State Policy Choices Are Likely to Affect the Extent of Medicaid Enrollment Declines During the Unwinding Period
NOTE: This analysis, originally published on April 26, 2023, was updated on May 9, 2023 to include newer state data.
Starting on April 1, 2023, all states have begun the process of unwinding the Medicaid continuous enrollment provision. Adopted in March 2020, the continuous enrollment provision has protected coverage for millions enrolled in Medicaid during the past three years. Because states were prohibited from disenrolling people from Medicaid in exchange for enhanced federal funding, enrollment in the program has grown by an estimated 23 million to reach 95 million as of the end of March 2023. Now that continuous enrollment has ended, over the next year (and more quickly in some states), states will redetermine eligibility for everyone enrolled in Medicaid and will disenroll those who are no longer eligible, as well as those who remain eligible but who face barriers to completing the renewal process. Millions of people are expected to lose Medicaid coverage nationally.
The unwinding of the continuous enrollment provision will play out differently across the states based on policy choices states have made and variation in their administrative infrastructures. Some states have adopted multiple policies that are more likely to promote continued coverage among those who remain eligible. Others have adopted fewer of these policies, which will likely lead to a larger number of people losing Medicaid coverage, including some who remain eligible. Additionally, some states have automated eligibility systems that can more easily and accurately process renewals, reducing the number of renewals staff will have to complete manually. Having some way to order states based on their adoption of polices and strategies to promote continued coverage, as well as the capacity of their systems to process the expected volume of renewals, can be helpful for identifying where larger decreases in Medicaid enrollment are more or less likely.
Key Unwinding Metrics
Using data from a survey of state Medicaid eligibility, enrollment, and renewal policies conducted by KFF and the Georgetown University Center for Children and Families (CCF) earlier this year, we have identified 9 key metrics that will support continued Medicaid coverage during the unwinding for those who remain eligible. They include a mix of policy choices and measures of systems capacity and are grouped into three categories: renewal policies in place during the unwinding, systems for processing of renewals, and eligibility policies that promote continued coverage. The metrics include:
Renewal Policies
- State will take 12-14 months to complete all renewals
- State follows up on returned mail
- State follows up with enrollees who have not responded to a renewal request before terminating coverage
System Capacity Measures
- Processing of renewals is mostly automated
- 50% or more of renewals are completed on an ex parte basis
- State has taken steps to improve ex parte renewal rates
Eligibility Policies
- State has adopted the Medicaid expansion
- State has adopted 12-month postpartum coverage
- State has adopted 12-month continuous eligibility for all children in Medicaid and CHIP
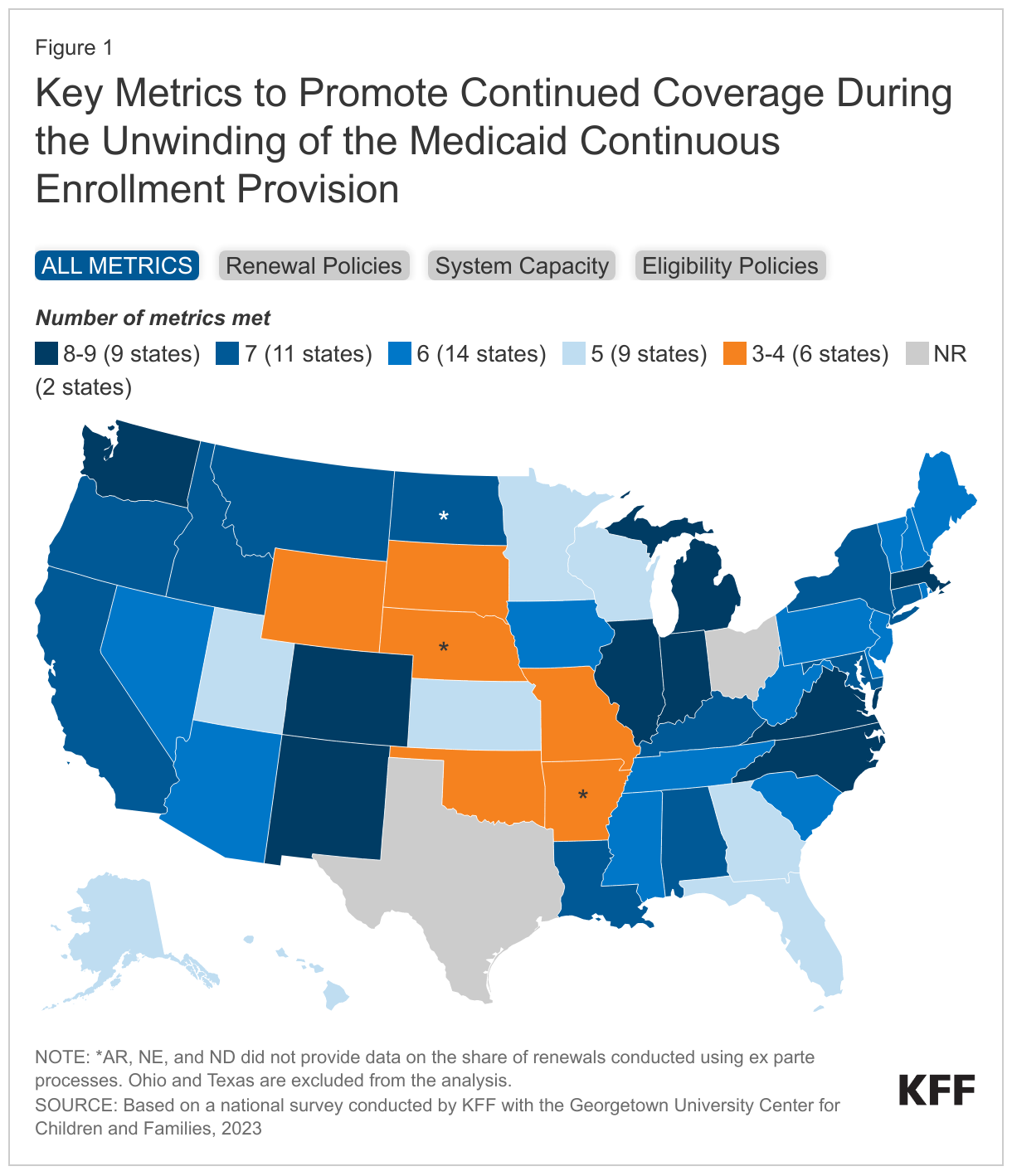
Importantly, the data included in this analysis reflect policies and procedures in place as of January 2023; it is possible, likely even, that states have updated some policies in response to guidance from the Centers for Medicare and Medicaid Services (CMS) or mitigation plans developed in coordination with CMS. In addition, some states indicated they were not processing ex parte renewals as of January 2023 and we cannot distinguish between states that paused ex parte renewals while the continuous enrollment provision was in place and those that may not have the system capacity to process ex parte renewals. Ex parte renewals involve automatically renewing coverage based on available data sources. Finally, some states did not provide data for one metric included in this analysis. States with missing data are noted in the figure below.
How Do States Compare Across Unwinding Metrics
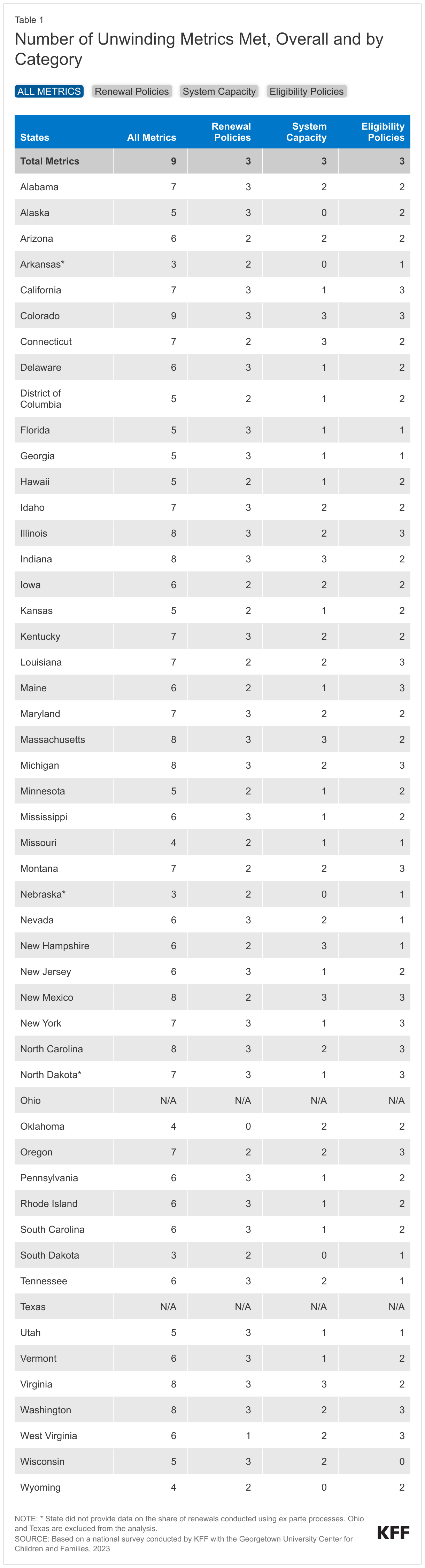
Overall, states fall along a spectrum on meeting the metrics. Nine states meet eight or more of the metrics for promoting continuity of coverage, including one state, Colorado, that meets all nine metrics. At the other end of the scale, six states meet four or fewer of the measures (Figure 1). The majority of states fall somewhere in the middle, meeting all of the metrics in some categories but not others. More states (29) meet all of the metrics related to adopting renewal policies that promote continued coverage during the unwinding than meet the standards for metrics in the other two categories (7 states for system capacity and 14 states for eligibility policies).
Most states do not have fully automated systems that are capable of completing a majority of renewals using ex parte processes. A total of 42 states do not meet all three of the metrics that measure the capacity of state systems to process ex parte renewals. The total includes 14 states that reported having mostly manual systems for processing renewals or reported processing less than 25% of renewals via ex parte despite having automated systems. The administrative burden on both staff and enrollees is likely to be higher in these states and they will likely face unique challenges as they work to complete the increased volume of renewals during the unwinding period.
Despite fairly broad adoption of the Medicaid expansion and 12-month postpartum coverage, only 14 states have adopted all three eligibility policies, which also includes 12-month continuous eligibility for all children. While these policies are not directly related to the ability to complete the renewal process, they do affect how frequently an enrollee may have their eligibility redetermined, and in the case of adoption of the Medicaid expansion, the likelihood that nonelderly adults will be able to retain coverage when their eligibility is redetermined during the unwinding period. All states will have to implement 12-month continuous eligibility for all children in both Medicaid and CHIP by January 1, 2024; however, currently, only 23 states have adopted this policy.
Implications
Unwinding the Medicaid continuous enrollment provision is expected to be challenging for all states, but state policy choices and system capacity will matter in terms of how many people are able to maintain Medicaid or transition to other types of coverage. This analysis offers one way to assess states on whether their approach to and capacity for processing renewals during the unwinding period are likely to lead to larger or smaller declines in Medicaid enrollment and can be useful for focusing monitoring efforts. However, state policies and procedures are likely evolving, and while this analysis examines state policies, how states implement those policies will be just as important a factor in how the unwinding proceeds across states. Implementation, in turn, will be affected by state staffing capacity, the effectiveness of state outreach to and communications with enrollees, and state engagement with key stakeholders, including MCOs, providers, and community organizations, to assist with enrollee outreach efforts.