Key Facts About Medicare Part D Enrollment and Costs in 2022
A version of this brief with information for 2023 is available: Key Facts About Medicare Part D Enrollment and Costs in 2023
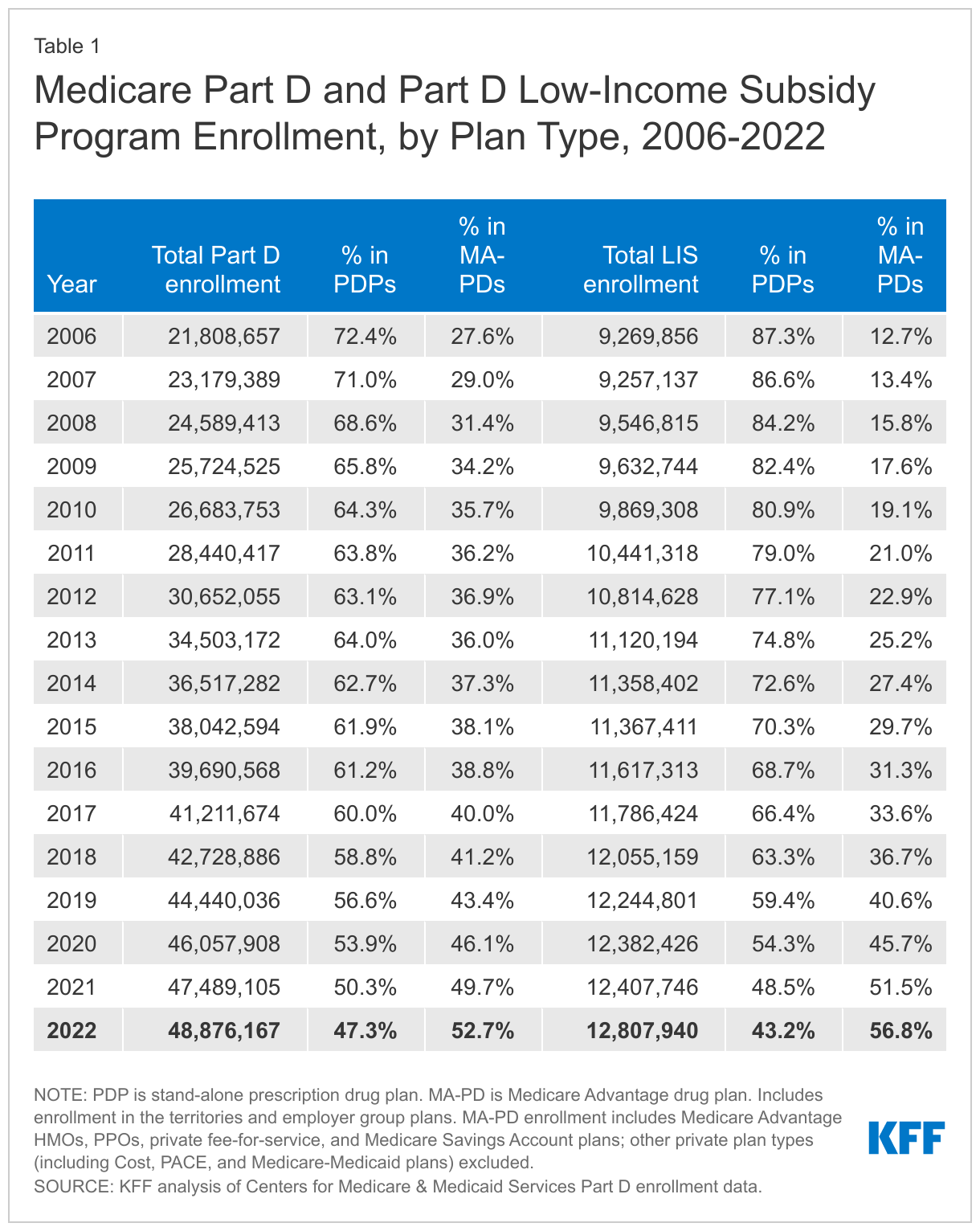
The Medicare Part D program provides an outpatient prescription drug benefit to older adults and people with long-term disabilities in Medicare who enroll in private plans, including stand-alone prescription drug plans (PDPs) to supplement traditional Medicare and Medicare Advantage prescription drug plans (MA-PDs) that include drug coverage and other Medicare-covered benefits. This analysis provides the latest data about Medicare Part D enrollment and costs in 2022 and trends over time, based on data from the Centers for Medicare & Medicaid Services (CMS).
Enrollment in Medicare Advantage drug plans has surpassed stand-alone prescription drug plan enrollment
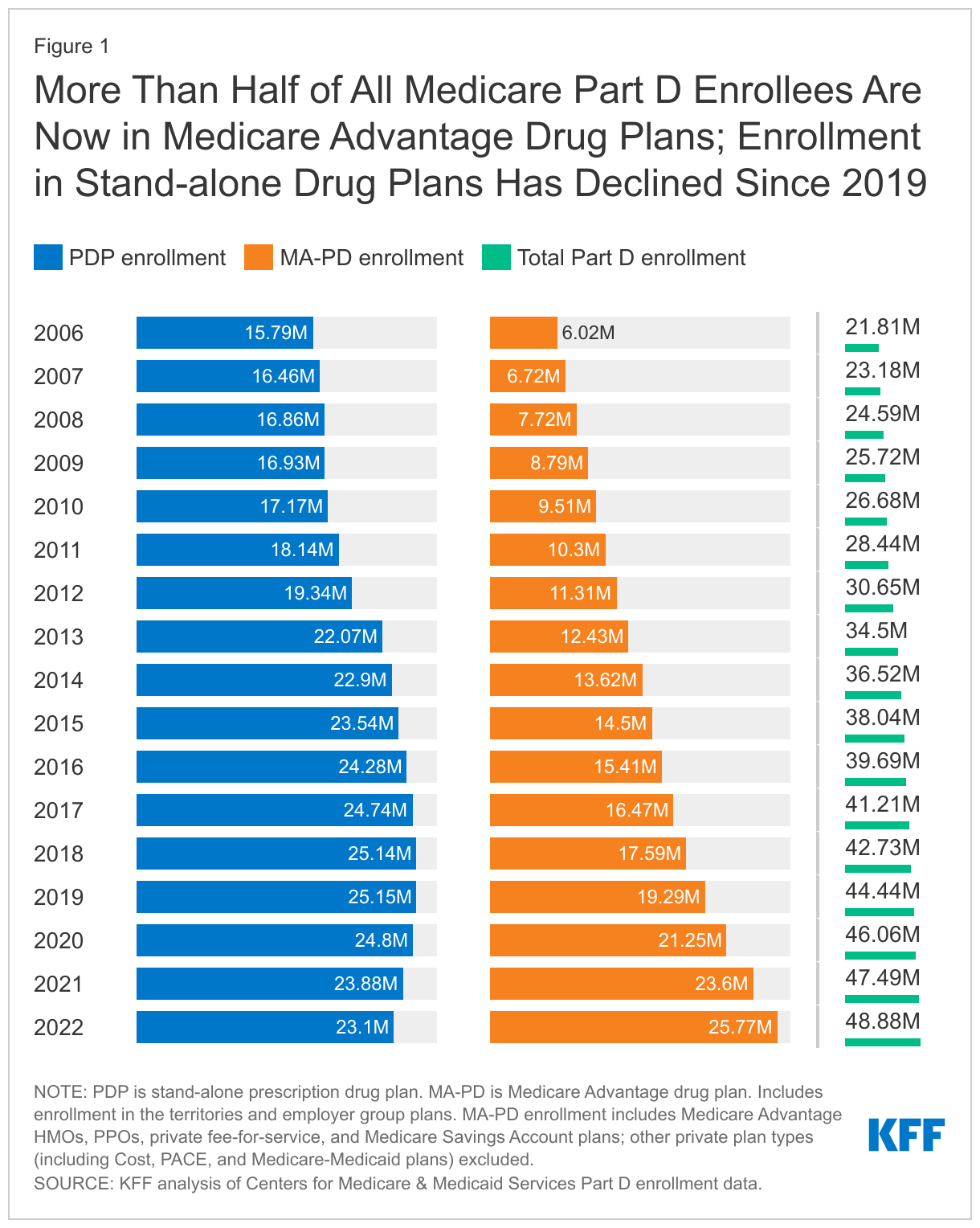
A total of 48.9 million people with Medicare are currently enrolled in plans that provide the Medicare Part D drug benefit, including plans open to everyone with Medicare (stand-alone PDPs and MA-PDs), and plans for specific populations (retirees of a former employer or union and Medicare Advantage Special Needs Plans, or SNPs).
In 2022, more than half of all Part D enrollees (53%, or 25.8 million) are enrolled in MA-PDs and 47% (23.1 million) are enrolled in stand-alone PDPs—the first year that MA-PD enrollment has surpassed PDP enrollment (Figure 1, Table 1). Over time, Part D enrollment in MA-PDs has increased, reflecting enrollment growth in Medicare Advantage plans overall, while enrollment in PDPs has decreased each year since 2019. Between 2019 and 2022, the number of MA-PD enrollees increased by 34%, while enrollment in PDPs decreased by 8%.
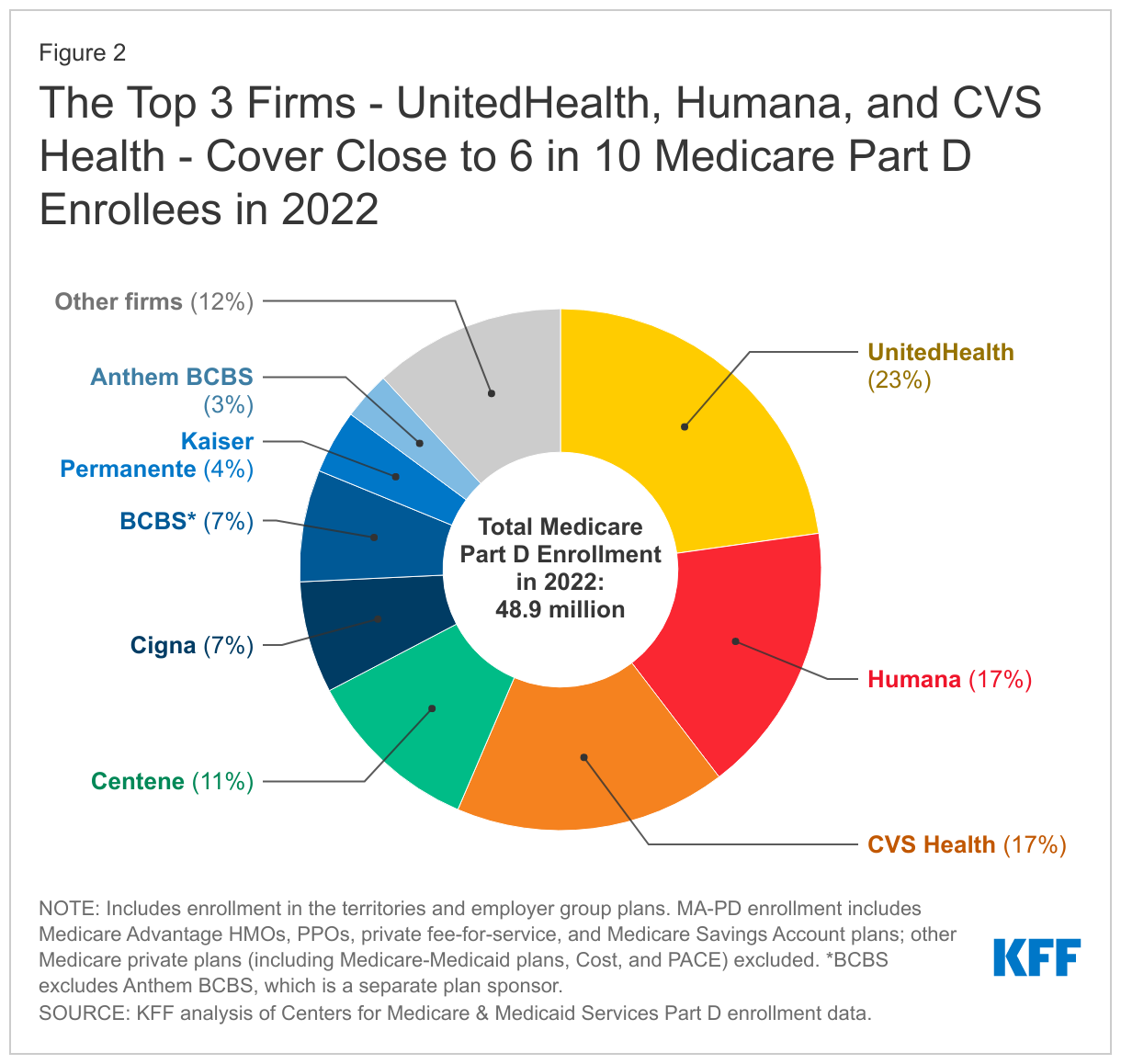
Part D enrollment is concentrated in 3 national firms – UnitedHealth, Humana, and CVS – which have a combined 57% of total enrollment
The top three firms – UnitedHealth, Humana, and CVS Health – cover close to 6 in 10 of all beneficiaries enrolled in Part D in 2022 (57%), while the top five firms – including Centene and Cigna – account for three-quarters of Part D enrollment (Figure 2). These shares are unchanged from 2021.
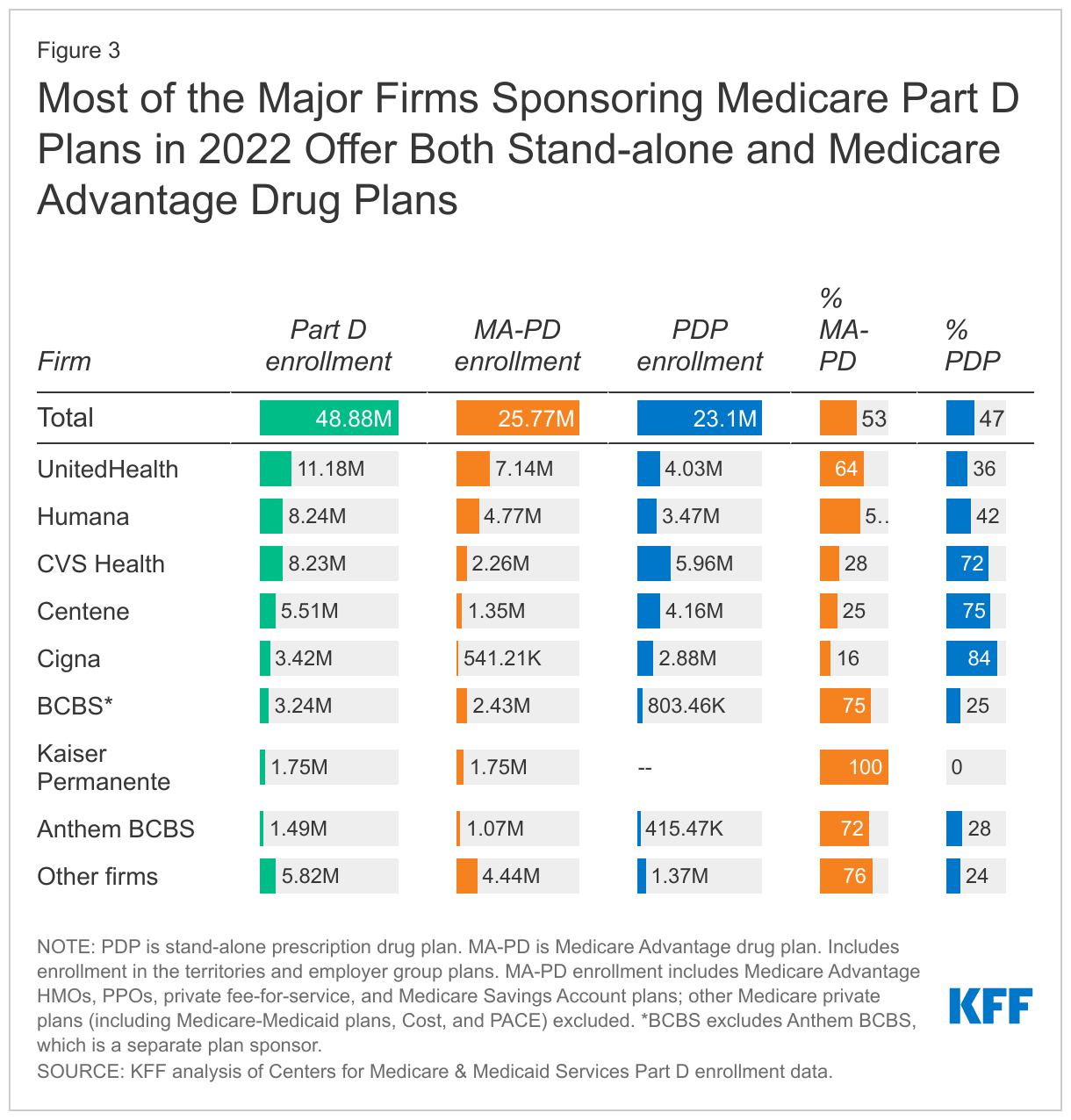
Apart from Kaiser Permanente, which exclusively offers MA plans, the top Part D plan sponsors offer both stand-alone PDPs and MA-PDs. For most firms, Part D enrollment is more concentrated in one market than the other; for example, CVS Health, Centene, and Cigna have greater enrollment in PDPs than MA-PDs, while UnitedHealth and Humana have higher MA-PD enrollment than PDP enrollment (Figure 3).
Nearly 6 in 10 beneficiaries receiving the Part D Low-Income Subsidy are enrolled in Medicare Advantage drug plans
In 2022, 12.8 million Part D enrollees (26% of all Part D enrollees) receive premium and cost-sharing assistance through the Part D Low-Income Subsidy (LIS) program. These additional financial subsidies, also called “Extra Help,” pay Part D premiums for eligible beneficiaries (as long as they enroll in stand-alone PDPs designated as premium-free “benchmark” plans) and reduce cost sharing. LIS enrollment in MA-PDs has been steadily increasing, and now totals 7.3 million, or 57% of all LIS enrollees (Figure 4, Table 1).
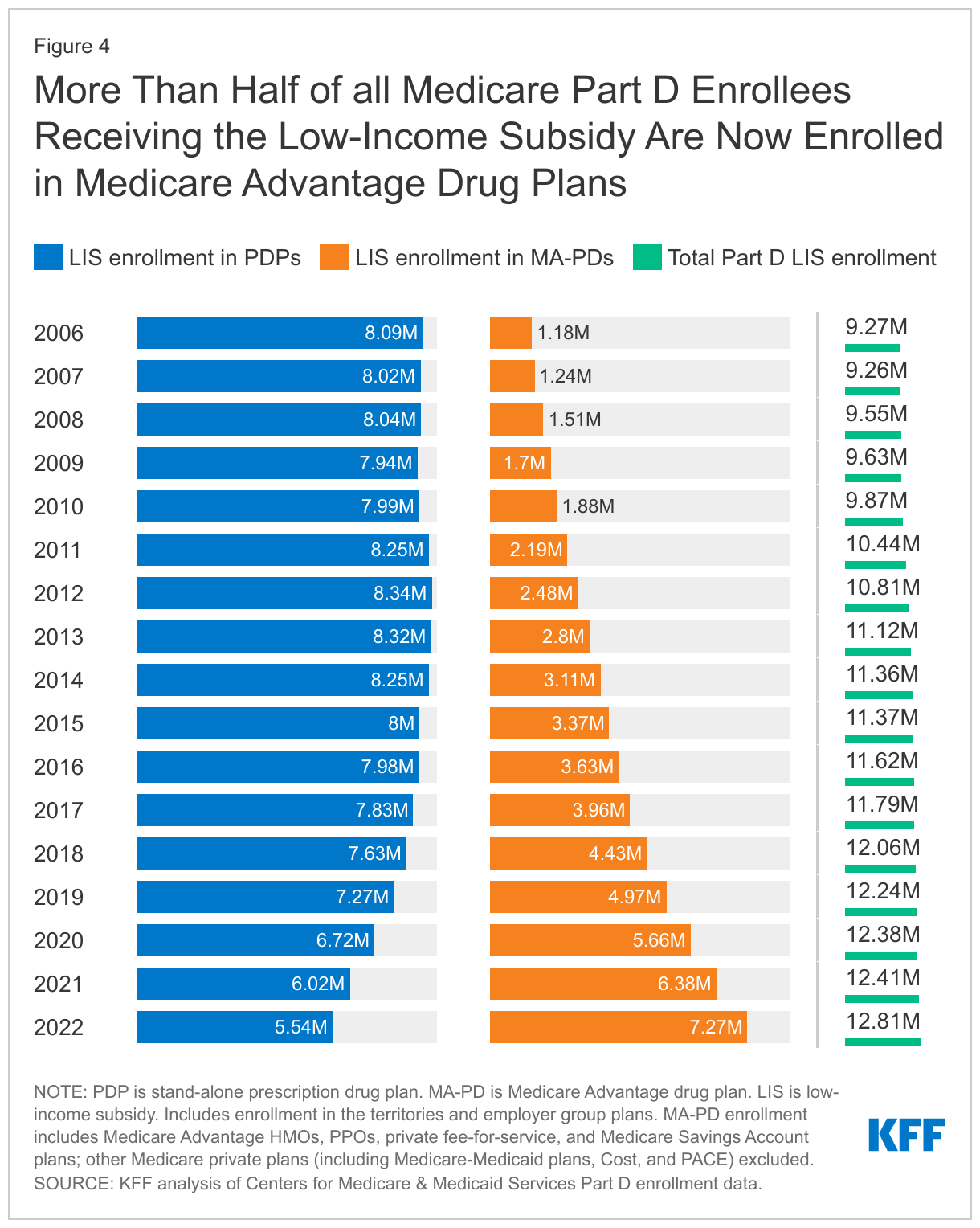
As part of increased enrollment in MA-PDs, close to one-third of all LIS enrollees (32%) are now enrolled in Medicare Advantage Special Needs Plans (SNPs), up from only 4% in 2006. Overall, 4.6 million Medicare beneficiaries are enrolled in SNPs in 2022. SNPs limit enrollment to beneficiaries with certain characteristics, including those with certain chronic conditions (C-SNPs), those who require an institutional level of care (I-SNPs), and those who are dually enrolled in Medicare and Medicaid (D-SNPs), which account for the majority of SNP enrollees.
The average monthly premium for PDPs is substantially higher than the premium for drug coverage in MA-PDs
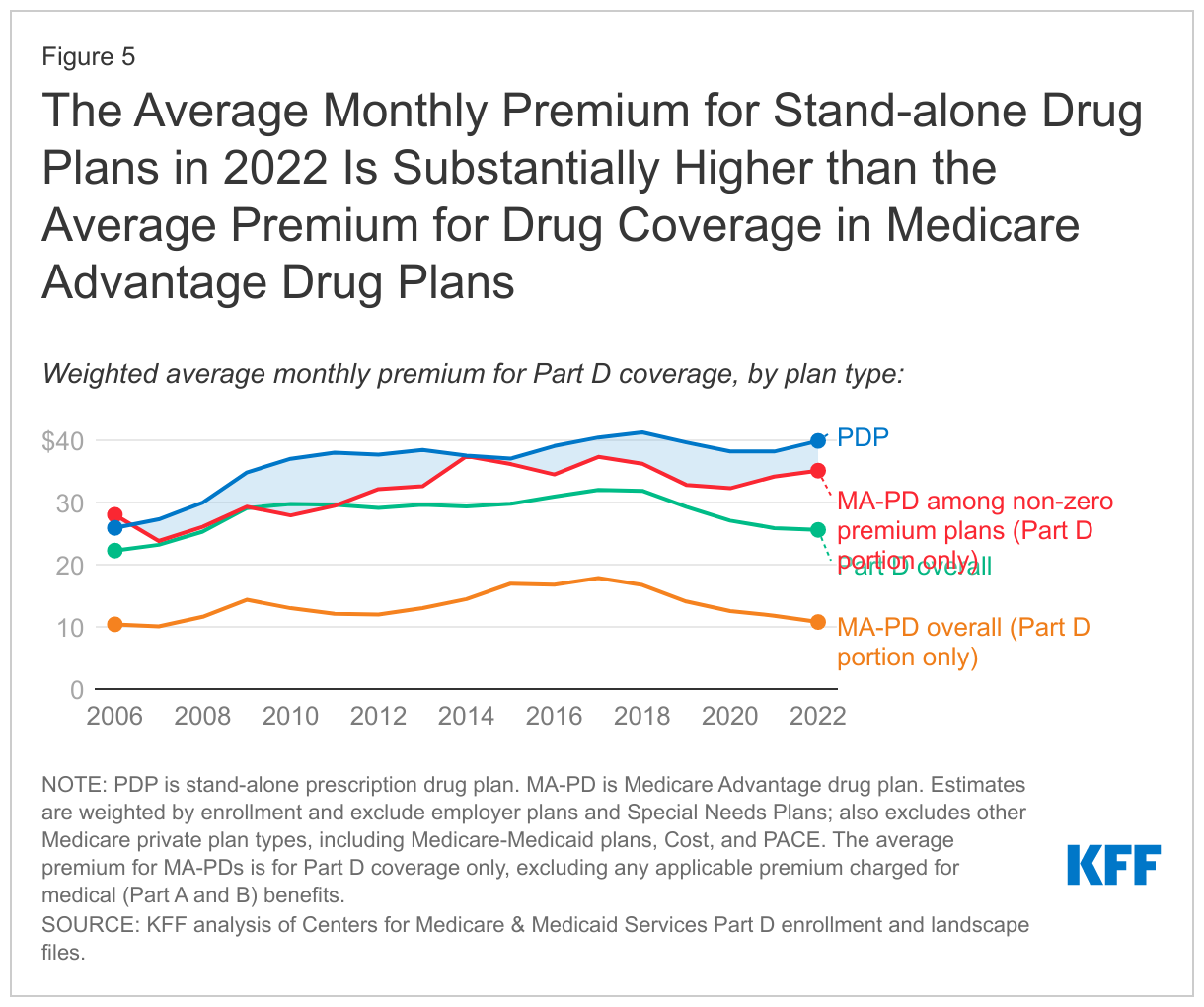
In 2022, the enrollment-weighted average monthly premium for PDPs is $40, a 4% increase from the weighted average PDP premium in 2021 ($38). The average monthly PDP premium is substantially higher than the enrollment-weighted average monthly portion of the premium for drug coverage in MA-PDs ($11 in 2022). Lower average premiums for Part D coverage in MA-PDs are mainly due to the ability of MA-PD sponsors to use rebate dollars from Medicare payments to lower or eliminate their Part D premiums. The total average premium for MA-PDs, including all Medicare-covered benefits, is $18 per month in 2022.
The calculation of the average monthly premium for Part D coverage in MA-PDs is relatively low because it includes the 69% of MA-PD enrollees in plans that do not charge a monthly premium in 2022. By comparison, all PDPs charge a monthly premium (although Part D enrollees who are receiving the full Part D Low-Income Subsidy and are enrolled in a benchmark PDP pay no monthly premium). The average enrollment-weighted premium for Part D coverage across the 31% of MA-PD enrollees in plans that charge a monthly premium is $35, which is within a few dollars of the average monthly premium for PDPs (Figure 5).
The average Part D deductible has increased for PDPs, while decreasing for MA-PDs; the 2022 weighted average annual drug deductible is 4.5 times larger in PDPs than in MA-PDs
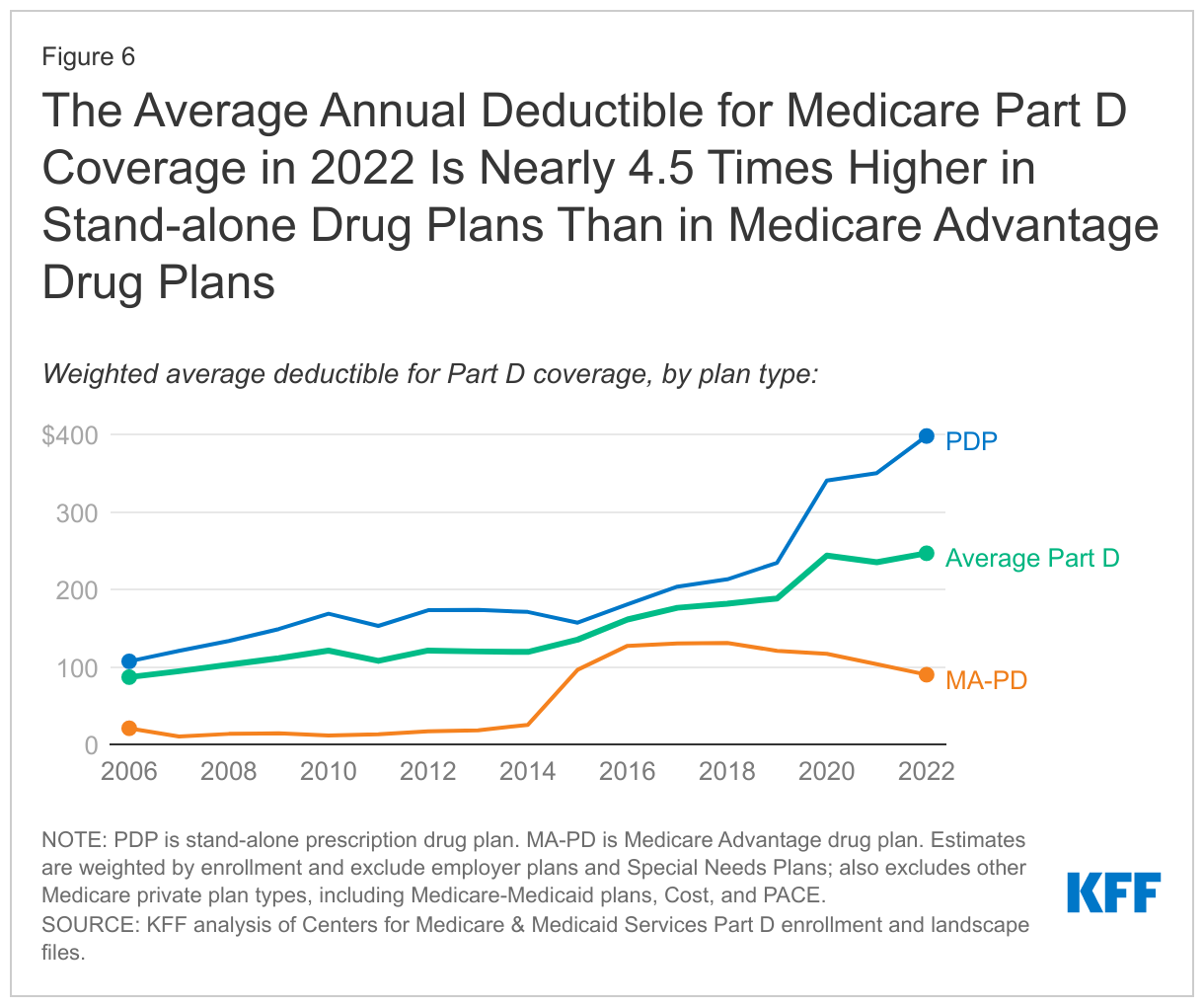
In 2022, a large majority of PDP enrollees (86%) are in plans that charge a deductible, with nearly 8 in 10 (79%) in PDPs that charge the standard amount of $480 in 2022. Conversely, 1 in 5 MA-PD enrollees are in plans that charge the standard Part D deductible, and just over half (51%) are in plans that charge no drug deductible. These enrollment patterns explain the wide divergence between PDPs and MA-PDs in the enrollment-weighted average Part D deductible amount. For PDPs, the average Part D deductible in 2022 is $398, nearly 4.5 times larger than the average drug deductible in MA-PDs ($90) (Figure 6).
Most Part D enrollees face low copays for generic drugs, higher copays for preferred brands, cost sharing up to $100 or 50% for non-preferred drugs, and 25-33% coinsurance for specialty drugs
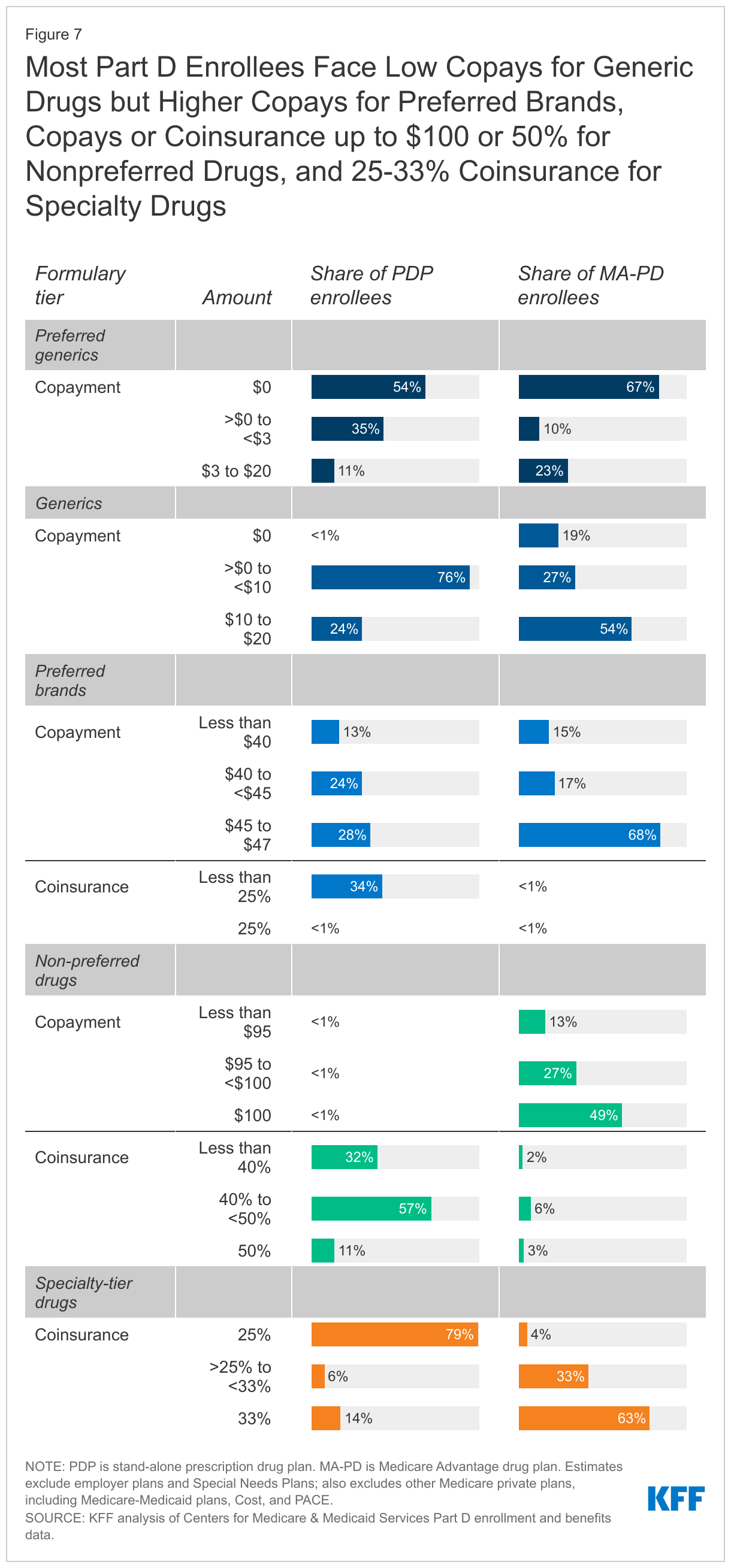
Most Part D enrollees pay low or no copayments for preferred generic drugs, but higher copays for generics not on the preferred tier. Over half of Part D enrollees (both PDP and MA-PD enrollees) pay $0 for preferred generics in 2022, but many pay $10 or more per prescription for generics that are not on the preferred tier (Figure 7). For these generic drugs, most PDP enrollees (76%) pay less than $10, while just over half of MA-PD enrollees (54%) pay between $10 and $20.
For preferred brands, virtually all MA-PD enrollees and two-thirds of PDP enrollees are in plans that charge copayments instead of coinsurance. Roughly two-thirds of MA-PD enrollees (68%) and 28% of PDP enrollees face copayments for preferred brands of $45 to $47, which is the maximum copayment amount permitted by CMS for preferred brand drugs. Another one third of PDP enrollees (34%) are in plans that charge a coinsurance for preferred brands of less than 25%, while only 1% of MA-PD enrollees pay a coinsurance for preferred brands.
For non-preferred drugs, most MA-PD enrollees (89%) are in plans that charge copayments while virtually all PDP enrollees are in plans that charge a coinsurance. For drugs on the non-preferred tier, which can be all brands or a mix of brands and generics, nearly half (49%) of all MA-PD enrollees are in plans that charge $100, the maximum copayment amount allowed by CMS for non-preferred drugs. More than half (57%) of PDP enrollees are in plans than charge 40% to less than 50% for non-preferred drugs and 11% of PDP enrollees are in plans that charge a 50% coinsurance rate, the maximum coinsurance allowed.
A larger share of MA-PD enrollees than PDP enrollees are in plans that charge the maximum 33% coinsurance rate for specialty tier drugs. For specialty tier drugs, defined by CMS as those that cost at least $830 per month in 2022, a much larger share of enrollees in MA-PDs (63%) than PDPs (14%) are in a plan that charges the maximum 33% coinsurance, while a much larger share of enrollees in PDPs (79%) than MA-PDs (4%) are in a plan that charges the minimum 25% coinsurance. Plans that waive some or all of the standard deductible – which is the case for most MA-PDs – are permitted to set the specialty tier coinsurance rate above 25%.
It is important to note that for this analysis, we did not compare which specific drugs are covered on each tier in PDPs and MA-PDs, which, in addition to the cost-sharing amounts that plans charge, would also influence enrollees’ out-of-pocket costs. Given the different cost-sharing structures adopted by MA-PDs and PDPs, particularly for non-preferred drugs, it can be difficult to compare the actual out-of-pocket costs that beneficiaries would face for different types of drugs across plan types. It can also be difficult to know how a coinsurance rate will translate into actual out-of-pocket costs without knowing the underlying list price of a drug.
Juliette Cubanski is with KFF. Anthony Damico is an independent consultant.