 1991-1998. However, in 1991, 1992, 1994, and 1997, only larger firms were sampled. In 1993, 1995, 1996, and 1998, KPMG interviewed both large and small firms. In 1998, KPMG divested itself of its Compensation and Benefits Practice, and part of that divestiture included donating the annual survey of health benefits to HRET.
This report uses historical data from the 1993, 1996, and 1998 KPMG Surveys of Employer-Sponsored Health Benefits and the 1999-2013 Kaiser/HRET Survey of Employer-Sponsored Health Benefits. For a longer-term perspective, we also use the 1988 survey of the nation’s employers conducted by the HIAA, on which the KPMG and Kaiser/HRET surveys are based. The survey designs for the three surveys are similar.
Endnotes
- Kaiser Commission on Medicaid and the Uninsured. The uninsured: a primer—key facts about health insurance on the eve of coverage expansions [Internet]. Washington (DC): The Commission; 2013 Oct 23 [cited 2014 Aug 5]. Available from: https://modern.kff.org/uninsured/report/the-uninsured-a-primer-key-facts-about-health-insurance-on-the-eve-of-coverage-expansions/ ↩︎
- Kaiser/HRET surveys use the April-to-April time period, as do the sources in this and the following note. The inflation numbers are not seasonally adjusted. Bureau of Labor Statistics. Consumer Price Index – All Urban Consumers [Internet]. Washington (DC): Department of Labor; 2014 [cited 2014 June 6]. Available from: http://data.bls.gov/timeseries/CUUR0000SA0?output_view=pct_1mth. Wage data are from the Bureau of Labor Statistics and based on the change in total average hourly earnings of production and nonsupervisory employees. Employment, hours, and earnings from the Current Employment Statistics survey [Internet]. Washington (DC): Department of Labor; 2014 [cited 2014 June 6]. Available from: http://data.bls.gov/timeseries/CES0500000008 ↩︎
- Federal Register. Vol. 75, No 221, November 17, 2010, http://www.gpo.gov/fdsys/pkg/FR-2010-11-17/pdf/2010-28861.pdf. ↩︎
- Because surveys only collect information from a portion of the total number of firms in the country there is uncertainty in any estimate. Since there are so many small firms, sometimes even seemingly large differences are not statistically different. For more information on the Employer Health Benefits Survey’s weighting and design please see the methods section. ↩︎
- A full-time equivalent accounts for one employee working thirty hours or more a week, therefore two employees working half a full workload account for one FTE. ↩︎
- Kaiser Family Foundation, Kaiser Commission on Medicaid and the Uninsured, The Uninsured: A Primer: Key Facts About Americans Without Health Insurance, October 2013. https://modern.kff.org/uninsured/report/the-uninsured-a-primer-key-facts-about-health-insurance-on-the-eve-of-coverage-expansions/. 56% of the non-elderly American population receives insurance coverage through an employer-sponsored plan. ↩︎
- In 2009, Kaiser/HRET began weighting the percentage of workers that take up coverage by the number of workers eligible for coverage. The historical take up estimates have also been updated. See the Survey Design and Methods section for more information. ↩︎
- Starting in 2010 we included firms that said they offer a plan type even if there are no covered workers in that plan type. ↩︎
- Estimates for premiums, worker contributions to premiums, and employer contributions to premiums presented in Section 6 do not include contributions made by the employer to Health Savings Accounts (HSAs) or Health Reimbursement Arrangements (HRAs). See Section 8 for estimates of employer contributions to HSAs and HRAs. ↩︎
- For definitions of Self-Funded and Fully Insured plans, see the introduction to Section 10. ↩︎
- This estimate has a relative standard error of 15%. ↩︎
- Some workers with separate per-person deductibles or out-of-pocket maximums for family coverage do not have a specific number of family members that are required to meet the deductible amount and instead have another type of limit, such as a per-person amount with a total dollar amount limit. These responses are included in the averages and distributions for separate family deductibles and out-of-pocket maximums. ↩︎
- Starting in 2010, the survey asked about the prevalence and cost of physician office visits separately for primary care and specialty care. Prior to the 2010 survey if the respondent indicated the plan had a copayment for office visits, we assumed the plan had a copayment for both primary and specialty care visits. The survey did not allow for a respondent to report that a plan had a copayment for primary care visits and coinsurance for visits with a specialist physician. The changes made in 2010 allow for variations in the type of cost sharing for primary care and specialty care. This year the survey includes cost sharing for in-network services only. See the 2007 survey for information on out-of-network office visit cost sharing. ↩︎
- There is no legal requirement for the minimum deductible in a plan offered with an HRA. The survey defines a high-deductible HRA plan as a plan with a deductible of at least $1,000 for single coverage and $2,000 for family coverage. Federal law requires a deductible of at least $1,250 for single coverage and $2,500 for family coverage for HSA-qualified HDHPs in 2014. See the Text Box for more information on HDHP/HRAs and HSA-qualified HDHPs. ↩︎
- The definitions of HDHP/SOs do not include other consumer-driven plan options, such as arrangements that combine an HRA with a lower-deductible health plan or arrangements in which an insurer (rather than the employer as in the case of HRAs or the enrollee as in the case of HSAs) establishes an account for each enrollee. Other arrangements may be included in future surveys as the market evolves. ↩︎
- The average out-of-pocket maximum for HDHP/HRAs is calculated for plans with an out-of-pocket maximum. About 3% of covered workers in HDHP/HRAs with single coverage or family coverage are in plans that reported having no limit on out-of-pocket expenses. ↩︎
- In the survey, we ask, “Up to what dollar amount does your firm promise to contribute each year to an employee’s HRA or health reimbursement arrangement for single coverage?” We refer to the amount that the employer commits to make available to an HRA as a contribution for ease of discussion. As discussed, HRAs are notional accounts, and employers are not required to actually transfer funds until an employee incurs expenses. Thus, employers may not expend the entire amount that they commit to make available to their employees through an HRA. Some employers may make their HRA contribution contingent on other factors, such as completing wellness programs. ↩︎
- The survey asks firms offering at least one wellness program if most of the wellness benefits are provided by the health plan or by the firm. ↩︎
- Firms that offer only web-based resources or a wellness newsletter were not asked questions about any financial incentives provided. ↩︎
- Federal Register. Vol. 75, No. 116, June 17, 2010, http://www.gpo.gov/fdsys/pkg/FR-2010-06-17/pdf/2010-14614.pdf, and No. 221, Nov. 17, 2010, http://edocket.access.gpo.gov/2010/pdf/2010-28861.pdf. ↩︎
- United States. Congressional Research Service CRS. Open CRS. By Bernadette Fernandez. Grandfathered Health Plans Under the Patient Protection and Affordable Care Act (PPACA), Jan. 3, 2011. http://assets.opencrs.com/rpts/R41166_20110103.pdf. ↩︎
- HDHP/SO includes high-deductible health plans offered with either a Health Reimbursement Arrangement (HRA) or a Health Savings Account (HSA). Although HRAs can be offered along with a health plan that is not an HDHP, the survey collected information only on HRAs that are offered along with HDHPs. For specific definitions of HDHPs, HRAs, and HSAs, see the introduction to Section 8. ↩︎
- HDHP/SO premium estimates do not include contributions made by the employer to Health Savings Accounts or Health Reimbursement Arrangements. ↩︎
- In total, 175 firms participated in 2012, 291 firms participated in 2013 and, and 1,121 firms participated in 2012, and 2013. ↩︎
- Response rate estimates are calculated by dividing the number of completes over the number of refusals and the fraction of the firms with unknown eligibility to participate estimated to be eligible. Firms determined to be ineligible to complete the survey are not included in the response rate calculation. ↩︎
- Estimates presented in Exhibits 2.1, 2.2 and 2.3 are based on the sample of both firms that completed the entire survey and those that answered just one question about whether they offer health benefits. ↩︎
- General information on the OES can be found at : http://www.bls.gov/oes/oes_emp.htm#scope. A comparison between the OES and the NCS is available at: http://www.bls.gov/oes/oes_ques.htm ↩︎
- Analysis of the 2011 survey data using both R and SUDAAN (the statistical package used prior to 2012) produced the same estimates and standard errors. Research Triangle Institute (2008). SUDAAN Software for the Statistical Analysis of Correlated Data, Release 10.0, Research Triangle Park, NC: Research Triangle Institute. ↩︎
- A supplement with standard errors for select estimates can be found online at Technical Supplement: Standard Error Tables for Selected Estimates, http://modern.kff.org/insurance/8345.cfm. ↩︎
