SCOTUS Ruling on Medina v. Planned Parenthood Will Limit Access to Care for Patients in South Carolina and Beyond
On June 26th, 2025, the Supreme Court of the United States issued its decision in Medina v. Planned Parenthood South Atlantic, finding that Medicaid enrollees cannot seek relief in federal court to enforce Medicaid’s “free-choice of provider provision.” This provision allows Medicaid enrollees to seek care from any provider that is qualified and willing to participate in the program. South Carolina’s policy barring Medicaid patients from obtaining care from clinics that provide abortion care is part of broader efforts by anti-abortion policymakers to exclude Planned Parenthood clinics from the Medicaid program, and ultimately, eliminate all federal payments to Planned Parenthood centers. Medicaid pays health care providers, including Planned Parenthood, for the delivery of health care services, but the program does not pay for abortion care except under very limited circumstances (abortions for pregnancies resulting from rape, incest or that are life-threatening).
This decision means that people enrolled in Medicaid in South Carolina, and in other states that exclude Planned Parenthood going forward, will not be able to use their Medicaid coverage to obtain any preventive services, such as contraceptive care, STI treatment and cancer screenings, at Planned Parenthood clinics. Medicaid is a major source of revenue for Planned Parenthood clinics. The loss of this revenue could result in the closure of many sites or scaling back service hours or staff and affect access for all patients, not only Medicaid enrollees. Nationally, one in three (32%) women and one in ten men (11%) have received health services from a Planned Parenthood clinic.
This case stems from a 2018 executive order issued by South Carolina’s governor that prohibited any clinic that provides abortion care from participating in the state’s Medicaid program. Planned Parenthood South Atlantic, which operates two clinics in South Carolina, and Julie Edwards, a patient who wanted Planned Parenthood to be her provider, challenged this decision to block Medicaid patients from having Planned Parenthood as their provider. The Court ruled that the “free-choice of provider” provision does not create a right enforceable by individuals under the civil right statute Section 1983 because the statute does not clearly confer an individual right. The majority opinion distinguished this case from the Court’s 2023 Talevski decision, which found a private right of action for nursing home residents, because the Federal Nursing Home Reform Act (FNHRA) includes explicit language giving residents’ rights. Without the word “right” in the Medicaid “free choice of provider” provision, the Court concluded that the provision is about states’ duties under Medicaid, but it does not confer individual rights to Medicaid enrollees to sue to get services from the participating provider of their choice.
Justice Jackson wrote a dissent, joined by Justices Kagan and Sotomayor, criticizing the majority and contesting their conclusion that because the word “right” does not appear in the free choice of provider provision, the section does not confer individual rights.
Enforcement of Free-Choice of Provider is Now Limited
The Court states that Planned Parenthood could challenge their exclusion from South Carolina’s Medicaid program through South Carolina’s administrative process and then appeal to state courts and ultimately seek review at the Supreme Court. However, the administrative process at the state level could be prolonged, and in the meantime, patients enrolled in Medicaid would not be covered for care at Planned Parenthood clinics. As a result, the clinics would likely close or reduce the scope or availability of services before the administrative process concludes.
How will this impact access to care for Medicaid patients across the country?
Many states have tried to exclude Planned Parenthood clinics from their Medicaid program, largely due to opposition to including a health care provider that also provides abortion. In the past decade, at least 14 states (AL, AR, AZ, FL, IA, ID, KS, LA, MO, MS, OK, SC, TN, TX) have used state-level policies or sought federal permission to block the provider from participating in their state Medicaid programs, though they have often been blocked by court action, until this ruling (Figure 1).

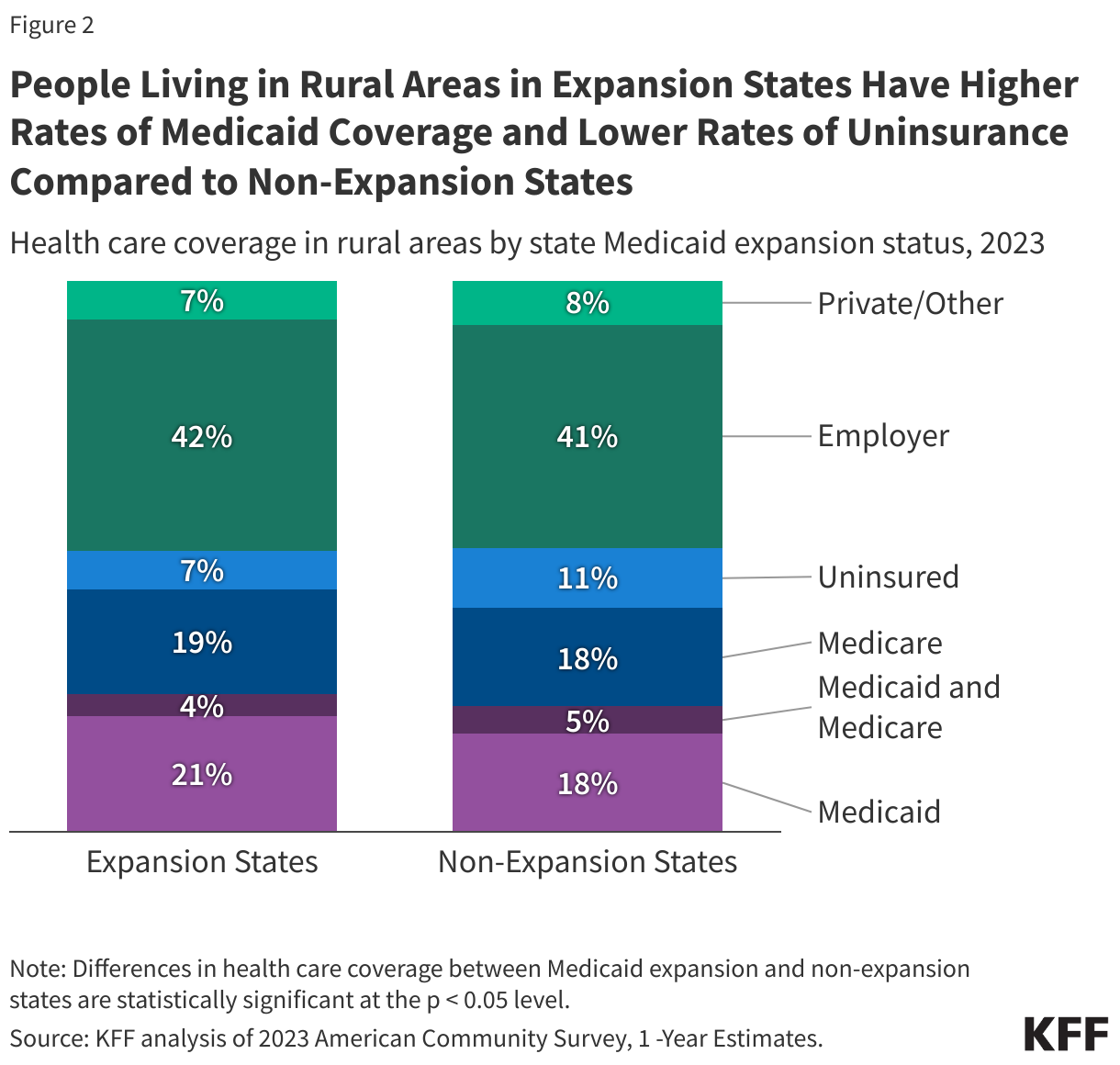
While the high court’s ruling opens the door for South Carolina and other states to disqualify Planned Parenthood from their Medicaid program, the House-approved reconciliation bill could have an even broader impact if passed by the Senate. It would ban federal health care payments by Medicaid for any services to Planned Parenthood and other providers who also offer abortion care (which is currently not covered by Medicaid) in every state. The Senate Parliamentarian is still reviewing the provision to see whether it can be included in the final Senate version of the bill or whether it runs afoul of the “Byrd Rule” and would therefore require 60 votes to pass. Regardless of the outcome, as a result of the Medina case, patients who rely on Planned Parenthood sites for their contraceptive, STI, and preventive care will be likely in some states to find themselves with fewer or no options to get that care, especially in rural or medically underserved communities where there are far fewer providers.