Women, Work, and Family During COVID-19: Findings from the KFF Women’s Health Survey
Findings
Key Takeaways
- One in ten women report quitting a job due to a pandemic related reason and almost half said that one of the reasons was because they felt unsafe at their workplace.
- School closures had a substantial effect on working mothers’ ability to fulfill work obligations. One in ten working mothers with children under 18 said they quit a job due to COVID and half of this group cited school closures as one of the reasons. Three out of ten working mothers said they had to take time off because school or daycare was closed.
- In addition to juggling new, increased home and work responsibilities, many women went without pay due to school closures. Almost half (47%) of working mothers said they took unpaid sick leave because their child’s school or daycare was closed. This rose to 65% among low-income mothers and 70% among those working part-time jobs.
- Family caregiving responsibilities before and after the pandemic have largely fallen on women. More than one in ten women report they were caring for a family member who needed special assistance prior to the pandemic. Over one in ten women report that they have new caregiving responsibilities as a result of the pandemic.
- Over half of mothers with school age children said that the stress and worry of the pandemic has affected their mental health, with one in five characterizing the impact as “major.” However, only 16% of mothers have sought mental health care. Given that the mental health effects are likely to persist for a long time, access to mental health care will be an important issue to watch, particularly for mothers.
Introduction
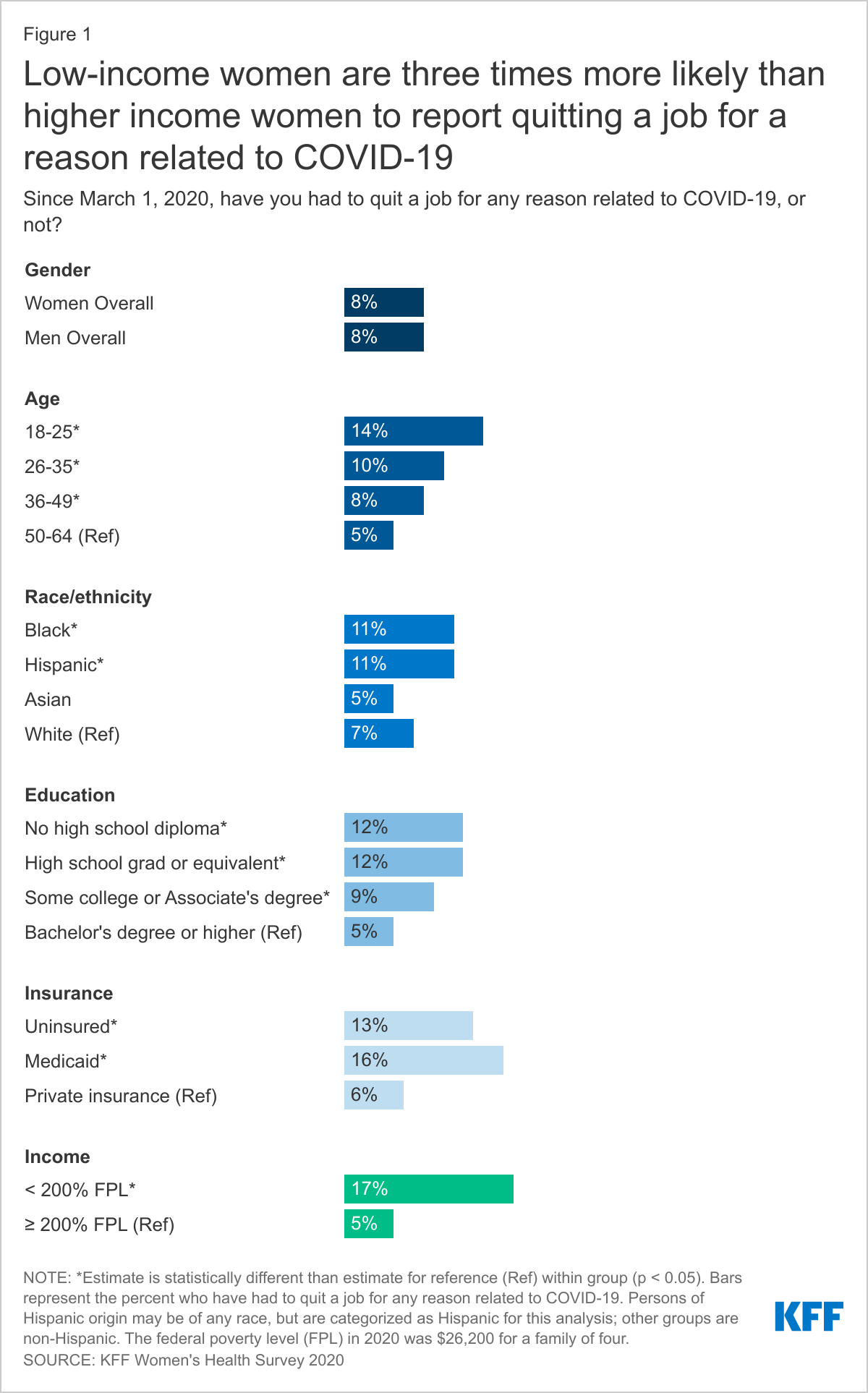
While the COVID-19 pandemic has impacted people across the US, changing the way we work, live, and access health care, gender-based disparities that existed prior to the pandemic have been magnified. Many women have been on the front lines of the COVID-19 emergency, as essential workers, mothers, and caregivers. Lack of paid leave, family caregiving responsibilities, traditional gender roles, and health concerns have placed many of the burdens of the pandemic squarely on the shoulders of women, falling particularly hard on women of color and those who are low-income. This brief provides new data from the KFF Women’s Health Survey, a nationally representative survey of 3,661 women and 1,144 men ages 18-64 (Methodology) conducted November 19, 2020 – December 17, 2020. Among several topics related to women’s health and well-being, we asked respondents about experiences during the COVID-19 pandemic. In this brief, we highlight how experiences during the COVID-19 pandemic related to work, childcare, and caregiving differ by gender and among different subpopulations of women.Nearly 1 in 10 women (8%) report quitting their job for a reason related to COVID-19. Larger shares are younger, Black or Hispanic,1 uninsured, low-income, and have less than a Bachelor’s degree (Figure 1). For example, 17% of low-income women had to quit a job for a COVID-related reason, compared to 5% with higher incomes.
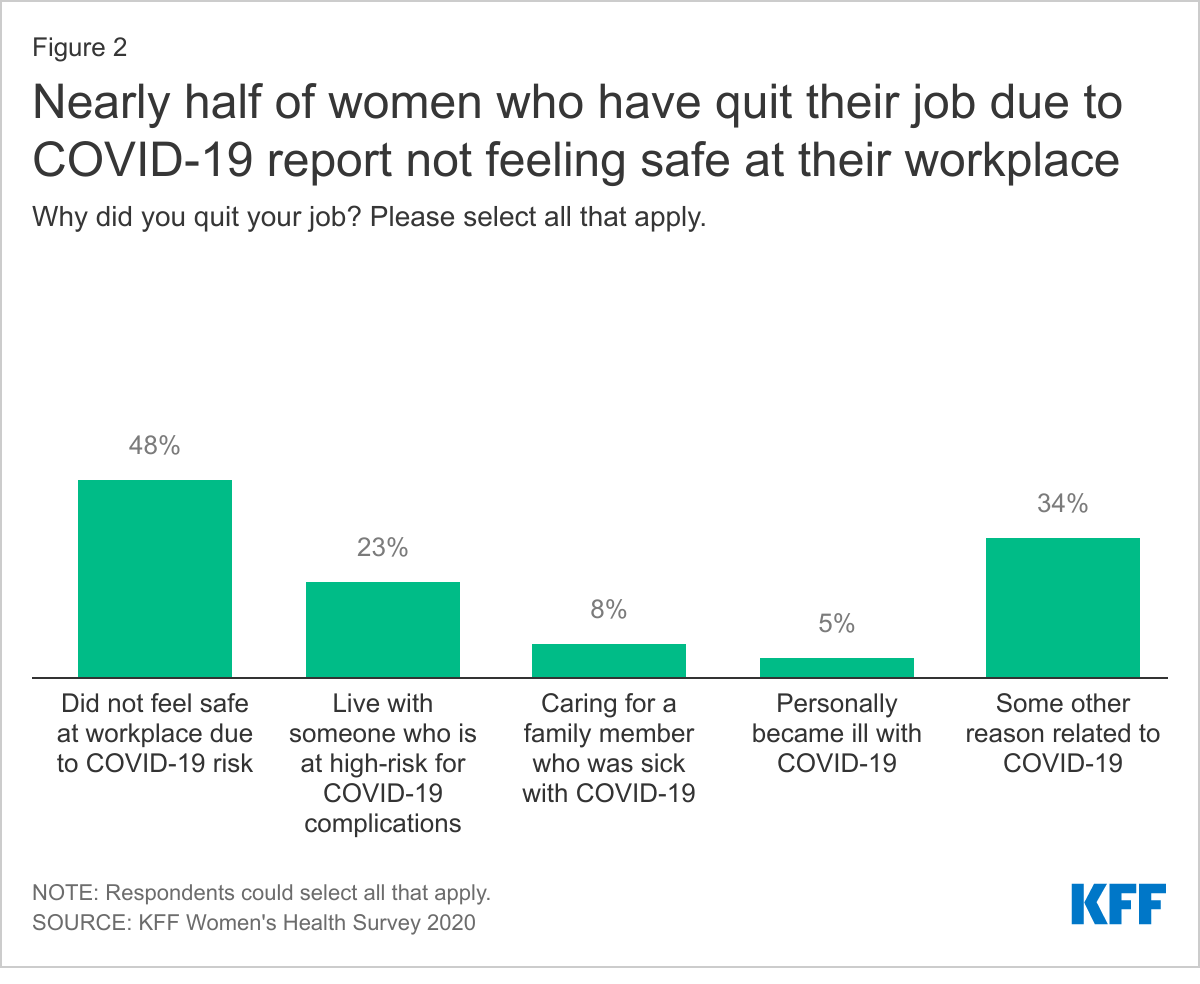
Almost half of women who have quit a job for a reason related to COVID-19 (48%) say they quit because they did not feel safe at their workplace. Three in ten women (30%) quit their job due to COVID-19 because their child’s school or daycare was closed (Figure 2). A larger share of women with Medicaid compared to women with private insurance (44% vs. 20%) and a larger share of low-income women compared to women with incomes ≥ 200% of the federal poverty level (FPL)2 (37% vs. 23%) say they had to quit their job because their child’s school or daycare was closed, leaving the most disadvantaged with a loss of income. Nearly a quarter of women say they quit a job because they live with someone at elevated risk for COVID-19 complications.
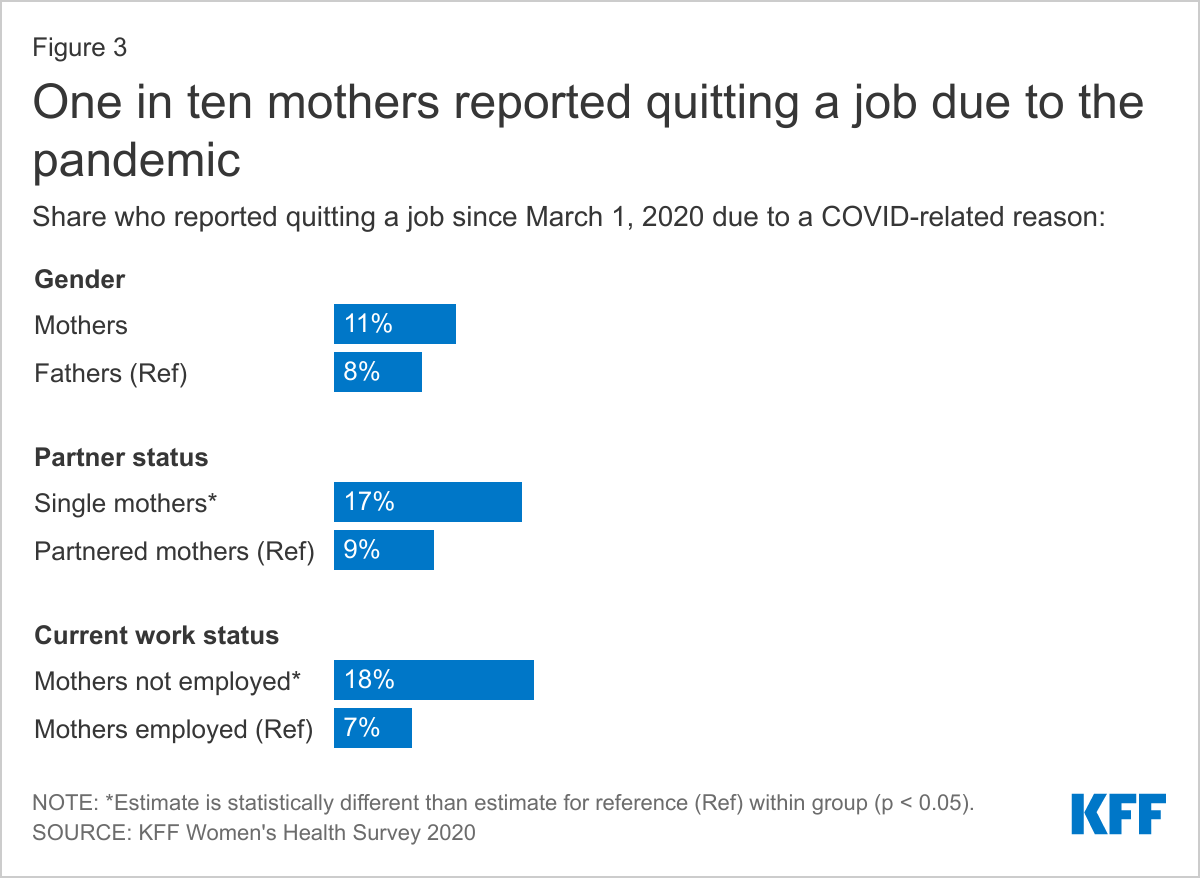
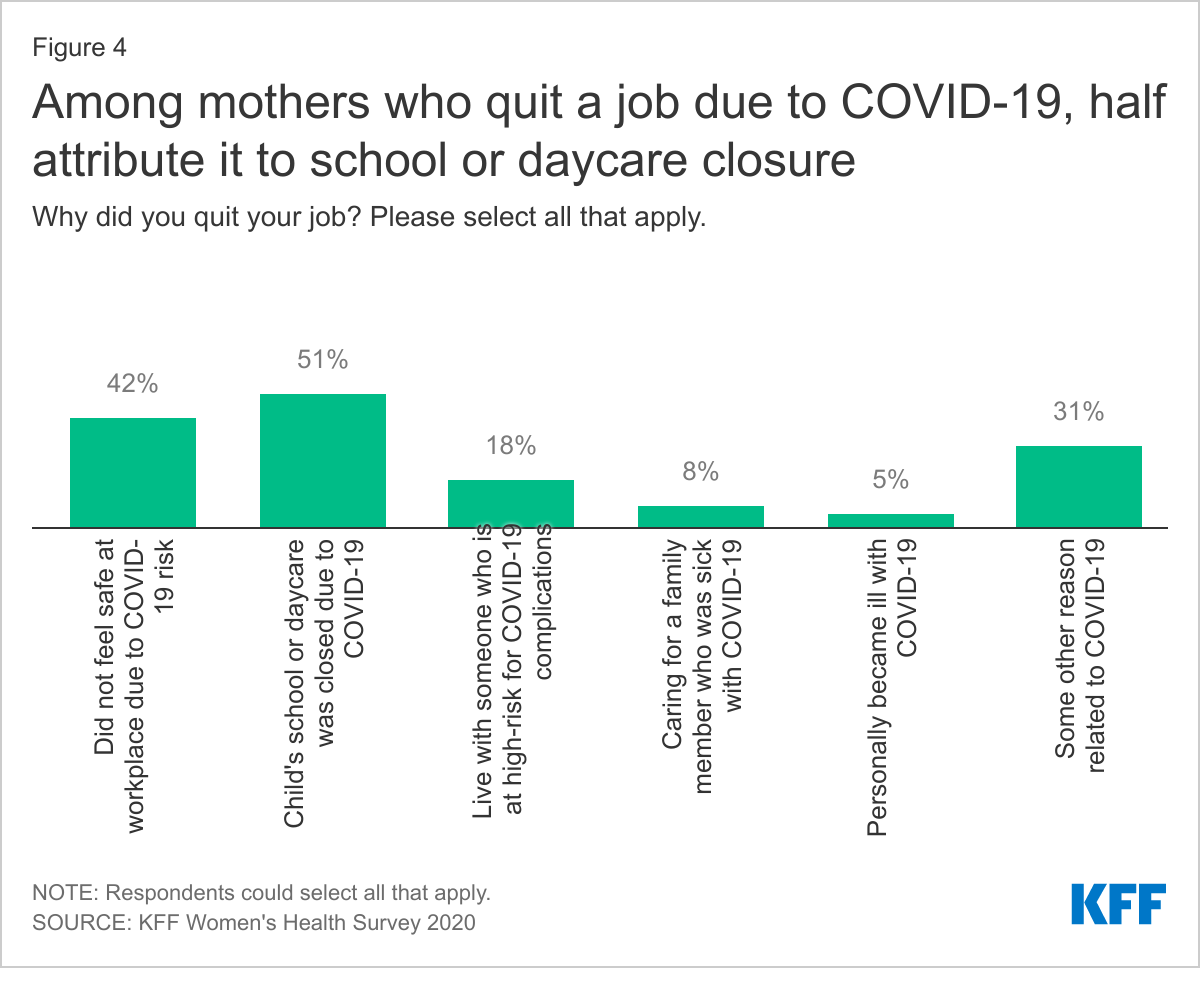
Half of mothers who quit a job because of the pandemic said one of the reasons was because their child’s school or daycare was closed. With in-person schools closed, mothers have taken on many new responsibilities, including even more childcare than usual, assisting with remote learning, and in some cases shifting to full homeschooling just to name a few. For mothers of young children who also work outside the home, they have been doing all of this while trying to maintain employment. While most mothers have been able to maintain their jobs, some with changes to their workload and schedules, it is not surprising that some have had to leave jobs as a result of school and daycare closures and the numerous new responsibilities that mothers now carry. One in ten women with young children (11%) say they quit a job due to the pandemic (Figure 3). Among this group, half (51%) said one of the reasons was because their child’s school or daycare was closed. Many mothers (42%) also said they quit because they did not feel safe at their workplace (Figure 4).
The share of women who report leaving a job is significantly higher among single mothers (17%) compared to those who are married or have partners (9%). Single mothers may face the double jeopardy of not having a partner to assist with childcare or another source of income, however. Almost one in five mothers who are not currently working (18%) report that they had to quit a job due to the pandemic, as do 7% of working mothers, suggesting that some mothers who had to quit a job during the pandemic have since found another one.
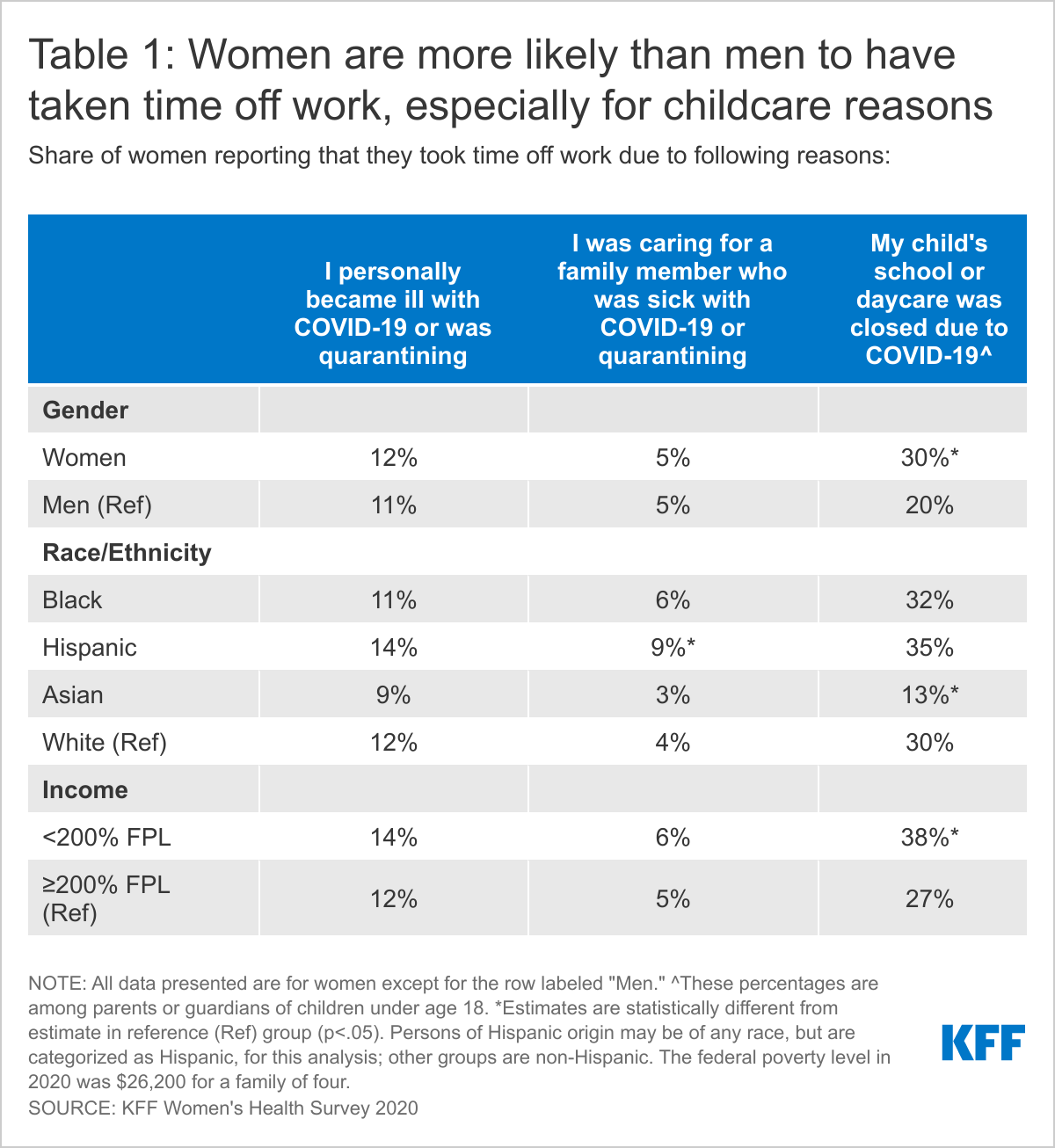
Mothers were more likely than fathers to miss work due to school and daycare closures. Many workers had to take time off due to the COVID pandemic, due to illness as well as school and daycare closures. The largest difference between women and men having to take time off work was because of school or daycare closure due to COVID-19 – this burden fell largely on women with school age children (30% vs. 20%) (Table 1). Low-income women were disproportionately affected, with almost four in ten (38%) taking time off because their child’s school or daycare was closed compared to 27% of women with incomes ≥200% FPL. Rates were similar among mothers of different racial and ethnic groups, except for Asian women, who were less likely to have taken time off because of school and daycare.
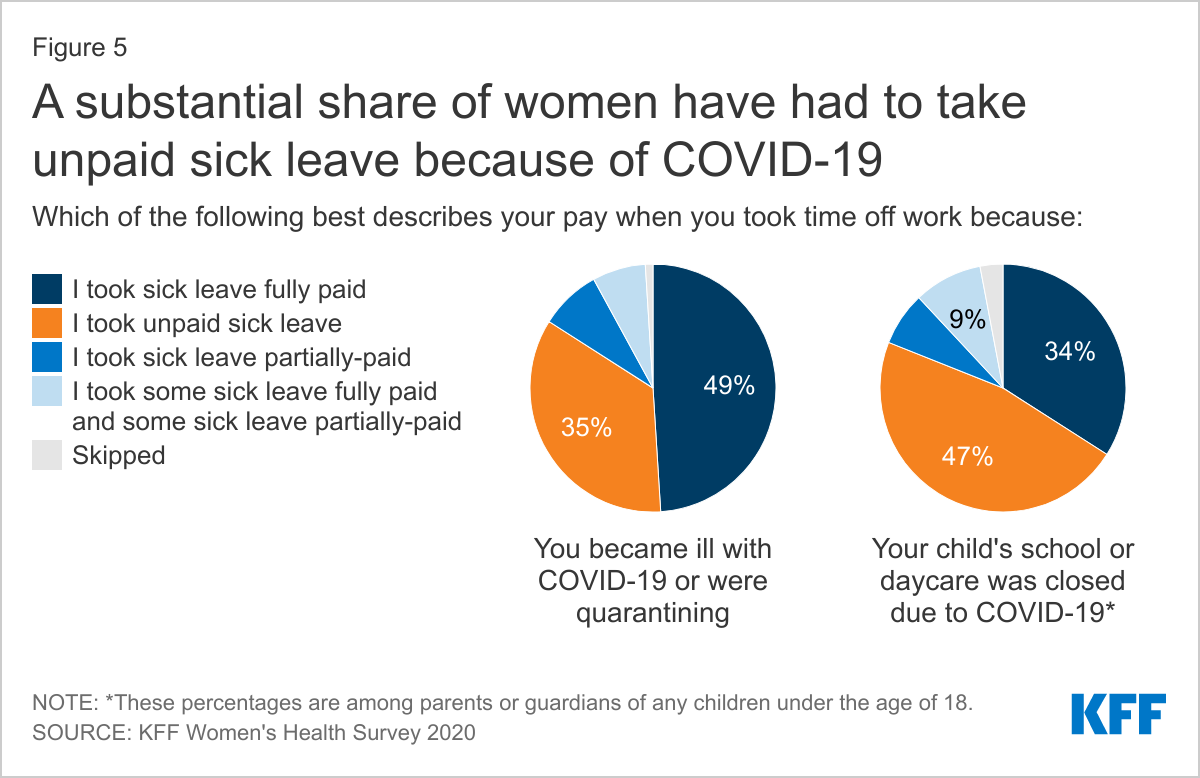
In addition to bearing the brunt of childcare and caregiving responsibilities, many women lost pay during the pandemic because they missed work due to quarantining or school closures. Over one-third of women (35%) say they took unpaid sick leave when they became ill with COVID-19 or were quarantining, and nearly half of women (46%) say they took unpaid sick leave when their child’s school or daycare was closed due to COVID-19 (Figure 5). Most employers offer some amount of paid sick leave and the federal government provided support for emergency paid sick leave to some employers in 2020, but these benefits were not available to all workers and are time limited. Many women may not have been eligible for paid sick leave or may have taken more time off than available for pay at their workplace.
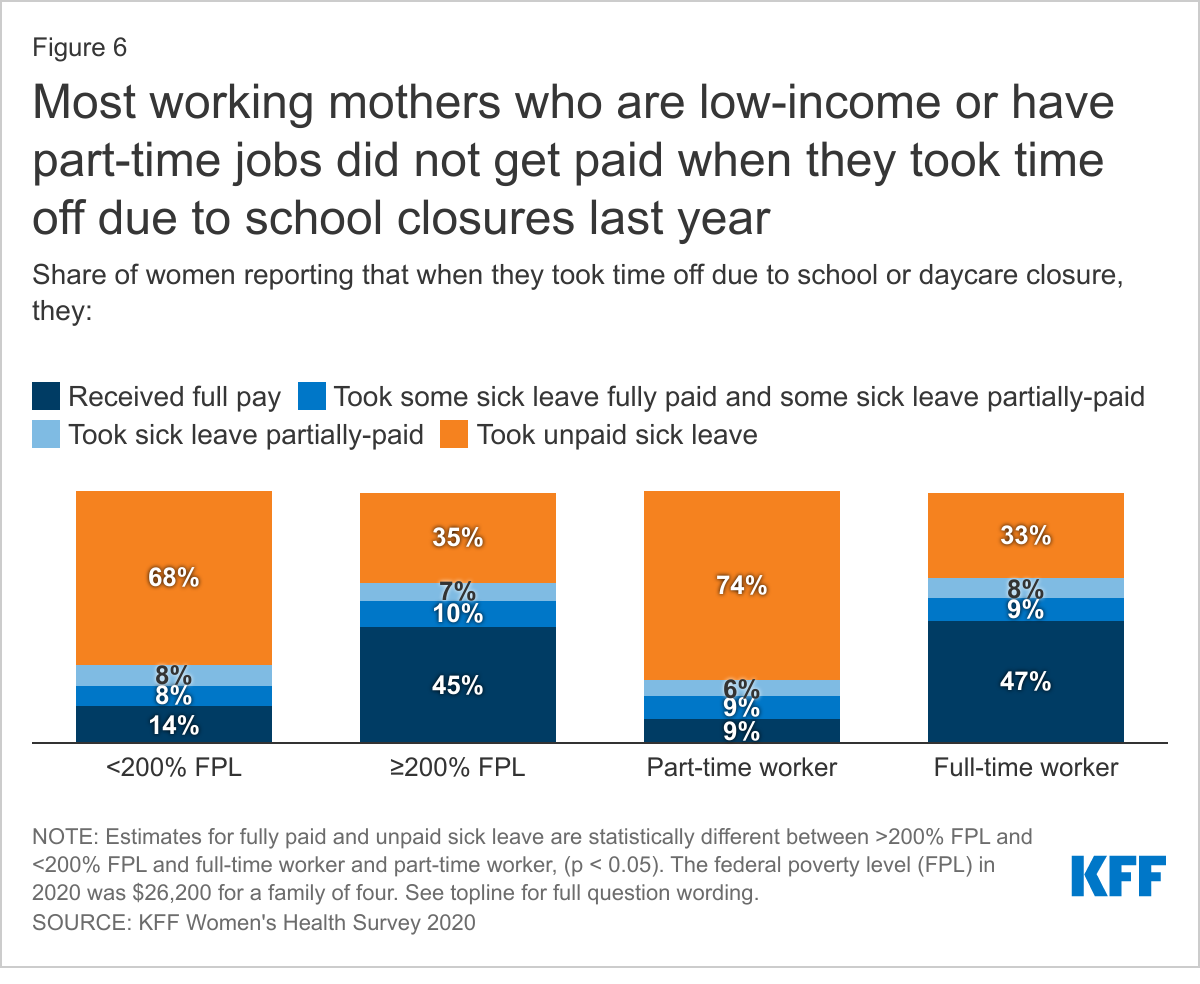
Over two-thirds of working mothers who were low-income and nearly three in four working part-time jobs were not paid when they had to take time off because their child’s school or daycare was closed due to the pandemic. Lack of a national paid leave policy disproportionately affects women, who are more likely than men to have to take time off work for childcare reasons, and some women are particularly affected. Part-time and low-wage jobs are less likely to offer paid leave benefits, as reflected in our survey. Most women in these jobs went without pay when they took time off due to school and daycare closures last year (Figure 6).
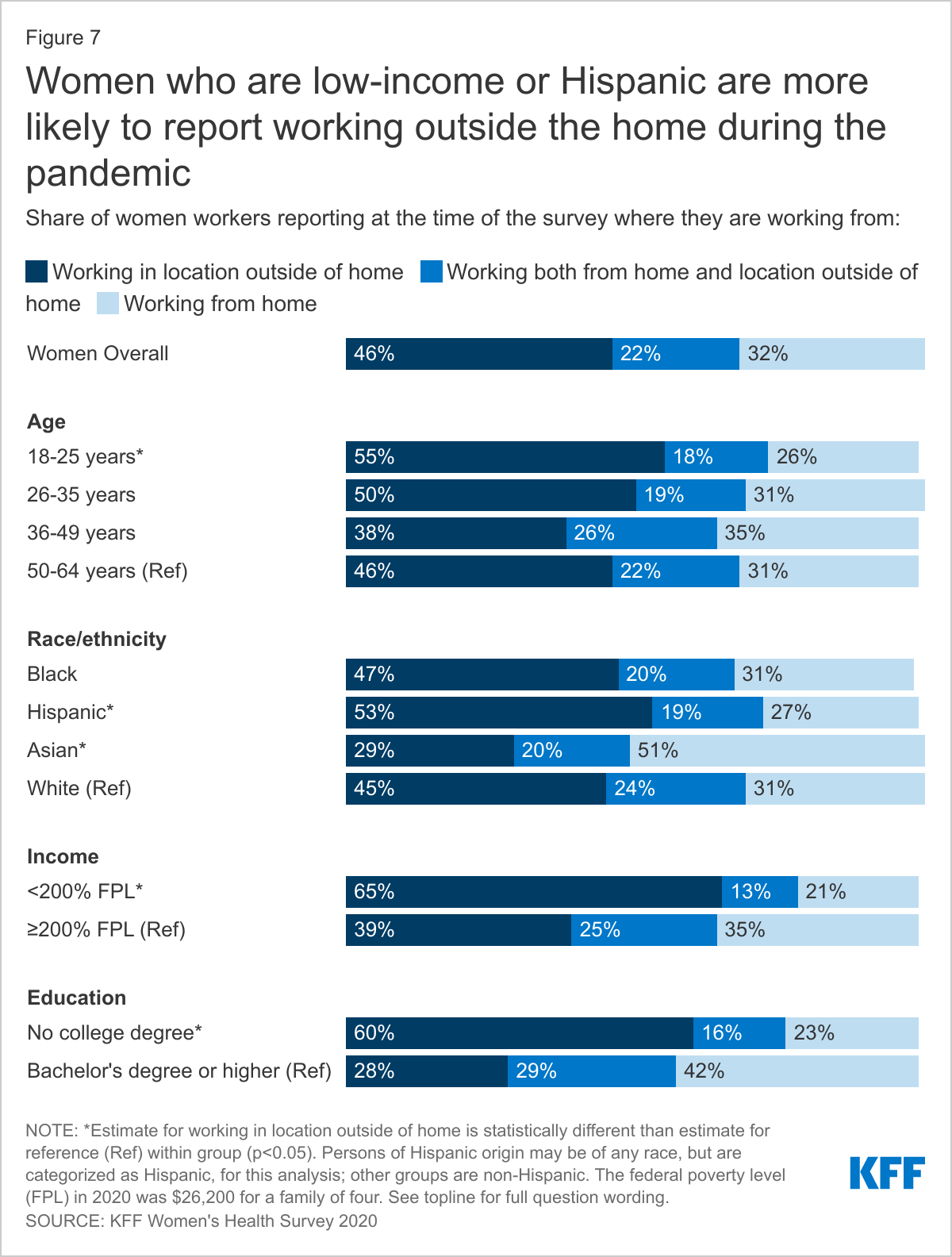
Nearly half of employed women have worked outside their home during the pandemic. More than half of men (53%) and nearly half of women (46%) report that they are working in a location outside their home during the pandemic. At the outset of the pandemic, some companies shifted to telecommuting, but many workers do not have this option as some industries and jobs are not amenable to remote work. Working outside of the home during the pandemic is more common among women who are younger, have lower educational attainment, live in rural areas, and report lower incomes. For example, more than half of Hispanic women (53%) compared to 45% of White women, have worked outside their home. Conversely, half of Asian women workers (51%) say they are working from home (Figure 7). More than half of women residing in rural areas (58%) report working outside the home, compared to 44% of women in urban communities.
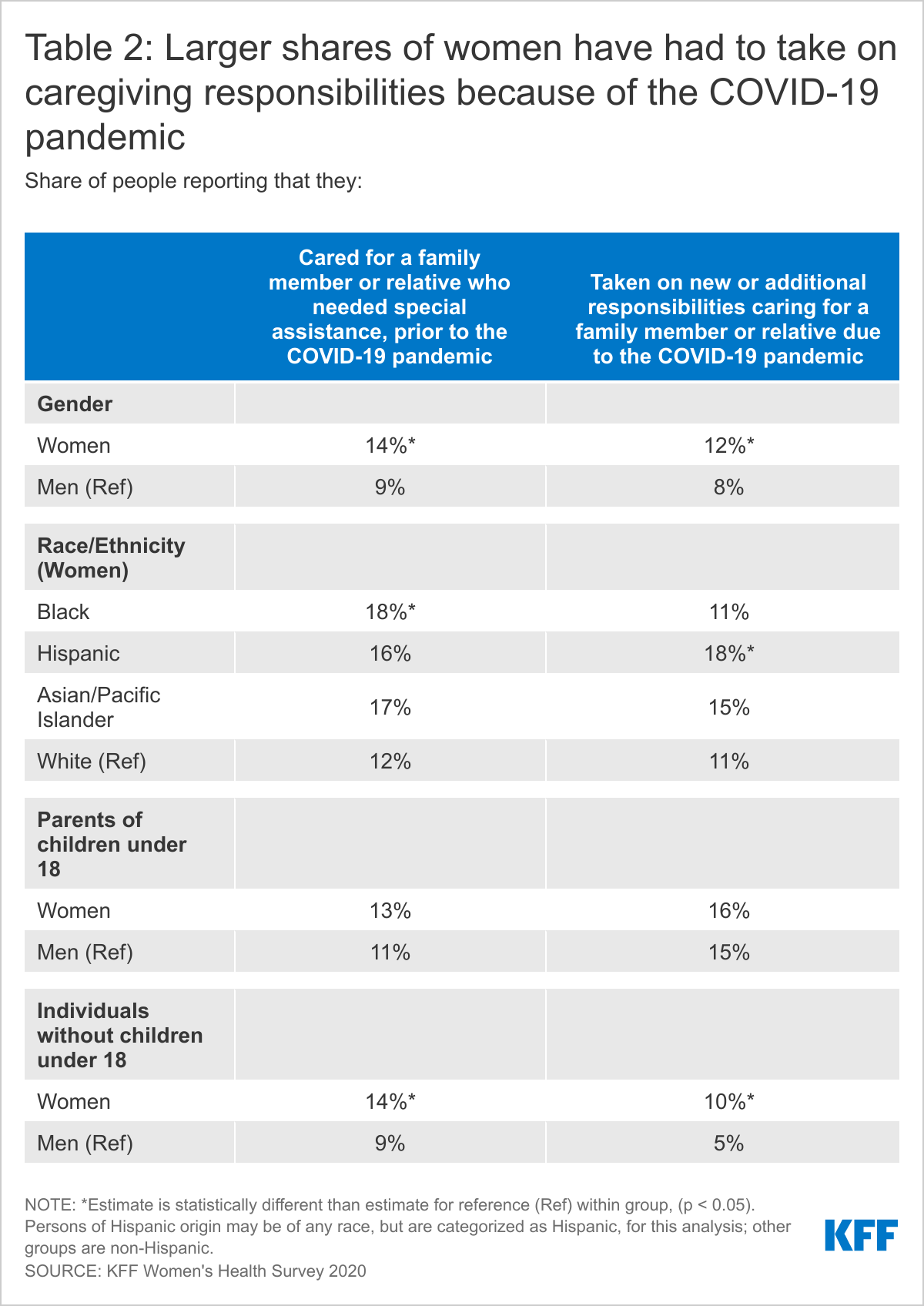
Family caregiving responsibilities before and after the pandemic have largely fallen on women. More than one in ten women report they were caring for a family member who needed special assistance prior to the pandemic. Over one in ten women report that they have new caregiving responsibilities as a result of the pandemic. A higher share of women (14%) than men (9%) say they were caring for a family member who needed special assistance prior to the pandemic. This gender difference in caregiving extends to new caregiving responsibilities due to reasons related to the pandemic (12% of women vs. 8% of men) (Table 2).
One in five women ages 50-64 say they were caring for a family member who needs special assistance prior to the pandemic, higher than women in their reproductive years (11%), but similar shares (12%) in both age groups report taking on new caregiving responsibilities as a result of the pandemic.
Women who are parents of a child younger than age 18 in their household are significantly more likely than women without children under 18 to have taken on new or additional responsibilities caring for a family member because of the pandemic (16% vs. 10%). The pattern is similar among men, with 15% of men with children under age 18 reporting they have taken on new caregiving due to the pandemic, compared to 5% of men without children. However, it is worth noting that some respondents, especially parents of young children, may have interpreted new and additional responsibilities caring for a family member or relative as homeschooling. Almost one in five low-income women (19%) were caregivers before the pandemic compared to 13% of higher-income women. Low-income women (15%) are also more likely than higher-income women (11%) to have gained new caregiving responsibilities as a result of the pandemic.
Family caregiving falls heavily on some women of color too. Almost one in five Black women (18%) report caring for someone who needed special assistance prior to the pandemic, significantly higher than the 12% of White women. Eighteen percent of Hispanic women say they have had to take on new caregiving responsibilities since the pandemic started. Nearly one in ten Hispanic women workers (9%) say they have had to take time off work because they were caring for a family member quarantining from or sick with COVID-19.
For some caregivers, the pandemic compounded existing responsibilities. Among women and men who were already caring for someone with special needs prior to March 1, 2020, many said they gained additional caregiving responsibilities as a result of the pandemic (44% and 37% respectively).
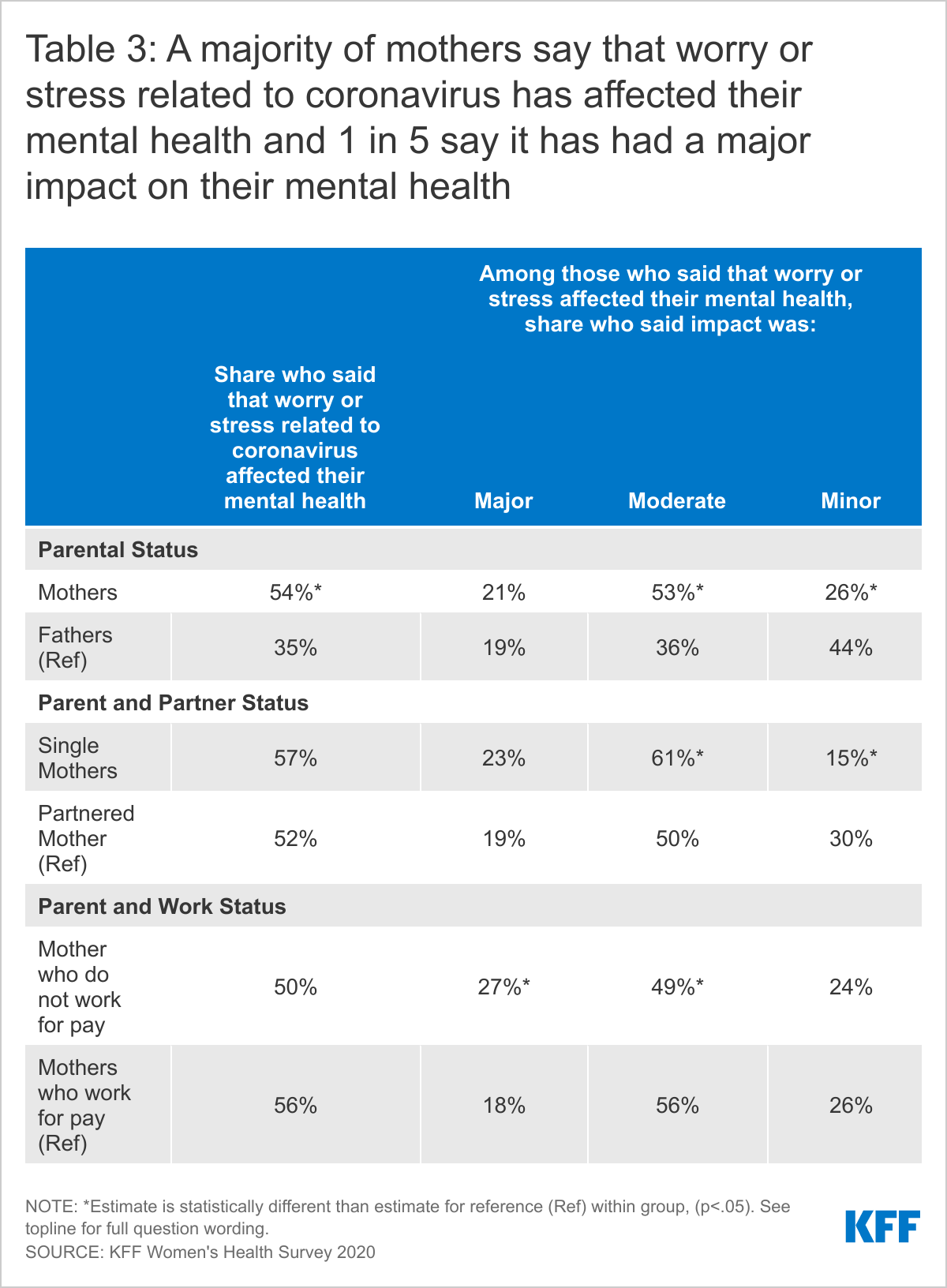
Most mothers report the pandemic has taken a toll on their mental health. A majority of mothers of children under 18 (54%) say that worry or stress related to coronavirus has affected their mental health, significantly higher than men with children under 18 (35%) (Table 3). Three in four mothers characterize the impact as major or moderate, as do 55% of fathers. More than half of mothers who are employed (56%) say that pandemic-related stress and worry have affected their mental health, as do 50% of those who are not working. However, only 16% of mothers with children under 18 have sought mental health care, with a significant difference between those who are single (21%) and partnered (14%).
Conclusion
The COVID-19 pandemic has had a disproportionate impact on women in a number of ways. While many have had to put themselves and their families at risk to work on the frontlines as essential workers, a number of women have also had to take on new homeschooling and caregiving responsibilities that have placed additional burdens on their work or resulted in their leaving the workforce entirely. Disparities that existed prior to the pandemic have been magnified and a larger share of women of color and those who are low-income have had to quit their jobs, as well as take on additional caregiving responsibilities. As the nation begins to turn a corner on the pandemic, more schools are re-opening but many remain closed or with limited hours, still placing additional childcare burdens on parents and limiting the ability of many mothers to work at the same level as pre-pandemic. Furthermore, as more businesses reopen, women’s roles in the workplace will not necessarily be restored at the same pace. Some still have additional childcare responsibilities, some may be handling COVID-related illnesses for themselves or family members as well as the major mental health toll on women and their families. Some jobs may not be available anymore, some women had to scale back their workload and lost income, and many women will have missed out on career advancement opportunities. Policies such as paid leave and the child tax credit in the newly enacted federal stimulus bill can support women in caring for their families, obtaining needed health care and balancing work and family responsibilities in this unprecedented time.
Methodology
The 2020 KFF Women’s Health Survey was designed and analyzed by researchers at the Kaiser Family Foundation (KFF) of a representative sample of 4,805 adults, ages 18-64 years old (3,661 women and 1,144 men). The survey was conducted online and telephone using AmeriSpeak®, the probability-based panel of NORC at the University of Chicago. U.S. households are recruited for participation using address-based sampling methodology and initial invitations for participation are sent by mail, telephone, and in-person interviews. Interviews for this survey were conducted between November 19 and December 17, 2020, among adults living in the United States. KFF paid for all costs associated with the survey.
The sample for this study was stratified by age, race/ethnicity, education, and gender as well as disproportionate stratification aimed at reaching uninsured women, women who identify as LGBT, and women 18-49 years old. The sampling also took into consideration differential survey completion rates by demographic groups so that the set of panel members with a completed interview for a study is a representative sample of the target population. Interviews were conducted in English and Spanish online (4,636) and via the telephone (169).
A series of data quality checks were run and cases determined to be poor-quality, as defined by surveys with a length of interview of less than 33% of the mean length of interview and with high levels of question refusal (>50%) were removed from the final data (n=96). Weighting involved multiple stages. First, the sample was weighted to match estimates for the national population from the 2020 Current Population Survey on age, gender, census division, race/ethnicity, and education. The second round of weights adjusted for the study’s sampling design. All statistical tests of significance account for the effect of weighting.
The margin of sampling error including the design effect for the full sample of women is plus or minus 2 percentage points. Numbers of respondents and margins of sampling error for key subgroups are shown in the table below. For results based on other subgroups, the margin of sampling error may be higher. Sample sizes and margins of sampling error for other subgroups are available by request. Note that sampling error is only one of many potential sources of error in this or any other public opinion poll.
| Group | N (unweighted) | M.O.S.E |
| Men Ages 18-64 | 1,144 | +/- 4 percentage points |
| Women Ages 18-64 | 3,661 | +/- 2 percentage points |
| Women Ages 18-49 | 2,695 | +/- 2 percentage points |
| White Women Ages 18-64 | 1,813 | +/- 3 percentage points |
| Black Women Ages 18-64 | 603 | +/- 5 percentage points |
| Hispanic Women Ages 18-64 | 801 | +/- 5 percentage points |
| Asian Women Ages 18-64 | 246 | +/- 8 percentage points |
| LGB Women Ages 18-64 | 392 | +/- 7 percentage points |
| Heterosexual Women Ages 18-64 | 3,239 | +/- 2 percentage points |
| Women < 200% FPL | 1,471 | +/- 3 percentage points |
| Women ≥200% FPL | 1,943 | +/- 3 percentage points |