National Data Show Continuing Disparities in Monkeypox (MPX) Cases and Vaccinations Among Black and Hispanic People
The current MPX outbreak in U.S. appears to be slowing down, following its emergence in May and rapid acceleration in June, with most cases having been reported among gay and bisexual men and other men who have sex with men. Cases peaked in August and have recently begun to decline, largely attributed to the deployment of MPX vaccines and to behavior change among those at higher risk. However, disparities in cases persist among Black and Hispanic people, a pattern also seen with HIV and COVID-19. Indeed, new cases among Black people began to exceed those among White people by early August and, while also trending down, have remained consistently higher. Moreover, although Black and Hispanic people account for a disproportionate share of cases relative to their share of the population, they account for a smaller share of vaccinations, which could pose challenges to addressing MPX in these communities moving forward. Finally, ongoing data limitations may hinder the public health response and efforts to mitigate these disparities.
This analysis examines MPX cases and vaccinations by race/ethnicity based on national data obtained from the Centers for Disease Control and Prevention (CDC). Data on race/ethnicity of people with MPX were available for 68% of cases reported as of September 23 (16,847 of 24,846 cases) in all 50 states, the District of Columbia, and Puerto Rico. Data on race/ethnicity of people who have received a first dose of the two-dose JYNNEOS MPX vaccine were available for 91% of vaccinations reported as of September 27 by 51 jurisdictions (526,692 of 576,420 doses). We find that:
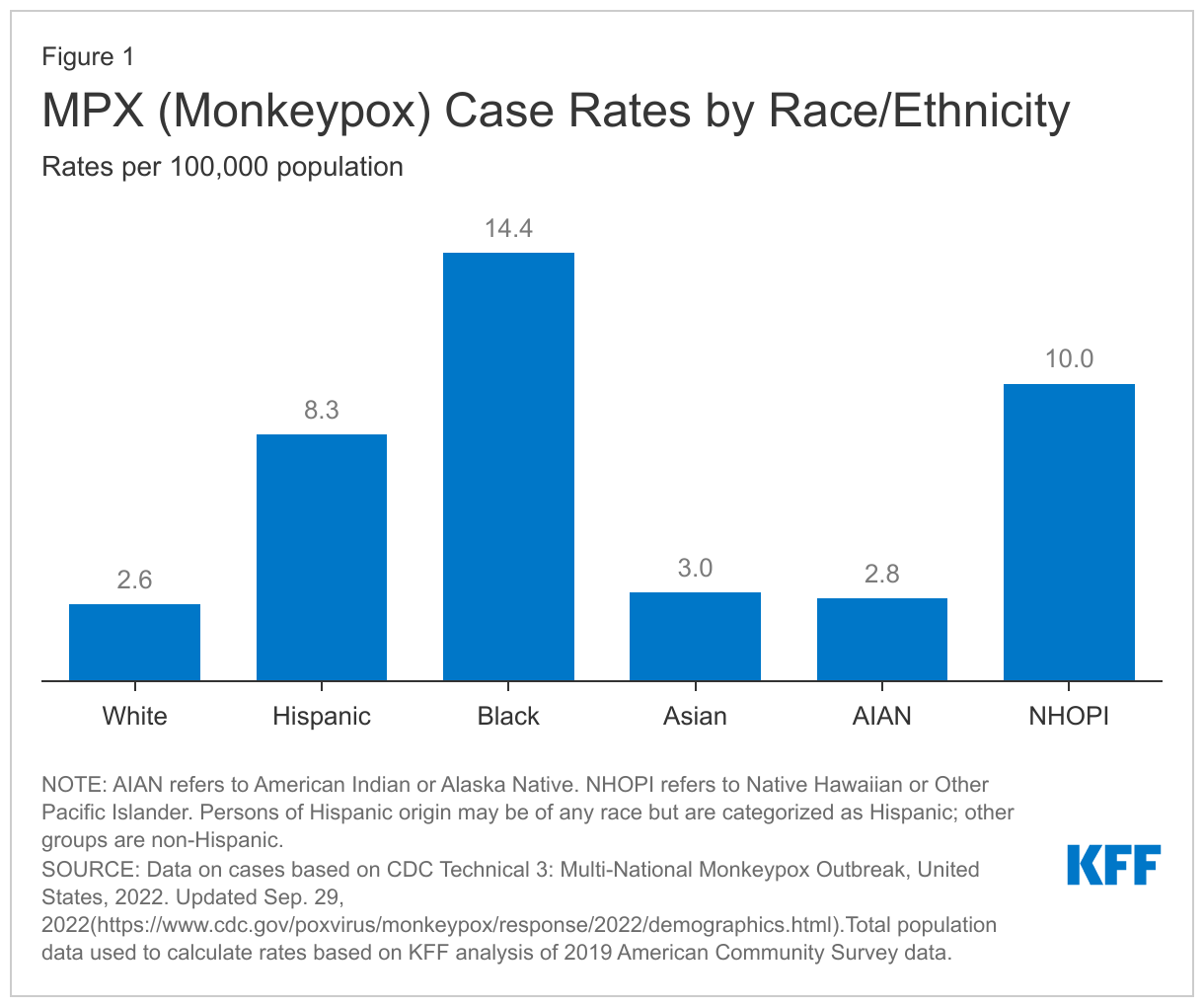
MPX case rates among Black people are over five times those of White people (14.4 vs. 2.6 per 100,000) (Figure 1). Native Hawaiian and Other Pacific Islander (NHOPI) and Hispanic people also have significantly higher rates of reported MPX cases at 10.0 and 8.3 per 100,000, respectively. Rates are lower and similar for Asian (3.0 per 100,000), American Indian and Alaska Native (AIAN) (2.8 per 100,000), and White (2.6 per 100,000) people.
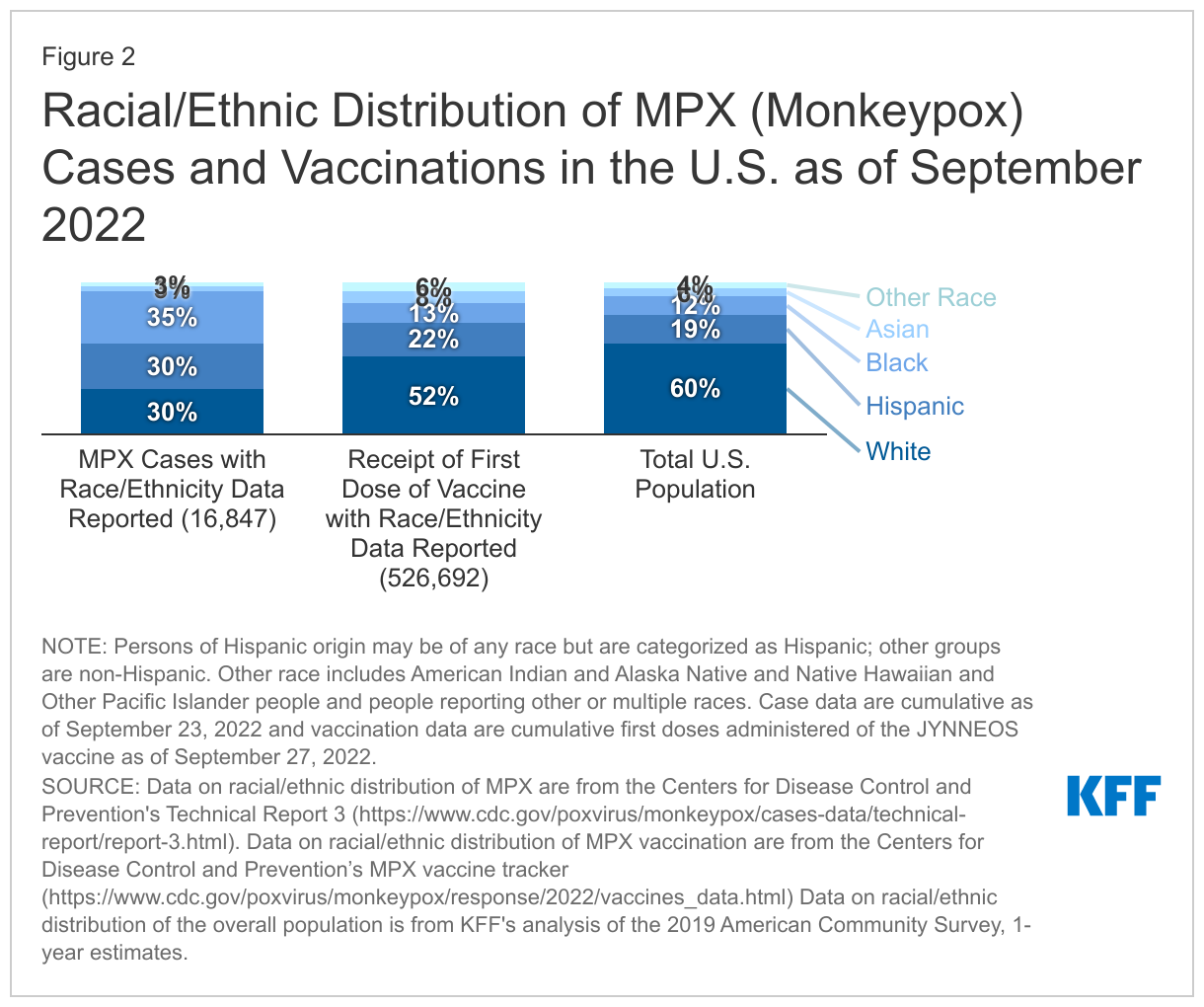
Overall, Black people account for the largest share of MPX cases, and both Black and Hispanic people account for larger shares of cases compared with their shares of the population (Figure 2). Of those with known race/ethnicity, 70% or 11,820 of cases are among people of color, while people of color account for 40% of the U.S. population. Black people account for more than a third (35% or 5,847) of cases, which is almost three times their share of the U.S. population (12%). Hispanic people account for 30% or 4,996 of cases, which is 1.6 times their share of the U.S. population (19%). By contrast, White people account for 30% or 5,027 of cases and 60% of the U.S. population. Asian people represent 3% or 549 of cases, which is smaller than their share of the population. Less than 1% or 117 of reported cases with available race/ethnicity data were among AIAN or NHOPI people, while the remaining 2% or 311 of cases were among individuals reporting other or multiple races.
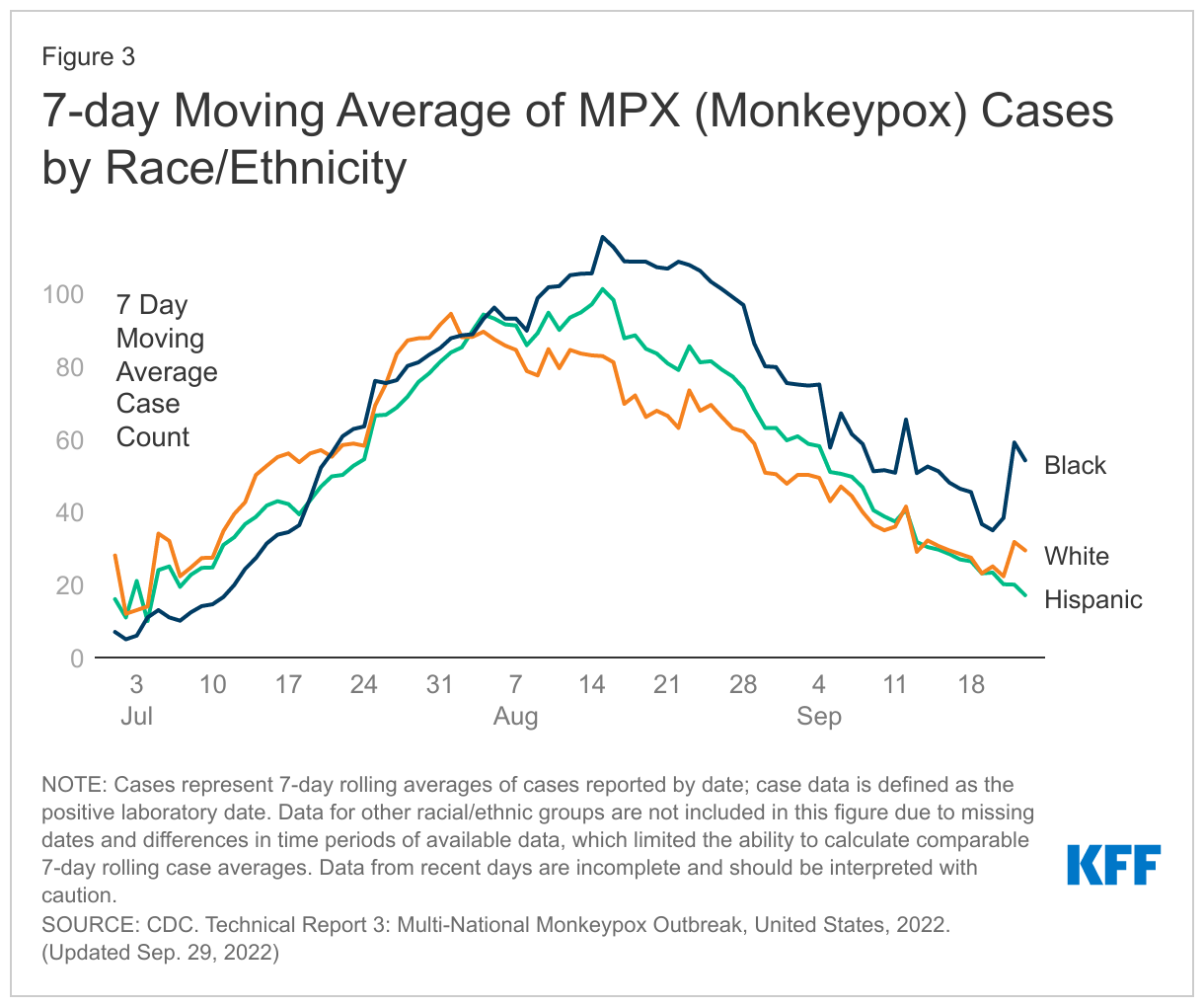
By late summer 2022, the number of new MPX cases among Black and Hispanic people surpassed the number among White people. Based on the 7-day rolling average of newly reported cases with race/ethnicity data, the number of new cases among Black people first surpassed those among White people on July 21, and, after some fluctuation, has remained consistently higher since August 2 (Figure 3). The 7-day rolling average of new cases reported among Hispanic people surpassed that among White people on August 3 and remained higher until recently. The average number of new cases among Asian, AIAN, and NHOPI people has remained lower than the number among White people over the period examined. While new cases have begun to fall across all racial and ethnic groups, they remain highest among Black people; new cases among Hispanic people have fallen below those among White people.
Black and Hispanic people have received smaller shares of MPX vaccines compared to their shares of cases. The deployment of effective MPX vaccines has been identified as one key factor contributing to the decline in cases. As of September 27, over half (51%) of MPX first doses of vaccinations have gone to White people, although they represent 30% of reported cases (Figure 2). In contrast, despite accounting for more than a third of cases (35%), only 13% of first doses administered went to Black people. Similarly, 22% of first doses have gone to Hispanic people, while they account for 30% of cases. The lower shares of vaccinations among these groups may in part explain why they have had higher numbers of new cases and complicate efforts to address disparities moving forward.
Ongoing data limitations may hinder the public health response and efforts to mitigate these disparities. The ability to monitor MPX cases and vaccination by race/ethnicity provides key measures of where disparities exist and could help to focus outreach and resources to hard hit communities. However, data limitations make tracking these demographic patterns challenging. These include missing race/ethnicity case data for almost a third (32%) of reported cases and for one in ten vaccinations (9%) the lack of available data to allow for intersectional analysis of disparities across multiple factors, such as by race/ethnicity, sex, gender identity, and risk; and the lack of state-level demographic data. Moreover, national-level data by risk factor are increasingly missing from jurisdictional reports to CDC, limiting an assessment of risk for current cases.
Together, these data indicate that there are significant disparities in MPX cases among Black, NHOPI, and Hispanic people, with case rates among Black people more than five times greater than those among White people. Moreover, to date, Black and Hispanic people have received lower shares of vaccinations compared to their shares of MPX cases. These disparities likely result from multiple factors, including structural barriers, which complicate access to information and interventions and contribute to more limited access to health care overall; stigma and homophobia, which may make some reluctant to seek care or be offered services; and data challenges which may delay or obscure recognition of the full scope of the impact of MPX among people of color. These findings highlight the importance of centering intersectional equity in MPX response efforts, including prevention, testing, and treatment. As has been seen with HIV and COVID-19, underlying structural inequities place people of color at increased risk for public health threats and focused efforts will be key to minimizing and preventing further disparities going forward. While the federal government has begun piloting efforts to reach communities of color with MPX vaccines in order to address disparities, it is unclear if such efforts will be enough to stave off further disproportionate impact, and much will also depend on what state and local jurisdictions do.