Mpox One Year Later: Where is the U.S. today?
Introduction
May 18, 2023 marked one year since a case of mpox (monkeypox) was identified in the United States as a part of a new multi-country outbreak in regions where it had not previously been endemic. As a result, the World Health Organization (WHO) declared the mpox outbreak to be a Public Health Emergency of International Concern (PHEIC) on July 23, 2022 and the U.S. declared a Public Health Emergency (PHE) on August 4, 2022. Unlike prior mpox outbreaks, most of those impacted were gay and bisexual men and other men who have sex with men, including those with HIV. Furthermore, the majority of those affected in the U.S. have been people of color.
After the deployment of vaccines and treatments last summer, coupled with growing awareness of the disease, cases began to decline and both the WHO and the U.S. government have since ended their emergency declarations or allowed them to expire. Still, while cases in the U.S. continue to remain low, public health officials have expressed concern that they could rise again this spring and summer; indeed, recently, there was a small but notable outbreak in Chicago, raising questions about whether this is a harbinger for what is to come.
This brief provides an overview of the impact of mpox in the U.S. one year later, the federal response to date, and discusses the future outlook.
The 2022 Mpox Outbreak (as of May 10, 2023)
Global Cases: 87,314
US Cases: 30,395
US Deaths: 42
The impact
The 2022 mpox outbreak was not evenly distributed across the US. The majority (52%) of cases have been concentrated in the four most populous states (CA, FL, NY, and TX) – disproportionate to their share of the total population — though all states, DC, and Puerto Rico have reported at least 3 cases. In addition, almost all cases have occurred among gay and bisexual men and other men who have sex with men, differing from prior outbreaks in endemic countries.
Data from the CDC indicate that 99% of cases reported between May and July of 2022 were among men and of those, 94% were among men who had sexual contact with other men. In addition, within this group, those living with HIV have been especially hard hit. Among mpox cases with data available on HIV status, 41% were also HIV positive.
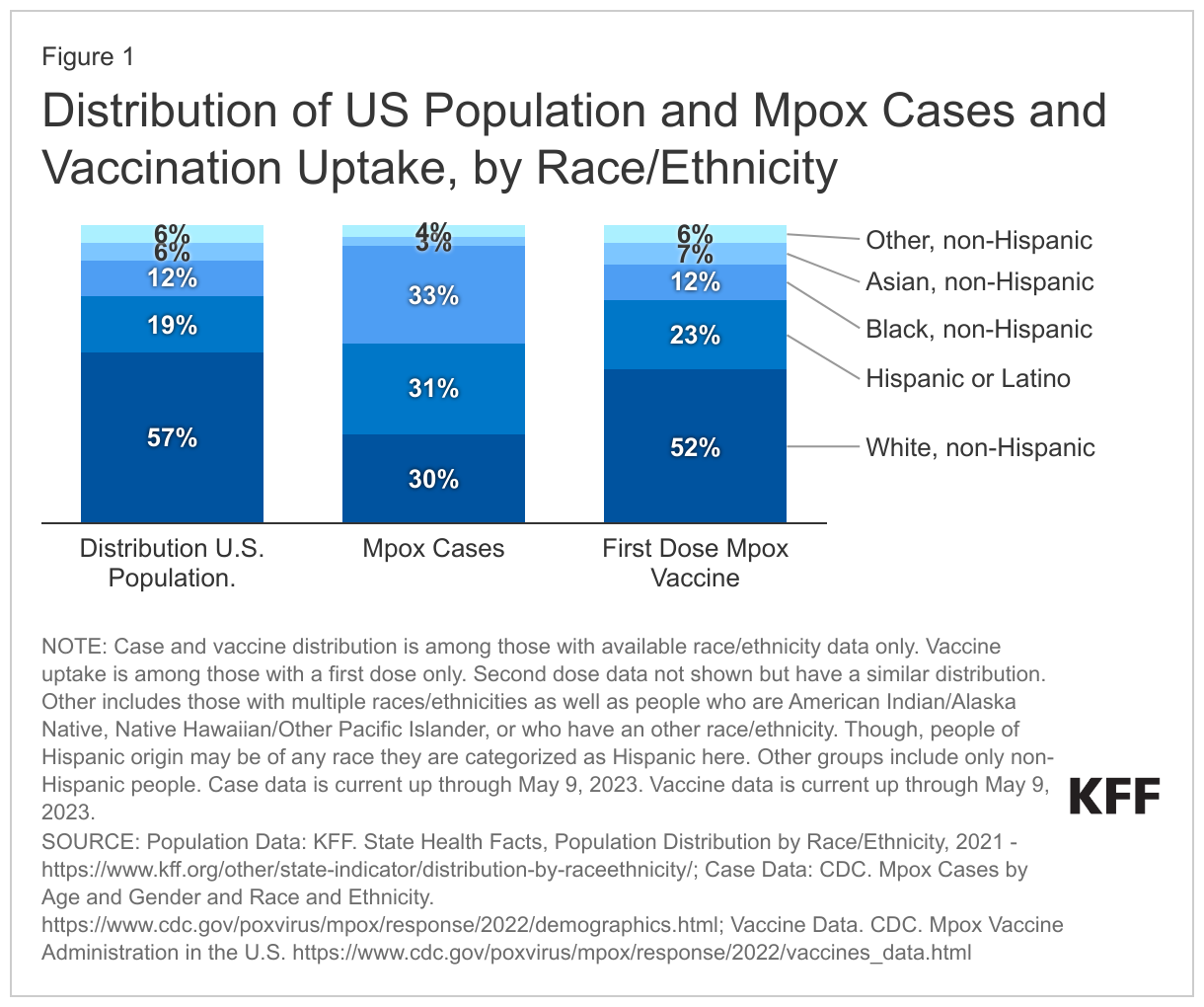
Additionally, people of color, particularly gay and bisexual men of color, have been disproportionately impacted by mpox. While Black people account for 12% of the US population, they account for 33% of mpox cases. Hispanic people account for 19% of the US population but 31% of mpox cases. There are also notable racial and ethnic disparities in deaths associated with mpox with almost all mpox deaths reported in the U.S. to date (92% of 38 deaths with available demographic data) being among Black and Latino people; some of this may have been driven by disproportionate access to mpox vaccines (see below). Further, 94% of those who died were HIV positive, not virally suppressed, and 40% were experiencing homelessness, pointing to overlapping and intersecting drivers of inequality.
Federal response to date
Coordination
After the first cases of mpox were identified in May of last year, the CDC and other agencies took initial response steps such as developing an updated case definition for mpox, providing guidance to states and other public health officials with respect to surveillance, reporting, and contact tracing, testing, vaccination, and coordinating with international partners. Some were critical that the initial response was slow and early on there were substantial hurdles related to testing and vaccine supply and accessibility. In June of 2022, the White House announced a government-wide strategy including an approach to scaling up surveillance, vaccination and testing efforts, and the CDC activated its Emergency Operations Center to enhance operational support, including monitoring and coordination. The federal government also worked to educate health care providers and the public and identify research priorities.
Today, the federal response is coordinated by the National Mpox Response Office at the White House and involves coordination across the federal government, especially within the U.S. Department of Health and Human Services (HHS) and its operating divisions and offices. These include the Office of the Assistant Secretary for Preparedness and Response (ASPR, which includes the Strategic National Stockpile under the Office of Operations and Resources as well as the Biomedical Advanced Research and Development Authority (BARDA)), the Food and Drug Administration (FDA), Health Resources and Services Administration (HRSA), and the National Institutes of Health (NIH). The White House Office of Science and Technology Policy (OSTP) also plays a role.
Testing
Testing for mpox initially took place through the CDC and other public health laboratories and was very limited, creating access challenges for patients and providers. However, capacity ramped up and eventually expanded to commercial laboratories nationwide. Testing capacity grew from 6,000 tests per week in June of 2022 to 80,000 per week by July, with expansions largely due to CDC partnering with commercial laboratories. Because newer assays under emergency use authorization (EUA) are not included in this number, capacity is potentially larger today.
Vaccination
JYNNEOS, the preferred mpox vaccine used in the U.S., has been approved by the FDA for both smallpox and mpox, and is made available to jurisdictions through the Strategic National Stockpile. JYNNEOS, a two-dose regimen, can be used following a known or likely exposure (i.e., post-exposure prophylaxis or PEP) or as a preventive measure before an exposure occurs (i.e., pre-exposure prophylaxis or PrEP).
In the early days of the outbreak, HHS began shipping what was then a very limited supply of vaccines to states on May 21, 2022, using a four-tier distribution strategy that prioritized jurisdictions with the highest mpox case rates (the U.S. had just 65,000 JYNNEOS doses in the stockpile in late June 2022). Additional doses were ordered for the 2020-2023 period, with 6.9 million doses of JYNNEOS expected to be available by mid-2023, enough to vaccinate 3.5 million people. (See our prior analysis for more details.) Recent information suggest this timeline is on track as of March 2023. Today, a jurisdictional threshold approach is being used based on each jurisdiction’s estimated percentage of the nation’s population for whom JYNNEOS vaccination is recommended; jurisdictions can order any quantity of vials up to the threshold.
HHS also maintains a store of more than 100 million doses of the ACAM2000 vaccine, a smallpox vaccine considered effective for mpox, in the strategic national stockpile. However, due to its safety profile, JYNNEOS is the preferred vaccine.
Data on vaccine efficacy against disease ranged from 66% to 86% for two doses and from 36% to 75% for a single dose, depending on the study. A separate analysis of men aged 18-49 found that mpox incidence among those who were unvaccinated was 9.6 times higher than for those fully vaccinated and 7.4 times higher than among those with a single dose.
As of May 5, 2023 more than 1.2 million vaccine doses had been administered. However, just 38% of those vaccinated had been fully vaccinated. In addition, there are significant racial and ethnic disparities in vaccine uptake. Black and Hispanic people account for a smaller share of those with first dose vaccinations than their share of cases while White people have seen a lower case burden relative to their share of the population as a whole and a higher rate of vaccination (see Figure 1). A recent analysis by CDC found that vaccination is low among those at risk, defined as men who have sex with men who have an indication for HIV PrEP. Nationwide, just 23% of the population at risk is estimated to have been fully vaccinated, with significant variation across the country, ranging from just 5% in West Virginia to 67% in Washington, D.C.
Treatment
There are no available treatments that specifically target the mpox virus. However, because the smallpox and mpox viruses are similar, Ticoviromat (TPOXX), an antiviral approved for smallpox, is used to treat severe mpox cases. TPOXX is prescribed for mpox treatment under an expanded access Investigational New Drug (EA-IND) protocol and available from the strategic national stockpile at no cost. On July 1, 2022, HHS reported that the strategic national stockpile had over 1.7 million TPOXX antiviral treatment courses. Through January 2023, 6,832 patients with mpox has been treated with TPOXX.
Because TPOXX for mpox is only available under an EA-IND protocol through the CDC, access can be challenging. Initially, there were many reports of providers facing lengthy and burdensome processes in accessing treatment, creating a barrier for patients and a challenge for provider. In response CDC streamlined the approval process, though it still can take some time for providers to navigate.
In an effort to promote equitable access, jurisdictions can also request oral TPOXX using a threshold approach. TPOXX thresholds are formula driven: 75% is based on the number of jurisdictional cases and 25% on the number of individuals at the highest risk.
Federal Funding
New federal funding to address mpox has not been appropriated by congress, though the White House requested $4.5 billion in the FY23 omnibus spending bill.
Given the lack of new federal investment, agencies have had to use existing resources to fund response activities. For example, CDC has allocated funding to jurisdictions on two occasions through its Public Health Crisis Response Cooperative Agreement: once in December 2022 when $12.5 million was awarded to 21 jurisdictions for vaccination and other mpox response activities and again in January 2023 when $33.7 million was awarded to 53 jurisdictions to respond to remaining cases, prevent future outbreaks through vaccination efforts, and strengthen capacity to respond to future cases. In addition, several agencies, including the CDC and HRSA’s Ryan White HIV/AIDS Program, provided guidance around flexibilities to allow grantees to use existing funding to address mpox. Federal investments have also been directed to mpox research activities across a range of government programs/agencies.
Surveillance
In partnership with states and local jurisdictions, CDC plays the central federal role in mpox surveillance. Jurisdictions collect data which is then reported to and combined by the CDC. CDC then provides surveillance data and reports on a range of variables including:
- Cases, including by patient demographic and trends.
- Vaccination, including on administration, coverage, and effectiveness.
- TPOXX Treatment
- Wastewater surveillance
Public communication and partnerships
The communication to the public and providers around mpox has largely come out of CDC. HHS’ Office of Infectious Disease and HIV/AIDS Policy, the Health Resources Services Administration (HRSA) - especially within the Ryan White Program - have also played a role.
CDC has provided public education materials to jurisdictions, providers, and individuals though webinars, website materials, and engagement at local events. This includes equity tool kits for local outreach and messaging specifically aimed at the hardest hit communities and communities of color in an effort to address racial/ethnic disparities. CDC also engaged with on the ground partners as part of its vaccine equity pilot project aimed at reducing vaccine inequalities). Applications are now closed but in total 28 applications from 14 states and Puerto Rico were accepted, grouped by two strategies: vaccination events developed to reach specific populations disproportionately affected and vaccination events with a broad reach (though still generally targeting hard hit communities). Examples for projects include events at Southern Decadence and Atlanta Black Pride to provide vaccines and education though community engagement and targeted messaging.
Communication from HHS’ Office of Infectious Disease and the Ryan White Program has focused on the syndemic nature of mpox, HIV, and other STIs. The Ryan White Program has provided education for providers and jurisdictions, flexibility with its grants to respond to mpox, and distributed vaccination through grantees dually funded by Ryan White and HRSA Health Centers.
(In addition, there have been several private sector efforts to address communications gaps such as the mpox education and awareness resources developed by KFF's Greater Than HIV program).
The Chicago outbreak and the future outlook nationwide
Overall mpox cases in the U.S. remain low but public health officials are monitoring whether there might be a surge of cases as we move into warmer months, a time often associated with more social gatherings and warned of a possible resurgence.
A recent outbreak in Chicago was reported via an alert from the city and raised concerns that this could occur. The alert stated that between mid-April and early May 2023, 13 confirmed or probable mpox cases had been identified in the city (compared to many weeks in February and March when the city reported no cases). Moreover, most cases were among those fully vaccinated, raising questions about vaccine effectiveness, and one-third were among virally suppressed people with HIV. Since this alert was published, more cases have been reported.
It is not yet known what the rest of the year will look like. There could be isolated local outbreaks as has occurred in Chicago or transmission could become more widespread, especially as vaccination lags in terms of initial uptake and second dose completion and potential wanning efficacy. On May 15, 2023, CDC released a Health Alert Network (HAN) message in response to the Chicago outbreak writing that the “spring and summer season in 2023 could lead to a resurgence of mpox as people gather for festivals and other events” and highlighting the important role vaccines play in potentially warding off more serious infection, even if full protection is not provided.
Separately, CDC estimates that if mpox is reintroduced and no additional risk mitigation occurs (i.e. vaccination or behavior changes), the risk of a resurgent outbreak is more than 35% in most jurisdictions and that such outbreaks could be large given that immunity among those most at risk is low.
Discussion
Overall, the public health system for addressing mpox in United States is in a markedly different place than it was one-year ago and is expected to be better able to respond should mpox cases rise. Additionally, providers are generally more knowledgeable about case identification and treatment and the communities most impacted have a better understanding of how to protect themselves, if cases climb.
However, disparities persist and those facing structural barriers and overlapping systems of discrimination -- including LGBTQ people, people of color, those with HIV, and people experiencing homelessness -- are particularly at risk. Building on lessons learned, including in terms of preparedness, coordination, engagement of hard-hit communities and leveraging an equity framework, will be important both to address lingering inequities today and to respond to potential future outbreaks tomorrow.